
Submitted:
02 October 2023
Posted:
03 October 2023
You are already at the latest version
Abstract
The interrelatedness of social-structural aspects and psychological features with the vaccination intention provides the context to explore personal psychological fea-tures related to general decision-making and vaccine-related dispositions, and their contribution to the intention to vaccinate, within post-pandemic circumstances, after the imposed possibility of choosing a vaccine brand. The aim of our study was to map the function (promotive, protective, risk, vulnerability) of a set of psychological aspects in the intention to vaccinate, in people with different social roles regarding the vaccination. We surveyed three samples of people: healthcare providers (HPs), parents, and lay people, within the context of the after-pandemic. Negative vaccine attitudes lower intention to vaccinate in all regression models (all βs ranging from -.128 to -.983, all ps < .01). The main results indicate that, regardless of the sam-ple/social role, there is a shared attitudinal core for positive vaccination intention. This core consists of [high] trust in large corporations, government, and healthcare systems, as well as perceived consensus on vaccine safety/efficacy and experience of freedom (protective factors), and [low] vaccination conspiracy beliefs, trust in social media, and choice overload (risk and vulnerability factors, respectively). There are no common promotive factors of intention to vaccinate; for parents, perceived consensus on vaccines, and trust in corporations and the healthcare system play such roles, for HPs experience of freedom is obtained as a unique promotive factor. In contrast, for laypeople, no unique promotive factors were found. These results and guidelines for the promotion of positive vaccination behavior are further discussed.
Keywords:
vaccination intention
; health-care providers
; parents
; lay people
; promotive factors
; protective factors
; risk factors
; vulnerability factors
; vaccine decision-making
; vaccination behavior
1. Introduction
The ability of humankind to develop knowledge for the advancement of society is one of the self-evident mechanisms of its survival, and the appropriate use of scientific evidence in public policies should inevitably lead to better population outcomes. This is not the case. Translating scientific insights into an effective policy isn’t simple, nor it is straightforward, it is simply not enough that the decision-makers proscribe an evidence-based immunization schedule. For this policy to be effective cooperation from its recipients (mostly laypeople) is necessary. The distinctive feature of vaccines as a medical procedure is that vaccines act at both the individual and community level, making the decision to vaccinate inherently social (Arnesen et al., 2018; Goldenberg, 2021), further emphasized by the psychological features of recipients (Damnjanović et al., 2018a; Goldenberg, 2021). Both recent data and recent global and local responses to the COVID-19 epidemic testify that this kind of unanimous cooperation is no longer easy to achieve (Enea et al., 2023; Lewandowsky & van der Linden, 2021). Over time, studies repeatedly demonstrated that peoples’ vaccination behavior changes in response to the outbreak of vaccine-preventable diseases (Funk et al., 2009; Lep et al., 2021; McClure et al., 2017; Schumpe et al., 2022). The complex interplay between outbreaks of infectious diseases and reactive behavior works as follows: awareness of the proximity of the disease leads people to take measures to reduce their susceptibility, which, in turn, impacts potential future epidemics, as illustrated by Chen & Orenstein (Chen & Orenstein, 1996). This reactive-preventive cycle is the costliest pattern to foster pro-vaccine attitudes, leads only to short-term herd immunity, and hinders people’s understanding of the causes of the outbreak and the mechanisms of the epidemics. In sum, having vaccines and being supported by the science is not enough for the sustainable vaccination program. In addition to policy and science, it is the sustainable vaccination behavior and intentional decisions that are prerequisites, both of which stemming from social and psychological landscape. This is indeed recognized by the stakeholders, who started design communication regarding vaccination (Arnesen et al., 2018; Camargo & Grant, 2015; Managing Epidemics, n.d.; Reyna, 2012).
An intention to vaccinate is thus of enormous importance to the success of vaccination programs and are not only changeable (Goldenberg, 2021; Rasmussen & Goodman, 2020), but also multi-determined (Damnjanović et al., 2018b), and whose roots may be traceable in structural and social conditions, psychological dispositions, and experience of the pandemic (experiential aspects of the person who is considering vaccination).
The social role a person plays in relation to the vaccination is inextricably linked to the vaccination behavior, since the intention to be vaccinated is a decision with social causes and social consequences. Two main roles which are highlighted by the literature as the pillars of vaccination program are healthcare providers (HP), and parents. The role of health-care provider in facilitating vaccination is one of the vitals, as the research shows (Corace et al., 2016; Nikic et al., 2023; Opel et al., 2013; Stöcker et al., 2023). Though there are some findings showing that HP do differ in terms of stance toward vaccination (Rosental & Shmueli, 2021), majority have strong positive consensus (Gesser-Edelsburg & Badarna Keywan, 2022). As stated, having a vaccine and a HPs positive attitude is not enough, as this scientific consensus needs to be communicated with the vaccine’s recipients, which is turns out to be challenging (Bavel et al., 2020; Lewandowsky & van der Linden, 2021), presumably due to the different views on vaccination.
Next to the HPs, the role of parents in acting as both vaccine-recipient and a crucial spokesperson for future generations, is recognized as the pivotal in realm of vaccination (Damnjanović et al., 2018b; Gowda & Dempsey, 2013; Opel et al., 2013). Parents represent a unique group in this matter because they make decisions on behalf of their children who are unable of doing so. For parents, this is a socially mandated highly involving decision, that affects the child’s health (Damnjanović et al., 2018b; Thompson, 2007). Parents are, hence, both decision makers and highly involved proxy decision makers. Due to their high involvement in the matters of child health, parental’ concerns may be overemphasized, missed to be addressed and supported by the officials and HPs, which leads to lowering their intention to vaccinate, both themselves and the children.
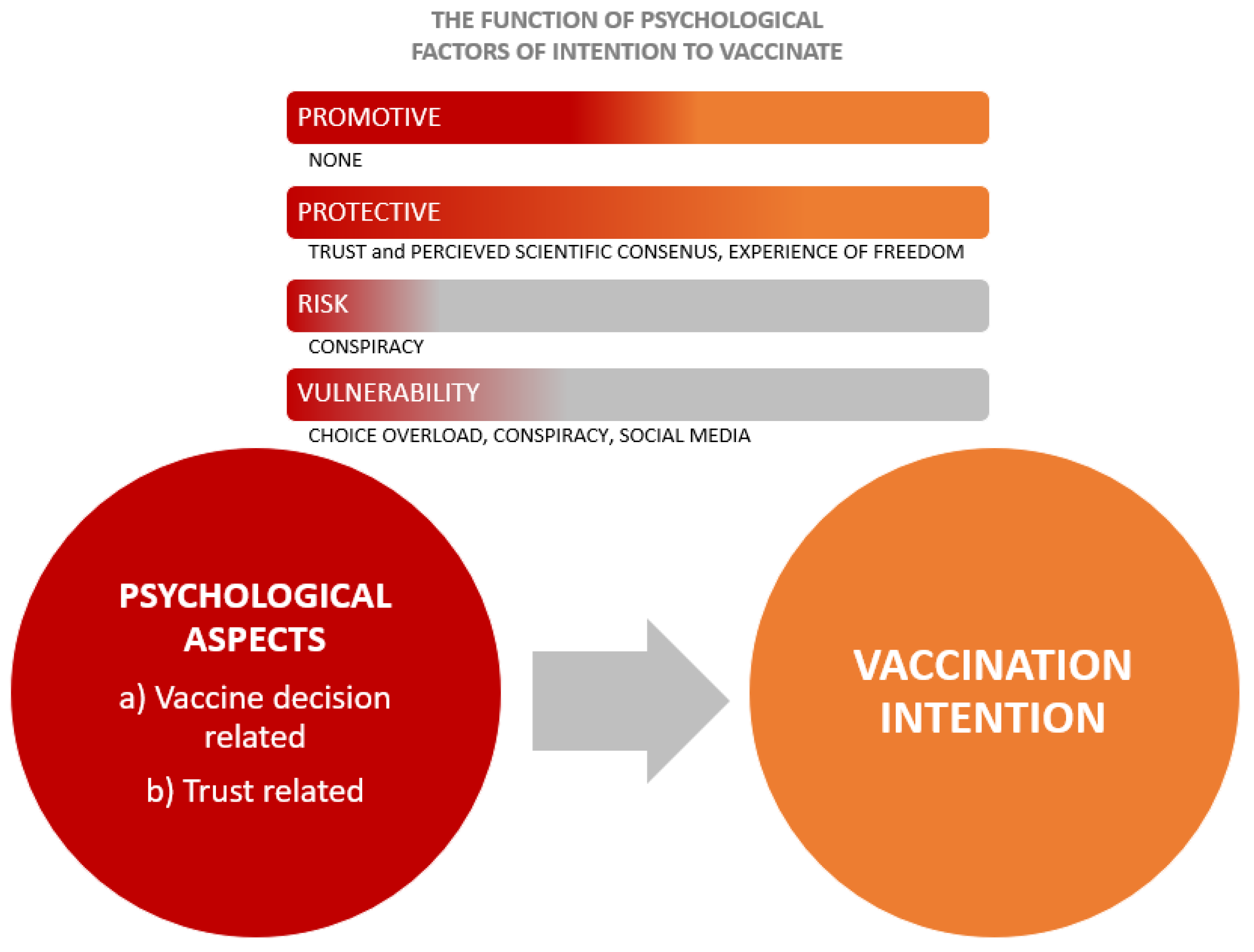
In addition to presented structural aspects, such as social roles, policies, official requirements, psychological features relevant for vaccination behavior are both general decision-making related, such as trust-related, and vaccine-decision-specific factors. The first ones are relatively stable psychological features of person, such as thinking styles (Kiviniemi et al., 2018; Stanovich & Toplak, 2023), risk-taking (Reyna, 2012), sources of information which person uses (Lancet, 2020; Lep et al., 2021; Lewandowsky & van der Linden, 2021), trust (both in system and personal) (Bangerter et al., 2012; Cheung & Tse, 2008; Goldenberg, 2021; Han et al., 2023; Hobson-West, 2007; Thomas et al., 2020). Specific for the vaccination-decision are perception of danger , involvement in the vaccination decision or psychological proximity (Damnjanović et al., 2018b; Thompson, 2007), vaccine hesitancy (McClure et al., 2017), feeling of being burdened by the decision (Lau et al., 2015), freedom of choice (Lau et al., 2015), perceived social consensus and norms and others (De Visser et al., 2011; Oraby et al., 2014), perceived vaccine safety and efficacy (Lazarus et al., 2022), knowledge and subjective knowledge (Lep et al., 2021; Zingg & Siegrist, 2012). Behavioral frameworks were developed to highlight the importance of psychological factors for vaccination intention. The most notable framework for explaining and influencing the intention to vaccinate are contemporary integrated behavioral models (IBM), which are assuming the equivalence between intention and behavior. IBMs integrate previous, more traditional behavioral models, such as theory of planned behavior (Ajzen, 1991), the health belief model (Rosenstock, 1974), or theory of reasoned action (Fishbein & Ajzen, 2011), and sometimes social-cognitive theory (Wicaksana et al., 2023). The main determinants of (behavioral) intention in this paradigm are attitudes, perceived norm, and personal agency (Fishbein & Ajzen, 2011; Glanz et al., n.d.; Sharma, 2021; Wicaksana et al., 2023). In sum, psychological variables have been empirically considered in and outside of IBMs, and the relationship between various psychological factors and the decision or intention to vaccinate has been demonstrated, as well as their interrelatedness (Gowda & Dempsey, 2013). IBMs have been used to analyze different roles in regard to the vaccination, such as students, nurses, patients (Rosental & Shmueli, 2021; Wicaksana et al., 2023). Psychological variables can operate as independent promotive or risk factors for health-related behaviors (National Research Council (US) and Institute of Medicine (US) Board on Children et al., 2001; Schneiderman et al., 2019; Thomas et al., 2020), such as directly influencing (positively or negatively) vaccination intention. Promotional factors are personal psychological aspects, regardless they are vaccine-related or not, that directly influence the intention to get vaccinated by promoting it, whereas risk psychological factors are those that decrease that intention. Psychological factors can also interact, thus protecting or undermining either a positive or a negative relationship between attitudes and vaccination intentions. We may illustrate this using the example of trust in HCPs, which is a psychological factor related to vaccination intention. High levels of trust in HCPs may protect vaccination intentions in people with relatively unfavorable attitudes towards vaccination, by reducing the correlation between these two variables. If it involves, for instance, a medical expert who is a loud opponent of the vaccination, even low trust might shield the intention to be vaccinated. In short, psychological features have possible multiple functions regarding the intention to vaccinate as a form of preventive health-related behavior (Schneiderman et al., 2019; Thomas et al., 2020). If they form straightforward either positive or negative influence on vaccination decision, they serve as a) promotive or b) risk factors. If they interact with other psychological features and skew the relationship between those and intention to vaccinate, they serve as c) protective or d) vulnerability factor.
