
Submitted:
09 October 2023
Posted:
10 October 2023
You are already at the latest version
Abstract
Infective endocarditis (IE) is a serious condition with a high mortality rate, even after surgery. Need for transfusion might be increased in surgery for IE. This review aims to identify the predictors for the need of transfusion in IE patients and the effect of transfusion on outcome. Only 17 manuscripts could be identified partially addressing this issue. Minimal access surgery and valve repair instead of replacement seems favorable in this respect. However, IE has opposing effects on the coagulation system with increase in bleeding and thromboembolic events. There are indications that in IE patients, transfusion need is higher but this might be compounded by the complexity of surgery and a prolonged cardiopulmonary bypass (CPB) time. Since organ dysfunction is associated with IE, this comorbidity could cloud the effect of the need for transfusion on outcome. To avoid potential adverse effect of transfusion, alternative methods have been proposed such as the use of cytokine absorbers during CPB run, intraoperative cell salvage and acute normovolemic hemodilution. These methods need further study in this subgroup of patients. In the meantime, allogeneic transfusion should be kept at a minimum, using only recently stored blood, to minimize harmful effects.
Keywords:
infective endocarditis
; cardiac surgery
; transfusion
; mortality
1. Introduction
The incidence of infective endocarditis (IE) is approximately 15 in 100,000 and is increasing. This rise is related to the use of cardiac implants [1]. Survival after cardiac valve implants can be long, during which there is a low but continuous risk for the development of prosthetic valve IE [1] or for other comorbid conditions such as colorectal neoplasia, which can serve as port-of-entry for bacteremia and subsequent IE [2]. Mortality of IE can be up to 20% in the first month and 30% at 6 months [3]. In some patients, cardiac surgery is required because of persisting sepsis, intracardiac tissue destruction, hemodynamic deterioration [4] or persisting vegetation with risk for septic emboli. The optimal timing of surgery remains a major challenge. For routine cardiac surgery, 20% to 40% of the patients require transfusion [5]. In complex cases, the transfusion rate is higher [6], especially with repeat surgery, urgent surgery during ongoing sepsis, or prolonged cardiopulmonary bypass (CPB) time because of intracardiac damage. In all these conditions, there is a risk for with subsequent increase in surgical bleeding, which affects need for transfusion. IE itself has also an effect on coagulation: IE activates the primary precursors of the coagulation cascade. This leads to an increased reactivity of platelet and to the propagation of enhanced coagulation because of a decreased fibrinolysis [7]. Moreover, elevated fibrinogen levels are often documented in the acute phase of infection and inflammation [8]. This hypercoagulable state has been observed through laboratory parameters [9]. A viscoelastic testing by rotational thromboelastometry can be used to direct preoperative supplementation of fibrinogen in patients with IE needing cardiac reoperation. A