
Submitted:
02 October 2023
Posted:
04 October 2023
You are already at the latest version
Abstract
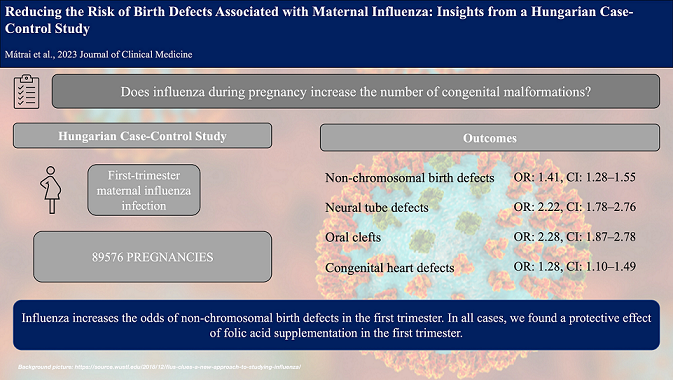
Influenza virus can cause several complications during pregnancy. Therefore, we aimed to inves-tigate the effects of influenza on the development of congenital abnormalities (CAs) by analyzing the database of the Hungarian Case-Control Surveillance of Congenital Abnormalities (HCCS-CA). In our multicenter, case-control, population-based study, we processed clinician-reported outcomes and diagnoses collected in the HCCSCA. The case group included newborns with dif-ferent non-chromosomal birth defects, while controls were newborns without CAs. Maternal in-fluenza, as a risk factor for CAs, was analyzed by using a logistic regression model and odds ra-tios with 95% confidence intervals (CIs). Our results showed that maternal influenza in the first trimester was associated with increased odds of developing non-chromosomal CAs (OR: 1.41, CI: 1.28–1.55). There were increased odds of neural tube defects (OR: 2.22, CI: 1.78–2.76), orofacial clefts (OR: 2.28, CI: 1.87–2.78) and congenital heart defects (OR: 1.28, CI: 1.10–1.49) after influenza infection. In all cases, we found a protective effect of folic acid supplementation in the first tri-mester. The odds of non-chromosomal birth defects are higher after maternal influenza in the first -trimester. Folic acid or pregnancy vitamin supplementation and antipyretic therapy may reduce the effect of maternal influenza during the first trimester.
Keywords:
influenza
; pregnancy
; first trimester
; non-chromosomal congenital malformations
1. Introduction
Since 2020, the COVID-19 pandemic has again highlighted the risk of viral infections during pregnancy. Moreover, compared to COVID-19, the incidence of influenza is much higher in pregnant women [1].
Influenza is an acute infectious disease that occurs in epidemic outbreaks during winter. It is caused by influenza viruses A, B or C; the incubation period is about two days. The recovery lasts usually 3-7 days for healthy individuals, but older adults, children, pregnant women, and people with chronic diseases are at increased risk of complications [2].
The incidence of congenital abnormalities (CAs) is 3-5% worldwide. Congenital abnormalities are considered the leading causes of infant mortality. Influenza can also occur during pregnancy [3]. During the critical time frame, in the first trimester, it can have a deleterious effect on the developing embryo, leading to various birth defects (BDs) [4]. The meta-analysis published by our working group last year also revealed associations between maternal influenza and the development of several malformations [5].
The aim of the present study was to estimate the odds of birth defects in the offspring of mothers with influenza during the first trimester in the Hungarian population. We hypotesized that influenza in the first trimester of pregnancy increases the likelihood of developing non-chromosomal CAs.
2. Materials and Methods
The study was reported according to the recommendations of the STROBE guidelines (Supplementary Table S1) [6].
Study design and setting
In our case-control study, we investigated the effects of maternal influenza during the first trimester of pregnancy on the development of non-chromosomal birth defects in the Hungarian population. The cases and controls were enrolled in the database of the Hungarian Case-Control Surveillance of Congenital Abnormalities (HCCSCA) between 1980 and 2009.