These social-structural and psychological factors are embedded in the realty of the presence (or not) of vaccine-preventable disease. To reiterate, the proximity of the disease raises the vaccination rate, which lowers as soon as the perceived proximity of the danger passes, so the intention to vaccinate changes depending on the proximity of the disease, as described by the reactive-preventive cycle (Chen & Orenstein, 1996). On the behavioral-psychological level, this means that the connection between structural (e.g., social roles) and psychological dispositions on the one hand, and vaccination intentions on the other, changes under the influence of the epidemic experience. Moreover, in an epidemic, these social roles become even more pronounced: ideally, doctors and parents have the same conceptualization of the vaccine and common goals and ground for communication. This more often than not is not the case: for the HPs vaccine is a routine procedure supported by professional knowledge, and for lay people and parents it is a highly-involving health-related decision, not supported by knowledge (Damnjanović et al., 2018b, 2019; Goldenberg, 2014).
The epidemic realm influences many aspects of (not only) vaccination behavior. It adds to the anxiety, shapes informing and perception of danger, and leads to overall overload by the health-related and vaccination intentions (Cheung & Tse, 2008; Lep et al., 2021). This is especially notable in case of countries in which citizens could choose the vaccine against COVID-19 type or manufacturer, which are to this day, Hungary and Serbia, with Serbia being the only country introducing the full free choice for citizens among all available vaccines, trough free digital tool accessible to every citizen. Five vaccines against COVID-19 were authorized and available Pfizer/BioNTech, Sinopharm, the Gamaleya Institute (Sputnik V), Oxford/AstraZeneca, and Moderna. Hungary employed opt-out system in which citizens had the possibility to refuse the assigned type of vaccine (Kutasi et al., 2022). The Serbian experience with COVID-19 provides particularly useful insights. The country was among first few countries globally to introduce COVID-19 vaccination beginning of January 2021. This intervention, being the reactive one, unfortunately did not overcome the absence of the timely vaccine-related education and communication, which is not endemic for Serbia, rather a global phenomenon, lead to the vaccination coverage of less than 50% of the total population at the end of March 2022.
As it is important to acknowledge the interrelatedness of social-structural aspects and psychological features with the vaccination decision, the rationale for our study was to explore personal psychological features related to the decision making in general and vaccine-related dispositions and their contribution to the intention to vaccinate, in three key-groups (HPs, parents, lay people), within post-pandemic circumstances, after the imposed possibility of choosing a vaccine brand. The intricate interaction of (a) structural-social roles regarding vaccination, (b) psychological characteristics (general decision making and vaccine related), and (c) vaccination intentions are illustrated in the Figure 1.
Literature overview indicates that people in different social roles regarding vaccination differ in terms of intention to vaccinate, more specifically that their vaccination decision stems from different grounds. For HCPs, this is (or it should be) knowledge and professional codex (Gesser-Edelsburg & Badarna Keywan, 2022; Stöcker et al., 2023), whereas for lay people, parents especially, it is based on trust and personal involvement in the decision (Bangerter et al., 2012; Goldenberg, 2021; Hobson-West, 2007). In addition to the social role, personal psychological aspects of HCPs, parents and lay people which a) concern vaccination itself, and b) general decision-making shape the intention to vaccinate. Since they themselves could partially be dependent on social role, it is not obvious whether every psychological aspect, whether vaccine related or of a general type, have a constant function in each group of people. To reiterate, they can serve to promote and protect, or as a risk or vulnerability factor. Hence, it could be that the same psychological variables have a different function in intention to vaccinate in different groups of people. The aim of our study was to map the function of vaccine related and general decision-making psychological aspects in intention to vaccinate, in three subsamples: HCPs, parents and laypeople, and to map those factors that are universally promotional, protective, risk, and/or vulnerable, as well to observe when their function differs in different samples.
2. Materials and Methods
2.1. Study Design
A cross-sectional study was carried out during June 2023 and July 2023. We employed a correlational design, with socio-structural and psychological dispositions, and vaccine-related measures as predictors of the intention to vaccinate one’s (hypothetical) child.
2.2. Setting and Sample
The present study was carried out online, via the snowballing method and Facebook advertising tool. The study was conducted in accordance with the Declaration of Helsinki regarding ethical protection of human participants in research, the General Data Protection Regulation (GDPR), and with ethical approval of the Institutional Review Board (IRB).
Special attention was given to sample size calculation. Based on the effect size (f2 = .136) obtained in similar research design study on psychological predictors of vaccination intention (e.g. Huynh & Senger, 2021), with the test power of 0.99 and α of 0.01 in hierarchical regression analysis with three parameters (predictor, moderator, and their interaction) in the prediction model of vaccination intention, the sample size to aim for was at least N = 226 per sample.
The inclusion criteria applicable to the entire sample was that participants were adults (N = 745). Since we collected three different subsamples (N_HPs = 219; N parents = 263; N lay people = 263), the specific inclusion criteria differed between the samples. Namely, participants were triaged according to their socio-structural status – whether they were healthcare providers in direct contact with patients, and if not, whether they were parents or not (lay people). Socio-demographic structure of the three samples regarding age, gender, marital status, and socio-economic status (SES) is given in Supplementary material 1, Table S1, while more specific information about vaccine-type choices is given in Table S2. Specific information applicable only to HPs and parents’ subsamples is given below.
2.2.1. HPs
The HPs subsample (N = 219) included healthcare providers employed in the medical (89%), dental (2.3%), and pharmaceutical (6.8%) fields of healthcare. The remainder of the sample (1.8%) comprised participants employed in the healthcare sector but do not belong to the medical, dental, and pharmaceutical fields. Majority of the participants (64.4%) were medical specialists. Also, two-thirds (69.4%) of HPs were employed in the government sector, while 21% worked in private practices, and 9.6% in both sectors.
2.2.2. Parents
The parents’ subsample consisted of lay people who were primary caretakers of one or more children (N = 263). The maximum number of children a participant was taking care of were four (1.8% parents). Nearly half of the parents’ sample (49.7%) comprised primary caretakers of two children, 9.6% had three children, and 39.3% had one child.
2.3. Procedure
All participants accessed the questionnaire via the same link, where they were triaged and referred to the three different questionnaires designed for each of the sample groups. This was done by asking participants whether they are healthcare providers in regular contact with patients. If yes, they were redirected to the questionnaire, and if not, they were directed to the next question regarding parenthood (are they parents/caretakers of a child, or not), and then, based on their answer redirected to one of the two questionnaires designed for parents or nonparents. This was done because participants completed a large battery of measures as a part of a larger project, some of which are beyond the scope of the present study and won’t be reported, and some that differed between the three sample groups (e.g. parents/caretakers answered questions regarding number of children they take care of, while this was not applicable for the sample of other lay people that are not parents).
After accessing the questionnaire that corresponds to the participants’ group based on parenthood and vocation, all participants included in the final sample gave informed consent to participation. Following this, they completed the questionnaire comprising the sociodemographic questions and questionnaires aimed to measure the intention to vaccinate one’s (future) child, social-structural aspects, and dispositional and vaccine-specific psychological features relevant for vaccination behavior (see Materials and Measures section).
2.4. Materials and Measures
As previously said, this study aims to explore the interrelatedness of social-structural aspects, as well as dispositional and trust-related, and vaccine-specific psychological features relevant for vaccination behavior, as well as their contribution to the intention to vaccinate one’s (future) child. For clarity, we have divided this section into five parts vis-a-vis measures’ conceptual grouping. All the instruments and variables used are given in full in Supplementary 2.
2.4.1. Social-structural aspects
Structural aspects pertain to one’s social role associated with vaccination facilitation - HPs, parents, and lay people. All groups defined by these social-structural aspects are decision-makers regarding vaccination; parents differ from others by their specific role as proxy decision-makers regarding vaccination of the child under their care, whereas HPs differ in their expert knowledge and thus a vital role of vaccination facilitation.
2.4.2. Psychological dispositions
These dispositions include relatively stable psychological features of a person that may contribute to the formulation and development of vaccination intentions. If not otherwise said, all continuous measurements below (including 2.3.3 section) were given on a 7-point Likert scale to make these constructs homogeneous and all scores are calculated as total averages.
Actively Open-Minded Thinking Scale (AOT) measures participants’ willingness to change their beliefs in the face of new information, and general open-minded attitude toward information and reflective belief maintenance thinking (Baron, 1993). We used a revised, short 8-item scale (Baron et al., 2015), where higher scores indicate an open-minded thinking while lower scores indicate more rigid, belief-preservation thinking.
Passive Risk-Taking Scale measures a tendency to passively engage in risks through inaction (Keinan & Bereby-Meyer, 2012). The adapted scale for the Serbian context we used consists of 19 items, where high scores indicate greater tendency toward risks by not taking some action and low scores indicate responsible low-risk behavior.
Epistemic Trust Mistrust and Credulity Questionnaire (ETMCQ) globally measures a person’s trust “in communication and communicated knowledge” which includes epistemic stances about the quality of information and its sources (Campbell et al., 2021). We used a short 15-item version of the scale which retains three separately scored subscales that refer to specific epistemic stances: Trust, Mistrust, and Credulity (5 items each). High scores indicate a tendency to be adequately open to information and learning (Trust), to be distrustful to any source of information thus tending to reject communicated knowledge (Mistrust), and to be undecided or unselective about the reliability and quality of information either way (Credulity) (Campbell et al., 2021).
2.4.3. Vaccine-specific factors
Vaccine-specific factors refer to other psychological features closely tied to- or crucial for vaccine decision-making more specifically realized through intention to vaccinate one’s (future) child.
Vaccine Attitudes Scale measures general positions on vaccines and vaccination behavior (Horne et al., 2015) consisting of 5-items. We coded the items such that higher scores denote negative attitudes toward vaccination, while lower scores indicate positive vaccination attitudes.
Vaccine Conspiracy Beliefs Scale, similarly to previous scale, measures negative attitudes toward vaccination, and more precisely a tendency to believe in negative vaccine-effects and attempts of various institutions (governments, pharmaceutical institutions, scientists) to hide such information (Shapiro et al., 2016). We used a short 6-item version of the scale where higher scores indicate conspiratorial beliefs about vaccines, while lower scores indicate the absence of such a tendency.
