Submitted:
30 September 2023
Posted:
03 October 2023
You are already at the latest version
Abstract
Background The workload of nurses in the intensive care unit (ICU) can affect the quality of nursing services. Aim This study aimed to determine the relationship between the nursing activity score and missed care in patients hospitalized in the ICU in Zanjan, Iran. Methods This observational and prospective study was conducted from April 3 to September 18 in 2021. In this study, the tools used included a patient and nurses' profile questionnaire, Nursing Activity Score (NAS). Missed care was observed in the 301 patients for whom the NAS was calculated. Analysis of variance (ANOVA) was used to investigate the differences in mean levels of missed care. Logistic regression models were used to assess the association between factors and missed nursing care. Results Results show that the Medical ICU's mean NAS was 76.31 (95% CI: -13.06 -14.89). In 9 dimensions of care, the extent of missed care was 40.7%. In the care dimensions of assessment, hand hygiene, and infection control, the mean NAS had a statistically significant increase at higher levels of missed care (P<.5). Furthermore, work experience was identified as a protective factor for missed care (OR =.59, 95% CI: .37–.94, χ2= =4.97, p =.026). Conclusion The study revealed a high incidence of missed care. The study revealed that the mean workload was high in certain dimensions of care such as assessment, hand hygiene, and infection control. The increase in workload for nurses results in lost care. Nonetheless, the utilization of experienced nurses can help mitigate this problem. However, utilizing experienced nurses can help reduce this problem.
Keywords:
Care left undone
; health services misuses
; medical errors of omission
; missed nursing care
; workload.
1. Introduction
The nursing workload is one factor that can affect patient safety and nursing care in the intensive care unit (ICU) (1). Because of the conditions of the patients in ICU, nurses working in the ICU spend more time directly caring for the patients and have various responsibilities (2, 3). Nurse workloads are defined as the amount of performance required to carry out nursing activities. The amount of nursing time, level of nursing qualification; direct patient care weight; the amount of physical activity; and the complexity of care are the attributes of nurses’ workload (4).
Undesirable consequences, such as physical and emotional fatigue, nurse burnout, omission of nursing care, and reduction in quality, have been linked to workload in some studies (5-8). Missed care refers to the delay or omission of any aspect of patient care (9). The review study revealed that a majority of nurses (55-98%) reported leaving at least one task incomplete (10). The most important reported injuries related to missed care include phlebitis, pressure ulcers, skin ulcers, infection, bed falls, delirium, uncontrolled pain, and death (11, 12). Patients can experience short-term and long-term effects when nursing care is intentionally or unintentionally omitted (13).
Thoroughly examining all aspects of missed care during healthcare studies is challenging. In case of incorrect treatment, such as nonstandard bandaging, it can be detected and evaluated, but in the absence of treatment, detection is difficult without special tools like video recording or direct observation (14). Identifying factors related to missed care in the ICU and the effects of nurses’ physical workload on the quality of care are important in any culture. Previous studies relied on nurses' self-reporting to investigate missed care. The current research employed the observation method to evaluate the missed care for enriched data. This study aimed to determine the relationship between the nursing activity score and missed care in patients hospitalized in the ICU in Zanjan, Iran
2. Methods
Study design and setting
This observational and prospective study was carried out in Zanjan City, Iran, between April 3 and September 18, 2021. This study was conducted in a medical ICU of one of the training hospitals in Zanjan (Figure 1).
Sampling
All patients who were admitted to the medical ICU during the study were included in the research. The patient's legal guardian's consent was a necessary inclusion criterion for the study. To identify missed care, the nurses' performance was observed. The study observed the performance of full-time nurses who will participate. The sample size was estimated using the following formula according to study Alizadeh et al., the sample size needed to be 298 patients with α = 0.05, δ =.88, and d = 0.1 (15).
Measures
This study employed three instruments: a questionnaire for patient and nurse profiling, the Nursing Activity Score (NAS), and a missed care checklist.
Patient and nurses’ profile questionnaire
The patient profile included age, gender, diagnosis, GCS, and ICU length of stay. The personal and professional profiles of nurses were constructed based on gender, age, marital status, educational level, and nurse-to-patient ratio.
Nursing activity score (NAS)
This instrument, comprising 23 items, was developed by Miranda et al. (Miranda et al., 2003). This scale measures the percentage of a nurse's time spent directly caring for a critically ill patient during 24 hours in the ICU. The scoring range for the 23 items is from zero to 177 percent. The items comprise titration and monitoring, medication, laboratory, hygiene procedures, support and care of relatives and patients, administrative and managerial tasks, care of drains, ventilatory support, renal support, neurological support, metabolic support, and specific interventions. The inter-rater reliability of the questionnaire was evaluated in this study using Cohen's kappa coefficient. This tool has been confirmed as valid in various countries (15-17). Regarding the validity of the translation process, the NAS was translated based on the standards recommended in the guidelines (18). The NAS was translated into Persian by two English-Persian translators using the forward-backward translation technique. The NAS was independently translated into Persian by two translators. A group of experts, including some of the authors of this article and two other professional translators, reviewed and commented on these two Persian versions of NAS. After being translated back into English by a Persian-English translator, a group of experts confirmed the accuracy of the Persian NAS. Content validity was assessed by 10 experts (6 faculty members from the Department of Intensive Care Nursing and Emergency Nursing and 4 nursing managers). These experts evaluated the content of the Persian NAS. Afterward, the item and scale level content validity indexes were calculated for the Persian NAS tool. The 10 experts rated the relevancy of items using a 4-point Likert scale. The range of acceptable CVI values is greater than 0.80. Furthermore, two researchers simultaneously evaluated the NAS for 30 patients. The score agreement between the two researchers was 93%.
