
Submitted:
30 September 2023
Posted:
02 October 2023
You are already at the latest version
Abstract
This research mapped significant social networks of victims of childhood sexual abuse, identifying relationships between childhood trauma and social bonds in adult life. Ten adult women, aged between 20 and 40 years, in psychiatric care for the consequences of trauma suffered in childhood participated in the research. For data collection, the map of significant social networks was used and analyzed through the structure, functions and attributes of the bonds. The network is composed of people from the Friendship, Family, Community, Work/Study and Health Teams group. The networks of friendships, family, co-workers or studies play a predominant role of emotional support, while the Health Teams also offer emotional support, but primarily provide clinical support in overcoming trauma and its consequences. The network of relationships has specific functions that maintain psychosocial integrity and help women to overcome the abuse suffered.
Keywords:
Child sexual abuse
; Social Networking
; Social Support.
1. Introduction
Sexual abuse against children and adolescents is a worldwide phenomenon found at all social levels, which represents a challenge for government agencies. Different studies [1,2,3,4] identified that, in the Brazilian scenario, children and adolescents victimized by sexual abuse are predominantly female (75% to 90% of cases), the abusers are mostly male (on average, 80% to 90% of cases), and with proximity to the victim – father, stepfather, uncle, grandfather or cousin – characterizing intra-family violence as a major occurrence, being that the extra-family cases usually involve neighbors. The age of onset for abuse is mostly between 5 to 14 years old, with the average age of greatest risk between 9 and 10 years old, for boys and girls, and an average time of six months to one year of abuse before notification [3,4].
In Brazil, the Law 13.431 [5] typifies sexual abuse in childhood, establishing the system for guaranteeing the rights of children and adolescents who are victims or witnesses of violence. The law defined the forms of violence against children (physical, psychological, sexual and institutional), with sexual abuse being a form of sexual violence and representing “any action that uses the child or adolescent for sexual purposes, whether it is a carnal conjunction or another libidinous act, performed in person or electronically for the sexual stimulation of the agent or third parties” [5].
A systematic review [6] collected data from studies on the victimization of female children and adolescents in poor or developing countries. The authors concluded that the closest community social network in conjunction with the conditions for victims to disclose abuse represent the main forms of prevention. In terms of scientific production, some authors emphasize the importance of community, social groups and interpersonal bonds in maintaining the individual's health, and the impact of the network of relationships in the stages of human development [6,7,8,9,10], but none of the surveys carried out the mapping of social support networks, or significant social networks, in relation to support for overcoming the experience of child sexual abuse.
The concept of significant social networks was proposed by Sluzki [11] based on the observation that the self is not something contained only within the limits of the body itself; the self results from the existence of other people and the interactions that emerge with them, as they are close and establish relationships that define the individual. The significant social network is characterized by the group of people with whom there are regular exchanges and interpersonal contacts, with short or extensive dialogues, or even just by the exchange of communicative signs [12]. According to this author, in social exchanges individuals in the social network embody and become real, and this experience delimited in time and space leads to the organization of identity, which is continually reconstructed from the interaction with other people. Considering the description of significant social networks [11,12], there is a need to identify the social bonds of victims of child sexual abuse, as it is an experience with numerous negative psychosocial repercussions throughout life and that the victims depend on healthy bonds to overcome the trauma.
Therefore, the analysis of significant social networks referring to structure, functions and attributes allows visibility to the network of relationships of people who suffered sexual abuse in childhood. At this point lies one of the main academic contributions that this research intends to make, bringing new data that add to other similar research, considering the relationship between sexual abuse in childhood and significant social networks. It also seeks to expand scientific knowledge about the importance of social bonds in promoting the integral health of victims of childhood sexual abuse. Finally, this research aimed to map the significant social networks of adult women in psychiatric care who are victims of childhood sexual abuse.
2. Materials and Methods
This research is based on a study that used a qualitative research design, using the significant social networks map in a clinical sample of adult women in psychiatric care who were victims of childhood sexual abuse.
2.1. Participants
Ten adult women from a psychiatric clinical sample with a history of sexual abuse in childhood or adolescence were selected for the study. In defining the sample, the main researcher (psychiatrist) and the second researcher and also research supervisor (psychologist) defined and assessed the consistency and applicability of the inclusion and exclusion criteria used in the sample selection.
The inclusion criteria were: 1) participation in previous psychiatric or psychological screening, verifying the occurrence of sexual abuse in childhood; 2) participation in previous psychiatric or psychological screening, confirming the absence of changes or cognitive disorders that would make participation unfeasible at the time of the research; 3) individuals with a history of medical, social, psychiatric or psychological care for the sexual abuse suffered; 4) women over 18 years of age. Exclusion criteria were: 1) previous finding of persistent and severe emotional fragility related to sexual abuse; 2) prior observation of any type of acute psychological distress that could be exacerbated by participation in the research; and 3) inability or resistance to expose the abuse situation.
