Submitted:
03 October 2023
Posted:
04 October 2023
You are already at the latest version
Abstract
To clarify whether changes in biological features of breast tumor cells and intra-tumor immunity after neoadjuvant chemotherapy (NAC) may correlate with pathological responses and prognosis in breast cancer patients treated with NAC, we investigated various biomarkers using both pre- and post-NAC tumor samples. The study subjects were 24 primary breast cancer patients, who were treated with NAC at the Department of Breast and Thyroid Surgery, Kawasaki Medical School Hospital between 2010 and 2011. All of them had a non-pathological complete response (pCR) to NAC and their pre- and post-NAC tumor samples were available for biomarker assays. Ki67 labeling index, apoptosis, factors related to cancer stem cells and epithelial-mesenchymal transition, tumor infiltrating lymphocytes (TILs), and expression levels of CD-8, CD-4, FoxP3, PD-L1, and PD-1 were studied using the paired samples. Biological characteristics of residual tumors such as nuclear grade (NG) and vascular invasion (v) were also investigated. The median age was 53 years-old and 14 patients had stage III tumors, while 10 had stage II tumors. A higher expression level of CD8, CD4, or PD-1 in pre-NAC samples and of CD8, CD4 or PD-L1 in post-NAC samples was significantly correlated with a better pathological response to NAC. Positivity of ZEB1, vimentin, and v or NG 3 in post-NAC samples was significantly correlated with either worse disease-free survival (DFS) or worse overall survival (OS) by univariate analyses. Multivariate analyses for DFS and OS revealed that positivity for v and vimentin expression in residual tumors were independent prognostic factors in this study. These findings indicate that activated intra-tumor immune microenvironments may play significant roles in pathological responses to NAC, and that the up-regulation of vimentin and v-positivity in residual tumors may be pivotal prognostic factors in non-pCR cases to NAC.
Keywords:
breast cancer
; neoadjuvant chemotherapy
; vimentin
; vascular invasion
; prognosis
1. Introduction
Neoadjuvant chemotherapy (NAC) has been widely used for down-staging of locally advanced breast cancer, expanding indications for breast-conserving surgery and/or selecting response-guided adjuvant therapy in patients with primary breast cancer [1]. Pathological complete response (pCR), residual cancer burden (RCB), clinical-pathologic scoring system (CPS), and biological features of residual tumors have been used as measures of the efficacy of NAC, and could predict the outcome of the patients [2,3,4,5,6,7,8].
It is known that the anti-tumor activity of NAC depends not only on the sensitivity of breast tumor cells to chemotherapy, but also on the status of intra-tumor microenvironments, such as immunological responses against tumor cells. The tumor cell proliferation rate, such as the Ki67 labeling index (LI), and intrinsic subtypes of tumor cells are reported to be important predictors for responses to NAC [9,10]. Intra-tumor immunity, such as the amount and distribution of tumor-infiltrating lymphocytes (TILs), and CD8-, CD4-, FoxP3-, PD-L1-, or PD-1-positive cells have been reported to correlate with responses to NAC [11].
In this study, we investigated various biological factors related to cell proliferation, apoptosis, cancer stem cells, epithelial-mesenchymal transition (EMT), and intra-tumor immune microenvironment using both pre- and post-NAC breast tumor samples in patients with non-pCR to NAC. Their pre- and post-NAC status and changes after NAC were analyzed to explore the relationships among pathological responses to NAC and patients’ outcome, such as disease-free survival (DFS) and overall survival (OS).
2. Results
2.1. Correlation between biomarkers and pathological responses to NAC
Biomarker analyses using pre-NAC samples revealed that positivity for CD8, CD4, or PD-1 expression was significantly correlated with a better pathological response grade 2 to NAC [12]. In addition, the positivity of TILs, PD-L1 or FoxP3 tended to correlate with the grade 2. In contrast, no other pre-NAC biomarker, such as cell proliferation or apoptosis, correlated with the response to NAC (Table 1).
Similarly, biomarker analyses using post-NAC samples revealed that positivity for CD8 and PD-L1 significantly correlated with grade 2. The positivity of TILs tended to correlate with grade 2 (Table 2).
Changes such as an increase in biomarker levels after NAC did not correlate with grade 2 at all (data not shown).
Representative microphotographs of TILs and the immunostaining for CD8 are shown in Figure 1.
2.2. Correlation between biomarkers and DFS
Univariate biomarker analyses using pre-NAC samples revealed no significant correlation with DFS in this study subjects (Table 3).
Univariate biomarker analyses using post-NAC samples revealed that positivity for the EMT-related factors ZEB1 and vimentin, NG 3 and v-positive (v+) was significantly correlated with a worse DFS. In addition, histological grade (HG) 3 tended to be correlated with a worse DFS (Table 4).
Increases in the expression levels of the EMT-related factors ZEB1 and vimentin were significantly correlated with a worse DFS by univariate analysis (Table 5).
Multivariate biomarker analyses using pre-NAC and post-NAC samples and changes in biomarker levels revealed that v+ in post-NAC samples and an increase in the expression levels of vimentin were independent predictive factors for worse DFS. The hazard rate (HR) was 7.52, the 95% confidence interval (CI) was 3.01–32.26, and P = 0.0070 for v+. HR was 4.69, the 95% CI was 1.08–20.41, and P = 0.0388 for the vimentin increase.
Representative microphotographs of the immunostaining for ZEB1 and vimentin are shown in Figure 2.
2.3. Correlation between biomarkers and OS
Univariate biomarker analyses using pre-NAC samples revealed no significant correlation with OS in this study’s subjects (Table 3).
Univariate biomarker analyses using post-NAC samples revealed that positivity for ZEB1 and vimentin, NG 3 and v+ was significantly correlated with a worse OS. In addition, HG 3 tended to be correlated with a worse OS (Table 4).
Increases in the expression levels of ZEB1 and vimentin were significantly correlated with a worse OS by univariate analysis (Table 5).
Multivariate biomarker analyses using pre-NAC and post-NAC samples and changes in biomarker levels revealed that v+ in post-NAC samples and an increase in the expression levels of vimentin were independent predictive factors for worse OS. HR was 12.2, the 95% CI was 2.19–66.67, and P = 0.0043 for v+. HR was 14.2, the 95% CI was 2.23–90.91, and P = 0.0048 for the vimentin increase.
