
Submitted:
29 September 2023
Posted:
30 September 2023
You are already at the latest version
Abstract
The Peripheral giant cell granuloma (PGCG) is an asymptomatic, non-neoplastic and proliferative lesion of unknown etiology. Some possible pre-disposing factors such as hormonal changes dur-ing pregnancy, have been suggested. However, the association between PGCG and pregnancy is controversial. There are few reported clinical cases of pregnancy-associated PGCG in the litera-ture, and they occurred only in the lower jaw. The present report is on a 35-year-old female pa-tient at 36 weeks of gestation who presented with a PGCG in the central and lateral incisors of the upper jaw. The management consisted of surgical excision, along with curettage of the affected bony walls. The diagnosis was based on clinical results and imaging examinations, and it was histopathologically confirmed. The patient underwent postoperative follow-up evaluations at 3, 6 and 12 months, and there were no signs of recurrence.
Keywords:
Peripheral giant-cell granuloma
; giant-cell epulis
; giant- cell hyperplasia
1. Introduction
Peripheral giant cell granuloma (PGCG) is the most common oral giant cell lesion. It appears as an extraosseous soft tissue nodule that originates from the connective tissue of the periosteum or the periodontal ligament membrane, and it is localized within the soft tissues [1,2,3,4]. This pathology is identified by other names such as giant cell reparative granuloma, osteoclastoma, giant cell epulis, and giant cell hyperplasia of the oral mucosa [5].
The lesion has a predilection for the lower jaw rather than the upper jaw, particularly in the anterior area [3,6]. It is frequently located in the interdental papilla, the edentulous alveolar ridge, or the marginal gingiva in totally or partially dentate patients, resulting in alterations in the gingival contour [4,7]. It is more common in women than in men, with a 2:1 incidence ratio, and the incidence is higher in the age group of 30 - 50 years [3,5,6,8]. The symptoms of PGCG are highly variable. In most cases, the lesion is asymptomatic, but symptoms do arise when it interferes with occlusion or is associated with an infectious or ulcerative process [3,4,5]. The size of the lesion may vary from a small papule to a massive enlargement which does not typically exceed a diameter of 2 cm [3,9]. However, lesions larger than 5 cm have also been reported, and their growth have been linked to factors such as poor oral hygiene and xerostomia [3,10]. In some cases, progressive growth may lead to significant tumors that compromise speech, chewing, or swallowing, with evolution time ranging from three months to four years [3].
Although the etiology of PGCG is still uncertain, some possible contributing factors, such as hormonal changes during pregnancy, have been suggested. However, due to the limited number of clinical cases described in the literature, the association between PGCG and pregnancy is controversial [11,12,13]. The objective of this study was to describe the surgical management of a clinical case of upper jaw PGCG associated with pregnancy.
2. Case Report
A 35-year-old female patient without systemic compromise, presented with an increase in volume in her gum near the upper lip that caused difficulty in chewing. The patient stated that the growth appeared during the 36th week of gestation. However, she refrained from seeking dental care until a week after terminating her pregnancy due to concerns about the impact of anesthetic dental procedures on her baby. We spoke with her and cleared her doubts regarding the risks of dental care, while emphasizing the importance of identifying an injury in its early stages.
Intraoral clinical examination identified an increase in volume of gum (measuring 1.0 cm x 0.7 cm x 0.3 cm) located between the central and upper left lateral incisors, and partially covering the vestibular surfaces. On palpation, the area presented a soft consistency, a rough texture, an oval base with slight mobility, and a pink coloration with irregular margins, but without bleeding or pain (Figure 1). Radiographic investigations did not reveal any signs of bone loss, root resorption, or increased periodontal ligament space (Figure 2). Based on the information obtained from the historical, clinical, and radiographic examinations, a presumptive diagnosis of pyogenic granuloma or PGCG was considered. The treatment consisted of removing the lesion along with a margin of healthy tissue under local anesthesia, followed by curettage of the adjacent fibers. Additionally, a slight milling of the alveolar bone was performed to remove irritating factors (Figure 3). Oral prophylaxis was performed using an ultrasonic device and Gracey 1-2 curettes to eliminate local irritants on adjacent teeth. Postoperative instructions were provided at the end. The sample obtained was fixed in 10% formalin prior to routine histopathological examination (Figure 4).