good understanding of the coagulation status is necessary, to avoid unnecessary transfusion. Nevertheless, measurement of INR, PT and aPTT are not helpful while the patient is still on heparin. A blood count (RBC, platelets) may indicate the need for transfusion, but such a count does not supply information concerning the platelet function. Measurement of plasma fibrinogen might be useful [10]. Transfusion itself has also serious adverse effects in 1.1%, of the recipients [11], but this may be underreported. A relation between the number of transfused units and 30-day morbidity and mortality rate was documented [12]. Examples were transfusion-related acute lung injury [13] and infections [14], even after attempts of removal of white blood cells [15,16]. Compared to a liberal transfusion policy, a restricted transfusion policy was associated with less time in the intensive care unit, a shorter mechanical ventilation time, and a reduced length of stay in the hospital [17]. There are several pathophysiologic processes that occur progressively during RBCs aging in cold storage: accumulation of lactic acid, formation of methemoglobin, and of reactive oxygenated compounds, denaturation and precipitation of hemoglobin degradation products, and a reduced cytoskeletal deformability [18]. These changes reduce the capacity of the RBC pass through narrow vessels and to deliver oxygen effectively. Moreover, a median of 17.6% of the transfused allogeneic RBC are removed from the recipient’s circulation, either by spontaneous destruction or by phagocytosis [19]. This contributes to acidosis, hyperkaliemia, high levels of free heme, and oxidized iron. Patients could become more vulnerable to postoperative acute renal injury, arrhythmias and infection [18]. This problem is illustrated in one series of cardiac surgical patients: those receiving older RBCs were more likely to suffer systemic infection and fatality, compared to those who received more recently stored blood [20]. These effects would not be expected with autologous whole blood collection with short storage time. Avoidance of these adverse transfusion should be attempted in patients with IE, which are uniquely vulnerable. The research questions are: can the need for transfusion be predicted in patients undergoing cardiac surgery for IE and what are the consequences of blood transfusion in these patients
2. Materials and Methods
The used search terms for Web of Science were “endocarditis” AND “transfusion”, for the last 10 years. Exclusion criteria were no cardiac valve surgery, case reports, meeting abstracts, editorials, reviews, letters to the editor, and meta-analyses, pediatric cardiac surgery, endocarditis as consequence of transfusion for non-cardiac surgery or other reasons, trans-catheter procedures, extraction of permanent pacemaker leads, animal studies and non-English manuscripts
3. Results
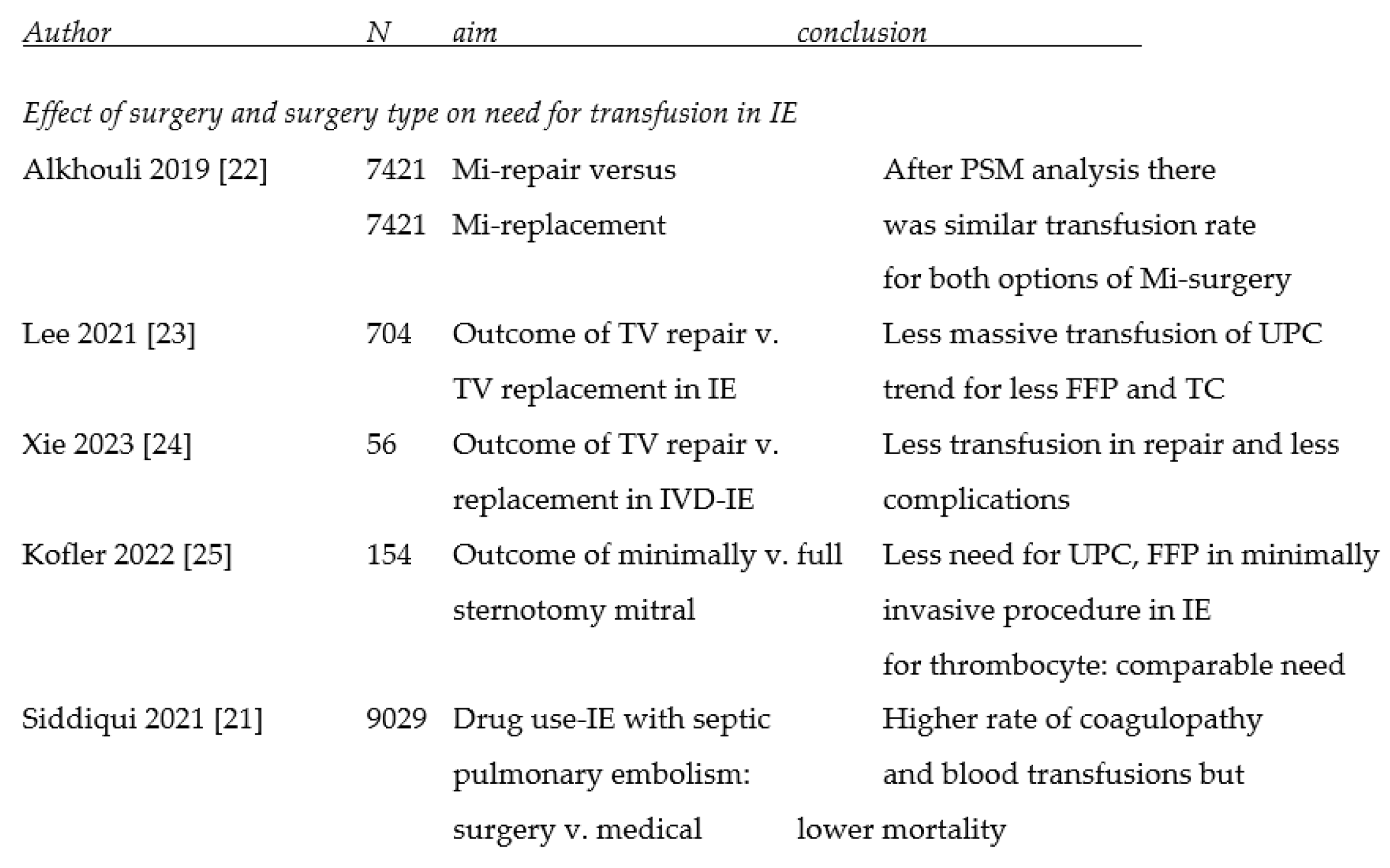
There were 168 initial hits which were further explored on basis of title and of abstract. Seventeen full articles with a focus on at least one of the research questions were identified for further analysis (table). However, need for transfusion was rarely the primary focus of attention in the included manuscripts.