These findings indicated that all prognostic factors for DFS and OS based on multivariate analyses were identical in this study.
3. Discussion
NAC for primary breast cancer patients is currently widely used in daily practice. It is well known that breast cancer patients with pCR to NAC have a significantly better outcome than those with non-pCR to NAC [2]. Additional postoperative adjuvant therapies are clearly needed to improve the outcome of non-pCR patients. However, a section of non-pCR patients have a relatively better outcome after standard adjuvant therapy. In such patients, additional adjuvant therapy is unnecessary. Therefore, an accurate prediction of the outcome of non-pCR patients is needed for a better personalized medicine.
To predict the outcome of non-pCR patients to NAC, several predictors have been investigated. One simple predictive system is the CPS. The CPS includes only clinical and pathologic AJCC substages. This system emphasized that the addition of post-NAC pathological substaging to pre-NAC clinical substaging significantly improved the prediction of the outcome of patients treated with NAC. In addition, further analysis revealed that estrogen receptor-negative and NG 3 were independent risk factors for poor prognosis, and these variables were added to the CPS to create a second scoring system, the CPS-EG system. The CPS-EG system provided a significantly more accurate prediction of the outcome [4]. The other widely-used system to improve prognostic information in patients treated with NAC is the RCB. The RCB is calculated as a continuous index combining pathologic measurements of the primary tumor and nodal metastases. The RCB was independently prognostic for distant relapse-free survival in a multivariate model including a pCR category, and can be used to define categories of near-complete response and chemotherapy resistance [3]. Recently, a large pooled analysis indicated that RCB was independently prognostic in all subtypes of breast cancer, and generalisable to multiple practice settings [13].
Furthermore, a number of biomarkers and their combination with standard clinico-pathological factors, such as nomograms, have been explored to improve the outcome prediction of breast cancer patients with non-pCR to NAC. These biomarkers include the tumor cell proliferation marker Ki67 LI, the cancer stem cell marker ALDH, the EMT markers ZEB1 and vimentin, the intra-tumor immune microenvironment marker TILs, the immune check point inhibitor PD-L1, and the invasive potential marker lympho-vascular invasion [5,6,7,8,9,10,11,13,14,15,16,17,18,19,20,21]. Most of these biomarkers were investigated in pre-NAC and/or post-NAC samples. As we hypothesized that changes in biomarker status after NAC might be important prognostic factors in patients with non-pCR to NAC, pre- and post-NAC status and changes in their status were investigated all together in this study.
Two independent prognostic factors, v+ and vimentin up-regulation, in post-NAC samples were selected based on the multivariate analysis in this study. It is difficult to evaluate v in pre-NAC samples due to the limited quantity of pre-NAC core needle biopsy samples. Positivity for v in post-NAC samples may demonstrate a high invasive capacity of residual tumor cells.
A higher expression level of vimentin in either pre-NAC samples or post-NAC samples has been suggested to correlate with worse prognosis in patients treated with NAC [15,16]. To the best of our knowledge, this study suggests for the first time that the up-regulation of vimentin in residual tumor cells may render a worse outcome in patients, that is, recurrence and cancer-related death. However, it should be noted that vimentin up-relation was found in only 3 patients with triple-negative breast cancer (TNBC) in this study. The prognostic roles of up-regulation of vimentin in residual tumor cells after NAC should be explored in other subtypes of breast cancer. Interestingly, a transcription factor, ZEB1, was a worse predictive factor for DFS and OS by univariate analysis in this study. Only 1 patient with a ZEB1- and vimentin-positive post-NAC tumor showed recurrence and died of breast cancer at a very early stage after curative surgery. Further investigation is clearly needed regarding the prognostic significance of ZEB1 in breast cancer patients with non-pCR to NAC.
Expression of vimentin, an EMT marker, in breast cancer cells has been indicated to be higher in TNBCs [22]. A higher expression level of vimentin in tumor cells was also reported to frequently make TNBCs progress during NAC [23]. Furthermore, some experimental studies have suggested that vimentin is involved in the chemotherapeutic treatment-induced enhancement of TNBC aggressiveness and the promotion of TNBC invasion and metastasis [24,25]. These findings strongly suggest that vimentin expression may play a pivotal role in promoting resistance to NAC and metastasis in TNBCs. Therefore, the up-regulation of vimentin expression after NAC presented in this study may be caused by the survival advantage of chemo-resistant vimentin-positive tumor cells. It is also plausible that vimentin-positive TNBC cells preferentially induce metastasis, recurrence, and cancer-related death. Vimentin could be considered as a new target in preventing drug resistance and recurrence of TNBCs.
Pre- and post-NAC status and changes after NAC in intra-tumor immune-related factors, TILs, and CD-8, CD-4, FoxP3, PD-L1, and PD-1 did not show any significant correlation with DFS and OS in this study (Table 1). A higher proportion of stromal TILs and a higher expression of PD-L1 in tumor tissues after NAC have been reported to correlate with a better outcome in patients [17,18]. Negative results of the prognostic roles of these immune-related factors in this study may be caused by the limited number of subjects and the distribution of subtypes in the breast tumors tested.
Recent studies have shown that the anti-tumor activity of NAC depends not only on tumor cell sensitivity to chemotherapy, but also on intra-tumor microenvironments such as immune-related factors [11]. As pathological responses to NAC in non-pCR cases seemed to be quite different between grade 2 (a relatively strong response) and grade 0 or 1 (no or a weak response) according to the evaluation criteria defined by the Japanese Breast Cancer Society [12], we decided to investigate the relationships among pre- and post-NAC biomarker status, their changes after NAC, and the pathological response grade 2 in subjects of this study. Although any biomarkers related to tumor cell characteristics, such as Ki67 LI, were not significantly correlated with pathological responses to NAC, the positivity of TILs, CD-8, CD-4, PD-L1, and/or PD-1 in either pre- or post-NAC samples was associated with a significantly better response in grade 2 ( Table 1; Table 2). Interestingly, expression levels of immune-related factors did not significantly change after NAC in tumor tissues (data not shown). These findings suggest that the activation of intra-tumor immunity in pre-NAC tumors may play a role in the anti-tumor activity of NAC, and that the activation may not be strongly influenced by NAC in tumor tissues.