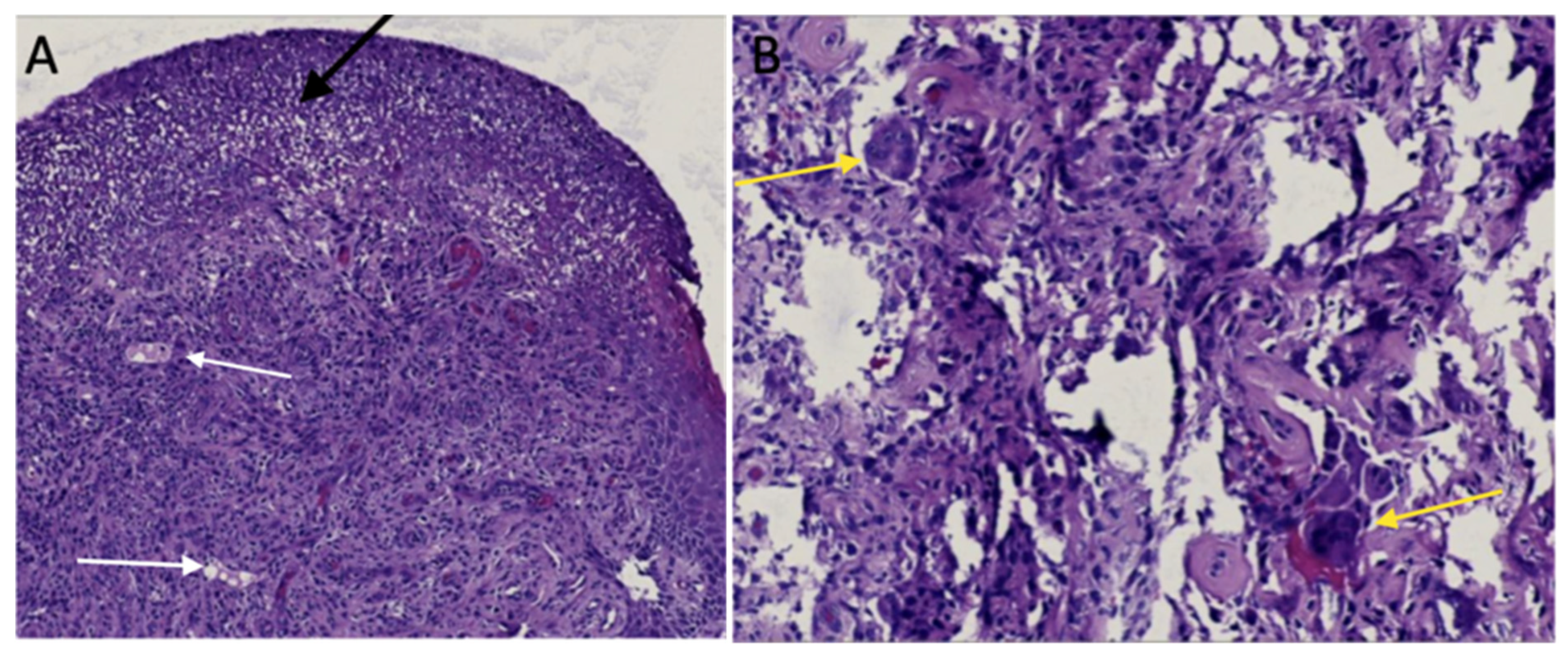
Histological analysis showed proliferation of granulation tissue (Figure 5). The benign enlargement consisted of numerous vascular and lymphatic spaces of different calibers (white arrow), some of them were congestive hemosiderin deposits, moderately diffuse and mixed inflammatory infiltrates comprising plasma cells, lymphocytes, histiocytes and polymorphonuclear cells, as well as multi-nucleated osteoclast-type giant cells (yellow arrow), containing two or more than ten nucleiome of these cells had pyknotic nuclei, with stroma containing abundant collagen fibers arranged in a lax and irregular manner. Additionally, in some areas, multiple spindle cells and presence of reactive bone tissue were recognized. The covering epithelium was of the stratified squamous para-keratinized type which exhibited loss of continuity, with deposits of eosinophilic material compatible with fibrin (black arrow). These characteristics corroborated the presumptive diagnosis of peripheral giant cell granuloma. Follow-up evaluations at 3, 6 and 12 months were implemented, during which satisfactory clinical conditions were observed, without recurrence.
