
Submitted:
09 October 2023
Posted:
10 October 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
To describe the main health surveillance strategies for the control of COVID-19 in Brazil, with emphasis on decisions and actions taken at the federal level to prevent the infection caused by the new SARS-CoV-2. This is a scoping review study carried out from November 2019 to January 2021 using the DECS and MeSH health descriptors in Portuguese and English in four databases, in addition to the legislation found on the Brazilian Government's legislation portal. Based on the analysis of the documents, the actions describe non-pharmacological and pharmacological measures, measures related to decisions on closing and opening international borders, the acquisition of supplies and essential services. Although some strategies for containing the pandemic were identified, discrete and unnoticed surveillance measures are observed in view of the number of cases and number of deaths during the period of research analysis. The results show the absence of the federal level as support for the states and municipalities and imply decision-making and planning of actions by the Unified Health System to control the pandemic.
Keywords:
Ministry of Health
; Public Health Surveillance
; COVID-19
; Brazil
1. Introduction
In December 2019, scientists identified a new coronavirus that was associated with an outbreak of pneumonia in Wuhan, China 1. Within weeks, more than 100,000 cases and thousands of deaths were confirmed globally, with numbers increasing rapidly daily 2. In view of this scenario, the World Health Organization (WHO) declared the outbreak a public health emergency of international concern on 30 January 2020. From that moment on, public health authorities mobilized to communicate critical information to the public, aiming to provide decision-making power for communities, organizations and individuals, so that they could take the necessary and appropriate precautions and governments could develop plans that could respond to the situation 3.
Several countries adopted strategies to face and control the COVID-19 pandemic, such as mass testing, contact tracing, social isolation and other public health and social measures. These were crucial to slow down disease transmission and reduce mortality. Minimizing the transmission of the virus, through the implementation of lockdowns, social distancing and isolation of those infected, was a major focus in most developed countries 4.
In fact, the main objective was to promote the so-called flattening of the curve 5. These measures were expected to reduce the burden on health systems, allowing the successful treatment of severe cases and thus reducing mortality in general 6.
In a historical context, the first confirmed case of COVID-19 in Brazil was on recorded on 26 February 2020 7. From then on, the number of cases increased and the disease spread rapidly 8. Although the scientific community declared a global public health emergency situation, this was minimized by the administration of the President of the Republic in Brazil, thus causing the delay of health measures aimed at preventing the disease in the country 9.
In this scenario of weak management and insecurity with the dissemination of fake news, society was plagued by incoherent discussions of information about the pandemic that were disconnected from the guidelines of Brazilian health surveillance 10.
A robust health surveillance is crucial to control the spread of diseases and guide the continuous implementation of prevention measures. It is essential in a public health system, since surveillance collects, analyzes and performs a continuous systematic interpretation of data, in addition to providing decision makers with directions, planning and timely intervention on the problem 11.
This scoping review addresses topics on control measures and the strategies and actions announced by the Brazilian government, along a timeline, from the first case of the disease detected in the country to January 2021. It is expected that this review can contribute to reflection on the subject, regarding the course of the new coronavirus pandemic in the country amid contradictions between the federal government and scientific evidence. Therefore, the article aims to describe the main health surveillance strategies in the control of the COVID-19 pandemic in Brazil, with emphasis on decisions and actions taken at the federal level to prevent the infection caused by SARS-CoV-2.
2. Method
2.1. Data Sources and Research Strategy
The present is a scoping review study. To carry out this review, a search strategy was carried out through the construction of concept mapping, in Portuguese and in English, using the acronym PCC with problem elements contained in the following research question: What are the actions to control COVID-19 and the measures adopted by the Federal Government of Brazil to control the disease? In this acronym, “P” represents the population under study, that is, people with COVID-19; the letter “C” includes the concept terms related to the research phenomenon, in this case, health surveillance actions; and “C” refers to terms related to the context, that is, Brazil. The terms were defined and identified in the DeCS and MeSH databases through concept mapping, and a search strategy was defined for each of the databases, which included: Pubmed, Embase, Scopus and Virtual Health Library (VHL). The health descriptors used in the search comprised: Brazil, Ministry of Health (MoH), Health Surveillance Secretariat (SVS, Secretaria de Vigilância de Saúde), Public Health Surveillance, Epidemiological Monitoring, Epidemiology, Health Services Research, Prevention and Control, Communicable Disease Control, Health Police, Coronavirus infections, Beta Coronavirus, COVID-19, in Portuguese and English.
2.2. Inclusion Criteria
The inclusion criteria were documents that dealt with Brazil, addressing health surveillance measures in COVID-19 and were within the pre-established period, with no language restriction.
2.3. Study Period
The period selected for the study had as its starting point the beginning of the pandemic in November 2019 in Wuhan (China) and data collection was until January 2021.
2.4. Study Selection
Together with the descriptors, Boolean operators AND and OR were used to constitute the search keys to be used for searches in the databases. First, we used AND within the same category (P, C and C) and then OR among them, to obtain the results. The search syntax, combining the descriptors, keywords and their variants are described in Table 1.
The identified articles were sent to the Mendeley platform to have duplicates removed and then were exported to the Rayyan platform (12). This tool was used to read the titles and abstracts of the articles and categorize the included, excluded and "doubtful" references. The blind reading of titles and abstracts of the articles was performed by two researchers (LAB and PHB). The articles selected according to the inclusion criteria were read in full.
The search for articles was also carried out in the gray literature on the Federal Government legislation portal, in the period between 4 February 2020 and 31 January 2021. Within this period, the following were included in the study: laws, decrees, ordinances, resolutions related to COVID-19. The reading of the title and caput of the laws was carried out by two researchers (LAB and PHB) blindly. The legislation that fit the definition of health surveillance measures in the fight against the new coronavirus were included. Discrepancies regarding the selection of documents were resolved by consensus. For data extraction, an instrument on the RedCap platform was created, including variables about the studies and for the identification of surveillance measures. After this step, the data were exported to a spreadsheet constructed using Microsoft Office® Excel®, generated by RedCap® itself to verify discrepancies in the data extraction. To describe the results, we used the flowchart proposed by the PRISMA guide.13 And for the writing of this article, we followed the PRISMA Extension for Scoping Reviews (PRISMA-ScR).
3. Results
The search strategy resulted in the identification of 9951 articles in the four searched databases and after excluding the duplicates, a total of 9935 articles remained, to which the two researchers applied the exclusion criteria. After this step, 234 articles were selected to be read in full. Of these, only ten were included in this review, as they met the inclusion criteria. Regarding the gray literature, it was searched manually, totaling in 535 documents. Of these, 85 entered the scope review. These data are illustrated in the flowchart (Figure 1).
The documents related to legislations published by the Federal Government by categories of surveillance measures aimed to fight COVID-19 are shown in Figure 2.