Experience of Freedom scale measures parents’ perceptions of freedom when deciding whether to vaccinate their child(ren) (Lau et al., 2015). The scale has 4 items where higher scores indicate greater feelings of freedom of choice, while lower scores indicate feelings of compulsion and lack of freedom in the vaccine decision-making process. Since this scale is intended for assessing parents’ perceptions regarding the vaccination of their children, it was only administered to parents’ sub-sample in its original form. We adapted the scale for sub-samples of lay people and HPs, as to ask them to assess “how they think parents feel while deciding whether to vaccinate their child(ren)”. Lay people and HPs also rated all items, but they were formulated as descriptive norms.
Choice overload scale measures parents’ feelings of informational pressure while making vaccination decisions for their children (Lau et al., 2015). The scale has 3 items where higher scores denote greater informational overload and lower scores indicate no choice overload. Note that, same as the previous scale, this is intended for parents’ assessments. In the same manner, we adapted the scale for lay people and HPs sub-samples to reflect their descriptive norms about the subject. Lay people and HPs thus assessed, for all items, “how they think parents feel while deciding whether to vaccinate their child(ren)”, while parents rated the scale in its original form.
Perceived Consensus and Norms About Vaccination scale measures perceived scientific consensus about vaccines, as well as vaccination norms in population. The scale consists of 3 items and is devised for this research, based on Van der Linden’s (Van Der Linden, 2011) work on vaccine consensus and norms. These items are scored as one average total score for consensus and one single-item variable for norms.
2.4.4. Trust-related measures
Trust related measures pertain to participants’ trust toward different authorities of knowledge on vaccines. Though these measures are in part vaccine-specific, they also pertain to the relationship of trust between participants and different epistemic authorities, whereas other measures we categorized as vaccine-related are based on one’s relationship or attitudes toward vaccines specifically and their experience in vaccine decision making. Since measures of trust are based on participants-authority relationships also shaped by attitudes toward such authorities independent of one’s beliefs about vaccines, we separated these measures as its own category.
Trust Toward Authorities (Jolley & Douglas, 2014) scale measures trust participants’ have in communicated vaccine-knowledge that comes from various sources of authority (corporations, national government, healthcare system, scientists, mainstream media, alternative media, social networks, and their child’s doctor (for parents) or their doctors (for lay people and HPs)). For every authority source, participants’ rate their trust on a 7-point Likert scale (1 - strongly mistrust; 7 - strongly trust) and items are separately scored as eight single-item variables.
2.4.5. Vaccination intention
Vaccination intention refers to the intention to vaccinate one’s (future) child and is used as a dependent/criterion variable in this research. It is a single-item variable (i.e., “Would you at this time vaccinate your child according to the official vaccination schedule”) expressed on a 7-point Likert scale (1 - definitively not; 7 - definitively yes); higher scores thus reflecting a greater vaccination intent. For lay people and HPs, a formulation “regardless of if you are a parent or not” was added, based on Stojkovic et al.’s (2017) research.
2.5. Data analysis
As stated, our general aim is to examine key psychological and vaccine-related factors of vaccination intention, as well as their interconnectedness, in each of the three groups based on their socio-structural roles in vaccine facilitation (HPs, parents, lay people). Vaccination decisions are inherently high-involvement, social decisions, at least for parents and other lay people (Damnjanović et al., 2018b, 2019; Goldenberg, 2014), whose concerns and questions often go unnoticed and unanswered thus leading to the under-coverage of vaccine-preventable diseases. Because of this, our specific interest is in vaccine attitudes that negatively influence vaccination intention and other psychological dispositions, trust-related, and vaccine-specific factors that moderate such relationships. To better formulate this negative influence on vaccination intent - which presumably leads to vaccination under-coverage - we focused on negative vaccination attitudes (see 2.4.3. section) as predictors of vaccination intent, and tried to map out moderators of such a relationship - specifically promotive, protective, vulnerability, and risk factors of vaccination intention across all three sub-samples. To achieve this, a series of hierarchical regression analyses were conducted, with negative vaccination attitudes as predictor, vaccination intent as criterion, and other psychological, trust-related, and vaccine-specific factors as moderator variables. All variables have been centered prior to creating a product between predictor and moderator variables. The first block of hierarchical regression analysis involved the inclusion of the predictor and moderator variables’ centered values in the model. Subsequently, in the second block, the interaction between these variables was added.
Due to the extensive number of conducted analyses, the findings were categorized based on the observed main and interaction effects, as follows:
Risk factors refer to moderating variables that negatively affect vaccination intention (main effect);
Promotive factors refer to moderating variables yielding positive effects on vaccination intention (main effect);
Vulnerability factors refer to moderating variables that strengthen the negative relationship between negative attitudes towards vaccination and vaccination intention (interacting effect);
Protective factors refer to moderating variables that weaken the negative association between negative attitudes towards vaccination and vaccination intention (interacting effect).
3. Results
3.1. Descriptive statistics
Descriptive statistics, as well as reliability indicators, indicate that we can use the data obtained on these scales in planned statistical analyses. All variables range from 1 to 7. Observed average values for most variables are around the theoretical average, while for some variables, the observed average values are above (e.g., vaccination intention, trust in scientists and health-care system, actively open-minded thinking and subjective norms) or below (e.g., negative vaccine attitudes, conspiracy beliefs, epistemic credulity, trust in corporations, mainstream media, and social networks) the theoretical average. The values of the distributions (a)symmetry (skewness) and tailedness (kurtosis) indicate, however, moderate to high deviations from the normal distribution for most variables in all three samples, except for the passive risk taking, epistemic mistrust, and trust toward government and independent media (in all three samples), as well as epistemic trust, experience of freedom and choice overload for HPs and lay people sub-samples. Negative asymmetry of AOT, vaccination intention, perceived consensus, subjective norms, and trust towards health-care system and scientists, is observable in all three samples. Meaning that, interestingly, our participants, regardless of the socio-structural roles, are open to new information, have high intention to vaccinate, perceive there is a scientific consensus on vaccine efficiency and safety, and have high trust in the healthcare system and scientist when in it comes to the knowledge of vaccination they communicate. Positive asymmetry in all three samples is seen in cases of epistemic credulity, negative vaccine attitudes, vaccination conspiracy beliefs, and trust in corporations, mainstream media, and social networks. Our participants are selective with information they adopt, have mostly positive attitudes and are not conspiratorial toward vaccines, and have little trust in corporations and mainstream and social media when it comes to them being sources of vaccination information. Additionally, specific to parents is negative asymmetry of epistemic trust and experience of freedom, as well as positive asymmetry of choice overload, meaning they are appropriately open (in an epistemic sense) to new information, and feel both free and not informationally burdened when deciding about vaccination. Detailed descriptive statistics (means, standard deviations, skewness, and kurtosis) for all measures broken down by health providers/parents/lay people sub-samples are shown in Supplementary material 1, Table S3 while internal metric characteristics for all scales are given in Table S4.
3.2. Do psychological dispositions moderate the relationships between negative attitudes toward immunization and vaccination intention?
A series of separate hierarchical regression analyzes were conducted to test the moderating role of psychological dispositions (passive risk-taking, AOT, epistemic trust, epistemic mistrust, and epistemic credulity) in the relationship between negative attitudes toward vaccination and vaccination intention on three sub-samples (HPs, parents, and lay people) (Table 1). In all analyses, negative attitudes towards vaccination have moderate to strong negative effects on vaccination intention (all βs ranging from -.531 to -.849, all ps < .01). None of the above-mentioned psychological dispositions have significant main effects on vaccination intentions. The negative relationship between negative attitudes towards vaccination and vaccination intention is stronger in conditions of high scores on passive risk-taking in a sub-sample of health professionals (β = -.115, p < .05). Similarly, the association between negative attitudes and vaccination intention is stronger under conditions of high scores on epistemic credulity in the parents’ sub-sample (β = -.079, p < .05). On the other hand, actively open-minded thinking weakens the association between negative attitudes towards vaccination and vaccination intention in the lay people sub-sample (β = .187, p < .01). However, in addition to the fact that 12 of the 15 examined interacting effects are not statistically significant, it should be highlighted that the effect sizes for the three statistically significant interactive effects are small.
Based on the classification described above, we conclude that:
- passive risk-taking is a vulnerability factor in the relationship between negative attitudes and vaccination intention in a sub-sample of health professionals;
- epistemic credulity is a vulnerability factor in the relationship between negative attitudes and vaccination intention in the parents sub-sample;
- open-minded thinking is a protective factor in the relationship between negative attitudes and vaccination intention in the lay people sub-sample.
3.3. Do vaccine-specific factors moderate the relationships between negative attitudes toward immunization and vaccination intention?
A series of separate hierarchical regression analyzes were conducted to test the moderating role of vaccine-specific factors (experience of freedom, choice overload, perceived consensus, subjective norms, and conspiracy beliefs) in the relationship between negative attitudes toward vaccination and vaccination intention on all three samples (Table 2). All tested models are statistically significant, explaining between 31.4% and 76.6% of the variance in vaccination intention. In all conducted analyses negative attitudes towards vaccination have significant but varying negative effects on vaccination intention (all βs ranging from -.128 to -.983, all ps < .01). Conspiracy beliefs achieves statistically significant negative main effects on vaccination intention in all three samples. In the HPs sub-sample (β = .167, p < .01), experience of freedom shows a positive correlation with vaccination intention. In addition to the previous, the main effect of perceived consensus on vaccination intention is registered in the parents’ sub-sample (β = .100, p < .05).
Based on the classification described above, we can conclude that:
- conspiracy beliefs are risk factors in all three sub-samples;
- experience of freedom is a promotive factor in the sub-sample of health professionals;
- perceived consensus is a promotive factor in a parents’ sub-sample.
Regarding interacting effects, the association between negative attitudes and vaccination intention is stronger in conditions of high conspiracy beliefs and choice overload, and weaker in conditions of high perceived consensus and experience of freedom in all three sub-samples.
Based on the classification described above, we can conclude that:
- conspiracy beliefs and choice overload are vulnerability factors in the relationship between negative attitudes and vaccination intention in all three sub-samples;
- perceived consensus and experience of freedom are a protective factor in the relationship between negative attitudes and vaccination intention in all three sub-samples;
3.4. Do trust-related measures moderate the relationships between negative attitudes toward immunization and vaccination intention??
A series of separate hierarchical regression analyzes were conducted to test the moderating role of trust-related measures (trust in corporations, government, health-care system, scientists, mainstream media, independent media, and social networks) in the relationship between negative attitudes toward vaccination and vaccination intention on all three subsamples (Table 4). All tested models are statistically significant, explaining between 32.4% and 73.8% of the variance in vaccination intention. In all conducted analyses, negative attitudes towards vaccination have significant, but varying, negative effects on vaccination intention (all βs ranging from -.184 to -.853, all ps < .01). In the parents’ sub-sample, trust in corporations (β = .149, p < .01) and trust in the health-care system (β = .172, p < .01) have statistically significant positive main effects on vaccination intention. Trust in social networks (β = -.086, p < .05), on the other hand, had statistically significant negative main effects on vaccination intention in a sample of lay people.
Based on the classification described above, we can conclude that:
- trust in corporations and trust in health-care system are promotive factors in the parents’ sub-sample;
- trust in social networks is a risk factor in the sub-sample of lay people.
