
Submitted:
09 October 2023
Posted:
10 October 2023
You are already at the latest version
Abstract
Objective: Polymyalgia rheumatica (PMR) and giant cell arteritis (GCA) are often overlapping conditions. We aimed to determine whether 18F-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET-CT) is useful in identifying PMR in the setting of large vessel vasculitis (LVV)-GCA.
Methods: Patients diagnosed with LVV-GCA by PET-CT at a tertiary referral hospital for a population of 450,000 people over a two-year period were reviewed. Scoring was performed based on potential significant FDG uptake at up to 16 sites in nine different extravascular areas (SCORE 16). Differences in extravascular sites of significant FDG uptake were evaluated between LVV-GCA with a clinical diagnosis of PMR or not.
Results: Fifty-four patients were diagnosed with LVV-GCA by 18F-FDG-PET-CT. Of them, 21 (38.8%) were clinically diagnosed with PMR. Significant extravascular FDG uptake was more frequently observed in those with a clinical diagnosis of PMR. In this sense, the SCORE 16 was higher in those with clinical PMR (5.10 ± 4.05 versus 1.73 ± 2.31 in those without a clinical diagnosis of PMR; p< 0.001). A SCORE 16 involving more than 4 sites of significant FDG uptake yielded a sensitivity of 52% and a specificity of 91% for establishing a clinical diagnosis of PMR associated with LVV-GCA. The best areas of significant FDG uptake to clinically identify PMR in patients with LVV were the shoulder, the greater trochanter and the lumbar interspinous regions with an area under the ROC curve of 0.810 (0.691-0.930).
Conclusion: Significant extravascular 18F-FDG-PET-CT uptake may help establish a clinical diagnosis of PMR in patients with LVV-GCA. These patients are more commonly diagnosed with PMR if they have significant FDG uptake in the shoulder, greater trochanter, and lumbar interspinous areas.
Keywords:
Positron emission computed tomography (PET-CT) with 18F-fluorodeoxyglucose (FDG)
; FDG uptake
; large vessel vasculitis
; giant cell arteritis
; polymyalgia rheumatica.
1. Introduction
Polymyalgia rheumatica (PMR) and giant cell arteritis (GCA) are common conditions in people older than 50 years from Western countries [1,2]. PMR is characterized by pain and stiffness involving bilaterally the shoulder girdle, proximal aspects of the arms, the neck, the hip girdle, and proximal aspects of the thighs [3]. GCA is a large vessel vasculitis (LVV) that in the classic pattern of the disease affects predominantly extracranial arteries derived from the carotid. In this sense, vascular inflammation due to the involvement of the branches of the external carotid artery is responsible for the typical manifestations of the disease, such as headache, scalp tenderness, jaw claudication or dysphagia, while the involvement of branches of the internal carotid promotes the development of the feared visual ischemic manifestations of the disease [4]. The advent of new imaging techniques has been a great step forward for the diagnosis of GCA [5]. Positron emission tomography-computed tomography (PET-CT) with 18F-fluorodeoxyglucose (18F-FDG) is one of the imaging techniques that has made it possible to identify GCA patients with a predominantly extracranial LVV pattern of the disease [6]. This functional imaging technique combines 18F-FDG-PET with CT allowing identifying LVV due to its ability to detect glucose uptake from the high activity of inflammatory cells in the vessel walls. In this regard, increased FDG uptake is seen after PET imaging is observed in more than 80% of patients with GCA. It is also useful to identify vascular inflammation affecting lower extremity arteries in patients with GCA [7,8]. Moreover, 18F-FDG-PET-CT may help to rule out other entities such as infection or malignancy [9,10].
During the last 25 years, different researchers, in particular the group of Cantini et al, have confirmed that magnetic resonance imaging and, in particular, ultrasonography are very useful for the diagnosis of PMR [11,12,13,14]. Due to this, experts who elaborated the 2012 provisional European League Against Rheumatism/American College of Rheumatology classification criteria included the presence of an ultrasonography showing shoulder bursitis and/or biceps tenosynovitis and/or glenohumeral synovitis and hip with synovitis and/or trochanteric bursitis as a criterion for the presence of PMR [15]. Although 18F-FDG-PET-CT is not included in these proposed classification criteria for the diagnosis of PMR, several studies support the role of 18F-FDG-PET-CT for the diagnosis of PMR [16,17]. In this regard, van der Geest et al performed a meta-analysis that included a systemic review of 636 patients from 9 studies. They concluded that 18F-FDG-PET-CT may be an important diagnostic tool for diagnosis in patients with suspected PMR [18]. Interestingly, 18F-FDG-PET-CT studies have demonstrated the presence an underlying LVV in 14% to 40% patients with PMR [17,18,19,20]. The frequency of an underlying LVV may be higher in patients with PMR and inflammatory low back pain, marked pelvic girdle, and diffuse lower limb pain [21].
An issue that from our point of view has been less evaluated is the usefulness of 18F-FDG-PET-CT to identify PMR in patients diagnosed with LVV-GCA. To address this question and determine the best predictors of 18F-FDG-PET-CT to clinically identify PMR in patients with LVV-GCA, we evaluated a cohort of patients diagnosed with LVV-GCA using 18F-FDG-PET-CT.
2. Patients and Methods
2.1. Study Design and Patient Recruitment
Retrospective study carried out at the Fundación Jiménez Díaz University Hospital (Madrid, Spain) of patients undergoing 18F-FDG-PET-CT between April 2021 and March 2023. As recently reported, 54 of them were diagnosed with LVV-GCA using 18F- FDG-PET-CT [22]. These 54 patients with LVV were evaluated for the presence of clinical and 18F-FDG-PET-CT features of PMR.
The study procedures acted in accordance with the Helsinki Declaration of 1975, as revised in 2000. Although it was a retrospective study, ethical committee approval was obtained (PIC034-23).
First, we identified those patients who were clinically diagnosed with PMR in the context of LVV-GCA by physicians with high experience in diagnosing PMR. We then analyzed possible differences in sites with significant extravascular FDG uptake between patients clinically diagnosed with PMR or not. Second, we evaluated the cutoff points for the diagnosis of PMR based on the sites of significant FDG uptake. In a third step, we evaluated the best areas of significant FDG uptake to clinically identify the presence of a clinical PMR in patients with LVV.
2.2. Study Protocol
2.2.1. Patient Disease Assessment
Fundación Jiménez Díaz University Hospital provides medical care to 450,000 people. During the study period, 1,302 patients underwent a PET-CT.