3. Discussion
Peripheral giant cell granuloma (PGCG) is an exophytic, extra-osseous, non-neoplastic pathology that originates in the periosteum or periodontal ligament [1], The etiology of PGCG is unknown. However, it may be related to trauma, inflammatory foci, nutritional impact, maladjusted restorations, overextended fillings, occlusal trauma, genetic predisposition, dental calculus, and use of orthodontic appliances [3,5,14]. Moreover, hormones have been considered as contributing factors, although this association is controversial. To our knowledge, only three clinical cases of pregnancy-associated PGCG have been described in the lower jaw [11,12,13]. This study has described the first clinical case of pregnancy-associated PGCG in the upper jaw.
The roles that sex hormones play in pregnancy in relation to the initiation, development, and progression of PGCG, are controversial. During pregnancy, hormonal changes, particularly those involving estrogen and progesterone, promote alterations in the oral cavity. These changes encompass vascular, microbiological, and cellular modifications, and they create a favorable environment for the initiation and development of various pathologies [15,16,17,18]. In 2017, Silva de Araujo reported that changes that occur in the microcirculatory system during pregnancy involve swelling of endothelial cells, increased adhesion of platelets and leukocytes to vessel walls, formation of microthrombi, alteration in perivascular mast cells, increased vascular permeability, and vascular proliferation [15]. Estrogen and progesterone, in association with inflammatory mediators, may induce changes in vascular responses and turnover of connective tissue in the periodontium, leading to higher prevalence of inflammatory processes during periods of hormonal fluctuation. The oral microbiota undergoes a series of changes, particularly increases in populations of aerobic and anaerobic bacteria such as Porphyromonas gingivalis, Bacteroides melaninogenicus, and Prevotella intermedia [15]. In the gingiva, these bacteria affect target cells such as keratinocytes and fibroblasts. Characteristically, the cellular changes in the gingival epithelium comprise decrease in keratinization, increase in glycogen content, proliferation of fibroblasts, and blockage of collagen degradation. These changes lead to alterations in the epithelial barrier which consequently result in greater responses to irritants, especially in the dental biofilm. [17]. Additionally, there is decreased antimicrobial activity of peripheral neutrophils which are essential components of the innate immune defenses of periodontal tissues. These conditions generated by hormonal changes during pregnancy favor the prevalence and/or severity of certain conditions in the oral cavity. This effect is particularly noticeable after the second month, as it is precisely at this point that there are increases in plasma levels of estrogen and progesterone [15,18]. In the description of a clinical case of PGCG associated with pregnancy, Caillouette & Mattar [1978] reported that the high levels of estrogens and gonadotropic hormones increase the level of glycogen deposition in the epithelium and exert a positive trophic effect on the buccal mucosa [11]. These changes lead to hyperplasia of the papillae and blood vessels, resulting in increased vascularity, which in turn, favors PGCG. Subsequently, Csillag [1997] reported that hormonal and hemodynamic changes during pregnancy may act as stimulating factors for PGCG [12]. In a descriptive study involving 26 patients with PGCG, Günhan [1998] identified the presence of estrogen and progesterone receptors using the immuno-peroxidase technique [19]. Estrogen receptor positivity was found in stromal cells in fourteen patients, and in ten of these patients, the osteoclast-like giant cells also exhibited estrogen receptor immunostaining. Based on these results, it was concluded that the cells forming the peripheral giant cell granuloma might be potential targets for estrogens, and that the lesion might be influenced by hormonal conditions. In contrast, Shirani [2008] did a descriptive study in 20 patients to determine the relationship between PGCG and circulating levels of sex hormones (testosterone, estrogen, and progesterone) [20]. However, no significant association was found between PGCG and sex hormones, and it was concluded that PGCG does not directly depend on testosterone, estrogen, and progesterone. Therefore, it was suggested that the role of sex hormones in the development of PGCG might be secondary to local factors such as trauma and poor oral hygiene. In the present clinical case described, we believe that the changes in the oral cavity caused by hormones during pregnancy may be considered as factors that contribute to the onset and progression of PGCG, since no other local triggering condition for this lesion was present. However, further studies are needed to clarify this association.
