
Submitted:
03 October 2023
Posted:
04 October 2023
You are already at the latest version
Abstract
Estrogens play a protective role during early life stages. However, endogenous 17β-estradiol (E2) can accelerate atherosclerosis progression in low-grade inflammatory conditions like established atherosclerosis. Our single-center cohort study assessed sex-specific associations of gonadal hormones with oxidative stress, inflammation, and myocardial injury markers in 111 patients (37% women) diagnosed with acute myocardial infarction (MI) between July 2011 and December 2013. Blood samples were collected within 48 hours of symptom onset, and we measured sex steroids (E2, total testosterone [T]), oxidized low-density lipoproteins, high-sensitive C-reactive protein (CRP), white blood cell counts (WBC), and cardiac enzymes (creatine kinase [CK], the CK Muscle-Brain fraction [CK-MB], and high-sensitive troponin T [hsTnT]). The SYNTAX score gauged coronary disease severity from coronary angiography results. In men with acute MI, peak cardiac enzyme levels were predicted by post-percutaneous coronary intervention (PCI) E2 plasma levels (OR 1.011, p=0.047 - CK; OR 1.018, p=0.013 - CK- MB; OR 1.019, p=0.005 - TnT), peak WBC count (OR 1.487, p=0.015 - CK ; OR 1,709, p=0,005 - CK- MB; OR 1.391, p=0.012 - TnT), and peak CRP plasma levels (OR 1.040, p=0.033 - CK; OR 1.024, p=0.029 - CK-MB; OR 1.063, p=0.006 - TnT). T levels and E2/T ratio were associated with post-PCI CRP in these men (OR 0.980, p = 0.024 - T, OR 1.010, p = 0.076 - CRP). For women, peak WBC was a marker of highest testosterone (OR 1.348, p = 0.062), and only WBC was a significant indicator of myocardial injury extent (OR 1.426, p=0.039 - CK; OR 1.384, p=0.036 - CK-MB; OR 1.299, p=0.048 - TnT). During acute MI, elevated endogenous estradiol levels correlate with myocardial necrosis severity in men, while in women, increased leukocyte levels indicate acute myocardial damage. Elevated plasma T is associated with increased WBC in women. In men, post-PCI plasma CRP specifically indicates endogenous T levels and E2/T ratio during the acute phase.
Keywords:
17β-estradiol
; total testosterone
; oxidized low-density lipoproteins
; high-sensitive C-reactive protein
; Acute Myocardial Infarction
1. Introduction
Early menopause has long been recognized as a risk factor for cardiovascular disease [1]. Researchers have found links between irregular menstrual cycles and an increased risk of acute myocardial infarction (AMI) [2]. Furthermore, women with polycystic ovary syndrome, characterized by hyperandrogenemia, are more prone to premature and extensive coronary artery disease [3]. Low plasma concentrations of endogenous 17β-estradiol in early life correlate with an atherogenic lipid profile and endothelial dysfunction in men [4,5,6]. In contrast, in cohorts with established cardiovascular disease, high serum estradiol levels in both men and women [7] and low serum testosterone and its precursors in men [7,8] predict the severity of coronary atherosclerosis. In postmenopausal women, high testosterone levels correlate with the degree of coronary artery disease (CAD) [9] and an increased risk of death [10]. An allele variant of the aromatase enzyme converts testosterone to estradiol in various tissues and is a risk indicator for mortality in men with acute coronary syndrome [11]. The ratio of endogenous estradiol to testosterone (E2/T)—also known as the aromatase index—indicates an adverse prognosis in older women with known cardiovascular disease [12].
The concentrations of endogenous gonadal steroids change during the acute phase of myocardial infarction (MI). Testosterone levels drop within the first 24 hours, whereas estradiol levels rise until the end of the second week post-MI [13,14,15]. The activity of the aromatase enzyme varies throughout life, especially during acute illnesses, leading to increased endogenous estradiol concentrations [16,17]. The clinical implications of these fluctuations in endogenous sex hormone concentrations and aromatase activity in acute coronary disease remain uncertain.
Previous studies suggest that men with low serum testosterone levels undergoing primary percutaneous coronary intervention (PCI) for MI with ST elevation experience inferior myocardial reperfusion and myocardial systolic function [18]. Conversely, elevated endogenous estradiol levels independently correlate with the risk of no-reflow in postmenopausal women [19].
Animal research indicates that bilateral ovariectomy increases ischemia-reperfusion (MI/R) injury of the myocardium. Estrogen treatment can mitigate this by inhibiting endoplasmic reticulum stress, reducing cardiomyocyte apoptosis, and lessening MI/R injury, resulting in smaller infarcts in ovariectomized female mice than untreated ones [20,21]. However, these animal models do not adequately represent the extent of atherosclerosis in older humans, limiting their relevance.
Purpose
This single-center cohort study aimed to assess the significant associations of gonadal hormones and the aromatase index with oxidative stress, inflammation, and myocardial damage extent in postmenopausal women and adult men with AMI.
2. Materials and Methods
We included 111 patients (37% women) diagnosed with AMI admitted to the Clinic of Cardiology, University Hospital “Alexandrovska,” Sofia, between July 2011 and December 2013. Blood samples were drawn 48 hours after symptom onset to measure levels of sex steroids (total 17β-estradiol [E2], total testosterone [T], dehydroepiandrosterone-sulfate), oxidized low-density lipoproteins (oxLDL), high-sensitive C-reactive protein (hsCRP), white blood cell counts (WBC), and cardiac enzymes (creatine kinase [CK], Muscle-Brain fraction of CK [CPK-MB], and high-sensitive troponin T [hsTnT]). To measure coronary disease severity, we calculated the SYNTAX score for each patient with angiographically-defined coronary atherosclerosis.
