Submitted:
30 September 2023
Posted:
02 October 2023
You are already at the latest version
Abstract
Sleep-disordered breathing affects the growth and development, mental aspect, and learning ability of affected children. Postoperative scarring causes anteroposterior and vertical develop-mental disorders of the maxilla. Obstructive apnea is likely to occur due to the influence on the maxillofacial and airway morphology. In this study, we investigated the sleep-respiratory dynamics of school-aged children with unilateral cleft lip and palate by performing a simple over-night sleep study, maxillofacial morphology and airway analysis using lateral cranial radiographs, and model analysis. Children with unilateral cleft lip and palate showed a significantly higher respiratory event index (REI) than normal children; the maxilla was located in the posterior position in terms of maxillofacial morphology, and airway morphology showed narrow values for all distance measurement items. Moreover, the width and length of the dental arch and the width of the alveolar base arch were significantly smaller. Furthermore, there was a negative correlation between REI and SNA, ANB, REI, and alveolar base arch width. Children with unilateral cleft lip and palate are more likely than normal children to develop sleep-disordered breathing due to in-creased airway resistance caused by undergrowth of the maxilla and narrowing of the upper airway and oral volume.
Keywords:
Cleft palate
; Apnea Hypopnea Index
; out-of-center sleep testing (OCST)
; respiratory event index (REI)
1. Introduction
Sleep-disordered breathing affects not only the growth and development of school-age children but also mental aspects such as learning and depressive symptoms. Obstructive Sleep Apnea Syndrome (OSAS) is defined as "apnea that lasts for ≥10 seconds during bedtime, which occurs ≥30 times per night (7 hours) or ≥5 times per hour"[1]. It causes a variety of disorders, such as daytime somnolence, fatigue, and a decline in learning ability due to reduced concentration [2]. The apnea-hypopnea index (AHI), which is essential for diagnosing OSAS, indicates the apnea-hypopnea index. Sleep apnea syndrome was considered when a patient experiences ≥5 apnea and hypopnea episodes per hour [3].
On the other hand, out-of-center sleep testing (OCST) is a device that records movement during sleep and can be easily transported outside the laboratory to diagnose OSAS and assess therapeutic effects. The test estimates or supplements the results of the diagnosis, severity evaluation, and treatment effect evaluation by polysomnography [2]. Because the OCST does not record electroencephalograms, the total number of apnea and hypopnea events was calculated using the respiratory event index (REI) instead of the AHI [2].
Aside from obesity, males, and advanced aged, it has been pointed out that OSAS is caused by a long soft palate, a low hyoid bone, receded mandible, and stenosis of the upper respiratory tract [3].
In this study, patients with cleft lip and palate who developed maxillary undergrowth as a result of lipoplasty or palatoplasty may have developed anteroposterior and vertical growth disorders, and upper airway stenosis may have caused sleep-breathing disorders compared to healthy children [4]. Postoperative maxillary growth has been a major problem since Grebern pointed out that palatoplasty using the Brophy method causes maldevelopment of the maxilla, postoperative maxillary growth has been a major problem [3,5,6].
In patients with cleft palate, maxillary bone growth is inhibited by scar tissue after palatoplasty. It is hypothesized that the sleep-disordered breathing status of children with cleft palate is reduced compared with that of normal patients because the maxilla is highly associated with the nasal cavity and function. Therefore, the purpose of this study was to compare the effects of maxillary growth suppression on sleep-disordered breathing dynamics in patients with cleft palate and thus on airway morphology, using a simple sleep test.
In this study, an OCST simplified overnight sleep study (Alice NightOne®️ manufactured by Philips Respironics LLC) was performed on the sleep breathing dynamics of school-age children with cleft lip and palate and compared with those of healthy children. Furthermore, the relationship between the upper respiratory area and oral cavity volume was examined for differences compared to healthy children.
2. Materials and Methods
The patients were ten patients who visited the orthodontic outpatient clinic at Ohu University Hospital and were diagnosed with unilateral cleft lip and palate (5 boys, 5 girls, average age 6.4±0.9), as well as 13 healthy children with mild crowding who did not have syndromes or systemic diseases, had no nasopharyngeal disease, and had not undergone tonsillectomy (2 boys, 11 girls, average age 8.4 ± 1.3 years, below target group). The study schedule targeted patients who visited the hospital over a three-year period. The following items were investigated using the dental model, cephalometric standard radiograph, and simple overnight sleep study (Alice NightOne® manufactured by Philips Respironics LLC) at the time of the first visit. The study was explained to the patients and their guardians. The results were used as research data only after obtaining informed consent. This study was approved by the Ethics Review Board of Ohu University (ethics review number: No. 328).
3.1. Simple overnight sleep test
The Alice NightOne device was placed on the solar plexus and secured using a constraining respiratory belt. A nasal cannula was attached to each patient. The SpO2 sensor that came with the main unit was attached to the participant's finger, and the child was instructed to go to bed. (Figure 1, Figure 2 and Figure 3.) Respiratory events were measured by chest movement from a constraining respiratory belt, respiratory events and snoring were measured by nasal pressure from a nasal cannula, and blood oxygen concentration and pulse were measured using an SpO2 sensor. (Figure 4.) The patient was instructed to use the product for two nights at home. The obstructive apnea index, central apnea index, mixed apnea index, and hypopnea index were measured using the International Classification of Sleep Disorders ICSD-2 as measurement items, and the REI was calculated. In addition, the recorded waveform complied with the American Academy of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events ver.2.5, and the analysis was performed using 1A as the criterion for hypopnea. In addition, the REI was calculated using a Master Scorer (technician certified by the Japanese Society of Sleep Research). (Figure 5.) In a report on accuracy control of sleep stage inspection judgment, the standard minimum match rate is ≥85% (K coefficient of 0.8 or more). When using this device, the patient is taught how to attach the device themselves to avoid improper sensor attachment. When the recording time was short, or an abnormality was found in the sensor, we attempted to improve the accuracy and avoid any deficiencies in the recording by lending the device again and instructing the patient and guardians about the attachment method. According to the severity classification of AHI (number of apnea and hypopnea per hour of sleep), the severity of REI is classified into three categories: mild (5 to 15 times/h for mild), moderate (15 to 30 times/h), and severe (≥30 times/h). For statistical analysis, the Mann-Whitney U test and Spearman’s rank correlation coefficient were used. The significance level was set at p<0.005.
3.2. Cephalometric radiograph image
3.2.1. Cephalometric analysis
Cephalometric radiographs were obtained according to the standard method, and the skeletal and dental patterns of the cleft lip, palate, and control groups were analyzed. Cephalometric radiographs of the facial skeleton were traced and analyzed.
