
Submitted:
10 October 2023
Posted:
11 October 2023
You are already at the latest version
Abstract
The purpose of this study is to develop and evaluate the effectiveness of a medical helicopter air transport training program for emergency medical personnel. The program was developed according to Rapid Prototyping Instructional System Design (RPISD) and finalized after content validity and usability evaluation. The effectiveness of the program was evaluated using a single-arm pre-post design to measure the performance of 11 convenience-sampled emergency medical technicians after the program was applied. Data analysis was performed using the SPSS 26.0 Program and Wilcoxon Signed-Rank test. The results of this study are summarized as follows. First, the developed doctor helicopter air transport training program applied RPISD, and the development stage was divided into analysis, design and usability evaluation, and development stages; the final program was derived. Secondly, the developed medical helicopter air transport training program is composed of a blended learning training program that combines online theory lectures and offline simulations for a total of 8 sessions. Third, as a result of applying the developed doctor helicopter air transport training program to 11 emergency medical workers, both pre- and post-air transport subjective job performance and objective job performance were statistically significantly increased. The Dr. Helicopter air transport training program developed in this study was found to be a program that can sufficiently evaluate the job performance of emergency medical personnel in air transport. Through this study, we hope that this training program can directly contribute to improving the survival rate of critically ill patients in the actual air transport field.
Keywords:
airlift
; job performance
; doctor
; helicopter
; RPISD
1. Introduction
The Republic of Korea is building an emergency medical system in an effort to provide the best medical care and has introduced a helicopter dedicated to emergency medical care, known as a doctor helicopter, as a way to supplement the emergency medical transportation system in vulnerable areas and build emergency medical infrastructure [1]. The doctor chopper provides specialized emergency medical services from the field, which is the pre-hospital stage, with emergency medical personnel, including emergency medicine specialists, directly on board, and establishes a safe air transport system according to air transport procedures [1,2]. In addition, emergency medical services using doctor choppers are known to provide rapid and optimized emergency medical care, protect the golden time of patients who need emergency surgery such as severe trauma and cardiac and cerebrovascular diseases, and play an important role in the transfer of emergency patients to medical institutions [3]. Since the introduction of doctor choppers in Korea in 2011, it has been reported that the survival rate of critically ill patients has increased and the mortality rate has decreased due to pre-hospital emergency treatment, showing excellent effectiveness [4].
Internationally, airborne healthcare has been recognized as an important enabler of effective multidisciplinary care delivery, particularly for patients in remote or rural areas [5-7]. Airborne healthcare supports the efficient use of ground resources by bringing clinical teams providing time-critical specialty care directly to the site and rapidly transporting patients to specialized healthcare facilities [8]. In particular, the slogan "centralization of complexity" is a global philosophy of healthcare delivery that calls for getting the right patient to the right place at the right time to save lives and reduce disability.
Emergency medical personnel on board a doctor's helicopter consist of doctors, nurses, and paramedics, who are required to perform at a high level according to their respective competencies in a limited medical field. In other words, they are required to have specialized first aid knowledge and performance skills in order to complete various tasks required for each stage of the mission, including dispatch, operation, field medical care, and patient transfer [9]. However, emergency medical management training programs for doctor helicopter emergency medical workers are insufficient [10], so a customized program based on scientific theory is needed for air transport medical work. In particular, existing education programs are mainly composed of theoretical education based on textbooks, and it is necessary to develop a more systematic air transport work education program in that it does not reflect the needs analysis and job analysis of the emergency transport site.
In this context, it has been suggested that an educational program designed to utilize the rich experience of emergency medical workers as a learning resource is needed [11], so we would like to mention RPISD, which is a user-centered educational program model in the field. Rapid Prototyping Instructional Systems Design (RPISD) is known as a model that can shorten development time by simultaneously analyzing, designing, and developing, and can develop user-centered instructional programs by involving various stakeholders such as instructors, learners, and experts to give voice to the actual field [12]. It has also been reported that this model can increase user convenience by actively reflecting the opinions of participants in the instructional design process [13], evaluate the effectiveness of specific teaching and learning strategies [13], and increase the satisfaction of the target audience with the educational program [14]. In particular, the application of the model can be considered as an appropriate framework for the doctor helicopter air transport training program because it should consider the situation and context of the medical field.
In addition, field-oriented experiential learning, such as the emergency medical transportation system using helicopters, is important for students to face problems and increase their confidence through critical thinking and communication skills [15]. Considering these points, experiential learning theory (ELT) provides an appropriate theoretical framework for designing various and specific learning experiences [16], so we will apply Kolb's ELT to examine the effectiveness of the program.
Therefore, this study aims to develop and apply a medical helicopter air transport training program based on Kolb's (1984) ELT and RPISD, a systematic training program development method, to promote the job performance of medical helicopter emergency medical personnel. ELT has been adopted and validated in various contexts [17-20]. Through this study, we hope to provide a theoretical basis for directly contributing to improving the survival rate of critically ill patients in the actual air transport field.
2. The conceptual foundation of research
This study was conducted to develop a doctor helicopter air transport work training program for emergency medical personnel and to evaluate the effectiveness of the program (Figure 1). The study was divided into development and application phases. Initially, the development phase was based on RPISD, wherein analysis, design, and usability evaluation were conducted simultaneously and cyclically. In the application phase, Kolb's ELT was applied to form the conceptual basis of this study.
3. Methods
In order to develop and evaluate the effectiveness of a doctor helicopter air transport training program for emergency medical personnel, this study was divided into two phases. The first phase is program development, which consists of analysis, prototype design, usability evaluation, and program development. The second phase encompasses program implementation and evaluation. Accordingly, the overall procedure of this study is as shown Table 1.
3.1. Development of a Training Program for Doctor Helicopter Air Transport Work
The Doctor Helicopter Air Transport Work Training Program was developed by applying RPISD, with a total of 15 participants, including doctors, nurses, and paramedics, participating in the development of the training program.
Firstly, in the program analysis stage, we assessed the training requirements by gathering opinions from expert groups to derive the training topics and contents needed for the program. We also analyzed the duties of doctor helicopter air transport work and reviewed domestic and overseas doctor helicopter training programs using data-com technology.
Secondly, in the prototype design stage, we designed educational goals, educational topics, educational contents, and educational methods in the first prototype by reflecting the results derived from the analysis of educational needs, job analysis of air transport work, and review of the doctor helicopter education program. Kolb's ELT was used as the basis for the goals and contents of the doctor helicopter training program.
Thirdly, we developed three prototypes and conducted two usability evaluations to derive the final training program. Additionally, we developed an operator's manual, instructor's manual, and learner's manual for standardized simulation training.