Data collection
The HCCSCA was established in 1980 [7], and the cases were recorded from the Hungarian Congenital Abnormality Registry (HCAR). This dataset contains details of 90,000 pregnancies. The data collection was changed in 1997, slightly modifying the structure of the dataset [8]. In a previous project, data collected in the HCCSCA between 1980 and 2009 were combined into an authenticated unified database [8].
The HCAR was established in 1962 as the first national-based registry of CAs in the world [9]. Physicians were required to report patients with CA to the HCAR from birth to the end of the first postnatal year. Given that almost all births in Hungary take place in inpatient obstetric wards, all deliveries were reported by obstetricians and pediatricians [9]. After 1984, prenatal diagnosis centers were also required to report malformed fetuses diagnosed prenatally to the HCAR. In each case, two designated geneticists of HCAR examined the affected newborns. The diagnosis of CA was confirmed with a physical examination, and then they were divided into subgroups.
Participants:
Cases with CAs were included in the HCCSCA from the HCAR based on three criterias: (1) Cases reported within three months of birth or elective termination of pregnancy, (2) Cases did not have dislocation of the hip, congenital inguinal hernia, and large hemangioma, (3) Co-occurrence of chromosomal abnormalities were excluded. The origin of CA-syndromes is periconceptional. The HCCSCA was used to detect teratogenic or fetotoxic effects during pregnancy.
Controls were specified as newborn infants without any CAs. They were matched to every cases according to sex, birth week, and district of the residence of parents. These controls were selected from the Hungarian National Birth Registry of the Central Statistical Office based on the HCCSCA case lists for each quarter of the year. If the controls were twins, only one was randomly selected for the HCCSCA [8].
Variables and data sources:
The following data were collected for each case and control patient in the database: CA(s), gender, birth year/month/day, birth weight, gestational age, area of residence of mother, maternal age, paternal age, birth order, education of mother and father, status and type of employment, marital status of mother, outcomes of previous pregnancies, maternal diseases during pregnancy (by month of pregnancy), medication taken during pregnancy (by month of pregnancy), folic acid and/or pregnancy vitamin supplement taken (by month of pregnancy), smoking habits and alcohol consumption patterns of mother [8].
Data were collected in three ways. First, there was a prospective, medically recorded data collection. Mothers were requested to send their prenatal maternity logbooks, medical records of their diseases during the pregnancy under study and the CA of newborn. A retrospective data collection was also performed when a structured questionnaire and a printed form of informed consent were sent by post to mothers of cases and controls after hospital discharge. Moreover, an additional way of data collection was also carried out. Regional nurses visited all cases and controls in their homes. They helped mothers collect their medical records and fill in the questionnaire [8].
The analysis used the International Classification of Diseases (ICD)-10 to identify congenital malformations and diseases during the analysis. Thus, the definition of influenza infection was based on reported data and ICD-10 definitions. For most major CAs, the critical period is the first trimester, i.e. the first three months of pregnancy. Therefore, cases were analyzed only if they met two criteria: influenza infection was reported in the first three gestational months and the National Center for Epidemiology recorded an influenza epidemic during that period. Gestational age was calculated from the first day of the last menstrual period.
Bias
Despite the long study period, the specific nature of data collection and verification increases the reliability of the data. However, the classification of the International Classification of Diseases (ICD) changed during the study period several times, so the conversion of different ICD categories into each other may have caused minor differences in the outcome groups. As with all case-control studies involving interviews and questionnaires, recall bias reduces the reliability of the study.
Statistical methods
Data were extracted from the unified database of the Hungarian Case Control Surveillance of Congenital Abnormalities to a Microsoft Excel datasheet, stored in data tables and re-validated before being used for data analysis. Statistical analysis was performed using R statistical software [10]. After data were described, a logistic regression model was fitted: we used the rate of congenital abnormalities as the response variable and the first-trimester influenza rate as the explanatory variable. The effect was adjusted for the intake of antipyretic drugs, folic acid, and maternal vitamins. There was no interaction term in the final model. To report our results, we used the prevalence odds ratios, their 95% confidence intervals (CI), and the outcome probabilities. A p-value of less than 0.05 was considered statistically significant.