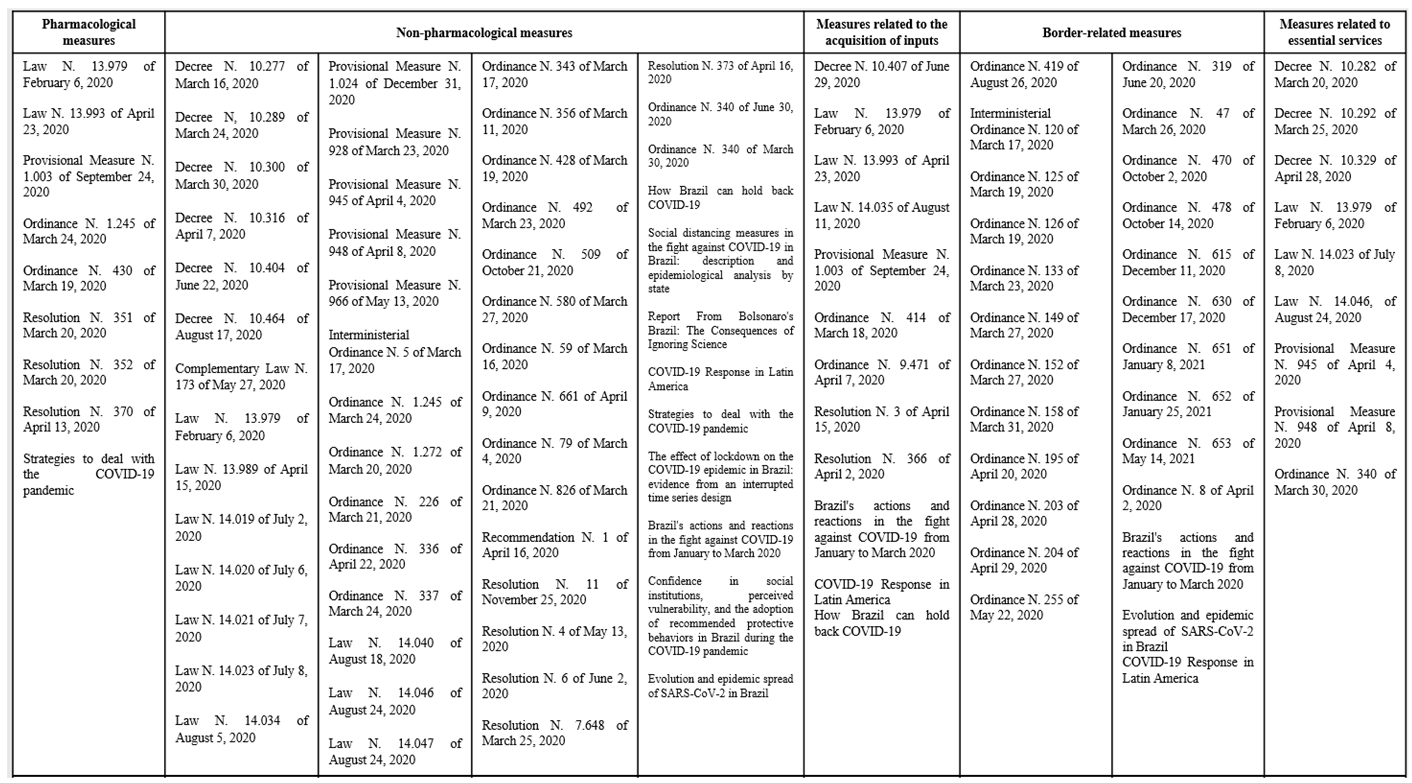
Based on the analysis of the documents, according to the inclusion criteria, 55% describe non-pharmacological measures, 9% pharmacological measures and 25% are related to decisions on the closing and opening of international borders, 12% were measures related to the acquisition of supplies, 5% fit into the “other” category and only 9% are related to essential services. The main measures are organized along a timeline by cat (Figure 3). The official documents and scientific articles included in the study are organized in Table 2.
On February 3, 2020, the government declared a Public Health Emergency of National Concern (PHENC), establishing the Public Health Emergency Operations Center (COE-NCoV, Centro de Operações de Emergências em Saúde Pública) as a national mechanism for the coordinated management in response to the emergency at national level 14.
On February 6, 2020, Law N. 13,979 was enacted, which provides for measures to fight the COVID-19 epidemic and lists the community Non-Pharmacological Interventions (NPI) that could be adopted 15. In this legal instrument, the federal government points out that it could adopt a series of measures to face the public health emergency, including: social isolation, quarantine, compulsory examinations, tests, vaccination, treatments, studies or epidemiological investigations, restrictions on entering and leaving the country, among others. Additionally, this law provided for the importation of materials, medications, equipment and supplies considered essential to help fight the coronavirus pandemic. This legislation also lists all professionals considered essential for disease control and maintenance of public order 15.
Also in February 2020, the MoH published the National Contingency Plan for Human Infection by the new Coronavirus (COVID-19); this plan subsequently had two more versions 16. On March 11, 2020, the Government issued Ordinance N. 356, regulating and implementing measures to face the public health emergency caused by the new coronavirus (COVID-19). This document established how social isolation and quarantine measures would be adopted. For the application of isolation and quarantine measures, the clinical protocols for the coronavirus (COVID-19) and the guidelines established in the National Contingency Plan for Human Infection by the new Coronavirus (COVID-19) should be observed, aiming to guarantee the performance of prophylactic measures and the necessary treatment 16.
Moreover, it established that the conditions for carrying out the measures to face the public health emergency are provided for in the aforementioned Epidemiological Bulletin and National Contingency Plan 17.
On March 14, the MoH issued a publication that contained recommendations on non-pharmacological intervention measures to be adopted 13. Overall, it included recommendations to promote personal and public hygiene; the isolation of people with symptoms for 14 days and the use of personal protective equipment (PPE) for patients and health professionals.
On March 16, 2020, Ordinance 59 was published, establishing the Integrated Office for the Monitoring of the Coronavirus-19 Epidemic (GIAC-COVID19, Gabinete Integrado de Acompanhamento à Epidemia do Coronavírus-19). The mission of the GIAC-COVID19 was to support the Attorney General's Office to ensure, from an administrative perspective, the operation of the Federal Public Ministry Office bodies and, from the ultimate perspective of defending the general interests of society, to promote the integration of the Brazilian Federal Public Ministry during the exercise of its functions in the fight against the COVID-19 epidemic 18.
At the same time, the Crisis Committee for Supervising and Monitoring the Impacts of COVID-19 was established, through Decree N. 10,277. This governmental body aimed at articulating government actions, advising the President of the Republic on the situational awareness of issues arising from the COVID-19 pandemic and the discussion of priorities, guidelines and strategic aspects related to the impacts of COVID-19 19.
On March 17, 2020, The Ministry of Education and Culture (MEC) published Ordinance N. 343, which provided for the replacement of in-person classes by remote ones using digital media classes (DE, distance education), while the pandemic situation lasted 20.
However, on March 19, the MoH legislated on those protective measures to deal with the public health emergency of international importance caused by the coronavirus (COVID-19) within the scope of the MoH units in the Federal District and in the federation states. This Ordinance characterized which public servants and employees should work remotely, aiming to safeguard the health of the so-called risk groups: the elderly, individuals with immunodeficiency, people with comorbidities, pregnant and lactating women 21.
On March 23, Ordinance N. 492 was published, establishing the Strategic Action “Brazil is Counting on Me”, aimed at students of courses in the health area, to face the coronavirus pandemic (COVID-19). This Ordinance aimed to optimize the availability of health services within the scope of the Brazilian Unified Health System (SUS, Sistema Único de Saúde) to contain the COVID-19 pandemic, in an integrated manner with undergraduate activities in the health area 22.
On April 7, Decree N. 10,316 was published, which establishes exceptional social protection measures to be adopted during the period of coping with the public health emergency of international importance resulting from the coronavirus (COVID-19). It established an emergency cash transfer program that paid R$ 600.00 (six hundred reais), which at that time would be granted for a period of three months 23.
On April 8, Provisional Measure N. 948 was enacted, which addressed events in the tourism and culture sectors during the pandemic; this measure was revoked and converted into Law N. 14046 in August of the same year 24.
Law N. 13,989 of April 15 provided for the authorization of the use of telemedicine during the pandemic. Telemedicine is understood, among others, as the practice of Medicine mediated by technologies for the purposes of assistance, research, prevention of diseases and injuries and health promotion 15.
On July 2, Law N. 14,019 established the mandatory use of individual face masks to circulate in public and private spaces, on public streets and in public transport. The obligation provided for in the caput of this article was waived in the case of people in the autism spectrum disorder, those with intellectual disabilities, sensory impairments or any other disabilities that prevented them from adequately using a face mask for protection against COVID-19, provided through a medical declaration of exemption, which could be obtained digitally, as well as in the case of children under 3 years of age 25.
Up to the 6th of July, there were no technical recommendations provided by the MoH regarding people under precarious living conditions, such as in slums and with no access to water, and Brazilian indigenous communities.
It was only on July 7, through Law N. 14,021, that the social protection of indigenous territories was described for the first time, also specifying measures to support quilombola communities, artisanal fishermen and other peoples and traditional communities to face COVID-19. Although it mentions traditional communities, the document does not specifically describe slums or specific actions for the reality in these places 26.
Seven long months after the establishment of the emergency cash transfer through Resolution N. 11 of November 25, 2020, a working group was implemented to coordinate the protection measures and provide the accountability of the benefits. This group was also responsible for proposing a coordination strategy among the social protection measures, proposing accountability mechanisms for recipients of social programs and evaluating and proposing, where applicable, the development of a simplified mechanism for the monthly registration updating by recipients of federal social programs 27.
3.1. Measures related to international borders
On March 19, Ordinance N. 125 was published, which addressed the exceptional and temporary restrictions on the entry of foreigners in Brazil, originating from the following countries: Argentina, Bolivia, Colombia, French Guiana, Guyana, Paraguay, Peru and Suriname. These restrictions were renewed through Ordinance N. 08, of April 2, as recommended by the National Health Surveillance Agency – Anvisa 28.