3.2. Applying the Doctor Helicopter Air Transport Work Training Program
3.2.1. Research Design and Research Hypothesis
The single-arm pretest-posttest experimental design to measure the effectiveness of the training program by applying the developed doctor helicopter air transport task training program is shown in the Table 2.
The research hypothesis is as follows:
First, the subjective job performance of air transport work will be higher after applying the Doctor Helicopter Air Transport Work Training Program than before applying it.
Second, the objective job performance of air transport work will be higher after applying the Doctor Helicopter Air Transport Work Training Program than before applying it.
3.2.2. Research subjects
The number of participants in the study to evaluate the program effectiveness of this study was based on previous research [21] that suggests that 10 to 40 participants per group is appropriate for a pilot evaluation to obtain an accurate estimate (effect size), and 11 emergency medical technicians were convenience sampled using the following selection criteria.
- At least 2 years of clinical experience or 2 years of ambulance ride-along experience [22].
- Never been in a helicopter before.
3.2.3. Research Tools
The subjective performance of air transport work is a self-assessment checklist that utilizes the Air Transport Work Measurement Tool developed by the American Association of Air and Ground Transport Nurses. The tool consisted of 15 questions on a 0-4 point Likert scale, with a score range of 0-60 points, with higher scores indicating higher subjective job performance. The reliability result of this study was Cronbach's alpha = .964.
The objective job performance of air transport work is a checklist format developed for instructor observational evaluation, and the tool was modified and supplemented based on the detailed guidelines for doctor helicopters [22]. The tool consists of a maximum score of 2 points and a minimum score of 0 points for each task, with a total of 20 questions, and the total score ranges from a maximum of 40 points to a minimum of 0 points.
To verify the content validity of the measurement tool development, a group of experts consisting of 2 doctors, 3 nurses, and 3 paramedics who work in air transportation was formed, and the content validity was found to be S-CVI 0.97. In addition, the intraclass correlation coefficient (ICC) was used to check the measurement agreement between the two instructors for the application of the measurement tool, and in this study, the ICCs=0.92 (95% CI 0.88~0.95), p< .001, which means that the larger the value, the higher the agreement [23].
3.2.4. Data Collection
Data collection was conducted from August to October 2021 at six hospitals in Korea that have deployed doctor helicopters. The purpose and method of the study were explained to the coordinator of the emergency medical center through an online chat message, and emergency medical workers who wished to participate in this study were conveniently sampled. To protect the rights and interests of the subjects, the purpose and methods of the study were explained to the subjects after review by the researcher's institutional review board, and consent to participate in the study was obtained.
First, before applying the developed training program, a preliminary survey was conducted to determine the general characteristics of the learners and their job performance in air transport.
Second, the developed training program was applied to 11 emergency medical technicians with more than 2 years of experience in the emergency department who had never been on a helicopter. The training program consisted of orientation and safety training in the first session, and theoretical lectures on field medical care in the fourth session. A diagnostic quiz was given after the lecture, and the simulation training method used team activities, lecture, practice, and debriefing.
Third, in the post-test, the subjects self-assessed their subjective job performance in air transportation, and their objective job performance in air transportation was evaluated by the instructor.
Fourth, the objective performance evaluation of the air transport work of 11 subjects in the application of the doctor's helicopter air transport work training program was conducted simultaneously by two instructors, and a research assistant was trained to reduce subjective bias evaluation.
3.2.5. Data analysis
The collected data were analyzed using the SPSS version 26.0 program.
First, we calculated the general characteristics of the subjects, real numbers, percentages, means, and standard deviations.
Second, the pre- and post-test differences in the subjects' subjective job performance and objective job performance in air transportation were analyzed using the Wilcoxon Signed-Rank test.
Third, we used Cronbach's alpha coefficient to test the reliability of the research instrument.
3.3. Ethical considerations
To protect the rights of participants in this study, we received two Institutional Review Board (IRB) approvals (1) for program development and (2) for program application (WKIRB-202107-SB-049, WKIRB-202109-HR-067).
Participants were informed that they could discontinue participation at any time and without penalty, that the data collected would be anonymous, and that the survey and results would not be used for any purpose other than the research.
4. Results
4.1. Developed a training program for doctor helicopter air transport work
The development of a Doctor Helicopter Air Transport Training Program to improve the performance of doctor helicopter air transport work was based on Kolb's ELT and developed according to the instructional design RPISD. In the development process, design and prototype development were executed simultaneously, including the initial analysis phase. In the analysis phase, the educational needs of emergency medical workers were analyzed, job duties of air transport were analyzed, and domestic and foreign doctor helicopter education programs were evaluated. In the design and development phase, the first prototype was proposed through instructional design, and the final program was derived after several usability evaluations.
4.1.1. Analysis phase
- Training Needs Analysis
After analyzing the contents of the interviews conducted with eight people, including two doctors, three nurses, and three paramedics, three categories were identified: education, manpower, and policy. The sub-components of education are 'curriculum,' 'teaching method,' and 'teaching topic'; the sub-components of manpower are 'individual competence' and 'teamwork'; and the sub-component of policy is 'quality control.'
In the curriculum sub-category, it was stated that a specialized curriculum for medical personnel is needed and that systematic and standardized training is needed to help them perform air transport in various situations. As for the training method, it is necessary to provide timely and quality medical services to emergency patients, and if the treatment is not done properly, it can be fatal to the patient, so high-quality training is required for various scenarios and variables. When designing the overall training program, they preferred hands-on training methods rather than theoretical lectures, and a classroom method that shares helicopter transfer cases to discuss what went well and what went wrong was needed. As for the training topics, the need for theoretical lectures to provide basic knowledge about the disease groups transported by medical helicopter and standardized treatment manuals according to the disease groups was raised. In addition, regarding teamwork with other professions, training needs were identified for elements necessary for team-based work. Regarding helicopters, the importance of helicopter safety training prior to emergency air transport training was pointed out, including training on helicopter structure, helicopter medical equipment, aerophysiology, aviation safety, flight control, and communication systems as required by the detailed guidelines of the Doctor Helicopter [22].
In the workforce category, the sub-components of individual competence and teamwork were identified. In terms of individual competence, the respondents said that they mainly learned how to do things by studying on their own, accumulating experience through trial and error, and learning from their colleagues' actions and explanations. The need for teamwork among emergency medical technicians for first aid in the helicopter and teamwork with other professions for emergency patient care and safe transportation in the field was identified. They pointed out that it is difficult to solve the problems of team-based work through one-way education in the form of knowledge transfer, and that experiential learning through simulation activities is necessary.
A sub-component of the policy category, quality management, was identified. The Central Emergency Medical Center expressed the need for a helicopter and financial support to train the hospitals where the doctor's helicopter is deployed to ensure quality management for emergency medical workers who regularly perform air transport. In addition, it was confirmed that it is necessary to issue a certificate of completion through the establishment of a curriculum to establish it as a field of medical care. It was suggested that national efforts should be made to develop and provide timely and level-specific training programs to manage the quality of air transport services and to establish doctor's helicopters as a field of the emergency medical system.