Patients diagnosed with secondary hypogonadism or diseases of the adrenal and pituitary glands were excluded. Other exclusion criteria included acute infectious disease, chronic inflammatory disease, known or suspected neoplastic processes, surgical procedures, and trauma within two weeks before hospital admission. Participants had not used hormone or immunoreactive therapies six months before or during the study.
We adhered to the Declaration of Helsinki and received approval from the ethics committee of the Medical University of Sofia. All participants provided written informed consent.
After a 12-hour fast, venous blood samples were collected into EDTA sample tubes, centrifuged at 12,000 rpm for 20 minutes, and stored at -20°C until analysis.
hsCRP concentrations were determined using a latex-enhanced immunoturbidimetric assay (Roche Diagnostics GmbH, Manheim, Germany) on the COBAS INTEGRA 700 analyzer. We assessed levels of steroid hormones and hsTNT using an electrochemiluminescent immunoassay with Roche Diagnostics reagents on the Elecsys 2010 analyzer. These methods have been detailed elsewhere [22,23]. Plasma levels of oxLDL were quantified using the OxiSelect Human Oxidized LDL immunosorbent assay (ELISA; MDA-LDL) kit (Cell Biolabs, San Diego, USA) and a sandwich ELISA [24].
Statistical Analysis
We checked variable distributions using the Kolmogorov-Smirnov and Sapiro-Wilk tests. We explored associations between variables using both parametric (independent samples t-test) and non-parametric (χ2 test, Fisher’s exact tests, Mann-Whitney U test) methods, further validated by univariate and multivariable analyses. Analyses were conducted using IBM SPSS Statistics for Windows, Version 19.0. (Armonk, NY: IBM Corp.). A two-tailed p-value less than 0.05 was deemed significant.
3. Results
Female patients were, on average, older than male patients (Table 1). In female patients, C-reactive protein (CRP) and cardiac enzyme levels were lower. During the acute phase of MI, E2 levels were higher in male patients, while the E2 to T ratio (E2/T) was lower in female patients (Table 1).
In male patients, post-PCI E2, CRP, and WBC counts were predictors of peak cardiac enzyme levels, as determined by univariable regression analysis. For female patients, peak WBC count was a significant indicator of myocardial injury (Table 2, Table 3 and Table 4).
For male patients, high plasma concentrations of E2 and CRP were significant markers for an increase in Troponin T (TnT) levels (OR 1.019, 95% CI 1.003-1.036, p=0.021 for E2; OR 1.052, 95% CI 1.009-1.095, p=0.016 for CRP). However, WBC count was not a significant marker (p=0.158). Peak WBC count was notably associated with the highest activities of both CK and CK-MB in a stepwise multiple regression model (CK: OR 1.487, 95% CI 1.081-2.045, p=0.015 for WBC; CK-MB: OR 1.709, 95% CI 1.174-2.488, p=0.005 for WBC).
An analysis of the correlations between gonadal steroid hormones and the E2/T ratio during the acute phase of MI revealed that in male patients, a high CRP level was inversely associated with total T plasma levels (OR 0.980, 95% CI 0.963-0.997, p=0.024). Additionally, a trend suggested that high CRP levels were associated with a higher E2/T ratio (OR 1.010, 95% CI 0.999-1.022, p=0.079). Among female patients with AMI, peak WBC count showed a trend toward marking the highest T levels (OR 1.348, 95% CI 0.985-1.846, p=0.062).
4. Discussion
During the acute phase of MI, male patients showed a significant relationship between the highest levels of endogenous estradiol and CRP and the severity of cardiomyocyte necrosis (as evidenced by peak plasma TnT levels). Conversely, the peak WBC count emerged as a sex-specific marker for acute myocardial damage in women. Interestingly, the peak plasma T in women correlated with the rise in WBC, while in men with AMI, T was related to the increase in CRP levels. Furthermore, a positive association was observed between CRP and the E2/T ratio in male patients.
4.1. Sex-Specific Relationship of oxLDL and CRP with E2 and E2/T
oxLDL may influence endogenous estradiol and testosterone production in both men and women [25,26]. During critical illnesses, a surge in aromatase activity in adipose tissue leads to a notable increase in the conversion of testosterone to estradiol, which is believed to be a response to elevated production of pro-inflammatory cytokines [27]. Under nonacute conditions, excess adipose tissue exhibits enhanced immune cell infiltration, predominantly macrophages, and increased aromatase expression, leading to elevated androgen breakdown and endogenous estradiol levels [28,29,30]. Notably, pro-inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α), induce the expression of the human aromatase gene in mammary adipose tissue [31]. Aromatase levels were higher in inflamed versus noninflamed areas of breast tissue in postmenopausal women [32]. Additionally, obesity might induce the production of chemokine ligand 2 (a receptor for MCP-1) in the adipose tissue of postmenopausal women, thereby instigating inflammation and stimulating local aromatase, amplifying estrogen levels [33]. E2 can increase estradiol concentrations by triggering the aromatase gene transcription through estrogen receptor-β [34]. A significant relationship between certain cytokines (IL-6) and E2 has been documented in male patients with metabolic syndrome [35].
Our analysis revealed that body mass index (BMI) did not significantly correlate with the levels of gonadal steroid hormones, aromatase index, or inflammatory markers. However, other studies have emphasized the stronger relationship between abdominal adipose tissue thickness (rather than BMI) and the levels of inflammatory mediators and sex hormones [36]. Inflammatory pathways are activated soon after high-fat diet consumption leading to inflammatory macrophage accumulation in white adipose tissue even before overt obesity manifests [37].