3. Results
Participants
In the unified HCCSCA database, we identified 32,345 cases and 57,231 controls, altogether 89,576 pregnancies. Of the 32,345 cases, 809 cases of influenza infection occurred during the first trimester. Of the 57,231 controls, we identified 1,020 control cases of influenza during the first trimester. Between 1980 and 2009, there were 3,009,303 live births in Hungary; therefore, our control group represents 1.9 % of total births in the country. These are shown in Figure 1.
Descriptive data
Basic characteristics of patients included
The baseline characteristics of patients included maternal age, education, smoking habits, folic acid intake, pregnancy vitamin intake, and the use of antipyretic therapy. These are presented in Table 1.
Outcome data
Non-chromosomal congenital abnormalities
We found a significant association between the development of maternal influenza in the first trimester and some non-chromosomal congenital malformations. If influenza is present in the first three months of pregnancy, the odds of of the developmant of non-chromosomal malformations increase almost one and a half times (OR: 1.41, CI: 1.28–1.55; p<0.001).
Of the 809 cases, we identified 88 cases of neural tube defects (NTDs), 110 cases of oral clefts and 190 cases of cardiovascular malformations.
Neural tube defects
Our findings highlighted a twofold increase in the development of NTDs (OR: 2.22, CI: 1.78–2.76; p<0.001) after influenza infection in the first trimester. We also performed a subgroup analysis for NTDs. The results showing the increased odds of developing spina bifida, hydrocephalus, anencephaly and encephalocele after maternal influenza are shown in Table 2.
Oral clefts
We found a significant increase in the odds of developing oral clefts after maternal influenza in the first trimester (OR: 2.28, CI: 1.87–2.78; p<0.001). The subgroup analysis found a more than twofold increase in the odds for cleft lip, cleft palate with unilateral cleft lip and unspecified cleft palate development. These findings are shown in Table 3.
Congenital heart defects
Overall, our findings also highlighted increased odds of developing congenital heart defects (CHD) (OR: 1.28, CI: 1.10–1.49; p<0.001). We found significant associations when subgroups were analyzed. The odds of developing ventricular septal defects increased after maternal influenza in the first trimester (OR: 1.38, CI: 1.09–1.72; p=0.006). The odds for different subcategories are shown in Table 4.
Effects of the drugs used
After determining the odds ratios after maternal influenza in the first trimester, we examined the association of folic acid use, the use of pregnancy multivitamins and antipyretic therapy with the development of congenital malformations. We identified a minimal odds ratio reductions for NTDs and oral clefts. For heart defects, we found a protective effect of folic acid supplementation in the first trimester, indicated by the reduced odds ratio, but these findings were not significant. These findings are shown in Table 5.
We also analyzed the use of pregnancy multivitamins and identified a protective effect of multivitamin supplementation on the development of neural tube defects. These findings are shown in Table 6.
Finally, we also examined whether the development of congenital malformations might be affected by antipyretics when the influenza occurred in the first trimester. We found no association between the use of antipyretics and the occurrence of all types of birth defects. However, in the case of neural tube defects, antipyretics reduced the odds. These findings are shown in Table 7.
The first trimester, i.e., the first 12 weeks of pregnancy, is particularly important in the development of birth defects. Organogenesis takes place during this crucial period, and any environmental impact on the mother can therefore adversely affect this developmental process [3]. In the current pandemic period, the importance of viral infections has been re-emphasized[1]. However, the emergence of COVID-19 should not be overlooked, nor the influenza virus, which appears as an epidemic every year. Since the 1980s, numerous studies have investigated the adverse effects of influenza on pregnancy outcomes and the development of birth defects [5,11,12,13,14].
4. Discussion
Our overall foundings represented increased odds of developing non-chromosomal birth defects after first trimester maternal influenza. In line with our findings, Oster et al. from the United States of America (USA) reported a large case-control study of nearly 6,000 patients with the same conclusion for influenza infection in the first trimester [14]. According to the literature and the meta-analysis previously performed by our working group, neural tube defects, oral clefts, and cardiovascular malformations are the three major types of non-chromosomal birth defects with an increased prevalence after influenza infection [5].