As shown above, although the current collective training of doctor helicopter passengers is necessary as the most basic level of introductory training that requires collaboration with other professions, it has been confirmed that it is insufficient to perform doctor helicopter air transport work by completing this course alone.
- 2.
- Job Analysis of Doctor Helicopter Air Transfer Work
The job analysis was conducted by applying the Daycom technique with four emergency medical technicians in a doctor's helicopter, two experts in the operation of a central emergency medical center, and one nursing professor with experience in job analysis. As a result of the job analysis, emergency report situation management, severity classification, establishment and maintenance of cooperative relationships, patient assessment, first aid, utilization of evaluation equipment, medical record keeping, document management, and safety accident management were analyzed in order, and the above factors were included in the development of a training program for doctor helicopter air transport.
4.1.2. Initial Prototype Design and Usability Evaluation
Based on the analysis of educational requirements, job analysis of air transport work, and review of domestic and foreign doctor helicopter training programs, the topics of Choi's program were constructed to reflect the requirements through job analysis. Using the step-by-step daily aviation team tasks presented in the detailed guidelines for doctor helicopters [22], the topics and detailed educational contents of the doctor helicopter air transport training program were organized, and teaching strategies suitable for each training program were established, and teaching methods were selected to effectively implement them. The first prototype consisted of a one-day, two-night blended learning training program that combined online theory lectures and offline simulation training for a total of 10 sessions.
Meanwhile, an expert team was organized to check the content validity of the initial prototype content, the effectiveness of the training method, and the appropriateness of the training period. The expert team consisted of 8 members, including 2 doctors, 3 nurses, and 3 paramedics who are emergency medical personnel who perform air transportation. The expert content validation was conducted to verify the content of the initial prototype designed based on the training needs analysis. As a result, the experts provided the following opinions, which were reflected in the development of PrototypeⅠ.
First, in organizing the training contents, it is necessary to add essential training topics that emergency medical workers must complete in the detailed guidelines for doctor helicopters [22], perform online tasks related to doctor helicopters, practice stretcher lifting, simulate patient transfer from the dispatch stage to the patient's handover, and manage infection control in the field and infection control for asymptomatic suspected patients.
Second, for the effectiveness of the training method, it is necessary to change the training method of the third dispatch phase I, which is to receive the dispatch request and perform precautions when dispatching, to an offline team activity.
Third, regarding the appropriateness of the training period, there was an opinion that the theory lectures of orientation on the 1st, safety training on the 2nd, dispatch stage I on the 3rd, end of operation on the 9th, and completion of learning on the 10th were long and had a high proportion of online.
- Revised PrototypeⅠ and First Usability Evaluation
The revised PrototypeⅠ was developed by incorporating the experts' feedback on the first prototype. The revised and supplemented contents include, first, the addition of aviation physiology to the safety training in the second stage, team activities in two-person teams in the fourth stage, stretcher lifting practice in the seventh stage of on-site boarding and transportation, simulation of all stages of patient handover in the eighth stage, and development of a learning sheet for self-assessment. Second, in terms of the effectiveness of the training method, the offline team activity was incorporated in the third dispatch phase I. Third, concerning the appropriateness of the training period, the training time for online theory lectures was revised and supplemented to 30 minutes, and offline simulation training time to 50 minutes.
PrototypeⅠ, modified to reflect the relevance of expert content, consisted of a total of 10 sessions, with orientation in the first session and safety training in the second session comprising 30 minutes of online lectures each, and the end of operation in the ninth session and the completion of learning in the tenth session comprising 20 minutes of online lectures each. The third and fourth dispatch stages were assigned to offline team activities for 30 minutes each, and the fifth and sixth field medical stages, on-site boarding and transportation, and the eighth patient accounting were modified to offline small group discussions and team activities for 50 minutes each.
To evaluate the appropriateness of the completed PrototypeⅠ, a usability evaluation was conducted with a total of 10 people, including 2 doctors, 4 nurses, and 4 paramedics, who are currently practicing air transport. The content validity evaluation was measured on a 4-point scale based on the criteria proposed by Lynn (1986), with 4 points for "very relevant and concise," 3 points for "relevant but needs some modification," 2 points for "unable to assess relevance without modifying the question," and 1 point for "not relevant," and comments were recorded on the modifications if necessary.
Content validity was evaluated by calculating the Content Validity Index for items (I-CVI) for each item and the Content Validity Index for scales (S-CVI) for all items. Items with an I-CVI of 0.8 or more were considered valid [24], and items with an I-CVI of less than 0.8 were deleted, modified, or supplemented to reflect the opinions expressed. The S-CVI was considered valid when it was 0.9 or higher [25].
Of the 10 lessons, the I-CVI for lessons 1 through 9 was 1.00, and the final lesson was 0.60. We believe that the low score is due to the unfamiliarity of action plan writing, and we included it without deleting it after gathering opinions from education experts that action plans are an ideal way to organize learning through image training.
After the usability evaluation, the aspects that needed to be modified were as follows: orientation and safety training were combined into an online lecture in the first stage; diagnostic evaluation of the doctor's helicopter was conducted after the safety training; the role of emergency medical providers in the pre-hospital stage was explained in the fifth stage of field medicine I; instructor observation evaluation and self-evaluation were conducted in the simulation of air transport work in the patient area in the seventh stage; guidance on how to use the document management and flight management system in the end-of-operation stage was provided in the eighth stage; and an action plan for the completion of learning was created in the ninth stage, which was modified and supplemented in PrototypeⅡ by accepting the opinion that it was necessary to modify.
- 3.
- Revised Prototype I and Second Usability Evaluation
The development of Prototype Ⅱ emerged from the feedback gathered on Prototype Ⅰ from experts. The restructured Prototype Ⅱ was organized into nine sessions. The initial session featured a 30-minute online lecture for orientation and safety training. The subsequent sessions, second and third, were structured as 30-minute offline team activities focused on preliminary learning and preparation for treatment during the dispatch phases I and II. On the 4th day, on-site medical care I included a 50-minute online theory lecture serving as a preliminary study of major transport disease groups, and on the 5th day, on-site medical care II entailed a 30-minute offline lecture to help recognize the role of emergency medical providers in the pre-hospital stage. The teaching methodology for the 6th session, on-site boarding and transportation, was refined and augmented with team activities and lectures. In the seventh session, patient accounting was enhanced with performance evaluation to allow both instructor and self-evaluation when executing air transportation duties. During the end-of-flight phase, a 30-minute offline lecture was organized to cover infection control and guidance on utilizing the flight management system. The final, 9th session was structured as a 30-minute offline discussion for lecture evaluation and reflection.