2.2. Instruments
Three instruments were used in this research: a semi-structured interview, the Significant Social Networks Map and a sociodemographic questionnaire. A semi-structured interview script was used to establish the initial rapport (researcher's presentation and dialogue construction), and as a way to prepare the interviewee for subsequent application of the network map. The interview aimed to provoke a free report of the initial evocation of sexual abuse in childhood, that is, a brief investigation of its occurrence. The sociodemographic questionnaire investigated aspects related to education, age, marital status, religiosity, whether the interviewee has children and professional monitoring to deal with the consequences of abuse.
The Significant Social Networks Map [12] aims to identify people, groups, and institutions that offer support in specific situations, as seen in Figure 1.
The Significant Social Networks Map integrates four quadrants: 1) Friendships; 2) Family; 3) Work or study relationships; and 4) Community Relations. This last quadrant also includes the relationships with the health system, social agencies or government assistance agencies, increasing the granularity and detailing of the types of care that the victim of childhood sexual abuse may have received. The quadrants comprise three concentric circles, with the level of intimacy of the relationship being increasingly represented from the inner circle towards the outer circle, that is, more intimate relationships are closer to the center of the Significant Social Networks Map, and occasional or less frequent relationships are closer to the edges of the map.
2.3. Procedures
The Research Ethics Committee of the Tuiuti University of Paraná issued a favorable report to the research (CAAE 35166220.5.0000.8040). The women, selected through the inclusion and exclusion criteria, were invited by the researcher to participate in the research, accepted by signing the Informed Consent Form.
Each participant was approached individually in the researcher’s psychiatric office, in a private room and free from external interference. After establishing the rapport, the significant social networks were mapped and, finally, the sociodemographic profile was characterized. The registered information was stored in a private and proper file for the tabulation of the results and later analysis. The whole procedure of filling in the network map was carried out in a single session, in a total application time ranging from 30 to 60 minutes. After the maps were applied individually, a single map was built to represent the participants.
2.4. Data Analysis
The data analysis was performed using recommendations of the Moré and Crepaldi [13] and according to the characteristics of significant social networks established by Sluzki [11,12]. Faced with the unique map constructed by each participant, a count of the significant people and exploration of the points that were selected (Structure and Functions of the network, and Attributes of the bond) was performed.
In the Structure the size of the network is verified, being considered as a small network that with up to seven elements, medium size network between eight and ten elements, and large size network with the number greater than ten people/institutions [12]. The density is identified, which refers to the connections between members, and the quality of relationships; the composition or distribution is described, the position that each member occupies in the quadrants, and the dispersion that refers to the geographical distance between members. Homogeneity and heterogeneity are analyzed, identifying gender and sociocultural diversity.
In Functions it is described what kind of support is offered by the network, for example, emotional support, material support, social companionship, cognitive guidance, or social regulation.
In the Attributes of the tie, the characteristics referring to reciprocity are verified, that is, the performance of similar functions among the participants and the intensity of the ties, estimating the degree of commitment and intimacy among the ties in the relationship. Next, multidimensionality, or the different roles a person may play in the network, is checked. The frequency of contacts, the manner in which people establish contacts, and the history of the relationship are also analyzed, with a description of the initial contact between people and the forms adopted to maintain the ties.
3. Results
The research participants had ages ranging from 20 to 40 years. For calculation purposes only complete years of age were considered, and the average age was 28.8 (SD=8.12). Four participants have completed college education, five have incomplete college education or are studying, and one participant has a Technological level. One participant has an incomplete Master's degree. Regarding marital status, six participants are single, three are married, and one is divorced. Only one of the participants has children (a boy and a girl).
Regarding religiosity, four participants declared that they do not follow any religion or spiritual line, and six participants divided themselves among Umbanda, Catholicism, Jehovah's Witnesses, Evangelical Religion, and Spiritualism. The participant with the longest period of psychiatric follow-up has been in this process since she was 15 years old, and one participant has been for one month. The participants undergo psychiatric follow-up for a variety of causes, usually linked to relational or emotional difficulties in present life, but involving sexual abuse suffered in childhood. Six participants reported intrafamilial sexual abuse and four suffered extrafamilial abuse.