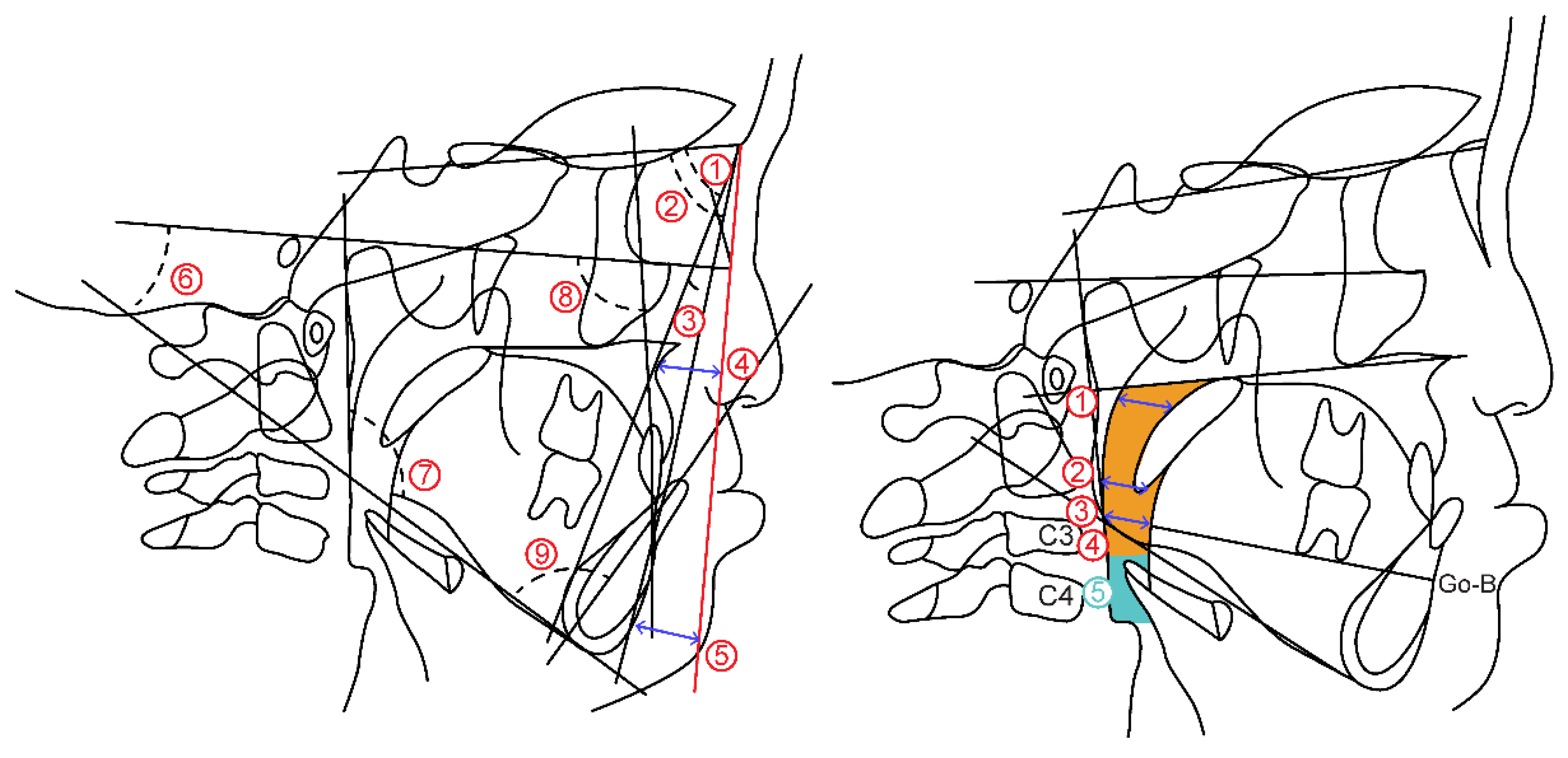
The measurement items are as follows. (Figure 6.A)
(1) Skeletal pattern
- ①
- SNA: SN angle between plane and straight-line NA
- ②
- SNB: SN angle between plane and straight-line NB
- ③
- ANB: Angle formed by straight line AN and straight line NB
- ④
- McNamara to A: Distance from McNamara line to point A
- ⑤
- Namara to Pog: Distance from McNamara line to Pog
- ⑥
- FH plane to Mandibular plane angle: Angle between mandibular plane and Frankfurt plane
- ⑦
- Gonial Angle: Angle between mandibular plane and mandibular posterior marginal plane
(2) Dental pattern
- ⑧
- U1 to FH plane angle: between maxillary central incisor tooth axis and Frankfurt plane Angle
- ⑨
- L1 to Mandibular plane angle: Mandibular central incisor tooth axis and mandibular plane Angle
3.2.2. Airway distance, area
Airway distance and area were measured based on the method of Alan A et al. [7] on the radiograph obtained from the lateral cephalometric radiograph. (Figure 6.B)
(1) Airway distance
- ①
- SPAS: Linear distance between the point where the axis parallel to the Go-B plane touches the posterior soft palate and the point where it touches the posterior pharyngeal wall
- ②
- MAS: Linear distance from the point where a line parallel to the Go-B line passes through the lowest point of the soft palate and touches the posterior pharyngeal wall
- ③
- IAS: Linear distance between two points extending the Go-B line and intersecting the posterior border of the tongue and posterior wall of the pharynx.
(2) Airway area
- ④
- Orpharynx: Area surrounded by a straight line connecting the point where the palatal plane intersects with the posterior pharyngeal wall, a straight line passing through the tip of the epiglottis parallel to the palatal plane and the posterior pharyngeal wall, hyoid bone, and soft palate wall
- ⑤
- Hypopharynx: Area bounded by two straight lines parallel to the Palatal plane passing through the hypopharyngeal area, tip of the epiglottis, anterior-inferior point of the fourth cervical vertebra, posterior pharyngeal wall, and posterior epiglottis wall
Figure 6.
(a) Cephalometric analysis items by lateral cranial X-ray standard photograph. (b) Airway distance/area measurement point.
Figure 6.
(a) Cephalometric analysis items by lateral cranial X-ray standard photograph. (b) Airway distance/area measurement point.
3.3. Model analysis
As the measurement points in the model analysis, the distance from the center of the line connecting the labial surfaces of both deciduous central incisors to the line connecting the cusps of both deciduous canines is defined as the anterior length of the maxillary coronal arch. The posterior length of the maxillary coronal arch was defined as the distance from the center of the line connecting the labial surfaces of both deciduous central incisors to the line connecting the most distal ends of the second deciduous molar on both sides. The distance between the deciduous canines and first deciduous teeth was defined as the anterior width of the maxillary coronal arch. The distance between the buccal grooves of the bilateral second deciduous molars was defined as the posterior width of the maxillary coronal arch. Furthermore, regarding the width of the alveola basal arch, the distance between the deepest part of the gingiva, which corresponds to the apex of both primary canines and primary molars, is defined as the anterior width of maxillary alveolar basal arch. The distance between the deepest gingival regions corresponding to the apical regions of the second primary molars on both sides was defined as the posterior width of the maxillary alveolar basal arch (Figure 7).