A secondary usability evaluation was administered, involving a total of 15 participants including 4 physicians, 5 nurses, and 6 paramedics who are currently engaged in air transport, to assess clinical relevance. The evaluation utilized the "Principles of Curriculum Content Selection and Organization" tool, post-approval from the original authors, and was measured on a 5-point scale (1='completely disagree', 5='strongly agree'), with participants afforded the liberty to freely express their opinions on each statement.
The usability evaluation of Prototype Ⅱ was ascertained through content selection criteria and organizational principles. The mean scores for the content selection criteria and organizational principles were 4.0±0.56 and 3.9±0.68 out of 5, respectively. Within the sub-areas of the content selection criteria, content significance and content balance scored below 4.0, whereas content validity, content usefulness, content learnability, content affordability, and both internal and external relevance scored above 4.0. For the sub-domains of the organizational principles, the scores were 3.9±0.74 for affiliation, 3.9±0.89 for continuity, and 3.9±0.60 for integration.
Post usability evaluation, certain areas identified for modification were revised and supplemented based on the feedback received. These included standardization of the dispatch request receipt record in the second dispatch stage I, development of a checklist for essential medical equipment, supplies, and medications required for dispatch preparation, and the requirement for a standardized manual according to the transport disease group in the fourth field medical stage I. The course was structured to transition to the simulation stage following online lecture learning, based on the dispatch order, aiming to ensure continuity in the learner's experience by fostering linkages between air transport tasks. Additionally, efforts were made to secure integration by organizing the concepts of 'air transport' and 'nursing' horizontally, and integrating them to learn 'air transport tasks' from a fresh perspective.
4.1.3. Develop the final training program (Doctor Helicopter Transport Training Program: Dr. HTTP)
The final Dr. Helicopter air transport training program was named Dr. HTTP. Dr. HTTP consisted of two stages of online theory lectures and offline simulation for a total of 8 sessions. Phase 1 consisted of two 30-minute online theory lectures on the topics of 'Orientation and Safety Education' and 'Field Medical I'. Phase 2 consisted of 6 offline simulations of 30 to 50 minutes each, covering 'Dispatch Phase I and II', 'Field Medical II', 'Onsite Boarding and Transfer', 'Patient Handover', and 'End of Operation', and the training contents for each session are as follows:
Session 1: Orientation and safety education consisted of program introduction, safety education, and infection control education.
Session 2: Dispatch phase I, after providing the virtual scenario, directly receives the dispatch call and creates a dispatch receipt record to identify patient assessment, severity classification, first aid, and the need for dispatch.
Session 3: Dispatch phase II consisted of sharing the dispatch authorization and preparing the necessary medications, medical equipment, and medical supplies with the identified patient information to board the helicopter.
Session 4: Field Medical Care I consists of theoretical lectures to help conceptualize each major group of infectious diseases by establishing four standardized treatments: clinical, patient assessment, first aid and procedures, and precautions for first aid.
Session 5: On-Site Care II was devoted to answering questions and providing feedback on the previous online lectures and training in the role of a prehospital emergency medical care provider.
Session 6: Scene Boarding and Transfer consisted of learning and practicing the mobility movements to consider when boarding patients, and collaboration with other professions.
Session 7: The patient system is the performance evaluation stage, which includes the provision of an objective performance evaluation table to assist the instructor in observational evaluation, a learning sheet to evaluate the learner's subjective performance, observational evaluation during the performance, and self-evaluation after the performance. Lecture, discussion, quiz, practice, and debriefing were selected as the main teaching and learning methods.
Session 8: The end of the flight was organized by selecting the teaching method of team activity, including how to create document management and mandatory records, guidance on how to use the flight management system, action plan creation, overall discussion and lecture evaluation.
The details of the final Doctor Helicopter Air Transport Training Program are shown in the Table 3.
4.2. Applying the Doctor Helicopter Air Transport Work Training Program
4.2.1. Performing Dr. HTTP
The composition of Dr. HTTP is based on Kolb's ELT to strengthen the job performance capabilities of doctor helicopter emergency medical personnel, and it is differentiated from previous training programs by being composed of practice-oriented sessions, unlike previous training programs that only transmit knowledge.
A preliminary evaluation of Dr. HTTP was conducted with 11 emergency physicians with at least two years of experience in the emergency department who had never been on a helicopter, using a combination of online and in-person training.
For the online training, the first and fourth batches were invited to go online for two pre-agreed training sessions during the period from September 17 to September 23, 2021. The first session was an online lecture for the first period. The main contents were orientation and safety education, including the procedure of the training program, introduction of the Dr. Helicopter business, safety education, and infection control. In the second and fourth sessions, theoretical lectures were given on on-site medical care I, including clinical features of major transport disease groups, patient assessment, first aid and procedures, and precautions for first aid. Participants were guided to create a first aid plan based on transportation cases. For those who were unable to attend the online training at the scheduled time, a video recording of the training was provided. After participating in the first and fourth online lectures, a diagnostic assessment was conducted to evaluate the level of understanding of the theoretical lectures, and then they were invited to participate in offline practical training.
For the offline training, three teams were formed with three to four people per team. From October 1 to October 17, 2021, a total of 3 practical training sessions were conducted at the mooring of the Dr. Helicopter at W University Hospital. All three teams performed the duties of the detailed guidelines in the same way, step by step, and then conducted a performance evaluation at the patient handover stage on the 7th day.
In the second stage of dispatching, users were asked to answer a real dispatch call after three rings to enhance realism. The calls presented the situation of various reporting organizations such as the 119 dispatch center, hospital, and coast guard. While filling out the dispatch log, the subjects were able to communicate with related agencies, perform patient assessments, and figure out what to request. The second step of the process was completed when the dispatcher said, "We're on our way" and hung up the phone. The completed call logs were presented to the team members for feedback, as well as feedback from the instructor on whether the team members understood all the necessary elements of a call log. A 50-minute team activity training was conducted to guide the team members on the precautions for receiving and dispatching dispatch requests.
The third period was a 50-minute offline team activity in which teams were asked to identify the patient's current condition based on the scenario in the second period and verbally describe what medications, medical equipment, etc. are needed to treat the patient while filling out a checklist. After preparing the necessary medicines, medical equipment, and medical devices from the warehouse and boarding the plane, the participants were asked to explain why they chose the medicines, medical equipment, and medical devices. Feedback from the instructor and peers concluded the 50-minute training.
The fifth session introduced the roles of pre-hospital emergency medical providers and provided an opportunity to summarize the roles of doctor helicopter air transport workers. After learning about the major groups of transported diseases in the 4th session, the offline lecture was held for 30 minutes to answer questions and provide feedback on the online lecture.