As previously described [22], the Big Data Department of the Jiménez Díaz Foundation Hospital was asked to carry out an exhaustive search of the patients who underwent PET-CT during the two years of the study. Then 18F-PET-CT of patients that included any of the following keywords: “vasculitis”, “large vessels”, “medium vessels”, “vascular wall”, “vascular”, “aortitis”, “vessel inflammation”, “increased FDG vessel uptake”, “polymyalgia rheumatica” and “giant cell arteritis” were reviewed by members of the Divisions of Rheumatology and Nuclear Medicine. Those patients in whom agreement on the presence of LVV-GCA was confirmed were included in the study.
In a second step, the sites of significant extravascular FDG uptake were assessed by the members of the Nuclear Medicine department. At the time of the study these sites of significant FDG uptake were again reviewed for confirmation. Subsequently, clinical information was obtained by reviewing medical records.
At the time of diagnosis of LVV-GCA, physicians with experience in autoimmune diseases had made a clinical diagnosis of PMR if patients had new-onset symmetrical pain and stiffness in the shoulder girdle and proximal arms, often associated with pain and stiffness in the pelvic girdle, hips, and the proximal part of the legs and neck. All were over 50 years old and complained of pain at night and morning stiffness that was worse in the morning. All but 6 had an erythrocyte sedimentation rate (ESR) greater than 40 mm/1st hour and/or a C-reactive protein (CRP) greater than 10 mg/l at the time of disease diagnosis of LVV and fulfilled the 2012 European League Against Rheumatism/American College of Rheumatology provisional classification criteria for polymyalgia rheumatica [15]. As previously reported in a small proportion of patients with PMR [23], the 6 PMR patients with low or normal ESR and CRP had typical inflammatory pain involving the arms and shoulder. In this regard, Cantini et al described that PMR patients with normal ESR have similar bilateral subacromial bursitis involvement to those with high ESR when magnetic resonance imaging or ultrasonography studies are performed [24]. Moreover, other conditions mimicking PMR including other rheumatic diseases or malignancies [25,26] were excluded at diagnosis or during follow-up.
2.2.2. FDG-PET-CT Equipment, Protocol, and Interpretation
PET-CT examinations were performed on an integrated digital PET-CT system (GE Discovery MI3R, with NEMA sensitivity of 7.5 cps/kbq, 3 rings and 15 cm axial field of view). Patients were administered 175-350 mbq (2.5-5.0 MBq/kg) of 18F-FDG after at least a 4-hour fast. The postinjection rest time was 60 minutes. PET-CT was performed in the supine position, with arms stretched above the head, and scans were acquired from the base of the skull to the femur. Low-dose CT was performed for PET co-registration (140 kv, 380 ma) followed by PET imaging (1.45 min per bed). Blood glucose levels before tracer injection were <200 mg/ml in all cases.
All PET-CT scans were reviewed by nuclear medicine physicians with experience in LVV. The nuclear medicine physicians visually evaluated the distribution of the radiopharmaceutical in the aorta carotids, brachiocephalic trunk, subclavian, axillary, vertebral, humeral, iliac, and femoral arteries using a visual uptake classification scale as recently described [22]. The standardized grading system from 0 to 3 (vascular to hepatic uptake): 0 = no uptake (≤mediastinum); 1 = low-grade uptake (<liver); 2 = intermediate-grade uptake (=liver), 3 = high-grade uptake (>liver), with grade 2 indicative and grade 3 considered strongly positive for LVV. In all cases, positive PET-CT scans were re-evaluated for confirmation [22].
Similar procedure was conducted to assess the sites of significant extravascular FDG uptake. With respect to this, extravascular sites of FDG uptake were evaluated using a semiquantitative analysis as previously described [27]: Grade 0= No uptake; Grade 1: Uptake < liver uptake; Grade 2: Uptake = liver uptake and Grade 3: Uptake > liver uptake. A site was considered as having significant extravascular FDG uptake if the score was ≥ 2.
We assessed 9 extravascular areas and a total of 16 sites of potential involvement: two acromioclavicular and sternoclavicular joints, two hips, two shoulders, two greater trochanters, two ischial tuberosities, two symphysis pubis enthesis, and the cervical and lumbar interspinous processes. We calculated a total score (0-16), corresponding to the sum of all sites with significant FDG uptake, for each patient. This score was called SCORE 16 throughout the manuscript.
2.3. Statistical Analysis
Fisher’s Exact Test (two-tailed) for a 2x2 contingency table was used to determine whether or not there was a significant association between two categorical variables. A logistic regression penalized via LASSO was carried out to identify the best areas of significant extravascular FDG uptake to identify clinically PMR. LASSO penalization used all 9 areas assessed and iteratively shrank their coefficients to 0 (i.e., delete the location from the model) to obtain a model with small number of predictors. The criterion for shrinking coefficients was obtained via cross-validation. All statistical analyses were carried out with the software Stata 18/SE (StataCorp, College Station, TX, US)
3. Results
3.1. Differences in Significant Extravascular Sites of FDG Uptake between Patients with LVV-GCA Clinically Diagnosed with PMR or Not
During the period of study 21 of the 54 patients with a diagnosis of LVV-GCA by 18F-FDG-PET-CT were also diagnosed clinically with PMR. Differences in the presence of significant extravascular uptake in the sixteen sites assessed between patients with or without PMR is shown in Table 1.
Table 1. Extravascular 18F-FDG PET-CT findings in 54 patients with LVV-GCA according to the presence of a clinical diagnosis of PMR or not.