- ①
- Anterior width of maxillary coronal arch
- ②
- Posterior width of maxillary coronal arch
- ③
- Anterior length of Maxillary coronal arch
- ④
- Posterior length of maxillary coronal arch
- ⑤
- Anterior width of maxillary alveolar basal arch
- ⑥
- Posterior width of maxillary alveolar basal arch
3. Results
3.1. Simple overnight sleep test
The REI values in the cleft lip and palate groups were significantly higher than those in the control group (P=0.015). There was no significant difference in SpO2 between the two groups (Table 1).
3.2. Cephalometric radiograph image
3.2.1. Cephalometric analysis
In the skeletal system, the mean values of SNA and McNamara to A were lower in the cleft lip and palate group than in the control group, and there was a significant difference in SNA (P=0.049). In the dental system, small and significant differences were observed between the U1 and FH and L1 and Mol groups. (Figure 2) We also found a negative correlation between the REI and SNA (P=0.038), and a negative correlation between the REI and ANB. years, respectively (P=0.028) (Table 2).
3.2.2. Antero-posterior airway distance and area
SPAS, MAS, and IAS were significantly narrower in the cleft lip and palate groups than in the control group. (P=0.001)(P=0.010)(P=0.006). Both the oropharynx and hypopharynx showed small values, with the oropharynx showing a significant difference (P=0.005) (Table 2).
3.3. Model analysis
In the cleft lip and palate group, the anterior and posterior widths of the maxillary alveolar basal arch were significantly narrower than in the control group (P=0.00). There was a narrow and significant difference in the anterior (P=0.001) and posterior (P=0.000). The length of the coronal arch was significantly shorter both anteriorly (p=.030) and posteriorly (P=0.000), and a significant difference was observed (Table 3). We also found a negative correlation between REI and the anterior width of the maxillary alveolar basal arch (P=0.006).
4. Discussion
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
According to the multifactorial threshold theory, cleft lip and palate is a congenital disease with one of the highest incidences in Japan, which occurs in approximately 1 in 500–600 newborns [8]. Patients with cleft lip and palate have speech, swallowing, and pronunciation problems; however, they also develop scar tissue after palatoplasty, inhibiting maxillary growth [4,9,10,11]. As such, early treatment and cooperation with various clinical departments are necessary because it affects the maxillofacial morphology. In this study, we quantitatively evaluated sleep-breathing dynamics and the upper respiratory tract by comparing targeted patients with cleft lip and palate and healthy participants without cleft lip and palate.
From sleep test results, first proposed by Guilleminault, OSA is a disease in which airway obstruction occurs during sleep, resulting in various symptoms such as physical, mental, and learning aspects due to inadequate sleep [12]. PSG is considered the gold standard for the diagnosis of OSAS. However, it is difficult to perform PSG in all patients because of cost and patient burden. Although the sleep breathing disorder index by a simple test is not currently defined as a diagnostic criterion, it is possible to judge the necessity of PSG for screening sleep-disordered breathing. Furthermore, the International Classification of Sleep Disorders (ICSD-3), issued in 2014, accepts the use of OCST for the diagnosis of OSAS in adults [13]. Murakami et al. [14] measured skeletal malocclusion using a simple sleep test equipment used in this study. Based on their research results, they reported that even a simple all-night sleep test can be evaluated as a sleep test. Therefore, we measured the patients’ sleep dynamics using a simple overnight sleep test machine. In this study, although events in cleft lip and palate patients did not reach ≥5 times/hour, the REI value was higher than that of the healthy participants, and a significant difference was observed. This may have been due to undergrowth of the maxillary bone caused by scarring from childhood palatoplasty, resulting in airway resistance and respiratory failure. Iwasaki et al. [15] reported that patients with cleft lip and palate had airflow obstructions in the nasal and nasopharyngeal cavities. Drettner et al. [16] reported deformation of the nasal septum, nasal obstruction, and thickening of the nasal mucosa in patients with cleft lip and palate. With these reports in mind, we believe that not only maxillary undergrowth, but also respiratory disorders are caused by higher nasal airway resistance in patients with cleft lip and palate than in healthy participants.
Analysis of the maxillofacial morphology of patients with cleft lip and palate using cephalometric radiographs was reported by Graber in 1949 using lateral cranial radiographs [6,17]. On the other hand, it has been reported that SNA and SNB are facial skeletal morphologies that have a high risk of sleep breathing disorders [18]. The results of this study also showed that the SNA, which indicates the anteroposterior positional relationship of the maxilla with respect to the cranium, was significantly smaller in patients with cleft lip and palate, based on lateral cranial radiographs. Furthermore, it has been reported that skeletal mandibular protrusion is related to the maxillary position and that the upper airway narrows when the maxilla recedes, which means that moving the maxilla forward widens the airway area and improves sleep-breathing disorders [19]. This is thought to be due to anteroposterior growth and developmental disorders of the maxilla caused by palatoplasty performed in childhood [20].
In addition, SPAS, MAS, and IAS showed short airway distance measurements. Reiley et al. [21,22] stated that patients with OSA have a narrower SPAS than healthy participants. In this study, the SPAS also showed a significantly small and narrow value, indicating that stenosis of the SPAS is an influencing factor that causes respiratory changes. The upper airway cross-sectional area of patients with cleft lip and palate is approximately 70% that of healthy individuals. There are also reports that the upper airway is narrower in healthy participants [23,24]. In this study, the airway distance was significantly smaller for all measurement items, and the airway area was smaller in patients with cleft lip and palate, consistent with previous reports. In addition, the fact that the SNA was significantly smaller in the posterior position confirmed that the narrowing of the anteroposterior diameter of the upper airway was related to maxillary undergrowth.
The width of the coronal arch in a child with cleft lip and palate immediately after birth was larger than that in a healthy child. This implies lateral displacement of the maxillary segment and loss of continuity between the perioral muscles, such as the buccal and superior pharyngeal constrictor muscles and the muscles near the pharynx, which increase the width of the patient's palate [25,26,27]. However, there was a marked reduction in the width after lip palatoplasty. In particular, the stenosis of the anterior part was remarkable, and the results of this study showed that the value of the maxillary dental arch was significantly smaller than that of healthy children. This is the effect of post-palatoplasty scar contraction due to the anterior extension of the rupture, and is consistent with the morphology of the maxillary arch in children with cleft lip and palate [28]. Moreover, in the width of the alveolar basal arch, Hama [29] reported developmental disorders of the maxillary alveolar basal as a characteristic of cleft lip and palate, and the anterior and posterior alveolar basal arch widths were narrow. In terms of the length of the coronal arch, children with cleft lip and palate showed smaller values for both the anterior and posterior lengths than healthy children. In addition, there was a negative correlation between REI and anterior alveolar basal arch width. In our study, cleft lip and palate had a high REI, and the model analysis showed significantly smaller values for the width of the coronal arch and alveolar basal arch, indicating stenosis. This is thought to be caused by postoperative scarring of the cleft lip and palate, resulting in undergrowth of the maxilla and narrowing of the intraoral volume, leading to an increase in airway resistance and REI.