In the 6th session, we learned about the transportation routes to consider when boarding the field, and provided videos of best and worst practices to discuss before the team activity. Afterward, we conducted a 50-minute team activity to load a patient on a mobile stretcher and board the patient on a doctor's helicopter. The situation was changed so that the team could be exposed to various environments such as field transportation and hospital transportation.
The seventh session is the patient handover stage, which is the process of performing all stages of air transport work from dispatch reception to patient handover. Evaluation sheets were provided to evaluate the subjects' job performance, and the subjects conducted self-evaluation after the performance was completed. We wanted to strengthen communication through patient handover to the doctor waiting at the hospital. The instructor's feedback was based on the air transportation objective performance evaluation sheet observed by the instructor.
At the end of the 8th session, the students learned how to use the flight management system and how to fill in the mandatory records. At the end of the lesson, the learners were evaluated on their overall performance in the action plan. After the end of the situation, learners had the opportunity to self-reflect on the nursing activities of the scenario case by writing self-reflection and learner action plan, and provided a debriefing process through peer feedback and discussion in the debriefing room between learners, instructors, and researchers. Finally, they presented, shared, and summarized their impressions of the program in front of their teammates. Dr. HTTP was composed of various topics and teaching-learning methods to improve successful patient transfer and job performance, and it was confirmed that it was composed of practical contents that can help emergency medical workers directly in clinical practice.
4.2.2. Evaluation of Dr. HTTP
- 1.
- General Characteristics of the Recipients
A total of 11 subjects participated in this study, comprising 5 males (45.5%) and 6 females (54.5%), with an average age of 28.91±4.35 years. Their occupations were divided between paramedics 7 (63.6%) and nurses 4 (36.4%), and their educational backgrounds were categorized as diploma 6 (54.5%), bachelor 3 (27.3%), and master 2 (18.2%). The average total clinical experience was 53.73±50.51 months, and the average emergency department experience was 43.82±30.32 months. All 11 participants in the study agreed that there is a need for a doctoral helicopter training program for emergency medical personnel. The details are shown in the Table 4.
- 4.
- Hypothesis Testing
Hypothesis 1: Subjects' subjective job performance will be higher after applying Dr. HTTP than before applying Dr. HTTP. As a result of applying Dr. HTTP, the average subjective job performance of air transportation after training was 47.63±7.20 points compared to the average subjective job performance of air transportation before training was 37.18±8.34 points, which is a statistically significant difference (Z=-2.94, p=.003), so the first hypothesis was accepted.
The mean score of the pre-training air transport subjective job performance was 1.73±0.47 for question 8, "I can act as a researcher to build a scientific basis for pre-hospital care interventions," and the mean score of question 7, "I can hand over patient information in air transport," was 3.18±0.41.
After the training, the mean score of subjective job performance in air transport was 2.55±0.69 for item 8, "I can act as a researcher to build a scientific basis for prehospital care interventions," and the mean score of item 7, "I can hand over patient information in air transport," was 3.91±0.30.
However, statements 3, "I can perform prehospital care according to an intervention plan appropriate to the patient's condition in air transport," 9, "I can serve as an educator for patient, community, and other provider education," and 12, "I can serve as a counselor to enhance communication between agencies and facility personnel in air transport," were not statistically significant. Table 5 describes the subjective job performance for air transportation work.
Hypothesis 2: Subjects' objective job performance in air transportation will be higher after applying Dr. HTTP than before applying Dr. HTTP.
As a result of applying Dr. HTTP, the mean of objective job performance in air transportation after training was 37.72±1.49 compared to the mean of objective job performance in air transportation before training was 29.81±2.63, which was a statistically significant difference (Z=-2.94, p=.003), so the second hypothesis was accepted.
Prior to the training, the mean score for objective performance of air transport tasks was 1.00±0.87 for question 3, "Share additional information about the patient using the communication equipment in the helicopter," and 1.73±0.46 for question 12, "Check the patient's vital signs, consciousness, etc. and apply patient monitoring devices," which was the highest.
After the training, the mean score of the objective performance of air transport work was 1.23±0. 69 for item 3, "Share additional information about the patient using the communication equipment in the helicopter. It was the lowest at 1.23±0.69, followed by items 5, "Select a first aid kit and necessary medical equipment and move it to the patient safely," 7, "Perform necessary treatment as directed by the doctor," 12, "Check the patient's vital signs, consciousness, etc. and apply patient monitoring devices," 16, "Move the patient safely using a stretcher and organize medical treatment equipment, The mean score for item 18, "Access the flight management system and complete the air transport logbook" and item 20, "Perform post-flight infection control and check the charging and operating status of medical equipment" was 2.00±0.00.
However, question 3, "Share additional information about the patient using communication equipment in the helicopter," question 6, "Check the patient's condition, check the applied medical treatment devices and medical equipment," and question 11, "Check medical equipment and residues, organize medical equipment and first aid kit," were not statistically significant. Table 6 shows the ojective job performance for air transportation work.
5. Discussion
This study was conducted to develop and evaluate Dr. HTTP for first responders. The main results of this study, divided into the development and application phases of the program, are discussed below.
First, the program development stage was executed through a three-step process of analysis, design and usability evaluation, and development according to the RPISD. Initially, in the analysis phase, to improve the reliability of the educational program content, the analysis was based on the analysis of educational needs, job analysis for selecting educational topics, and literature review of domestic and foreign medical helicopter education programs. Dr. HTTP was developed based on the analysis of educational needs and job duties of doctor helicopter emergency medical personnel, who actually perform air transport duties such as dispatch reception and dispatch, operation to the scene, on-site medical care, on-site boarding, and patient transfer to the deployment hospital. It can be seen that it is differentiated from the simulation training program [26], which includes fragmented training contents, as it consists of practical training contents that encompass all seven steps of the patient handover mission after arriving at the hospital.
Then, in the design and development phase, we utilized the contents of the analysis phase to develop a prototype, set educational goals, and established teaching and learning methods. Additionally, the final educational program was developed through one expert content validity and two usability evaluations of the prototype. The prototype design and usability evaluation stages stated specific goals for the program and designed educational contents, teaching models, learning processes, and teaching and learning methods to achieve the goals, as well as evaluation methods to verify the effectiveness of the program. Generally, RPISD's prototype design is done through learner needs analysis, job analysis, and expert focus group interviews, so this study also collected opinions through the needs analysis of emergency medical workers, job analysis of step-by-step daily flight team tasks presented in the detailed instructions of the doctor's helicopter, and expert focus group interviews in the field of emergency medicine. In this study, the prototype was designed by systematically considering the medical situation in the field and actively reflecting the educational needs of learners. This was similar to the results of a previous study that developed a training program for health coaching professionals using RPISD [27] and a study by Kim, et al. [28] that developed an online training program for health checkups.