Generally, PGCGs occur in soft tissue without affecting the bone, as was observed in the present study, which is consistent with findings from other studies [21,22]. However, giant cells may be activated as an inflammatory response, making them participate as osteoclasts, leading to the resorption of alveolar bone [3]. Osteoclastic activity may be associated with exuberant stromal cell proliferation and bone remodeling [19]. Resorptive functions may be modulated by estrogen receptors on osteoclasts. On the other hand, the proliferation of osteoclasts in the pathology may be related to other factors. Indeed, it has also been demonstrated that estrogens not only limit osteoclastogenesis, but also alter the functional capacity of osteoclasts and, simultaneously, stimulate their apoptosis [23,24].
The treatment of choice for PGCG is surgical excision, as implemented in the present clinical case and in previous studies [1,7,25,26]. This surgical removal method involves excising the lesion along with extensive curettage of the periosteum at the base of the lesion. The associated teeth do not need to be extracted if they are healthy. In fact, it has even been suggested that extraction is contraindicated [3,4]. In addition, it is advisable to remove local irritants. Other treatment options include PGCG removal using CO2 laser or electrocautery [9]. The CO2 laser offers benefits such as reduced intraoperative bleeding, wound sterilization, and less postoperative discomfort for the patient. However, this method cannot be used when the lesion affects the adjacent bone, in which case a thorough surgical curettage will be necessary [9]. In a study [Chaparro, 2005], CGCG excision-biopsy was performed with CO2 laser in an operation involving two cases, and with a cold scalpel in three cases. No recurrence was observed during the postoperative follow-up spanning from 10 months to 4 years [9].
The recurrence rate of PGCG varies widely [27,28]. Chrcanovic [2018] analyzed 2,824 reported cases of PGCG lesions in the literature and found that the overall recurrence rate after treatment was 9.5% [6]. The analysis revealed that when PGCG was treated solely with surgical excision, the recurrence rate was 16%. However, when surgical excision was followed with curettage, the chance of recurrence was reduced by 85%, relative to excision alone. Interestingly, other factors such as age, lesion size, duration of follow-up, gender, location of lesion, clinical symptoms, and bone erosion did not appear to influence the probability of recurrence.
Finally, healthcare professionals need to be aware of the potential impact of pregnancy-associated hormones on the oral cavity. Dentists should be vigilant in monitoring oral lesions during prenatal care. Managing PGCG during pregnancy requires a multidisciplinary approach involving dental professionals, obstetricians, and other healthcare providers. Collaboration amongst specialists ensures the formulation of a safe and effective treatment plan that considers the unique challenges posed by pregnancy [29]. Having a patient-centered approach that addresses her concerns is essential for optimizing treatment outcomes and overall patient satisfaction. Providing reassurance and addressing any anxiety or concerns regarding dental treatment during pregnancy lead to better patient compliance and outcomes [30]. Additionally, it is important to inform pregnant patients that the use of local anesthesia during surgery is safe and does not pose a significant risk to the fetus [31]. Implementing oral care recommendations for pregnant women is essential for aiding the prevention and early detection of developing oral lesions. These recommendations include promotion of good oral hygiene practices [32,33], undergoing regular dental check-ups [34], maintenance of a balanced diet [35], and implementation of monitoring and follow-up when lesions are seen [36].