Missed care checklist
Previous studies were used as a basis for providing missed cares in the ICU (19-24). A checklist for missed care was reviewed by a panel of experts. This panel consisted of 6 critical care nursing faculty, 2 intensive care specialists, and 2 ICU head nurses. These experts identified 9 dimensions of missing care. The 9 dimensions of care comprise: 1. Assessment, 2. Mobility and motion, 3. Response to patient’s needs and call alarm within 5 min, 4. Patient education, 5. Hand hygiene, 6. Infection control (eye, skin, mouth, perineum and wound or sore care, IV/central line site care and change of disposable devices according to hospital policy), 7. Oxygen therapy, 8. Implementation of urgency order, 9. The nutritional care. In each of these nine dimensions, there are four items. This checklist employs a rating scale of 0 (not applicable), 1 (not done), 2 (done incompletely), and 3 (done completely), with 3 being the highest score. The mean ratio was used to compute the score of each of the 9 dimensions of missed care, following this formula.
The missed care assessment had 4 levels. A scoring range of 1-25 indicates a very high level of missed care, while 26-50 indicates a high level, 51-75 indicates a moderate level, and 76-100 indicates a low level. The missed care checklist for 30 patients was scored by two researchers simultaneously to calculate inter-observer reliability. These two researchers achieved an 89% agreement in their scores.
Procedures
The NAS was compiled for each patient according to the reporting of the previous 24 hours by first author. Missed care in patients was evaluated through direct observation using the missed care checklist. Missed care was observed in the patients whose NAS was calculated. The nurse's care performance was observed on the patient to calculate their NAS. On average, each nurse participating in the study had their care performance observed eight times. Missed cares in patients were observed by a nursing master's intern researcher in the same medical ICU. Nurses were aware of the aim of the study. They were aware their performance would be observed, but the exact timing and details were unknown. The researcher's own presence in the ward allowed for natural observations of nurse behavior and performance.
Ethical considerations
This study was conducted after approving Iran’s National Committee for Ethics in Biomedical Research (IR. ZUMS.1397.324). Written consent was obtained from the legal guardian of the patient and nurses participating in the study. The purpose of the research was explained to the legal guardian of the patient and the nurses.
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, N.Y., USA). In this study, the kurtosis and skewness of the data were in the range (2, -2), so the data had a normal distribution. Descriptive statistics were reported as N (%) for categorical variables and the mean and confidence interval (CI) for continuous variables. Analysis of variance (ANOVA) was used to evaluate the mean difference based on the levels of missed care.
Logistic regression was used to assess the association of variables with the level of missed care. The regression analysis used the backward variable selection method because of the high number of variables included in the analysis. The following variables were included in the regression analysis: NAS, patient related variables (gender, age, patient diagnosis, level of consciousness based on GCS and type of oxygen therapy), nurse related variables (gender, age, marriage status, employment status, education level, work experience, working hours/months, and nurse-patient ratio).
To conduct a logistic regression, the high/low of missed care was summarized for each individual as follows. The high-missed care group was defined as ‘very high missed care’ or ‘high missed care’ and the low-missed care group was defined as ‘moderate missed care’ and ‘low missed care. Therefore, for each dimension, missed care was defined as ‘high missed’ if the option was 0-1, and as ‘moderate missed’ if the response was 2-3.
3. Results
Participant
Patient
Most of the patients hospitalized in this ward were men, with a mean age of 60.02±21.17 (95 % CI: -19.98-22.20). Metabolic disorders were the most frequently hospitalized in the medical ICU, and the patients were often intubated (endotracheal) and under ventilation (Table 1).
Nurses
The study involved 38 of 45 nurses. Table 2 shows that most nurses were female, married, with a bachelor's degree, and 3-5 years of experience.
NAS
The mean NAS in this Medical ICU was 76.31± 14.01 (95 % CI: -13.06 -14.89).
Frequency and percentage of missed care in each care
The results of Table 3 showed that the most frequently missed care include: Applying deep vein thrombosis (DVT) prevention (53.8%), skin and vascular assessment of the upper and lower limbs at the place of restriction (49.5%), attention to ventilator settings at the beginning of the shift (46.5%), change the direction of the endotracheal tube to prevent ischemia at least once per shift (34.6%), assessment and recording the patient’s mental state (35.5%), hand hygiene before touching a patient (33.2 %), assessment and recording of SPO2 of the patient (34.6), hand hygiene before performing care procedures (34.2%), checking the correct location of the endotracheal tube and measuring endotracheal tube intracuff pressure at least once per shift (25.9) and measuring gastric residual volume (28.2%).
Frequency and percentage of missed care dimensions
Motion and mobility had high missed care at 1.7%, while oxygen therapy, patient education, and urgency order implementation had low missed care. Missed care was moderate for responding to patient needs and alarms within 5 minutes, hand hygiene, infection control, and nutritional care. The score for missed care was moderate. Table 3 shows that missed care did not happen in 59.3% of cases.
The compare means of NAS according to levels of missed care dimensions
The results of evaluating the mean NAS based on the levels of missed care showed that, except for the evaluation dimensions, hand hygiene, and infection control (p<0.05), there was no mean difference in NAS in other dimensions and the total score of missed care (Table 4). Also, the results of the LSD post hoc test showed that, in the dimension of assessment (p=.018), hand hygiene (p=.013), and infection control (p=.016), the workload based on NAS at the medium level was significantly higher than the low level.
Factors related to the occurrence of missed nursing care
Work experience was the only remaining variable with R2=0.02 in the backward method of logistic regression. The prevalence of missed care was significantly lower in participants with higher work experience (OR =.59, 95% CI: .37–.94, χ2= =4.97, p =.026). Therefore, work experience is a protective factor for missing care.
4. Discussion
Results show that the mean NAS in Medical ICU was 76.31 of 177% (95 % CI: -13.06 -14.89).