Our findings indicated that in female patients with AMI, markers of myocardial injury did not directly correlate with endogenous estradiol and testosterone levels. Still, the peak WBC count was significantly associated with T levels and myocardial injury severity. This observation aligns with findings from studies on chronic CAD in women [38]. In contrast, our results show that for male AMI patients, inflammatory mediators, and E2 correlated with both aromatase activity and infarct size but endogenous testosterone levels did not emerge as a significant marker of myocardial injury. Many observational studies have highlighted variable in respect to significance associations of gonadal steroid hormones with markers of ongoing low-grade vascular inflammation in atherosclerosis in male patients with chronic coronary disease [7,39,40].
Many preclinical studies have confirmed the roles of inflammation and elevated E2 in acute coronary disease. In the absence of inflammatory stimuli, estrogens protect the initial stages of atherosclerosis in both sexes. However, in conditions such as established atherosclerosis, which can be considered a low-grade inflammatory state, E2 can destabilize atherosclerotic plaques by inducing molecules like MCP-1, matrix metalloproteinases (specifically MMP-2 and MMP-9), and TNF-α [41,42,43,44]. When atherosclerotic lesions are present, the altered expression of estrogen receptors on the vascular wall further exacerbates arterial wall damage [41,45].
Several human studies have reported fluctuations in E2 and testosterone levels during acute coronary events [13,14]. Persistently elevated E2 and declining testosterone have been associated with changes in hemostatic factors (notably increased plasminogen activator inhibitor-1, PAI-1) in men with AMI [13]. Elevated cardiac PAI-1 post-myocardial infarction may contribute to tissue remodeling and augmented cardiac fibrosis [46]. It leads to a prothrombotic profile in male AMI patients, increasing the risk of extended myocardial necrosis due to in-situ microthromboses.
4.2. Relationship of WBC with TnT in Female Patients
In female patients, a higher WBC count indicates an underlying inflammatory state associated with obesity, hyperandrogenemia, and polycystic ovary syndrome (PCOS) [38]. Moreover, testosterone has been linked directly to increased platelet thromboxane A receptor density and maximal platelet aggregation [47]. In particular conditions, in which tissue factor biological action is crucial, such as acute myocardial infarction neutrophils count increases substantially [48]. Endothelial cells, platelets, neutrophils express the tissue factor [48]. Inflammatory molecules, such as P-selectin and TNF-α share the ability to induce tissue factor messenger ribonucleic acid, as well as the ex-novo synthesis and up-regulation of tissue factor on the neutrophil surface [48]. A testosterone-rich environment may intensify platelet-leukocyte interactions, potentially leading to increased fibrin deposition and extensive coronary thrombus formation which could be a potential source of distal embolization. Testosterone associations with thrombin generation parameters (like fibrinogen, factor VIIc, PAI-1) and peak thrombin concentration have been documented in young women with PCOS [49] and middle-aged women [50].
4.3. Lack of overt Relationship of E2 and E2/T with Myocardial Injury in Women with AMI
Interestingly, only E2 emerged as a predictor of myocardial injury in men. In contrast, for female AMI patients, troponin levels were associated with higher WBC counts as markers of myocardial injury. Notably, the plasma concentration of estradiol and its production rate is significantly higher in men than in age-matched postmenopausal women, with approximately 20% of circulating E2 being secreted by the testis [51]. Most E2 production in men arises from the extragonadal aromatization of adrenal androgens and testosterone in muscle and adipose tissues. The rate of testosterone conversion to estradiol is lower than that of androstenedione aromatization to estrone [52]. Elevated testosterone levels [39] and increased adrenal androgens might explain the higher E2 concentration in older men versus postmenopausal women, suggesting its potential significance as a male-specific marker of myocardial injury in small AMI cohorts. In our study, the severity of myocardial damage and inflammatory response was greater in male AMI patients than in females, likely due to the more extensive coronary atherosclerosis. Hence, our study's E2/T ratio correlated with peak CRP levels only in the male cohort.
Author Contributions
Conceptualization, N.S. and A.T.; methodology, M.G., V.L., V.L., A.T., J.H., S.D., P.A.,M.C.; software, N.S.; validation, V.L., Y.Y. and V.L.; formal analysis, N.S.; investigation, N.S., M.G., V.L., V.L., A.T., J. H., S.D., P.A.,M.C.; resources, N.S.; data curation, N.S.; writing—original draft preparation, N.S.; writing—review and editing, N.S., M.G., V.L., V.L., A.T., J. H., S.D., P.A.,M.C. ; visualization, N.S.; supervision, M.G., V.L., V.L., A.T., J.H., S.D., P.A.,M.C.; project administration, M.G.; funding acquisition, N.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Medical University, Sofia grant number 5D/2013.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Medical University, Sofia (protocol code 262/May 7, 2013).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
This research data is available to the corresponding author and details regarding data supporting reported results can be send to editors and reviews upon request.