3.1. Effect of surgery, surgical technique and mode of access on the need for transfusion
For the effect of surgery itself, only one manuscript was identified: surgery for tricuspid valve IE with septic emboli in IV drug users was compared to medical treatment. There was a higher rate of coagulopathy and need for transfusion in surgically treated patients compared to medically treated patients. Surgery improved mortality, however. To adjust for the differences between the surgical and medical cohort, an inverse probability of treatment weighted analysis was used [21]. For the effect of type of surgical procedure and the mode of access, four manuscripts were identified. In a nationwide series, repair of the mitral valve for IE had a similar transfusion rate compared to mitral valve replacement. In patients undergoing valve repair, use of other resources and of complications were lower. Sensitivity analysis and propensity score matching did not alter these results. Multivariate logistic regression did not reveal the need for transfusion as predictor for mortality [22]. The repair of the tricuspid valve in a nationwide population-based cohort study showed a lower rate of massive transfusion of RBC (red blood cells), compared to valve replacement. For FFP (fresh frozen plasma) and thrombocytes, there was a trend. The impact of confounding factors was reduced by using the inverse probability of treatment weighting on the propensity score [23]. A small scale series patients with tricuspid valve IE confirmed this observation: there was a lower transfusion need for RBC in patients undergoing repair compared to replacement, while both procedures were effective in improving the cardiac status [24]. The mode of access had also an effect: minimal invasive access mitral surgery for native valve IE, compared to full sternotomy, showed a lower transfusion rate of RBC, FFP and thrombocytes. CPB and cross-clamp time were comparable for both approaches, but overall operation time was shorter for minimal invasive access. The series was small but a propensity score matching was performed to minimize the effect of confounding factors [25].
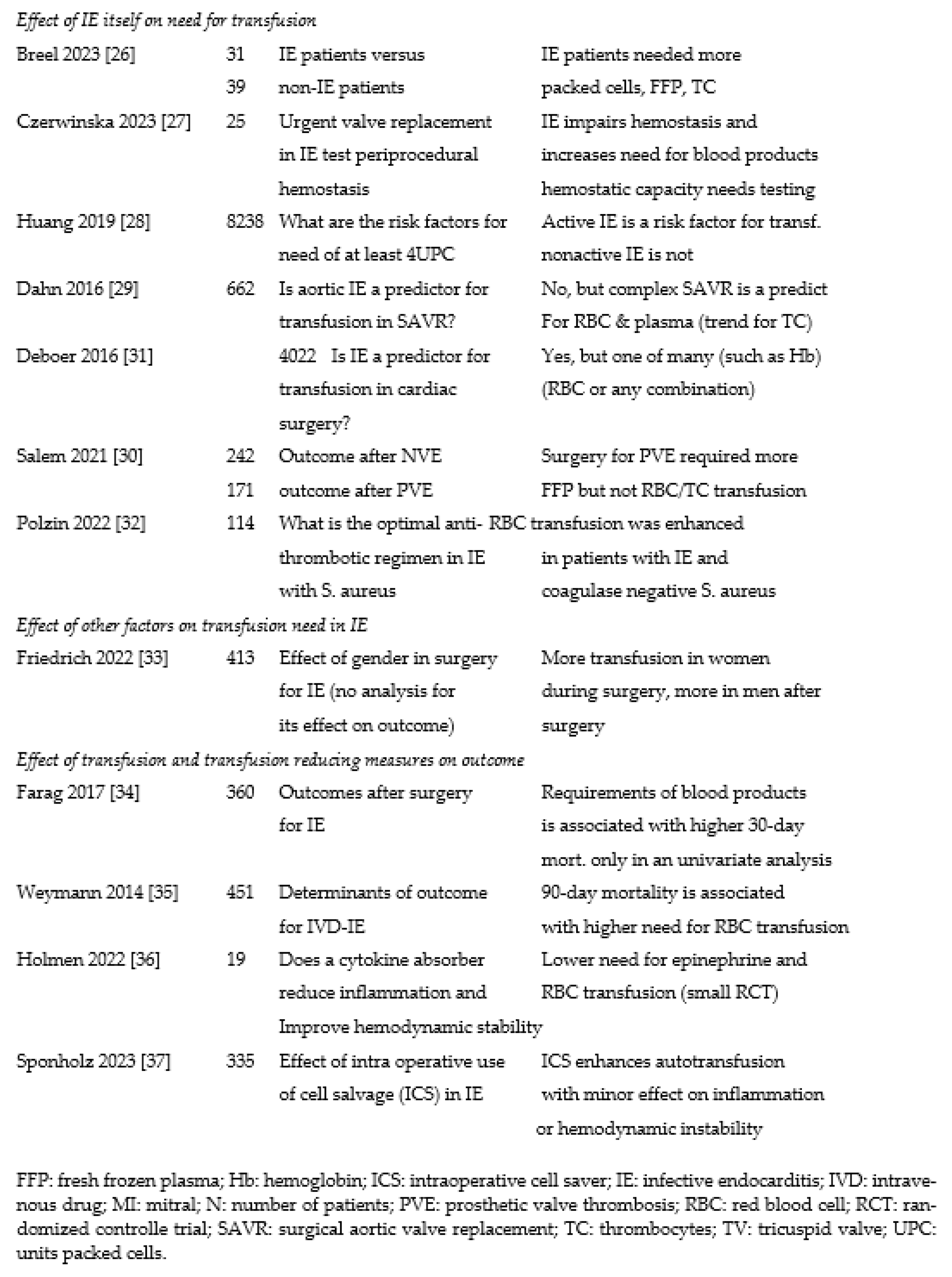
3.2. Effect of infective endocarditis on transfusion need
In an exploratory small series, IE affected thromboelastometry parameters profoundly, with an increased tendency for bleeding complications, a lower hemoglobin content and a higher need for re-exploration. Need for RBC, FFP and thrombocytes was also significantly higher in patients with IE [26]. In another observational small series in which patients with IE needed urgent surgery, the presence of IE also resulted in impaired hemostatic parameters, reduced clot strength, and therefore in an increased bleeding tendency and need for blood products. This was confirmed after adjustment in a multivariate analysis [27], at least when it concerned an active IE. A healed IE showed no such an effect [28]. Remarkably, in patients with aortic valve IE and valve regurgitation, IE was associated with a higher transfusion rate, but it was not identified as an independent predictor for need of RBC and plasma products. However, the need for aortic root repair was predictive for this need [29]. This seemed in line with a higher need of intra and postoperative plasma transfusion in cases with prosthetic valve IE compared to native valve IE [30]. In prosthetic valve infection, more paravalvular involvement, intracardiac abscesses and damage could be expected, with a concomitant longer duration of surgery. In one large series of patients undergoing cardiac surgery, IE was identified as predictor, but only as the 4th of a series of 8 predictors with a relatively low odds ratio. Preoperative hemoglobin was much more important [31]. The type of infectious agent such as coagulase negative S. aureus seemed also to have a deleterious effect concerning the need for transfusion, especially if acetylsalicylic acid was not discontinued [32]. In patients with IE, the need for transfusing during surgery was higher in female patients. Postoperatively, this need was higher in male patients. The effect of transfusion on outcome was not further investigated [33].
3.3. Effect of transfusion (and measures to reduce this) on outcome