Finally, in the development stage, we developed a combined online and offline Dr. HTTP based on content relevance and usability evaluation. The rationale for developing online learning was to enhance the effectiveness of learning in a pandemic situation where emergency medical workers have time constraints due to shift work. In a pandemic situation, online courses have advantages such as convenience, accessibility, cost savings, and time savings [29]. Considering the advantages of online lectures, it has been shown that if face-to-face classes are expanded and non-face-to-face classes are combined at the same time, the educational effectiveness increases more than if only one method is implemented [30]. Therefore, this study was organized as a blended learning teaching and learning method, which is a blended learning method to consider the current situation and increase learning effectiveness. Based on the opinions derived from the analysis, the sequence of online and offline education, the time of education, the operating hours for each time, the learning process and teaching and learning methods, and the evaluation method were specifically developed. We reflected previous studies [31-33] that blended learning, which integrates online and offline, increases the effectiveness of education in terms of flexibility, efficiency, and scalability of learning by participating in offline simulations after completing online theory lectures. Since identifying learners' characteristics and abilities in advance is a useful framework for determining teaching methods [34], this course provided a basis for an actual educational program based on blended learning.
Second, we'll discuss the application of Dr. HTTP in two phases: performing Dr. HTTP and evaluating Dr. HTTP. Initially, the implementation of Dr. HTTP is as follows. The offline simulation consisted of various teaching and learning methods such as lectures, discussions, team activities, peer learning observation, peer and instructor feedback, debriefing, reflection journals, and action plans. All the subjects practiced the medical helicopter air transport task step by step, and at the end of the step-by-step practice, the subjects received an objective evaluation of the medical helicopter air transport task. After the end of the offline simulation training, the subjects self-evaluated the subjective performance of the doctor's helicopter air transfer work.
Looking at previous studies using simulation, Lee and Shin [35] found that knowledge and performance improved after simulation training for professionals, and You and Yang [36] reported that applying virtual simulation scenarios improved job performance and problem solving, which is similar to the results of this study. Lavelle, et al. [37] found that simulation training in bleeding management improved communication and performance, and simulation in clinical education has a positive impact on skills, communication, and performance [38]. Zulkosky, et al. [39] reported that simulation training with scenario repetition improves knowledge and performance in clinical education for healthcare workers. Goldshtein, et al. [40] reported that simulation-based training has a positive impact on job performance, which is generally consistent with the results of this study.
Then, as a result of applying Dr. HTTP in the evaluation stage of Dr. HTTP, the subjective and objective job performance of air transporters increased significantly, and it was found that the developed Dr. HTTP was able to fully evaluate the job performance of air transporters. These results indicate that the customized training program fully reflected the needs of the learners despite the provision of situational scenarios and the application of training in an unfamiliar environment of a helicopter. Additionally, the subjects were able to have self-reflection and iterative learning effects [41,42] by not only directly participating in the scenario situation but also observing the performance of their fellow learners, and during the debriefing, they were able improve their conceptualization, knowledge, and skills through peer and instructor feedback.
The implications of these findings and discussions are as follows.
First, this study is expected to develop the first air transport training program using RPISD, a systematic research procedure, and to serve as a foundation for future studies to explore and validate interventions to improve the performance of emergency medical technicians performing air transport, and to serve as a basis for program development and effectiveness measurement in studies related to simulation-based learning and air transport nursing. In addition, air transport is an emerging field for nurses that requires continued research and attention.
Second, Dr. HTTP, which was developed in this study, was created including training and evaluation to improve job performance, and as a result, it was found that the job performance of emergency medical personnel performing air transport was improved. If Dr. HTTP is applied continuously and repeatedly as a clinical practice training program for emergency medical personnel performing air transport, they will be able to recognize the immediate situation when performing air transport and be proactive and active in various environments without panic, and as a result, they will be able to directly contribute to improving the survival rate of patients.
This study is a short-term study to check the job performance of emergency medical technicians in doctor's helicopter air transport through simulation in a politicized helicopter. Through simulation training, we identified the job competencies required for air transport and the role of prehospital emergency medical technicians, and we found that the job performance of emergency medical technicians in doctor's helicopter air transport was improved by improving the identified job competencies. If the effectiveness of simulation training is evaluated through repeated studies and continuous learning processes, more positive results can be obtained. In addition, it is significant that Dr. HTTP has provided a basis for the spread of air transport practice through this process.
Nevertheless, there are limitations to this study. First, the study should not be limited to the development of a one-time training program, but rather the development of specialized ongoing programs for basic and advanced training and the use of training programs for the quality management of emergency medical personnel performing air transport. Second, since this study was a one-time application of the program and was evaluated through a single-group pre-post design, future studies are needed to identify the educational effects of the training program by comparing the control group and extending the number of training sessions.
Funding
This paper was supported by Wonkwang University in 2021.
Institutional Review Board Statement
To protect the rights of participants in this study, we received two Institutional Review Board (IRB) approvals (1) for program development and (2) for program application (WKIRB-202107-SB-049, WKIRB-202109-HR-067).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Center, C.E.M. 2013 Emergency Patient Air (Helicopter) Transportation Support Project. Available online: file:///C:/Users/user/Downloads/2013%EB%85%84%20%EC%9D%91%EA%B8%89%ED%99%98%EC%9E%90%20%ED%95%AD%EA%B3%B5(%ED%97%AC%EA%B8%B0)%20%EC%9D%B4%EC%86%A1%EC%A7%80%EC%9B%90%20%EC%82%AC%EC%97%85%20%EA%B2%B0%EA%B3%BC%EB%B3%B4%EA%B3%A0%EC%84%9C[20150310145909]%20(3).pdf (accessed on September 25).