Acknowledgments
N.S. wants to thank to Z.Radulova, M. Radulov, N.Enchev, P.Emilov for their contribution for validation of the results of study. We thank to Servier Medical Bulgaria for the financial support for providing a reagent for the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Atsma, F.; Bartelink, M.-L.E.L.; Grobbee, D.E.; van der Schouw, Y.T. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: a meta-analysis. Menopause 2006, 13, 265–279. [CrossRef]
- Bertuccio, P.; Tavani, A.; Gallus, S.; Negri, E.; La Vecchia, C. Menstrual and reproductive factors and risk of non-fatal acute myocardial infarction in Italy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 134, 67–72. [CrossRef]
- Birdsall, M.A. Association between Polycystic Ovaries and Extent of Coronary Artery Disease in Women Having Cardiac Catheterization. Ann. Intern. Med. 1997, 126, 32–5. [CrossRef]
- Rochira, V.; Carani, C. Aromatase deficiency in men: a clinical perspective. Nat. Rev. Endocrinol. 2009, 5, 559–568. [CrossRef]
- Tomaszewski, M.; Charchar, F.J.; Maric, C.; Kuzniewicz, R.; Gola, M.; Grzeszczak, W.; Samani, N.J.; Zukowska-Szczechowska, E. Association between lipid profile and circulating concentrations of estrogens in young men. Atherosclerosis 2009, 203, 257–262. [CrossRef]
- Lew, R.; Komesaroff, P.; Williams, M.; Dawood, T.; Sudhir, K. Endogenous Estrogens Influence Endothelial Function in Young Men. Circ. Res. 2003, 93, 1127–1133. [CrossRef]
- Naessen, T.; Sjogren, U.; Bergquist, J.; Larsson, M.; Lind, L.; Kushnir, M.M. Endogenous Steroids Measured by High-Specificity Liquid Chromatography-Tandem Mass Spectrometry and Prevalent Cardiovascular Disease in 70-Year-Old Men and Women. J. Clin. Endocrinol. Metab. 2010, 95, 1889–1897. [CrossRef]
- Wranicz, J.K.; Cygankiewicz, I.; Kula, P.; Walczak-Jedrzejowska, R.; Slowikowska-Hilczer, J.; Kula, K. Endogenous Estradiol and Testosterone may Predispose toward Atherogenic Lipid Profile, but Higher Blood Level of Testosterone is Associated with Lower Number of Stenoses in the Coronary Arteries of Men with Coronary Disease. 2006, 2, 135–142.
- Phillips, G.B.; Pinkernell, B.H.; Jing, T.-Y. Relationship Between Serum Sex Hormones and Coronary Artery Disease in Postmenopausal Women. Arter. Thromb. Vasc. Biol. 1997, 17, 695–701. [CrossRef]
- Benn, M.; Voss, S.S.; Holmegard, H.N.; Jensen, G.B.; Tybjærg-Hansen, A.; Nordestgaard, B.G. Extreme Concentrations of Endogenous Sex Hormones, Ischemic Heart Disease, and Death in Women. Arter. Thromb. Vasc. Biol. 2015, 35, 471–477. [CrossRef]
- Beitelshees, A.L.; Johnson, J.A.; Hames, M.L.; Gong, Y.; Cooper-DeHoff, R.M.; Wu, J.; Cresci, S.; Ma, C.X.; Pepine, C.J.; Province, M.A.; et al. Aromatase Gene Polymorphisms Are Associated with Survival among Patients with Cardiovascular Disease in a Sex-Specific Manner. PLOS ONE 2010, 5, e15180. [CrossRef]
- Laughlin, G.A.; Ix, J.H.; Cummins, K.; Allison, M.A.; Daniels, L.B. Extremes of an aromatase index predict increased 25-year risk of cardiovascular mortality in older women.. Clin. Endocrinol. 2011, 77, 391–8. [CrossRef]
- Pugh, P.J.; Channer, K.S.; Parry, H.; Downes, T.; Jones, T.H. Bio-Available testosterone levels fall acutely following myocardial infarction in men: association with fibrinolotic factors. Endocr. Res. 2002, 28, 161–173.
- Tripathi, Y.; Hegde, B.M. Serum estradiol and testosterone levels following acute myocardial infarction in men.. 1998, 42, 291–4.
- Luria, M.H.; Johnson, M.W.; Pego, R.; Seuc, C.A.; Manubens, S.J.; Wieland, M.R.; Wieland, R.G. Relationship between sex hormones, myocardial infarction, and occlusive coronary disease. Arch. Intern. Med. 1982, 142, 42–44.
- Simpson, E.R.; Zhao, Y.; Agarwal, V.R.; Michael, M.D.; E Bulun, S.; Hinshelwood, M.M.; Graham-Lorence, S.; Sun, T.; Fisher, C.R.; Qin, K.; et al. Aromatase expression in health and disease.. 1997, 52, 185.
- Kumar, R.G.; DiSanto, D.; Awan, N.; Vaughan, L.E.; Levochkina, M.S.; Weppner, J.L.; Wright, D.W.; Berga, S.L.; Conley, Y.P.; Brooks, M.M.; et al. Temporal Acute Serum Estradiol and Tumor Necrosis Factor-α Associations and Risk of Death after Severe Traumatic Brain Injury. J. Neurotrauma 2020, 37, 2198–2210. [CrossRef]
- Separham, A.; Ghaffari, S.; Sohrabi, B.; Aslanabadi, N.; Bavil, M.H.; Lotfollahi, H. Association of admission testosterone level with ST-segment resolution in male patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Basic Clin. Androl. 2017, 27, 1–9. [CrossRef]
- Dong, M.; Mu, N.; Ren, F.; Sun, X.; Li, F.; Zhang, C.; Yang, J. Prospective Study of Effects of Endogenous Estrogens on Myocardial No-Reflow Risk in Postmenopausal Women with Acute Myocardial Infarction. J. Interv. Cardiol. 2014, 27, 437–443. [CrossRef]
- Chen, J.; Liu, Y.; Pan, D.; Xu, T.; Luo, Y.; Wu, W.; Wu, P.; Zhu, H.; Li, D. Estrogen inhibits endoplasmic reticulum stress and ameliorates myocardial ischemia/reperfusion injury in rats by upregulating SERCA2a. Cell Commun. Signal. 2022, 20, 1–16. [CrossRef]
- van Eickels, M.; Patten, R.D.; Aronovitz, M.J.; Alsheikh-Ali, A.; Gostyla, K.; Celestin, F.; Grohe, C.; E Mendelsohn, M.; Karas, R.H. 17-Beta-Estradiol increases cardiac remodeling and mortality in mice with myocardial infarction. J. Am. Coll. Cardiol. 2003, 41, 2084–2092. [CrossRef]
- Wood, W.G.; Lüdemann, J.; Mitusch, R.; Heinrich, J.; Maass, R.; Frick, U. Evaluation of a sensitive immunoluminometric assay for the determination of C-reactive protein (CRP) in serum and plasma and the establishment of reference ranges for different groups of subjects.. 2000, 46, 131–40.