In the study by Momennasab et al. in Shiraz (Iran), the mean NAS in the trauma ICUs was 65.3% ± 23.19% (25). The mean NAS in 16 hospitals in Belgium was 68.6% (26). In the study by Camuci et al., the highest mean NAS was reported in the burn ICU at 70.4% (27). In 19 ICUs across seven countries, Padilha et al. observed a mean NAS of 72.8%, ranging from 44.5% in Spain to 101.8% in Norway (28). The disparity in workload among studies may be because of distinctions in ICU typology. The workload of nurses in the burn, trauma, cardiac, and medical ICUs differs, as expected. In certain hospitals, ICUs are specialized for particular diseases, while in others, medical, trauma, and burn patients are admitted in one ICU. The mix of patients with various illnesses affects the nurses' workload.
This study showed that 40.7% of care was missed in 9 dimensions. Chegini et al.'s research discovered that 72.1% of nurses usually miss at least one nursing care during their last shift (29). Results Haftu et al. showed that 299 (74.6%) nurses and midwives commonly missed at least one nursing care in the perinatal setting (30). The study conducted by Ball et al. revealed that 86% of nurses couldn't complete one or more care activities because of insufficient time during their last shift (21). Ball et al. found that 74% of nursing care omissions occurred in general medical and surgical wards (31). Various settings have been used to conduct these studies. Most studies report a higher percentile of missed care than the present study. These studies have been conducted in different environments (wards and ICUs). The results in all these studies were based on self-reporting (21, 29-31), which can lead to either overestimation or underestimation by participants. Although this study was conducted observationally, it made the data more objective than previous studies.
The most missed care was mobility, motion, and hand hygiene dimensions, and the least missed care was the patient education dimension. A study showed that nurses had better hand hygiene practices with fewer instances of missed care, in contrast to our findings..(32). On the other hand, patient mobility is a crucial aspect of ICU recovery, and neglecting it may lead to complications and slow down the healing process (33). It's important for head nurses to supervise the careful administration of this care. Also, our result differs from the results of Chegini et al., who reported a high percentage of missed care in the dimension of patient education (29). Discrepancy in the results is attributed to the difference in the study setting. Due to low levels of consciousness, this dimension was inapplicable for most ICU patients in the present study.
The results of evaluating the mean difference of NAS based on the levels of missed care showed that, except for the dimensions, assessment, hand hygiene and infection control, there was no significant mean difference in NAS in other dimensions and the total score of missed care.
In the present study, infection control and hand hygiene were significantly related to NAS. The increase in workload led to a loss of care. In a study, hand hygiene was associated with workload (34). Hand hygiene and infection control can shorten ICU patients' hospital stays, so it is necessary to teach ICU nurses about the importance of hand hygiene.
Unlike previous research (35-37), the current study found no association between missed care and the personal or professional characteristics of nurses or patient characteristics. The present study has different results as Ball et al. observed a significant relationship between nurse-patient ratio and missed care (21). A review study found that missed nursing care reports were linked to low registered nursing staff (36). Tubbs-Cooley et al. found that missed care was associated with nurses' workload (35). In a review study, it was found that missed nursing care correlated with patient acuity, workload, work environment, and nurse characteristics, resulting in patients staying in the hospital for a longer period (37). The findings of previous studies varied because of differences in nurse-to-patient ratios between general wards and the ICU.
The study discovered that nurses' workload had little effect on the frequency and completeness of some routine care behaviors. Care that was not provided was sometimes documented in the nursing record, as noted in another study (38). De Marinis et al. found nursing records unsuitable for quality care evaluation (39).
In Iran, nurses have faced a high volume of documentation work (40). Although documenting care is vital, it may override patient care, causing nurses to unintentionally or intentionally exclude specific care. Complications from not providing adequate patient care often develop slowly. All healthcare providers, not only the nurse, are responsible for these patient complications. Studies in most countries have reported missed cares, indicating a lack of patient safety culture (21, 29-31). Missed care can be prevented by enhancing nurses' knowledge and changing the culture of patient safety, particularly among nursing managers (22, 41, 42). According to Tubbs-Cooley et al., system factors may be a contributing factor to missed care in this setting (32).
In line with Plein's research, our study found that work experience helps prevent missed care (43). Novice nurses, who had less work experience, were responsible for more patients. They also took care of patients who were far from the nursing station and the treatment room, requiring them to travel a long distance during their shift. These cases increased the workload of nurses. Appropriate staffing and fair work distribution prevent missed care. Missed care was found to be related to the work environment in prior studies (44-46).
5. Conclusion
The study revealed a high incidence of missed care. The study revealed that the mean workload was high in certain dimensions of care such as assessment, hand hygiene, and infection control. The increase in workload for nurses results in lost care. Nonetheless, the utilization of experienced nurses can help mitigate this problem. To assess the factors related to ICU nurses' workload and patient care quality, additional studies are recommended.
6. Strength and limitation
The study's strength was in using the observation method to measure missed care. Compared to previous studies, the data in this study is richer. Altering participant behavior and invading personal privacy are factors that limit observations. Nurses in the study had informed consent and awareness of objectives study, but were not informed of case details to reduce behavior change. By trying to keep the anonymity of the hospital and nurses, the rights of the participants were respected.
Acknowledgments
The present study was supported by the Zanjan University of Medical Sciences as a MSc thesis of the first author. We sincerely appreciate all the nurses and patients who participated in this study.