Neural tube defects are congenital abnormalities of the brain, spine, or spinal cord. Reviewing the literature, Saxén et al.[15] and Kurppa et al.[16] investigated the development of neural tube defects, and reported the same increased odds of the development of NTDs after maternal influenza in the first trimester. Among the causes of NTDs, maternal factors should also be mentioned, such as obesity, hyperthermia (fever), and diabetes. Valproate or low folate intake are also known as main risk factors of the disease [17]. Therefore, it is essential to raise awareness of pregnant women about folic acid supplementation or prenatal vitamin intake even before becoming pregnant.
Oral cleft screening is part of the ultrasound scan at week 20. These types of birth defects occur in 1.5 out of a 1,000 live births [18]. Newborns born with these anomalies have feeding difficulties and speech problems, or conductive hearing loss [19]. Our results suggest that maternal influenza in the first trimester is a risk factor for developing these congenital malformations. Saxén et al. [20,21] and Dymanus et al. [22] confirmed the link between maternal influenza and the development of orofacial clefts. A previous study based on our database confirmed that maternal influenza occurring in the first trimester and other lifestyle factors (gender, birthweight, smoking) are risk factors for the development of cleft palate [20]. Among the causes of oral clefts, alcohol consumption, anticonvulsive therapy or folic acid deficiency must be mentioned [21].
Particular attention should be paid to congenital heart defects. These birth defects are common anomalies and are leading causes of neonatal or infant deaths. After reviewing the literature, many studies [11,12,25] investigated the origin of cardiovascular malformations. Among the underlying causes confirming our findings, maternal influenza infection [12,13,22], low maternal employment status, pregestational diabetes, maternal clotting disorders, prescriptions of anticoagulants should be mentioned [14].
Focusing on the prevention of these types of anomalies, there are several studies in the literature confirming our findings. Several studies have concluded that folic acid supplementation reduces the chance of some developmental disorders [17]. We can also identify studies analyzing the use of antipyretic drugs during influenza. Some of these studies confirmed that the odds of developing these types of birth defects were lower after using these drugs [11]. Our results, however, could not confirm these findings for all types of malformations. We observed this effect only in the case of neural tube defects.
Strengths and limitations
Among the strengths of our analysis, we have to mention the large number of cases and the HCCSCA database, which is unique in the world due to the large number of cases. We can also mention the data collection methods, which contributed to data quality. Among the strengths, it should also be mentioned that the controls were assigned to the cases thanks to a very precise matching.
As for the limitations of this analysis, although data collection was performed using three methods, the identification of influenza was determined based on the symptoms and self reported retrospective data. Thus, due to the measurement of risk factors and case-control studies was made the risk of bias high.
Implications for practice and research
The translation of scientific findings into everyday patient care is decisive in medicine today; therefore, we should try to prevent influenza during pregnancy [23]. We must raise awareness among pregnant women about the safe use of vaccination. Awareness-raising campaigns should be organized on the importance of folic acid and its modern counterpart, pregnancy vitamins. In the future, it would be recommended to start a prospective study in which influenza would be identified on the basis of Polymerase Chain Reaction (PCR).
5. Conclusions
Our findings suggest that maternal influenza occurring in the first trimester is associated with non-chromosomal birth defects, mainly neural tube defects, oral clefts, and congenital heart defects. Prevention is of significant importance, including vaccination and folic acid/pregnancy vitamin intake.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. representing the STROBE Checklist, Table S2. representing the prevalence of specific types of congenital anomalies after first- trimester influenza infection.
Author Contributions
ÁM: conceptualization, project administration, writing – original draft; BT: project administration, conceptualization, methodology, writing, review, editing; BP data curation, review, editing; AK: formal analysis; visualization; PH: project administration, methodology, review, editing; NÁ: conceptualization; supervision; writing – original draft. All authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript.
