
Submitted:
09 October 2023
Posted:
10 October 2023
You are already at the latest version
Abstract
Background: Number of joint infections caused by Vancomycin-resistant pathogens is emerging. Currently no PMMA cement is commercially available to cover VRE. Daptomycin shows promising results in infection treatment, offers a good safety profile and reduced risk for resistance development. Purpose of this in vitro study is to investigate the mechanical stability, handling properties, elution behavior and antimicrobial effectiveness of PMMA cement loaded with three different Daptomycin concentrations in comparison to commercially available ALBC; Methods: Mechanical properties and handling characteristics (ISO 5833, DIN 53435), HPLC elution, antimicrobial effectiveness with proliferation assay (DIN 17025) and inhibition zone testing were investigated; Results: All tested Daptomycin concentrations fulfilled ISO and DIN mechanical strength. Dosage of 0.5. g added Daptomycin did not show any antimicrobial effectiveness in contrast to 1.0 g and1.5 g. Cement with 1.5 g Daptomycin was best in elution and effectiveness, showed good mechanical ISO strength, ISO doughing was a little longer sticky and setting was faster as Vancomycin containing reference cement; Conclusion: PMMA cement containing 0.5 g Gentamicin and 1.5 g Daptomycin could be a good alternative to the already established COPAL® G+V for PJI treatment of VRE.
Keywords:
Daptomycin
; PMMA cement
; mechanical properties
; elution
; antimicrobial effectiveness
; inhibition zone test
; Vancomycin-resistant germs
; PMMA spacer
1. Introduction
Periprosthetic Joint Infections (PJI) are a challenging complication in joint replacement surgery that often results in worse outcome for the patients, especially when the causing pathogen is a multi-resistant germ [1] and/or the patient is at high risk [2,3]. PMMA bone cements loaded with a single (SALBC) or two antibiotics (DALBC) are used for PJI prevention or treatment, e.g. for a spacer in the interim period of a two-stage exchange procedure [4,5,6,7]. Especially DALBC support PJI reduction compared to SALBC [8]. Commercially available antibiotic loaded bone cements (ALBCs) mainly contain the antibiotics Gentamicin or Tobramycin (amynoglycosides), Vancomycin (glycopetide), Clindamycin (lincosamide) [9]. The number of PJIs caused by resistant germs, among them Vancomycin-resistant Staphylococcus aureus (VRSA), Vancomycin-resistant Enterococci (VRE), Methicillin-resistant Staphylococcus aureus (MRSA) and Methicillin-resistant Staphylococcus epidermidis (MRSE) is rising [10,11] and the manually addition of vancomycin or commercially available ALBCs lack to cover these germs. The named bacterial species developed resistance mainly against Vancomycin and Methicillin therefore antibiotics used for treatment must be adapted to the resistance pattern [12]. An antibiotic found to be effective against Vancomycin-intermediate resistant S. aureus (VISA), VRSA and VRE is Daptomycin; it also shows antimicrobial activity against anaerobic bacteria but none against gram-negative bacteria [10,13]. Daptomycin has a unique mode of action and disrupts the cell membrane integrity of bacteria [14].
There is no Daptomycin ALBC commercially available and the manually admixing of Daptomycin is highly expensive (Cubicin, ~ 780 € / 2 g). In clinical practice, surgeons increase the Vancomycin concentration up to 4 g/40g polymer powder to treat Vancomycin-resistant germs (VRE). But a massively increased antibiotic concentration in PMMA spacers negatively influences their mechanical stability [15] and the risk of local as well as systemic kidney toxicity is highly increased. According to “Pocket Guide to Diagnosis & Treatment of PJI” from PRO-IMPLANT Foundation (PIF) 2 g of Daptomycin can be added to a fixation cement and 3 g of Daptomycin to a spacer cement [16]. The addition of more than 2 g Daptomycin results in non-compliant ISO mechanical properties.
With this investigation we wanted to figure out which concentration of Daptomycin can be added to PMMA cement to efficiently inhibit bacterial growth and at the same time deliver mechanical stability according to ISO standards.
2. Results
2.1. Antimicrobial Effectiveness determined by Proliferation Assay
For Methicillin-resistant S. epidermidis (MRSE) blank sample and PMMA cement loaded with 0.5 g Gentamicin and Daptomycin (GD0.5) did not show any antimicrobial activity (Figure 1a). GD1.0 and GD1.5 can inhibit bacterial growth and GD1.5 shows better antimicrobial properties compared to GD1.0. For Vancomycin-resistant S. aureus (VRSA) blank sample and GD0.5 did not show antimicrobial activity (Figure 1b) whereas GD1.0 and GD1.5 are able to inhibit bacterial growth. The same observation was done for Vancomycin-resistant E. faecium (VRE) when only GD1.0 and GD1.5 show antimicrobial activity (Figure 1c). For S. aures (MRSA) blank sample and GD0.5 did not inhibit bacterial growth in contrast to GD1.0 and GD1.5. Overall, the antimicrobial efficacy of GD1.5 and GD1.0 did not differ widely with GD1.5 showing highest effect on bacterial growth.
2.2. Antimicrobial Effectiveness based on Inhibition Zone Test
Inhibition zones of Daptomycin-containing PMMA cements showed the best effectiveness with a concentration of 1.5 g Daptomycin concentration. In Figure 2 the tested samples were related to the added amount of Daptomycin: 1.5 g led to an average inhibition zone of 2,269 mm2, 1.0 g of 2,219 mm2 and 0.5 g of 2,134 mm2. GD1.5, GD1.0 and GD0.5 showed antimicrobial effectiveness against B. subtilis (Figure 2).
2.3. Influence of Sterilization Method
Non-sterilized as well as gamma irradiated pure Daptomycin powder showed comparable effectivity against B. subtilis (Figure 3). The effectivity of Daptomycin sterilized by ethylene oxide was significantly reduced in comparison to the unsterile and gamma-irradiated powder.
2.4. Antibiotic Release Profile of Gentamicin, Daptomycin and Vancomycin
The highest volume of Gentamicin release from GD-PMMA cement samples was observed on day 1 followed by a continuous decrease in antibiotic release (Figure 4a). The Gentamicin release was higher for those samples with a higher Daptomycin concentration: GD1.5 showed over five days the highest Gentamicin release compared to GD1.0 and GD0.5, indicating a synergistic elution effect. PALACOS® R+G and COPAL® G+V showed the highest antibiotic release on day 1 compared to the test samples with manual admixed Daptomycin. The total release of Daptomycin was higher (1039.7 µg) compared to Gentamicin (734.1 µg) for sample GD1.5 (Figure 4b, c). Adding 0.5 g of Daptomycin resulted in a two-fold higher antibiotic release rate: GD1.5 with 1039.7 µg, GD1.0 with 611.4 µg and GD0.5 with 263.8 µg. Ref2 was assessed for Vancomycin elution (Figure 4d) showing highest initial release of all tested samples on day 1 (1460.2 µg) with a massive decrease to 221.4 µg on day 2. Compared to GD samples and Ref1, Ref2 showed the highest total amount of antibiotics eluted. Compared to Vancomycin release (Figure 4d) from Ref2 the total amount of Daptomycin was lower, indicating an overall better elution from Ref2 compared to GD samples.
2.5. Mechanical Stability of Daptomycin-loaded Bone Cement
All tested Daptomycin-containing PMMA cement samples fulfilled the ISO and DIN requirements (Figure 5a). Ref1 showed a bending strength of 71 MPa surpassing the threshold of 50 MPa. Ref2 was close to the threshold with a bending strength of 58.0 MPa. ISO Bending strength was highest for GD1.0 (72 MPa), followed by GD0.5 (70 MPa) and GD1.5 (67 MPa), which comes therefor with a higher bending strength than Ref2. Bending modulus of Ref1 (2922 MPa) was comparable to Ref2 (2900 MPa) fulfilling the minimum threshold of 1800 MPa (Figure 5b). GD1.0 had the highest value for bending modulus with 3342 MPa, followed by GD1.5 (3148 MPa) and GD0.5 (3120 MPa); all GD samples surpassed the references. Ref2 fulfilled the minimum requirement (70 MPa) for ISO compressive strength with 78 MPa whereas Ref1 exceeded it (87 MPa) (Figure 5c). Compressive strength was highest for GD1.5 (93 MPa) followed by GD0.5 (92 MPa) and GD1.0 (90 MPa).
All GD cement samples fulfilled the requirements for mechanical stability according to DIN 53435. Ref2 exceeded the minimum threshold (50 N/mm2) of DIN bending strength with 69 N/mm2 as well as Ref1 with 81 N/mm2 (Figure 6a). DIN bending strength decreased with an increase of the Daptomycin concentration from 74 N/mm2 (GD0.5) to 70 N/mm2 (GD1.0) to 64 N/mm2 (GD1.5). GD1.0 showed a comparable DIN bending strength to Ref2, whereas GD1.5 was slightly below Ref2. DIN impact resistance was measured for Ref2: 3.0 kJ/m2 which was set as reference. DIN impact resistance is shown as difference to Ref2 (Figure 6b). Ref1 (3.5 kJ/m2), GD1.0 (3.2 kJ/m2) and GD0.5 (3.1 kJ/m2) exceeded the impact resistance of Ref2 whereas GD1.5 (2.6 kJ/m2) showed the highest difference in DIN impact resistance. The higher the Daptomycin concentration the lower the measurements for DIN bending strength and impact resistance, indicating that a high Daptomycin concentration in PMMA bone cement reduces its mechanical properties. ISO bending strength for GD1.5 was lower compared to all other concentrations and the references.