There are several limitations to this study, including the small number of study subjects, the fact that the NAC protocols and distribution of subtypes were not homogeneous, and the limited number of biomarkers tested. In particular, the effects of biomarker status in tumor tissues on the responses to NAC and the outcome of patients seemed to depend on the subtype classification of breast cancers [10]. As previously described, the up-regulation of vimentin may play an important role in the outcome of patients with TNBCs. Validation studies to clarify the prognostic utility of vimentin expression are clearly needed using each subtype of breast cancers. However, this small-scaled exploratory study has indicated that activated intra-tumor immune microenvironments may play an important role in pathological responses to NAC, and that the up-regulation of vimentin and v+ in the residual tumors may be pivotal prognostic factors in non-pCR cases to NAC. Enhancement of intra-tumor immunity before the NAC introduction using pre-operative radiotherapy or immune-potentiating agents might provide a greater anti-tumor activity of NAC [27,28,29]. Additionally, anti-EMT agents together with NAC might improve the outcome of patients with TNBCs [30,31].
4. Patients and Methods
4.1. Characteristics of the study subjects
A total of 35 primary breast cancer patients were treated with NAC between January 2010 and December 2011 at the Department of Breast and Thyroid Surgery, Kawasaki Medical School Hospital. The subjects of this study were 24 patients out of the 35 patients who had non-pCR to NAC, and breast tumor samples both before NAC (core-needle biopsy samples) and after NAC (surgically excised samples) were available for the examinations of various biological factors.
The median age of the subjects was 53 years-old (range: 30–67). Ten patients had stage II and 14 had stage III breast cancer before NAC. There were 23 cases of invasive ductal carcinomas and 1 case of invasive lobular carcinoma after NAC. The tumors were categorized as hormone receptor (HR)-negative and human epidermal growth factor receptor (HER)-negative subtype in 10 patients, HR-positive and HER2-negative subtype in 10 patients, HR-negative and HER2-positive subtype in 2 patients, and HR-positive and HER2-positive subtype in 2 patients after NAC. The clinical response rate was 50%, and pathological responses were categorized as grade 0 in 1 patient, grade 1 in 17 patients, and grade 2 in 6 patients [12].
NAC was administered with epirubicin + cyclophosphamide (EP) in 7 patients, EP + docetaxel + doxifluridine (DF) in 15 patients, EP + DF with trastuzumab in 1 patient and DF + trastuzumab in 1 patient. Total mastectomy was performed in 19 patients and breast-conserving surgery in 5 patients. Axillary dissection was performed in 23 patients and the sentinel node biopsy in 1 patient. As the postoperative adjuvant therapy, radiotherapy was performed in 12 patients, endocrine therapy in 12 patients, and trastuzumab therapy in 4 patients. The median observation time was 103 months for DFS and 110 months for OS, respectively. Recurrence and cancer-related death were observed in 12 and 8 out of the 24 patients, respectively,
4.2. Biomarker measurements and evaluations
To explore pre- and post-NAC status and changes after NAC in various biological factors either in tumor cells or intra-tumor microenvironments, we investigated, using both pre-NAC and post-NAC samples, the Ki-67 LI as a cell proliferation marker, apoptosis in tumor cells by the TUNEL method, expression levels of ZEB1 and vimentin in tumor cells as EMT markers, those of Bmi-1 and aldehyde dehydrogenase (ALDH) in tumor cells as cancer stem cell markers, and stromal TILs and expression levels of CD8, CD4, FoxP3, PD-L1, and PD-1 in tumor tissues as immunological biomarkers. Stromal TILs were evaluated from hematoxylin and eosin stained sections of tumor samples using a previously published method [32]. Briefly, quantification of TILs in the tumor stroma was recorded as a percentage of the occupied stromal areas. The procedures and conditions to examine the other biomarkers are shown in Table 6.
Positive or negative cut-off values were defined as 20% for Ki67 LI in nuclear staining, 1% for apoptosis, 10% for ZEB1 in cytoplasmic staining [33], 25% for E-cadherin in membrane staining [34], 10% for vimentin in cytoplasmic staining [35], 50% for Bmi-1 in nuclear staining, 10% for ALDH in cytoplasmic staining, and 50% for stromal TILs. A score of 4, based on the combined positive score system recommended by the recommendation by Agilent Dako Co., was defined as positive for PD-L1 staining. The immune staining for CD8, CD4, FoxP3, and PD-1 was categorized as scores of 1 to 3 (weak to strong) and a score of 3 was defined as positive.
Following the evaluation criteria defined by the Japanese Breast Cancer Society [12], the pathological responses to NAC were categorized as grade 0 to 3 (no response to pCR). Grade 2 (a strong degraded changes in invasive tumor cells in more than two-thirds of the tumor area or near pCR status) was defined as a better response, and grade 0 or 1 was defined as a poor response in non-pCR samples in this study.
Positivity for HR was defined as more than or equal to 1% in tumor cells. That of HER2 was defined as 3+ for the immune-histochemical score or 2+ combined with a positive result for the fluorescence in-situ hybridization method. Lymphatic invasion and v were basically evaluated with hematoxylin-eosin staining. When necessary, Elastica-Masson staining or Victoria blue staining was additionally performed.
Histopathological evaluation was performed by two certificated pathologists (T.M. and F.S.) in a blinded manner.
4.3. Statistical analysis
The relationships between pathological responses to NAC and pre- or post-NAC status or changes in various biomarkers were analyzed using the contingency table and chi-square test or Fisher’s exact test. Univariate analysis on DFS and OS was performed using the Kaplan-Meier method and logrank test. Multivariate analysis was performed using the Cox proportional hazards model. The final regression model was selected using the forward stepwise method. P < 0.05 was defined as statistically significant.
Author Contributions
Conceptualization, J.K. and Y.Y.; methodology, J.K., T.I., T.M. (Tomoka Mikami), F.S. and T.M. (Takuya Moriya), software, J.K.; investigation, J.K., T.I., T.M. () and F.S.; data curation, J.K., Y.K. and Y.Y.; writing, J.K. and T.I.; visualization, T.M. (Tomoka Mikami), F.S. and T.M. (Takuya Moriya); supervision, T.M. (Takuya Moriya) and N.T.; project administration, J.K., T.I., Y.K. and Y.Y.; funding acquisition, J.K. and Y.Y. All authors read and agreed to the final version of the manuscript.