Author Contributions
Study design: Nasrin Hanifi and Fatemeh Mohammadi; data gathering: Fatemeh Mohammadi; statistical analysis and interpretation of the data: All authors; drafting of the manuscript: All authors; critical revision of the manuscript: All authors.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Pereira Lima Silva R, Gonçalves Menegueti M, Dias Castilho Siqueira L, de Araújo TR, Auxiliadora-Martins M, Mantovani Silva Andrade L, Laus AM. Omission of nursing care, professional practice environment and workload in intensive care units. Journal of Nursing Management. 2020;28(8):1986-96. [CrossRef]
- Lebet RM, Hasbani NR, Sisko MT, Agus MSD, Nadkarni VM, Wypij D, Curley MAQ. Nurses’ Perceptions of Workload Burden in Pediatric Critical Care. American Journal of Critical Care. 2021;30(1):27-35. [CrossRef]
- Chang LY, Yu HH, Chao YC. The Relationship Between Nursing Workload, Quality of Care, and Nursing Payment in Intensive Care Units. Journal of Nursing Research. 2019;27(1):1-9. [CrossRef]
- Alghamdi MG. Nursing workload: a concept analysis. Journal of Nursing Management. 2016;24(4):449-57. [CrossRef]
- Tubbs-Cooley HL, Mara CA, Carle AC, Mark BA, Pickler RH. Association of Nurse Workload With Missed Nursing Care in the Neonatal Intensive Care Unit. JAMA Pediatrics. 2019;173(1):44-51.
- Carvalho DPd, Rocha LP, Pinho ECd, Tomaschewski-Barlem JG, Barlem ELD, Goulart LS. Workloads and burnout of nursing workers. Revista brasileira de enfermagem. 2019;72(6):1435-41. [CrossRef]
- Pastores SM, Kvetan V, Coopersmith CM, Farmer JC, Sessler C, Christman JW, D’Agostino R, Diaz-Gomez J, Gregg SR, Khan RA, Kapu AN, Masur H, Mehta Gargi, Moore J, Oropello JM, Price K. Workforce, Workload, and Burnout Among Intensivists and Advanced Practice Providers: A Narrative Review. Critical Care Medicine. 2019;47(4):550-557. [CrossRef]
- Orique SB, Patty CM, Woods E. Missed Nursing Care and Unit-Level Nurse Workload in the Acute and Post-Acute Settings. Journal of Nursing Care Quality. 2016;31(1):84-9. [CrossRef]
- Chaboyer W, Harbeck E, Lee B-O, Grealish L. Missed nursing care: An overview of reviews. The Kaohsiung Journal of Medical Sciences. 2021;37(2):82-91. [CrossRef]
- Jones TL, Hamilton P, Murry N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. International journal of nursing studies. 2015;52(6):1121-37. [CrossRef]
- Juvé-Udina M-E, González-Samartino M, López-Jiménez MM, Planas-Canals M, Rodríguez-Fernández H, Batuecas Duelt IJ, Tapia-Pérez M, Pons Prats M, Jiménez-Martínez E, Barberà Llorca MÀ, Asensio-Flores S, Berbis-Morelló C, Zuriguel-Pérez E, Delgado-Hito P, Rey Luque Ó, Zabalegui A, Fabrellas N, Adamuz J. Acuity, nurse staffing and workforce, missed care and patient outcomes: A cluster-unit-level descriptive comparison. Journal of Nursing Management. 2020;28(8):2216-29. [CrossRef]
- Wieczorek-Wojcik B, Gaworska-Krzemińska A, Owczarek AJ, Kilańska D. In-hospital mortality as the side effect of missed care. Journal of Nursing Management. 2020;28(8):2240-6. [CrossRef]
- Janatolmakan M, Khatony A. Explaining the consequences of missed nursing care from the perspective of nurses: a qualitative descriptive study in Iran. BMC nursing. 2022;21(1):1-7.
- Bae S-H, Kim J, Lee I, Oh SJ, Shin S. Video Recording of Nursing Care Activities in Gerontological Nursing to Compare General Units and Comprehensive Nursing Care Units. Journal of Korean Gerontological Nursing. 2019;21(3):165-72. [CrossRef]
- Alizadeh M, Heidari Gorji MA, Khalilian AR, Esmaeili R. Assessment of nursing workload and related factors in intensive care units using the nursing activities score. Journal of Mazandaran University of Medical Sciences. 2015;24(122):147-57.
- Nieri A-S, Manousaki K, Kalafati M, Padilha KG, Stafseth SK, Katsoulas T, Matziou V, Giannakopoulou M. Validation of the nursing workload scoring systems “Nursing Activities Score” (NAS), and “Therapeutic Intervention Scoring System for Critically Ill Children” (TISS-C) in a Greek Paediatric Intensive Care Unit. Intensive and Critical Care Nursing. 2018;48:3-9. [CrossRef]
- Luiking ML, van Linge R, Bras L, Grypdonck M, Aarts L. Psychometric properties of the Dutch version of the American Nursing Activity Scale in an intensive care unit. Journal of advanced nursing. 2012;68(12):2750-5. [CrossRef]
- Beaton D, Bombardier C, Guillemin F, Ferraz MB. Recommendations for the cross-cultural adaptation of health status measures. New York: American Academy of Orthopaedic Surgeons. 2002;12:1-29.
- Kim KS, Kwon S-H, Kim J-A, Cho S. Nurses’ perceptions of medication errors and their contributing factors in South Korea. Journal of Nursing Management. 2011;19(3):346-53. [CrossRef]
- Taheri HabibAbadi E, Noorian M, Rassouli M, Kavousi A. Nurses' Perspectives on Factors Related to Medication Errors in Neonatal and Neonatal Intensive Care Units. Iran Journal of Nursing (2008-5923). 2013;25(80).
- Ball JE, Murrells T, Rafferty AM, Morrow E, Griffiths P. ‘Care left undone’ during nursing shifts: associations with workload and perceived quality of care. BMJ Quality & Safety. 2014;23(2):116. [CrossRef]
- Kim K-J, Yoo MS, Seo EJ. Exploring the Influence of Nursing Work Environment and Patient Safety Culture on Missed Nursing Care in Korea. Asian Nursing Research. 2018;12(2):121-6. [CrossRef]
- Joolaee S, Shali M, Hooshmand A, Rahimi S, Haghani H. The relationship between medication errors and nurses’ work environment. Medical-Surgical Nursing Journal. 2016;4(4):e68079.