4. Conclusions
The featured case report highlighted the intriguing association between PGCG and pregnancy, and it has shed light on the importance of recognizing and effectively managing oral pathologies during this crucial period. Although PGCG is relatively rare, it may manifest in pregnant women due to hormonal fluctuations and altered immune responses. Early detection and accurate diagnosis are essential for the initiation of appropriate treatment and prevention of possible complications.
Author Contributions
Conceptualization, F.J.A.B. and S.M.L.M.; methodology, J.S.Z.N.; formal analysis, F.N.N.G.; investigation, M.R.S. and M.M.N.; data curation, F.J.A.B., B.F.N.G. and M.M.N; writing—original draft preparation, F.J.A.B., S.M.L.M. and B.F.N.G; writing—review and editing, J.S.Z.N., M.M.N. and M.R.S. ; visualization, S.M.L.M.; supervision, F.J.A.B. and S.M.L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wu, Y.H; Wu, Y.C; Lee, Y.P; Chiang, C.P. Peripheral giant cell granuloma - Case report. J Dent Sci. 2022, 17, 1434–1436. [Google Scholar] [CrossRef] [PubMed]
- Balaji, P.; Balaji, S.M. Central giant cell granuloma - A case report. . 2019, 30, 130–132. [Google Scholar] [PubMed]
- Cristino BA; Cruz B; Borges A; Aldape B. Granuloma periférico de células gigantes. Revisión de 87 casos. Revista ADM 2016, 73, 175–182.
- Vasconcelos, R. G.; Vasconcelos, M. G; Queiroz, L. M. G. Peripheral and central giant cell lesions: etiology, origin of giant cells, diagnosis and treatment. Jornal Brasileiro De Patologia E Medicina Laboratorial 2013, 49, 446–452. [Google Scholar] [CrossRef]
- Shadman, N.; Ebrahimi, S.F.; Jafari, S.; Eslami, M. Peripheral Giant Cell Granuloma: A Review of 123 Cases. 2009, 6, 47–50.
- Chrcanovic, B.R.; Gomes, C.C.; Gomez, R.S. Peripheral giant cell granuloma: An updated analysis of 2824 cases reported in the literature. J. Oral Pathol. Med. 2018, 47, 454–459. [Google Scholar] [CrossRef]
- Sharma, N.; Rana, S.; Jetley, S. Peripheral giant cell granuloma of maxilla. J. Indian Soc. Periodontol. 2022, 26, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Curtis, N.; Walker, D. A case of aggressive multiple metachronous central giant cell granulomas of the jaws: differential diagnosis and management options. Int. J. Oral Maxillofac. Surg. 2005, 34, 806–808. [Google Scholar] [CrossRef]
- Chaparro A; Angie V; Berini A; Leonardo; Gay E; Cosme. Granuloma periférico de células gigantes: A propósito de 5 casos y revisión de la literatura. Medicina Oral, Patología Oral y Cirugía Bucal 2005, 10, 41–47.
- Bodner, L.; Peist, M.; Gatot, A.; Fliss, D.M. Growth potential of peripheral giant cell granuloma. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. Endodontology 1997, 83, 548–551. [Google Scholar] [CrossRef]
- Caillouette JC; Mattar N. Massive peripheral giant-cell reparative granuloma of the jaw: a pregnancy dependent tumor, Am J Obstet Gynecol 1978, 15, 176–9.
- Csillag, A.; Pharoah, M.; Gullane, P.; Mancer, K.; Disney, T.V. A central giant cell granuloma influenced by pregnancy. Dentomaxillofacial Radiol. 1997, 26, 357–360. [Google Scholar] [CrossRef]
- Kalele, K.; Kanakdande, V.; Patil, K. Peripheral giant cell granuloma: A comprehensive review of an ambiguous lesion. J. Int. Clin. Dent. Res. Organ. 2014, 6, 118. [Google Scholar] [CrossRef]
- Jerkins, D.; Malotky, M.; Miremadi, R.; Dole, M. Central Giant Cell Granuloma of the Mandible Requiring Multiple Treatment Modalities: A Case Report. J. Oral Maxillofac. Surg. 2016, 74, 1596–1607. [Google Scholar] [CrossRef]
- Silva de Araujo, F.C; Gonçalves, C.R.C; Costa, C.A.L; Abreu, F.T; Fontoura, N.C. Systemic alterations and their oral manifestations in pregnant women, J Obstet Gynaecol Res 2017, 43, 16–22.