Funding
Funding was provided by the ÚNKP-22-3 New National Excellence Program from the National Research, Development and Innovation Fund (to BT - ÚNKP-22-3-I-PTE-1693). Further funding was provided by the National Research, Development, and Innovation Fund (ITM-NRDIF) (TKP2021-EGA-23). Sponsors had no role in the design, data collection, analysis, interpretation, and manuscript preparation.
Institutional Review Board Statement
In our study, cases and controls were obtained from the Hungarian Case-Control Surveillance of Congenital Anomalies (HCCSCA). Ethics approval for data analysis was obtained from the Scientific and Research Ethics Committee of the Medical Research Council, Hungary (BMEÜ/920-3 /2022/EKU). The study was conducted in accordance with the Helsinki Declaration.
Data Availability Statement
All data were included in the manuscript.
Conflicts of Interest
None to declare.
References
- Morens, D.M. , et al., Pandemic COVID-19 Joins History's Pandemic Legion. mBio, 2020. 11(3). [CrossRef]
- Pleschka, S. , Overview of influenza viruses. Curr Top Microbiol Immunol, 2013. 370: p. 1-20.
- Silasi, M. , et al., Viral infections during pregnancy. Am J Reprod Immunol, 2015. 73(3): p. 199-213. [CrossRef]
- Mai, C.T. , et al., National population-based estimates for major birth defects, 2010-2014. Birth Defects Res, 2019. 111(18): p. 1420-1435.
- Mátrai, Á. , et al., First-Trimester Influenza Infection Increases the Odds of Non-Chromosomal Birth Defects: A Systematic Review and Meta-Analysis. Viruses, 2022. 14(12). [CrossRef]
- von Elm, E. , et al., The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med, 2007. 147(8): p. 573-7.
- Czeizel, A.E. , et al., Description and mission evaluation of the Hungarian case-control surveillance of congenital abnormalities, 1980-1996. Teratology, 2001. 63(5): p. 176-85. [CrossRef]
- Ács, N., Á. Mátrai, and A. Kaposi, First data from the new, unified database of the Hungarian case-control surveillance of congenital abnormalities. J Matern Fetal Neonatal Med, 2021. 34(17): p. 2887-2892. [CrossRef]
- Czeizel, A.E., J. Métneki, and J. Béres, 50 years of the Hungarian Congenital Abnormality Registry. Congenit Anom (Kyoto), 2014. 54(1): p. 22-9. [CrossRef]
- R:, R.C.T. A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing. Available from: https://www.R-project.org.
- Acs, N. , et al., Maternal influenza during pregnancy and risk of congenital abnormalities in offspring. Birth Defects Res A Clin Mol Teratol, 2005. 73(12): p. 989-96. [CrossRef]
- Li, M. , et al., Maternal influenza-like illness, medication use during pregnancy and risk of congenital heart defects in offspring. J Matern Fetal Neonatal Med, 2014. 27(8): p. 807-11. [CrossRef]
- Botto, L.D., M. C. Lynberg, and J.D. Erickson, Congenital heart defects, maternal febrile illness, and multivitamin use: a population-based study. Epidemiology, 2001. 12(5): p. 485-90. [CrossRef]
- Oster, M.E. , et al., Associations between maternal fever and influenza and congenital heart defects. J Pediatr, 2011. 158(6): p. 990-5. [CrossRef]
- Saxén, L. , et al., Influenza epidemics and anencephaly. Am J Public Health, 1990. 80(4): p. 473-5. [CrossRef]
- Kurppa, K. , et al., Anencephaly and maternal common cold. Teratology, 1991. 44(1): p. 51-5. [CrossRef]
- Avagliano, L. , et al., Overview on neural tube defects: From development to physical characteristics. Birth Defects Res, 2019. 111(19): p. 1455-1467. [CrossRef]
- Allam, E., L. Windsor, and C. Stone, Cleft lip and palate: etiology, epidemiology, preventive and intervention strategies. Anat Physiol, 2014. 4(3): p. 1-6. [CrossRef]
- Mitchell, J.C. and R.J. Wood, Management of cleft lip and palate in primary care. J Pediatr Health Care, 2000. 14(1): p. 13-9. [CrossRef]
- Ács, L. , et al., Maternal-related factors in the origin of isolated cleft palate—A population-based case-control study. Orthodontics & Craniofacial Research, 2020. 23(2): p. 174-180.