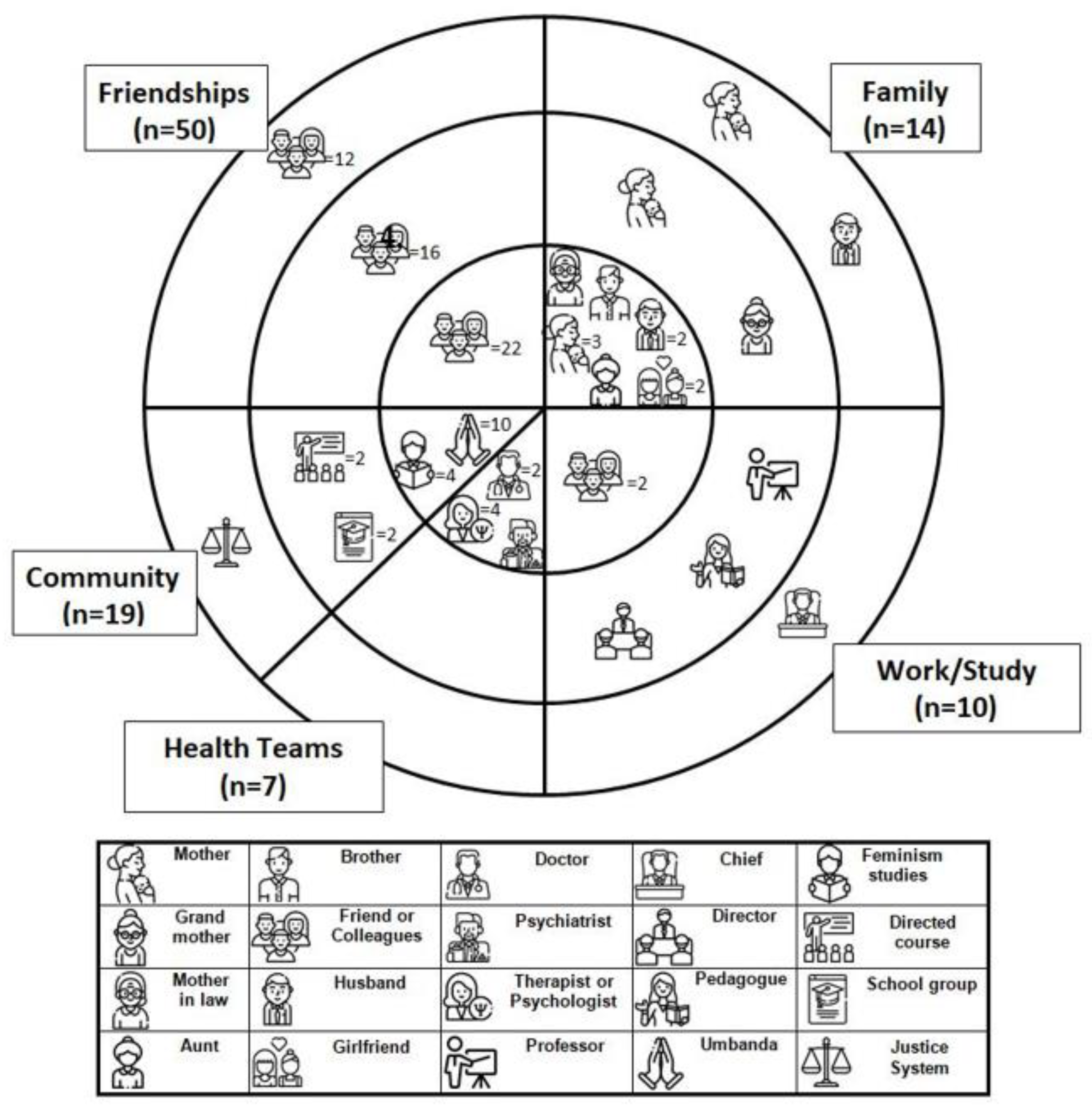
Each of the interviewees was invited to create her own map of significant networks with the assistance of the main researcher. The results of each individual map were collected, compiled, and, from the identification of each interviewee's most important ties, a single map representative of the ten participants was structured. The unified map contains standardized symbols to identify the social bonds (e.g., "mother," "husband," "therapist," etc.), which were also assigned numbers referring to the frequency of social bonds. The analysis of each quadrant of the interviewees was performed, and then it was possible to identify the main characteristics of the individual maps regarding the structure, functions, and attributes of the ties in the network of relationships. The unified map is shown in Figure 2.
As can be seen in Figure 2, the Friendships quadrant was the most populous, followed by Community, Family, and Work/Study. The smallest number of members occurred in the Health Team quadrant. The next topics present the analysis of the results of the significant social network map divided by quadrants.
3.1. Friendships
The Friendships quadrant is considered the most populous, compared to the other quadrants of the network. The network is large in size, with high density, low dispersion and high distribution, with all three circles filled. It was also observed heterogeneous composition
due to the various modalities of friendships composed of men and women of different ages, which are characterized as an important source of support. In this sense, it is possible to understand that the network of friendships has a high bond that contributes to people staying physically close. The largest number of relationships was observed in the inner circle, that is, of greater affective proximity.
The functions of the support network that stood out were: 1) Emotional support, with positive emotional attitudes and absence of judgment. Empathy, when the friend is able to put himself or herself in their place, is perceived as an opening to talk about the feeling of guilt which, for the interviewees, seems to be the greatest focus of suffering; 2) Material support: characterized, for example, when clothes from older children are passed on to friends who have younger children; 3) Social companionship, highlights the importance of being together with another person, even if it is in silence, and the value of sharing laughter with someone at certain times. It was also highlighted the fact of having company to go somewhere that generated anxiety, since memories of the abuse could be evoked by the place.