Funding
This study was supported by a Research Project Grant from Kawasaki Medical School (R03-004).
Institutional Review Board Statement
The protocol of this study was approved by the Ethical Committee of Kawasaki Medical School and Hospital.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, J.K., upon reasonable request.
Acknowledgments
We thank Wataru Saitoh of Miyake Ohfuku Clinic for his contribution to patient selection and obtaining pathological samples and Kaoru Tsuboi and Megumi Kuriyama for their technical assistance. Junichi Kurebayashi has been working as a visiting researcher at the Department of Breast and Thyroid Surgery, Kawasaki Medical School.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Untch, M.; Blohmer, J.-U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and Impact of Pathologic Complete Response on Prognosis After Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef]
- Symmans, W.F.; Wei, C.; Gould, R.; Yu, X.; Zhang, Y.; Liu, M.; Walls, A.; Bousamra, A.; Ramineni, M.; Sinn, B.; et al. Long-Term Prognostic Risk After Neoadjuvant Chemotherapy Associated With Residual Cancer Burden and Breast Cancer Subtype. J. Clin. Oncol. 2017, 35, 1049–1060. [Google Scholar] [CrossRef]
- Mittendorf, E.A.; Jeruss, J.S.; Tucker, S.L.; Kolli, A.; Newman, L.A.; Gonzalez-Angulo, A.M.; Buchholz, T.A.; Sahin, A.A.; Cormier, J.N.; Buzdar, A.U.; et al. Validation of a Novel Staging System for Disease-Specific Survival in Patients With Breast Cancer Treated With Neoadjuvant Chemotherapy. J. Clin. Oncol. 2011, 29, 1956–1962. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Vila, J.; Tucker, S.L.; Chavez-MacGregor, M.; Smith, B.D.; Symmans, W.F.; Sahin, A.A.; Hortobagyi, G.N.; Hunt, K.K. The Neo-Bioscore Update for Staging Breast Cancer Treated With Neoadjuvant Chemotherapy. JAMA Oncol. 2016, 2, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Lan, A.; Li, H.; Chen, J.; Shen, M.; Jin, Y.; Dai, Y.; Jiang, L.; Dai, X.; Peng, Y.; Liu, S. Nomograms for Predicting Disease-Free Survival Based on Core Needle Biopsy and Surgical Specimens in Female Breast Cancer Patients with Non-Pathological Complete Response to Neoadjuvant Chemotherapy. J. Pers. Med. 2023, 13, 249. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wu, S.; Xing, H.; Han, M.; Li, J.; Liu, Y. Development and Validation of a Novel Model for Predicting Prognosis of Non-PCR Patients After Neoadjuvant Therapy for Breast Cancer. Front. Oncol. 2021, 11, 675533. [Google Scholar] [CrossRef]
- Hou, N.; Wu, J.; Xiao, J.; Wang, Z.; Song, Z.; Ke, Z.; Wang, R.; Wei, M.; Xu, M.; Wei, J.; et al. Development, verification, and comparison of a risk stratification model integrating residual cancer burden to predict individual prognosis in early-stage breast cancer treated with neoadjuvant therapy. ESMO Open 2021, 6, 100269. [Google Scholar] [CrossRef]
- Tao, M.; Chen, S.; Zhang, X.; Zhou, Q. Ki-67 labeling index is a predictive marker for a pathological complete response to neoadjuvant chemotherapy in breast cancer. Medicine 2017, 96, e9384. [Google Scholar] [CrossRef]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Dieci, M.V.; Miglietta, F.; Guarneri, V. Immune Infiltrates in Breast Cancer: Recent Updates and Clinical Implications. Cells 2021, 10, 223. [Google Scholar] [CrossRef] [PubMed]
- Kurosumi, M.; Akashi-Tanaka, S.; Akiyama, F.; Komoike, Y.; Mukai, H.; Nakamura, S.; Tsuda, H. ; (Committee for Production of Histopathological Criteria for Assessment of Therapeutic Response of the Japanese Breast Cancer Society) Histopathological criteria for assessment of therapeutic response in breast cancer (2007 version). Breast Cancer 2007, 15, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Yau, C.; Osdoit, M.; van der Noordaa, M.; Shad, S.; Wei, J.; de Croze, D.; Hamy, A.-S.; Laé, M.; Reyal, F.; Sonke, G.S.; et al. Residual cancer burden after neoadjuvant chemotherapy and long-term survival outcomes in breast cancer: a multicentre pooled analysis of 5161 patients. Lancet Oncol. 2021, 23, 149–160. [Google Scholar] [CrossRef]
- Xie, L.-Y.; Wang, K.; Chen, H.-L.; Shi, Y.-X.; Zhang, Y.-Q.; Lin, H.-Y.; Liang, Y.-K.; Xiao, Y.-S.; Wu, Z.-Y.; Yuan, Z.-Y.; et al. Markers Associated With Tumor Recurrence in Patients With Breast Cancer Achieving a Pathologic Complete Response After Neoadjuvant Chemotherapy. Front. Oncol. 2022, 12, 860475. [Google Scholar] [CrossRef]
- Wu, Z.; Zhang, L.; Xu, S.; Lin, Y.; Yin, W.; Lu, J.; Sha, R.; Sheng, X.; Zhou, L.; Lu, J. Predictive and prognostic value of ZEB1 protein expression in breast cancer patients with neoadjuvant chemotherapy. Cancer Cell Int. 2019, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Elzamly, S.; Badri, N.; Padilla, O.; Dwivedi, A.K.; A Alvarado, L.; Hamilton, M.; Diab, N.; Rock, C.; Elfar, A.; Teleb, M.; et al. Epithelial-Mesenchymal Transition Markers in Breast Cancer and Pathological Responseafter Neoadjuvant Chemotherapy. Breast Cancer: Basic Clin. Res. 2018, 12. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; Von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: A pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef]