- Voigt, A. , et al., [Cleft lip and palate]. Pathologe, 2017. 38(4): p. 241-247.
- Ou, Y. , et al., Risk factors of different congenital heart defects in Guangdong, China. Pediatr Res, 2016. 79(4): p. 549-58. [CrossRef]
- Hegyi, P. , et al., Accelerating the translational medicine cycle: the Academia Europaea pilot. Nat Med, 2021. 27(8): p. 1317-1319. [CrossRef]
Figure 1.
Flowchart of the selection.
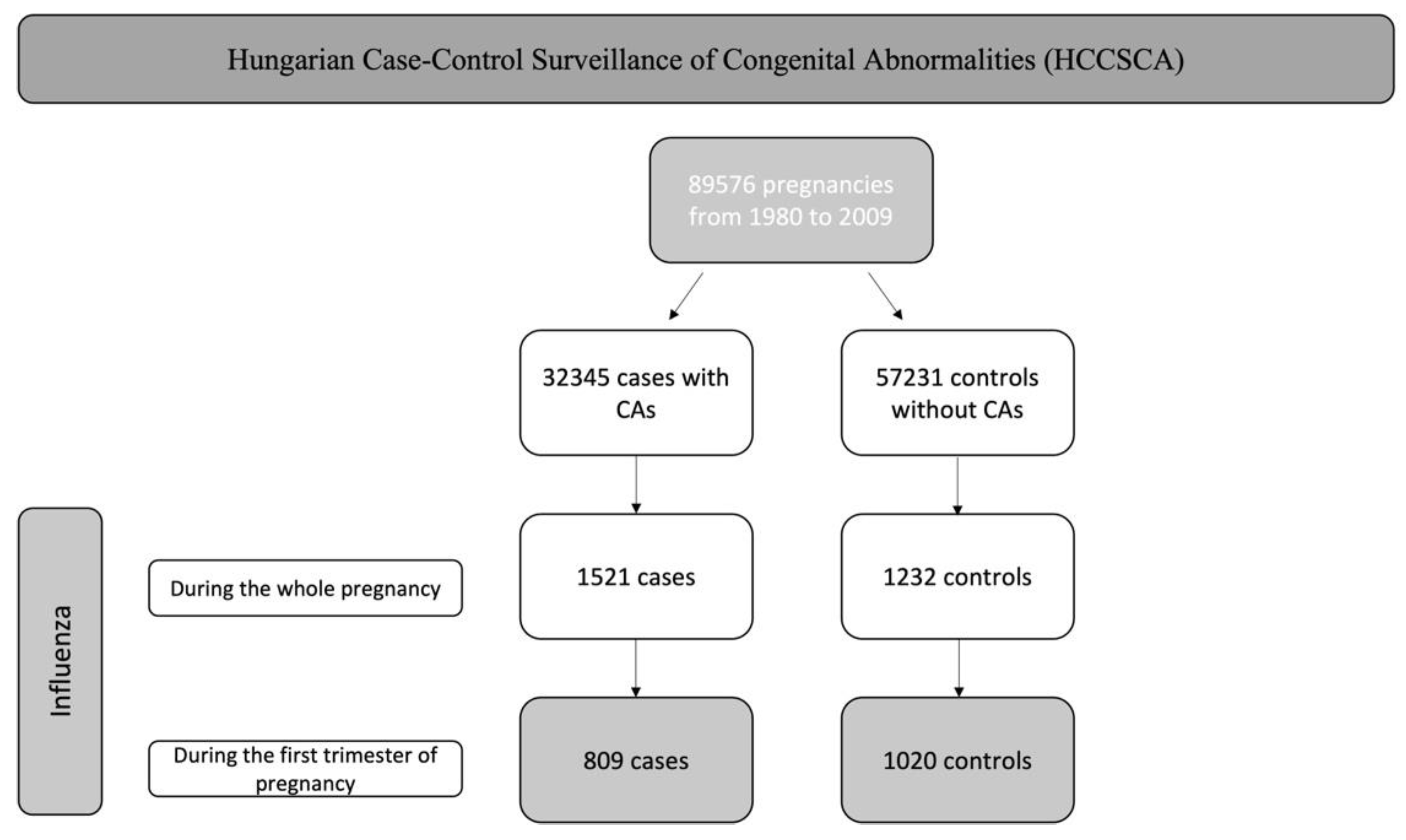

Table 1.