General orthodontic treatment for children with cleft lip and palate
Children with cleft lip and palate are prone to reverse skeletal occlusion due to maxillary cleft growth. In contrast, in orthodontic treatment during the growth period, a maxillary protractor (MPA) is widely used to improve jaw relationships by promoting the forward movement and growth of the jawbone. There are also reports of favorable treatment results due to forward growth of the maxilla using MPA [30,31,32,33,34,35]. In addition, as there are reports that moving the maxilla forward expands the upper airway and improves sleep breathing disorders [19], the use of MPA in children with cleft lip and palate promotes anterior maxillary growth and increases the airway area, thus affecting sleep respiratory dynamics. Therefore, further research on this topic is required.
5. Limitations
Under normal circumstances, research reliability must be improved by further increasing the number of participants in terms of clinical statistics. However, this study was conducted in children with cleft lip and palate, and among the patients who wished to receive orthodontic treatment at our hospital, the number of children with cleft lip and palate was small. The number was limited and could not be increased; even if consent was obtained, data collection was difficult and could not be performed if the patient was uncooperative or had a systemic disease is a limitation of this study.
6. Conclusions
In this study, we calculated the REI using a simple overnight sleep test for sleep-breathing dynamics in children with cleft lip and palate. Simultaneously, we analyzed skeletal morphology, airway distance, and airway area from lateral cranial radiographs. Furthermore, we compared the width and length of the coronal arches from the oral cavity model with those of healthy children and compared the characteristics of children with cleft lip and palate and the differences in respiratory disorders with those of healthy children. The results revealed that children with cleft lip and palate had a higher REI than healthy children, and their maxillofacial morphology showed that the maxilla was displaced posteriorly. Airway morphology was constricted based on the airway distance and area. In addition, the model analysis revealed that the anterior and posterior maxillary arch lengths were small, the anterior and posterior widths of the maxillary arch were narrow, and the anterior and posterior widths of the alveolar basal arch were narrow. A correlation was observed between the anterior width of the alveolar basal arch and REI. Based on these results, in children with cleft lip and palate, MPA is used to position the maxilla forward to improve postoperative maxillary tears, and an expansion bed is used to expand the intraoral volume without increasing airway resistance is important.
We intend to further increase the number of cases in the future.
Author Contributions
Formal analysis, N.N.; Investigation, N.N.; Supervision, H.K.; Project administration, H.K., K.F., A.O. and K.S.; Data analysis, T.O.; Writing - Original Draft, N.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Review Board of Ohu University (ethics review number: No. 328).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article.The data presented in this styudy are available in journal of clinical medicine.
Acknowledgments
Division of Orthodontics and Dentofacial Orthopedics, Department of Oral Growth and Development, Ohu University School of Dentistry.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guilleminault, C.; Hoed, J.; Muter, M.M. Clinical overview of the sleep apnea syndromes. In : Sleep Apnea Syndromes, edited by Guil- leminault, C. & Dement, W., New York Alan R. Liss Inc., 1977,p. 1.
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C.; Bassiri, A. Clinical features and evalunation of obstructive sleep apnea-hyponea syndrome. Kryger M.H., Roth T.et al;Principles and Practice of Sleep Medicine Fourth ed. Elsevier Saunders Co,Philadelphia,2005,p.1043-1052.
- Levin, H.S. A cephalometoric analysis of cleft palate deficiencies in the middle third of the face. Angle Orthod 1963, 33, 186–194. [Google Scholar]
- Graber, T. Changing philosophies in cleft palate management. J. Pediatr. 1950, 37, 400–415. [Google Scholar] [CrossRef] [PubMed]
- Graber, T.M. Craniofacial morphology in cleft lip and plate deformities. Surg Gynec Obstet 1949, 88, 359–369. [Google Scholar] [PubMed]
- Lowe, A.A.; Ono, T.; Ferguson, K.A.; Pae, E.-K.; Ryan, C.F.; Fleetham, J.A. Cephalometric comparisons of craniofacial and upper airway structure by skeletal subtype and gender in patients with obstructive sleep apnea. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Garrahy, A.; Millett, D.T.; Ayoub, A.F. Early Assessment of Dental Arch Development in Repaired Unilateral Cleft Lip and Unilateral Cleft Lip and Palate versus Controls. Cleft Palate Craniofac J 2005, 42, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Shi,B.,et al.:The impact of cleft lip and palate on maxillofacial growth. Int J Oral Sci,7:14-17,2015.
- Tarun Vyas,Prabhakar Gupta,et al: Cleft of lip and palate:A review. J Family Med Prim Care.2020 Jun;9(6):2621-2625. 2: Jun;9(6).
- Otsuki, K.; Yamanishi, T.; Tome, W.; Shintaku, Y.; Seikai, T.; Fujimoto, Y.; Kogo, M. Occlusion at 5 Years of Age Following Hard Palate Closure With Vestibular Flap. Cleft Palate-Craniofacial J. 2019, 57, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C., Tilkian, A. and Dement, C. W. : The sleep apnea syndromes. Ann Rev Med. 27: 465-484, 1976. 4: 27.
- The International Classification of Sleep Disorders,3rd ed. Westchester: American Academy of Sleep Medi- cine,2014.
- Ayano Murakami, Hitoshi Kawanabe.,et al:Effect of sleep-disturbed breathing on maxillofacial growth and development in school-aged children. ORTHODONTIC WAVES.2021,VOL80,NO.2,87-95.
- Iwasaki T, Yanagisawa-Minami A, Suga H, Shirazawa Y, Tsujii T, Yamamoto Y, Ban Y, Sato-Hashiguchi M, Sato H, Kanomi R and Yamasaki Y: Rapid maxillary expansion effects of nasal airway in children with cleft lip and palate using computational fluid dynamics. Orthod Craniofac Res 22, 201-207 (2019).
- DRETTNER,B.,:The nasal airway and hearing in patients with cleft palate. Acta Otolaryng.,52,131-142,1960.
- Graber, T. M.: A cephalometric analysis of the developmental pattern and facial morphology in cleft palate. Angle Orthod., 19 : 91-100, 1949.
- Riley R,Guilleminault C,Herran J,Powell N:Cephalometric analyses and flow-volume loops in obstractive sleep apnea patients. Sleep 6,303-311,1983.
- Okushi T,Tonogi M,Arisaka T,Kobayashi S,Tsukamoto Y,Morishita H,Sto K,Sano C,Chiba S,Yamane GY,Nakajima T(2011) Effect of maxillomandibular advancement on morphology of velopharyngeal apace. J Oral Maxillofac Surg 69,877-8.
- Shibasaki, Y.; Ross, R.B. Facial growth in children with isolated cleft palate. Cleft Palate J. 1969, 6, 290–302. [Google Scholar] [PubMed]
- Reiley, R., Guilleminault, C., Powell, N., et al.: Palatopharyngoplasty failure, ce- phalometric roentgenograms, and obstructive sleep apnea. Otolaryngol. Head Neck Surg., 93: 240-243,1985.