- Zhang, M.; Zhang, Y.; Qiu, Z.; Wu, H. Two-Stage Covering Location Model for Air–Ground Medical Rescue System. Sustainability 2019, 11, 3242. [Google Scholar] [CrossRef]
- Choi, H.J.; Kim, H.I. Introduction and characteristics of helicopter emergency medical services. Journal of the Korean Medical Association/Taehan Uisa Hyophoe Chi 2020, 63. [Google Scholar] [CrossRef]
- Kim, T.-y.; LEE, S.-A.; Park, E.-C.; Huh, Y.; Jung, K.; Kwon, J.; Moon, J.; Kim, J.; Kim, J.; Hwang, K. Effectiveness of the trauma team-staffed helicopter emergency medical service. Health policy and management 2018, 411–422. [Google Scholar]
- Hennelly, D.; Deasy, C.; Jennings, P.; O'Donnell, C.; Masterson, S. The Development of Helicopter Emergency Medical Services in the Republic of Ireland. Air Medical Journal 2023, 42, 150–156. [Google Scholar] [CrossRef]
- Bronfman, A.; Beneventti G, D.; Alvarez, P.P.; Reid, S.; Paredes-Belmar, G. The Casualty Stabilization–Transportation Problem in a Large-Scale Disaster. Sustainability 2022, 14, 621. [Google Scholar] [CrossRef]
- Strohmandl, J.; Tomek, M.; Molnár, V.; Jakubčeková, J.M.; Fedorko, G.; Maláková, S. Using travel times for optimization numbers of medical rescue service points—case study from Slovakia. Sustainability 2020, 13, 207. [Google Scholar] [CrossRef]
- Ruan, J.; Chan, F.T.; Zhao, X. Re-planning the intermodal transportation of emergency medical supplies with updated transfer centers. Sustainability 2018, 10, 2827. [Google Scholar] [CrossRef]
- Lee, M.; Ahn, Y.M.; Cho, I.; Sohn, M.; Lee, M.; Ahn, Y.; Cho, I.; Sohn, M. Effectiveness of Simulation Integrated with Problem Based Learning on Clinical Competency and Self-efficacy in Nursing Students. Child Health Nursing Research 2014, 20, 123–131. [Google Scholar] [CrossRef]
- Center, C.E.M. Collective training for emergency medical helicopter occupants. Available online: https://edu.nemc.or.kr/main.do# (accessed on.
- Lee, Y.H.; Kim, B.S. Applications of experiential learning theory to graduate medical education. Korean Medical Education Review 2009, 11, 11–20. [Google Scholar] [CrossRef]
- Lim, C.; Song, Y.; Hong, S.; Park, C. A study on the application and improvement of the Rapid Prototyping to Instructional Systems Design (RPISD) model. Journal of Educational Technology 2020, 36, 589–617. [Google Scholar] [CrossRef]
- Zemke, R.; Rossett, A. A hard look at ISD. Training 2002, 39. [Google Scholar]
- Lim, C.; Kim, M.; Kim, Y. A developmental study on the paper-based rapid prototyping methodology for Web-based Instruction. Journal of Educational Technology 2005, 21, 3–28. [Google Scholar] [CrossRef]
- Kolb, D.A. Experiential learning: Experience as the source of learning and development; FT press: 1984.
- Kim, J. A Qualitative Study on Self-directed Learning Process In the Enterprises : Based on Kolb's.
- Experiential Learning Theory. Hanyang University, 2021.
- Su, C.-H.; Cheng, T.-W. A sustainability innovation experiential learning model for virtual reality chemistry laboratory: An empirical study with PLS-SEM and IPMA. Sustainability 2019, 11, 1027. [Google Scholar] [CrossRef]
- Hsu, T.-C.; Abelson, H.; Lao, N.; Chen, S.-C. Is it possible for young students to learn the AI-STEAM application with experiential learning? Sustainability 2021, 13, 11114. [Google Scholar] [CrossRef]
- Chen, C.-C. Effects of flipped classroom on learning outcomes and satisfaction: An experiential learning perspective. Sustainability 2021, 13, 9298. [Google Scholar] [CrossRef]
- Urquidi-Martín, A.C.; Tamarit-Aznar, C.; Sánchez-García, J. Determinants of the effectiveness of using renewable resource management-based simulations in the development of critical thinking: An application of the experiential learning theory. Sustainability 2019, 11, 5469. [Google Scholar] [CrossRef]
- Hertzog, M.A. Considerations in determining sample size for pilot studies. Research in nursing & health 2008, 31, 180–191. [Google Scholar]
- Welfare, M.o.H.a. Basic and detailed guidelines for emergency medical helicopters; 2016; pp. 1-110.
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. biometrics 1977, 159–174. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nursing research 1986, 35, 382–386. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: are you sure you know what's being reported? Critique and recommendations. Research in nursing & health 2006, 29, 489–497. [Google Scholar]
- Lee, J.I.; Lee, K.H.; Cha, K.C.; Cha, Y.S.; Kim, O.H.; Kim, H.; Hwang, S.O. Effective medical training courses for medical helicopter crews in South Korea. Journal of The Korean Society of Emergency Medicine 2013, 24, 353–361. [Google Scholar]
- Lim, C.-I.; Yeon, E.-K. Corporate Education Program Development and Teaching System Design; Education Science History: Paju, Republic of Korea 2015. [Google Scholar]
- Kim, E.-H.; Kim, K.-H.; Bae, K.-E. Development of Online Continuing Education Courses on National Health Examination for Community Health Nurses: Using the Rapid Prototyping Method. Journal of Korea Academia-Industrial cooperation Society 2019, 20, 250–263. [Google Scholar]
- Park, J.-J. The future of flexible learning and emerging technology in medical education: reflections from the COVID-19 pandemic. Korean Medical Education Review 2021, 147–153. [Google Scholar] [CrossRef]
- Ku, J.-H.; Choi, W.-S. Development and Application of Blended Learning Strategy for Collaborative Learning. Journal of the Korean Institute of industrial educators 2009, 34, 267–285. [Google Scholar]
- Park, S. A development and an analysis of effectiveness of a blended learning program for enhancing parental efficacy. Soongsil University, 2014.
- Driscoll, M. Blended learning: Let’s get beyond the hype. E-learning 2002, 1, 1–4. [Google Scholar]
- Eryilmaz, M. The effectiveness of blended learning environments. Contemporary Issues in Education Research (CIER) 2015, 8, 251–256. [Google Scholar] [CrossRef]
- Lee, H. A Study on Practical Plans for Systematic Instruction in General Education at University Level. Korean Journal of General Education 2013, 7, 343–376. [Google Scholar]
- Lee, H.; Shin, S. Effects of elementary school health teachers' COVID-19 knowledge and resilience on their performance at infection control. Journal of Korean Public Health Nursing 2021, 35, 297–309. [Google Scholar]
- You, H.; Yang, B. The effects of virtual reality simulation scenario application on clinical competency, problem solving ability and nursing performance confidence. J. Korea Acad. Industr. Coop. Soc 2021, 22, 116–126. [Google Scholar]
- Lavelle, M.; Reedy, G.B.; Simpson, T.; Banerjee, A.; Anderson, J.E. Interprofessional teamwork for managing medical deterioration in pregnancy: what contributes to good clinical performance in simulated practice? BMJ Simulation & Technology Enhanced Learning 2021, 7, 463. [Google Scholar]
- Koukourikos, K.; Tsaloglidou, A.; Kourkouta, L.; Papathanasiou, I.V.; Iliadis, C.; Fratzana, A.; Panagiotou, A. Simulation in clinical nursing education. Acta Informatica Medica 2021, 29, 15. [Google Scholar] [CrossRef]
- Zulkosky, K.; Minchhoff, D.; Dommel, L.; Price, A.; Handzlik, B.M. Effect of repeating simulation scenarios on student knowledge, performance, satisfaction and self-confidence. Clinical Simulation in Nursing 2021, 55, 27–36. [Google Scholar] [CrossRef]
- Goldshtein, D.; Krensky, C.; Doshi, S.; Perelman, V.S. In situ simulation and its effects on patient outcomes: a systematic review. BMJ Simulation & Technology Enhanced Learning 2020, 6, 3. [Google Scholar]
- Jeffries, P.R.; Rizzolo, M.A. Summary report: Designing and implementing models for the innovative use of simulation to teach nursing care of ill adults and children: A national, multi-site, multi-method study. Retrieved November 2006, 10, 2011. [Google Scholar]
- Scherer, Y.K.; Foltz-Ramos, K.; Fabry, D.; Chao, Y.-Y. Evaluating simulation methodologies to determine best strategies to maximize student learning. Journal of Professional Nursing 2016, 32, 349–357. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Conceptual Framework for Research.