Baseline characteristics of patients in the case and control groups.
| First-Trimester Influenza Infection | ||
|---|---|---|
| Characteristic | Cases (N = 809) | Controls (N = 1020) |
| Maternal age | ||
| <25 | 392 (48.45%) | 462 (45.29 %) |
| 25-29 | 252 (31.15 %) | 357 (35.00 %) |
| >29 | 165 (20.40 %) | 201 (19.71 %) |
| Mean ± SD | 25.61 ± 5.27 | 25.53 ± 4.72 |
| Birth order | ||
| Primiparous | 109 (13.47 %) | 120 (11.76 %) |
| Multiparous | 5 (0.62 %) | 0 |
| NA | 695 (85.91%) | 900 (88.24 %) |
| Maternal employment status | ||
| Professional | 25 (3.09 %) | 38 (3.73 %) |
| Managerial | 46 (5.69 %) | 51 (5.00 %) |
| Skilled worker | 27 (3.34 %) | 30 (2.94 %) |
| Semiskilled worker | 13 (1.61 %) | 8 (0.78 %) |
| Unskilled worker | 1 (0.12 %) | 0 |
| Housewife | 1 (0.12 %) | 0 |
| Others/NA | 696 (86.03 %) | 893 (87.55 %) |
| Maternal smoking | ||
| Smoker | 16 (1.98 %) | 162 (15.88 %) |
| Non-smoker | 77 (9.52 %) | 473 (46.37 %) |
| NA | 716 (88.50 %) | 385 (37.75 %) |
| Folic acid supplementation | ||
| Yes | 328 (40.54 %) | 490 (48.04 %) |
| No | 481 (59.46 %) | 530 (51.96 %) |
| Pregnancy vitamin supplementation | ||
| Yes | 65 (8.03 %) | 68 (6.67 %) |
| No | 744 (91.97 %) | 952 (93.33 %) |
| Use of antipyretics | ||
| Yes | 250 (30.90 %) | 322 (31.57 %) |
| No | 559 (69.10 %) | 698 (68.43 %) |
Table 2.
Detailed odds ratios for developing neural tube defects.
| Case mothers N=1829 | Matched controls N=87747 | Comparison | |||
|---|---|---|---|---|---|
| Type of CAs | No. | No. | Odds Ratio | 95%–CI | p |
| Neural tube defects | 88 (4.81 %) | 1954 (2.23 %) | 2.22 | 1.78–2.76 | < 0.001 |
| Spina bifida | 30 (1.64 %) | 578 (0.66 %) | 2.52 | 1.70–3.57 | < 0.001 |
| Hydrocephalus | 19 (1.04 %) | 289 (0.33 %) | 3.18 | 1.93–4.92 | < 0.001 |
| Anencephalia | 13 (0.71 %) | 301 (0.34 %) | 2.08 | 1.31–3.48 | 0.010 |
| Encephalocele | 10 (0.55 %) | 190 (0.22 %) | 2.53 | 1.25–4.54 | 0.004 |
Table 3.