- Lyberg, T., Krogstad, 0., and Djupesland, G.: Cephalometric analysis in patients with obstructive sleep apnea syndrome : II. Soft tissue morphology. J. Laryngol. Otol., 103 293-297,198.
- Hairfield, W.M.; Warren, D.W. Dimensions of the cleft nasal airway in adults: a comparison with subjects without cleft. Cleft Palate J. 1989, 26, 9–13. [Google Scholar] [PubMed]
- Drake, A.F.; Davis, J.U.; Warren, D.W. Nasal airway size in cleft and noncleft children. Laryngoscope 1993, 103, 915–917. [Google Scholar] [CrossRef] [PubMed]
- Mazaheri, M., Harding, R. L. and Nanda, S.: The effect of surgery onmaxillary growth and cleft width. Plast. Reconstr. Surg., 40 ; 22-30,1967.
- Subtelny, J. Width of the nasopharynx and related anatomic structures in normal and unoperated cleft palate children. Am. J. Orthod. 1955, 41, 889–909. [Google Scholar] [CrossRef]
- Brodie, A.G. Anatomy and physiology of head and neck musculature. Am. J. Orthod. 1950, 36, 831–844. [Google Scholar] [CrossRef] [PubMed]
- Pruzansky, S. Description, classification, and analysis of unoperated clefts of the lip and palate. Am. J. Orthod. 1953, 39, 590–611. [Google Scholar] [CrossRef]
- Hama,K.:Morphological study of the craniofacial skeleton with in a profile in Cleft Lip and Plate, J.Osaka Univ.,4:41,1964.
- Ralph Steegman,Adriaan Schoeman et al: Three-dimensional volumetric changes in the airway of growing unilateral complete cleft lip and palate patients after bone-anchored maxillary protraction. American Journal of Orthodontics and Dentofacial Orthopedics.,volme162,lssue6,850-860,2022.
- Nelson, F. O.: A new Extra-Oral Orthodontic Appliance, Internat. J. Orthod., 6; 24-27, 1968.
- Friede, H.; Lennartsson, B. Forward traction of the maxilla in cleft lip and palate patients. Eur. J. Orthod. 1981, 3, 21–39. [Google Scholar] [CrossRef] [PubMed]
- Ranta, R. : Protraction of the cleft maxilla. Eur. J. Orthod., 10 : 215-222, 1988.
- Tindlund, R. S., Rygh, P., Boe, O. E. : Orthopedic protraction of the upper jaw in cleft lip and palate patients during the deciduous and mixed dentition periods in comparison with normal growth and devel- opment. Cleft Palate-Craniofac J., 30 : 182- 194. 1993.
- Buschang, P. H. Porter, C., Genecov, E., et al : Face mask therapy of preadolescents with unilateral cleft lip and palate. Angle Orthod., 64 : 145-150, 1994.
Figure 1.
Attaching the Alice NightOne device. A: Alice NightOne Unit; B: Constraining the Respiratory Belt.
Figure 1.
Attaching the Alice NightOne device. A: Alice NightOne Unit; B: Constraining the Respiratory Belt.
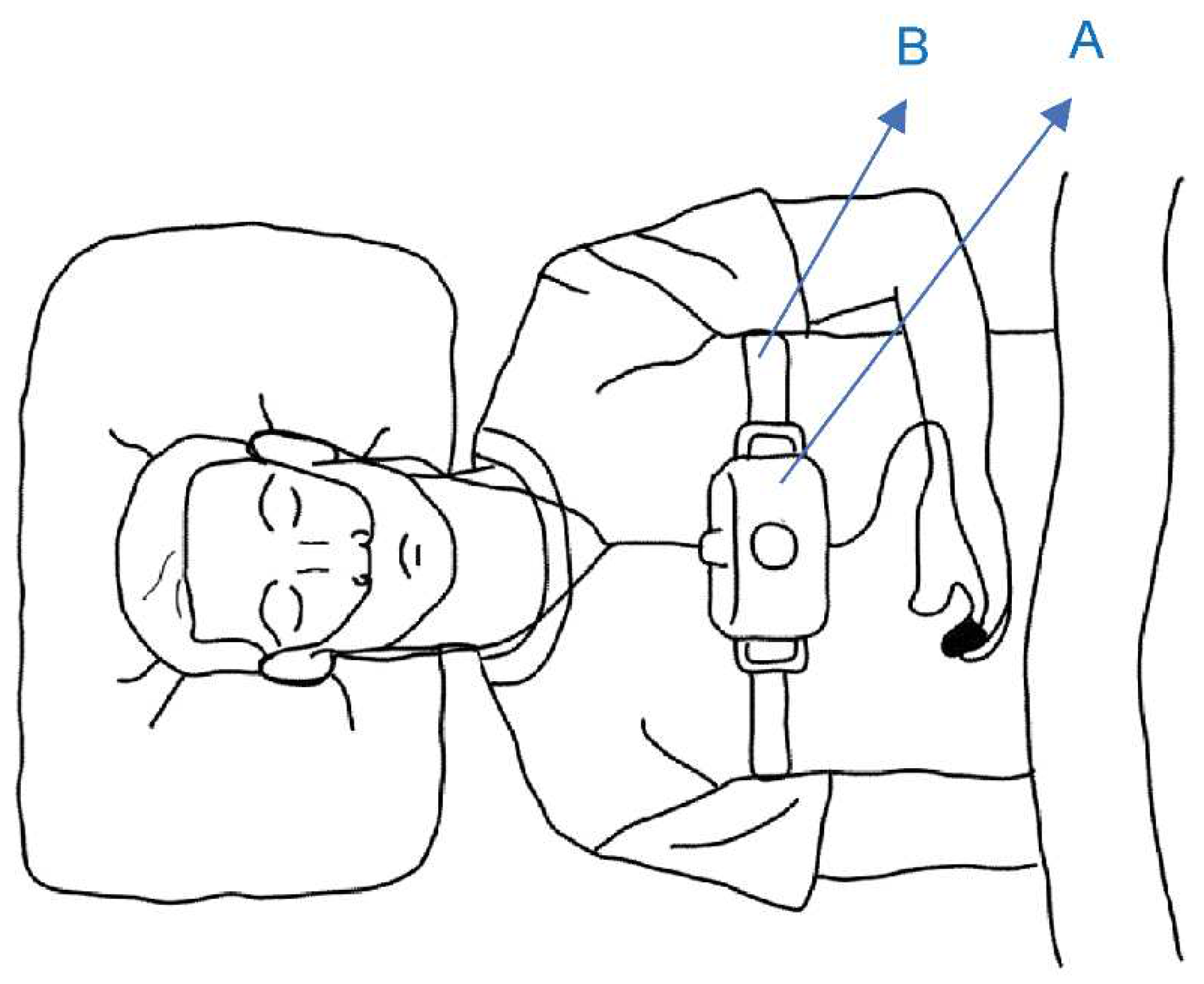
Figure 2.
Nasal cannula attachment. C: Nasal cannula.