In terms of interacting effects, the association between negative attitudes and vaccination intention is weaker in conditions of high scores on trust in corporations, government, and health-care systems in all three sub-samples. Similarly, in conditions of high trust in scientists, the relationship between negative attitudes and vaccination intention is weaker in the sub-samples of HPs and lay people, but not in the sub-sample of parents. In conditions of high trust in mainstream and independent media the negative relationship between attitudes and intention is also weaker but only on a sample of health providers. On the other hand, in conditions of high trust in social networks, the negative association between negative attitudes and vaccination intention is stronger in all three sub-samples.
Based on the classification described above, we can conclude that:
- trust in corporations, government, and health-care system are a protective factors in the relationship between negative attitudes and vaccination intention in all three sub-samples;
- trust in scientists is a protective factor in the relationship between negative attitudes and vaccination intention in sub-samples of HPs and lay people;
- trust in mainstream and independent media is a protective factor in the relationship between negative attitudes and vaccination intention in sub-samples of health providers;
- trust in social networks is a vulnerability factor in the relationship between negative attitudes and vaccination intention in all three sub-samples.

Table 3.
Trust-related measures as moderators in the relationships between negative attitudes toward immunization and vaccination intention.
Table 3.
Trust-related measures as moderators in the relationships between negative attitudes toward immunization and vaccination intention.
| Moderator (always TA) | Health providers | Parents | Lay people | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| B | S.E | Β | B | S.E | Β | B | S.E | β | |||
| TA: corporations | R = .608**, ΔR2 = .062** | R = .799**, ΔR2 = .024** | R = .846**, ΔR2 = .021** | ||||||||
| Negative attitudes | -.482 | .101 | -.339** | -1.181 | .090 | -.667** | -1.106 | .068 | -.702** | ||
| TA: corporations | .159 | .082 | .111 | .283 | .080 | .149** | .076 | .055 | .052 | ||
| Interaction | .468 | .101 | .317** | .393 | .095 | .133** | .286 | .065 | .193** | ||
| TA: government | R = .619**, ΔR2 = .078** | R = .791**, ΔR2 = .015** | R = .852**, ΔR2 = .029** | ||||||||
| Negative attitudes | -.451 | .103 | -.317** | -1.204 | .100 | -.649** | -.892 | .077 | -.616** | ||
| TA: government | .110 | .083 | .077 | .204 | .083 | .110 | .133 | .055 | .092 | ||
| Interaction | .438 | .084 | .351** | .321 | .099 | .164** | .323 | .062 | .251** | ||
| TA: health-care system | R = .665**, ΔR2 = .117** | R = .813**, ΔR2 = .037** | R = .859**, ΔR2 = .038** | ||||||||
| Negative attitudes | -.261 | .104 | -.184* | -.882 | .114 | -.475** | -.792 | .082 | -.547** | ||
| TA: health-care system | .090 | .089 | .064 | .319 | .090 | .172** | .106 | .064 | .073 | ||
| Interaction | .390 | .058 | .486** | .377 | .070 | .273** | .271 | .044 | .306** | ||
| TA: scientists | R = .625**, ΔR2 = .070** | R = .786**, ΔR2 = .004 | R = .839**, ΔR2 = .007* | ||||||||
| Negative attitudes | -.520 | .095 | -.366** | -1.281 | .101 | -.690** | -1.112 | .067 | -.768** | ||
| TA: scientists | -.079 | .107 | -.055 | .101 | .099 | .054 | -.038 | .078 | -.027 | ||
| Interaction | .316 | .064 | .382** | .108 | .064 | .088 | .118 | .047 | .132* | ||
| TA: mainstream media | R = .576**, ΔR2 = .024** | R = .781**, ΔR2 = .000 | R = .838**, ΔR2 = .004 | ||||||||
| Negative attitudes | -.707 | .084 | -.497** | -1.428 | .083 | -.769** | -1.160 | .064 | -.801** | ||
| TA: mainstream media | .084 | .080 | .059 | .058 | .081 | .031 | -.050 | .053 | -.035 | ||
| Interaction | .246 | .088 | .165** | .031 | .103 | .014 | .118 | .064 | .078 | ||
| TA: independent media | R = .569**, ΔR2 = .017* | R = .780**, ΔR2 = .000 | R = .836**, ΔR2 = .000 | ||||||||
| Negative attitudes | -.783 | .080 | -.551** | -1.453 | .074 | -.783** | -1.235 | .055 | -.853** | ||
| TA: independent media | .060 | .080 | .042 | -.016 | .073 | -.009 | -.085 | .052 | -.059 | ||
| Interaction | .184 | .080 | .129* | -.011 | .072 | -.006 | -.004 | .043 | -.003 | ||
| TA: social networks | R = .586**, ΔR2 = .027** | R = .793**, ΔR2 = .011** | R = .848**, ΔR2 = .013** | ||||||||
| Negative attitudes | -.683 | .084 | -.481** | -1.357 | .073 | -.741** | -1.185 | .048 | -.819** | ||
| TA: social networks | -.139 | .079 | -.098 | -.153 | .071 | -.082 | -.124 | .049 | -.086* | ||
| Interaction | -.216 | .073 | -.274** | -.167 | .059 | -.110** | -.144 | .041 | -.116** | ||
4. Discussion
4.1. General findings
The main goal of the present study was to investigate the interplay between social roles regarding vaccination and the role of psychological dispositions, both vaccine-specific factors and trust-related measures, in the relationship between negative attitudes toward vaccination and vaccination intention. According to different theoretical models constituting the Integrated Behavioral Model (IBM) core, attitudes toward certain health behaviors are the strongest predictors of behavioral intention (Chaulagain et al., 2021). However, less is known about which intrapersonal, interpersonal, and social factors may change the strength of this relationship. Though previous findings indicate the possibility of differences in vaccination attitudes of healthcare providers, parents, and laypeople (Bedford, 2014; Gowda & Dempsey, 2013; Opel et al., 2013; Rosental & Shmueli, 2021; Stöcker et al., 2023) these social roles have not, to our knowledge, been directly compared and analyzed. Regarding different health behaviors, the above is critical to raise as a study question since some external features might minimize the association between (negative) attitudes and behavioral intention and contribute to the strengthening of such relationship. Examining protective and promotive factors in the context of vaccination intention is critical in building a knowledge basis for developing evidence-based promotional campaigns to boost vaccination coverage. By the same token, mapping out various risk and vulnerability factors that influence vaccination intention and straighten its relationship with negative vaccination attitudes is needed to devise policies that will address, and answer lay people’s concerns about vaccination, and may, in turn, promote positive vaccination behaviors.
To provide a more comprehensive picture of which personal, situational, and social factors strengthen or weaken the negative relationship between negative attitudes and vaccination intention, we added many psychological dispositions, vaccine-specific factors, and trust-related measures into the model. In addition, we looked at promotive, protective, risk, and vulnerability factors in three relevant sub-samples in this context: healthcare providers, parents, and lay people. The main findings of this study were that different factors contribute in the same way to the understanding of vaccination intention in all three sub-samples, but that there are some differences between them, i.e., different variables play different, sometimes opposing roles in understanding vaccination intention in different sub-samples.
4.2. Similarities between parents, healthcare providers, and laypeople
The findings of our study indicate that conspiracy beliefs play a significant role as both risk and vulnerability factors in explaining vaccination intention across all three sub-samples. This result is in line with individual findings of recent studies according to which people’s beliefs in conspiracy theories regarding vaccination are related to negative attitudes and lower intentions to be vaccinated (Allington et al., 2021; Bertin et al., 2020; Seddig et al., 2022; Teovanović et al., 2021). For example, Hornsey et al. found that people with the highest levels of conspiracy beliefs had the strongest anti-vaccination attitudes (Hornsey et al., 2018), while Jolley and Douglas (2014) showed that believing in anti-vaccine conspiracy theories causes low vaccination intentions. So, these findings suggest that the presence of conspiracy beliefs not only contributes to a decrease in overall vaccination intention but also strengthens the negative relationship between negative attitudes towards vaccination and vaccination intention.
Next, choice overload proved to be a vulnerability factor, meaning that if present, it strengthens the relationship between negative attitudes and vaccination intention. This is in line with findings that show that having several options can cause a delay in making the decision to vaccinate. Worrying about making a "bad" choice and the perception that there are better and worse options requires extra time and effort to make an informed selection among accessible alternatives (Iyengar & Lepper, 2000).
In addition to the foregoing, our results revealed that trust in social networks acts as a common vulnerability factor in the relationship between vaccination attitudes and intention. This is hardly unexpected given that most vaccination conspiracy ideas as well as anti-vaccination propaganda are disseminated through these channels of communication (Lep et al., 2021; Shahsavari et al., 2020). Conversely, trust in more controlled sources of information i.e., government, health-care system, and corporations, serves as a protective factor, and in a similar vein, the perception that there is a vaccination consensus among scientists plays a protective role in the relationship between negative attitudes and vaccination intention. These results are consistent with earlier studies, which show that communicating scientific consensus leads to attitudes and behavioral intentions becoming more aligned with those norms (Ruggeri et al., 2022). According to the findings of Bartoš et al. (2022), public communication of medical consensus on the efficacy and safety of COVID-19 vaccination contributed to an increase in vaccine uptake over the next 9 months. Similarly, the level of trust in institutions responsible for disseminating information regarding vaccination has a significant role in mitigating the influence of negative attitudes on behavioral intentions. Institutional trust is related to the perceived credibility of institutions and acceptance of formal and informal norms (Bartoš et al., 2022; Cheung & Tse, 2008; De Visser et al., 2011; Khodyakov, 2007; Oraby et al., 2014; Ruggeri et al., 2022). So, people who trust their institutions are more likely to think that official information about the safety and efficacy of vaccines is true, which can protect them from the consequences of negative attitudes toward vaccination (Seddig et al., 2022).
Finally, the experience of freedom emerged as another protective factor. Namely, regardless of the social role relative to vaccination, participants who perceive themselves, or in the case of HPs and lay people perceive parents in general, as having the ability to make a free choice, review and think clearly, and not under constraints of limited choice, have their decision to vaccinate less influenced by their negative attitudes towards vaccination. This finding points to the importance of incorporating the deliberative model of the physician-patient relationship in practice, which is not the case in Serbia where the current model of this relationship de facto takes the form of a paternalistic one (Ninković et al., 2022). Any medical decision, including the one regarding childhood vaccination, should be informed and not pressured (Iyengar & Lepper, 2000), and such a setting can apparently mitigate the negative effects of previously existing negatively valenced attitudes regarding vaccination.
Figure 2.
Functions of vaccine-related and trust-related psychological aspects in shaping vaccination intention.
Figure 2.
Functions of vaccine-related and trust-related psychological aspects in shaping vaccination intention.
4.3. Differences between parents, healthcare providers, and laypeople
It is important to highlight there are no common promotive factors (factors directly influencing) for vaccination intention across samples.
For parents, greater perception of vaccination scientific consensus, and greater trust in large corporations and the health-care system are unique promotive factors for vaccination intention. Though publicly communicated medical knowledge and consensus on vaccines weakens the negative relationship between negative vaccine attitudes and vaccination intention for HPs, parents, and lay people alike, and is shown to be an important factor for more positive behavioral intentions about vaccines in other research as well (Bartoš et al., 2022; Ruggeri et al., 2022) it seems to have a much greater role in the case of parents. For them, such a consensus has a direct positive influence on their behavioral vaccination intentions and plays a protective role in the influence of negative vaccine attitudes on such intentions. Additionally, their trust in institutions, specifically corporations and healthcare systems, leads to acceptance of vaccination norms those institutions prescribe, e.g., intention to vaccinate, which is corroborated in previous research as well (Khodyakov, 2007). Specific to parents is also the role of epistemic credulity as a vulnerability factor - the only role credulity had in the present study. Epistemic credulity is shown to be negatively associated with both willingness to vaccinate and confidence in the safety of COVID-19 vaccines, as well as with greater difficulty in discerning false from real information (Campbell et al., 2021). Given that, parents may be a specifically vulnerable group regarding information hesitancy precisely because they are their children’s decision-makers, a role with enormous health- and social- responsibilities. Their decision-making process could be relieved with more structured public communication about medical/scientific stances and knowledge of vaccines.