The need for transfusion of RBC, FFP and thrombocytes was associated with a higher 30-day mortality, but only in a univariate analysis. Liver cirrhosis and prolonged CPB time were the only independent predictors. However, prolonged CPB time could be a marker for more complex surgery [34]. The higher requirement of RBC had also an effect on 90-day mortality in a small series of active IV drug users with IE, mostly caused by S. aureus. This was not the case for FFP and thrombocytes. Longer operating time, as potential marker for more complex surgery had also an effect [35]. IE needing urgent surgery was a risk for developing a systemic inflammatory response syndrome with consequently hemodynamic instability. The use of a cytokine absorber in a small RCT, led to a lower need for transfusion of RBC [36]. Intraoperative use cell salvage enhanced the use of autotransfusion, but with a minor effect of inflammation and without an adverse effect on hemodynamics. However, CPB time and cross-clamp time were longer and procedures were more complex [37].

Table 1.
transfusion need, its predictors and effect on outcome.
 |
 |
4. Discussion
4.1. Endocarditis, complexity of surgery and coagulation
Routine cardiac surgery requires blood transfusion in 20 to 40% of the cases. For patients with IE this rate might be higher due to the effect of IE on coagulation, to more complex cardiac procedures in case of cardiac damage and in redo surgery. The pros and cons of transfusion and its alternatives have to be balanced. The interaction between endocarditis and coagulation is very complex, with opposing tendencies. On the on hand, there is an enhanced activation of primary and secondary hemostasis, with activation of platelets with increased adhesion to the subendothelial matrix of the endocardium through the von Willebrand factor. There could be an excessive generation of thrombin through the extrinsic coagulation cascade by microbial proteases, while in its turn, thrombin, endotoxin and bacterial adhesive molecules can activate platelets. Apart from direct bacterial effects in IE, the inflammatory response from the host alters hemostasis by endothelial injury, excess release of tissue factor, triggering of the hemostasis by endothelial injury and by inhibition of fibrinolysis and of anticoagulant pathways [27,37]. The latter are affected by alterations of protein S and C, antithrombin III and plasminogen activator inhibitor-1 [27]. On the other hand, an increased consumption of platelets and clotting factors during IE has an opposing effect on coagulation. This balancing makes it difficult to derive a statistical effect of IE on the need for transfusion [29]. In some series of patients needing urgent surgery, an increased risk for bleeding as well as for thromboembolism was observed. Transfusion need for all components was increased [27]. The effect of IE on coagulation could even be more complicated in patients who take anticoagulant or antiplatelet medication. Postoperative parameters for clot formation and strength could be more important than preoperative values. Reasons for discrepancy with the supposedly prothrombotic state of IE are possibly administration of heparin, especially during the development of postoperative acute renal injury, dysregulation of protein C, antithrombin III, increased postoperative consumption plasminogen activator inhibitor-1 with fibrinolysis as well as with CPB related consumption of platelets and clotting factors. The latter should resolve within 24 hours [27]. A preoperative lower fibrinogen [28] and a greater loss of fibrinogen during surgery, with decreased firmness of blood clots, was associated with an increased need for transfusion [26]. Apart from preoperative coagulopathy, anemia and renal failure associated with IE were also held accountable for transfusion need [26,28]. The best predictor for the transfusion of RBC was preoperative hemoglobin level [31]. The type of microbial agents could also have an effect on the transfusion need: in a small series investigating the effect of acetylsalicylic acid in coagulase positive and negative S. aureus, only in coagulase negative S. aureus (CoNS), increased reactivity of platelets was abrogated by acetylsalicylic acid. Patient with IE caused by CoNS taking acetylsalicylic acid, transfusion need was higher [32]. A longer CPB time, as perioperative factor, was associated with a need increased transfusion since CPB caused hemodilution and RBC are consumed under CPB [28,36]. PVE requires a longer CPB time, if there is paravalvular involvement. Perioperative need for transfusion is higher in PVE compared to NVE, but this need is not observed at 24-48 hours after surgery. Need for transfusion was not investigated for its effect on outcome [30]. More prior operations, which is the case in patients with PVE, have a higher risk for perivalvular abscesses, multiple valve involvement [37], requiring longer and more complex surgery. Repeat surgery is associated with transfusion need [28].