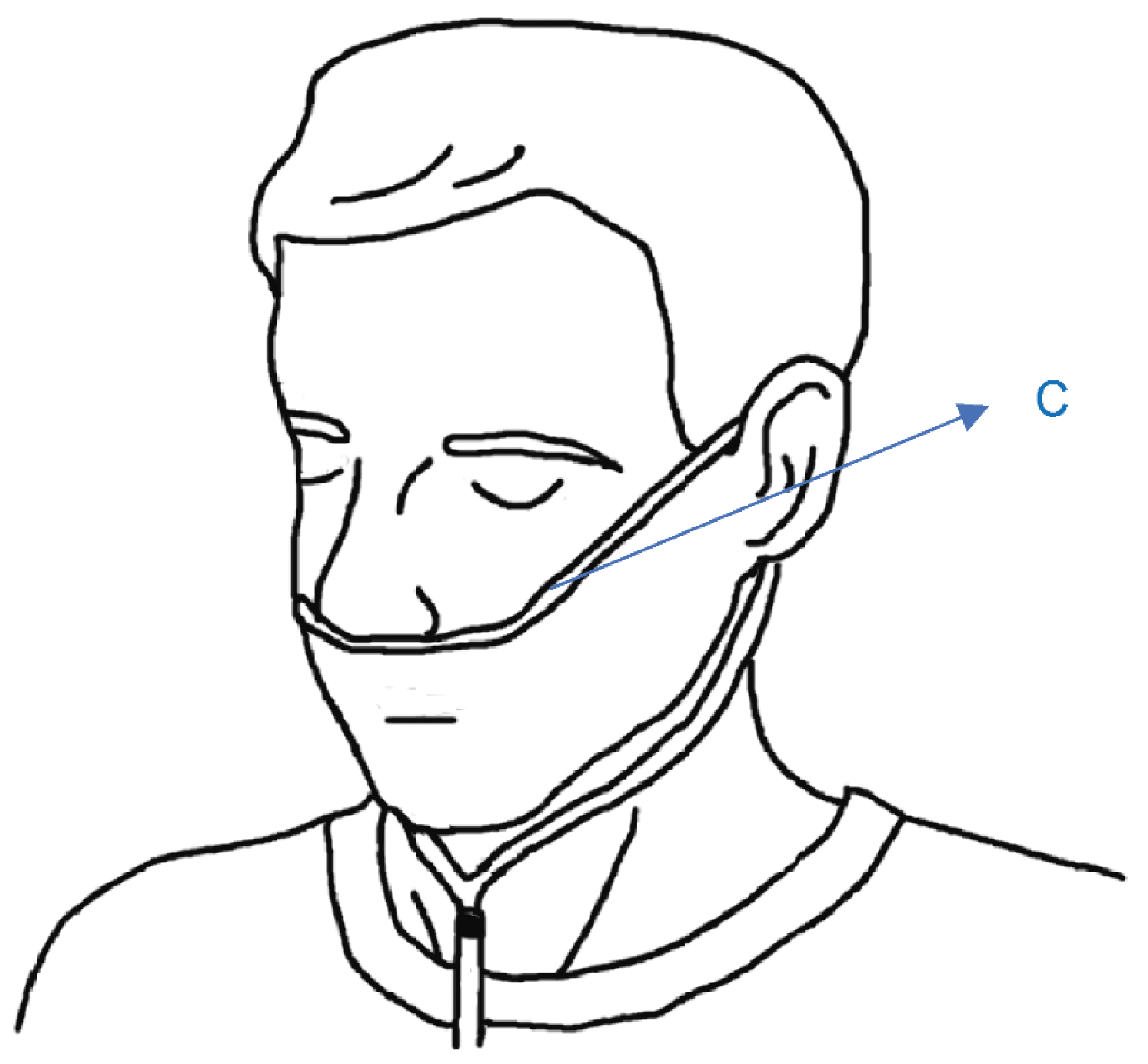
Figure 3.
SpO2 sensor attachment. D: SpO2 sensor.
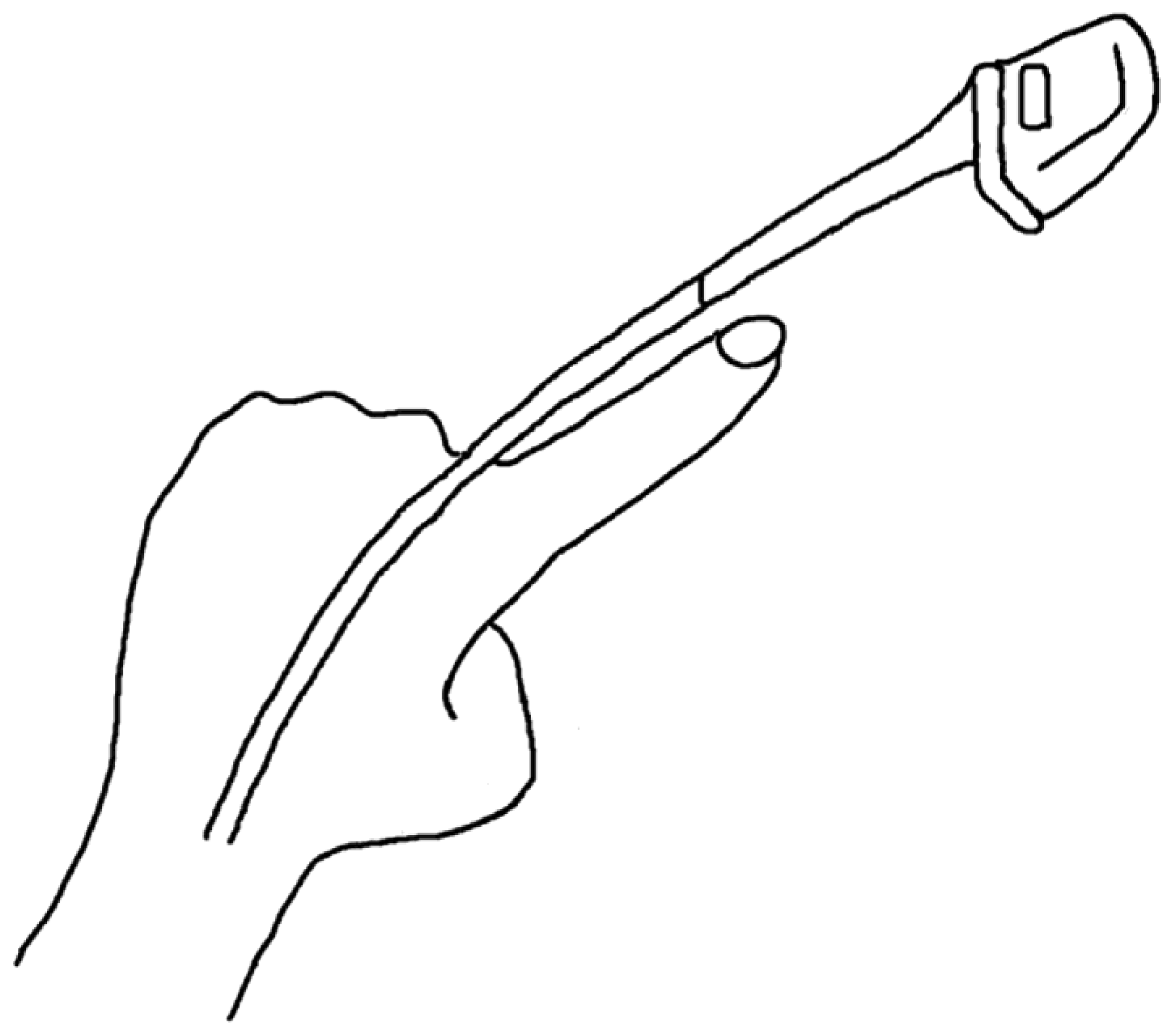
Figure 4.