- Chen, S.; Wang, R.-X.; Liu, Y.; Yang, W.-T.; Shao, Z.-M. PD-L1 expression of the residual tumor serves as a prognostic marker in local advanced breast cancer after neoadjuvant chemotherapy. Int. J. Cancer 2017, 140, 1384–1395. [Google Scholar] [CrossRef]
- Liu, Y.L.; Saraf, A.; Lee, S.M.; Zhong, X.; Hibshoosh, H.; Kalinsky, K.; Connolly, E.P. Lymphovascular invasion is an independent predictor of survival in breast cancer after neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2016, 157, 555–564. [Google Scholar] [CrossRef]
- Hamy, A.-S.; Lam, G.-T.; Laas, E.; Darrigues, L.; Balezeau, T.; Guerin, J.; Livartowski, A.; Sadacca, B.; Pierga, J.-Y.; Vincent-Salomon, A.; et al. Lymphovascular invasion after neoadjuvant chemotherapy is strongly associated with poor prognosis in breast carcinoma. Breast Cancer Res. Treat. 2018, 169, 295–304. [Google Scholar] [CrossRef]
- Ryu, Y.J.; Kang, S.J.; Cho, J.S.; Yoon, J.H.; Park, M.H. Lymphovascular invasion can be better than pathologic complete response to predict prognosis in breast cancer treated with neoadjuvant chemotherapy. Medicine 2018, 97, e11647. [Google Scholar] [CrossRef] [PubMed]
- Karihtala, P.; Auvinen, P.; Kauppila, S.; Haapasaari, K.-M.; Jukkola-Vuorinen, A.; Soini, Y. Vimentin, zeb1 and Sip1 are up-regulated in triple-negative and basal-like breast cancers: association with an aggressive tumour phenotype. Breast Cancer Res. Treat. 2013, 138, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, Y.; Tsuda, H.; Yoshida, M.; Yunokawa, M.; Yonemori, K.; Shimizu, C.; Yamamoto, S.; Kinoshita, T.; Fujiwara, Y.; Tamura, K. Pathological features of triple-negative breast cancers that showed progressive disease during neoadjuvant chemotherapy. Cancer Sci. 2017, 108, 1520–1529. [Google Scholar] [CrossRef] [PubMed]
- Grasset, E.M.; Dunworth, M.; Sharma, G.; Loth, M.; Tandurella, J.; Cimino-Mathews, A.; Gentz, M.; Bracht, S.; Haynes, M.; Fertig, E.J.; et al. Triple-negative breast cancer metastasis involves complex epithelial-mesenchymal transition dynamics and requires vimentin. Sci. Transl. Med. 2022, 14, eabn7571. [Google Scholar] [CrossRef]
- Winter, M.; Meignan, S.; Völkel, P.; Angrand, P.-O.; Chopin, V.; Bidan, N.; Toillon, R.-A.; Adriaenssens, E.; Lagadec, C.; Le Bourhis, X. Vimentin Promotes the Aggressiveness of Triple Negative Breast Cancer Cells Surviving Chemotherapeutic Treatment. Cells 2021, 10, 1504. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; Loibl, S.; Noske, A.; Roller, M.; Müller, B.M.; Komor, M.; Budczies, J.; Darb-Esfahani, S.; Kronenwett, R.; Hanusch, C.; et al. Tumor-Associated Lymphocytes As an Independent Predictor of Response to Neoadjuvant Chemotherapy in Breast Cancer. J. Clin. Oncol. 2010, 28, 105–113. [Google Scholar] [CrossRef]
- Williamson, C.W.; Sherer, M.V.; Zamarin, D.; Sharabi, A.B.; Dyer, B.A.; Mell, L.K.; Mayadev, J.S. Immunotherapy and radiation therapy sequencing: State of the data on timing, efficacy, and safety. Cancer 2021, 127, 1553–1567. [Google Scholar] [CrossRef]
- Ying-Rui, M.; Bu-Fan, B.; Deng, L.; Rong, S.; Qian-Mei, Z. Targeting the stimulator of interferon genes (STING) in breast cancer. Front. Pharmacol. 2023, 14, 1199152. [Google Scholar] [CrossRef]
- Pratelli, G.; Carlisi, D.; Di Liberto, D.; Notaro, A.; Giuliano, M.; D’anneo, A.; Lauricella, M.; Emanuele, S.; Calvaruso, G.; De Blasio, A. MCL1 Inhibition Overcomes the Aggressiveness Features of Triple-Negative Breast Cancer MDA-MB-231 Cells. Int. J. Mol. Sci. 2023, 24, 11149. [Google Scholar] [CrossRef]
- Hashemi, M.; Arani, H.Z.; Orouei, S.; Fallah, S.; Ghorbani, A.; Khaledabadi, M.; Kakavand, A.; Tavakolpournegari, A.; Saebfar, H.; Heidari, H.; et al. EMT mechanism in breast cancer metastasis and drug resistance: Revisiting molecular interactions and biological functions. Biomed. Pharmacother. 2022, 155, 113774. [Google Scholar] [CrossRef]
- Cho, E.S.; Kang, H.E.; Kim, N.H.; Yook, J.I. Therapeutic implications of cancer epithelial-mesenchymal transition (EMT). Arch. Pharmacal Res. 2019, 42, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef] [PubMed]
- .Zhang, W.; Shi, X.; Peng, Y.; Wu, M.; Zhang, P.; Xie, R.; Wu, Y.; Yan, Q.; Liu, S.; Wang, J. HIF-1α Promotes Epithelial-Mesenchymal Transition and Metastasis through Direct Regulation of ZEB1 in Colorectal Cancer. PLOS ONE 2015, 10, e0129603. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Ma, X.; Li, Y.; He, Y.; Huang, D.; Cai, S.; Peng, J. The Characteristics and Prognostic Effect of E-Cadherin Expression in Colorectal Signet Ring Cell Carcinoma. PLOS ONE 2016, 11, e0160527. [Google Scholar] [CrossRef]
- Tian, W.; Yang, Y.; Qin, Q.; Zhang, L.; Wang, Z.; Su, L.; Zeng, L.; Chen, H.; Hu, L.; Hong, J.; et al. Vimentin and tumor–stroma ratio for neoadjuvant chemoradiotherapy response prediction in locally advanced rectal cancer. Cancer Sci. 2022, 114, 619–629. [Google Scholar] [CrossRef]
Figure 1.