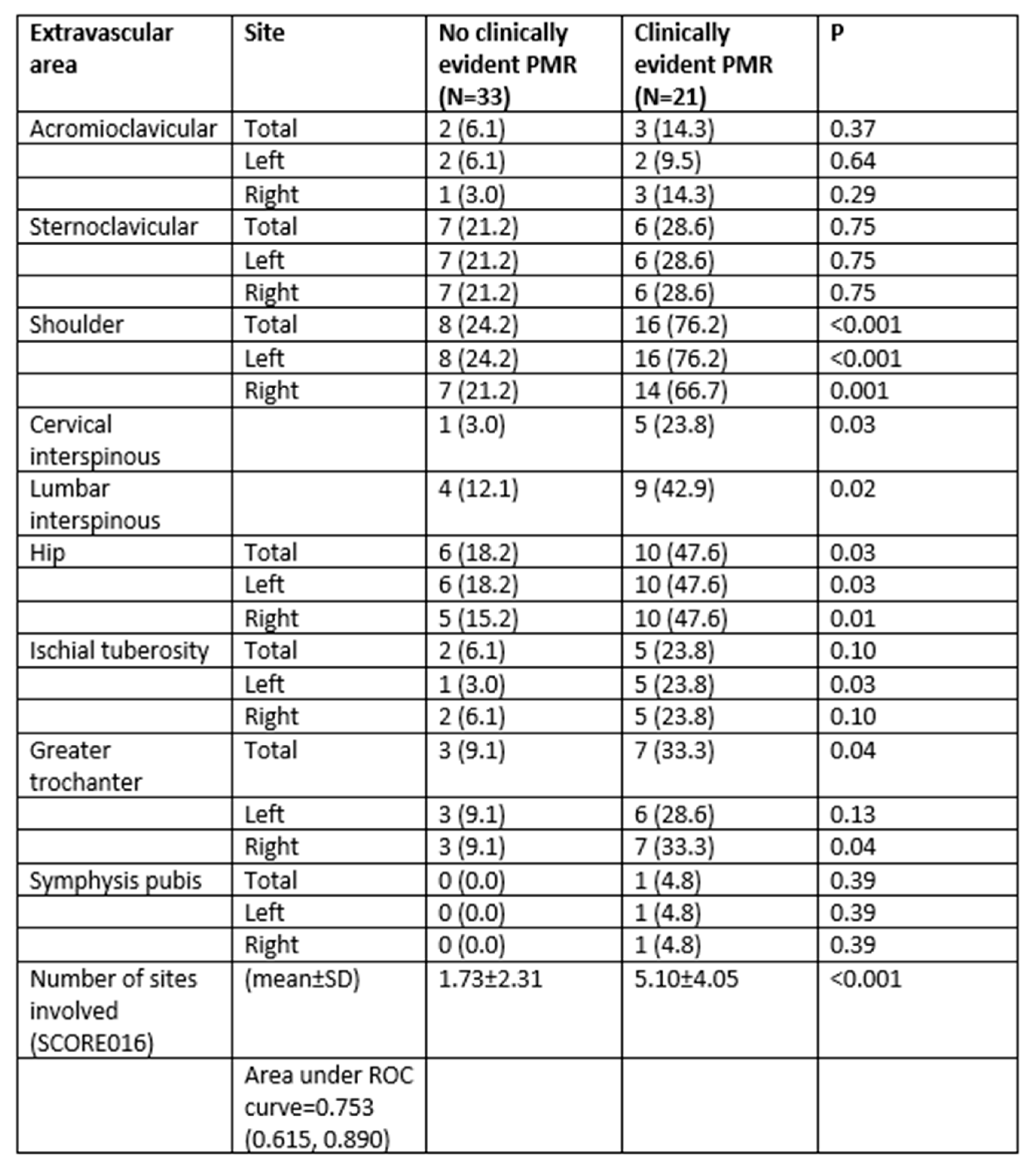
Patients with a clinical diagnosis of PMR had more commonly significant extravascular FDG uptake in the sites explored. This was especially true when comparisons of significant FDG uptake in the shoulders were assessed (76,2% in those with a clinical diagnosis of PMR versus 24.2% in those without PMR; p<0.001). Other areas such as cervical and lumbar interspinous processes, the hip and the greater trochanter also showed more commonly significant FDG uptake in those with a clinical diagnosis of PMR (p value for all the comparisons < 0.05). Differences in significant FDG uptake in other areas are shown in Table 1. Consequently, the SCORE 16 of significant FDG uptake was higher in patients with LVV-GCA and PMR than in those without PMR (5.10±4.05 versus 1.73±2.31; p<0.001). According to these results, the number of affected extravascular sites was greater in patients with PMR.
Figure 1.
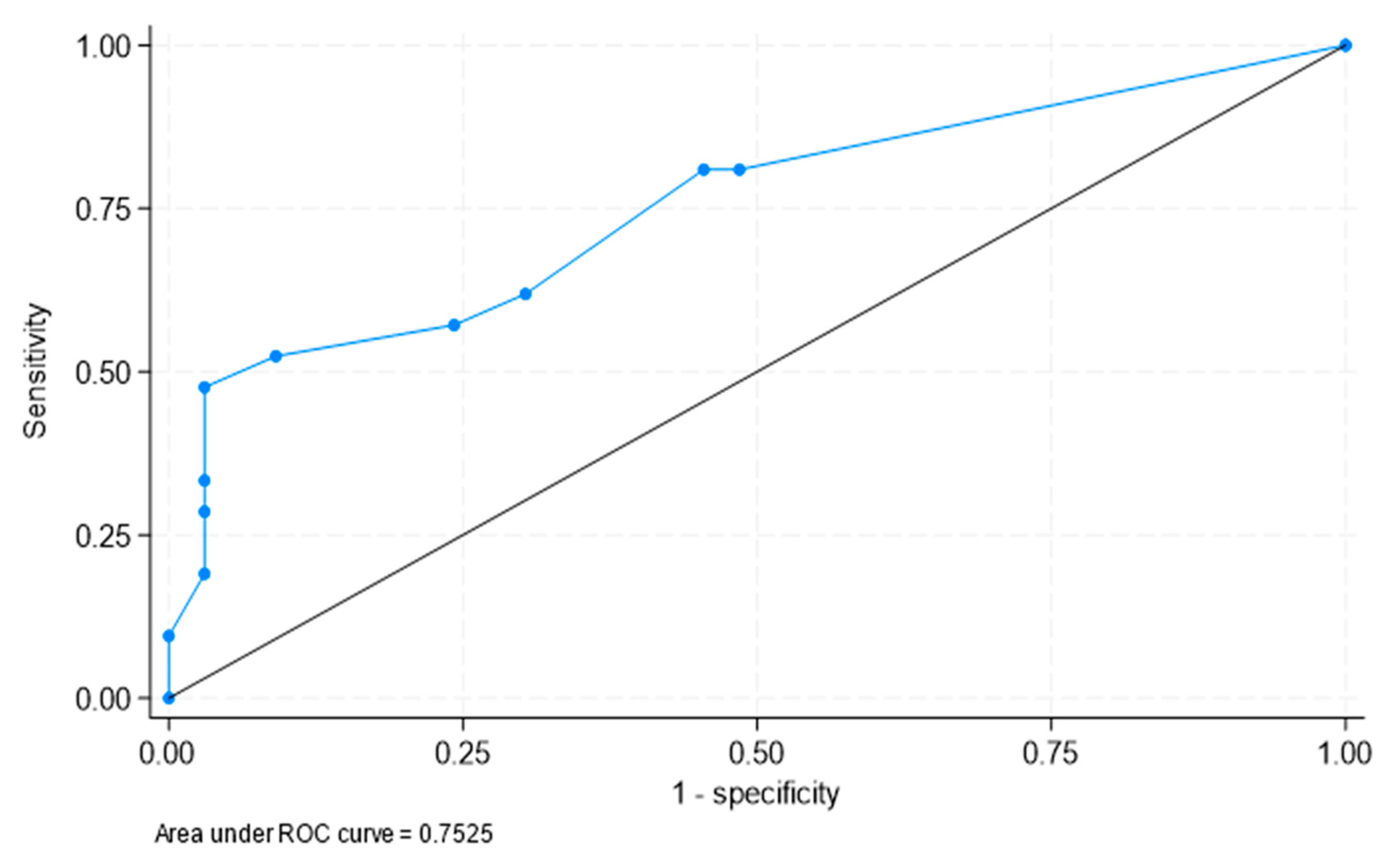
ROC curve on the diagnostic capacity of SCORE 16 to identify clinical PMR. The area under the ROC curve was 0.753 (95% confidence interval [CI]: 0.615, 0.890).