Detailed odds ratios for developing oral clefts.
| Case mothers N=1829 | Matched controls N=87747 | Comparison | |||
|---|---|---|---|---|---|
| Type of CAs | No. | No. | Odds Ratio | 95%–CI | p |
| Oral clefts | 110 (6.01 %) | 2393 (2.73 %) | 2.28 | 1.87–2.78 | < 0.001 |
| Cleft palate with unilateral cleft lip | 41 (2.24 %) | 920 (1.05 %) | 2.16 | 1.55–2.93 | < 0.001 |
| Cleft lip | 33 (1.80 %) | 649 (0.74 %) | 2.47 | 1.70–3.45 | < 0.001 |
| Cleft palate, unspecified | 32 (1.75 %) | 722 (0.82 %) | 2.15 | 1.47–3.01 | < 0.001 |
Table 4.
Detailed odds ratios for developing congenital heart defects.
| Case mothers N=1829 | Matched controls N=87747 | Comparison | |||
|---|---|---|---|---|---|
| Type of CAs | No. | No. | Odds Ratio | 95%–CI | p |
| Cardiovascular malformations | 190 (10.40 %) | 7296 (8.31 %) | 1.28 | 1.10–1.49 | < 0.001 |
| Ventricular septal defects | 79 (4.32 %) | 2783 (3.17 %) | 1.38 | 1.09–1.72 | 0.006 |
| Congenital malformations of heart, unspecified | 29 (1.59 %) | 752 (0.86 %) | 1.86 | 1.25–2.66 | < 0.001 |
| Atrial septal defects | 28 (1.53 %) | 1865 (2.13 %) | 0.72 | 0.48–1.02 | 0.081 |
| Other congenital malformations of cardiac chambers and connections | 12 (0.66 %) | 325 (0.37 %) | 1.78 | 0.94–3.02 | 0.051 |
| Patent ductus arteriosus | 12 (0.66%) | 689 (0.79 %) | 0.83 | 0.44–1.41 | 0.536 |
Table 5.
Detailed odds ratios for developing congenital abnormalities with or without folic acid supplementation.
Table 5.
Detailed odds ratios for developing congenital abnormalities with or without folic acid supplementation.
| All | With folic acid | ||||
|---|---|---|---|---|---|
| Study groups | No. | Odds Ratio, 95%–CI | No. | Odds Ratio, 95%–CI | p |
| Neural tube defects | 88 | 2.22; (1.78–2.76) | 39 | 2.20; (1.59–3.05) | < 0.001 |
| Oral clefts | 110 | 2.28; (1.87–2.78) | 38 | 1.78; (1.28–2.48) | < 0.001 |
| Congenital heart defects | 190 | 1.28; (1.10–1.49) | 68 | 0.90; (0.70–1.16) | 0.424 |
Table 6.
Detailed odds ratios for developing congenital abnormalities with or without maternal vitamin supplementation.
Table 6.
Detailed odds ratios for developing congenital abnormalities with or without maternal vitamin supplementation.
| All | With maternal vitamin | ||||
|---|---|---|---|---|---|
| Study groups | No. | Odds Ratio, 95%–CI | No. | Odds Ratio, 95%–CI | p |
| Neural tube defects | 88 | 2.22; (1.78–2.76) | 3 | 0.92; (0.29–2.88) | 0.882 |
| Oral clefts | 110 | 2.28; (1.87–2.78) | 10 | 2.73; (1.43–5.22) | 0.002 |
| Congenital heart defects | 190 | 1.28; (1.10–1.49) | 25 | 2.66; (1.72–4.12) | < 0.001 |
Table 7.
Detailed odds ratios for developing congenital abnormalities with or without antipyretic drugs.
Table 7.
Detailed odds ratios for developing congenital abnormalities with or without antipyretic drugs.
| All | With antipyretic drugs | ||||
|---|---|---|---|---|---|
| Study groups | No. | Odds Ratio, 95%–CI | No. | Odds Ratio, 95%–CI | p |
| Neural tube defects | 88 | 2.22; (1.78–2.76) | 21 | 1.73; (1.12–2.69) | 0.014 |
| Oral clefts | 110 | 2.28; (1.87–2.78) | 35 | 2.43; (1.72–3.42) | < 0.001 |
| Congenital heart defects | 190 | 1.28; (1.10–1.49) | 64 | 1.41; (1.08–1.83) | 0.010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