Ordinance n. 126, published on the same day, restricted the entry into the country, by air, of foreigners from the following countries for 30 days: China, European Union, Iceland, Norway, Switzerland, United Kingdom of Great Britain and Northern Ireland, Australia, Japan, Malaysia and Korea 30.
The disembarkation of foreigners at a port or point in the Brazilian territory, by waterway, was restricted for a period of thirty days, regardless of their nationality, through Ordinance N. 47, of March 26, 2020 31.
Five day later, Ordinance n. 152 restricted, for a period of thirty days, the entry into the country, by air, of foreigners, regardless of their nationality. On March 31, 2020, Ordinance N. 158 restricted, for a period of thirty days, the entry into the country, by road or land, of foreigners from the Bolivarian Republic of Venezuela 32.
By the end of 2020, these restrictions had been updated 25 times by Anvisa, temporarily restricting the entry of foreigners into the country. These ordinances often dealt with countries in Latin America, which share borders with Brazil, but also with foreigners from anywhere in the world. In April 2020, the Executive Office of the President of Brazil started to publish ordinances that restricted the entry of foreigners of any nationality, by road, by other land or waterway transport, and in some periods, by air. In January 2021, this Ordinance was updated, highlighting this restriction due to the new variants of SARS-CoV-2 that were circulating.
On March 26, 2020, the Office of the Vice President of Brazil signed an Ordinance restricting the entry of foreigners into the country by waterway transport. This Ordinance was revoked and updated several times during the year. These also established rules for foreigners who were on Brazilian soil and wanted to return to their countries of origin 31.
3.2. Pharmacological Measures
On March 20, Anvisa published Resolution N. 351, which provides for the update of Annex I (Lists of Narcotic, Psychotropic, Precursor and Other Substances under Special Control), and this Differentiated Contract Regime (RDC, Regime Diferenciado de Contratação) includes Chloroquine and Hydroxychloroquine in the list of special control drugs in category C. Chloroquine and hydroxychloroquine-based drugs are subject to the Special Control Prescription requiring two copies, the 1st copy being retained at the pharmaceutical establishment and the 2nd copy returned to the patient 33.
On the same day, Resolution N. 352 was also published, which provides for prior authorization for the purpose of exporting chloroquine and hydroxychloroquine, and products subject to health surveillance intended to fight COVID-19. The export of chloroquine, hydroxychloroquine, azithromycin, fentanyl, midazolam, ethosuximide, propofol, pancuronium, vecuronium, rocuronium, succinylcholine and ivermectin in the form of raw material, semi-finished product, bulk product or finished product would temporarily require prior authorization from Anvisa. For the purposes of this Resolution, exports were considered as the exportation of the product in any form or for any export purpose 34.
Also in April, ANVISA published another RDC providing for the importation of products for the in vitro diagnosis of the Coronavirus, and on the ban on exports of medical, hospital and hygiene products essential to fight the pandemic 31.
In September 2020, a provisional measure was signed, authorizing the Federal Executive Branch to adhere to the Instrument for Global Access to COVID-19 Vaccines - COVAX Facility, with the purpose of acquiring vaccines against COVID-19. This Ordinance was converted into Law N. 14121 in March 2021, which established guidelines for the immunization of the population 35.
In January 2021, a provisional measure was published, which dealt with exceptional measures regarding the acquisition of vaccines, supplies, goods and logistics services and the national plan for implementing the vaccination against COVID-19 36.
3.3. Measures related to supply acquisition
On March 18, Ordinance N. 414 was published authorizing the opening of beds in the Adult and Pediatric Intensive Care Units, for the exclusive care of COVID-19 patients 37.
On the following day, the MoH established a federal financial incentive package for Primary Health Care, on an exceptional basis, to support the extended operation of the Family Health Strategy (USF, Unidade de Saúde da Família) or Basic Health Unit (UBS, Unidade Básica de Saúde) in the country to face the pandemic 38.
On April 7, the Ministry of Economy established an additional measure regarding the sale of respiratory protection PPE. This Ordinance established that PPE classified as Air-Purifying Respirators (APRs) of the one-quarter face or half-face type, with a P2 or P3 particulate matter filter, whose Certificates of Approval (CA) that had expired in the period from January 1, 2018 to the date of publication of this Ordinance and which, perhaps, did not yet have new updated evaluation tests, could be sold upon presentation of the test report contained in the Certificate of Approval. This use of expired materials reflects the scarcity of materials for the protection of health professionals that occurred at the beginning of the pandemic 39.
Through Resolution N. 3, of April 15, 2020, a working group was set up for the construction of federal field hospitals and international logistics of medical equipment and health supplies. This group consisted of the following representatives: one from the Executive Office of the President of the Republic, who coordinates it; two from the MoH; and two from the Ministry of Infrastructure 40.
In June, Decree N. 10,407 regulated the law that provided for the prohibition of exports of essential medical, hospital and hygiene products in the fight against COVID-19 in the country.41 On August 4, 2020, the competence for the acquisition of medications, equipment, immunobiologicals, and other health supplies was delegated to the Secretary of Specialized Health Care. This Ordinance was revoked by Ordinance N. 197 of February 2021, delegating this competence to the director of the Department of Logistics in Health 42.
This Ordinance was repealed by Ordinance N. 199 of February 10, 2021, which provided for the deadlines regarding the processes and procedures related to Government bodies and entities of the National Transit system and public and private entities providing services related to transit, to face the COVID-19 pandemic in the state of Amazonas. It had no relation with the purchase of medications and health supplies, not being at the federal level, which demonstrates the disorganization of the MoH management related to the acquisition of these medications and supplies, as well as the publication of laws and ordinances in the fight against COVID-19 43.
On August 11, 2020, Law N. 14,035 was published to provide for procedures related to the acquisition of goods and supplies or the hiring of services to fight the pandemic. This law brought some flexibility regarding purchasing processes 44.
In cases of electronic or in-person bidding, whose object is the acquisition of goods and supplies or hiring of services necessary to face the public health emergency of international importance addressed in this Law, the terms of the bidding procedures were reduced by half. The contracts rules by this Law will have a duration of up to six months and may be extended for successive periods.
4. Discussion
On February 6, 2020, Law N. 13,979 was published, which provided some basic definitions and emphasized the actions the authorities could take to control the pandemic. Among these actions, the following were described: social isolation, quarantine, compulsory examinations, tests, collections, vaccination, epidemiological studies and travel restrictions on roads, ports and airports 46. With the publication of this law, it seemed that Brazil would take a meticulous and firm posture regarding the pandemic, which did not occur. The President of the Republic, from the beginning, showed contempt for the pandemic, refuting control measures and urging the population to “face the virus”. The fact is that three types of non-pharmacological interventions, namely, greater surveillance and hygiene measures; identification and isolation of infected individuals and their contacts; and lockdowns 48 could have been adopted from the beginning to mitigate the impacts of the pandemic. Greater surveillance and hygiene measures aimed at increasing the state of alert, aimed at the entire population, urging everyone to avoid crowds, restrict physical contact and adopt frequent hand washing, cleaning of objects and the use of face masks were expected. However, for these measures to take place, some factors would be required, such as: a population with a good level of schooling, cooperation, discipline and trust in its leaders and authorities 48.
In an attempt to contain the pandemic and enforce rules, on March 17, an Ordinance was published that provided for the compulsory nature of measures to deal with the public health emergency provided for in Law N. 13,979 46.
That said, on June 2, through Resolution N. 6, a working group was created to consolidate the governance and risk management strategies of the federal government in response to the impacts related to the coronavirus. A somewhat late event, given that in June 2020 the pandemic reached its record high in Brazil, even though these figures would later reach new records 50. On June 5, 2020, the WHO released their guidelines for the use and manufacturing of fabric masks as a means of protection against COVID-19 48.
Law N. 14,019 was published only on July 2, 2020, providing for the mandatory use of individual face masks as a requirement for people to circulate in society. It should also be noted that the president himself always appeared without a mask at events, interviews and press conferences 51.
These conflicting messages between the president and health authorities caused a decline in the population’s trust in social institutions, leaving the Brazilian people unsure about the merits of protective measures to prevent the spread of the virus 54.