4.2. Effect of mode of access and surgical techniques on transfusion need
Repair of the valve [22,23,24] or minimally invasive access [25] was leading to lower transfusion rates. Patients who underwent surgical treatment of an infected tricuspid valve complicated by pulmonary embolism had a higher need for transfusion, compared to medically treated patients. This was also the only report comparing a surgical with a medical approach [21]. There was also only one report on the specific effect of gender in the need for transfusion [33]. In only two series, the effect of CPB and cross-clamp time was investigated, but only with respect to surgical technique [24] or to gender. Women had more need for transfusion during surgery [28,33], for men this was after surgery [33]. Active IE was also one of the predictors for transfusion need [28]. Anemia [23,25,33] and coagulopathy [23,24,25,33] were not investigated in several series. In the remaining surgical series, no clear picture could be seen: anemia was borderline higher [22] or comparable [24] in the repair groups, but lower in the surgical group v. medical group [21]. Coagulopathy was higher in de surgical v. the medical group [21], but lower in the repair v. the replacement group [22]. In none of these series, the predictors for the need of transfusion, nor the effect of transfusion on outcome was the primary focus of investigation. Moreover, there was no apparent correlation between need for transfusion and the outcome for the need of transfusion could not be discerned. In the three replacement v. repair groups, a similar transfusion rate was associated with a worse outcome in the replacement group [22], a higher need for transfusion was associated with more postoperative infection and acute renal injury but with a comparable mortality in the replacement group [23], or no association with an individual outcome was observed [24]. The full sternotomy group also had a higher transfusion rate [25]. As could be expected, transfusion rate was higher in a surgical group compared the a medically treated group. There was a higher cardiovascular complication rate but a lower mortality in the surgical group [21].
4.3. Effect of IE on transfusion needs In six series of varying size,
IE itself led to hemostatic problems leading to an increased need for transfusion [26,27,31], especially with active IE [28], prosthetic valve IE [30] or when coagulase negative staphylococcus aureus was involved [32]. In one report, IE itself had no effect but its potential consequence, the need for complex aortic valve surgery was associated with this increased need for transfusion. There were also more comorbid conditions such as renal dysfunction, anemia, lower LVEF and a higher need for urgent and complex surgical procedure. Moreover, organ dysfunction associated to IE were compounding factors for the effect of transfusion on outcome, since organ dysfunction could make these patients more vulnerable to transfusion related adverse events [29].
4.4. Effect of transfusion on outcome of IE and techniques to improve outcome
The 30-day mortality after surgery for IE was close to 20% and was negatively affected by comorbid conditions, inflammation, duration of surgery, CPB and cross-clamp times and higher requirements of blood products as well as coagulation disorders. Only liver cirrhosis and prolonged CPB were independent predictors. Transfusion was not identified as such [34]. Platelet and RBC transfusions were associated with prolonged bleeding time and impaired strength of the final clot under high shear forces. FFP transfusion was also associated with impaired clot formation under low and high shear conditions which reflects combined involvement of primary and secondary hemostasis. This may indicate the presence of excessive fibrinolysis and a reduction of fibrin deposition related to hemodilution early after the procedure [27]. However, two reports indicate an increased mortality rate associated to need for blood products [34,35]. The use of a cytokine absorber, as an attempt to eliminate the undesirable effects of these factors showed a favorable outcome [36]. The use of an intraoperative cell salvage system showed also a positive effect: there was a higher degree of autotransfusion with a lower need for inotropes [37]. In patients with IE associated with IV drug use, several clinical and perioperative factors such as Euroscore II and operation time, as well as the need for RBC (but not for FFP and thrombocytes) had an effect on 90-day mortality. There was no further analysis with respect to need for RBC [35]. A systemic inflammation is a hallmark from disseminated bacteria in IE patients. In a small experimental series, a cytokine absorber during CPB, as an attempt to eliminate their undesirable effects, was hemodynamically tolerated. The need for RBC, FFP and thrombocytes were lower, which could be beneficial since there were not significantly more complications [36]. Intraoperative cell salvage (ICS) involved aspiration of blood at the start and at the end of surgery for IE, but not when infected tissue was handled. These RBC can be washed and be readministered, but there might a risk for contamination with bacteria and toxins, restricting its use in IE patients. In one series of patients with left-sided IE, use of ICS resulted in higher WBC, but not of C-reactive protein. Hence, this observation was probably clinically unimportant. There was no concomitant hemodynamic instability, coagulation or organ dysfunction, in spite of a higher Euroscore, longer CPB time, and more complex procedure in patients receiving ICS. Coagulation factors might be reduced by ICS through wash-out, but CPB itself had also such an effect. The policy of restriction of ICS for IE-surgery should be re-evaluated. For patients with IE undergoing surgery, decisions need to be made on a case-to-case basis, keeping in mind the advantages of ICS: potential reduction of allogeneic RBC transfusion and the associated immune response [37].