Representative microphotographs of stromal TILs and immunostaining for CD8 in the study samples (X200, HPF). (A) The level of stromal TILs was more than 50% in this sample. (B) The level of stromal TILs was less than 10% in this sample. (C) More than 50% of stromal TILs showed positive staining for CD8 in this sample. (D) No stromal TILs showed positive staining for CD8 in this sample.
Figure 1.
Representative microphotographs of stromal TILs and immunostaining for CD8 in the study samples (X200, HPF). (A) The level of stromal TILs was more than 50% in this sample. (B) The level of stromal TILs was less than 10% in this sample. (C) More than 50% of stromal TILs showed positive staining for CD8 in this sample. (D) No stromal TILs showed positive staining for CD8 in this sample.
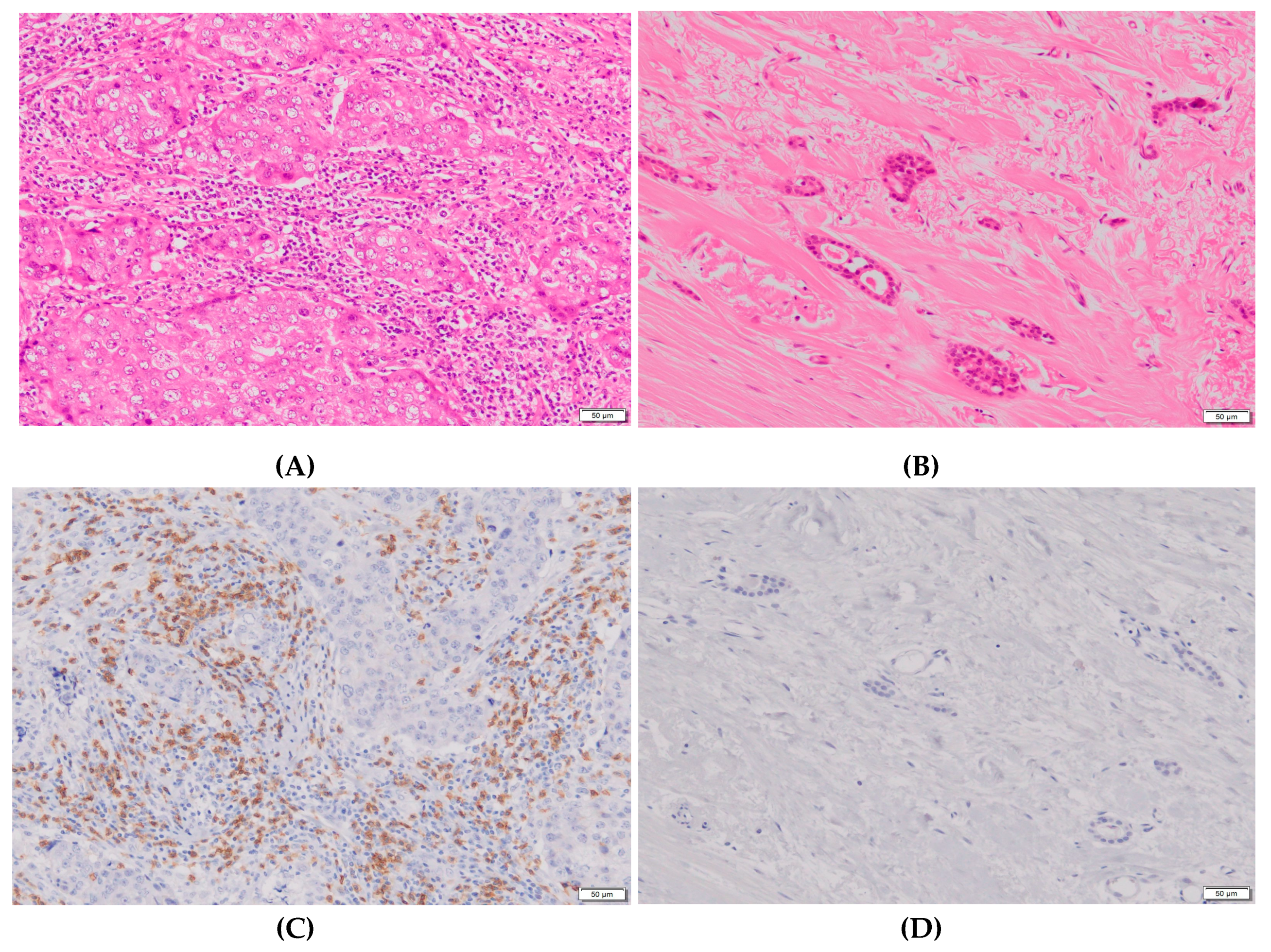
Figure 2.
Representative microphotographs of immunostaining for ZEB1 and vimentin in the study samples (X200, HPF). (A) More than 10% of tumor cells showed positive cytoplasmic staining for ZEB1 in this sample. (B) No tumor cells showed positive staining for ZEB1 in this sample. (C) More than 10% of tumor cells showed positive cytoplasmic staining for vimentin in this sample. (D) No tumor cells showed positive staining for vimentin in this sample.
Figure 2.
Representative microphotographs of immunostaining for ZEB1 and vimentin in the study samples (X200, HPF). (A) More than 10% of tumor cells showed positive cytoplasmic staining for ZEB1 in this sample. (B) No tumor cells showed positive staining for ZEB1 in this sample. (C) More than 10% of tumor cells showed positive cytoplasmic staining for vimentin in this sample. (D) No tumor cells showed positive staining for vimentin in this sample.