- Kalisch BJ, Williams RA. Development and Psychometric Testing of a Tool to Measure Missed Nursing Care. JONA: The Journal of Nursing Administration. 2009;39(5):211-219. [CrossRef]
- Momennasab M, Karimi F, Dehghanrad F, Zarshenas L. Evaluation of Nursing Workload and Efficiency of Staff Allocation in a Trauma Intensive Care Unit. Trauma Monthly. 2018;23(1):1-5. [CrossRef]
- Bruyneel A, Tack J, Droguet M, Maes J, Wittebole X, Miranda DR, Pierdomenico LD, Measuring the nursing workload in intensive care with the Nursing Activities Score (NAS): A prospective study in 16 hospitals in Belgium. Journal of Critical Care. 2019;54:205-11. [CrossRef]
- Camuci MB, Martins JT, Cardeli AAM, Robazzi MLdCC. Nursing Activities Score: nursing workload in a burns Intensive Care Unit. Revista latino-americana de enfermagem. 2014;22(2):325-31. [CrossRef]
- Padilha KG SS, Solms D, Hoogendoom M, Monge FJC, Gomaa OH, Giakoumidakis K, Giannakopoulou M, Gallani MC, Cudak E, Nogueira LS, Santoro C, Sousa RC, Barbosa RL, Miranda DR. Nursing Activities Score: an updated guideline for its application in the Intensive Care Unit. Rev Esc Enferm USP 2015;49(spe):131-7. [CrossRef]
- Chegini Z, Jafari-Koshki T, Kheiri M, Behforoz A, Aliyari S, Mitra U, Islam SMS. Missed nursing care and related factors in Iranian hospitals: A cross-sectional survey. Journal of Nursing Management. 2020;28(8):2205-15. [CrossRef]
- Haftu M, Girmay A, Gebremeskel M, Aregawi G, Gebregziabher D, Robles C. Commonly missed nursing cares in the obstetrics and gynecologic wards of Tigray general hospitals; Northern Ethiopia. PLOS ONE. 2019;14(12):e0225814. [CrossRef]
- Ball JE, Griffiths P, Rafferty AM, Lindqvist R, Murrells T, Tishelman C. A cross-sectional study of ‘care left undone’ on nursing shifts in hospitals. Journal of advanced nursing. 2016;72(9):2086-97. [CrossRef]
- Tubbs-Cooley HL, Pickler RH, Younger JB, Mark BA. A descriptive study of nurse-reported missed care in neonatal intensive care units. Journal of advanced nursing. 2015;71(4):813-24. [CrossRef]
- Zang K, Chen B, Wang M, Chen D, Hui L, Guo S, Ji T, Shang F. The effect of early mobilization in critically ill patients: A meta-analysis. Nursing in Critical Care. 2020;25(6):360-7. [CrossRef]
- Biswas A, Bhattacharya SD, Singh AK, Saha M. Addressing Hand Hygiene Compliance in a Low-Resource Neonatal Intensive Care Unit: a Quality Improvement Project. Journal of the Pediatric Infectious Diseases Society. 2019;8(5):408-13. [CrossRef]
- Tubbs-Cooley HL, Pickler RH, Mark BA, Carle AC. A research protocol for testing relationships between nurse workload missed nursing care and neonatal outcomes: the neonatal nursing care quality study. Journal of advanced nursing. 2015;71(3):632-41. [CrossRef]
- Griffiths P, Recio-Saucedo A, Dall'Ora C, Briggs J, Maruotti A, Meredith P, Smith GB, Ball J. The association between nurse staffing and omissions in nursing care: A systematic review. Journal of advanced nursing. 2018;74(7):1474-87. [CrossRef]
- Ogboenyiya AA, Tubbs-Cooley HL, Miller E, Johnson K, Bakas T. Missed Nursing Care in Pediatric and Neonatal Care Settings: An Integrative Review. MCN: The American Journal of Maternal/Child Nursing. 2020;45(5). [CrossRef]
- Tajabadi A, Ahmadi F, Sadooghi Asl A, Vaismoradi M. Unsafe nursing documentation: A qualitative content analysis. Nursing Ethics. 2019;27(5):1213-24. [CrossRef]
- De Marinis MG, Piredda M, Pascarella MC, Vincenzi B, Spiga F, Tartaglini D, Alvaro R, Matarese M. ‘If it is not recorded, it has not been done!’? consistency between nursing records and observed nursing care in an Italian hospital. Journal of Clinical Nursing. 2010;19(11-12):1544-52. [CrossRef]
- Mirzaei S, Noorihekmat S, Oroomiei N, Vali L. Administrative challenges of clinical governance in military and university hospitals of Kerman/Iran. The International Journal of Health Planning and Management. 2019;34(2):e1293-e301. [CrossRef]
- Hessels AJ, Paliwal M, Weaver SH, Siddiqui D, Wurmser TA. Impact of Patient Safety Culture on Missed Nursing Care and Adverse Patient Events. Journal of Nursing Care Quality. 2019;34(4):287-94. [CrossRef]
- Reis CT, Paiva SG, Sousa P. The patient safety culture: a systematic review by characteristics of Hospital Survey on Patient Safety Culture dimensions. International Journal for Quality in Health Care. 2018;30(9):660-77. [CrossRef]
- Phelan A, McCarthy S, Adams E. Examining missed care in community nursing: A cross-section survey design. Journal of advanced nursing. 2018;74(3):626-36. [CrossRef]
- Lake ET, French R, O'Rourke K, Sanders J, Srinivas SK. Linking the work environment to missed nursing care in labour and delivery. Journal of Nursing Management. 2020;28(8):1901-8. [CrossRef]
- Smith JG, Morin KH, Wallace LE, Lake ET. Association of the Nurse Work Environment, Collective Efficacy, and Missed Care. Western Journal of Nursing Research. 2017;40(6):779-98. [CrossRef]
- Song Y, Hoben M, Norton P, Estabrooks CA. Association of Work Environment With Missed and Rushed Care Tasks Among Care Aides in Nursing Homes. JAMA Network Open. 2020;3(1):e1920092-e. [CrossRef]
Figure 1.