2.6. Handling Properties of Daptomycin-loaded Bone Cement
GD1.5 was slightly faster in setting compared to Ref2 and even more compared to Ref1 (Table 1) resulting in a faster setting behavior. ISO doughing time was lowest for Ref2 and highest for GD1.5 indicating a slower doughing process for GD1.5. The density of all tested cement samples was similar.
3. Discussion
As PJI especially when caused by resistant germs still poses a threat for patients and the health care system, any kind of support to prevent a PJI or treat it in a two-stage revision protocol are needed [17]. Daptomycin containing PMMA cement is recommended in PJI when combatting vancomycin resistance germs e.g., VRE.
In clinical practice, spacers for two-stage revision procedures are created by using industrially manufactured cement already containing Vancomycin or by manually admixing Vancomycin to PMMA cement [6,18,19]. The use of the commercially available cement COPAL® G+V is already established in PJI prevention especially against the most frequent PJI germs S. aureus and S. epidermidis [8,18] – but does not cover VRSA, VISA or VRSE. In general, it's recommended to use a fixation or spacer cement containing two complementary antibiotics to best cover the spectrum of PJI pathogens [12]. The spectrum of Vancomycin is predominantly limited to gram-positive bacteria and therefore a broad-spectrum antibiotic is needed to also cover gram-negative bacteria, e.g. Gentamicin [13]. Additionally, the combination of two antibiotics offers a synergistic elution effect that leads to an overall increased antibiotic elution from PMMA bone cement resulting in a stronger antimicrobial effect [2]. Antibiotic-loaded bone cement with Gentamicin and Daptomycin can make a difference in prevention and treatment of PJI with Vancomycin-resistant pathogens [20]. Daptomycin offers a good safety profile and has a unique mode of action maybe also effective against bacteria in biofilms [20] coming with a low resistance profile [21]. According to Gray and Wenzel, 2020 [14] knowledge on the exact mode of action is still missing, but they observed that the resistance development of Daptomycin is slower compared to other antibiotics with single protein targets. Rouse et al. [22] figured out with a rat model that a PMMA cement with Daptomycin may be an option for the local treatment of resistant bacteria causing osteomyelitis. The manual admixture of Daptomycin to PMMA bone cement is suggested for PJI cases caused by VRSA, VRE, MRSA and MRSE with a Vancomycin MIC of greater than 2 µg/mL [10]. A first case study 2013 already showed the ability of PMMA spacers with Daptomycin to eradicate an infection in a two-stage revision hip surgery [23]. In our study we found an antimicrobial effectiveness for GD1.5 and GD1.0 whereas a concentration of 0.5 g Daptomycin was not sufficient. This is in line with findings from Eick et al. [24] who concluded from their inhibition zone testing, that 1.5 g of Daptomycin shows an antimicrobial effect in contrast to 0.5 g. This may also be caused by the combination of two antibiotics Gentamicin and Daptomycin and the resulting synergistic elution effect. The combination of 0.5 g Gentamicin and 1.5 g Daptomycin showed the best antibiotic elution profile, as well as a synergistic elution effect supporting infection prevention [15]. The overall elution profile of Daptomycin is comparable to the findings from Meeker et al. [25] showing a peak elution for the first 24 hours. Our observed synergistic elution effect is in contrast to the studies quoted by Antonello et al. [20] concluding a rather antagonistic interaction of Daptomycin and Gentamicin from their study review. But also studies in the larvae biofilm model Galleria melonella showed a synergistic effect combining Gentamicin with Daptomycin for Vancomycin resistant E. faecium [26]. We observed an effect on the bacterial growth comparable to Webb et al. [27] indicating an inhibitory effect of Daptomycin on the growth of resistant strains of gram-positive bacteria. Overall, the synergistic elution effect as well as the high Daptomycin release suggested a positive effect in combining 0.5 g Gentamycin and 1.5 g Daptomycin in PMMA bone cement. We also investigated on the Vancomycin elution as COPAL® G+V was set as reference: despite we found the highest Vancomycin elution for day 1, we assume this concentration is not sufficient to cover Vancomycin-resistant germs. Especially as the elution already decreased by ~85 % on day 2.
To ensure patient safety Daptomycin must be sterilized with either ethylene oxide or gamma radiation. Our findings suggested that Daptomycin-loaded bone cement should be sterilized using gamma radiation to maintain its antimicrobial effectiveness because a sterilization by ethylene oxide reduced the efficacy of Daptomycin significantly.
To best treat MRSE, MRSA or enterococci PIF pocket guide [16] recommends to increase the Vancomycin concentration of commercially available COPAL® G+V by another 2 g. But an increase of added antibiotic powder exceeding a total concentration of 10 % results in a spacer cement that does not longer fulfill the mechanical ISO requirements for bone cement [15,19,28]. Despite Lunz et al. [29] point out, that an antibiotic concentration exceeding 10 % of powder volume significantly reduces the mechanical strength of PMMA spacers, they recommend to manually admix 4 g of Vancomycin to PALACOS® R+G instead of using the commercially available COPAL® G+V. These spacers do not comply with the ISO requirements as the bending strength for PALACOS® R+G + 4 g Vancomycin is below the minimum threshold of 50 MPa and comes with the potential risk of bone cement or spacer fracture [15,19,21,29] [15]. Therefore, we assessed the mechanical stability of a Daptomycin-containing bone cement. ISO bending modulus of GD samples was increased compared to the reference samples as admixing antibiotics increases the hydrophilic characteristics of PMMA cements which results in an increased elasticity of the cement [15]. The mechanical properties of GD1.5, GD1.0 and GD0.5 were all above the corresponding minimum thresholds as the concentration of the added Daptomycin was below 10 % of total PMMA cement powder [15,22,30]. Considering the mechanical properties, a concentration of 1.0 g Daptomycin would be ideal, but does not offer a sufficient antibiotic release needed for infection prevention. As the bone cement GD1.5 showed antimicrobial effectiveness and promising mechanical properties handling characteristics were only assessed for this bone cement sample. ISO setting time, assessed according to ISO 5833:2002 [31], determines the time point when the bone cement is completely set and cannot be handled any longer. ISO doughing time describes the time till PMMA cement reaches the dough state. ISO setting time as well as ISO doughing time were comparable to PALACOS® R+G and COPAL® R+V indicating a slightly faster setting time for GD1.5 which means that the application time window shortens.
Our investigations indicate that the performance of a PMMA bone cement containing 0.5 g Gentamicin and 1.5 g Daptomycin is the choice considering its antibiotic effectiveness, antibiotic release, and mechanical stability (Figure 7). According to the recommendations from PRO-IMPLANT Foundation 3.0 g Daptomycin can be added to a PMMA spacer cement [16], but Kühn [15] suggested not to add more than 2 g Daptomycin, which is in line with our findings. PMMA spacers with manually added antibiotics also must fulfill the legal requirements for medical devices and comply with the ISO standards [15]. This is rather from a legal perspective important as the surgeon becomes – by admixing antibiotics – the legal manufacturer of the product. We assumed that the concentration of 3 g Daptomycin was recommended because the antimicrobial effect was perceived as not sufficient, so this indicates that the antibiotic release is too weak. It’s also described in literature that the “Daptomycin dose in ALBC for spacer should be 3.3-times the original dose to double the release” [21]. As the mode of action of Daptomycin is dependent on calcium ions, solely adding more Daptomycin does not necessarily improve the antimicrobial effectiveness [14]. The mode of action is dependent on a sufficient concentration of calcium-ions [14] in the surrounding tissue: to increase the inhibitory effect of Daptomycin eluted from PMMA bone cement potentially calcium ions could be added [30]. We want to investigate on that in a further study. As manually admixed ALBC is mainly used for spacers we recommend investigating a longer time period of more than 14 days to better simulate the spacer interim period of a two-stage revision protocol [19]. Despite this we also recommend further investigations with Daptomycin-containing PMMA cement in biofilm models.
We want to highlight, that a surgeon ordering Daptomycin from the pharmacy will receive a product other from the industrially used Daptomycin. The clinical available “Cubicin” [32] contains beside Daptomycin also natrium hydroxide, its potential influence on the mechanical properties and antibiotic elution from PMMA bone cement is not yet clarified. Following the recommendations from PRO-IMPLANT foundation [16] the addition of Cubicin is costly: for a fixation cement ~ 780 € (2 g) and even more for a spacer cement ~1,500 € (3 g); not yet including the price for a Gentamicin-loaded PMMA bone cement as basis for admixing. From a financial perspective, a commercially available PMMA bone cement with Gentamicin and Daptomycin could be of interest.
4. Materials and Methods
4.1. PMMA Cements and Bacteria
PALACOS® R, PALACOS® R+G and COPAL® G+V (Heraeus Medical GmbH, Wehrheim, Germany) were used. PALACOS® R+G was loaded with 1.5 g, 1.0 g, and 0.5 g of Daptomycin powder (Xellia Pharmaceuticals ApS, Denmark). PALACOS® R, PALACOS® R+G and COPAL® G+V were used as references (Table 1). Daptomycin was manually admixed in three different concentrations with 1.5 g (GD1.5), 1.0 g (GD1.0) and 0.5 g (GD0.5). Test strains derived from clinical isolates from the Eugen Domann culture collection (EDCC) and Culture Collection University of Gothenburg (CCUG) with different resistance patterns against Gentamicin, Methicillin and Vancomycin were used to test the antimicrobial properties of the bone cement samples in vitro (Figure 8).
4.2. Certika® Proliferation Assay
Certika® microplate proliferation assay was used to determine the antimicrobial efficacy of material surfaces by measuring their ability to prevent the multiplication of microorganisms and germs on a surface. The testing was conducted according to a method developed by QualityLabs BT GmbH, published by Bechert et al., 2000, [33,34,35]. Bone cement samples (seven replicates each) with a diameter of 6 mm were prepared using moulds. Tested material was defined as antimicrobial if the formation of at least 99.9% of the daughter cells during the observation time was prevented in comparison to the blank sample. Statistical analysis was performed in line with DIN EN ISO/EC 17025 [36].