4.5. Alternative approaches to deal with the need for transfusion and transfusion reaction
Another alternative for allogeneic transfusion, which had been described earlier, is acute normovolemic hemodilution (ANH), which could also be used as blood conservation technique. The hemodilution technique reduced the need for allogeneic transfusion about tenfold. The collected blood could be used to manage post CPB coagulopathy [11,38]. Its usefulness was not well established but it could be a part of a concerted effort to conserve blood [39]. The technique varied in its practical application concerning patient selection with respect to hemodynamic status and the blood volume to be drawn or to the target hematocrit levels [40]. If it can be hemodynamically tolerated, 500 to 1000mL of blood is removed and replaced by a crystalloid solution. One meta-analysis showed that this technique is effective in reducing transfusion need [41], but at the cost of a lower hematocrit and an increased morbidity and hospital mortality [42]. ANH also requires a high hematocrit at the start point. In patients with sepsis and IE, the hemodilution technique was considered to be a contraindication, but few to no studies are available to support this view. Endotoxin could be produced during the temporary storage of infected blood after being withdrawn from the circulation [43]. Especially with Staphylococcus aureus, heat-resistant superantigen toxins, could remain active, causing a so-called cytokine storm, followed by vascular injury, vasodilatation and cardiovascular collapse [44]. Although hemodilution could improve regional blood flow, the oxygenation of renal tissue could be impaired [45]. There is a lack of data concerning the effect on improvement of morbidity, mortality, and LOS. To date, there have not been any studies or even case reports describing an increased risk of postoperative infection with the use of ANH in patients with IE. There seems to be only a theoretical evidence to suggest that the use of this proven blood conservation technique has caused any harm to this population. Routinely scheduled prophylactic antibiotics should mitigate the risk of proliferation bacteria in the harvested units
5. Conclusions
In conclusion, no firm data exist to identify independent predictors for the need for transfusion in patients with IE, nor for the predictive effect of transfusion on outcome. This observation is at the same time the main limitation of this review. This is partly due to 1) the complex relationship between IE and the coagulation cascade, in which opposing bleeding and thrombotic tendencies have been documented, 2) the confounding effect of long CPB time associated to a more complex cardiac procedure, 3) the diversity of the included study designs and 4) no series were identified having both current research questions as primary focus. However, minimal access approach and valve repair, if feasible, seemed to have favorable results over full sternotomy resp. valve replacement. Additional techniques such as intraoperative cell salvage, cytokine absorbers and ANH could have a place in selected patients. If transfusion is required, only recently stored blood should be used. Perioperative point-of-care coagulation testing are indicated. For example a Total Thrombus Formation System during the operation can be helpful. A multicentric international standardized registry for patients with infective endocarditis treated by cardiac surgery is highly desirable. One of the aspects under scrutiny should be the research questions of the current manuscripts.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflict of interest.