Figure 1.
ROC curve on the diagnostic capacity of SCORE 16 to identify clinical PMR. The area under the ROC curve was 0.753 (95% confidence interval [CI]: 0.615, 0.890).
3.2. Determination of the Best Cut-Offs for the Diagnosis of PMR in Patients with LVV-GCA
ROC curve analysis was performed to determine the optimal cut-offs to clinically identify PMR in patients with LVV-GCA according to the number of sites of significant FDG-uptake. In this regard, a model that included patients with SCORE 16>4 would be 52% sensitive and 91% specific for clinical diagnosis of PMR. However, a lower cut off of SCORE 16 would decrease the specificity to clinically identify PMR. In this regard, the inclusion of patients with SCORE 16>3 would be 57% sensitive and 76% specific.
3.3. Best Areas of Significant FDG Uptake to Clinically Identify PMR in Patients with LVV-GCA
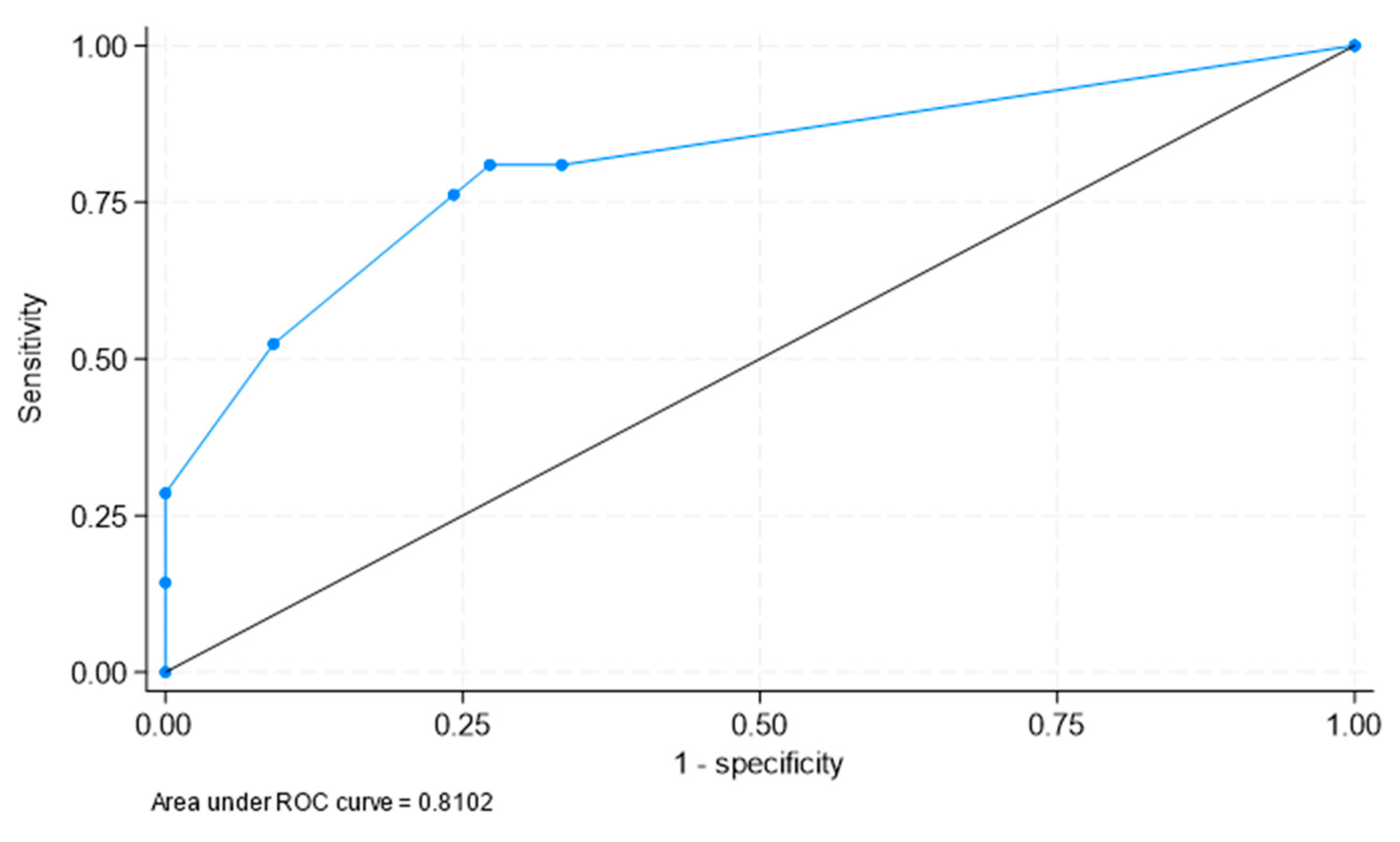
A logistic regression penalized via LASSO was carried out to identify the best areas of significant FDG to clinically identify PMR in patients with LVV-GCA. The final model included only three locations: shoulder (odds ratio [OR] = 8.6, 95% CI: 2.0, 36.4), greater trochanter (OR=4.4, 95% CI: 0.8, 26.1) and lumbar interspinous (OR=1.6, 95% CI: 0.3, 7.9), with area under the ROC curve = 0.810 (95% CI: 0.691, 0.930) (Figure 2).