- Prieto, B.; Miguel, D.; Costa, M.; Coto, D.; Alvarez, F.V. New quantitative eletrochemiluminescence method (ECLIA) for interleukin-6 (IL-6) measurement. Clin. Chem. Lab. Med. 2010, 48, 835–838.
- E Fraley, A.; Tsimikas, S. Clinical applications of circulating oxidized low-density lipoprotein biomarkers in cardiovascular disease. Curr. Opin. Infect. Dis. 2006, 17, 502–509. [CrossRef]
- Jing, J.; Ding, N.; Wang, D.; Ge, X.; Ma, J.; Ma, R.; Huang, X.; Jueraitetibaike, K.; Liang, K.; Wang, S.; et al. Oxidized-LDL inhibits testosterone biosynthesis by affecting mitochondrial function and the p38 MAPK/COX-2 signaling pathway in Leydig cells. Cell Death Dis. 2020, 11, 1–15. [CrossRef]
- Weitzel, J.M.; Vernunft, A.; Krüger, B.; Plinski, C.; Viergutz, T. LOX-1 regulates estrogenesis via intracellular calcium release from bovine granulosa cells. Cytom. Part A 2013, 85, 88–93. [CrossRef]
- Infante, M.; Pieri, M.; Lupisella, S.; D’Amore, L.; Bernardini, S.; Fabbri, A.; Iannetta, M.; Andreoni, M.; Morello, M. Low testosterone levels and high estradiol to testosterone ratio are associated with hyperinflammatory state and mortality in hospitalized men with COVID-19. Eur. Rev. Med. Pharm. Sci. 2021, 25, 5889–5903.
- Ostinelli, G.; Laforest, S.; Denham, S.G.; Gauthier, M.-F.; Drolet-Labelle, V.; Scott, E.; Hould, F.-S.; Marceau, S.; Homer, N.Z.M.; Bégin, C.; et al. Increased Adipose Tissue Indices of Androgen Catabolism and Aromatization in Women With Metabolic Dysfunction. J. Clin. Endocrinol. Metab. 2022, 107, e3330–e3342. [CrossRef]
- Bruun, J.M.; Helge, J.W.; Richelsen, B.; Stallknecht, B. Diet and exercise reduce low-grade inflammation and macrophage infiltration in adipose tissue but not in skeletal muscle in severely obese subjects. Am. J. Physiol. Metab. 2006, 290, E961–E967. [CrossRef]
- Rana, B.K.; Flatt, S.W.; Dennis Health; Pakiz, B.; Quintana, E.L.; Natarajan, L.; Rock, C.L.; Dennis D. Health The IL6 Gene Promoter SNP and Plasma IL-6 in Response to Diet Intervention. Nutrients 2017, 9, 552, doi:10.3390/nu9060552.
- Martínez-Chacón, G.; Brown, K.A.; Docanto, M.M.; Kumar, H.; Salminen, S.; Saarinen, N.; Mäkelä, S. IL-10 suppresses TNF-α-induced expression of human aromatase gene in mammary adipose tissue. FASEB J. 2018, 32, 3361–3370. [CrossRef]
- Brown, K.A.; Iyengar, N.M.; Zhou, X.K.; Gucalp, A.; Subbaramaiah, K.; Wang, H.; Giri, D.D.; Morrow, M.; Falcone, D.J.; Wendel, N.K.; et al. Menopause Is a Determinant of Breast Aromatase Expression and Its Associations With BMI, Inflammation, and Systemic Markers. J. Clin. Endocrinol. Metab. 2017, 102, 1692–1701. [CrossRef]
- Martínez-Chacón, G.; Yatkin, E.; Polari, L.; Dinç, D.D.; Peuhu, E.; Hartiala, P.; Saarinen, N.; Mäkelä, S. CC chemokine ligand 2 (CCL2) stimulates aromatase gene expression in mammary adipose tissue. FASEB J. 2021, 35, e21536. [CrossRef]
- Massillo, C.; Dalton, G.N.; Porretti, J.; Scalise, G.D.; Farré, P.L.; Piccioni, F.; Secchiari, F.; Pascuali, N.; Clyne, C.; Gardner, K.; et al. CTBP1/CYP19A1/estradiol axis together with adipose tissue impacts over prostate cancer growth associated to metabolic syndrome. Int. J. Cancer 2018, 144, 1115–1127. [CrossRef]
- Gautier, A.; Bonnet, F.; Dubois, S.; Massart, C.; Grosheny, C.; Bachelot, A.; Aubé, C.; Balkau, B.; Ducluzeau, P. Associations between visceral adipose tissue, inflammation and sex steroid concentrations in men. Clin. Endocrinol. 2012, 78, 373–378. [CrossRef]
- Wake, D.J.; Strand, M.; Rask, E.; Westerbacka, J.; Livingstone, D.E.W.; Soderberg, S.; Andrew, R.; Yki-Jarvinen, H.; Olsson, T.; Walker, B.R. Intra-adipose sex steroid metabolism and body fat distribution in idiopathic human obesity. Clin. Endocrinol. 2007, 66, 440–446. [CrossRef]
- Shan, B.; Shao, M.; Zhang, Q.; Hepler, C.; Paschoal, V.A.; Barnes, S.D.; Vishvanath, L.; An, Y.A.; Jia, L.; Malladi, V.S.; et al. Perivascular mesenchymal cells control adipose-tissue macrophage accrual in obesity. Nat. Metab. 2020, 2, 1332–1349. [CrossRef]
- Folsom, A.R.; Golden, S.H.; Boland, L.L.; Szklo, М. Association of endogenous hormones with C-reactive protein, fibrinogen, and white blood count in postmenopausal women. Eur. J. Epidemiol. 2005, 20, 1015–1022.