Another non-pharmacological measure would be the identification and isolation of infected individuals and their contacts, through the so-called mass testing. This intervention consists of identifying infected individuals and their contacts through diagnostic tests and isolation. This intervention is considered to be a high-cost one and requires a great deal of effort to recruit and train workers to perform the tests. In addition, support from the population would also be required, to adhere to the constant testing. The experiences of Asian countries show us that testing should be carried out frequently and on a large scale 48.
In Brazil, the decentralization of testing would be a crucial strategy for increasing the detection of new cases. However, since the beginning of the pandemic, the country has faced some challenges, such as socioeconomic inequalities in the distribution of equipment and in the infrastructure available for this diagnosis 55.
The main issues comprised the limited access and the capacity to screen SARS-CoV-2 cases using Real-Time Polymerase Chain Reaction (RT-PCR). As an example of a successful experience, South Korea offered tests to all suspected cases, being considered an example of how to deal with the COVID-19 pandemic. New Zealand is also an example of successful control of the disease, having managed to control the pandemic in its territory and eliminate community transmission by combining social isolation measures with large-scale testing for contact tracing and rapid detection of cases, in addition to the implementation of quarantine. In Brazil, as described in the literature, factors associated with the low number of SARS-CoV-2 RT-PCR tests performed in the country included: a) difficulty in acquiring supplies to perform the RT-PCR of SARS-CoV-2 due to the high market demand; b) increase in the price of materials and equipment for carrying out the SARS-CoV-2 RT-PCR; c) low availability of equipment; d) number of qualified people available to perform the RT-PCR technique; e) number of centers or laboratories able to carry out the exam; and f) transportation of the material to the locations where the test could be performed 55.
The other non-pharmacological intervention would be the so-called lockdown, which includes interventions such as the closure of commerce and services, restrictions in transport and closure of schools, up to the recommended or forced confinement of the entire population, with the exception of essential workers (for instance, health professionals, food-related activities and the police) 48.
The publication of an Ordinance in March 2020 authorizing the replacement of in-person classes by remote ones during the pandemic situation was undoubtedly an essential measure for expanding social distancing.
Moreover, there were only two decrees at the federal level regarding the definition of essential services. The first was Decree N. 10,282 of March 20, 2020, which regulated Law N. 13,979 and defined public services and essential activities. This decree initially listed 57 essential services, of which 22 were later revoked by other decrees. The other legal instrument dealing with this issue brought changes to the description of essential services. In fact, it reinforces that the federal government did not position itself on a lockdown intervention 52.
Contrary to the president's denialist attitude, some state governors adopted lockdown policies to prevent the spread of the SARS-CoV-2 pandemic, with specific measures to restrict social contact being introduced for the first time in the North and Northeast regions. On May 5, 2020, the State of Maranhão, in the Northeast Region, implemented strict rules enforcing social distancing. After this experience, other state governors and city mayors also adopted stricter social distancing measures. A heated debate accompanied the implementation of stringent lockdown measures on how stringent they could be, how much they would cost and how long they should last 58.
As for pharmacological interventions, the federal government first included Chloroquine and Hydroxychloroquine in the list of special control drugs in category C1, in an attempt to control the sale of these drugs.
In March 2020, the WHO actually approved studies with these drugs for the treatment of patients with COVID-19. Some world leaders were enthusiastic about these drugs and argued that they would be the cure for COVID-19 infection; this caused a frantic search for these drugs in pharmacies. In vitro studies with preliminary results of clinical trials with inadequate methods led to a distorted view of reality, making many doctors, the media and the population believe in this “miracle drug” 48.
Another pharmacological measure worth mentioning was Brazil's adherence to the Covax Facility, aiming to acquire vaccines against COVID-195. This adherence took place as a provisional measure in September 2020. However, it was only in January 2021 that it culminated in the national plan for implementing vaccination against COVID-19, albeit with a delay, when compared to other countries. On December 8, 2020, the United Kingdom became the first country in the West to vaccinate the population against the new coronavirus. The vaccine approved for emergency use was developed by the partnership between the American pharmaceutical company Pfizer and the German biotechnology company BioNTech. Meanwhile, in Brazil, on October 21, 2020, the President of the Republic deauthorized the MoH to purchase a batch of 46 million doses of the vaccine, with the President’s emphasis “any and all vaccines are ruled out” 60,64.
The situation was aggravated in August 2020 by successive denials and lack of responses from the MoH to Pfizer pharmaceutical contacts aimed to establish the supply of vaccines. Only after great popular pressure, in January 2021, the federal government signed the first purchase contract for 46 million doses of CoronaVac 62.
Regarding measures related to the acquisition of supplies, we highlight the legislation that brought new rules such as the waiver of tenders in an attempt to speed up the arrival of supplies used to face the pandemic.
As for hospital beds, SUS controls 44% of the total number of beds in Intensive Care Units (ICUs) in the country, while the private sector holds 56%, which highlights a disproportion, since only 24.6% of Brazilian citizens have a private health insurance plan 63. The pandemic put enormous pressure on health systems, especially regarding the availability of beds, equipment and human resources in the ICUs.
In Brazil, where the number of beds in the private sector, especially in the ICUs, is known to be higher than in the public sector, the prioritized strategy was not using the existing resources, 63 even with the construction of field hospitals through Resolution N. 3 62, aimed at increasing the number of beds. It can be said that the implementation of public beds occurred late and was not enough to guarantee full care and the right to health in different municipalities. There was also the contrast represented by the waiting time in the SUS versus unoccupied and closed beds in the private sector, which made clear the inequalities in health care access 65.
5. Conclusion
Health surveillance measures in Brazil to control the pandemic caused by the new coronavirus SARS-CoV-2 in the assessed documents were timidly scarce, contrasting with the extensive set of articles criticizing the delay in decision-making, the discrepancy between the WHO recommendations and those dictated by the President of the Republic, in addition to the constant changes of Health Ministers and the instability and lack of confidence that ministerial authorities conveyed to the population.
In order to control the pandemic and preserve the economy, the country would need a leadership that would centralize and coordinate actions with states and municipalities. Unfortunately, the federal government did not fulfill this role, becoming one more obstacle in controlling the pandemic. This negative leadership and lack of coordination caused many deaths and seriously impaired the lives of survivors by delaying the resumption of economic and social activities. As limitations, we had to face the fact that there were very few studies on health surveillance on COVID-19 in Brazil, and that's why we had to resort to access the federal government's legislation portal.
The main effort of the federal government in the fight against the virus was centered on the use of antimalarial and anti-parasitic drugs and disregard for non-pharmacological interventions. While there was a surplus of medications without scientific proof of being effective, there was a lack of beds and coordination.
Many Brazilian citizens could not breathe due to the lack of compassion by government authorities, questioning the principles of universality of the SUS: the guarantee to life and social rights.
Considering that health surveillance exists, in addition to its relevance in the policies of a country and in reducing vulnerability and health risks, this study brings data from a period related to the catastrophic historical line in the context of the COVID-19 pandemic in Brazil. These data reveal contradictory, distorted measures, which were in opposition to science, taken by the Brazilian government in the 2019-2022 administration, which culminated in a tragedy foretold of almost 700,000 deaths in the country. And that it is necessary to prioritize science, education and support for scientific advancement.
References
- Garfin D, Silver R, Holman E. O novo surto de coronavírus: amplificação das consequências para a saúde pública pela exposição à mídia. Health Psychol [publicação online] 2020 [acesso em 5 jan 2021].
- WHO. Relatório da situação 11 [Internet]. WHO. 2020 [cited 2021 Jan 29].
- Perlman S. Outra década, outro coronavírus. N Engl J Med 2020; 382:760-762.
- Paterlini M.A linha de frente do Coronavirus: a resposta italiana à COVID-19. The BMJ. 2020;368.
- Block P, Hoffman M, Raabe I, Beam Dowd J, Rahal C, Kashyap R, et al. Social network-based distancing strategies to flatten the COVID-19 curve in a post-lockdown world. Nat Human Behaviour. 2020;4; 4:588–96. [CrossRef]
- Arshed N, Meo MS, Farooq F. Empirical assessment of government policies and flattening of the COVID 19 curve. J Public Aff. 2020; e2333. [CrossRef]
- Jesus JG, de Sacchi C, Candido D da S, Claro IM, Sales FCS, Manuli ER, et al. Importation and early local transmission of COVID-19 in Brazil. Rev Ins Med Trop São Paulo. 2020;62. [CrossRef]
- Croda J, Oliveira WK de, Frutuoso RL, Mandetta LH, Baia-da-Silva DC, Brito-Sousa JD, et al. COVID-19 in Brazil: advantages of a socialized unified health system and preparation to contain cases. Rev Soc Bras Med Trop [publicação online]. 2020 [acesso em 25 set 2020];53. [CrossRef]
- Freitas CM de, Silva IV de M e, Cidade N da C, Freitas CM de, Silva IV de M e, Cidade N da C. COVID-19 AS A GLOBAL DISASTER: Challenges to risk governance and social vulnerability in Brazil. Ambiente & Sociedade [publicação online]. 2020 [acesso em 25 jul 2021];23.