Regarding the attributes of the ties, the predominant function was emotional support. Multidimensionality was observed in the case of friendships, with emotional support, material support, and social companionship, which offer victims the possibility of receiving support in various areas of their lives, be it material, financial, counseling, sheltering, organization, or referral to services. The frequency of contacts is high, and Reciprocity was also observed, with Intensity in the bonds, which results in a high degree of intimacy. In the History of the relationship, some of the friendships reported by the participants present an initial bond characterized by similar stories of childhood sexual abuse, although this is not a determinant for initiating or deepening the friendship.
3.2. Community
The community quadrant presents a large network size, high distribution and density, and low dispersion, with most of the links belonging to the inner circle. A high degree of bonding was observed among people who are physically close to each other, and the network presents a heterogeneous character, due to the high diversity among institutions and the differences in ages and genders of the people inserted in this quadrant. The following institutions stood out: History College and State College; Justice System; Umbanda; Evangelical Church; Feminist movement groups, and Jehovah's Witnesses. The role of study and discussion groups with specific themes (feminism, beauty, among others) stands out, in which participants can share opinions about theoretical concepts and their applications in their daily lives.
Observed functions of the support network: 1) Emotional support, represented as a source of relief when they feel alone; 2) Social companionship, the women reported that they meet for study groups and after that they have group leisure activities. 3) Cognitive guide: religious bonds bring people who serve as advisors, helping to make decisions to reflect in moments of difficulty. Ties from religious institutions, for example, Umbanda and the Evangelical Church, play parental roles that help in the choice of paths for life. 4) Material support: religious institutions and feminist movement groups offer financial help when needed.
Regarding the attributes of the bond, the predominant Function was emotional support. There is multidimensionality in the attachment functions of emotional support, material support, cognitive guidance, and social companionship. The frequency of contact is high due to the regularity of participation in groups, courses, and religious services, which usually have scheduled days and times for meetings. There is reciprocity with high intensity bonds that are reflected in their interactions, which often include mutual help among the components and support for various aspects of community life.
3.3. Family
In this quadrant the structural characteristics show a large network size, high distribution, low dispersion, and high density. The composition is heterogeneous with links distributed between both genders, and with people of various age groups, educational backgrounds, and sociocultural levels. The main ties in this quadrant refer to the mother figure, important for five of the participants. Also making up the quadrant of significant relationships are sister, brother, aunt, mother-in-law, and husbands. The largest number of relationships is in the inner circle of this quadrant, which shows affective ties with intimacy.
The main functions of the support network are: 1) Emotional support: mothers stand out as the first to know about the abuse, which was reported by four participants, and therefore they became an important bond throughout life and development; 2) Cognitive guidance and advice: mothers, husbands, and girlfriends are behavioral guides indicating ways to function in other relationship groups; 3) Social regulation: participants indicated that other family members are considered role models, people they admire and to whom they try to resemble in their own lives; 4) Material support: through donations and financial loans, paying bills, and offering services, such as rides, trips, among others.
Concerning the attributes of the bond, it is observed that the predominant role is that of emotional support, mainly because mothers are the first to be informed about the abuse, which is followed by siblings, mothers-in-law, grandmothers, and partners. Multidimensionality is observed, with the family playing the roles of emotional support, cognitive support and advice, material support, social regulation, and cognitive guidance. Contacts are frequent, with a high level of intimacy in the relationships, and the Intensity of the bond is high. There is Reciprocity: the abuse in some cases became an element that provoked closeness among family members. In the History of the relationship, although maternal figures were mostly the first to know about the abuse suffered, some interviewees reported difficulty in disclosing the experience of abuse. In the situations of disclosure in which there was acceptance and understanding, this event enabled cohesion and strengthening of the relationship, something often observed in the relationship with the husband, for example.
3.4. Work/Study
The structure of the Work and Study network is considered medium in size, with links showing high distribution and density. The dispersion is low, with relationships geographically close. The composition is heterogeneous, indicated by coexistence in work and study environments with people of different ages, genders, and socioeconomic levels. One participant indicated her master's advisor as an important relationship in the study place, and at work the director, the pedagogue, and the psychologist represent significant bonds. The boss, study colleagues, and a professor were also mentioned.
The main functions of this support network are: 1) Emotional support: which occurs through active and empathetic listening, with displays of affection by bosses and coworkers; 2) Social companionship: offered by work and study colleagues, who are also companions for leisure activities, going out together, shopping, and having fun; 3) Cognitive guidance and advice: coworkers and bosses offer teachings that are important for the performance of professional tasks. 4) Social regulation: the behavior of bosses, teachers and some colleagues are seen as examples, which stimulate the development of forms of negotiation and conciliation at work or study.