- Maggio, M.; Ceda, G.P.; Lauretani, F.; Bandinelli, S.; Metter, E.J.; Artoni, A.; Gatti, E.; Ruggiero, C.; Guralnik, J.M.; Valenti, G.; et al. Estradiol and Inflammatory Markers in Older Men. J. Clin. Endocrinol. Metab. 2009, 94, 518–522. [CrossRef]
- Pour, H.R.N.; Grobbee, D.E.; Muller, M.; Van Der Schouw, Y.T. Association of endogenous sex hormone with C-reactive protein levels in middle-aged and elderly men. Clin. Endocrinol. 2007, 66, 394–398. [CrossRef]
- Nasiri-Ansari, N.; Spilioti, E.; Kyrou, I.; Kalotychou, V.; Chatzigeorgiou, A.; Sanoudou, D.; Dahlman-Wright, K.; Randeva, H.S.; Papavassiliou, A.G.; Moutsatsou, P.; et al. Estrogen Receptor Subtypes Elicit a Distinct Gene Expression Profile of Endothelial-Derived Factors Implicated in Atherosclerotic Plaque Vulnerability. Int. J. Mol. Sci. 2022, 23, 10960. [CrossRef]
- Georgakis, M.K.; van der Laan, S.W.; Asare, Y.; Mekke, J.M.; Haitjema, S.; Schoneveld, A.H.; de Jager, S.C.; Nurmohamed, N.S.; Kroon, J.; Stroes, E.S.; et al. Monocyte-Chemoattractant Protein-1 Levels in Human Atherosclerotic Lesions Associate With Plaque Vulnerability. Arter. Thromb. Vasc. Biol. 2021, 41, 2038–2048. [CrossRef]
- Galis, Z.S.; Sukhova, G.K.; Lark, M.W.; Libby, P. Increased expression of matrix metalloproteinases and matrix degrading activity in vulnerable regions of human atherosclerotic plaques. J. Clin. Invest. 1994, 90, 775–778.
- Inoue, S.; Nakazawa, T.; Cho, A.; Davastan, F.; Shilling, D.; Daum, G.; Reidy, M. Regulation of arterial lesions in mice depends on differential smooth muscle cell migration: A role for sphingosine-1-phosphate receptors. J. Vasc. Surg. 2007, 46, 756–763. [CrossRef]
- Nakamura, Y.; Suzuki, T.; Sasano, H. Estrogen actions and in situ synthesis in human vascular smooth muscle cells and their correlation with atherosclerosis. J. Steroid Biochem. Mol. Biol. 2005, 93, 263–268. [CrossRef]
- Takeshita, K.; Hayashi, M.; Iino, S.; Kondo, T.; Inden, Y.; Iwase, M.; Kojima, T.; Hirai, M.; Ito, M.; Loskutoff, D.J.; et al. Increased Expression of Plasminogen Activator Inhibitor-1 in Cardiomyocytes Contributes to Cardiac Fibrosis after Myocardial Infarction. Am. J. Pathol. 2004, 164, 449–456. [CrossRef]
- Ajayi, A.A.L.; Mathur, R.; Halushka, P.V. Testosterone Increases Human Platelet Thromboxane A 2 Receptor Density and Aggregation Responses. Circulation 1995, 91, 2742–2747. [CrossRef]
- Maugeri, N.; Manfredi, A.A.; Maseri, A. Clinical and experimental evidences on the prothrombotic properties of neutrophils. Srp. Arh. za Celok. Lek. 2010, 138, 50–52. [CrossRef]
- Glintborg, D.; Sidelmann, J.J.; Altinok, M.L.; Mumm, H.; Andersen, M. Increased thrombin generation in women with polycystic ovary syndrome. Metabolism 2015, 64, 1272–1278. [CrossRef]
- Sowers, M.R.; Jannausch, M.; Randolph, J.F.; McConnell, D.; Little, R.; Lasley, B.; Pasternak, R.; Sutton-Tyrrell, K.; Matthews, K.A. Androgens Are Associated with Hemostatic and Inflammatory Factors among Women at the Mid-Life. J. Clin. Endocrinol. Metab. 2005, 90, 6064–6071. [CrossRef]
- Vermeulen, A.; Kaufman, J.M.; Goemaere, S.; van Pottelberg, I. Estradiol in elderly men. Aging Male 2002, 5, 98-102.
- Longcope, C.; Pratt, J.H.; Stephen, H.S.; Fineberg, S.E. Aromatization of Androgens by Muscle and Adipose Tissue in Vivo*. J. Clin. Endocrinol. Metab. 1978, 46, 146–152. [CrossRef]

Table 1.
Characteristics of the Patients – Comparison by Sex.