- Aquino EML. Medidas de distanciamento social no controle da pandemia de COVID-19: Potenciais impactos e desafios no Brasil [publicação online]. 2020 [acesso em Mar 3 2022].
- Ministério da Saúde. Portaria n° 188, de 3 de Fevereiro De 2020. Declara Emergência em Saúde Pública de importância Nacional (ESPIN) em decorrência da Infecção Humana pelo novo Coronavírus (2019-nCoV). Diário Oficial da União.
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Systematic Reviews [publicação online]. 2016 [acesso em 5 set 2021];5(1). [CrossRef]
- PRISMA. PRISMA [Internet]. Prisma-statement.org. 2020.
- Ministério da Saúde. Lei nº 13.989, de 15 de abril de 2020.Dispõe sobre o uso da telemedicina durante a crise causada pelo coronavírus (SARS-CoV-2). Diário Oficial da União.
- Ministério da Saúde. Portaria nº156, de 1 de abril de 2020. Suspende, temporária e excepcionalmente, o tempo máximo para o contato direto com o atendente no Serviço de Atendimento ao Consumidor - SAC, previsto na Portaria nº 2.014, de 13 de outubro de 2008, do Ministério da Justiça. Diário Oficial da União.
- Ministério da Saúde. Plano de Contingência Nacional para Infecção Humana pelo novo Coronavírus COVID-19 2020. Diário Oficial da União.
- Ministério da Saúde. Portaria nº 59, de16 de março de 2020. Fica instituído o Gabinete Integrado de Acompanhamento à Epidemia do Coronavírus-19 (GIAC-COVID19). Diário Oficial da União.
- Ministério da Saúde.Decreto n° 10.277, de 16 de março de 2020. Institui o Comitê de Crise para Supervisão e Monitoramento dos Impactos da COVID-19. Diário Oficial da União.
- Ministério da Educação. Portaria nº 343, de 17 de março de 2020. Dispõe sobre a substituição das aulas presenciaispor aulas em meios digitais enquanto durar a pandemia do novo coronavírus. Diário Oficial da União.
- Ministério da Saúde.Portaria nº428, de 19 de março de 2020. Dispõe sobre as medidas de proteção para enfrentamento da emergência de saúde pública de importância internacional decorrente do coronavírus (COVID-19) no âmbito das unidades do Ministério da Saúde no Distrito Federal e nos Estados. Diário Oficial da União.
- Ministério da Saúde.Portaria nº 492,de 23 de Março de 2020. Institui a Ação Estratégica "O Brasil Conta Comigo", voltada aos alunos dos cursos da área de saúde, para o enfrentamento à pandemia do coronavírus (COVID-19). Diário Oficial da União.
- Ministério da Saúde. Decreto nº 10.316, de 7 de abril de 2020. Regulamenta a Lei nº 13.982, de 2 de abril de 2020, que estabelece medidas excepcionais de proteção social a serem adotadas durante o período de enfrentamento da emergência de saúde pública de importância internacional decorrente do coronavírus. Diário Oficial da União.
- Presidência da República SG. Lei nº 14.046, de 24 de agosto de 2020.Planalto.gov.br. 2022. Dispõe sobre medidas emergenciais para atenuar os efeitos da crise decorrente da pandemia da COVID-19 nos setores de turismo e de cultura. Diário Oficial da União.
- Ministério da Saúde. Lei nº 14.019, de 2 de julho de 2020. Altera a Lei nº 13.979, de 6 de fevereiro de 2020, para dispor sobre a obrigatoriedade do uso de máscaras de proteção individual para circulação em espaços públicos e privados acessíveis ao público, em vias públicas e em transportes públicos, sobre a adoção de medidas de assepsia de locais de acesso público, inclusive transportes públicos, e sobre a disponibilização de produtos saneantes aos usuários durante a vigência das medidas para enfrentamento da emergência de saúde pública de importância internacional decorrente da pandemia da COVID-19. Diário Oficial da União.
- Ministério da Saúde.Lei nº 14.021, de 7 de julho de 2020. Dispõe sobre medidas de proteção social para prevenção do contágio e da disseminação da COVID-19 nos territórios indígenas; cria o Plano Emergencial para Enfrentamento à COVID-19 nos territórios indígenas; estipula medidas de apoio às comunidades quilombolas, aos pescadores artesanais e aos demais povos e comunidades tradicionais para o enfrentamento à COVID-19; e altera a Lei nº 8.080, de 19 de setembro de 1990, a fim de assegurar aporte de recursos adicionais nas situações emergenciais e de calamidade pública. Diário Oficial da União.
- Ministério da Saúde.Resolução nº 11, de 25 de novembro de 2020. Institui Grupo de Trabalho para a coordenação das medidas de proteção e a prestação de contas de benefícios, em resposta aos impactos relacionados ao coronavírus, no âmbito do Comitê de Crise da COVID-19. Diário Oficial da União.
- Ministério da Saúde.Portaria nº125, de 19 de março de 2020. Dispõe sobre a restrição excepcional e temporária de entrada no País de estrangeiros oriundos dos países que relaciona, conforme recomendação da Agência Nacional de Vigilância Sanitária - Anvisa. Diário Oficial da União.
- Ministério da Saúde. Portaria nº 125, de 19 de março de 2020. Dispõe sobre a restrição excepcional e temporária de entrada no País de estrangeiros oriundos dos países que relaciona, conforme recomendação da Agência Nacional de Vigilância Sanitária - Anvisa. Diário Oficial da União.
- Ministério da Saúde.Portaria n°126, de 19 de março de 2020. Dispõe sobre a restrição excepcional e temporária de entrada no País de estrangeiros oriundos dos países que relaciona, conforme recomendação da Agência Nacional de Vigilância Sanitária – Anvisa. Diário Oficial da União.
- Ministério da Saúde.Portaria nº 47, de 26 de março de 2020. Dispõe sobre a restrição excepcional e temporária de entrada no País de estrangeiros por transporte aquaviário, conforme recomendação da Agência Nacional de Vigilância Sanitária – Anvisa. Diário Oficial da União.
- Ministério da Saúde. Portaria nº158, de 31 de março de 2020. Dispõe sobre a restrição temporária e excepcional de entrada no País de estrangerios provenientes da República Bolivariana da Venezuela.Diário Oficial da União.
- Ministério da Saúde. Resolução - Rdc nº 351, de 20 de março de 2020. Dispõe sobre a atualização do Anexo I (Listas de Substâncias Entorpecentes, Psicotrópicas, Precursoras e Outras sob Controle Especial) da Portaria SVS/MS nº 344, de 12 de maio de 1998, e dá outras providências. Diário Oficial da União.
- Ministério da Saúde. Portaria nº 356, de 11 de março de 2020. Dispõe sobre a regulamentação e operacionalização do disposto na Lei nº 13.979, de 6 de fevereiro de 2020, que estabelece as medidas para enfrentamento da emergência de saúde pública de importância internacional decorrente do coronavírus (COVID-19). Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República. Autoriza o Poder Executivo federal a aderir ao Instrumento de Acesso Global de Vacinas COVID-19 - Covax Facility. Diário Oficial da União.
- Ministério da Saúde.Medida Provisória nº 1.026, de 6 de janeiro de 2021. Dispõe sobre as medidas excepcionais relativas à aquisição de vacinas, insumos, bens e serviços de logística, tecnologia da informação e comunicação, comunicação social e publicitária e treinamentos destinados à vacinação contra a COVID-19 e sobre o Plano Nacional de Operacionalização da Vacinação contra a COVID-19. Diário Oficial da União.
- Ministério da Saúde.Portaria nº414, de 18 de março de 2020. Autoriza a habilitação de leitos de Unidade de Terapia Intensiva Adulto e Pediátrico, para atendimento exclusivo dos pacientes COVID-19. Diário Oficial da União.