Therefore, patients with LVV-GCA were more commonly diagnosed with PMR if they had significant FDG uptake in the shoulder, the greater trochanter and the lumbar interspinous areas.
4. Discussion
The present study shows that in patients with LVV-GCA a significant uptake of FDG in some extravascular anatomical areas helps to establish a clinical diagnosis of PMR. This is especially true when the shoulder, greater trochanter, and lumbar interspinous areas are affected. These findings are consistent with previously reported information on 18F-FDG-PET-CT in PMR. In this regard, in a systematic review of the literature, van der Geest et al. highlighted that the shoulders, sternoclavicular joints, interspinous bursae, ischial tuberosities, hips, and greater trochanters are relevant anatomical areas that should be evaluated by 18F-FDG-PET-CT in patients with suspected PMR [18]. They also concluded that significant FDG uptake at a combination of anatomical sites is highly informative for the diagnosis of PMR [18].
Casadepax-Soulet et al. recently performed a retrospective study in 85 patients with new-onset PMR and 75 controls who underwent 18F-FDG PET-CT [28]. In addition to a quantitative analysis of FDG uptake, they also performed a semiquantitative analysis using the same methodology applied in our report. In this sense, they analyzed the significant absorption of FDG in sixteen sites, corresponding to the nine areas studied in our work. Patients with new-onset PMR had a significantly higher mean number of sites with significant FDG uptake than controls [28]. The most common sites of significant FDG uptake were the hips, shoulders, and ischial tuberosity, with 89%, 88%, and 88% significant FDG uptake, respectively. Although the location of hypermetabolic involvement was not very different from that found in our study, the frequency of increased FDG uptake was greater than in our series of PMR associated with LVV. The smaller number of patients included in our study and the different type of patients, since they basically evaluated patients with an initial diagnosis of PMR while we analyzed patients who in all cases presented LVV, may explain these differences.
Shoulder involvement is the hallmark of PMR. This area showed the highest frequency of significant FDG uptake (76.2%) in our series. This was greater than in the series of 50 patients with PMR reported by Sondag et al. (58%) [16] but lower than that reported by Henckaerts et al. and Yamashita et al. who studied 99 consecutive patients with a possible clinical diagnosis of PMR and 14 untreated patients with active PMR, respectively [17,29].
In keeping with Casadepax-Soulet et al. who described in their PMR series a low frequency of significant FDG uptake in the acromioclavicular joints compared to other areas [28], patients with PMR associated with LVV-GCA in our series had a lower frequency of significant FDG uptake in acromioclavicular and sternoclavicular involvement. Furthermore, we observed no statistically significant differences in hypermetabolic FDG uptake in these areas when comparing LVV-GCA with PMR to those without PMR.
Several studies showed a strong correlation of cervical interspinous bursitis seen as high-contrast enhancement magnetic resonance imaging and high 18F-FDG-PET-CT uptake in patients with PMR [4,29]. A strong association between interspinous bursitis in the lumbar spine with PMR was also disclosed using MRI [30]. In this regard, increased FDG uptake in the interspinous process seems to have high specificity for PMR [31,32]. This was also the case in our series of PMR associated with LVV-GCA. In this sense, the presence of significant FDG uptake in the lumbar interspinous process was one of the predictors of PMR in LVV-GCA found in our study.
In our study we also aimed to establish the best cut-off point for the diagnosis of PMR in patients with LVV-GCA. We found that a model including patients with more than 4 sites of significant FDG uptake produced high specificity (91%) but low sensitivity (52%) for a clinical diagnosis of PMR in patients with LVV-GCA. In contrast, Casadepax-Soulet et al. achieved much better sensitivity and specificity. They described that ≥5 hypermetabolic sites provided a sensitivity of 96.5% and a specificity of 100% for the diagnosis of PMR [28]. Lower sensitivity and specificity for the diagnosis of PMR have been reported in other studies and these differences may be explained by the different definitions of significant FDG uptake and the different scoring system, as well as the variable use of glucocorticoids before 18F-FDG-PET-CT evaluation. However, although we were unable to achieve robust cutoffs for diagnosing PMR in patients with LVV, we observed that a model with three locations (shoulder, greater trochanter, and lumbar interspinous) was very useful in identifying clinical PMR in LVV-GCA patients. Of note, Flaus et al. established a decision tree with only two extravascular musculoskeletal sites to make a diagnosis of PMR by 18F-FDG PET-CT [33]. These authors used machine learning to define a short decision tree capable of detecting patients with PMR in a large retrospective cohort that included 55 patients with PMR and 85 patients with other inflammatory rheumatic diseases. Machine learning facilitated increasing the diagnostic value of visually assessed musculoskeletal sites. Splitting rules of the decision tree were based on a positive interspinous bursa or, if negative, a positive trochanteric bursa. Following the decision tree, the sensitivity and specificity for diagnosing PMR were respectively 73.2 and 87.5% in the training cohort and 78.6 and 80.1% in the validation cohort [33]. In agreement with these results, besides shoulders, greater trochanter and lumbar interspinous process were the best areas of significant FDG to clinically identify PMR in patients with LVV-GCA in our study.