| Variables | Men n=70 | Women n=41 | P-value |
|---|---|---|---|
| Age, years | 62.8±12.7 | 70.7±10 | 0.001 |
| Hypertension, n % | 66 (94%) | 40 (97%) | NS |
| Dyslipidemia, n % | 58 (83%) | 38 (93%) | NS |
| Diabetes mellitus, n % | 24 (34) | 18 (43) | 0.320 |
| oxLDL, mg/ml | 10.4±7.3 | 8.1±4.9 | 0.099 |
| CRP, mg/l | 27.7±52 | 16.9±21.7 | 0.032 |
| WBCx109 l | 10.3±3.8 | 9.8±3.3 | 0.662 |
| Syntax score | 14.1±10.6 | 11.2±9.2 | 0.027 |
| EF, % | 53.6±10 | 52.4±12.9 | 0.606 |
| BMI, kg/m2 | 28.4±4.3 | 27.4±5.3 | 0.330 |
| CK, U/l | 1178.9±1486.4 | 474±722.4 | 0.001 |
| CK-MB, U/l | 116.1±146 | 63.6±82.1 | 0.057 |
| hsTnT, ng/ml | 2.5±3.4 | 1.4±2.5 | 0.036 |
| E2, pg/ml | 155.8±69.6 | 108.7±126.9 | <0.0001 |
| T, ng/ml | 13.4±5.2 | 1.7±3 | <0.0001 |
| E2/T | 0.02±0.03 | 0.23±0.51 | <0.0001 |
Abbreviations: oxLDL, oxidized low-density lipoproteins; CRP, C-reactive protein; WBC, white blood cells; EF, ejection fraction; BMI, body mass index; CK, creatine kinase; CK-MB, MB fraction of CK; hsTnT, high-sensitive troponin T; E2, endogenous 17β-estradiol; T, total testosterone.
Table 2.
Gonadal Steroids, Inflammatory, and Oxidative Stress Markers - Association with Peak Creatine Kinase (CK) Activity.
Table 2.
Gonadal Steroids, Inflammatory, and Oxidative Stress Markers - Association with Peak Creatine Kinase (CK) Activity.
| CK | Lowest tertile | Highest tertile | P-value | OR | 95% CI | P-value |
|---|---|---|---|---|---|---|
| Male patients | ||||||
| oxLDL | 10±8.9 | 10±7.9 | 0.317 | 0.985 | 0.908-1.070 | 0.725 |
| WBC | 8.4±1.9 | 11.9±4.4 | 0.002 | 1.487 | 1.081-2.045 | 0.015 |
| CRP | 11.6±20.5 | 49.5±56.3 | 0.005 | 1.040 | 1.003-1.078 | 0.033 |
| Syntax score | 15.9±10.8 | 17.5±10.2 | 0.301 | 1.016 | 0.958-1.077 | 0.593 |
| E2 | 133.6±54.4 | 185.6±92.8 | 0.015 | 1.011 | 1.000-1.022 | 0.047 |
| T | 14.5±6.2 | 13±4.6 | 0.179 | 0.947 | 0.843-1.062 | 0.352 |
| E2/T | 0.016±0.016 | 0.021±0.017 | 0.156 | 6.788 | 0.154-298.9 | 0.321 |
| Female patients | ||||||
| oxLDL | 9.6±7.9 | 10.9±7.3 | 0.314 | 1.026 | 1.026-1.134 | 0.620 |
| WBC | 8.6±2.1 | 11.2±3.3 | 0.026 | 1.426 | 1.017-1.998 | 0.039 |
| CRP | 10.9±16.8 | 22.5±25.8 | 0.170 | 1.030 | 0.985-1.078 | 0.198 |
| Syntax score | 10.7±8.1 | 13.8±9.9 | 0.395 | 1.041 | 0.951-1.141 | 0.381 |
| E2 | 105.5±109.1 | 155.6±178.1 | 0.377 | 1.033 | 0.997-1.009 | 0.383 |
| T | 0.98±1.57 | 3.23±4.5 | 0.050 | 1.346 | 0.882-2.054 | 0.169 |
| E2/T | 0.39±0.84 | 0.18±0.21 | 0.181 | 0.446 | 0.063-3.167 | 0.419 |
Abbreviations: oxLDL, oxidized low-density lipoproteins; CRP, C-reactive protein; WBC, white blood cells; CK, creatine kinase; CK-MB, MB fraction of CK; E2, endogenous 17β-estradiol; T, total testosterone.
Table 3.
Estradiol (E2) and Testosterone (T), Inflammation, and Oxidative Stress Relationship with Post-PCI Activity of CK-MB.
Table 3.
Estradiol (E2) and Testosterone (T), Inflammation, and Oxidative Stress Relationship with Post-PCI Activity of CK-MB.
| CK-MB | Lowest tertile | Highest tertile | P-value | OR | 95% CI | P-value |
|---|---|---|---|---|---|---|
| Male patients | ||||||
| oxLDL | 10.4±8.3 | 9.8±7.7 | 0.794 | 0.983 | 0.910-1.074 | 0.787 |
| WBC | 8.2±1.8 | 12.7±4.7 | <0.0001 | 1.709 | 1.174-2.488 | 0.005 |
| CRP | 15.7±27.7 | 58.4±66.2 | 0.008 | 1.024 | 1.002-1.046 | 0.029 |
| Syntax score | 15.5±10.2 | 18.1±9.5 | 0.370 | 1.028 | 0.968-1.092 | 0.364 |
| E2 | 128±45.9 | 188.9±90.1 | 0.003 | 1.018 | 1.004-1.032 | 0.013 |
| T | 13.8±5.4 | 12.9±4.5 | 0.268 | 0.963 | 0.856-1.083 | 0.528 |
| E2/T | 0.019±0.021 | 0.019±0.015 | 0.470 | 0.879 | 0.033-23.517 | 0.939 |
| Female patients | ||||||
| oxLDL | 8.9±6.6 | 8.9±3.7 | 0.993 | 0.991 | 0.913-1.076 | 0.838 |
| WBC | 8.3±2.5 | 11.1±3.3 | 0.022 | 1.384 | 1.022-1.875 | 0.036 |
| CRP | 11.7±16.3 | 22.3±25.9 | 0.195 | 1.027 | 0.984-1.072 | 0.217 |
| Syntax score | 13.2±16.3 | 22.3±25.9 | 0.195 | 0.979 | 0.890-1.076 | 0.659 |
| E2 | 101.1±106.9 | 137.9±171.1 | 0.245 | 1.002 | 0.996-1.008 | 0.489 |
| T | 0.73±0.53 | 3.1±4.6 | 0.039 | 2.115 | 0.594-7.527 | 0.248 |
| E2/T | 0.36±0.81 | 0.16±0.20 | 0.188 | 0.443 | 0.057-3.472 | 0.439 |
Abbreviations: PCI, percutaneous coronary intervention; oxLDL, oxidized low-density lipoproteins; CRP, C-reactive protein; WBC, white blood cells; CK, creatine kinase; CK-MB, MB fraction of CK; E2, endogenous 17β-estradiol; T, total testosterone.