For lay people a unique protective factor in the relationship between negative vaccine attitudes and vaccination intention is greater open-minded thinking, whereas a unique risk factor is a trust in social media. Since AOT is positively associated with (positive) vaccine attitudes and vaccination intention, and negatively associated with COVID-19 misperceptions about vaccines (e.g., Newton et al., 2023), it is interesting that similar results are obtained only for laypeople in our study. HPs’ and parents’ vaccination behavior and attitudes may be primarily shaped by other factors, such as expert knowledge (HPs) or concerns regarding one’s key role as a child’s decision-makers (parents) that can only be mitigated through institutional sources and authorities such as healthcare system and scientific community, while specific thinking styles become more important with people who do not share HPs’ or parents’ social roles. Similarly, the unique role of social media as a risk factor that negatively affects vaccination intention in lay people, although small, and a vulnerability factor for all sub-samples, may reflect their greater reliance on such sources of information, which are shown to have unclear communication about medical information as well as a greater dissemination of conspiratorial narratives (Enea et al., 2023; Jolley & Douglas, 2014; Shahsavari et al., 2020).
Finally, for healthcare providers, passive risk-taking has been singled out as a unique vulnerability factor, while the experience of freedom is a unique promotive factor. Additionally, trust in both mainstream and independent media represents a unique protective factor in the relationship between negative attitudes and vaccination intention, which will be further discussed in section 4.4. while we here focus on the former two factors. It is expected that passive risk-taking would be associated with bad health practices since these behaviors represent a facet of passive risk examples (Keinan & Bereby-Meyer, 2012). However, it is seemingly unexpected that passive risk-taking would be demonstrated as a vulnerability factor only in HPs sub-sample, having no effects in parents’ and lay people’s sub-samples. As passive risk-taking primarily refers to risks taken through inaction in mostly everyday practices, these results reflect previously discussed differences between HPs’ and lay people’s conceptualizations of vaccines. While for HPs vaccination represents a routine procedure supported by their expert knowledge, for lay people and specifically for parents this is a high-involvement, health-related, and social decision not supported by their professional knowledge. The “risks” lay people take by deciding (not) to vaccinate themselves or others are actively taken risks; actions and judgments that do not constitute their every day, but rather extraordinary circumstances. From this perspective, it is reasonable that passive risk-taking behavior will influence the relationship between attitudes and behavioral intention in cases where such a behavioral intention is a common practice. It would be interesting to further examine differences in vaccination conceptualization between HPs and lay people using both active and passive risk-taking measures - we hypothesize vulnerability factors would differ based on the “activity level” of behavioral intention.
Interestingly, the experience of freedom emerged as a unique promotive factor for HPs, in addition to its common protective role in all sub-samples. It should be again noted that the experience of freedom regarding vaccination of one’s child for HPs and lay people represents a descriptive assessment of how parents feel. At first it seems unconventional that HPs evaluations of parents’ experience of freedom in decision-making about vaccines would have a direct positive influence on their intention to vaccinate their own (hypothetical) child. However, this again illustrates differences in HPs and parents’ perspectives on medical systems, immunization, and its goals, as well as a gap in understanding the needs and positions between parents and HPs decision-makers with their own unique socio-structural roles in immunization. For parents, feelings of freedom when making an involving health decision about one’s child, could mitigate known negative influences of worries, stress, and epistemic overload on vaccination behavior (e.g. Iyengar & Lepper, 2000) and thus be a protective factor in negative attitudinal influences on their vaccination intention. In a way, the experience of freedom reflects parents’ concerns and needs regarding such important medical decisions being met. But what does the experience of freedom of parents mean for HPs? Given the traditional paternalistic medical models still represented in most healthcare systems in the world, but specifically in the country of the present study (Ninković et al., 2022), “too much freedom” may signify to physicians, in such a paternalistic model, that patients might ignore their medical advice. In other words, in cases of lack of medical expertise knowledge, fewer choices lead to better choices. HPs needs are shaped by- and consistent with medical practices and goals - in this case, a proper vaccine coverage of the population. If parents/patients’ freedom signifies “medical disobedience” from HPs framework of institutionalized medical care (Stankovic, 2017), it may prompt HPs’ intention to vaccinate their own children as a response to their predictions of suboptimal vaccination reach in the population, to both protect their own child and achieve herd immunity. It seems there is fear of wrong choices and a lack of understanding on both sides of the patient-physician relationship. The solution for a better-functioning healthcare system lies in the true adoption of deliberative medical models which foster active patient-physician communication about diagnoses, and their possible and alternative treatment directions (Ninković et al., 2022). Patients actively involved in their health are more informed, educated patients who better understand their bodies and mechanisms of possible treatments thus making better health decisions. In this way, deliberative models answer the needs of both patients and physicians, leading to lasting positive health outcomes.
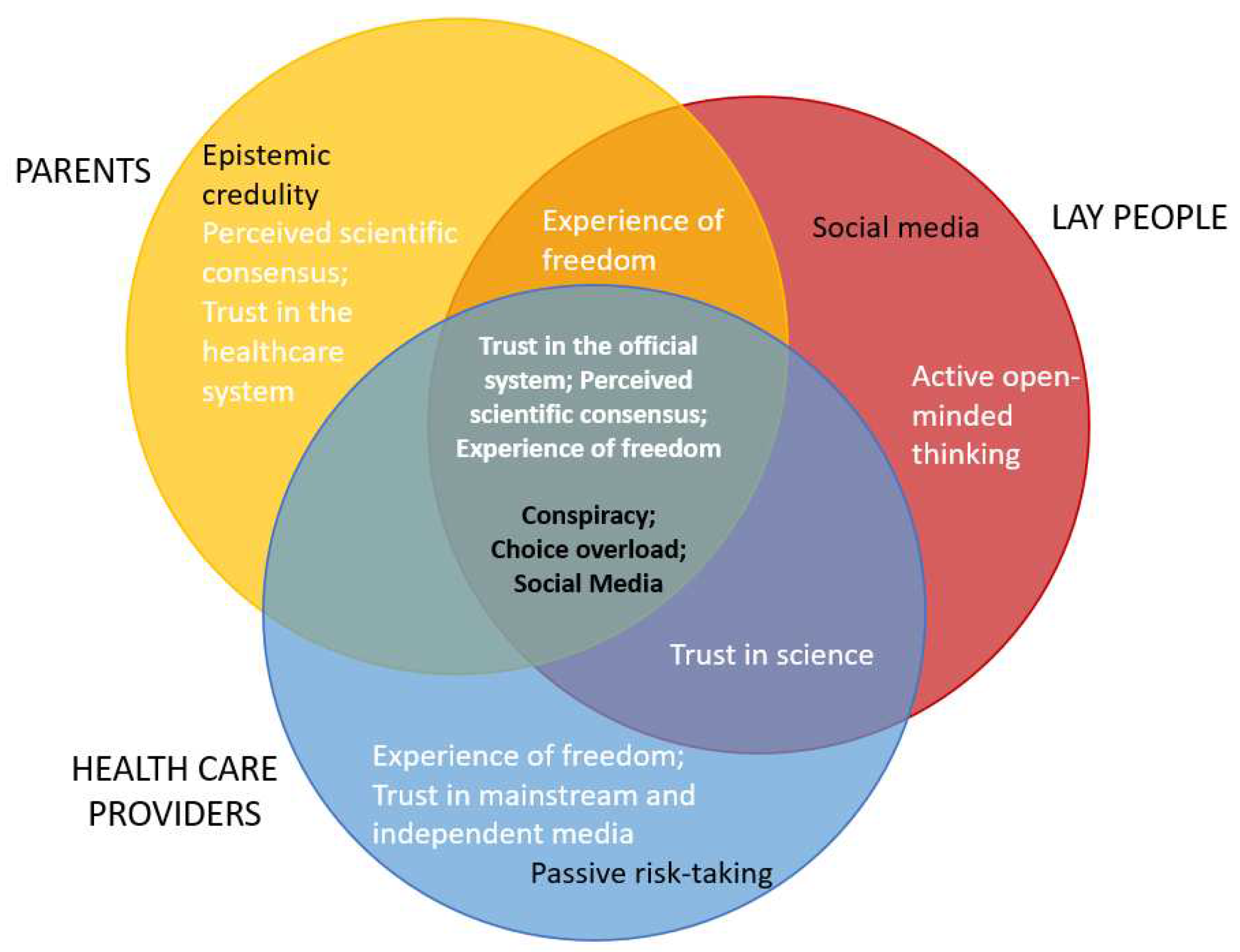
Figure 3.
Schematic overview of common and unique protective/promotive (white letters) and risk/vulnerable (black letters) factors in three subsamples.
Figure 3.
Schematic overview of common and unique protective/promotive (white letters) and risk/vulnerable (black letters) factors in three subsamples.
4.4. Moderating and direct effects of trust in different sources of information across three samples
The role of trust in vaccination intention varied based on the object of trust,. i.e. specific institutions, across samples. Trust in government, healthcare systems, and large corporations regarding vaccine information served as a protective factor across all samples, while the latter two were also promotive factors for parents’ sample. Similarly, trust in scientists was a protective factor for the negative influence of attitudes on vaccine intention for HPs and lay people, but interestingly had no effects when it came to parents. On the other hand, trust in social networks was a vulnerability factor of such a relationship for all three samples, while it was additionally a risk factor for lay people thus exerting a direct negative influence on their intention to vaccinate. First, more “traditional” sources of expert knowledge of public interest, such as governments, corporations, healthcare systems, and scientists, have a vital and positive role in shaping vaccination intention, while different social networks influence such intention negatively. As previously said, this is expected given the less clear and structured manner of information dissemination when it comes to social media sources, which can delay or hinder positive health behavior, as well as spread conspiracy beliefs and misinformation about vaccines (e.g. Enea et al., 2023; Lazić & Zezelj, 2021; Shahsavari et al., 2020). However, our results also show that mainstream and independent media take on a protective role, and only in the sample of HPs. This finding is surprising since in Serbia, these mediums of information dissemination are not consistent in choice of information, nor mostly expert-oriented, and are often sensationalist and prone to spreading misinformation. However, it is possible that healthcare providers, whose opinions are, by their very vocation, shaped by official expert and scientific influences, can discern between misinformation and facts in such media. Thus, factual information regardless of its source might positively influence the relationship between negative attitudes and intention to vaccinate in this sub-sample. In favor of this interpretation is the finding that exposure to health-related information in mainstream media positively influences vaccination intention in other cultural contexts (Lin & Lagoe, 2013). However, this hypothesis should be tested in further research considering social roles relative to vaccination intention.