As mentioned above, an important difference between our study and most reports on 18F-FDG-PET-CT in PMR was that all of our patients had been diagnosed with LVV-GCA. In this sense, classic studies highlighted the frequent overlap between PMR and GCA [34]. This fact has recently been discussed in depth by Salvarani et al. [35]. Patients with isolated PMR have some clinical differences from patients with biopsy-proven GCA who exhibit the classic cranial pattern of the disease. In comparison, patients with isolated PMR were found to be younger, with a lower frequency of constitutional manifestations, and a less severe inflammatory response manifested by lower ESR levels, higher hemoglobin values, and lower platelet counts than patients with PMR associated with biopsy-proven GCA [36]. This does not appear to be the case when silent LVV-GCA is diagnosed in patients presenting as isolated PMR. In this regard, patients with the predominant extracranial LVV-GCA phenotype are generally younger, have a longer duration of symptoms before GCA diagnosis, have more disease relapses, show less frequently a positive temporal artery biopsy, and generally require a longer duration of treatment [37]. Furthermore, these patients have features of PMR more frequently than those with the predominantly cranial pattern of GCA [35,37,38]. This fact may indicate that in some cases PMR may constitute a warning sign of the possible presence of an underlying LVV-GCA [35,38]. In this sense, Salvarani et al. noted that LVV-GCA is observed in at least 22-25% of patients presenting with isolated PMR [35]. This high number of patients with silent LVV-GCA raises the question of whether we should routinely perform an imaging technique to identify underlying LVV-GCA in patients with PMR. Certainly, early identification of a LVV-GCA can help prevent vascular complications such as aortic aneurysms and dissection and arterial stenosis [39]. Moreover, 18F-FDG-PET-CT performed at the time of LVV-GCA diagnosis can help estimate the risk of aortic aneurysm formation [40]. With respect to this, we recently proposed that imaging techniques should be used to identify an underlying LVV in patients presenting with PMR without the typical cranial ischemic manifestations of GCA if they have inflammatory low back pain, severe pelvic girdle manifestations, bilateral diffuse pain in the lower extremities, presence of a high inflammatory response manifested by an ESR greater than 80-90 mm/1st hour, thrombocytosis or a hemoglobin lower than 11 g/dl or an incomplete response to 20 mg/day of prednisone [41].
Since 18F-FDG-PET-CT remains an expensive technique, we recently suggested that in typical cases of GCA associated with cranial ischemic manifestations, Doppler ultrasound and/or biopsy of the temporal arteries should be the first tools to be used to confirm a diagnosis of GCA [22]. Because of that, in clinical practice we perform 18F-FDG-PET-CT when GCA is suspected, and cranial ischemic manifestations are not relevant. In keeping with to this procedure, Desvages et al. pointed out that the use of 18F-FDG-PET/CT should not be routinely recommended in typical cases of PMR [42]. These authors recommend performing 18F-FDG-PET-CT if patients with PMR present some atypical features, serological markers of inflammation are not high, or if there is a history of cancer. Nevertheless, these authors confirmed that 18F-FDG-PET-CT can be an important diagnostic tool in patients with suspected PMR [42].
We realize that our study has several limitations, mainly due to its retrospective nature and the number included in the assessment. However, it also has strengths. The most important is the monocentric design with the inclusion of consecutive LVV-GCA patients homogeneously evaluated and the careful analysis of the imaging by a highly experienced nuclear medicine physician. Furthermore, unlike most studies that addressed 18F-FDG-PET-CT in PMR, we studied the role of 18F-FDG-PET-CT in identifying PMR in patients diagnosed with LVV-GCA.
In conclusion, significant extravascular 18F-FDG-PET-CT uptake may help establish a clinical diagnosis of PMR in patients with LVV-GCA. These patients are most commonly diagnosed with PMR if they have significant FDG uptake in the shoulder, greater trochanter, and lumbar interspinous areas.
5. Significance and Innovation
- 18F-FDG-PET-CT may be a useful diagnostic tool to identify PMR in patients with LVV-GCA.
- In patients with LVV-GCA, the presence of significant 18F-FDG-PET-CT uptake in the shoulder, greater trochanter and lumbar interspinous areas allows PMR to be identified.
Author Contributions
Conceptualization, E.H-R. and M.A. G-G.; Methodology, E.H-R., L.C.L-K., M.M.B-A., L.M-D., JL. and M.A. G-G.; Software, JL. and J.A.M-L.; Validation, E.H-R., L.C.L-K, M.M.B-A., L.M-D. and M.A. G-G, Formal analysis, E.H-R., IJL.,R.L. and M.A. G-G.; Investigation, E.H-R., T.B-S., A.T-R., M.A-R., M.B-G. and M.A. G-G.; Resources, M.A. G-G.; Writing–original draft, E.H-R., R.L. and M.A. G-G; Supervision, M.A. G-G. All authors have read and agreed to the submitted version of the manuscript.
Funding
Funding for this study were provided by the Instituto de Salud Carlos III (Spain) through grant FIS PI22/01263 (PI: Dr. Miguel A. González-Gay) and the Spanish Red de Investigación RICORS RD21/0002/0025 (PI: Miguel A. González-Gay).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethic Committee of IIS-Fundación Jiménez Díaz, Madrid, Spain.
Informed Consent Statement