As for the bond attributes, the predominant function was emotional support, identifying significant relationships of the interviewees with supervisors, co-workers, and other students. There is Multidimensionality, with emotional support, cognitive guidance, social companionship, and social regulation of supervisors, co-workers, and students, offering possibilities to deal with professional situations. Frequency of contact is high due to regularity of classes or work schedules with extended periods of contact, with Reciprocity due to the need for cooperation for an academic assignment to be completed or a professional goal to be achieved. Intensity of the bond is high, reinforced by shared leisure activities during work or study shifts, and in Relationship History, disclosure of child sexual abuse was reported to co-workers, students, and supervisors who offered cordiality, support, and listening in daily relationships.
3.5. Health Teams
The Health Team network is small, distribution and dispersion are low, and density is high. The network presents heterogeneity, with professionals of different genders and ages. Although it is a small network, it was observed that all the links in the quadrant are in the inner circle, with close and intimate relationships.
The main functions of the network are related as follows: 1) Emotional support: function that includes the actions of a doctor, psychologist, and psychiatrist to help the victim face situations with a realistic attitude toward the concrete world, while providing a welcoming and safe space to overcome the abuse. Two participants indicated that the psychologist was the first person to know about the sexual abuse. Another interviewee spoke of the importance of establishing a positive bond with the psychiatrist and feeling welcomed; 2) Cognitive and advice guide: refers to the importance of having direct and objective help from all health professionals. The increase in self-esteem and self-confidence are also attributed to the lessons coming from living with the health team; 3) Social regulation: participation in the psychotherapeutic process helps patients to also experience the place of other people around them, which allows them to understand how to establish social bonds.
In regard to the attributes of the bond, the predominant Function is emotional support, and the victim usually seeks this type of help due to psychic suffering or damage to their affective relationships. There is Multidimensionality, with emotional support and cognitive guidance as predominant functions, and health professionals play different roles. Contact Frequency is high due to the regularity of care sessions and consultations. Reciprocity is also high, and in Intensity of the bond, respondents indicated that the bond with the psychologist is important in their lives, progressively adding new roles usually linked to other bonds, such as friendships or community relationships.
4. Discussion
In this research it was found that friends provide important emotional support for the women interviewed, since the quadrant of friendships has the largest number of relationships. It is possible to infer that they occupy a space of support that was not filled by family ties, especially in cases where the woman did not receive support from her mother, father, or siblings, or when she decided to keep silent about the abuse she suffered. Silencing is common in cases of childhood sexual abuse perpetrated by relatives or family friends, aiming to protect the family dynamic [14]. Friends, outside this dynamic, do not present the same obligation to accept the "silence pact," which brings an important support role to the victim, who finds a circle of relationships in which she can expose her feelings and reveal the abuse.
The interviewees cited that friends are equivalent to family, or that certain friendships are considered part of their original family because of the proximity that allowed the disclosure of the abuse. The family group is the key element in the disclosure of the abuse, because they are the first people of reference who should provide the listening by making the first referrals to the competent authorities [15].
In the community quadrant, the institutional ties of religious groups were shown to be important, as well as the studies and ideas of feminism that were also helpful in understanding and coping with the consequences of abuse. Most victims of childhood sexual abuse are female, between 75% and 90% of cases, on average across the reviewed studies, which indicates a social perception of the female gender as more vulnerable to sexual abuse [1,2,3,16]. In this sense, the support structure offered by feminist groups restores self-esteem by promoting positive changes for women.
With regard to the intrafamilial sexual abuse reported by the participants in this research, the abuse was not disclosed in the family for fear of retaliation or aggression against the abuser, who often also belonged to the family itself, or for fear of losing ties. As indicated by Platt et al. [4], most abusers are known to the victims, a fact that was repeated in this research. This may be a hindrance to family support network formation, and some of the victims disclosed the abuse only when they formed their own families, leaning emotionally on their spouses. In the case of intrafamily sexual violence, "pacts of silence" are common, described as "family and group arrangements that aim to accommodate roles, so that some submit to others, in a hierarchy usually of power, following the example of the authority of parents over children" [3].
Brattfjell and Flam [17] identified that disclosure depends on the existence of a trusted person and, in the family quadrant, the role of mothers was evidenced, who offered support from the beginning, corresponding to the role of primary trust. There are data that indicate the increase in reporting by the victims themselves, but even so, the mother or whoever occupies this role in the family remains the person who accompanies the victim to the police station or other official body [18].
The Work and Study network showed an average size that was smaller than the Friendships, Community, and Family quadrants. The presence of fewer ties in this quadrant may have been caused by the loss of studies or work due to the abuse suffered, a fact reported by the research participants and that is included as one of the diagnostic criteria for Post-Traumatic Stress Disorder in the DSM-V of the American Psychiatric Association [19].
Sabella [20] presented evidence that abused children experience more emotional problems than other children, because the cognitive system of sexually abused children becomes engaged with concerns that are unusual for their age group [21]. This confirms the fact that the participants in this research seek psychiatric follow-up, which allows highlighting the need for health professionals to be prepared to attend to complaints and offer efficient forms of treatment.