However, here, we have a hopeful way out - institutions with a positive impact on behavioral intentions regarding vaccines, and an opportunity for the cooperation of the media with such institutions. This, of course, is not a one-way street. As we can see, scientists exert no influence on parents’ vaccination decisions; and the exclusion of scientific, expert perspectives on problems of public interest leaves many doors open for misinformation and distrust. The cure seems obvious - greater visibility and epistemic accessibility of scientific, evidence-based communication in public and media spheres (Kahan, 2013). However, such evidence-based communication practices often rely on continuous repetition of evidence and, in practice, prove to be unproductive (Larson et al., 2013). Hence, “attitude roots models” of countering anti-vaccination sentiments start to arise. The basic idea of these models is founded on mapping psychological differences and other characteristics that influence vaccination intention, which are not directly related to a specific belief about vaccines. From this, further interventions and communication strategies are tailored to respond to those underlying psychological needs and not to counter un unspecified, the general public base of knowledge about a subject (Larson et al., 2013). If scientific communication can respond to and fulfill those needs, it should mitigate concerns about vaccines and foster trust in scientific and public knowledge.
4.5. Limitations and future directions
Although this study is an important step forward in understanding vaccination intention, several limitations should be noted. First, none of the three sub-samples are statistically representative of the population they belong to, which limits the generalization of our findings. In addition, we used a cross-sectional design, which limits us in causal inference when it comes to the various relationships tested in the previously discussed models. Also, our data are restricted to a single country, and cross-cultural data is needed to evaluate the role of psychological dispositions, vaccine-specific factors, and trust-related measures in understanding vaccination intention in different cultures and sub-samples. Overall, future studies tackling the factors of influence on vaccination intention in populations that differ by social roles relative to vaccination should aim for more representative samples, in multiple cultural contexts, and countries, and should include more participants who in some regard oppose adult vaccination (e.g., vaccination against COVID-19). Further, a longitudinal or repeated measures design would enable the assessment of changes in attitudes due to changes in the overall climate regarding immunization among adults that manifest as the reactive-preventive pattern. Another possible research direction includes measurements of reasoning-related cognitive constructs, such as omission, hindsight, or outcome bias. This would enable insight into the characteristics of the decision-making processes regarding immunization. Further, investigating intricacies of vaccination intention should also include contextual data, e.g., exposure to anecdotal cases about vaccine (side)effects or personal experience with vaccines, and some other dispositional constructs such as elaboration of possible outcomes (positive, negative, etc.), overall tendency for preventive behaviors, active risk taking, agreeableness, as well as sociodemographic variables that could be potential moderators of vaccine intention.
5. Conclusions
It is of immense importance to map psychological differences and similarities in groups that differ by social role relative to vaccination, especially in the light of sustainable positive discourse regarding vaccination, and with the aim of consensual and shared decision-making. The aim of the present study was thus, to investigate the interplay between social roles regarding vaccination and the role of psychological, vaccine-specific, and trust-related dispositions in the relationship between negative attitudes toward vaccination and vaccination intention. In other words, we identified factors that have a direct influence on vaccination intention i.e., promotive and risk factors, as well as factors that skew the relationship between vaccination attitudes and intention to vaccinate, that serve as protective and vulnerability factors. Our findings provide insights into the differences between social roles regarding immunization relative to these factors and their different roles. Namely, what differentiates parents from the remaining two samples is the moderating role that epistemic credulity - undecidedness about the reliability and quality of information they are exposed to, has on the relationship between attitudes and vaccination intention. Additionally, perceived scientific consensus on vaccines, as well as trust in corporations and the healthcare system are unique promotive factors for parents. For lay people, the differentiating protective factor is the propensity to revise beliefs due to new information, while their unique risk factor is found to be trust in social media. Finally, HPs unique vulnerability factor was the propensity for passive risk-taking, predominantly by inaction and unique promotive and protective factors were the experience of freedom, and trust in mainstream and independent media, respectively. Further, and equally important, the results of the present paper indicate that regardless of the social role, a shared attitudinal core for a positive stance regarding vaccines comprises high trust in the health-care system, government, and corporations, high perceived scientific consensus, high experience of freedom, low choice overload, low conspiracy-beliefs, and low trust in social networks as a source of information. Considering this data, communication strategies to improve vaccination uptake aimed at all groups should instigate low choice overload via clear and structured dissemination of information, reflect high scientific consensus, be consistent, and be conveyed via both official expert channels of communication and social networks and independent media. Although this seems trivial, not all national and cultural contexts reflect these aims in practice. Moreover, due to differences in factors that shape vaccination intentions among people taking on different social roles, a custom-made approach should be devised to both mitigate the specific risk or vulnerability factors and make use of protective and promotive factors registered in these different groups.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, D.K., I.S., K.M., L.M.; and D.P; methodology, D.K., I.S., K.M., and L.M.; formal analysis, D.K., I.S., K.M., and L.M; investigation, D.K., I.S., K.M., and L.M.; data curation, D.K., I.S., K.M., and L.M.; writing—original draft preparation, D.K., I.S., K.M., and L.M.; writing—review and editing, D.K., I.S., K.M., and L.M.; visualization, D.K., I.S., K.M., and L.M.; supervision, D.K.; project administration, D.K.; funding acquisition, D.K., and D.P. The contributions were listed according to the Contributor Roles Taxonomy (CRediT). All authors have read and agreed to the published version of the manuscript.
Funding
Supported in part (APC incl.) by a research grant from Investigator-Initiated Studies Program of Merck Sharpe & Dohme doo. The opinions expressed in this paper are those of the authors and do not necessarily represent those of Merck, Sharpe & Dohme doo.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Department of Psychology, Faculty of Philosophy, University of Belgrade (protocol code: #2022-64; date: 28.09.2022).” for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are openly available in Researchbox.org at https://researchbox.org/2030&PEER_REVIEW_passcode=WJWCBK , reference number Box #2030.
Acknowledgments
Žan Lep: Johanna Graeber, Wing Y. Lam, Sara Morales, Tero Pulkkinen, and Loes Vingerhoets.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. [CrossRef]
- Allington, D., Duffy, B., Wessely, S., Dhavan, N., & Rubin, J. (2021). Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency – CORRIGENDUM. Psychological Medicine, 51(10), 1770–1770. [CrossRef]
- Arnesen, S., Bærøe, K., Cappelen, C., & Carlsen, B. (2018). Could information about herd immunity help us achieve herd immunity? Evidence from a population representative survey experiment. Scandinavian Journal of Public Health. [CrossRef]
- Bangerter, A., Krings, F., Mouton, A., Gilles, I., Green, E. G. T., & Clémence, A. (2012). Longitudinal investigation of public trust in institutions relative to the 2009 H1N1 pandemic in Switzerland. PloS One, 7(11), e49806. [CrossRef]
- Baron, J. (1993). Why Teach Thinking?-An Essay. Applied Psychology, 42(3), 191–214. [CrossRef]
- Baron, J., Scott, S., Fincher, K., & Emlen Metz, S. (2015). Why does the Cognitive Reflection Test (sometimes) predict utilitarian moral judgment (and other things)? Journal of Applied Research in Memory and Cognition, 4(3), 265–284. [CrossRef]
- Bartoš, V., Bauer, M., Cahlíková, J., & Chytilová, J. (2022). C ommunicating doctors’ consensus persistently increases COVID-19 vaccinations. Nature, 606(7914), Article 7914. [CrossRef]
- Bavel, J. J. V., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., Crockett, M. J., Crum, A. J., Douglas, K. M., Druckman, J. N., Drury, J., Dube, O., Ellemers, N., Finkel, E. J., Fowler, J. H., Gelfand, M., Han, S., Haslam, S. A., Jetten, J., … Willer, R. (2020). Using social and behavioural science to support COVID-19 pandemic response. Nature Human Behaviour, 4(5), 460–471. [CrossRef]
- Bedford, H. (2014). Pro-vaccine messages may be counterproductive among vaccine-hesitant parents. BMJ Evidence-Based Medicine, 19(6), 219–219. [CrossRef]
- Bertin, P., Nera, K., & Delouvée, S. (2020). Conspiracy Beliefs, Rejection of Vaccination, and Support for hydroxychloroquine: A Conceptual Replication-Extension in the COVID-19 Pandemic Context. Frontiers in Psychology, 11. https://www.frontiersin.org/articles/10.3389/fpsyg.2020.565128.
- Camargo, K., & Grant, R. (2015). Public Health, Science, and Policy Debate: Being Right Is Not Enough. American Journal of Public Health, 105(2), 232–235. [CrossRef]
- Campbell, C., Tanzer, M., Saunders, R., Booker, T., Allison, E., Li, E., O’Dowda, C., Luyten, P., & Fonagy, P. (2021). Development and validation of a self-report measure of epistemic trust. PLOS ONE, 16(4), e0250264. [CrossRef]
- Chaulagain, S., Pizam, A., & Wang, Y. (2021). An Integrated Behavioral Model for Medical Tourism: An American Perspective. Journal of Travel Research, 60(4), 761–778. [CrossRef]
- Chen, R. T., & Orenstein, W. A. (1996). Epidemiologic methods in immunization programs. Epidemiologic Reviews, 18(2), 99–117. [CrossRef]
- Cheung, C., & Tse, J. W. (2008). Institutional Trust As a Determinant of Anxiety During the SARS Crisis in Hong Kong. Social Work in Public Health, 23(5), 41–54. [CrossRef]
- Corace, K. M., Srigley, J. A., Hargadon, D. P., Yu, D., MacDonald, T. K., Fabrigar, L. R., & Garber, G. E. (2016). Using behavior change frameworks to improve healthcare worker influenza vaccination rates: A systematic review. Vaccine, 34(28), 3235–3242. [CrossRef]
- Damnjanović, K., Graeber, J., Ilić, S., Lam, W. Y., Lep, Ž., Morales, S., Pulkkinen, T., & Vingerhoets, L. (2018a). Parental Decision-Making on Childhood Vaccination. Frontiers in Psychology, 9, 326661. [CrossRef]
- Damnjanović, K., Graeber, J., Ilić, S., Lam, W. Y., Lep, Ž., Morales, S., Pulkkinen, T., & Vingerhoets, L. (2018b). Parental Decision-Making on Childhood Vaccination. Frontiers in Psychology, 9. https://www.frontiersin.org/articles/10.3389/fpsyg.2018.00735.
- Damnjanović, K., Ilić, S., Pavlović, I., & Novković, V. (2019). Refinement of Outcome Bias Measurement in the Parental Decision-Making Context. Europe’s Journal of Psychology, 15(1), Article 1. [CrossRef]
- De Visser, R., Waites, L., Parikh, C., & Lawrie, A. (2011). The importance of social norms for uptake of catch-up human papillomavirus vaccination in young women. Sexual Health, 8(3), 330. [CrossRef]
- Enea, V., Eisenbeck, N., Carreno, D. F., Douglas, K. M., Sutton, R. M., Agostini, M., Bélanger, J. J., Gützkow, B., Kreienkamp, J., Abakoumkin, G., Abdul Khaiyom, J. H., Ahmedi, V., Akkas, H., Almenara, C. A., Atta, M., Bagci, S. C., Basel, S., Berisha Kida, E., Bernardo, A. B. I., … Leander, N. P. (2023). Intentions to be Vaccinated Against COVID-19: The Role of Prosociality and Conspiracy Beliefs across 20 Countries. Health Communication, 38(8), 1530–1539. [CrossRef]
- Fishbein, M., & Ajzen, I. (2011). Predicting and Changing Behavior: The Reasoned Action Approach. Taylor & Francis.
- Funk, S., Gilad, E., Watkins, C., & Jansen, V. A. A. (2009). The spread of awareness and its impact on epidemic outbreaks. Proceedings of the National Academy of Sciences, 106(16), 6872–6877. [CrossRef]
- Gesser-Edelsburg, A., & Badarna Keywan, H. (2022). Physicians’ Perspective on Vaccine-Hesitancy at the Beginning of Israel’s COVID-19 Vaccination Campaign and Public’s Perceptions of Physicians’ Knowledge When Recommending the Vaccine to Their Patients: A Cross-Sectional Study. Frontiers in Public Health, 10, 855468. [CrossRef]
- Glanz, K., Rimer, B. K., & Viswanath, K. (n.d.). Theory, Research, and Practice.