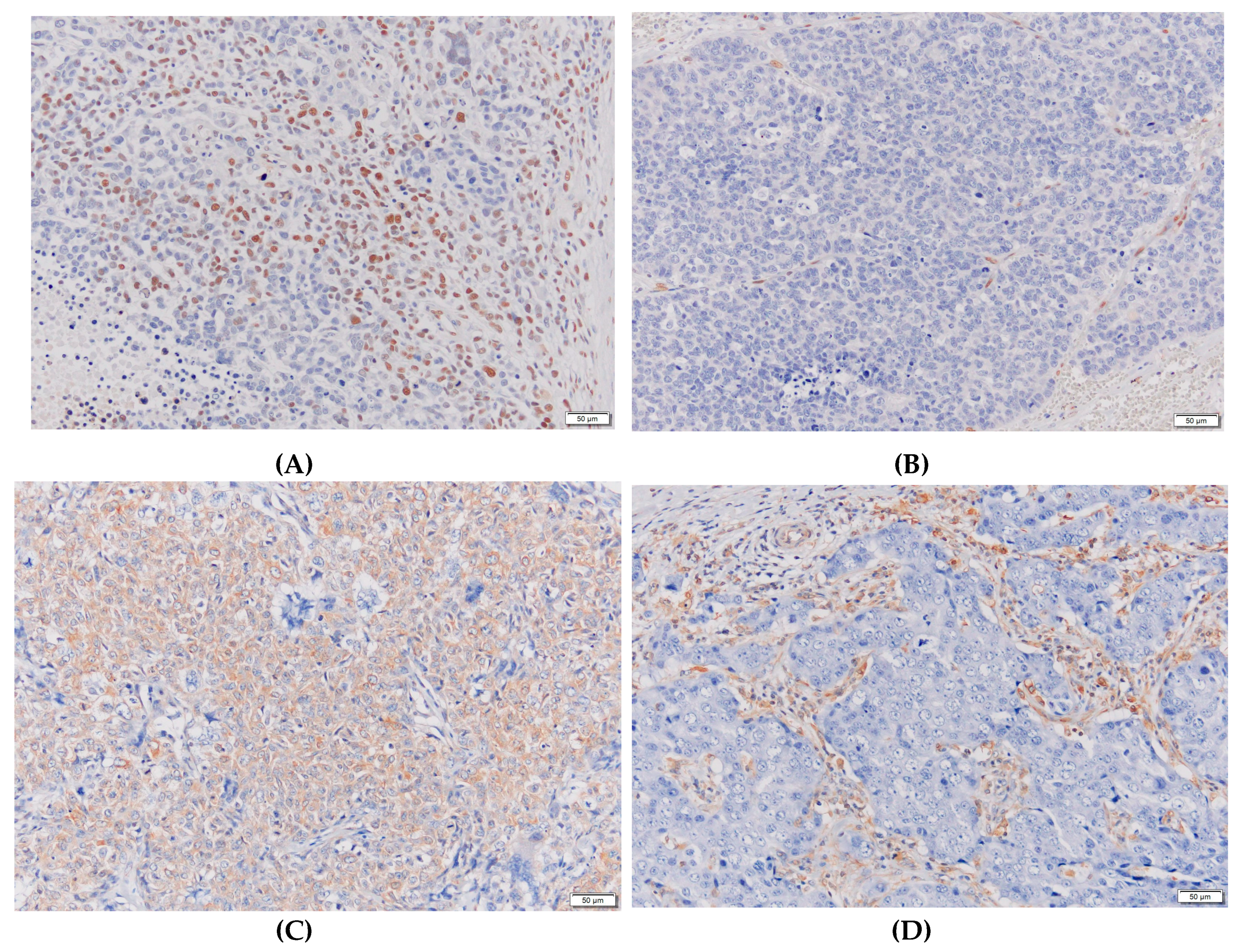

Table 1.
Correlations between biomarkers and pathological responses to NAC in pre-NAC samples.
| Biomarkers | Classification | Number of cases | Rate of grade 2 | P-value |
|---|---|---|---|---|
| Ki67LI | < 20% | 8 | 25% | NS* |
| > 20% | 15 | 27% | ||
| Apoptosis | < 1% | 7 | 14% | NS |
| > 1% | 17 | 29% | ||
| ZEB1 | < 10% | 24 | 25% | NA** |
| > 10% | 0 | |||
| Vimentin | < 10% | 24 | 25% | NA |
| > 10% | 0 | |||
| E-cadherin | < 25% | 3 | 0% | NS |
| > 25% | 21 | 29% | ||
| Bmi-1 | < 50% | 5 | 0% | NS |
| > 50% | 19 | 32% | ||
| ALDH | < 10% | 20 | 25% | NS |
| > 10% | 4 | 25% | ||
| TILs | < 50% | 21 | 19% | 0. 0748 (trend) |
| > 50% | 3 | 67% | ||
| PD-L1 | Scores 0–3 | 15 | 13% | 0.0884 (trend) |
| Score 4 | 9 | 44% | ||
| PD-1 | Score 1 or 2 | 19 | 11% | 0.0014 |
| Score 3 | 5 | 80% | ||
| CD8 | Score 1 or 2 | 20 | 15% | 0.0114 |
| Score 3 | 4 | 75% | ||
| CD4 | Score 1 or 2 | 21 | 14% | 0.0053 |
| Score 3 | 3 | 100% | ||
| FoxP3 | Score 1 or 2 | 21 | 19% | 0.0748 (trend) |
| Score 3 | 3 | 67% |
*NS, not significant; **NA, not assessable.
Table 2.
Correlations between biomarkers and pathological responses to NAC in post-NAC samples.
| Biomarkers | Classification | Number of cases | Rate of grade 2 | P-value |
|---|---|---|---|---|
| Ki67LI | < 20% | 9 | 33% | NS* |
| > 20% | 15 | 20% | ||
| Apoptosis | < 1% | 10 | 30% | NS |
| > 1% | 13 | 23% | ||
| ZEB1 | < 10% | 23 | 26% | NS |
| > 10% | 1 | 0% | ||
| Vimentin | < 10% | 21 | 29% | NS |
| > 10% | 3 | 0% | ||
| E-cadherin | < 25% | 7 | 14% | NS |
| > 25% | 17 | 29% | ||
| Bmi-1 | < 50% | 5 | 0% | NS |
| > 50% | 19 | 32% | ||
| ALDH | < 10% | 15 | 27% | NS |
| > 10% | 9 | 22% | ||
| TILs | < 50% | 21 | 19% | 0.0748 (trend) |
| > 50% | 3 | 67% | ||
| PD-L1 | Scores 0–3 | 17 | 12% | 0.0196 |
| Score 4 | 7 | 57% | ||
| PD-1 | Score 1 or 2 | 21 | 24% | NS |
| Score 3 | 3 | 33% | ||
| CD8 | Score 1 or 2 | 20 | 15% | 0.0114 |
| Score 3 | 4 | 75% | ||
| CD4 | Score 1 or 2 | 24 | 25% | NA** |
| Score 3 | 0 | |||
| FoxP3 | Score 1 or 2 | 22 | 23% | NS |
| Score 3 | 2 | 50% |
*NS, not significant; **NA, not assessable.