In an integrative review on the repercussions of sexual abuse in childhood and adolescence [22], highlighted that the psychological, physical, sexual, and social consequences of the event occur throughout the victimized individual's life. Jong and Dennison [23] also agree with the long-term repercussions, as there are specific factors that affect victims in their adult life, for example, losses in educational attainment or income levels. Sexual abuse in childhood can lead to socialization and relationship problems in adulthood, difficulties in relationships with the opposite sex, and losses in the formation of professional bonds [24]. On the other hand, in this research it was found that women were able to establish social bonds in adulthood, which represented a form of support, and also initiated marital relationships, which represents overcoming the experience of abuse experienced in childhood. Although the authors emphasize the consequences of abuse throughout life, it is important to highlight that the establishment of a significant social network represents a protective factor, and each person experiences this in a particular way with their personality characteristics, so it is necessary to develop a relativized analysis.
The health team network is small, composed of psychologist, doctor and psychiatrist. The interviewees establish relationships with several professionals, which agrees with the observation of [25] regarding childhood sexual abuse, which refers to a diverse experience and composed of several elements for each victim, which determines the need for a multiprofessional approach. The interviewees sought professional help highlighting the need for a specialized team.
The functions performed by health professionals are different from those offered by friends and family. Researchers [26] and agencies [27] indicate the need for specialized listening for victims of sexual abuse, the application of protocols, and particularized care to rescue the capacity for personal growth and social development. It is understood, from the results generated, that although it is a small network, the health team plays an important role in the significant social network of women victims of childhood sexual abuse, which represents a protective factor for health promotion [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. In summary, studies on social support networks allow identifying protection, risk and vulnerability factors to build intervention strategies [29,30].
5. Conclusions
The significant social networks of adult women in psychiatric care who are victims of childhood sexual abuse are diverse and with different types of support. Thus, this represents a protective factor to overcome the effects of this childhood experience. We highlight the bonds of friendship and family relationships, which helped the women to overcome the trauma.
The identification of significant social networks is important for the definition of public policies for prevention and treatment, as it allows official agencies to clearly understand how victims behave to overcome abuse, and which relational points need reinforcement in this process. Thus, diverse resources can be directed to the networks that prove effective in the prevention and treatment of childhood sexual abuse.
Regarding the limitations of this research, the sample was small and is supported by the qualitative data presented by the participants. There is a need to expand the sample in future research, investigating clinically relevant variables (depression, anxiety) and their relationships with significant social networks.
It is important to include in future studies victims who are male and who are in psychiatric or psychological treatment. It is recommended that future research based on the mapping of significant social networks be longitudinal, following the participants for an extended period, seeking to apply the map annually. Finally, psychometric instruments can be added to the research, aiming to establish in a detailed way the level of psychological distress and coping strategies. In regards to the practical applications of this research, we highlight that the network map represents an instrument that allows health professionals to identify the social bonds of their patients, making the necessary recommendations and treatment. The use of the network map is recommended in clinical practice to assist in decision making.
Author Contributions
The authors K.C.B. and A.V.S.A. were responsible: conceptualization, methodology, formal analysis, investigation, data curation and writing (original draft preparation, review and editing). All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Araújo, G.; Ramos, M.; Zaleski, T., Rozin, L., Sanches, L. Determinantes da violência sexual infantil no estado do Paraná – Brasil. Rev Espaço para a Saúde, 2019, 20(2), 42-54.
- Delziovo, C.R.; Bolsoni, C. C.; Nazário, N. O.; Coelho, E. B. S. Características dos casos de violência sexual contra mulheres adolescentes e adultas notificados pelos serviços públicos de saúde em Santa Catarina, Brasil. Cadernos de Saúde Pública, 2017, 33(6).
- Ministry of Women, Family and Human Rights. Violência contra Crianças e Adolescentes: Análise de Cenários e Propostas de Políticas Públicas. 2018. Brasília: MDH. https://www.mdh.gov.br/biblioteca/consultorias/conada/violencia-contra-criancas-e-adolescentes-analise-de-cenarios-e-propostas-de-politicas-publicas.pdf.
- Platt, V. B.; Back, I.C.; Hauschild, D.B.; Guedert, J.M. Violência sexual contra crianças: autores, vítimas e consequências. Ciência & Saúde Coletiva, 2018, 23(4), 1019–1031. [Google Scholar]
- Law 13.431 of April. Estabelece o sistema de garantia de direitos da criança e do adolescente vítima ou testemunha de violência e altera a Lei nº 8.069, de 13 de julho de 1990 (Estatuto da Criança e do Adolescente). 2017. Brasília, DF: Presidência da República. http://www.planalto.gov.br/ccivil_03/_Ato2015-2018/2017/Lei/L13431.htm.