- Goldenberg, M. J. (2014). How can Feminist Theories of Evidence Assist Clinical Reasoning and Decision-making? Social Epistemology. https://www.tandfonline.com/doi/abs/10.1080/02691728.2013.794871.
- Goldenberg, M. J. (2021). Vaccine Hesitancy: Public Trust, Expertise, and the War on Science. University of Pittsburgh Press. [CrossRef]
- Gowda, C., & Dempsey, A. F. (2013). The rise (and fall?) of parental vaccine hesitancy. Human Vaccines & Immunotherapeutics, 9(8), 1755–1762. [CrossRef]
- Han, Q., Zheng, B., Cristea, M., Agostini, M., Bélanger, J. J., Gützkow, B., Kreienkamp, J., Collaboration, P., & Leander, N. P. (2023). Trust in government regarding COVID-19 and its associations with preventive health behaviour and prosocial behaviour during the pandemic: A cross-sectional and longitudinal study. Psychological Medicine, 53(1), 149–159. [CrossRef]
- Hobson-West, P. (2007). ‘Trusting blindly can be the biggest risk of all’: Organised resistance to childhood vaccination in the UK. Sociology of Health & Illness, 29(2), 198–215. [CrossRef]
- Horne, Z., Powell, D., Hummel, J. E., & Holyoak, K. J. (2015). Countering antivaccination attitudes. Proceedings of the National Academy of Sciences of the United States of America, 112(33), 10321–10324. [CrossRef]
- Hornsey, M. J., Harris, E. A., & Fielding, K. S. (2018). The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychology, 37(4), 307–315. [CrossRef]
- Huynh, H. P., & Senger, A. R. (2021). A little shot of humility: Intellectual humility predicts vaccination attitudes and intention to vaccinate against COVID-19. Journal of Applied Social Psychology, 51(4), 449–460. [CrossRef]
- Iyengar, S. S., & Lepper, M. R. (2000). When choice is demotivating: Can one desire too much of a good thing? Journal of Personality and Social Psychology, 79(6), 995–1006. [CrossRef]
- Jolley, D., & Douglas, K. M. (2014). The Effects of Anti-Vaccine Conspiracy Theories on Vaccination Intentions. PLoS ONE, 9(2), e89177. [CrossRef]
- Kahan, D. M. (2013). Social science. A risky science communication environment for vaccines. Science (New York, N.Y.), 342(6154), 53–54. [CrossRef]
- Keinan, R., & Bereby-Meyer, Y. (2012). “Leaving it to chance”—Passive risk taking in everyday life. Judgment and Decision Making, 7(6), 705–715. [CrossRef]
- Khodyakov, D. (2007). Trust as a Process: A Three-Dimensional Approach. Sociology, 41(1), 115–132. [CrossRef]
- Kiviniemi, M. T., Ellis, E. M., Hall, M. G., Moss, J. L., Lillie, S. E., Brewer, N. T., & Klein, W. M. P. (2018). Mediation, moderation, and context: Understanding complex relations among cognition, affect, and health behaviour. Psychology & Health, 33(1), 98–116. [CrossRef]
- Kutasi, K., Koltai, J., Szabó-Morvai, Á., Röst, G., Karsai, M., Biró, P., & Lengyel, B. (2022). Understanding hesitancy with revealed preferences across COVID-19 vaccine types. Scientific Reports, 12(1), 13293. [CrossRef]
- Lancet, T. (2020). COVID-19: Fighting panic with information. The Lancet, 395(10224), 537. [CrossRef]
- Larson, H., Leask, J., Aggett, S., Sevdalis, N., & Thomson, A. (2013). A Multidisciplinary Research Agenda for Understanding Vaccine-Related Decisions. Vaccines, 1(3), 293–304. [CrossRef]
- Lau, S., Hiemisch, A., & Baumeister, R. F. (2015). The experience of freedom in decisions—Questioning philosophical beliefs in favor of psychological determinants. Consciousness and Cognition: An International Journal, 33, 30–46. [CrossRef]
- Lazarus, J. V., Wyka, K., White, T. M., Picchio, C. A., Rabin, K., Ratzan, S. C., Parsons Leigh, J., Hu, J., & El-Mohandes, A. (2022). Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nature Communications, 13(1), 3801. [CrossRef]
- Lazić, A., & Zezelj, I. (2021). A systematic review of narrative interventions: Lessons for countering anti-vaccination conspiracy theories and misinformation. PsyArXiv. [CrossRef]
- Lep, Ž., Ilić, S., Teovanović, P., Hacin Beyazoglu, K., & Damnjanović, K. (2021). One Hundred and Sixty-One Days in the Life of the Homopandemicus in Serbia: The Contribution of Information Credibility and Alertness in Predicting Engagement in Protective Behaviors. Frontiers in Psychology, 12. https://www.frontiersin.org/articles/10.3389/fpsyg.2021.631791.
- Lewandowsky, S., & van der Linden, S. (2021). Countering misinformation and fake news through inoculation and prebunking. European Review of Social Psychology, 32(2), 348–384. [CrossRef]
- Lin, C. A., & Lagoe, C. (2013). Effects of News Media and Interpersonal Interactions on H1N1 Risk Perception and Vaccination Intent. Communication Research Reports, 30(2), 127–136. [CrossRef]
- Managing epidemics: Key facts about major deadly diseases. (n.d.). Retrieved 17 September 2023, from https://www.who.int/publications-detail-redirect/managing-epidemics-key-facts-about-major-deadly-diseases.
- McClure, C. C., Cataldi, J. R., & O’Leary, S. T. (2017). Vaccine Hesitancy: Where We Are and Where We Are Going. Clinical Therapeutics, 39(8), 1550–1562. [CrossRef]
- National Research Council (US) and Institute of Medicine (US) Board on Children, Y., Fischhoff, B., Nightingale, E. O., & Iannotta, J. G. (2001). Vulnerability, Risk, and Protection. In Adolescent Risk and Vulnerability: Concepts and Measurement. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK223737/.
- Newton, C., Feeney, J., & Pennycook, G. (2023). On the Disposition to Think Analytically: Four Distinct Intuitive-Analytic Thinking Styles. Personality and Social Psychology Bulletin, 01461672231154886. [CrossRef]
- Nikic, P., Stankovic, B., Santric, V., Vukovic, I., Babic, U., Radovanovic, M., Bojanic, N., Acimovic, M., Kovacevic, L., & Prijovic, N. (2023). Role of Healthcare Professionals and Sociodemographic Characteristics in COVID-19 Vaccination Acceptance among Uro-Oncology Patients: A Cross-Sectional Observational Study. Vaccines, 11(5), Article 5. [CrossRef]
- Ninković, M., Damnjanović, K., & Ilić, S. (2022). Structure and Misuse of Women’s Trust in the Healthcare System in Serbia. PsyArXiv. [CrossRef]
- Opel, D. J., Heritage, J., Taylor, J. A., Mangione-Smith, R., Salas, H. S., DeVere, V., Zhou, C., & Robinson, J. D. (2013). The Architecture of Provider-Parent Vaccine Discussions at Health Supervision Visits. Pediatrics, 132(6), 1037–1046. [CrossRef]
- Oraby, T., Thampi, V., & Bauch, C. T. (2014). The influence of social norms on the dynamics of vaccinating behaviour for paediatric infectious diseases. Proceedings. Biological Sciences, 281(1780), 20133172. [CrossRef]
- Rasmussen, S. A., & Goodman, R. A. (2020). Field epidemiology and COVID-19: Always more lessons to be learned. International Journal of Epidemiology, dyaa221. [CrossRef]
- Reyna, V. F. (2012). Risk perception and communication in vaccination decisions: A fuzzy-trace theory approach. Vaccine, 30(25), 3790–3797. [CrossRef]
- Rosenstock, I. M. (1974). The Health Belief Model and Preventive Health Behavior. Health Education Monographs, 2(4), 354–386. [CrossRef]
- Rosental, H., & Shmueli, L. (2021). Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines, 9(7), Article 7. [CrossRef]
- Ruggeri, K., Stock, F., Haslam, S. A., Capraro, V., Boggio, P., Ellemers, N., Cichocka, A., Douglas, K., Rand, D. G., Cikara, M., Finkel, E., Linden, S. V. D., Druckman, J., Wohl, M. J. A., Petty, R., Tucker, J. A., Peters, E., Shariff, A., Gelfand, M., … Willer, R. (2022). Evaluating expectations from social and behavioral science about COVID-19 and lessons for the next pandemic [Preprint]. PsyArXiv. [CrossRef]
- Schneiderman, N., McIntosh, R. C., & Antoni, M. H. (2019). Psychosocial risk and management of physical diseases. Journal of Behavioral Medicine, 42(1), 16–33. [CrossRef]
- Schumpe, B. M., Van Lissa, C. J., Bélanger, J. J., Ruggeri, K., Mierau, J., Nisa, C. F., Molinario, E., Gelfand, M. J., Stroebe, W., Agostini, M., Gützkow, B., Jeronimus, B. F., Kreienkamp, J., Kutlaca, M., Lemay, E. P., Reitsema, A. M., vanDellen, M. R., Abakoumkin, G., Abdul Khaiyom, J. H., … Leander, N. P. (2022). Predictors of adherence to public health behaviors for fighting COVID-19 derived from longitudinal data. Scientific Reports, 12(1), Article 1. [CrossRef]
- Seddig, D., Maskileyson, D., Davidov, E., Ajzen, I., & Schmidt, P. (2022). Correlates of COVID-19 vaccination intentions: Attitudes, institutional trust, fear, conspiracy beliefs, and vaccine skepticism. Social Science & Medicine, 302, 114981. [CrossRef]
- Shahsavari, S., Holur, P., Wang, T., Tangherlini, T. R., & Roychowdhury, V. (2020). Conspiracy in the time of corona: Automatic detection of emerging COVID-19 conspiracy theories in social media and the news. Journal of Computational Social Science, 3(2), 279–317. [CrossRef]
- Shapiro, G. K., Holding, A., Perez, S., Amsel, R., & Rosberger, Z. (2016). Validation of the vaccine conspiracy beliefs scale. Papillomavirus Research (Amsterdam, Netherlands), 2, 167–172. [CrossRef]
- Sharma, M. (2021). Theoretical Foundations of Health Education and Health Promotion. Jones & Bartlett Learning.