4.3. Inhibition Zone Testing
To detect the antimicrobial effectiveness inhibition zone tests were performed. Agar plates with Bacto-Agar (2% Agarose) and tris-buffered minimum medium (Ca 10µM, phosphate 130 µM) were prepared and incubated with Bacillus subtilis ssp. Bacillus spizizenzii ATCC 6633 [37]. Two bone cement samples with a diameter of 6.0 mm were placed on one plate executing four repetitions per cement sample. Agar plates were incubated for 48 h at 36° C. IMAGE pro scanning software was used to determine the sizes of the inhibition zone. Afterwards average values and standard deviation was calculated for all test samples. If Daptomycin was effective against B. subtilis, it would diffuse in the agar creating a clear area, known as the zone of inhibition. In this clear zone the growth of the bacteria is inhibited. The size of this zone was measured and used to interpret the effectiveness of PMMA bone cement containing Daptomycin as antimicrobial agent.
To determine the influence of sterilization on the antimicrobial effectiveness of non-sterilized, ethylene oxide- and gamma-sterilized Daptomycin against B. subtilis an inhibition zone test was performed by an external certified lab INNOVENT e.V. Jena.
4.4. High-Performance Liquid Chromatography (HPLC)
To determine the release profile of Gentamicin and Daptomycin over 5 days, dissolved from bone cement samples (60 dissolution samples each) a HPLC with MS/MS detection was performed [38,39]. As medium for dissolution 0.1 M tris-hydrochloride buffer (pH 7.4) was used. Gentamicin was determined by analyzing its major components separately (resulting in three signals/peaks during LC-MSMS) and summing these three signals to a total concentration. Daptomycin was directly determined using LC-MSMS. The method was online validated using one set of matrix calibration standard and two sets of quality control samples. The calibration samples were used for calculation of results and the quality control samples to monitor the quality of the analytical run.
4.5. Mechanical stability testing according to ISO 5833 and DIN 53435
To ensure that the added Daptomycin does not negatively influence the mechanical stability of the PMMA cement a mechanical testing for bending strength, bending modulus and compressive strength according to ISO 5833:2002 [31] was performed. To determine the compressive strength the cement rods (12 mm height, 6 mm diameter) were loaded with a constant crosshead speed of 19.8-25.4 mm/min. The tests were run at 23 ± 1° C with dry specimens prepared 24 h before testing. For the bending strength and bending modulus, rectangular specimens (3.3 mm x 75.0 mm x 10.0 mm) were used, they were loaded with a constant crosshead speed of 5 mm/min. The tests were run at 23 ± 1° C with dry specimens prepared 24 h before testing. The four-point bending test rig had 60 mm between the outer loading points and 20 mm between the inner loading points. The tests were continued until failure and the maximum force was used to calculate the bending strength. Value calculations and statistical analysis was performed as described in the ISO standard [31]
DIN impact strength and bending strength were also determined according to DIN 53435 [40]. The rectangular specimens (3.0 mm x 15.0 mm x 10.0 mm) were stored at least 12 h under standard climatic conditions using the appropriate impact direction (consumption of at least 10 %, at most 80 %, of the maximum impact by the test specimens). Bone cement samples were placed vertical in the test device and the pendulum was adjusted to 90° the height of the drop. According to DIN 53435 [40] the average and standard deviation was calculated in kJ/m2. For the DIN bending strength a bending force of 400 Ncm was applied to the bone cement samples till they broke. The bending strength was measured and calculated as well as statistical analysis was performed according to DIN 53435 [40].
4.6. Handling Properties of PMMA Cement
ISO setting and ISO doughing time were assessed and statistical analysis was performed [31].
5. Conclusions
All mechanical and handling properties, elution profile and effectivity of 1.5 g of Daptomycin to 40 g of PMMA fulfill all clinical requirements. Due to its antimicrobial spectrum against Vancomycin-resistant germs (e.g., VRE) a PMMA cement containing 0.5 g Gentamicin and 1.5 g Daptomycin instead of Vancomycin could be a good option to the already established Vancomycin containing PMMA-cements like COPAL® G+V for PJI treatment. Further investigations on its performance in biofilm models and against clinical isolates are recommended.
Author Contributions
Conceptualization, methodology, and investigations: K.-D.K., S.V., R.S., and M.H. The topic is a derived and in-depth scientific question. Writing – review, M.H.; writing – review and editing, K.-D.K.; supervision, K.-D.K., K.T., E.D., C.F. and V.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Heraeus Medical GmbH. The APC* was funded by Heraeus Medical GmbH.
Institutional Review Board Statement
Not applicable. It is an in vitro study. No animals included.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are presented in this article. The data are also available at Heraeus Medical GmbH.
Conflicts of Interest
K.T., E.D., C.F., V.A. and K.-D.K declare no conflicts of interest. S.V., R.S. and M.H. are employees of Heraeus Medical GmbH.
References
- Morgenstern, M.; Erichsen, C.; Militz, M.; Xie, Z.; Peng, J.; Stannard, J.; Metsemakers, W.-J.; Schaefer, D.; Alt, V.; Søballe, K.; et al. The AO trauma CPP bone infection registry: Epidemiology and outcomes of Staphylococcus aureus bone infection. J. Orthop. Res. 2021, 39, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Berberich, C.; Josse, J.; Ruiz, P.S. Patients at a high risk of PJI: Can we reduce the incidence of infection using dual antibiotic-loaded bone cement? Arthroplasty 2022, 4, 41. [Google Scholar] [CrossRef] [PubMed]
- Patel, R. Periprosthetic Joint Infection. N. Engl. J. Med. 2023, 388, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Izakovicova, P.; Borens, O.; Trampuz, A. Periprosthetic joint infection: current concepts and outlook. EFORT Open Rev. 2019, 4, 482–494. [Google Scholar] [CrossRef] [PubMed]
- Sax, F.H.S.; Fink, B. Total Knee Arthroplasty in Unrecognized Septic Arthritis—A Descriptive Case Series Study. antibiotics 2023. [Google Scholar] [CrossRef]
- Cui, Q.; Mihalko, W.M.; Shields, J.S.; Ries, M.; Saleh, K.J. Antibiotic-impregnated cement spacers for the treatment of infection associated with total hip or knee arthroplasty. J. Bone Joint Surg. Am. 2007, 89, 871–882. [Google Scholar] [CrossRef]
- Hasandoost, L.; Rodriguez, O.; Alhalawani, A.; Zalzal, P.; Schemitsch, E.H.; Waldman, S.D.; Papini, M.; Towler, M.R. The Role of Poly(Methyl Methacrylate) in Management of Bone Loss and Infection in Revision Total Knee Arthroplasty: A Review. J. Funct. Biomater. 2020, 11. [Google Scholar] [CrossRef]
- Blersch, B.P.; Barthels, M.; Schuster, P.; Fink, B. A Low Rate of Periprosthetic Infections after Aseptic Knee Prosthesis Revision Using Dual-Antibiotic-Impregnated Bone Cement. antibiotics 2023, 1368. [Google Scholar] [CrossRef]
- Leta, T.H.; Fenstad, A.M.; Lygre, S.H.L.; Lie, S.A.; Lindberg-Larsen, M.; Pedersen, A.B.; W-Dahl, A.; Rolfson, O.; Bülow, E.; Ashforth, J.A.; et al. The use of antibiotic-loaded bone cement and systemic antibiotic prophylactic use in 2,97,357 primary total knee arthroplasties from 2010 to 2020: an international register-based observational study among countries in Africa, Europe, North America, and Oceania. Acta Orthopaedica 2023, 416–425. [Google Scholar] [CrossRef]
- Shariati, A.; Dadashi, M.; Moghadam, M.T.; van Belkum, A.; Yaslianifard, S.; Darban-Sarokhalil, D. Global prevalence and distribution of vancomycin resistant, vancomycin intermediate and heterogeneously vancomycin intermediate Staphylococcus aureus clinical isolates: a systematic review and meta-analysis. Sci. Rep. 2020, 10, 12689. [Google Scholar] [CrossRef]
- Markwart, R.; Willrich, N.; Haller, S.; Noll, I.; Koppe, U.; Werner, G.; Eckmanns, T.; Reuss, A. The rise in vancomycin-resistant Enterococcus faecium in Germany: data from the German Antimicrobial Resistance Surveillance (ARS). Antimicrob. Resist. Infect. Control 2019, 8, 147. [Google Scholar] [CrossRef] [PubMed]
- Abdel, M.P.; Barreira, P.; Battenberg, A.; Berry, D.J.; Blevins, K.; Font-Vizcarra, L.; Frommelt, L.; Goswami, K.; Greiner, J.; Janz, V.; et al. Hip and Knee Section, Treatment, Two-Stage Exchange Spacer-Related: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplasty 2019, 34, S427–S438. [Google Scholar] [CrossRef] [PubMed]
- LaPlante, K.; Rybak Michael. Daptomycin a novel antibiotic against gram positive pathogens. Expert Opoin. Pharmacother. 2004. [Google Scholar] [CrossRef]
- Gray, D.A.; Wenzel, M. More Than a Pore: A Current Perspective on the In Vivo Mode of Action of the Lipopeptide Antibiotic Daptomycin. antibiotics 2020. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, K.-D. PMMA Cements Are we aware what we are using? Springer-Verlag, p. 58-59; 88-89; 96-109; 157-158: Berlin, Heidelberg, 2014, ISBN 13 978-3-642-41535-7.