Flow diagram showing the study design and sampling.
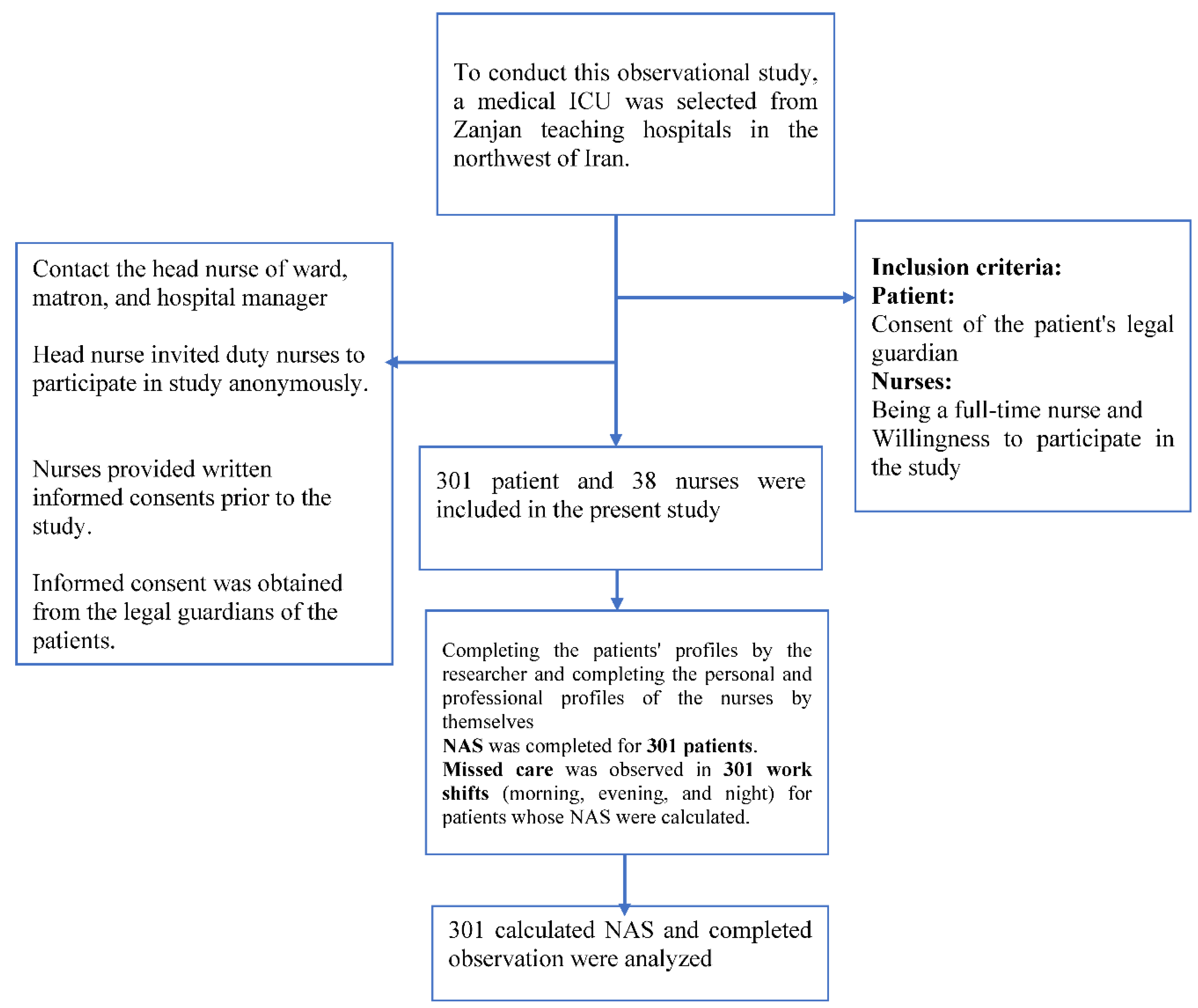

Table 1.
Personal and professional profile of the nurses participating in the study (N =38).
| Variable | N (%) | Variable | N (%) |
|---|---|---|---|
| Gender | Employment status | ||
| Female | 31 (81.58) | Casual employees | 24 (68.16) |
| Male | 7 (18.42) | Fixed employment contracts | 5 (13.16) |
| Age (years) | Permanent full-time employment | 9 (23.98) | |
| 22-30 | 25 (65.78) | Work experiences (years) | |
| 31-40 | 13 (34.21) | 6 month-2 years | 10 (26.32) |
| Marital status | 3 years-5 years | 19 (50) | |
| Single | 8 (21.05) | 6 years- 10 years | 7 (18.42) |
| Married | 30 (78.95) | 11 years-15 years | 2 (5.26) |
| Educational level | Number of working hours/months | ||
| Bachelor’s degree | 35 (92.11) | >200 hours | 2 (5.3) |
| Master’s degree | 3 (7.89) | 208-240 hours | 20 (52.6) |
| Nurse-to-patient ratio | < 240 hours | 16 (42.1) | |
| 1:1 | 4 (10.5) | working hours / months | |
| 1:2 | 27 (71.1) | 200 hours/month | 2 (5.3) |
| 1:3 | 7 (18.4) | 200-240 hours/month | 20 (52.6) |
| >240 hours/month | 16 (42.1) |
Table 2.