- Stankovic, B. (2017). Women’s Experiences of Childbirth in Serbian Public Healthcare Institutions: A Qualitative Study. International Journal of Behavioral Medicine, 24(6), 803–814. [CrossRef]
- Stanovich, K. E., & Toplak, M. E. (2023). Actively Open-Minded Thinking and Its Measurement. Journal of Intelligence, 11(2), Article 2. [CrossRef]
- Stöcker, A., Hoffmann, J., Mause, L., Neufeind, J., Ohnhäuser, T., & Scholten, N. (2023). What impact does the attitude toward COVID-19 vaccination have on physicians as vaccine providers? A cross sectional study from the German outpatient sector. Vaccine, 41(1), 263–273. [CrossRef]
- Teovanović, P., Lukić, P., Zupan, Z., Lazić, A., Ninković, M., & Žeželj, I. (2021). Irrational beliefs differentially predict adherence to guidelines and pseudoscientific practices during the COVID-19 pandemic. Applied Cognitive Psychology, 35(2), 486–496. [CrossRef]
- Thomas, K., Nilsson, E., Festin, K., Henriksson, P., Lowén, M., Löf, M., & Kristenson, M. (2020). Associations of Psychosocial Factors with Multiple Health Behaviors: A Population-Based Study of Middle-Aged Men and Women. International Journal of Environmental Research and Public Health, 17(4), 1239. [CrossRef]
- Thompson, A. G. H. (2007). The meaning of patient involvement and participation in health care consultations: A taxonomy. Social Science & Medicine (1982), 64(6), 1297–1310. [CrossRef]
- Van Der Linden, S. (2011). Charitable Intent: A Moral or Social Construct? A Revised Theory of Planned Behavior Model. Current Psychology, 30(4), 355–374. [CrossRef]
- Wicaksana, B., Yunihastuti, E., Shatri, H., Pelupessy, D. C., Koesnoe, S., Djauzi, S., Mahdi, H. I. S., Waluyo, D. A., Djoerban, Z., & Siddiq, T. H. (2023). Predicting Intention to Receive COVID-19 Vaccination in People Living with HIV using an Integrated Behavior Model. Vaccines, 11(2), Article 2. [CrossRef]
- Zingg, A., & Siegrist, M. (2012). Measuring people’s knowledge about vaccination: Developing a one-dimensional scale. Vaccine, 30(25), 3771–3777. [CrossRef]
Figure 1.
Illustration of interrelatedness of structural and psychological aspects (general and vaccine related) with their possible function in intention to vaccinate, and their contribution to the vaccination intention.
Figure 1.
Illustration of interrelatedness of structural and psychological aspects (general and vaccine related) with their possible function in intention to vaccinate, and their contribution to the vaccination intention.
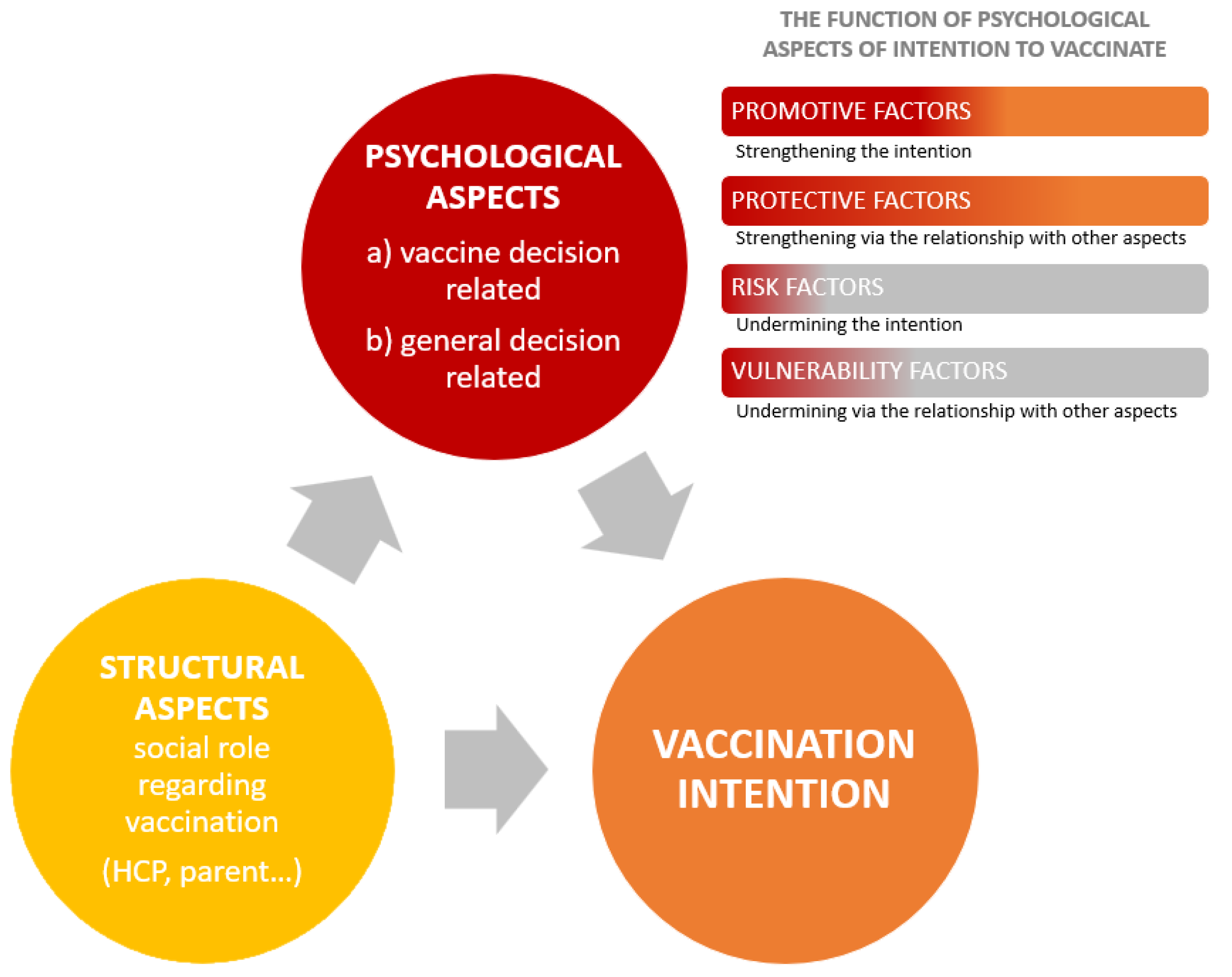
Table 1.
Psychological dispositions as moderators in the relationships between negative attitudes toward immunization and vaccination intention.
Table 1.
Psychological dispositions as moderators in the relationships between negative attitudes toward immunization and vaccination intention.
| Moderator: | Health providers | Parents | Lay people | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| B | S.E | β | B | S.E | β | B | S.E | β | |||
| Passive risk-taking | R = .565**, ΔR2 = .013* | R = .782**, ΔR2 = .002 | R = .835**, ΔR2 = .000 | ||||||||
| Negative attitudes | -.755 | .082 | -.531** | -1.439 | .073 | -.775** | -1.229 | .055 | -.849** | ||
| Passive risk taking | -.028 | .081 | -.020 | .014 | .073 | .008 | .054 | .052 | .037 | ||
| Interaction | -.137 | .068 | -.115* | -.073 | .066 | -.043 | .016 | .054 | .011 | ||
| AOT | R = .556**, ΔR2 = .004 | R = .781**, ΔR2 = .000 | R = .850**, ΔR2 = .022** | ||||||||
| Negative attitudes | -.776 | .082 | -.546** | -1.439 | .073 | -.775** | -1.002 | .063 | -.692** | ||
| AOT | .005 | .082 | -.004 | .047 | .073 | .025 | .084 | .055 | .058 | ||
| Interaction | -.090 | .082 | -.063 | .038 | .067 | .022 | .189 | .042 | .187** | ||
| Epistemic trust | R = .558**, ΔR2 = .003 | R = .780**, ΔR2 = .000 | R = .834**, ΔR2 = .000 | ||||||||
| Negative attitudes | -.798 | .082 | -.561** | -1.448 | .074 | -.780** | -1.201 | .051 | -.829** | ||
| Epistemic trust | -.079 | .081 | -.056 | -.008 | .074 | -.004 | .018 | .050 | .050 | ||
| Interaction | .079 | .084 | .054 | .008 | .063 | .005 | .021 | .045 | .045 | ||
| Epistemic mistrust | R = .564**, ΔR2 = .002 | R = .781**, ΔR2 = .000 | R = .834**, ΔR2 = .000 | ||||||||
| Negative attitudes | -.796 | .080 | -.560** | -1.449 | .072 | -.781** | -1.211 | .050 | -.836** | ||
| Epistemic mistrust | .146 | .080 | .103 | .067 | .073 | .036 | -.002 | .050 | -.002 | ||
| Interaction | -.063 | .086 | -.042 | .022 | .087 | .010 | .019 | .043 | .043 | ||
| Epistemic credulity | R = .557**, ΔR2 = .001 | R = .785**, ΔR2 = .006* | R = .834**, ΔR2 = .001 | ||||||||
| Negative attitudes | -.773 | .083 | -.543** | -1.461 | .072 | -.787** | -1.207 | .051 | -.831** | ||
| Epistemic credulity | .078 | .081 | .055 | -.039 | .072 | -.021 | .008 | .052 | .006 | ||
| Interaction | .052 | .078 | .039 | -.161 | .078 | -.079* | -.041 | .046 | -.031 | ||
Table 2.
Vaccine-specific factors as moderators in the relationships between negative attitudes toward immunization and vaccination intention.
Table 2.
Vaccine-specific factors as moderators in the relationships between negative attitudes toward immunization and vaccination intention.
| Moderator: | Health providers | Parents | Lay people | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| B | S.E | β | B | S.E | β | B | S.E | β | |||
| Experience of freedom | R = .608**, ΔR2 = .036** | R = .788**, ΔR2 = .008* | R = .847**, ΔR2 = .022** | ||||||||
| Negative attitudes | -.564 | .091 | -.397** | -1.323 | .086 | -.713** | -1.072 | .058 | -.740** | ||
| Experience of freedom | .238 | .081 | .167** | .085 | .084 | .046 | .055 | .050 | .038 | ||
| Interaction | .236 | .068 | .216** | .148 | .064 | .102* | .242 | .054 | .170** | ||
| Choice overload | R = .598**, ΔR2 = .048** | R = .792**, ΔR2 = .008* | R = .838**, ΔR2 = .005* | ||||||||
| Negative attitudes | -.548 | .096 | -.385** | -1.231 | .093 | -.663** | -1.141 | .057 | -.788** | ||
| Choice overload | -.126 | .080 | -.089 | -.163 | .069 | -.088 | -.075 | .052 | -.052 | ||
| Interaction | -.322 | .081 | -.264** | -.166 | .069 | -.116* | -.117 | .058 | -.077* | ||
| Perceived consensus | R = .678**, ΔR2 = .128** | R = .794**, ΔR2 = .017** | R = .848**, ΔR2 = .023** | ||||||||
| Negative attitudes | -.340 | .092 | -.239** | -1.137 | .107 | -.612** | -.913 | .085 | -.621** | ||
| Perceived consensus | .110 | .083 | .077 | .185 | .085 | .100* | -.030 | .066 | -.021 | ||
| Interaction | .388 | .054 | .463** | .243 | .072 | .171** | .207 | .045 | .242** | ||
| Subjective norms | R = .560**, ΔR2 = .004 | R = .785**, ΔR2 = .005 | R = .836**, ΔR2 = .003 | ||||||||
| Negative attitudes | -.783 | .081 | -.550** | -1.381 | .078 | -.744** | -1.424 | .146 | -.983** | ||
| Subjective norms | .105 | .081 | .074 | .068 | .077 | .037 | .024 | .051 | .017 | ||
| Interaction | -.087 | .082 | -.061 | .125 | .065 | .078 | .047 | .029 | .163 | ||
| Conspiracy beliefs | R = .656**, ΔR2 = .094** | R = .825**, ΔR2 = .039** | R = .874**, ΔR2 = .040** | ||||||||
| Negative attitudes | -.182 | .119 | -.128* | -.582 | .131 | -.314** | -.561 | .091 | -.387** | ||
| Conspiracy beliefs | -.170 | .107 | -.119* | -.547 | .106 | -.295** | -.318 | .085 | -.220** | ||
| Interaction | -.307 | .051 | -.466** | -.368 | .065 | -.306** | -.236 | .036 | -.332** | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