- PRO-IMPLANT Foundation. Pocket Guide to Diagnosis & Treatment of the Periprosthetic Joint Infection 2023.
- Steadman, W.; Chapman, P.R.; Schuetz, M.; Schmutz, B.; Trampuz, A.; Tetsworth, K. Local Antibiotic Delivery Options in Prosthetic Joint Infection. Antibiotics (Basel) 2023, 12. [Google Scholar] [CrossRef]
- Andréa Cara; Mathilde Ballet; Claire Hemery; Tristan Ferry; Fédéric Laurent; Jérôme Josse. Antibiotics in Bone Cements Used for Prosthesis Fixation: An Efficient Way to Prevent Staphylococcus aureus and Staphylococcus epidermidis Prosthetic Joint Infection. frontiers in Medicine, 2021. [CrossRef]
- Lunz, A.; Schonhoff, M.; Omlor, G.W.; Knappe, K.; Bangert, Y.; Lehner, B.; Renkawitz, T.; Jaeger, S. Enhanced antibiotic release from bone cement spacers utilizing dual antibiotic loading with elevated vancomycin concentrations in two-stage revision for periprosthetic joint infection. Int. Orthop. 2023. [Google Scholar] [CrossRef]
- Antonello, R.M.; Canetti, D.; Riccardi, N. Daptomycin synergistic properties from in vitro and in vivo studies: a systematic review. J. Antimicrob. Chemother. 2022, 78, 52–77. [Google Scholar] [CrossRef]
- Hansen, E.; Kühn, K.-D. Essentials of Cemented Knee Arthroplasty; Springer Berlin Heidelberg, p. 542-548; p. 686-700, 2022, ISBN 978-3-662-63112-6.
- Rouse, M.S.; Piper, K.E.; Jacobson, M.; Jacofsky, D.J.; Steckelberg, J.M.; Patel, R. Daptomycin treatment of Staphylococcus aureus experimental chronic osteomyelitis. Journal of Antimicrobial Chemotherapy 2006, 301–305. [Google Scholar] [CrossRef]
- Cortes, N.J.; Lloyd, J.M.; Koziol, L.; O’Hara, L. Successful clinical use of daptomycin-impregnated bone cement in two-stage revision hip surgery for prosthetic joint infection. Ann. Pharmacother. 2013, 47, e2. [Google Scholar] [CrossRef]
- Eick, S.; Hofpeter, K.; Sculean, A.; Ender, C.; Klimas, S.; Vogt, S.; Nietzsche, S. Activity of Fosfomycin- and Daptomycin-Containing Bone Cement on Selected Bacterial Species Being Associated with Orthopaedic Infections. BioMed Research International 2017. [Google Scholar] [CrossRef]
- Meeker, D.G.; Cooper, K.B.; Renard, R.L.; Mears, S.C.; Smeltzer, M.S.; Barnes, C.L. Comparative Study of Antibiotic Elution Profiles From Alternative Formulations of Polymethylmethacrylate Bone Cement. J. Arthroplasty 2019, 34, 1458–1461. [Google Scholar] [CrossRef] [PubMed]
- Luther, M.K.; Arvanitis, M.; Mylonakis, E.; LaPlante, K. Activity of Daptomycin or Lenezolid in Combination with Rifampin or Gentamicin against Biofilm-Forming Enterococcus faecalis or E. faecium in an In Vitro Parmacondynamic Model Using Simulated Endocardial Vegetations and an In Vivo Survival Assay Using Galleria melonella Larvae. Antimicrob. Agents Chemother. 2014, 4612–4620. [Google Scholar] [CrossRef]
- Webb, N.D.; McCanless, J.D.; Courtney, H.S.; Bumgardner, J.D.; Haggard, W.O. Daptomycin eluted from calcium sulfate appears effective against Staphylococcus. Clin. Orthop. Relat. Res. 2008, 466, 1383–1387. [Google Scholar] [CrossRef] [PubMed]
- Dunne, N.J.; Hill, J.; McAfee, P.; Kirkpatrick, R.; Patrick, S.; Tunney, M. Incorporation of large amounts of gentamicin sulphate into acrylic bone cement: effect on handling and mechanical properties, antibiotic release, and biofilm formation. Proceedings of the I MECH E Part H Journal of Engineering in Medicine 2008, 222, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Lunz, A.; Knappe, K.; Omlor, G.W.; Schonhoff, M.; Renkawitz, T.; Jaeger, S. Mechanical strength of antibiotic-loaded PMMA spacers in two-stage revision surgery. BMC Muscoskeletal Disorders 2022. [Google Scholar] [CrossRef]
- Hertzberg-Boelch, S.P. von; Luedemann, M.; Rudert, M.; Steinert, A.F. PMMA Bone Cement: Antibiotic Elution and Mechanical Properties in the Context of Clinical Use. biomedicines 2022. [Google Scholar] [CrossRef]
- SO 5833:2002. Implants for surgery - Acrylic resin cements. ISO: Geneva, Switzerland, 2002.
- MSD SHARP & DOHME GMBH. Cubicin. Instruction for Use. (In German).
- Alt, V.; Bechert, T.; Steinrücke, P.; Wagener, M.; Seidel, P.; Dingeldein, E.; Domann, E.; Schnettler, R. An in vitro assessment of the antibacterial properties and cytotoxicity of nanoparticulate silver bone cement. Biomaterials 2004, 25, 4383–4391. [Google Scholar] [CrossRef]
- Alt, V.; Bechert, T.; Steinrücke, P.; Wagener, M.; Seidel, P.; Dingeldein, E.; Domann, E.; Schnettler, R. In vitro testing of antimicrobial activity of bone cement. Antimicrob. Agents Chemother. 2004, 48, 4084–4088. [Google Scholar] [CrossRef]
- Bechert, T.; Steinrücke, P.; Guggenbichler, J.P. A new method for screening anti-infective biomaterials. Nat. Med. 2000, 6, 1053–1056. [Google Scholar] [CrossRef]
- DIN EN ISO/IEC 17025:2017. General requirements for the competence of testing and calibration laboratories. ISO: Geneva, Switzerland, 2017.
- Fuchs, P.; Barry, A.; Brown, S. Evaluation of daptomycin susceptibility testing by Etest and the effect of different batches of media. Journal of Antimicrobial Chemotherapy 2001, 557–561. [Google Scholar] [CrossRef]
- Aiken, S.S.; Cooper, J.J.; Florance, H.; Robinson, M.T.; Michell, S. Local release of antibiotics for surgical site infection management using high-purity calcium sulfate: an in vitro elution study. Surg. Infect. (Larchmt) 2015, 16, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Amin, T.J.; Lamping, J.W.; Hendricks, K.J.; McIff, T.E. Increasing the elution of vancomycin from high-dose antibiotic-loaded bone cement: a novel preparation technique. J. Bone Joint Surg. Am. 2012, 94, 1946–1951. [Google Scholar] [CrossRef] [PubMed]
- DIN 53435:2018. Testing of plastics - bending test and impact test on dynstat test specimens. GlobalSpec: Albany, NY, USA, 2018.
Figure 1.
Antimicrobial efficacy of different Daptomycin concentration (0.5 g, 1.0 g, 1.5 g) in PMMA bone cement samples determined by Certika® proliferation assay for: (a) Methicillin-resistant S. epidermidis; (b) Vancomycin-resistant S. aureus; (c) Vancomycin-resistant E. faecium; (d) Methicillin-resistant S. aureus.
Figure 1.
Antimicrobial efficacy of different Daptomycin concentration (0.5 g, 1.0 g, 1.5 g) in PMMA bone cement samples determined by Certika® proliferation assay for: (a) Methicillin-resistant S. epidermidis; (b) Vancomycin-resistant S. aureus; (c) Vancomycin-resistant E. faecium; (d) Methicillin-resistant S. aureus.