Patient consent was waived due to the retrospective design of the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We thank Antonio Herrero González, Head of the Big Data Department at the Jiménez Díaz Foundation Hospital, Madrid, Spain for his available help in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Salvarani, C.; Cantini, F.; Hunder, G.G. Polymyalgia rheumatica and giant-cell arteritis. Lancet 2008, 372, 234–245. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gay, M.A.; Vazquez-Rodriguez, T.R.; Lopez-Diaz, M.J.; Miranda-Filloy, J.A.; Gonzalez-Juanatey, C.; Martin, J.; Llorca, J. Epidemiology of giant cell arteritis and polymyalgia rheumatica. Arthritis Care Res. 2009, 61, 1454–1461. [Google Scholar] [CrossRef] [PubMed]
- A González-Gay, M.; Matteson, E.L.; Castañeda, S. Polymyalgia rheumatica. Lancet 2017, 390, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Pipitone, N.; Versari, A.; Hunder, G.G. Clinical features of polymyalgia rheumatica and giant cell arteritis. Nat. Rev. Rheumatol. 2012, 8, 509–521. [Google Scholar] [CrossRef]
- Serling-Boyd, N.; Stone, J.H. Recent advances in the diagnosis and management of giant cell arteritis. Curr. Opin. Rheumatol. 2020, 32, 201–207. [Google Scholar] [CrossRef]
- Prieto-Peña, D.; Castañeda, S.; Martínez-Rodríguez, I.; Atienza-Mateo, B.; Blanco, R.; González-Gay, M.A. Imaging Tests in the Early Diagnosis of Giant Cell Arteritis. J. Clin. Med. 2021, 10, 3704. [Google Scholar] [CrossRef]
- van der Geest, K.S.; Slijkhuis, B.G.; Tomelleri, A.; Gheysens, O.; Jiemy, W.F.; Piccolo, C.; Nienhuis, P.; Sandovici, M.; Brouwer, E.; Glaudemans, A.W.; et al. Positron Emission Tomography Imaging in Vasculitis. Cardiol. Clin. 2023, 41, 251–265. [Google Scholar] [CrossRef]
- Germanò G, Versari A, Muratore F, Pipitone N, Bajocchi GL, Catanoso MG, Salvarani C. Isolated vasculitis of the lower extremities in a patient with polymyalgia rheumatica and giant cell arteritis. Clin Exp Rheumatol. 2011, 29, S138–S139. [PubMed]
- Duftner, C.; Dejaco, C.; Sepriano, A.; Falzon, L.; Schmidt, W.A.; Ramiro, S. Imaging in diagnosis, outcome prediction and monitoring of large vessel vasculitis: a systematic literature review and meta-analysis informing the EULAR recommendations. RMD Open 2018, 4, e000612. [Google Scholar] [CrossRef]
- Schäfer, V.S.; Jin, L.; Schmidt, W.A. Imaging for Diagnosis, Monitoring, and Outcome Prediction of Large Vessel Vasculitides. Curr. Rheumatol. Rep. 2020, 22, 1–14. [Google Scholar] [CrossRef]
- Cantini, F.; Salvarani, C.; Niccoli, L.; Nannini, C.; Boiardi, L.; Padula, A.; Olivieri, I.; Valentino, M.; Barozzi, L. Fat suppression magnetic resonance imaging in shoulders of patients with polymyalgia rheumatica. J Rheumatol. 2004, 31. [Google Scholar]
- Cantini, F.; Salvarani, C.; Olivieri, I.; Niccoli, L.; Padula, A.; Macchioni, L.; Boiardi, L.; Ciancio, G.; Mastrorosato, M.; Rubini, F.; et al. Shoulder ultrasonography in the diagnosis of polymyalgia rheumatica: a case-control study. J Rheumatol. 2001, 28, 1049–55. [Google Scholar]
- Cantini F, Salvarani C, Olivieri I, Niccoli L, Padula A, Bozza A. Hip bursitis in active polymyalgia rheumatica: report of a case. Clin Exp Rheumatol. 1999, 17, 512–513. [PubMed]
- Salvarani, C.; Barozzi, L.; Cantini, F.; Niccoli, L.; Boiardi, L.; Valentino, M.; Pipitone, N.; Bajocchi, G.; Macchioni, P.; Catanoso, M.G.; et al. Cervical interspinous bursitis in active polymyalgia rheumatica. Rheumatol. 2008, 67, 758–761. [Google Scholar] [CrossRef]
- Dasgupta, B.; A Cimmino, M.; Maradit-Kremers, H.; A Schmidt, W.; Schirmer, M.; Salvarani, C.; Bachta, A.; Dejaco, C.; Duftner, C.; Jensen, H.S.; et al. 2012 provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Rheumatol. 2012, 71, 484–492. [Google Scholar] [CrossRef]
- Sondag, M.; Guillot, X.; Verhoeven, F.; Blagosklonov, O.; Prati, C.; Boulahdour, H.; Wendling, D. Utility of 18F-fluoro-dexoxyglucose positron emission tomography for the diagnosis of polymyalgia rheumatica: a controlled study. Rheumatol. 2016, 55, 1452–1457. [Google Scholar] [CrossRef]
- Henckaerts, L.; Gheysens, O.; Vanderschueren, S.; Goffin, K.; Blockmans, D. Use of 18F-fluorodeoxyglucose positron emission tomography in the diagnosis of polymyalgia rheumatica—A prospective study of 99 patients. Rheumatol. 2017, 57, 1908–1916. [Google Scholar] [CrossRef]
- van der Geest, K.S.M.; Treglia, G.; Glaudemans, A.W.J.M.; Brouwer, E.; Jamar, F.; Slart, R.H.J.A.; Gheysens, O. Diagnostic value of [18F]FDG-PET/CT in polymyalgia rheumatica: a systematic review and meta-analysis. Eur. J. Nucl. Med. 2020, 48, 1876–1889. [Google Scholar] [CrossRef]
- Moya-Alvarado, P.; Leon, A.F.; Corica, M.E.; Marti, V.C.; López-Mora, D.A.; Castellví, I.; Corominas, H. "The added value of 18f-FDG PET/CT in the assessment of onset and steroid resistant polimyalgia rheumatica". PLOS ONE 2021, 16, e0255131. [Google Scholar] [CrossRef]
- Rehak, Z.; Vasina, J.; Nemec, P.; Fojtik, Z.; Koukalova, R.; Bortlicek, Z.; Rehakova, D.; Adam, J.; Vavrusova, A.; Adam, Z. Various forms of 18F-FDG PET and PET/CT findings in patients with polymyalgia rheumatica. Biomed. Pap. 2015, 159, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Peña, D.; Martínez-Rodríguez, I.; Loricera, J.; Banzo, I.; Calderón-Goercke, M.; Calvo-Río, V.; González-Vela, C.; Corrales, A.; Castañeda, S.; Blanco, R.; et al. Predictors of positive 18F-FDG PET/CT-scan for large vessel vasculitis in patients with persistent polymyalgia rheumatica. Semin. Arthritis Rheum. 2019, 48, 720–727. [Google Scholar] [CrossRef]
- Heras-Recuero, E.; Landaeta-Kancev, L.C.; de Bourio-Allona, M.M.; Torres-Rosello, A.; Blázquez-Sánchez, T.; Ferraz-Amaro, I.; Castañeda, S.; Martínez-López, J.A.; Martínez-Dhier, L.; Largo, R.; et al. Positron Emission Computed Tomography Spectrum of Large Vessel Vasculitis in a Tertiary Center: Differences in 18F-fluorodeoxyglucose Uptake between Large Vessel Vasculitis with Predominant Cranial and Extracranial Giant Cell Arteritis Phenotypes. J. Clin. Med. 2023, 12, 6164. [Google Scholar] [CrossRef]