References
- Wang A, Gaca JG, Chu VH. Management considerations in infective endocarditis: A review. JAMA 2018;320:72-83. [CrossRef]
- Mistiaen WP, Gebruers N. How to manage patients in whom malignancy and infective endocarditis are associated: a review. Scand Cardiovasc J. 2020;54:70-76. [CrossRef]
- Mostaghim AS, Lo HYA, Khardori N. A retrospective epidemiologic study to define risk factors, microbiology, and clinical outcomes of infective endocarditis in a large tertiary-care teaching hospital. SAGE Open Med 2017;5:2050312117741772. [CrossRef]
- Mistiaen WP. What are the main predictors of in-hospital mortality in patients with infective endocarditis: a review. Scand Cardiovasc J. 2018;52:58-68. [CrossRef]
- Bennett-Guerrero E, Zhao Y, O’Brien SM, et al. Variation in use of blood transfusion in coronary artery bypass graft surgery. JAMA. 2010;304:1568-1575. [CrossRef]
- Karkouti K, Wijeysundera DN, Yau TM, et al. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion. 2004;44:1453-1462. [CrossRef]
- Durante-Mangoni ER, Molaro R, Iossa D. The role of hemostasis in infective endocarditis. Curr Infect Dis Rep 2014;16:435. [CrossRef]
- Grottke O, Mallaiah S, Karkouti K, et al. Fibrinogen supplementation and its indications. Semin Thromb Hemost 2020;46:38-49. [CrossRef]
- Koltsova EM, Sorokina MA, Pisaryuk AS, et al. Hypercoagulation detected by routine and global laboratory hemostasis assays in patients with infective endocarditis. PLoS One 2021;16:e0261429. [CrossRef]
- Bartoszko J, Karkouti K. Managing the coagulopathy associated with cardiopulmonary bypass. J Thromb Haemost. 2021;19:617-632. [CrossRef]
- Hendrickson JE, Roubinian NH, Chowdhury D, et al. Incidence of transfusion reactions: A multicenter study utilizing systematic active surveillance and expert adjudication. Transfusion 2016;56:2587-2596. [CrossRef]
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: The TRACS randomized controlled trial. JAMA 2010;304:1559-1567. [CrossRef]
- Vlaar AP, Hofstra JJ, Determann RM, et al. The incidence, risk factors, and outcome of transfusion-related acute lung injury in a cohort of cardiac surgery patients: A prospective nested case-control study. Blood 2011;117:4218-4225. [CrossRef]
- Rohde JM, Dimcheff DE, Blumberg N, Saint S, Langa KM, Kuhn L, et al. Health care-associated infection after red blood cell transfusion: a systematic review and meta-analysis. JAMA. 2014;311:1317-26. doi: 10.1001/jama.2014.2726. Erratum in: JAMA. 2014;312:2045. [CrossRef]
- Simancas-Racines D, Osorio D, Martí-Carvajal AJ, Arevalo-Rodriguez I. Leukoreduction for the prevention of adverse reactions from allogeneic blood transfusion. Cochrane Database Syst Rev. 2015(12):CD009745. [CrossRef]
- Remy KE, Hall MW, Cholette J, et al. Mechanisms of red blood cell transfusion-related immunomodulation. Transfusion 2018;58:804-815. [CrossRef]
- Mazer CD, Whitlock RP, Fergusson DA, et al. Restrictive or liberal red cell transfusion for cardiac surgery. N Engl J Med 2017;377:2133-2144. [CrossRef]
- Youssef LA, Spitalnik SL. Transfusion-related immunomodulation: A reappraisal. Curr Opin Hematol 2017;24:551-557. [CrossRef]
- Dumont LJ, AuBuchon JP. Evaluation of proposed FDA criteria for the evaluation of radiolabeled red cell recovery trials. Transfusion 2008;48:1053-1060. [CrossRef]
- Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008;358:1229-1239. [CrossRef]
- Siddiqui E, Alviar CL, Ramachandran A, Flattery E, Bernard S, Xia Y, Nayar A, Keller N, Bangalore S. Outcomes After Tricuspid Valve Operations in Patients With Drug-Use Infective Endocarditis. Am J Cardiol. 2022;185:80-86. [CrossRef]
- Alkhouli M, Alqahtani F, Berzingi C, Cook CC. Contemporary trends and outcomes of mitral valve surgery for infective endocarditis. J Card Surg. 2019;34:583-590. Epub 2019 Jun 18. PMID: 31212382. [CrossRef]
- Lee HA, Chou AH, Wu VC, Chan YS, Cheng YT, Chang CH, Chang SH, Hung KC, Chu PH, Chen SW. Nationwide cohort study of tricuspid valve repair versus replacement for infective endocarditis. Eur J Cardiothorac Surg. 2021;59:878-886. [CrossRef] [PubMed]
- Xie L, Chen X, He J, Lin S, Chen X, Wu Q, Chen L, Zhuang J, Qiu Z, Chen L. Comparison of valvuloplasty and replacement for surgical treatment of tricuspid infective endocarditis. BMC Cardiovasc Disord. 2023;23:213. [CrossRef] [PubMed]
- Kofler M, Van Praet KM, Schambach J, Akansel S, Sündermann S, Schönrath F, Jacobs S, Falk V, Kempfert J. Minimally invasive surgery versus sternotomy in native mitral valve endocarditis: a matched comparison. Eur J Cardiothorac Surg. 2021;61:189-194. [CrossRef] [PubMed]
- Breel JS, Wensing AGCL, Eberl S, Preckel B, Schober P, Müller MCA, Klautz RJM, Hollmann MW, Hermanns H. Patients with infective endocarditis undergoing cardiac surgery have distinct ROTEM profiles and more bleeding complications compared to patients without infective endocarditis. PLoS One. 2023;18:e0284329. [CrossRef]