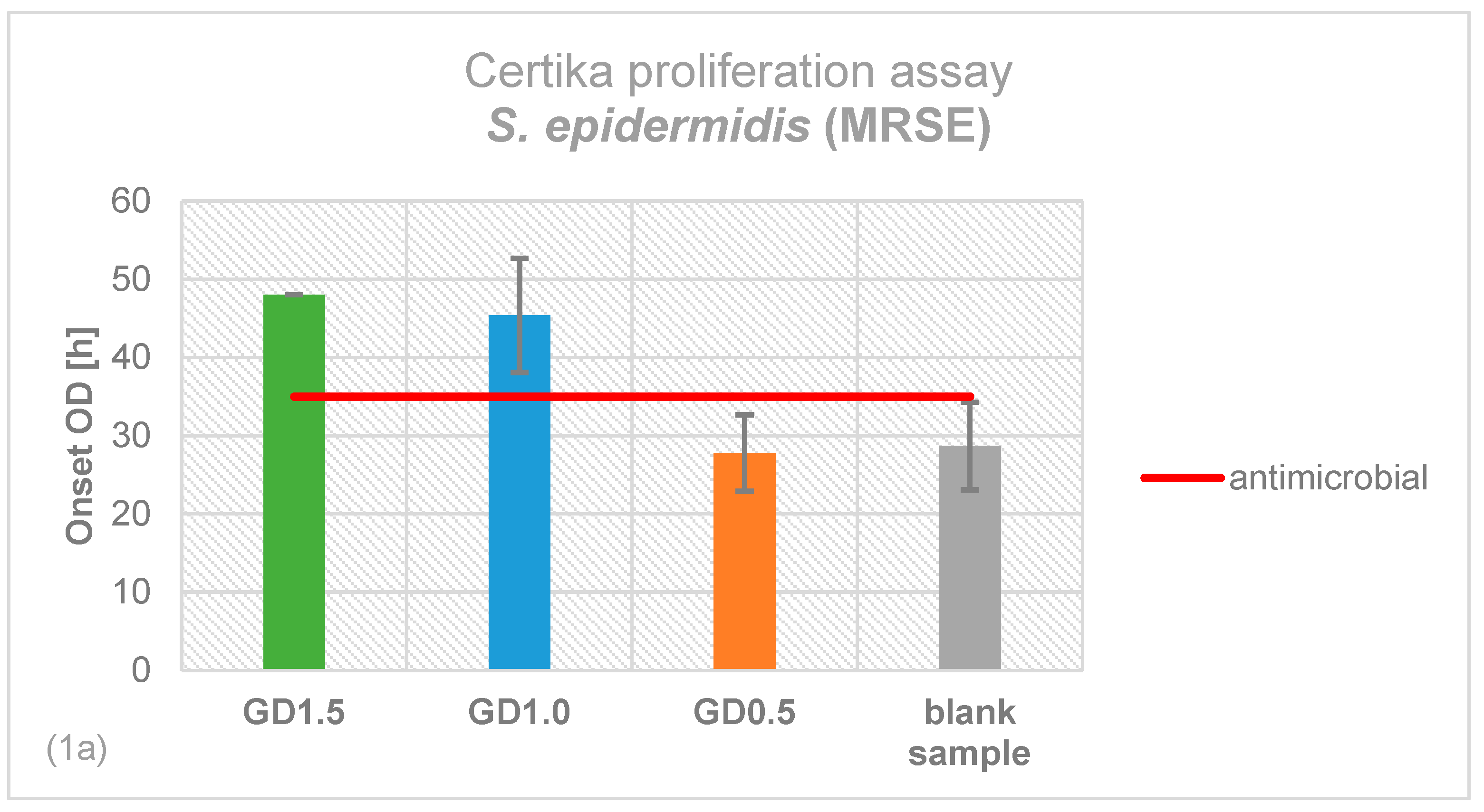
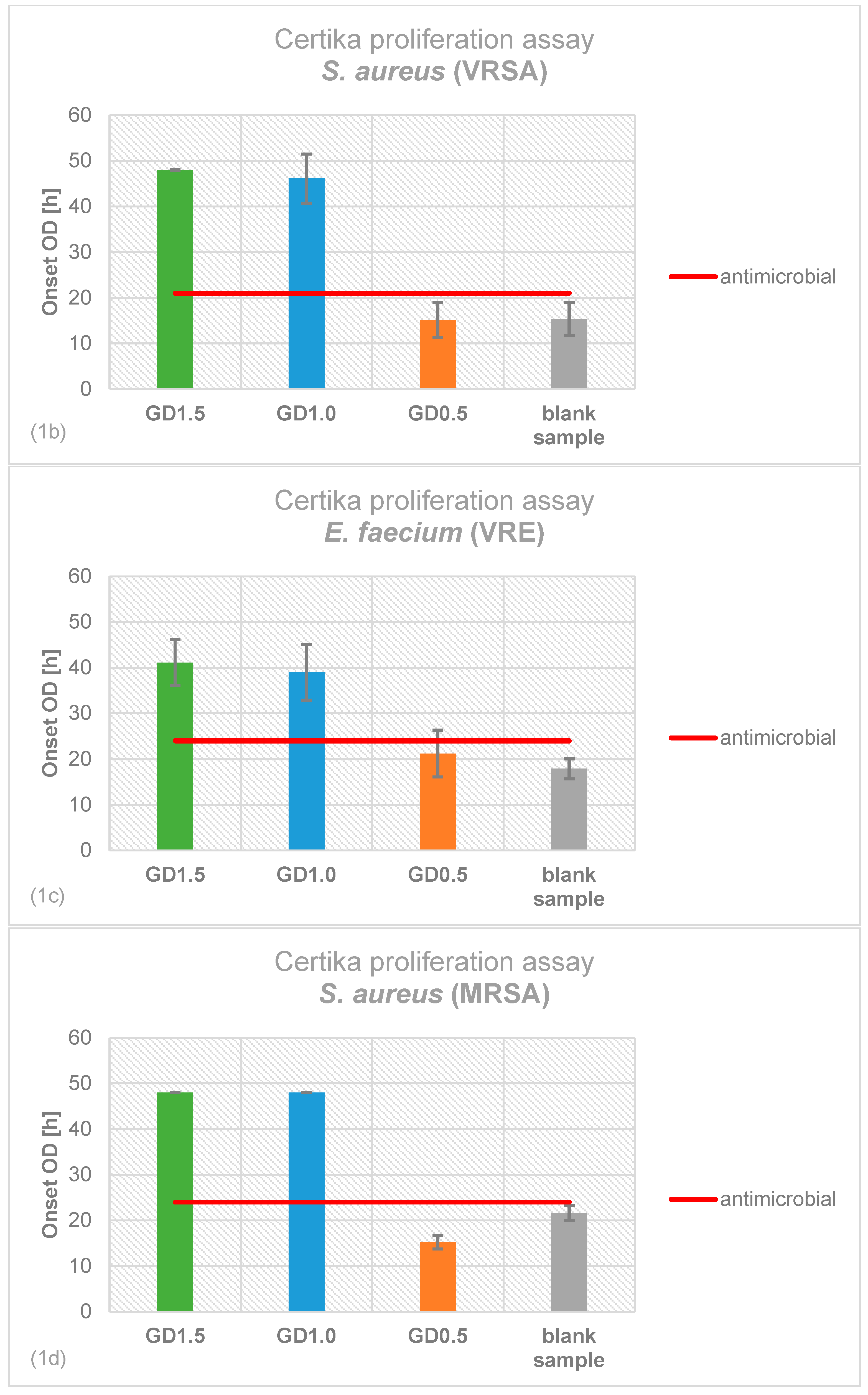
Figure 2.
Average inhibition zones determined by inhibition zone test for all three different Daptomycin concentrations.
Figure 2.
Average inhibition zones determined by inhibition zone test for all three different Daptomycin concentrations.
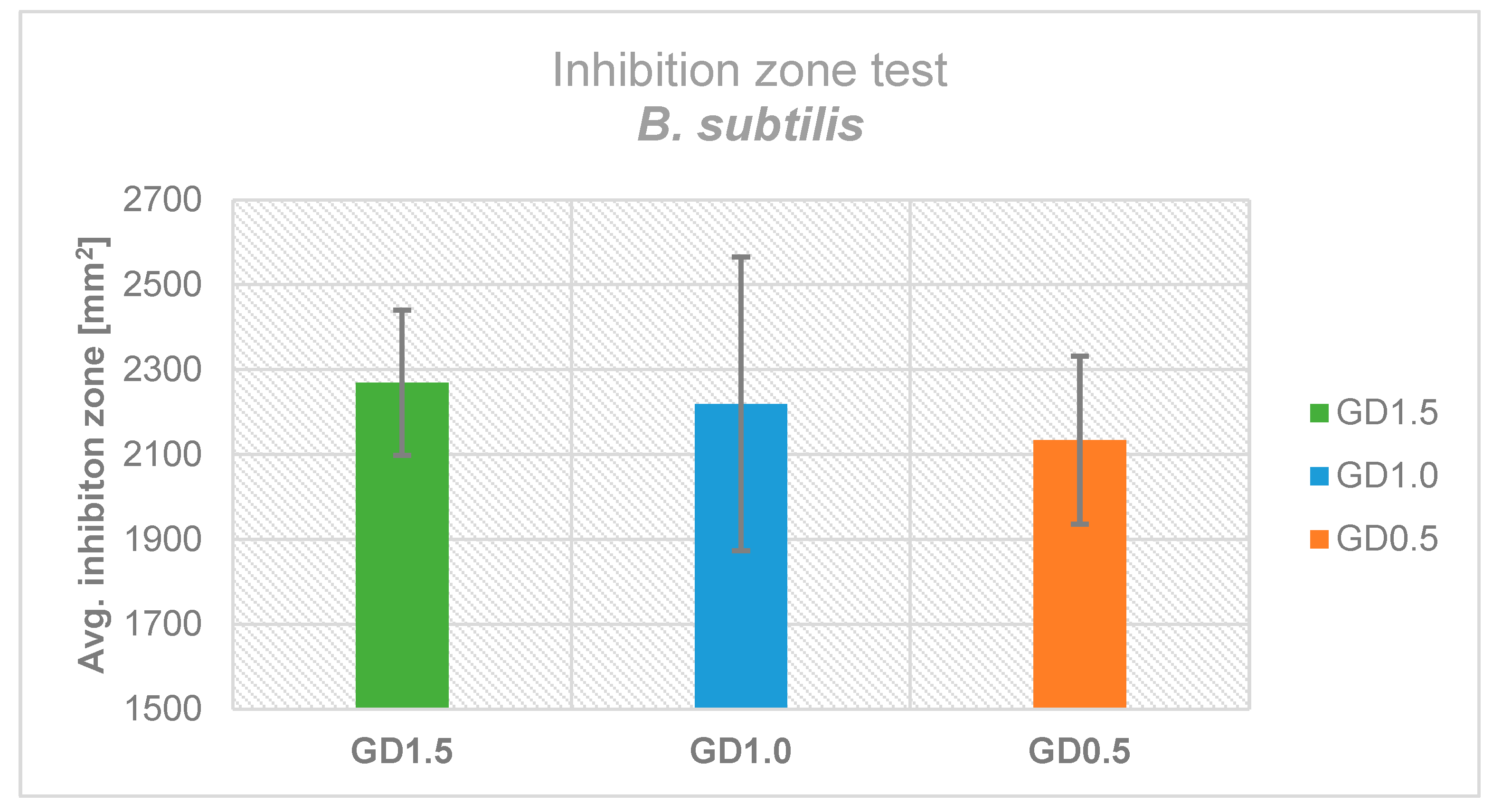
Figure 3.