- Wiener, R.C.; Wiener-Pla, R. Literacy, pregnancy and potential oral health changes: the Internet and readability levels. Matern. Child Heal. J. 2013, 18, 657–62. [Google Scholar] [CrossRef]
- Figuero, R.E; Prieto, P.I; Bascones, M. A; Cambios hormonales asociados al embarazo. Afectación gingivo-periodontal, Av Periodon Implantol 2006, 18 (2), 101-113.
- Cardoso, J.A.; Spanemberg, J.C.; Cherubini, K.; de Figueiredo, M.A.Z.; Salum, F.G. Oral granuloma gravidarum: a retrospective study of 41 cases in Southern Brazil. J. Appl. Oral Sci. 2013, 21, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Günhan M; Günhan O; Celasun B; Mutlu M; Bostanci H. Estrogen and progesterone receptors in the pe-ripheral giant cell granulomas of the oral cavity. J Oral Sci 1998, 40, 57–60.
- Shirani G; Arshad M. RELATIONSHIP BETWEEN CIRCULATING LEVELS OF SEX HORMONES AND PERIPHERAL GIANT CELL GRANULOMA, Acta Med Iran. 2008, 46, 429–433.
- Oliva; Luis; de Oliva; Mercy; Herrera; Néstor & Andrade; Roberto. Giant cell peripheral granuloma: post-surgical recurrence. Literature review and clinical case report. Revista odontológica mexicana 2014, 18, 180–185.
- Falaschini, S; Ciavarella, D; Mazzanti, R; Di Cosola, M; Turco, M; Escudero, N; Bascones, A; Lo Muzio L. Peripheral giant cell granuloma: immunohistochemical analysis of different markers. Study of three cases, Av. Falaschini S; Ciavarella D; Mazzanti R; Di Cosola M; Turco M; Escudero N; Bascones A; Lo Muzio L. Peripheral giant cell granuloma: immunohistochemical analysis of different markers. Study of three cases, Av. Odontoestomatol, 2007 23 (4): 189-196.
- Oursler MJ; Pederson L; Fitzpatrick L; Riggs BL; Spelsberg T. Human giant cell tumors of the bone (os-teoclastomas) are estrogen target cells. Proc Natl Acad Sci U S A. 1994, 7;91, 5227-31.
- Kameda T; Mano H; Yuasa T; Mori Y; Miyazawa K; Shiokawa M; Nakamaru Y; Hiroi E; Hiura K; Kameda A; Yang N. N; Hakeda Y; Kumegawa M. Estrogen inhibits bone resorption by directly inducing apoptosis of the bone-resorbing osteoclasts. J Exp Med 1997, 18, 489–95.
- Alarcón, A.; MUÑOZ, R. M; Schnettler, K; Ulloa, M. C. Granuloma periférico de células gigantes e hiperparatiroidismo. presentación de un caso. Int. J. Odontostomat. 2019, Vol. 13, 266-270.
- Tandon, PN; Gupta, SK; Gupta, D. S; Jurel, S.K; Saraswat A. Peripheral giant cell granuloma. Contemp Clin Dent. 2012, 3, 118–21.
- Boffano, P; Gallesio, C; Roccia, F; Gallesio, C; Garzaro, M; Pecorari, G. Granuloma periférico de células gigantes de la cavidad oral: una revisión sistemática, Med Oral Patol Oral Cir Bucal 2021, 26, e244–e253.