- Yount, K.M.; Krause, K.H.; Miedema, S.S. Preventing gender-based violence victimization in adolescent girls in lower-income countries: Systematic review of reviews. Social Science & Medicine, 2017, 192, 1–13. [Google Scholar]
- Buccieri, K.C.K.; Azevêdo, A.V.S.A. Abuso sexual na infância e redes de apoio social: guia prático para avaliação e clínica forense. 2023. Dialética.
- Fontes, L. F. C.; Conceição, O. C.; Machado, S. Violência sexual na adolescência, perfil da vítima e impactos sobre a saúde mental. Ciência & Saúde Coletiva, 2017, 22(9), 2919-2928.
- Herbell, K.; Bloom, T. A Qualitative Metasynthesis of Mothers’ Adverse Childhood Experiences and Parenting Practices. Journal of Pediatric Healt Care, 2020, 34(5), 409–417. [Google Scholar] [CrossRef] [PubMed]
- Konya, J.; Perôt, C.; Pitt, K.; Johnson, E.; Gregory, A.; Brown, E.; Feder, G.; Campbell, J. Peer-led groups for survivors of sexual abuse and assault: a systematic review. Journal of Mental Health, 2020, 1-13.
- Sluzki, C. E. Personal Social Networks and Health: Conceptual and Clinical Implications of Their Reciprocal Impact. Families, Systems, & Health, 2010, 28(1), 1–18. [Google Scholar]
- Sluzki, C. E. A rede social na prática sistêmica: alternativas terapêuticas. 1997. Casa do Psicólogo.
- Moré, C.L.O.O.; Crepaldi, M.A. O Mapa de Rede Social Significativa como Instrumento de Investigação no Contexto da Pesquisa Qualitativa. Nova Perspectiva Sistêmica, 2012, 43, 84–98. [Google Scholar]
- Hohendorff, J.V.; Patias, N.D. Violência sexual contra crianças e adolescentes: identificação, consequências e indicações de manejo. Barbarói, 2017, 49, 239–257. [Google Scholar] [CrossRef]
- Coutinho, M.M. L.; Morais, N.A. O processo de revelação do abuso sexual intrafamiliar na percepção do grupo familiar. Estudos e Pesquisas em Psicologia, 2018, 18(1), 93–113. [Google Scholar] [CrossRef]
- Silva, R.W.S. , Azambuja, C.V.; Santana, A. Perfil de crianças e adolescentes vítimas de maus-tratos atendidos em ambulatório de psicologia da região sul do Brasil. Aletheia, 2015, 47/48, 136–141. [Google Scholar]
- Brattfjell, M. L.; Flam, A.M. “They were the ones that saw me and listened.” From child sexual abuse to disclosure: Adults’ recalls of the process towards final disclosure. Child Abuse & Neglect, 2019, 89, 225–236. [Google Scholar]
- Mastroianni, F.C.; Silva, B.P.; Mauro, F.G.; Gouvêa, N.M.F.; Leão, A.M.C. Violência sexual infantojuvenil em processos criminais: uma pesquisa documental. Psicologia em Pesquisa, 2021, 15(2), 1–25. [Google Scholar] [CrossRef]
- American Psychiatric Association. Manual Diagnóstico e Estatístico de Transtornos Mentais. 5a ed. 2014. Porto Alegre: Artmed.
- Sabella, D. Revisiting Child Sexual Abuse and Survivor Issues. AJN, 2016, 116(3), 48–54. [Google Scholar] [CrossRef]
- Schaefer, L.S.; Brunnet, A.E.; Lobo, B.O.M.; Carvalho, J.C.N.; Kristensen, C.H. Indicadores Psicológicos e Comportamentais na Perícia do Abuso Sexual Infantil. Temas em Psicologia, 2018, 26(3), 1467–1482. [Google Scholar] [CrossRef]
- Cruz, M. A.; Gomes, N. P.; Campos, L. M.; Estrela, F. M.; Whitaker, M.C.O.; Lírio, J. G.S. Repercussões do abuso sexual vivenciado na infância e adolescência: revisão integrativa. Ciência & Saúde Coletiva, 2021, 26(4),1369-1380.
- Jong, R.; Dennison, S. Recorded offending among child sexual abuse victims: A 30-year follow-up. Child Abuse & Neglect, 2017, 72, 75–84. [Google Scholar]
- Gatuguta, A.; Colombini, M.; Seeley, J.; Soremekun, S.; Devries, K. Supporting children and adolescents who have experienced sexual abuse to access services: Community health workers’ experiences in Kenya. Child Abuse & Neglect, 2021, 116(1), e104244.
- Florentino, B.R.B. As possíveis consequências do abuso sexual praticado contra crianças e adolescentes. Fractal: Revista de Psicologia, 2015, 27(2), 139–144. [Google Scholar] [CrossRef]
- Campos, J. L. Criança vítima de violência sexual: Recortes de um caso atendido na Abordagem Centrada na Pessoa. Psicólogo inFormação, 2016, 20(20), 25–47. [Google Scholar] [CrossRef]
- Conselho Federal de Psicologia. Referências Técnicas para Atuação de Psicólogas(os) na Rede de Proteção às Crianças e Adolescentes em Situação de Violência Sexual. 2020. Brasília/DF.