- Czerwińska-Jelonkiewicz K, Sanetra K, Buszman PP, Gryszko L, Wood A, Crescenzi O, Milewski K, Buszman PE. Hemostatic disorders in patients with infective endocarditis undergoing urgent surgical valve replacement - Rethinking current beliefs. Int J Cardiol. 2023;388:131112. [CrossRef]
- Huang D, Chen C, Ming Y, Liu J, Zhou L, Zhang F, Yan M, Du L. Risk of massive blood product requirement in cardiac surgery: A large retrospective study from 2 heart centers. Medicine. 2019;98:e14219. [CrossRef]
- Dahn H, Buth K, Legare JF, Mingo H, Kent B, Whynot S, Scheffler M. Endocarditis is not an Independent Predictor of Blood Transfusion in Aortic Valve Replacement Patients With Severe Aortic Regurgitation. J Cardiothorac Vasc Anesth. 2016;30:687-691. [CrossRef]
- Salem M, Friedrich C, Saad M, Frank D, Salem M, Puehler T, Schoettler J, Schoeneich F, Cremer J, Haneya A. Active Infective Native and Prosthetic Valve Endocarditis: Short- and Long-Term Outcomes of Patients after Surgical Treatment. J Clin Med. 2021;10:1868. [CrossRef]
- de Boer WJ, Visser C, Ganushchak YM. Preoperative hemoglobin level: the best predictor of transfusion of packed red cells. Perfusion. 2016;31:691-698. [CrossRef]
- Polzin A, Dannenberg L, M’Pembele R, Mourikis P, Naguib D, Zako S, et al. Staphylococcus aureus increases platelet reactivity in patients with infective endocarditis. Sci Rep. 2022;12:12933. [CrossRef]
- Friedrich C, Salem M, Puehler T, Panholzer B, Herbers L, Reimers J, Hummitzsch L, Cremer J, Haneya A. Sex-Specific Risk Factors for Short- and Long-Term Outcomes after Surgery in Patients with Infective Endocarditis. J Clin Med. 2022;11:1875. [CrossRef]
- Farag M, Borst T, Sabashnikov A, Zeriouh M, Schmack B, Arif R, Beller CJ, Popov AF, Kallenbach K, Ruhparwar A, Dohmen PM, Szabó G, Karck M, Weymann A. Surgery for Infective Endocarditis: Outcomes and Predictors of Mortality in 360 Consecutive Patients. Med Sci Monit. 2017;23:3617-3626. [CrossRef]
- Weymann A, Borst T, Popov AF, Sabashnikov A, Bowles C, Schmack B, Veres G, Chaimow N, Simon AR, Karck M, Szabo G. Surgical treatment of infective endocarditis in active intravenous drug users: a justified procedure? J Cardiothorac Surg. 2014;9:58. [CrossRef]
- Holmén A, Corderfeldt A, Lannemyr L, Dellgren G, Hansson EC. Whole Blood Adsorber During CPB and Need for Vasoactive Treatment After Valve Surgery in Acute Endocarditis: A Randomized Controlled Study. J Cardiothorac Vasc Anesth. 2022;36[8 Pt B]:3015-3020. [CrossRef]
- Sponholz C, Sommerfeld O, Moehl C, Lehmann T, Franz M, Bauer M, Doenst T, Faerber G, Diab M. Intraoperative Cell Savage, Infection and Organ Failure in Infective Endocarditis Patients-A Retrospective Single Center Evaluation. J Clin Med. 2023;12:382. [CrossRef]
- Henderson RA, Judd M, Strauss ER, et al. Hematologic evaluation of intraoperative autologous blood collection and allogeneic transfusion in cardiac surgery. Transfusion 2021;61:788-798. [CrossRef]
- Society of Thoracic Surgeons Blood Conservation Guideline Task Force, 2011 update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines. Ferraris VA, Brown JR, Despotis GJ, et al. Ann Thorac Surg 2011;91:944-982. [CrossRef]
- Society of Thoracic Surgeons Blood Conservation Guideline Task Force; Ferraris VA, Ferraris SP, Saha SP, et al.; Society of Cardiovascular Anesthesiologists Special Task Force on Blood Transfusion; Spiess BD, Shore-Lesserson L, Stafford-Smith M, et al. Perioperative blood transfusion and blood conservation in cardiac surgery: the Society of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologists clinical practice guideline. Ann Thorac Surg. 2007 May;83(5 Suppl):S27-86. [CrossRef]
- Zhou Z-F, Jia X-P, Sun K, et al. Mild volume acute normovolemic hemodilution is associated with lower intraoperative transfusion and postoperative pulmonary infection in patients undergoing cardiac surgery - a retrospective, propensity matching study. BMC Anesthesiol 2017;17:13. [CrossRef]
- Pagano D, Milojevic M, Meesters MI, et al. 2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. Eur J Cardiothorac Surg 2018;53:79-111. [CrossRef]
- Benjamin RJ. Transfusion-related sepsis: A silent epidemic. Blood 2016;127:380-381. [CrossRef]
- Spaulding AR, Salgado-Pabon W, Kohler PL, et al. Staphylococcal and streptococcal superantigen exotoxins. Clin Microbiol Rev 2013;26:422-447. [CrossRef]
- Konrad FM, Mik EG, Bodmer SI, et al. Acute normovolemic hemodilution in the pig is associated with renal tissue edema, impaired renal microvascular oxygenation, and functional loss. Anesthesiology 2013;119:256-269. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