- Ministério da Saúde.Portaria n° 430, de 30 de dezembro de 2020. Ficam divulgados os dias de feriados nacionais e estabelecidos os dias de ponto facultativo no ano de 2021, para cumprimento pelos órgãos e entidades da Administração Pública federal direta, autárquica e fundacional do Poder Executivo, sem prejuízo da prestação dos serviços considerados essenciais. Diário Oficial da União.
- Ministério da Saúde.Portaria nº 9.471 de 07 de abril de 2020. Estabelece medida extraordinária e temporária quanto à comercialização de Equipamentos de Proteção Individual - EPI de proteção respiratória para o enfrentamento da emergência de saúde pública decorrente do Coronavírus (COVID-19). Diário Oficial da União.
- Ministério da Saúde. Resolução nº 3, de 15 de abril de 2020. Institui Grupo de Trabalho para a Coordenação de Ações Estratégicas para Construção de Hospitais de Campanha Federais e Logística Internacional de Equipamentos Médicos e Insumos de Saúde, em resposta aos impactos relacionados ao coronavírus, no âmbito do Comitê de Crise da COVID-19. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República. Decreto No 10.407 De 29 De Junho De 2020. Regulamenta a Lei nº 13.993, de 23 de abril de 2020, que dispõe sobre a proibição de exportações de produtos médicos, hospitalares e de higiene essenciais ao combate à epidemia da COVID-19 no País. Diário Oficial da União.
- Ministério da Saúde. Portaria Gm/Ms nº 197, de 1 de fevereiro de 2021. Delega competência ao Diretor do Departamento de Logística em Saúde do Ministério da Saúde, para realizar requisição de medicamentos, equipamentos, imunobiológicos e outros insumos de interesse para saúde, durante a vigência da declaração de emergência em saúde pública de importância internacional decorrente do coronavírus (COVID-19). Diário Oficial da União.
- Ministério da Infraestrutura. Portaria nº 199, de 10 de fevereiro de 2021. Dispõe sobre os prazos de processos e de procedimentos afetos aos órgãos e entidades do Sistema Nacional de Trânsito e às entidades públicas e privadas prestadoras de serviços relacionados ao trânsito, por força das medidas de enfrentamento da pandemia de COVID-19 no Estado do Amazonas. Diário Oficial da União.
- Ministério da Saúde.Lei nº 14.035, De 11 De Agosto De 2020. Altera a Lei nº 13.979, de 6 de fevereiro de 2020, para dispor sobre procedimentos para a aquisição ou contratação de bens, serviços e insumos destinados ao enfrentamento da emergência de saúde pública de importância internacional decorrente do coronavírus responsável pelo surto de 2019. Diário Oficial da União.
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses-PRISMA. [Homepage da internet]. Prisma-statement.org. [acesso em 30 set 2021].
- Brasil.Secretaria Geral da Presidência da República. Lei nº 13.979, de 6 de fevereiro de 2020. Dispõe sobre as medidas para enfrentamento da emergência de saúde pública de importância internacional decorrente do coronavírus responsável pelo surto de 2019. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República.Portaria Interministerial nº 5, de 17 de março de 2020.Dispõe sobre a compulsoriedade das medidas de enfrentamento da emergência de saúde pública previstas na Lei nº 13.979, de 06 de fevereiro de 2020. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República. Portaira nº 1272GM-MD, de 20 de março de 2020. Aprovação da Diretriz Ministerial de Execução nº 7/2020, que autoriza a execução das ações de apoio para mitigar os impactos do COVID-19. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República. Medida provisória no 966, de 13 de maio de 2020. Dispõe sobre a responsabilização de agentes públicos por ação e omissão em atos relacionados com a pandemia da COVID-19. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República.Resolução no 6, de 2 de junho de 2020. Institui Grupo de Trabalho para a Consolidação das Estratégias de Governança e Gestão de Riscos do Governo federal em resposta aos impactos relacionados ao coronavírus, no âmbito do Comitê de Crise da COVID-19. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República. Lei no 14.019, de 2 de julho de 2020. Altera a Lei nº 13.979, de 6 de fevereiro de 2020, para dispor sobre a obrigatoriedade do uso de máscaras de proteção individual para circulação em espaços públicos e privados acessíveis ao público, em vias públicas e em transportes públicos, sobre a adoção de medidas de assepsia de locais de acesso público, inclusive transportes públicos, e sobre a disponibilização de produtos saneantes aos usuários durante a vigência das medidas para enfrentamento da emergência de saúde pública de importância internacional decorrente da pandemia da COVID-19. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República. DECRETO Nº 10.282, DE 20 DE MARÇO DE 2020. Regulamenta a Lei nº 13.979, de 6 de fevereiro de 2020, para definir os serviços públicos e as atividades essenciais. Diário Oficial da União.
- Brasil.Secretaria Geral da Presidência da República.Plano de Contingência Nacional para Infecção Humana pelo novo Coronavírus COVID-19. Diário Oficial da União.
- Tang W, Cao Z, Han M, Wang Z, Chen J, Sun W, et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomized controlled trial. BMJ. 2020 May 14; m1849. [CrossRef]
- Garcia LP, Duarte E. Intervenções não farmacológicas para o enfrentamento à epidemia da COVID-19 no Brasil. Epidemiol Serv Saude.2020 Apr 9;29:e2020222.
- Ministério da Saúde. Política Nacional de Vigilância em Saúde. Diário Oficial da União.
- Nadanovsky P, Santos App dos. Strategies to deal with the COVID-19 pandemic. Braz Oral Res. 2020;34.
- World Health Organization - Who. Advice on the use of masks in the community, during home care and in healthcare settings in the context of the novel coronavirus (COVID-19) outbreak. Diário Oficial da União.
- Ortega F, Orsini M. Governing COVID-19 without government in Brazil: Ignorance, neoliberal authoritarianism, and the collapse of public health leadership. Glob Public Health. 2020 Jul 14;1–21. [CrossRef]
- Marson FAL. COVID-19 – Six million cases worldwide and an overview of the diagnosis in Brazil: A tragedy to be announced. Diagnostic Microbiol and Infect Dis. 2020 Jun;115113.
- Romero M, Passos L. COVID-19 in Brazil: “So what?”. The Lancet [ revista em internet] 2020. [acesso em Janeiro 2021]; 32(2).
- Cornwall W. Can you put a price on COVID-19 options? Experts weigh lives versus economics [revista em internet] 2020.
- Agência Lupa [homepage na internet]. Após mudança de discurso do presidente, redes bolsonaristas elogiam vacinação [acesso em Mar 4 2022].
- Aguiar P. Toda e qualquer vacina está descartada.R7.com.[revista em internet] 2020.
- Lima LD, Pereira AM, Machado CV. Crise, condicionantes e desafios de coordenação do Estado federativo brasileiro no contexto da COVID-19. [publicação online];2020[acesso em 14 jan 2021].
- Homero V. Butantan entregará 46 milhões de doses da CoronaVac até abril, diz Pazuello [publicação online]; 2021 [acesso em 4 mar 2022].
- Costa D CAR, Bahia L, Carvalho EMCL de, Cardoso AM, Souza PMS. Oferta pública e privada de leitos e acesso aos cuidados à saúde na pandemia de COVID-19 no Brasil.Saúde em Debate [publicação online]; 2020 [acesso em 5 jan 2021].
Figure 1.
Flowchart for systematic review, including databases, records and other sources. Source: the authors. Made using PRISMA13.
Figure 1.
Flowchart for systematic review, including databases, records and other sources. Source: the authors. Made using PRISMA13.