- González-Gay, M.A.; Rodríiguez-Valverde, V.; Blanco, R.; Fernández-Sueiro, J.L.; Armona, J.; Figueroa, M.; Martínez-Taboada, V.M. Polymyalgia Rheumatica Without Significantly Increased Erythrocyte Sedimentation Rate. Arch. Intern. Med. 1997, 157, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Cantini F, Salvarani C, Olivieri I, Niccoli L, Macchioni P, Boiardi L, et al. Inflamed shoulder structures in polymyalgia rheumatica with normal erythrocyte sedimentation rate. Arthritis Rheum. 2001, 44, 1155–1159. [CrossRef] [PubMed]
- A Gonzalez-Gay, M.; Garcia-Porrua, C.; Salvarani, C.; Olivieri, I.; Hunder, G.G. The spectrum of conditions mimicking polymyalgia rheumatica in Northwestern Spain. J Rheumatol. 2000, 27, 2179–2184. [Google Scholar]
- Paltta, J.; Suuronen, S.; Pirilä, L.; Palomäki, A. Differential diagnostics of polymyalgia rheumatica in a university hospital in Finland. Scand. J. Rheumatol. 2023, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Slart, R.H.J.A.; Writing Group. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1250–1269. [Google Scholar] [CrossRef] [PubMed]
- Casadepax-Soulet, C.; Benali, K.; Crestani, B.; Piekarski, E.; Mahida, B.; Ebstein, E.; Juge, P.-A.; Forien, M.; Dieudé, P.; Ottaviani, S. Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography in polymyalgia rheumatica: an observational study. Rheumatol. 2022, 41, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, H.; Kubota, K.; Takahashi, Y.; Minaminoto, R.; Morooka, M.; Ito, K.; Kano, T.; Kaneko, H.; Takashima, H.; Mimoiri, A. Whole-body fluorodeoxyglucose positron emission tomography/computed tomography in patients with active polymyalgia rheumatica: evidence for distinctive bursitis and large-vessel vasculitis. Mod. Rheumatol. 2011, 22, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Salvarani C, Barozzi L, Boiardi L, Pipitone N, Bajocchi GL, Macchioni PL, et al. Lumbar interspinous bursitis inactive polymyalgia rheumatica. Clin Exp Rheumatol. 2013, 31, 526–531. [PubMed]
- Owen, C.E.; Poon, A.M.T.; Yang, V.; McMaster, C.; Lee, S.T.; Liew, D.F.L.; Leung, J.L.; Scott, A.M.; Buchanan, R.R.C. Abnormalities at three musculoskeletal sites on whole-body positron emission tomography/computed tomography can diagnose polymyalgia rheumatica with high sensitivity and specificity. Eur. J. Nucl. Med. 2020, 47, 2461–2468. [Google Scholar] [CrossRef]
- Rehak, Z.; Vasina, J.; Nemec, P.; Fojtik, Z.; Koukalova, R.; Bortlicek, Z.; Rehakova, D.; Adam, J.; Vavrusova, A.; Adam, Z. Various forms of 18F-FDG PET and PET/CT findings in patients with polymyalgia rheumatica. Biomed. Pap. 2015, 159, 629–636. [Google Scholar] [CrossRef]
- Flaus, A.; Amat, J.; Prevot, N.; Olagne, L.; Descamps, L.; Bouvet, C.; Barres, B.; Valla, C.; Mathieu, S.; Andre, M.; et al. Decision Tree With Only Two Musculoskeletal Sites to Diagnose Polymyalgia Rheumatica Using [18F]FDG PET-CT. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Gonzalez-Gay, M.A. Giant cell arteritis and polymyalgia rheumatica: two different but often overlapping conditions. Semin. Arthritis Rheum. 2004, 33, 289–293. [Google Scholar] [CrossRef]
- Salvarani, C.; Padoan, R.; Iorio, L.; Tomelleri, A.; Terrier, B.; Muratore, F.; Dasgupta, B. Subclinical giant cell arteritis in polymyalgia rheumatica: Concurrent conditions or a common spectrum of inflammatory diseases? Autoimmun. Rev. 2023, 103415. [Google Scholar] [CrossRef] [PubMed]
- A González-Gay, M.; García-Porrúa, C.; Vázquez-Caruncho, M. Polymyalgia rheumatica in biopsy proven giant cell arteritis does not constitute a different subset but differs from isolated polymyalgia rheumatica. J Rheumatol. 1998, 25, 1750–1755. [Google Scholar]
- Muratore, F.; Kermani, T.A.; Crowson, C.S.; Green, A.B.; Salvarani, C.; Matteson, E.L.; Warrington, K.J. Large-vessel giant cell arteritis: a cohort study. Rheumatology 2014, 54, 463–470. [Google Scholar] [CrossRef]
- Farina, N.; Tomelleri, A.; Campochiaro, C.; Dagna, L. Giant cell arteritis: Update on clinical manifestations, diagnosis, and management. Eur. J. Intern. Med. 2022, 107, 17–26. [Google Scholar] [CrossRef]
- Therkildsen, P.; de Thurah, A.; Nielsen, B.D.; Hansen, I.T.; Eldrup, N.; Nørgaard, M.; Hauge, E.-M. Increased risk of thoracic aortic complications among patients with giant cell arteritis: a nationwide, population-based cohort study. Rheumatol. 2021, 61, 2931–2941. [Google Scholar] [CrossRef] [PubMed]
- Moreel, L.; Coudyzer, W.; Boeckxstaens, L.; Betrains, A.; Molenberghs, G.; Vanderschueren, S.; Claus, E.; Van Laere, K.; Blockmans, D. Association Between Vascular 18F-Fluorodeoxyglucose Uptake at Diagnosis and Change in Aortic Dimensions in Giant Cell Arteritis. Ann. Intern. Med. 2023. [Google Scholar] [CrossRef] [PubMed]
- González-Gay, M.A.; Vicente-Rabaneda, E.F.; Heras-Recuero, E.; Castañeda, S. Polymyalgia rheumatica: when should we suspect an underlying large vessel vasculitis? Rheumatology 2023, 41, 774–776. [Google Scholar] [CrossRef]
- Desvages, A.; Hives, F.; Deprez, X.; Pierache, A.; Béhal, H.; Flipo, R.-M.; Paccou, J. Usefulness of 18F-Fluorodeoxyglucose Positron Emission Tomography in Diagnosing Polymyalgia Rheumatica and Large-Vessel Vasculitis: A Case-Control Study. J. Clin. Med. 2023, 12, 2844. [Google Scholar] [CrossRef]
Figure 2.
ROC curve on the ability of a model with three locations (shoulder, greater trochanter and lumbar interspinous) to identify clinical PMR. The area under the ROC curve is 0.810 (95% CI: 0.691, 0.930).
Figure 2.
ROC curve on the ability of a model with three locations (shoulder, greater trochanter and lumbar interspinous) to identify clinical PMR. The area under the ROC curve is 0.810 (95% CI: 0.691, 0.930).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