Frequency and percentage of missed care in each care (N=301 observe)
| Missed cares | Not applicable N (%) |
Not done N (%) |
Done incompletely N (%) |
Don completely N (%) |
| Assessment | ||||
| Patient Identification with patient bracelet during shift delivery | 13 (4.3) | 288 (95.7) | ||
| Attention to ventilator settings at the beginning of the shift | 140 (46.5) | 149 (49.5) | 12 (4.0) | |
| Assessment and recording the patient’s mental state (delirium, depression and anxiety) | 120 (39.9) | 107 (35.5) | 64 (21.3) | 10 (3.3) |
| Control vital signs and record them in time according to the order | 25 (8.3) | 8 (2.7) | 167 (55.5) | 101 (33.6) |
| Report abnormal vital signs immediately after being notified | 282 (93.7) | 9 (3.0) | 6 (2.0) | 4 (1.3) |
| Assessment and evaluation and re-recording if the patient’s condition changes | 292 (97.0) | 7 (2.3) | 1 (.3) | 1 (.3) |
| Control and record blood sugar according to the order | 159 (52.8) | 92 (30.6) | 12 (4.0) | 38 (12.6) |
| Taking appropriate treatment in case of abnormal blood sugar within 15 minutes | 300 (99.7) | 1 (.3) | ||
| Checking the correct location of the endotracheal tube and measuring endotracheal tube cuff pressure at least once per shift | 208 (69.1) | 78 (25.9) | 4 (1.3) | 11 (3.7) |
| Skin and vascular assessment of the upper and lower limbs at the place of restriction | 142 (47.2) | 149 (49.5) | 3 (1.0) | 7 (2.3) |
| Assessment and recording of SPO 2 of the patient | 67 (22.3) | 104 (34.6) | 21 (7.0) | 109 (36.2) |
| Treatment for abnormal SPO2 within 5 minutes | 236 (78.4) | 7 (2.3) | 56 (18.6) | 2 (.7) |
| Assessment the need for suction and performing it on time | 108 (35.9) | 123 (40.9) | 59 (19.6) | 11 (3.7) |
| Recording of endotracheal tube secretions volume and its characteristics | 217 (72.1) | 1 (.3) | 1 (.3) | 82 (27.2) |
| Checking and recording the content characteristics of the bag connected to the nasogastric tube | 291 (96.7) | 5 (1.7) | 5 (1.7) | |
| Reporting the abnormal content of nasogastric tube secretions | 293 (97.3) | 6 (2.0) | 2 (.7) | |
| Measuring the volume and color of urine and recording it | 1 (.3) | 1 (.3) | 2 (19) | 280 (93) |
| Reporting the abnormal the volume and color of urine | 281 (93.4) | 16 (5.3) | 1 (.3) | 3 (1.0) |
| Assessment and recording the volume and color of chest tube discharges | 292 (97.0) | 3 (1.0) | 6 (2.0) | |
| Reporting abnormal the volume and color of chest tube discharges | 296b (98.3) | 1 (.3) | 4 (1.3) | |
| Assessment and recording the status of any kind of drain or wound | 290 (96.3) | 1 (.3) | 4 (1.3) | |
| Reporting the abnormal discharge of any type of drain or wound | 294 (97.7) | 5 (1.7) | 1 (.3) | 1 (.3) |
| Mobility and motion | ||||
| Change position every 2 hours | 300 (99.7) | 1 (.3) | ||
| Moving and walking the patient according to the order | 296 (98.3) | 5 (1.7) | ||
| Applying deep vein thrombosis (DVT) prevention: intermittent bandaging or Intermittent pneumatic compression (IPC) | 137 (45.5) | 162 (53.8) | 2 (.7) | |
| Using proper protection and restraint (bed side rail and bed harness) | 31 (10.3) | 21 (7.0) | 140 (46.5) | 109 (36.2) |
| Response to patient’s needs and devices alarmwithin 5 min | ||||
| Response to the rational request of the patient (defecation, thirst, hunger, movement, etc.) within 5 minutes of the request | 266 (88.4) | 1 (.3) | 29 (9.6) | 5 (1.7) |
| Responding to device alarms within 1 to 5 minutes of its start | 23 (7.6) | 43 (14.3) | 144 (47.8) | 91 (30.2) |
| Patient education | ||||
| Explaining and education to the conscious patient before performing the procedures |
237 (78.7) | 7 (2.3) | 7 (2.3) | 50 (16.6) |
| Explaining and education to the conscious patient after the procedures | 244 (81.1) | 7 (2.3) | 5 (1.7) | 45 (15.0) |
| Hand hygiene | ||||
| Hand hygiene before touching a patient | 100 (33.2) | 201 (66.8) | ||
| Hand hygiene before performing care procedures | 103 (34.2) | 198 (65.8) | ||
| Hand hygiene after performing care procedures | 6 (2.0) | 291 (96.7) | 4 (1.3) | |
| Hand hygiene after body fluid exposures risk | 2 (.7) | 5 (1.7) | 294 (97.7) | |
| Hand hygiene after touching a patient | 1 (.3) | 12 (4.0) | 288 (95.7) | |
| Infection control | ||||
| Eye care based according to hospital policy | 253 (84.1) | 35 (11.6) | 11 (3.7) | 2 (.7) |
| Skin care on ward according to hospital policy | 228 (75.7) | 42 (14.0) | 14 (4.7) | 17 (5.6) |
| Mouthwash based on the needs of the patient in each shift | 241 (80.1) | 34 (11.3) | 13 (4.3) | 13 (4.3) |
| Perineal Care: Washing the perineum based on the ward’s routine | 253 (84.1) | 18 (6.0) | 13 (4.3) | 17 (5.6) |
| Caring for any type of wound on the body (rinsing the wound if necessary and dressing) | 277 (92.0) | 8 (2.7) | 9 (3.0) | 7 (2.3) |
| Central venous catheter dressing | 281 (93.4) | 5 (1.7) | 15 (5.0) | |
| Replacement of venous line within half an hour of phlebitis | 294 (97.7) | 1 (.3) | 2 (.7) | 4 (1.3) |
| Prevention of contact of drains, bags and connections of the patient with the ground | 22 (7.3) | 1 (.3) | 1 (.3) | 277 (92.0) |
| Change the direction of the endotracheal tube to prevent ischemia at least once per shift | 196 (65.1) | 104 (34.6) | 1 (.3) | |
| change of disposable devices according to hospital policy (micro set, serum, serum set, central venous pressure monitor equipment, infusion syringe, extension tube, Foley catheter, nasogastric tube, feeding set, gavage syringe, closed suction, etc.) | 200 (66.4) | 6 (2.0) | 95 (31.6) | |
| Oxygen Therapy | ||||
| Resetting the new ventilator items according to the order within 10 minutes | 301 (100) | |||
| Appropriately providing oxygenation according to the order | 48 (15.6) | 10 (3.3) | 10 (3.3) | 233 (77.4) |
| Implementation of urgency order | ||||
| Execution of STAT medication orders within 15 minutes after the order | 170 (56.5) | 5 (1.7) | 126 (41.9) | |
| Sending emergency samples within 15 minutes after the order | 170 (56.5) | 5 (1.7) | 126 (41.9) | |
| The nutritional care | ||||
| Feeding the patient within 15 minutes after food distribution | 137 (45.5) | 3 (1.0) | 68 (22.6) | 93 (30.9) |
| Measuring gastric residual volume | 193 (64.1) | 85 (28.2) | 6 (2.0) | 17 (5.6) |
| Adjusting the feed pump | It was not evaluated due to the absence of nutritional bag in the ward during the study. | |||
| Filling the bag connected to the feeding pump within 15 minutes after its completion | ||||
| Observing the semi-sitting position during feeding | 134 (44.5) | 2 (.7) | 33 (11.0) | 132 (43.9) |
Table 3.