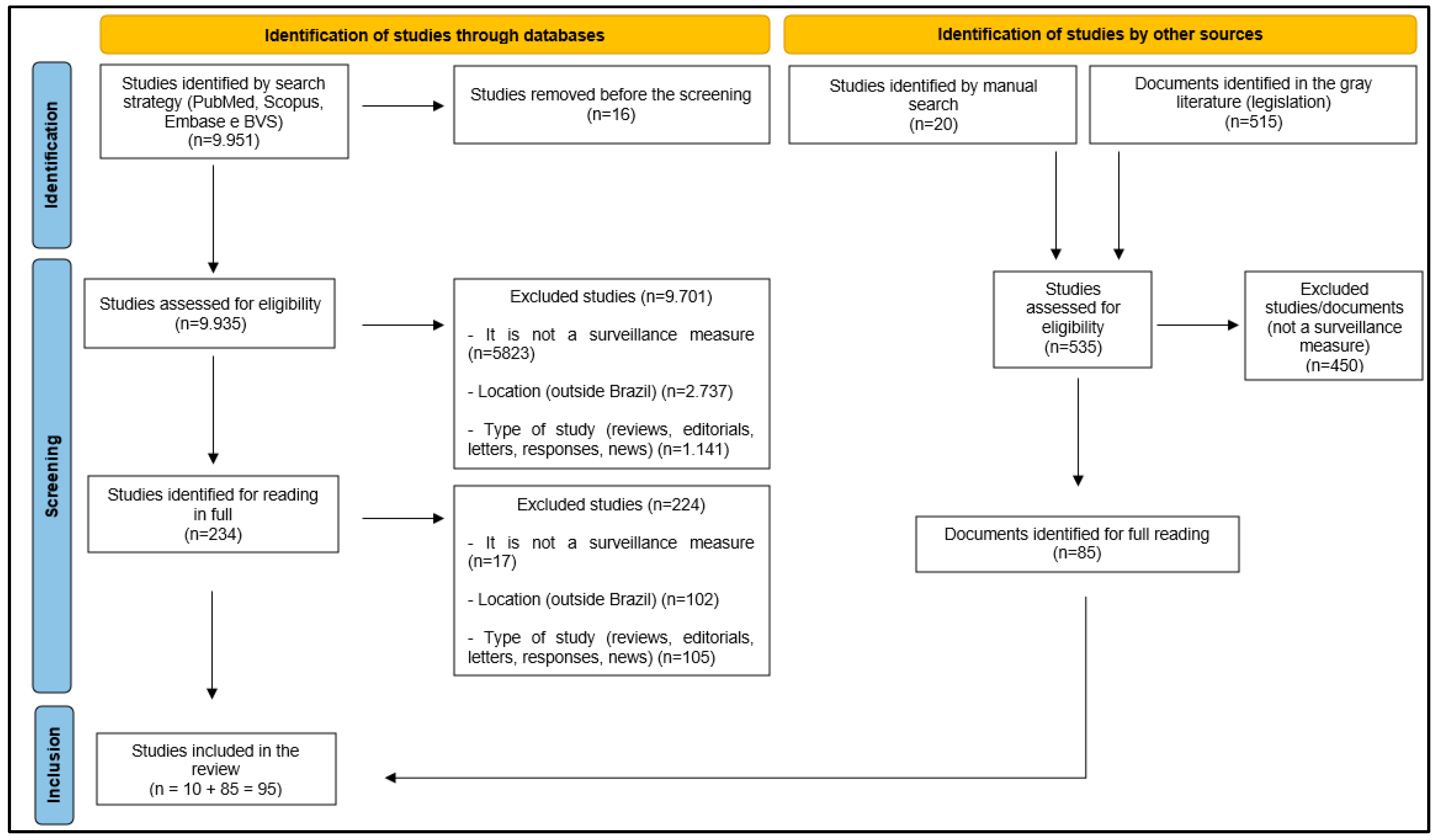
Figure 2.
Legislation on health surveillance measures for COVID-19, according to categories, February 2020 to January 2021, Brazil.
Figure 2.
Legislation on health surveillance measures for COVID-19, according to categories, February 2020 to January 2021, Brazil.
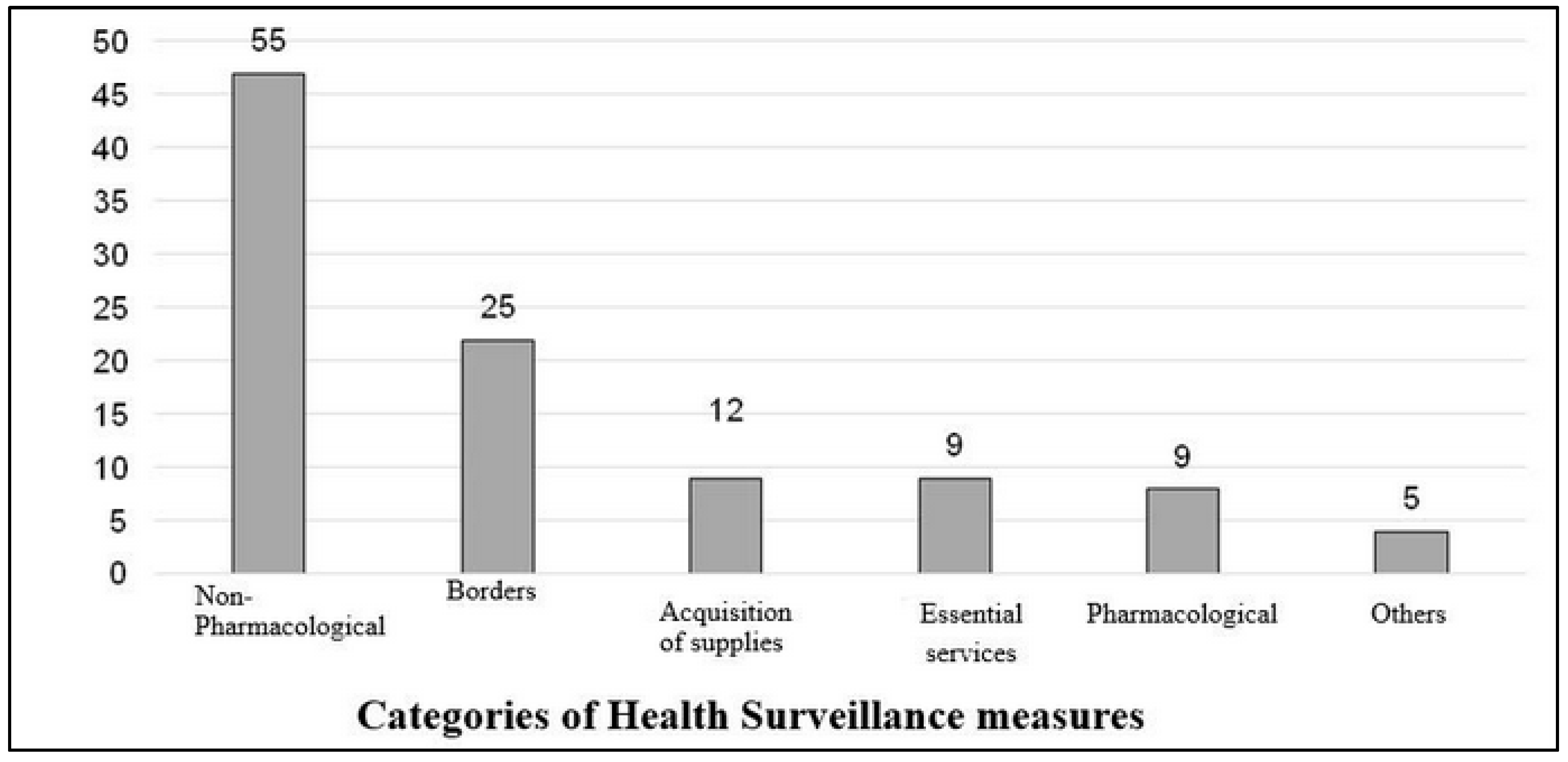
Figure 3.
Chronology of non-pharmacological measures, pharmacological measures, border-related measures, measures related to the acquisition of inputs adopted by the Brazilian Ministry of Health, 2020.
Figure 3.
Chronology of non-pharmacological measures, pharmacological measures, border-related measures, measures related to the acquisition of inputs adopted by the Brazilian Ministry of Health, 2020.