An example of analysis results. PFlow: nasal pressure; THO: thoracoabdominal exercise.
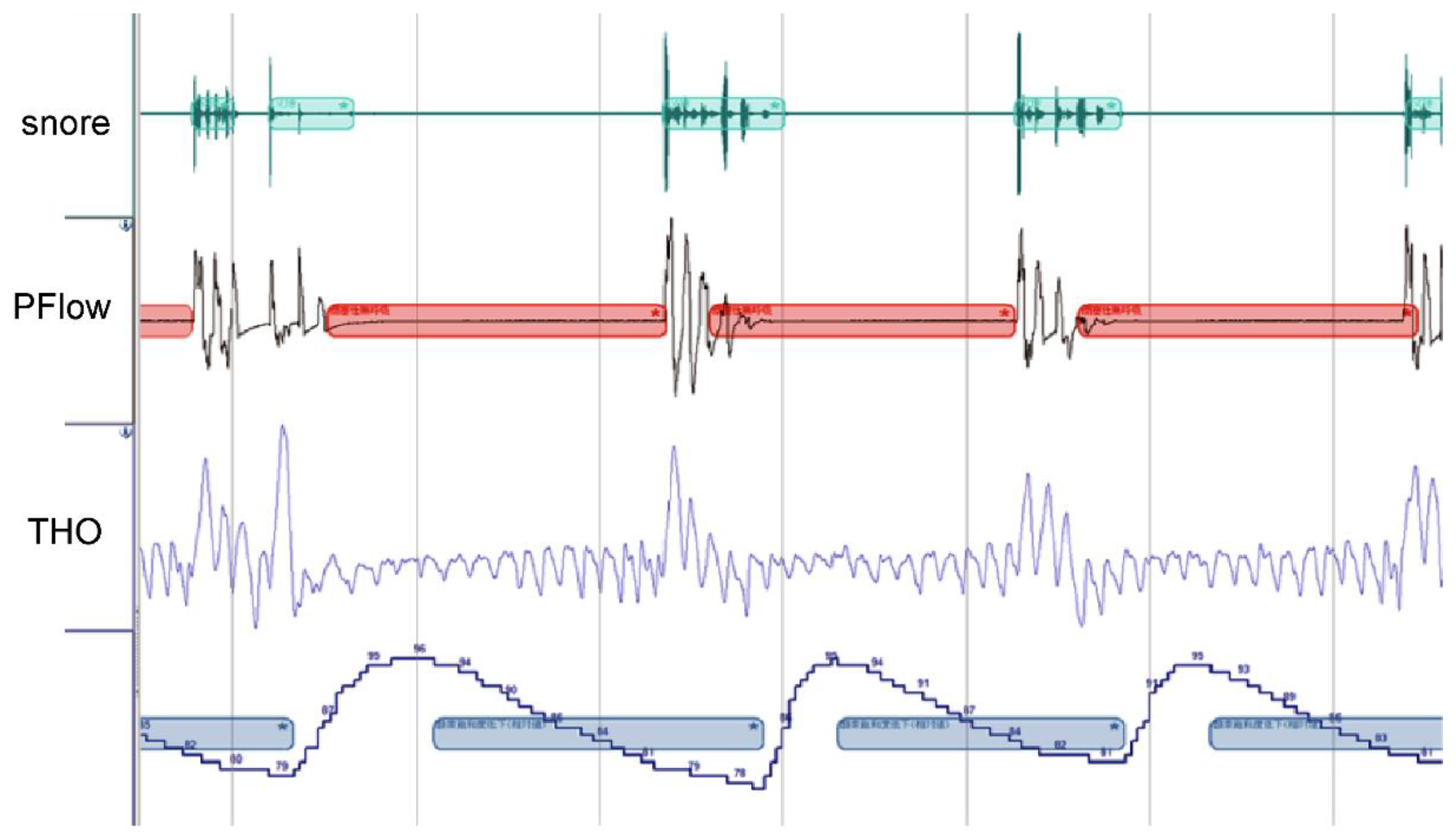
Figure 5.
Analysis system.
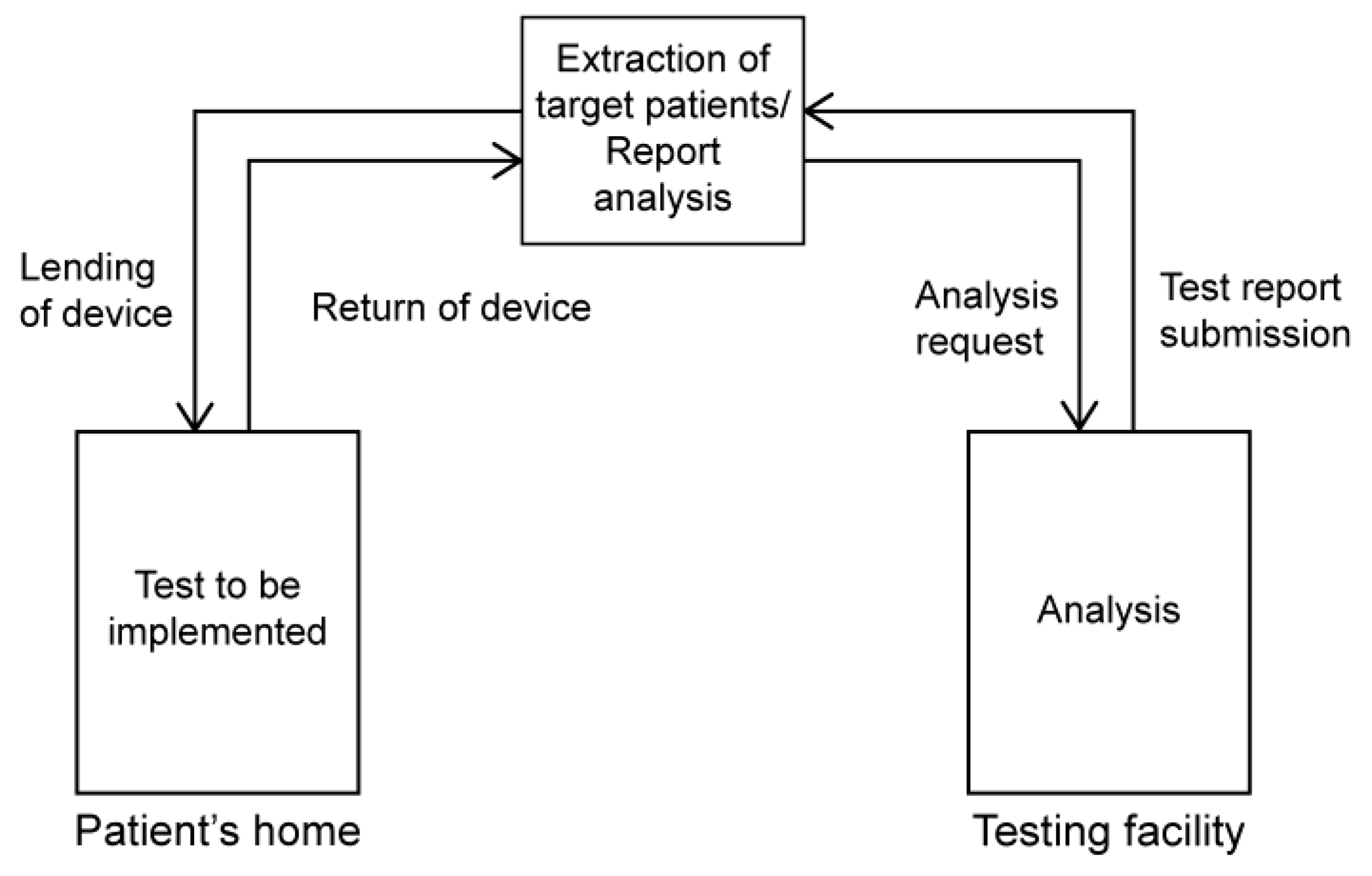
Figure 7.