The compare of NAS means based on levels of missed care dimensions (N: 301 observe).
| Not applicable N (%) |
Very high N (%) |
High N (%) |
Moderate N (%) |
Low N (%) |
Mean (95% CI) (1-10 score) |
|
|---|---|---|---|---|---|---|
| Assessment | - | - | 5 (1.7) | 209 (69.4) | 87 (28.9) | 70.32 (69.05, 71.54) |
| Mobility and motion | 14 (4.7) | 5 (1.7) | 91 (30.2) | 163 (54.2) | 28 (9.3) | 58.88 (56.44, 61.26) |
| Response to patient’s needs and call lightwithin 5 min | 1 (.3) | - | 45 (15) | 159 (52.8) | 96 (31.9) | 71.93 (69.43, 74.47) |
| Patient education | 234 (77.7) | - | 8 (2.7) | 9 (3.0) | 50 (16.6) | 19.49 (34.46, 41.27) |
| Hand hygiene | - | - | 6 (2.0) | 293 (97.3) | 2 (.7) | 68.37 (67.55, 69.15) |
| Infection control | - | - | 20 (6.6) | 105 (34.9) | 176 (58.5) | 80.90 (78.75, 82.92) |
| Oxygen Therapy | 48 (15.9) | - | 10 (3.3) | 10 (3.3) | 233 (77.4) | 80.73 (76.52,84.93) |
| Implementation of urgency order | 178 (59.1) | - | - | 5 (1.7) | 118 (39.2) | 40. 31 (34.77,45.95) |
| The nutritional care | 139 (46.2) | - | 1 (.3) | 64 (21.3) | 97 (32.2) | 42.84 (38.13, 47.80) |
| Total of missed care score | - | - | 114 (37.9) | 184 (61.1) | 3 (1) | 59.31 (58.32, 60.43) |
SD=Standard deviation
Table 4.
The means and standard deviation of nursing activity score according to levels of missed care dimensions.
Table 4.
The means and standard deviation of nursing activity score according to levels of missed care dimensions.
| Variable | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | ANOVA | ||
|---|---|---|---|---|---|---|---|---|
| Very high | High | Moderate | Low | Not applicable | df | F | p | |
| Assessment | 67.26 (61.26, 74.37) | 77.70 (75.80,79.42) | 73.49 (70.99,76.63) | 2 | 3.90 | .021 | ||
| Mobility and motion | 75.64 (70.44,80.71) | 73.56 (69.16, 77.96) | 74.46 (71.62, 77.55) | 77.47 (75.23,79.48) | 76.43 (71.77, 80.98) | 4 | .73 | .573 |
| Response to patient’s needs and call lightwithin 5 min | 78.05 (74.34, 82.13) | 74.61 (72.49, 76.86) | 78.31 (75.55,81.03) | 75.40 (75.4, 75.4) | 3 | 1.67 | .174 | |
| Patient education | 82.66 (73.25, 92.73) | 78.33 (65.21,90.23) | 73.62 (70.06,76.96) | 76.59 (74.77, 78.37) | 3 | 1.26 | .289 | |
| Hand hygiene | 82.40 (69.32, 95.73) | 76.02 (74.44,77.48) | 100 (100, 100) | 2 | 3.70 | .026 | ||
| Infection control | 78.55 (71.18, 86.82) | 78.74 (75.98,81.48) | 74.60 (72.80, 76.41) | 2 | 3.19 | .043 | ||
| Oxygen Therapy | 74.07 (64.02, 83.54) | 80.24 (70.98, 90.80) | 76.31 (74.66, 78.14) | 75.96 (72.15,79.67) | 3 | .36 | .79 | |
| Implementation of urgency order | 83.10 (73.46,91.68) | 77.46 (74.72, 80.00) | 75.36 (73.34, 77.23) | 2 | 1.40 | .249 | ||
| The nutritional care | 106.70 (106.70, 106.70) | 75.11 (71.59, 78.39) | 75.45 (72.40, 78.40) | 77.25 (75.10, 79.43) | 3 | 2.08 | .104 | |
| Total of missed care score | 76.24 (73.04, 79.49) | 76.31 (74.52,78.25) | 76.52 (69.05, 83.61) | 2 | .002 | .998 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