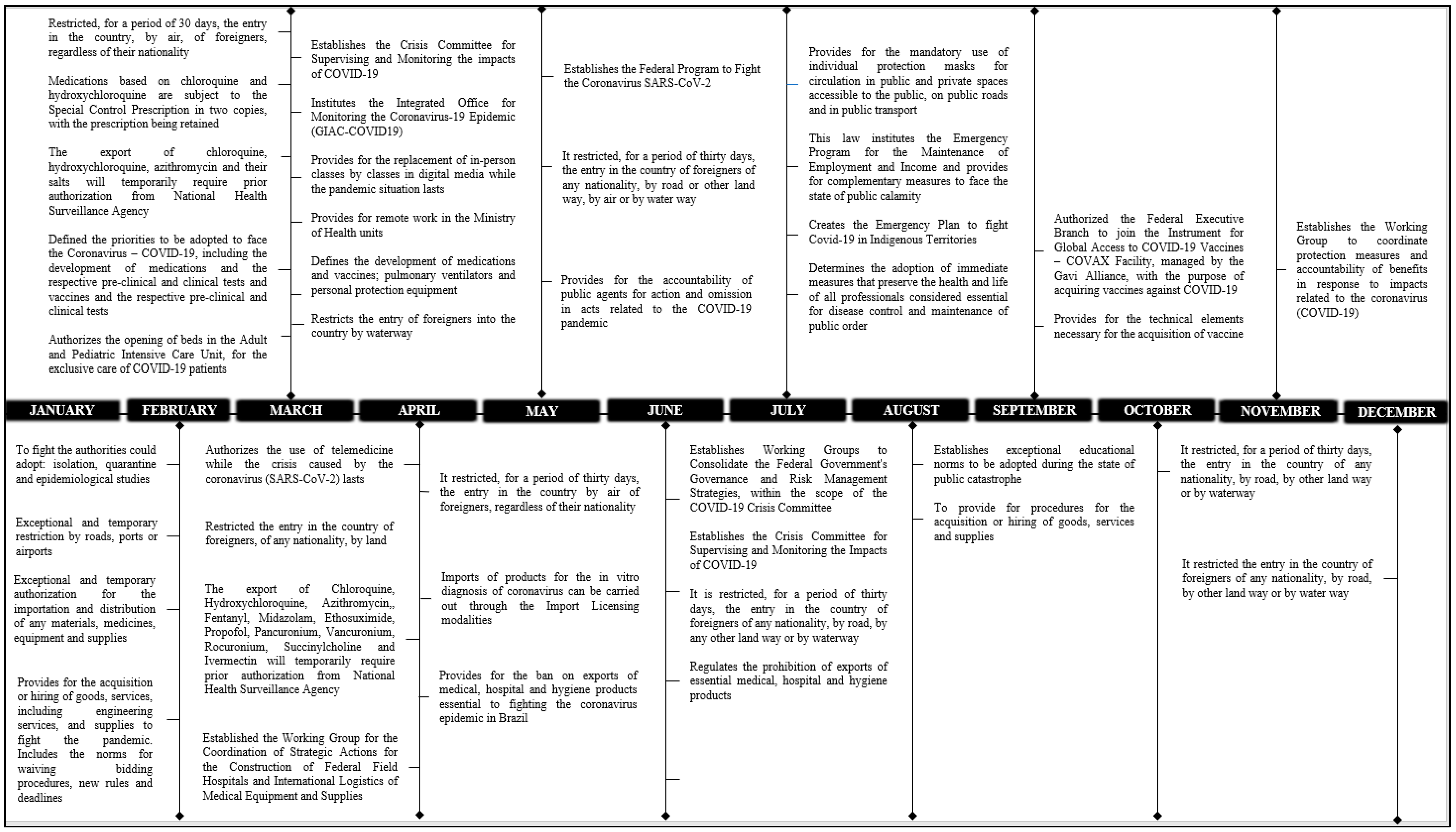

Table 1.
Search strategy for articles and documents in indexed databases.
| Database | Search syntaxes |
|---|---|
| PUBMED | ("public health surveillance"[MeSH Terms] OR "public health surveillance"[Title/Abstract] OR "epidemiological monitoring"[Title/Abstract] OR "Epidemiology"[MeSH Terms] OR "Epidemiology"[Title/Abstract] OR "health services research"[MeSH Terms] OR "communicable disease control"[MeSH Terms] OR (("prevent"[All Fields] OR "preventability"[All Fields] OR "preventable"[All Fields] OR "preventative"[All Fields] OR "preventatively"[All Fields] OR "preventatives"[All Fields] OR "prevented"[All Fields] OR "preventing"[All Fields] OR "prevention and control"[MeSH Subheading] OR ("prevention"[All Fields] AND "control"[All Fields]) OR "prevention and control"[All Fields] OR "prevention"[All Fields] OR "prevention s"[All Fields] OR "preventions"[All Fields] OR "preventive"[All Fields] OR "preventively"[All Fields] OR "preventives"[All Fields] OR "prevents"[All Fields]) AND "control groups"[MeSH Terms]) OR "prophylaxis"[Title/Abstract] OR "preventive measures"[Title/Abstract] OR “prevention"[Title/Abstract] OR "control"[Title/Abstract] OR "health policy"[MeSH Terms] OR "health policy"[Title/Abstract] OR (("Policy"[MeSH Terms] OR "Policy"[All Fields] OR "policies"[All Fields] OR "policy s"[All Fields]) AND "national health"[Title/Abstract])) AND ("coronavirus infections"[MeSH Terms] OR "betacoronavirus"[MeSH Terms] OR "epidemics"[MeSH Terms] OR "epidemic*"[Title/Abstract]) AND ("brazil"[MeSH Terms] OR "brazil"[All Fields] OR "brazil s"[All Fields] OR "brazils"[All Fields] OR (("ministries"[All Fields] OR "ministry"[All Fields] OR "ministry s"[All Fields]) AND ("Health"[MeSH Terms] OR "Health"[All Fields] OR "health s"[All Fields] OR "healthful"[All Fields] OR "healthfulness"[All Fields] OR "healths"[All Fields])) OR (("Health"[MeSH Terms] OR "Health"[All Fields] OR "health s"[All Fields] OR "healthful"[All Fields] OR "healthfulness"[All Fields] OR "healths"[All Fields]) AND ("Epidemiology"[MeSH Subheading] OR "Epidemiology"[All Fields] OR "Surveillance"[All Fields] OR "Epidemiology"[MeSH Terms] OR "surveilance"[All Fields] OR "surveillances"[All Fields] OR "surveilled"[All Fields] OR "surveillence"[All Fields]) AND ("secretariat"[All Fields] OR "secretariat s"[All Fields] OR "secretariats"[All Fields]))) |
| Scopus | Brazil OR ministry AND of AND health OR health AND surveillance AND secretariat AND public AND health AND surveillance OR public AND health AND surveillance OR epidemiological AND monitoring OR epidemiology OR health AND services AND research OR communicable AND disease AND control OR prevention AND control OR control AND groups OR prophylaxis OR preventive AND measures OR prevention OR control OR health AND policy OR policy OR national AND health AND betacoronavirus OR coronavirus AND infections OR COVID-19 OR covid19 OR coronavirus AND disease 2019 OR sars AND cov 2 infection OR covid 19 pandemic OR sars-cov-2 OR coronavirus 2 sars OR severe AND acute AND respiratory OR syndrome AND coronavirus 2 |
| Virtual Health Library (VHL) | (Brasil ) OR (Ministério da Saúde ) OR (Secretaria de Vigilância de Saúde)) AND ((mh:(Vigilância em saúde pública )) OR (Vigilância em saúde pública) OR (mh:(Monitoramento Epidemiológico)) OR (Vigilância Epidemiológica) OR (Monitoramento Epidemiológico) OR (Vigilâncias Epidemiológicas) OR (mh:(Pesquisa de Serviços de Saúde)) OR (Pesquisa de Serviços de Saúde) OR (mh:(Prevenção e controle)) OR (Prevenção e controle) OR (mh:(Controle de Doenças Transmissíveis)) OR (Controle de Doenças Transmissíveis) OR (profilaxia) OR (terapia preventiva ) OR (medidas preventivas ) OR (prevenção *) OR (controle) OR (mh:(Polícia da saúde)) OR (Polícia da saúde) OR (Política de Saúde ) OR (Políticas Nacionais de Saúde)) AND ((mh:(Betacoronavirus)) OR (Betacoronavirus) OR (mh:(COVID-19)) OR (COVID-19) OR (COVID 19) OR (Doença pelo Novo Coronavírus (2019-nCoV)) OR (Infecção por Coronavirus 2019-nCoV) OR (Surto por Coronavírus 2019-nCoV) OR (SARS-CoV-2 ) OR (SARS-CoV-2 ) OR (Síndrome Respiratória Grave Aguda)) |
Table 2.
Legal provisions and scientific articles organized by category in relation to the surveillance measures adopted by the Brazilian Ministry of Health to combat COVID-19 between February 2020 and January 2021.
Table 2.
Legal provisions and scientific articles organized by category in relation to the surveillance measures adopted by the Brazilian Ministry of Health to combat COVID-19 between February 2020 and January 2021.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