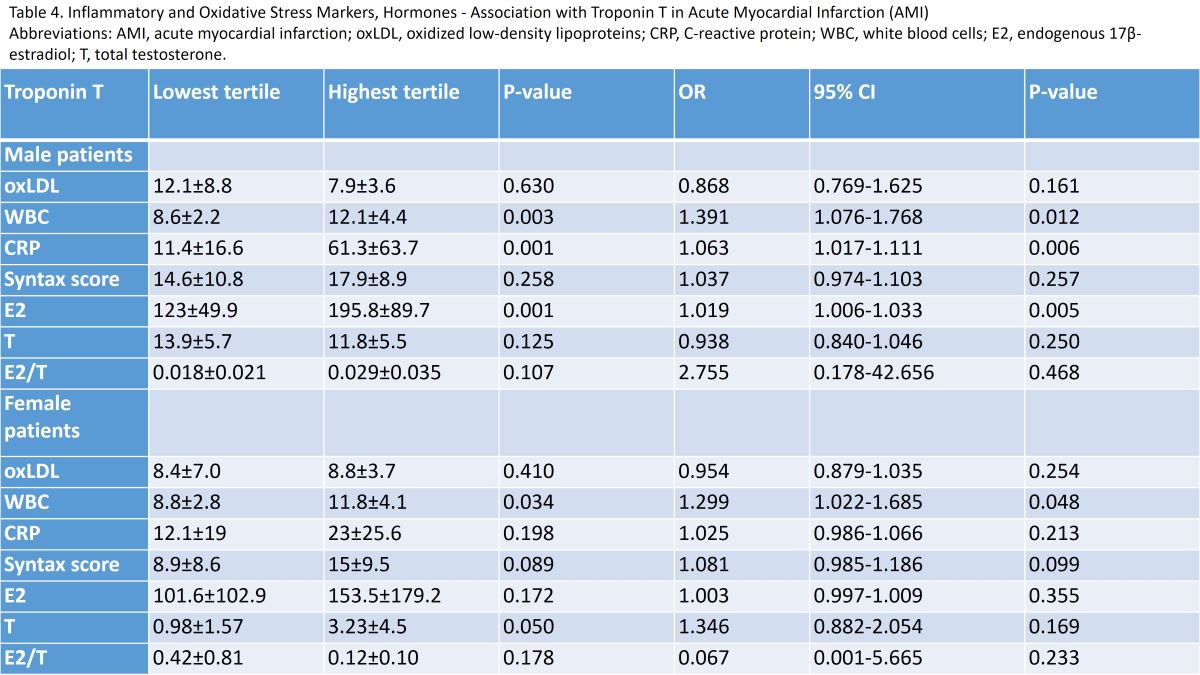
Table 4.
Inflammatory and Oxidative Stress Markers, Hormones - Association with Troponin T in Acute Myocardial Infarction (AMI).
Table 4.
Inflammatory and Oxidative Stress Markers, Hormones - Association with Troponin T in Acute Myocardial Infarction (AMI).
| Troponin T | Lowest tertile | Highest tertile | P-value | OR | 95% CI | P-value |
|---|---|---|---|---|---|---|
| Male patients | ||||||
| oxLDL | 12.1±8.8 | 7.9±3.6 | 0.630 | 0.868 | 0.769-1.625 | 0.161 |
| WBC | 8.6±2.2 | 12.1±4.4 | 0.003 | 1.391 | 1.076-1.768 | 0.012 |
| CRP | 11.4±16.6 | 61.3±63.7 | 0.001 | 1.063 | 1.017-1.111 | 0.006 |
| Syntax score | 14.6±10.8 | 17.9±8.9 | 0.258 | 1.037 | 0.974-1.103 | 0.257 |
| E2 | 123±49.9 | 195.8±89.7 | 0.001 | 1.019 | 1.006-1.033 | 0.005 |
| T | 13.9±5.7 | 11.8±5.5 | 0.125 | 0.938 | 0.840-1.046 | 0.250 |
| E2/T | 0.018±0.021 | 0.029±0.035 | 0.107 | 2.755 | 0.178-42.656 | 0.468 |
| Female patients | ||||||
| oxLDL | 8.4±7.0 | 8.8±3.7 | 0.410 | 0.954 | 0.879-1.035 | 0.254 |
| WBC | 8.8±2.8 | 11.8±4.1 | 0.034 | 1.299 | 1.022-1.685 | 0.048 |
| CRP | 12.1±19 | 23±25.6 | 0.198 | 1.025 | 0.986-1.066 | 0.213 |
| Syntax score | 8.9±8.6 | 15±9.5 | 0.089 | 1.081 | 0.985-1.186 | 0.099 |
| E2 | 101.6±102.9 | 153.5±179.2 | 0.172 | 1.003 | 0.997-1.009 | 0.355 |
| T | 0.98±1.57 | 3.23±4.5 | 0.050 | 1.346 | 0.882-2.054 | 0.169 |
| E2/T | 0.42±0.81 | 0.12±0.10 | 0.178 | 0.067 | 0.001-5.665 | 0.233 |
Abbreviations: AMI, acute myocardial infarction; oxLDL, oxidized low-density lipoproteins; CRP, C-reactive protein; WBC, white blood cells; E2, endogenous 17β-estradiol; T, total testosterone.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