- Azevêdo, A. V. S; Silva, M.A.; Reis, T.C.M. Promoção da saúde no contexto das redes sociais significativas. Nova Perspectiva Sistêmica, 2019, 28(63), 55-66.
- Reis, T.C.M.; Azevêdo, A.V.S. Redes sociais significativas de homens em situação de rua no sul do Brasil. Estudos de Psicologia (Natal), 2020, 25(3), 324-334.
- Silva, M.A.; Azevêdo, A.V.S. Mulheres em projetos comunitários: redes sociais significativas e a promoção da saúde. Estudos de Psicologia (Natal), 2020, 25(4), 436-448.
Figure 1.
Significant Social Networks Map model. Source: Adapted from Sluzki [12].
Figure 1.
Significant Social Networks Map model. Source: Adapted from Sluzki [12].
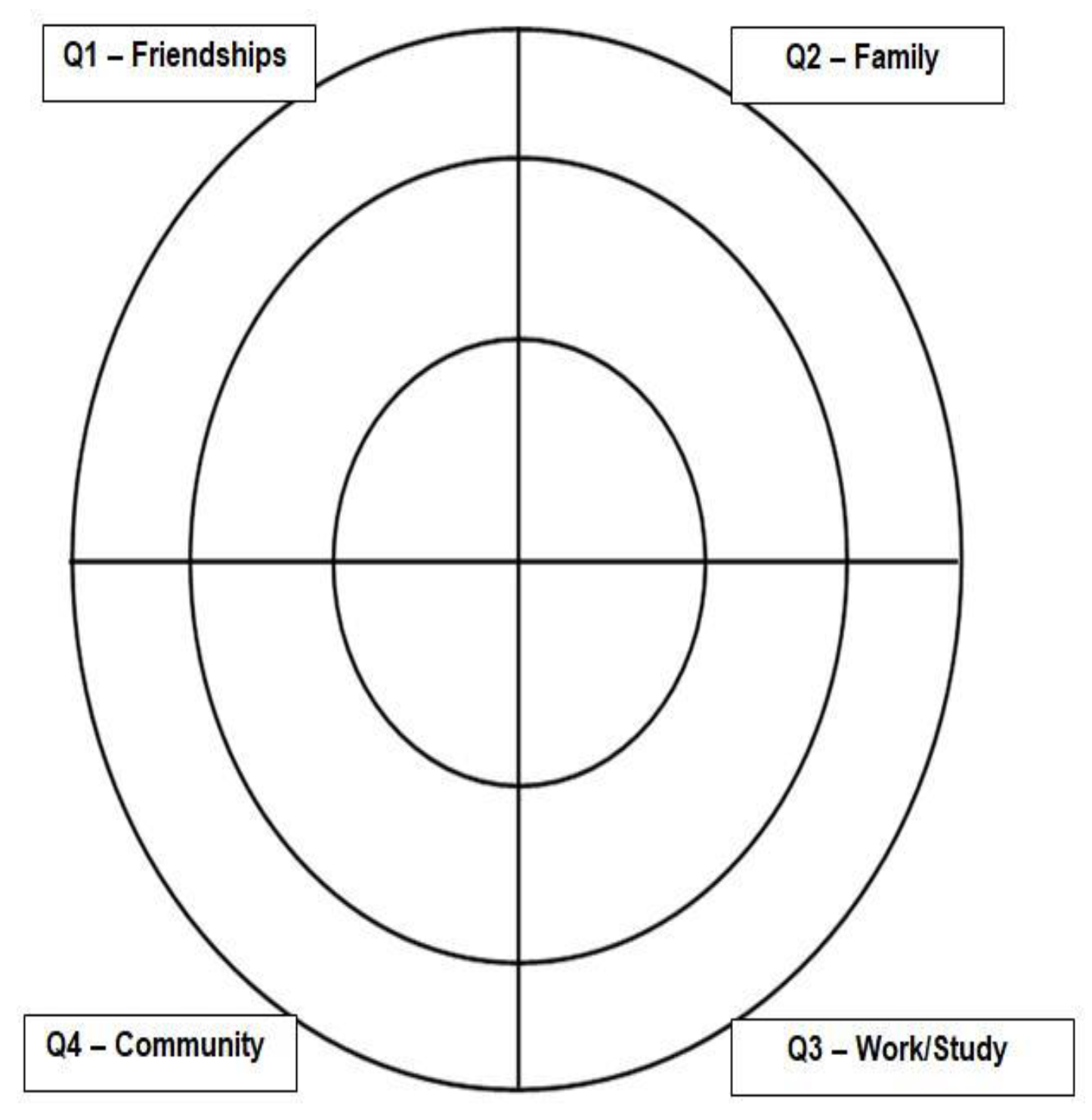
Figure 2.
Significant Social Networks Map for the research participants.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