- Lester, S.R.; Cordell, K.G.; Rosebush, M.S.; Palaiologou, A.A.; Maney, P. Peripheral giant cell granulomas: a series of 279 cases. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Boffano, P; Gallesio, C; Barreca, A; Bianchi, F. A; Garzino-Demo P. Granuloma periférico de células gi-gantes de la cavidad oral: una revisión sistemática. Med Oral Patol Oral Cir Bucal. 2021, 26, e244–e253. [CrossRef]
- Greenwall, L.H; Greene, J.C; Sirois, D. Maintaining and Improving the Oral Health of Young Children. American Academy of Pediatric Dentistry, 2014.
- Reddy, VS; Madhireddy, M; Surapaneni, S; Kotha, S.B; Prasad, L.K; Reddy, B.S. Peripheral Giant Cell Granuloma in Pregnancy: A Case Report and Review of Literature. J Orofac Sci 2014, Vol. 6, 119-122.
- Neville, B.W; Damm, D.D; Allen, C.M; Chi, A.C. Oral and Maxillofacial Pathology. 4th edition. Elsevier; 2016.
- Alawi, F. Peripheral giant cell granuloma: a review of 123 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008, 105, e14–e21. [Google Scholar]
- Jain, N; Rathore, A. S; Singh, A; Agarwal, R; Meena, B. Peripheral giant cell granuloma: A review of 123 cases, Natl J Maxillofac Surg 2019, 10, 50–54.
- American College of Obstetricians and Gynecologists Committee on Obstetric Practice. ACOG Com-mittee Opinion No. 462: Moderate caffeine consumption during pregnancy. Obstet Gynecol. 2010, 116, 1000–8.
- Stomaci, D; Poti, S. A; Mariano, F; Monaco, A. Peripheral Giant Cell Granuloma: A Review of the Literature and Report of a Case. The Open Dentistry Journal 2017, 11, 163–171.
Figure 1.
Preoperative clinical view of PGCG in the patient, showing an increase in gum volume corresponding to the circumscribed and well delimited lesion between maxillary central and lateral incisors. (A) Frontal view; (B) lateral view.
Figure 1.
Preoperative clinical view of PGCG in the patient, showing an increase in gum volume corresponding to the circumscribed and well delimited lesion between maxillary central and lateral incisors. (A) Frontal view; (B) lateral view.
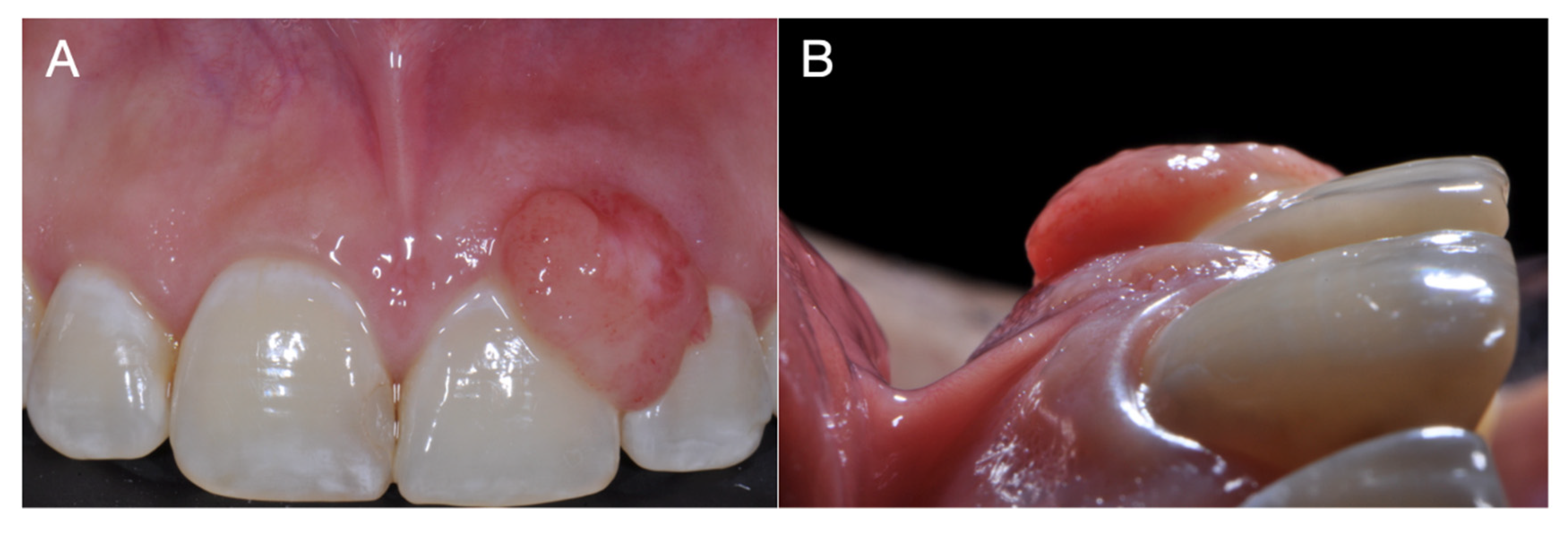
Figure 2.