Influence of gamma and ethylene oxide sterilization on the antimicrobial effectiveness of Daptomycin against B. subtilis in contrast to non-sterilized Daptomycin.
Figure 3.
Influence of gamma and ethylene oxide sterilization on the antimicrobial effectiveness of Daptomycin against B. subtilis in contrast to non-sterilized Daptomycin.
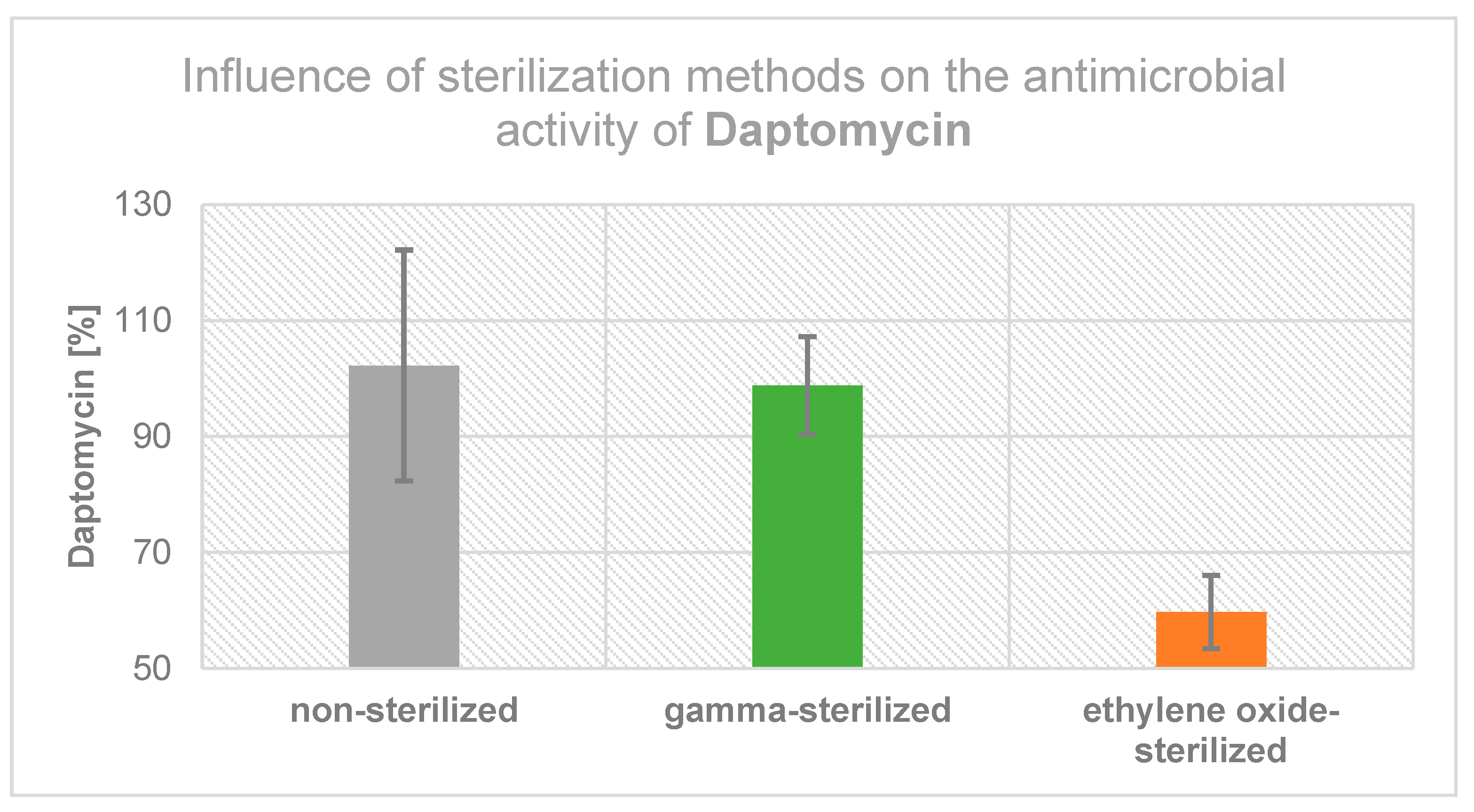
Figure 4.
Release profile from PMMA bone cement was determined with HPLC for (a) Gentamicin day 1-5; (b) Daptomycin day 1-5; (c) Daptomycin day 2-5; (d) Vancomycin day 1-5.
Figure 4.
Release profile from PMMA bone cement was determined with HPLC for (a) Gentamicin day 1-5; (b) Daptomycin day 1-5; (c) Daptomycin day 2-5; (d) Vancomycin day 1-5.
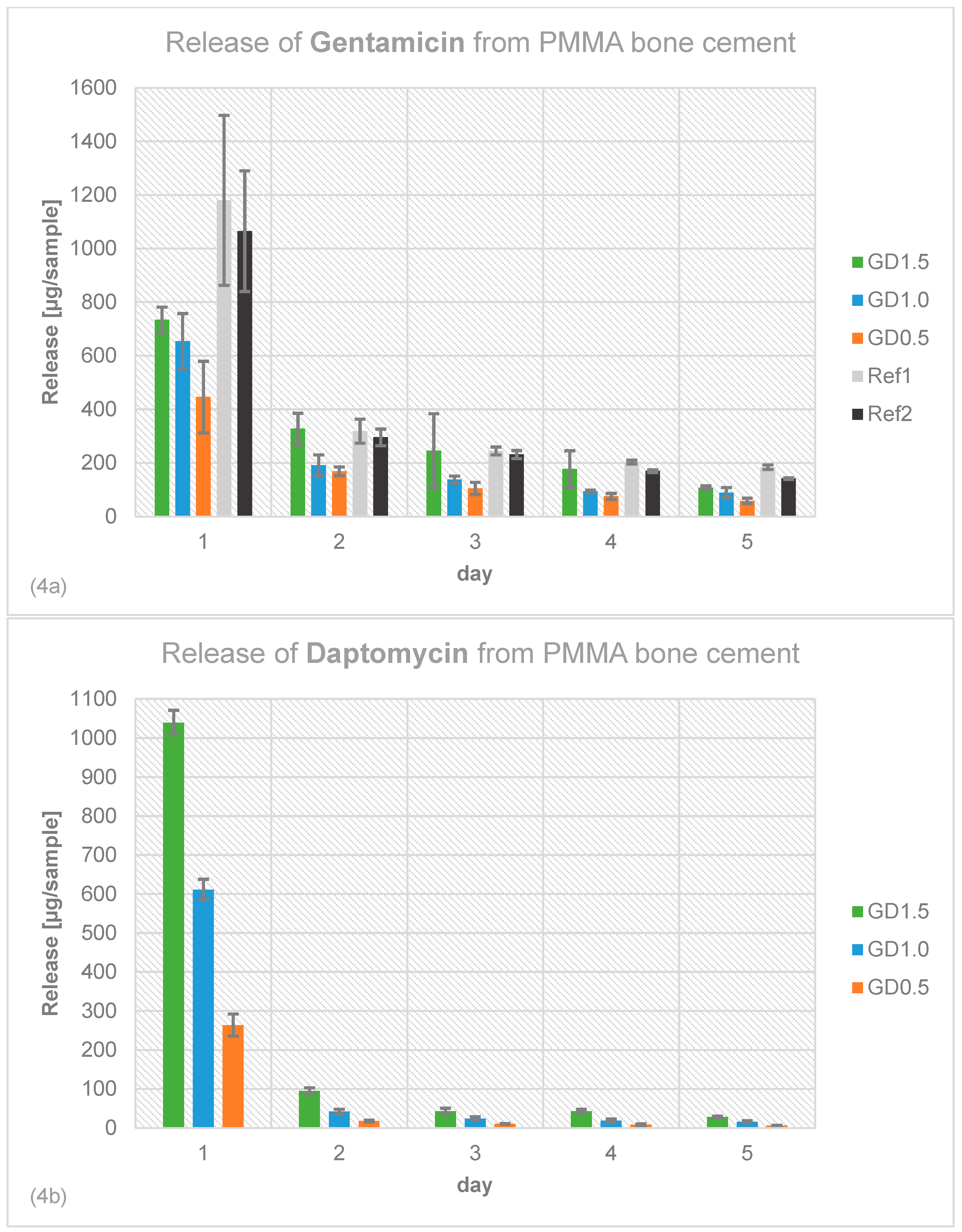
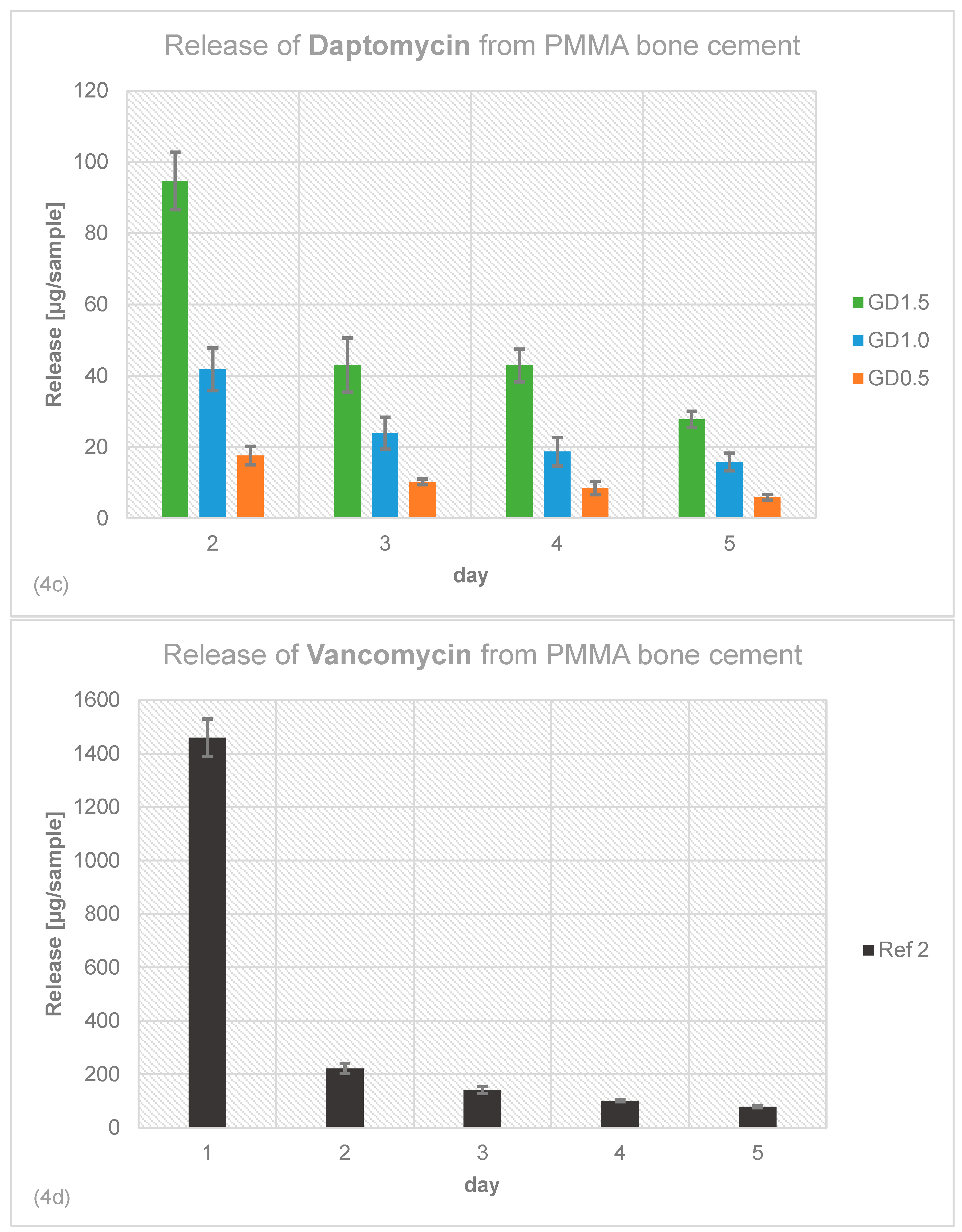
Figure 5.