Table 3.
Correlations between biomarkers and DFS/OS in pre-NAC samples.
| Biomarkers | Classification | Number of cases | DFS | OS |
|---|---|---|---|---|
| P-value | P-value | |||
| Ki67LI | < 20% | 8 | NS* | NS |
| > 20% | 15 | |||
| Apoptosis | < 1% | 7 | NS | NS |
| > 1% | 17 | |||
| ZEB1 | < 10% | 24 | NA** | NA |
| > 10% | 0 | |||
| Vimentin | < 10% | 24 | NA | NA |
| > 10% | 0 | |||
| E-cadherin | < 25% | 3 | NE*** | NE |
| > 25% | 21 | |||
| Bmi-1 | < 50% | 5 | NS | NS |
| > 50% | 19 | |||
| ALDH | < 10% | 20 | NS | NS |
| > 10% | 4 | |||
| TILs | < 50% | 21 | NE | NE |
| > 50% | 3 | |||
| PD-L1 | Scores 0–3 | 15 | NS | NS |
| Score 4 | 9 | |||
| PD-1 | Score 1 or 2 | 19 | NS | NS |
| Score 3 | 5 | |||
| CD8 | Score 1 or 2 | 20 | NS | NS |
| Score 3 | 4 | |||
| CD4 | Score 1 or 2 | 21 | NS | NS |
| Score 3 | 3 | |||
| FoxP3 | Score 1 or 2 | 21 | NE | NE |
| Score 3 | 3 |
*NS, not significant; **NA, not assessable; ***NE, not evaluable.
Table 4.
Correlations between biomarkers and DFS/OS in post-NAC samples.
| Biomarkers | Classification | Number of cases | DFS | OS |
|---|---|---|---|---|
| P-value | P-value | |||
| Ki67LI | < 20% | 9 | 0.0831 | NS* |
| > 20% | 15 | |||
| Apoptosis | < 1% | 10 | NS | NS |
| > 1% | 13 | |||
| ZEB1 | < 10% | 23 | 0.0014 | 0.0014 |
| > 10% | 1 | |||
| Vimentin | < 10% | 20 | 0.0255 | 0.005 |
| > 10% | 4 | |||
| E-cadherin | < 25% | 7 | NS | NS |
| > 25% | 17 | |||
| Bmi-1 | < 50% | 5 | NS | NS |
| > 50% | 19 | |||
| ALDH | < 10% | 15 | NS | NS |
| > 10% | 9 | |||
| TILs | < 50% | 21 | NE*** | NE |
| > 50% | 3 | |||
| PD-L1 | Scores 0–3 | 17 | NS | NS |
| Score 4 | 7 | |||
| PD-1 | Score 1 or 2 | 21 | NS | NE |
| Score 3 | 3 | |||
| CD8 | Score 1 or 2 | 20 | NE | NE |
| Score 3 | 4 | |||
| CD4 | Score 1 or 2 | 24 | NA** | NA |
| Score 3 | 0 | |||
| FoxP3 | Score 1 or 2 | 21 | NE | NS |
| Score 3 | 3 | |||
| ly | Negative | 6 | NE | NE |
| Positive | 18 | |||
| v | Negative | 20 | 0.0019 | 0.0032 |
| Positive | 4 | |||
| NG | 1 or 2 | 11 | 0.0446 | 0.0250 |
| 3 | 12 | |||
| HG | 1 or 2 | 12 | 0.0924 (trend) | 0.0696 (trend) |
| 3 | 11 | |||
| pN | Negative | 11 | NS | NS |
| Positive | 13 |
*NS, not significant; **NA, not assessable; ***NE, not evaluable.
Table 5.
Correlations between changes in biomarkers and DFS/OS.
| Biomarkers | Classification | Number of cases | DFS | OS |
|---|---|---|---|---|
| P-value | P-value | |||
| Ki67LI | Increase | 10 | NS* | NS |
| Apoptosis | Increase | 12 | NS | NS |
| ZEB1 | Increase | 1 | 0.0014 | 0.0014 |
| Vimentin | Increase | 3 | 0.0255 | 0.0050 |
| E-cadherin | Increase | 19 | NS | NS |
| Bmi-1 | Increase | 5 | NS | NS |
| ALDH | Increase | 8 | NS | NS |
| TILs | Increase | 6 | NS | NS |
| PD-L1 | Increase | 5 | NS | NS |
| PD-1 | Increase | 5 | NS | NS |
| CD8 | Increase | 5 | NS | NS |
| CD4 | Increase | 1 | NE*** | NE |
| FoxP3 | Increase | 3 | NS | NS |
*NS, not significant; ***NE, not evaluable.
Table 6.
Reagents, procedures, and conditions for the measurement of biomarkers tested in this study.
Table 6.
Reagents, procedures, and conditions for the measurement of biomarkers tested in this study.
| Biomarkers | Providers | Clone | Conditions |
|---|---|---|---|
| Ki67 | Dako | MIB-1 | Following provider's recommendation |
| TUNEL | Exalpha | Not applicable | Following provider's recommendation |
| ZEB1 | SantaCruz | H-102 | Dilution, ×200; incubation, 4 °C, overnight |
| E-Cadherin | Dako | NCH-38 | Dilution, ×100; incubation, room temperature, 30min |
| Vimentin (Ready to Use) | Dako | V9 | Dilution, ×1; incubation, room temperature, 30 min |
| Bmi-1 | abcam | EPR3745(2) | Dilution, ×400; incubation, room temperature, 60 min |
| ALDH | BD | 44/ALDH | Dilution, ×100; incubation, 4 °C, overnight |
| CD4 | Thermo | 4B12 | Dilution, ×10; incubation, room temperature, 60 min |
| CD8 | Thermo | SP16 | Dilution, ×50; incubation, 4 °C, overnight |
| FoxP3 | abcam | 236A/E7 | Dilution, ×100; incubation, 4 °C, overnight |
| PD-L1 | abcam | 28-8 | Dilution, ×200; incubation, room temperature, 60 min |
| PD-1 | abcam | NAT105 | Dilution, ×100; mechanical staining |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