Periapical radiograph of the affected dental organs without the presence of bone disease.

Figure 3.
Postoperative clinical view. (A) Frontal view; (B) lateral view.
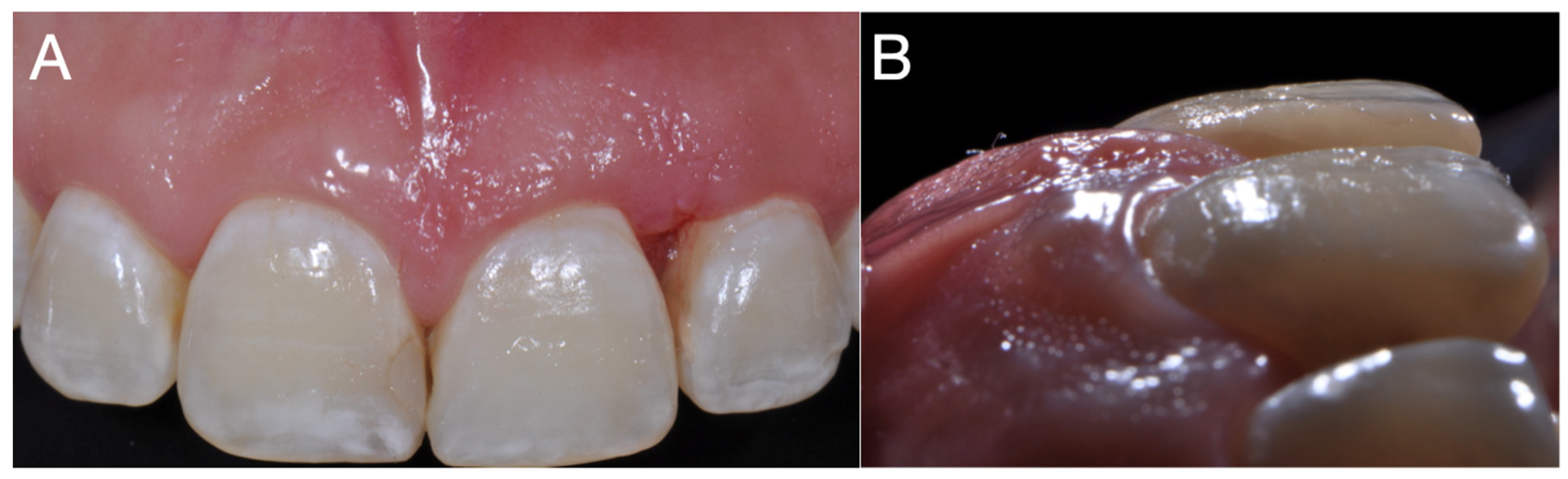
Figure 4.
Excised tissue samples for histopathological examination.

Figure 5.
Histopathological examination of the excised specimen showing proliferation of multi-nucleated giant cells in the cell matrix. Magnification: (A) x10; (B) x20.
Figure 5.
Histopathological examination of the excised specimen showing proliferation of multi-nucleated giant cells in the cell matrix. Magnification: (A) x10; (B) x20.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