Mechanical stability tested for all Daptomycin concentrations compared to Ref1 and Ref2: (a) four-point bending strength; (b) four-point bending modulus; (c) compressive strength.
Figure 5.
Mechanical stability tested for all Daptomycin concentrations compared to Ref1 and Ref2: (a) four-point bending strength; (b) four-point bending modulus; (c) compressive strength.
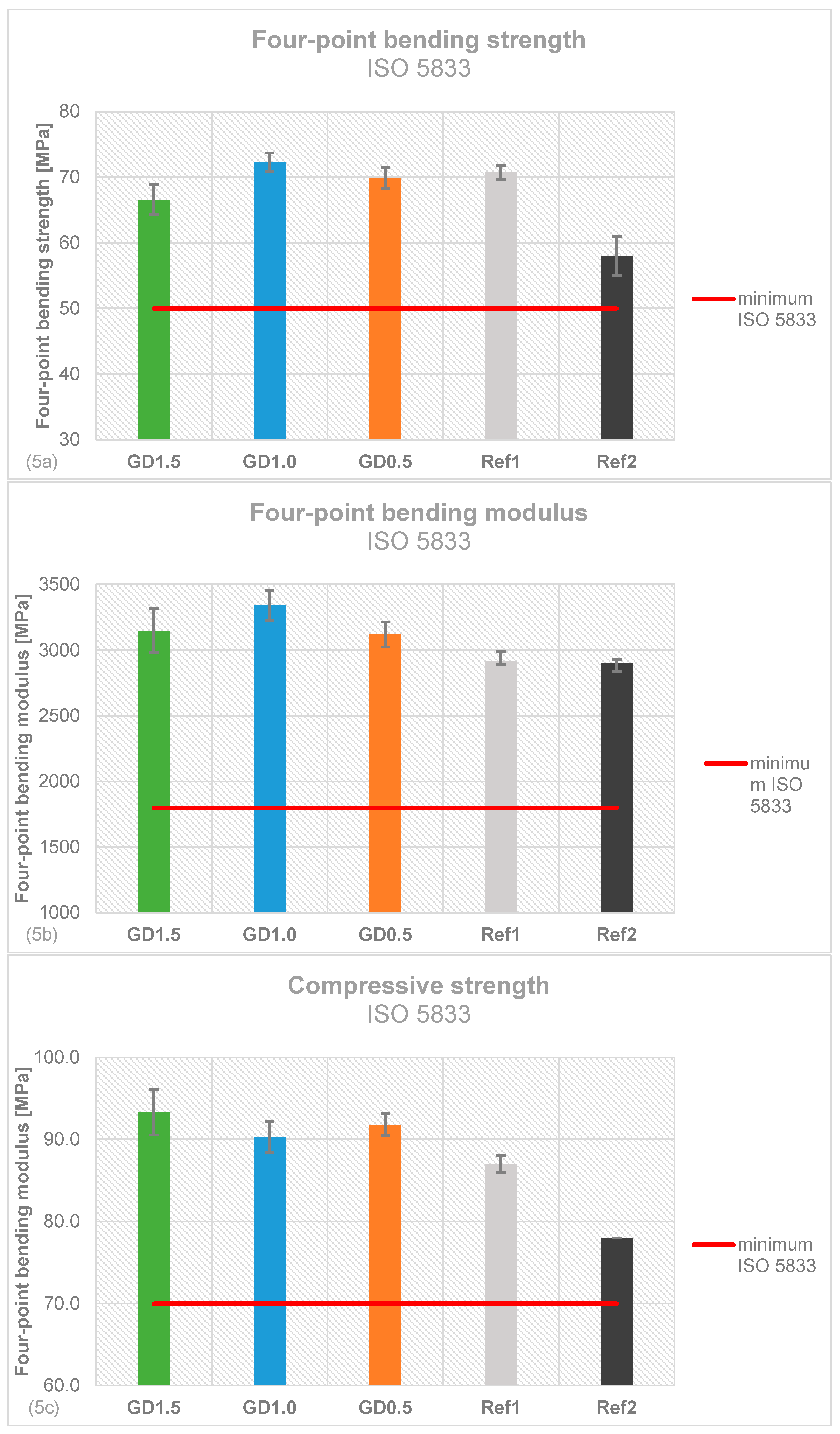
Figure 6.
Mechanical stability tested for all Daptomycin concentrations GD1.5, GD1.0, GD0.5 compared to Ref1 and Ref2 (a) DIN bending strength; (b) DIN impact strength showed as difference to Ref2.
Figure 6.
Mechanical stability tested for all Daptomycin concentrations GD1.5, GD1.0, GD0.5 compared to Ref1 and Ref2 (a) DIN bending strength; (b) DIN impact strength showed as difference to Ref2.
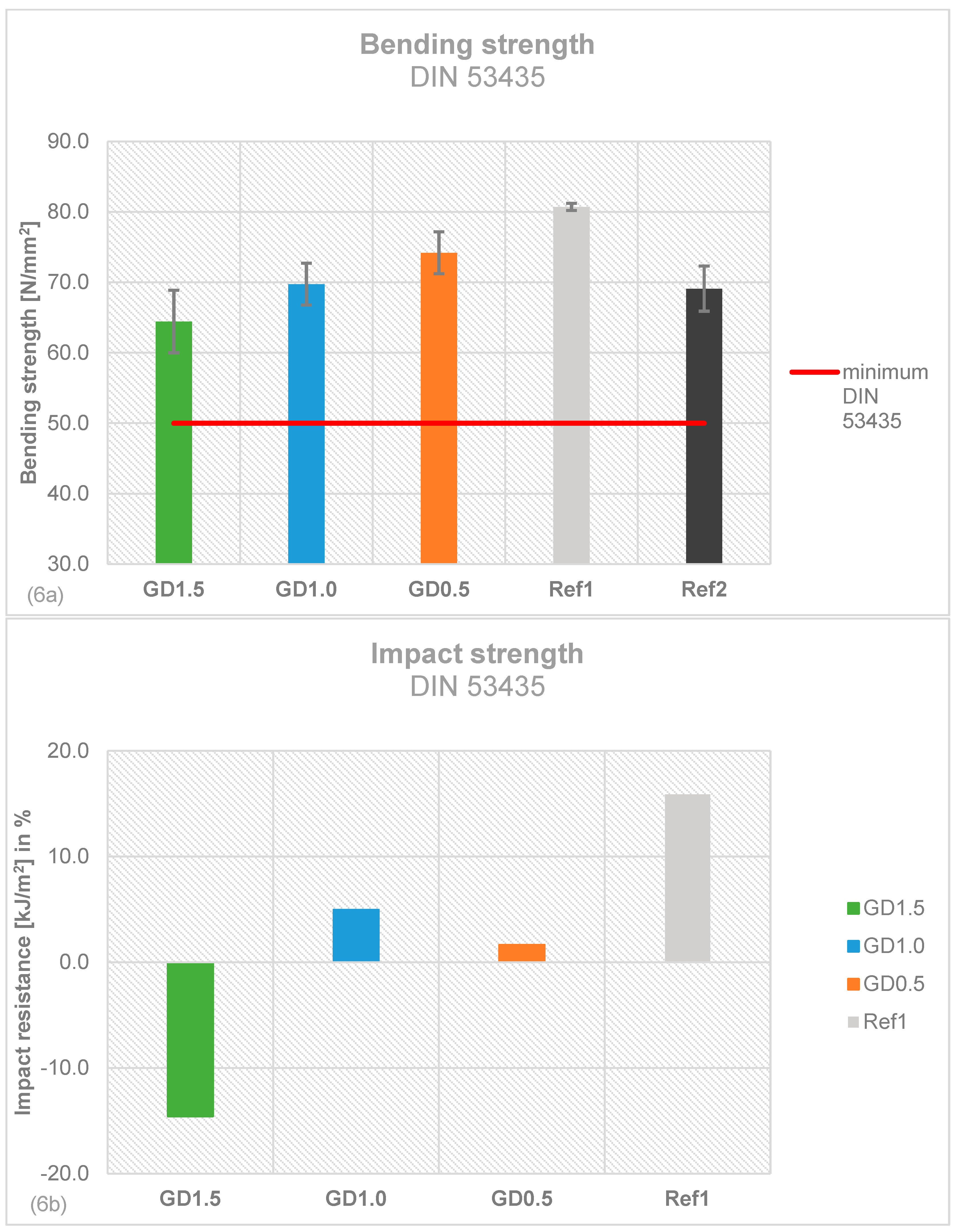
Figure 7.