Model analysis items.
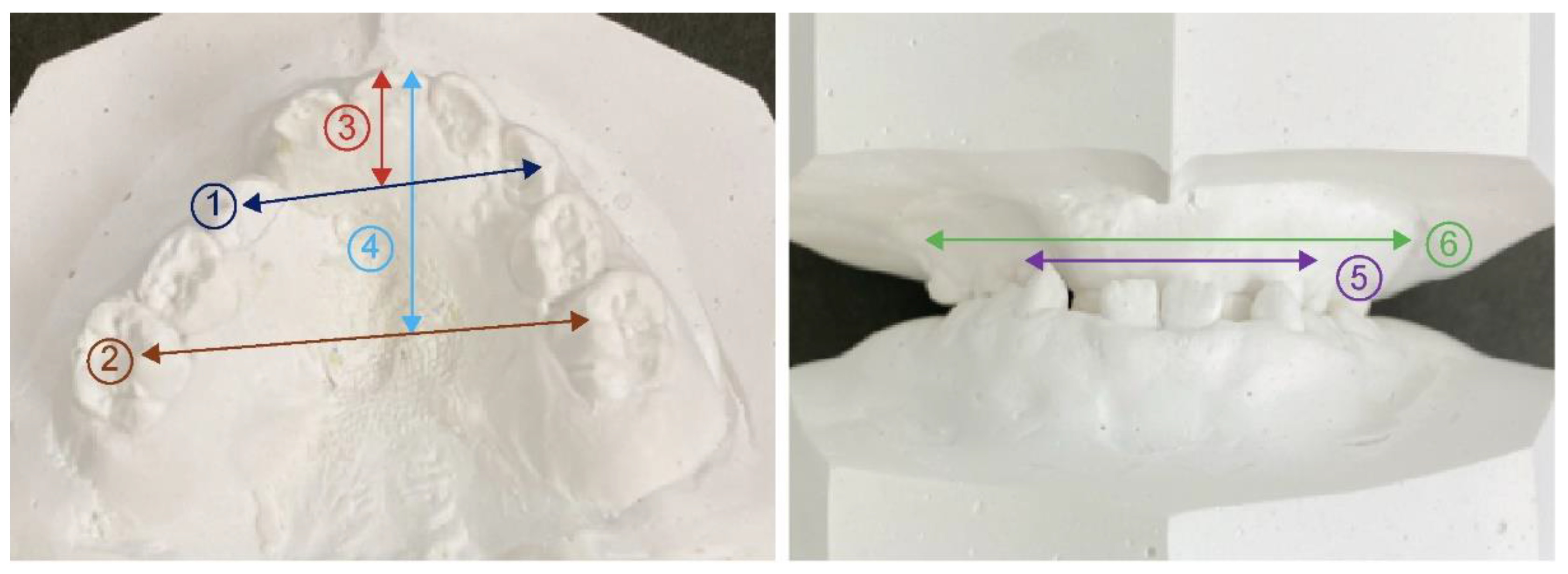

Table 1.
Simple overnight sleep test results.
| Cleft lip and palate group | Control group | Significant difference | |
|---|---|---|---|
| REI | 4.4±2.9 | 1.8±0.7 | .015* |
| SP02 | 96.3±0.8 | 96.0±0.6 | .446 |
Table 2.
Cephalometric analysis results and Airway distance and area results.
| Cleft lip and palate group | Control group | Significant difference | |
|---|---|---|---|
| SNA | 76.8±4.2 | 80.2±2.8 | .049* |
| SNB | 77.6±2.7 | 77.6±2.1 | .648 |
| ANB | -0.7±4.0 | 2.7±1.9 | .003** |
| McNamara to A | -2.2±4.6 | -1.3±2.5 | .483 |
| McNamara to Pog | -6.0±4.8 | -7.4±3.8 | .483 |
| Mand.P | 28.8±4.8 | 30.5±6.4 | .648 |
| Gonial.A | 126±7.1 | 127.0±7.2 | .879 |
| U1 to FH | 93.6±10.2 | 111.0±5.2 | .000** |
| L1 to Mand.P | 80.1±6.6 | 93.2±8.7 | .000** |
| APAS | 7.8±1.7 | 12.2±3.4 | .011* |
| MAS | 8.2±1.6 | 12.3±3.4 | .010** |
| IAS | 9.5±4.3 | 13.4±3.7 | .006** |
| Orpharynx | 411.0±105.3 | 564.6±130.6 | .005** |
| Hypopharynx | 164.0±44.2 | 195.7±62.8 | .313 |
Table 3.
Model analysis results.
| Cleft lip and palate group | Control group | Significant difference | |
|---|---|---|---|
| Anterior width of maxillary alveolar basal arch | 36.4±2.5 | 40.3±2.6 | .000** |
| Posterior width of maxillary alveolar basal arch | 53.6±3.8 | 59.4±2.6 | .002** |
| Anterior width of maxillary coronal arch | 28.6±2.3 | 33.0±2.5 | .001** |
| Posterior width of maxillary coronal arch | 38.9±3.2 | 47.2±2.0 | .000** |
| Anterior length of maxillary coronal arch | 11.0±1.7 | 12.9±2.1 | .030* |
| Posterior length of maxillary coronal arch | 22.8±3.6 | 32.4±1.8 | .000** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