Overview of performed tests to evaluate the best concentration of Daptomycin that can be added to PMMA bone cement (color coding: white = not evaluated, green = effective or requirements fulfilled; red = non effective or requirements not fulfilled).
Figure 7.
Overview of performed tests to evaluate the best concentration of Daptomycin that can be added to PMMA bone cement (color coding: white = not evaluated, green = effective or requirements fulfilled; red = non effective or requirements not fulfilled).
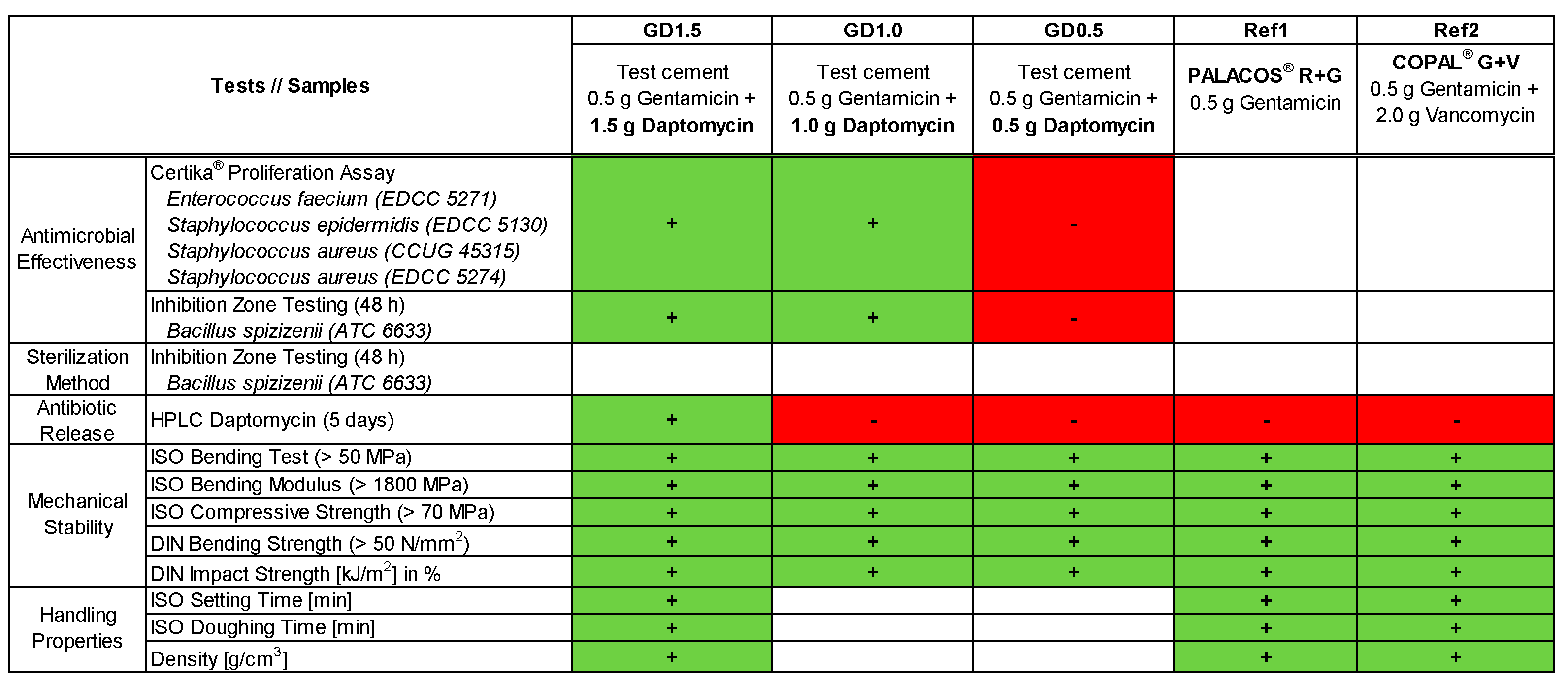
Figure 8.
PMMA bone cement test samples and tests performed to determine antimicrobial effectiveness, antibiotic release, mechanical stability, and handling properties (x = tested; / = not tested).
Figure 8.
PMMA bone cement test samples and tests performed to determine antimicrobial effectiveness, antibiotic release, mechanical stability, and handling properties (x = tested; / = not tested).
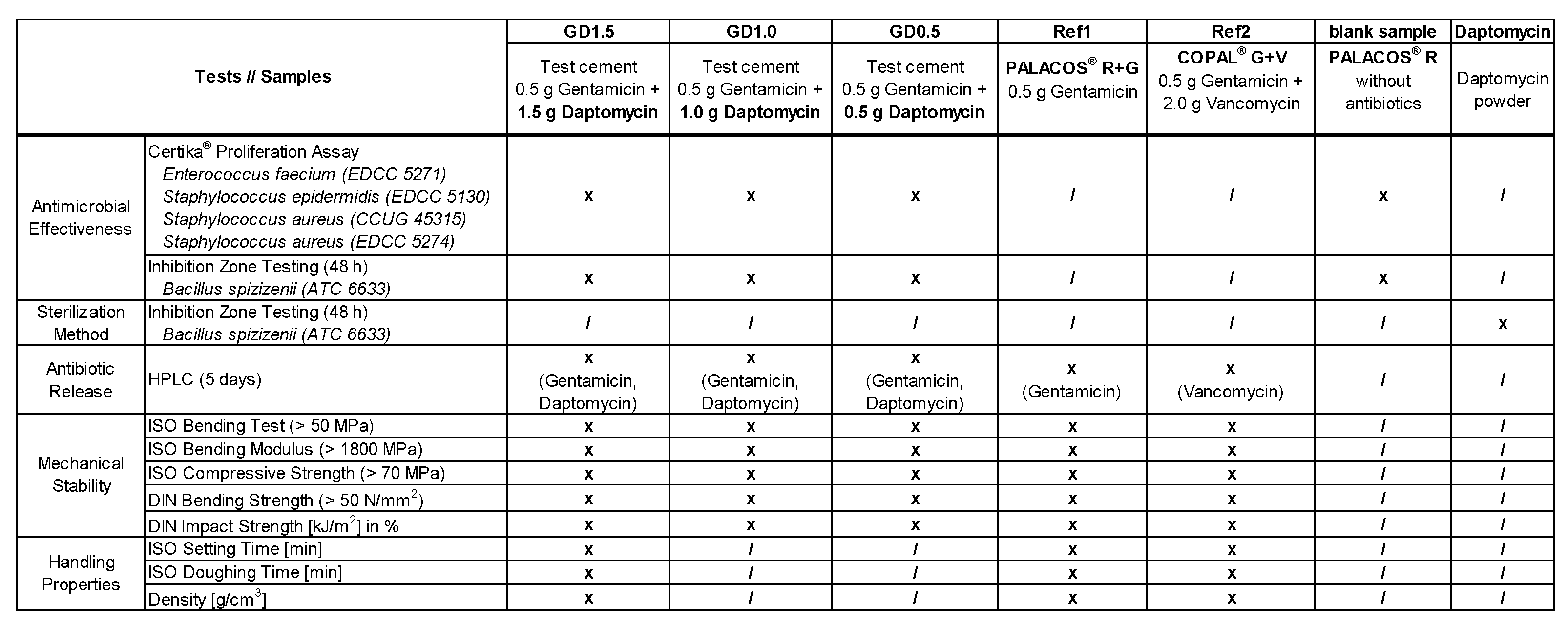

Table 1.
Handling properties of PMMA bone cement containing 0.5 g Gentamicin + 1.5 g Daptomycin compared to commercially available bone cements Ref1 and Ref2.
Table 1.
Handling properties of PMMA bone cement containing 0.5 g Gentamicin + 1.5 g Daptomycin compared to commercially available bone cements Ref1 and Ref2.
| Handling Properties | GD1.5 | PALACOS® R+G Ref1 |
COPAL® G+V Ref2 |
|---|---|---|---|
| ISO Setting Time [min] | 06:45 ± 00:00 | 09:30 ± 00:10 | 08:15 ± 00:18 |
| ISO Doughing Time [min] | 01:30 ± 00:00 | 00:55 ± 00:05 | 01:00 ± 00:05 |
| Density [g/cm3] | 1.13 ± 0.01 | 1.15 ± 0.00 | 1.12 ± 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