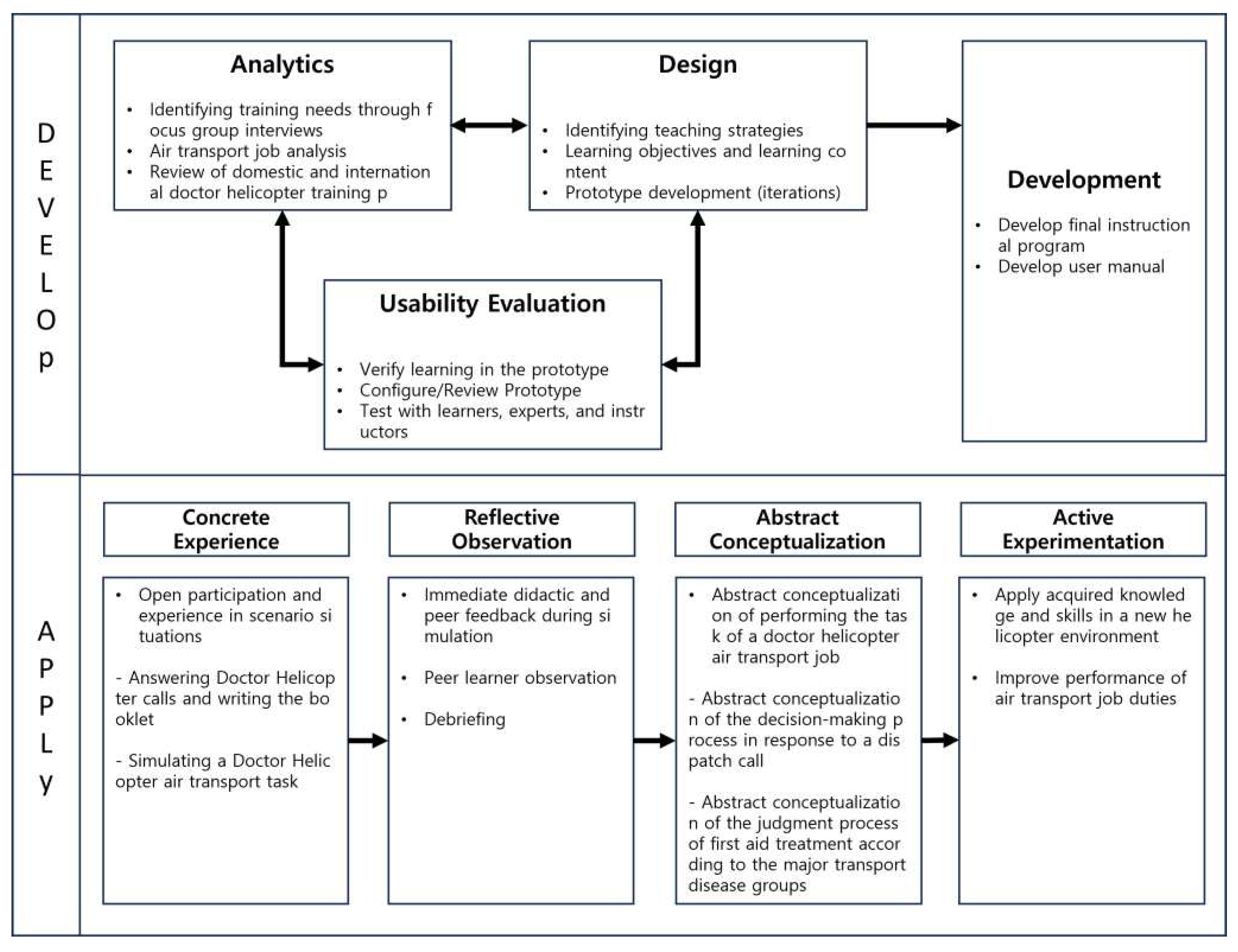

Table 1.
Overall procedure of the study.
| Step | Research Procedures | Research | ||
| Step 1 Program Development |
Analytics | ⦁Training needs analysis ⦁Job analysis of air transportation ⦁Domestic and international doctor helicopters Training Program Review |
⦁Doctor chopper for first responders Check your training needs ⦁Detailed Guidelines for Doctor Helicopter Air Transfer Job Analysis ⦁Review domestic and international helicopter training programs |
|
| Prototype design and Usability Evaluation |
⦁Initial prototype development and Feasibility assessment |
⦁Review expert content validity through interviews | ||
| ⦁Development of revised Prototype I and primary usability assessments |
⦁Usability evaluation (CVI) | |||
| ⦁Revised Prototype ⅡDevelopment and secondary usability assessments |
⦁Usability assessment (Tools - Principles of Instructional Design, Principles of Organization) |
|||
| Programs Development |
⦁Define the final training program ⦁User manual development |
⦁Develop the final training program (Dr. HTTP)* | ||
| Step 2 Apply the program |
Programs Perform |
⦁Newly developed training programs Apply |
⦁Pilot test 11 people |
⦁Provide scenarios ⦁Instructor and peer feedback, Debriefing ⦁Theory lectures, step-by-step labs |
| Programs Evaluation |
Evaluate training program effectiveness | ⦁Pre- and post-assessment of air transportation job performance | ||
Note: *Dr. HTTP (Doctor Helicopter Transport Training Program).
Table 2.
Research Design of Doctor Helicopter Air Transfer Work Training Program.
| Group | Pre-test | Moderation Apply the program |
Post-test |
|---|---|---|---|
| Experimental group |
E1 | X | E2 |
Note: E1: Preliminary investigation - general characteristics, ability to perform air transportation duties; X : Applying experimental treatment and doctor helicopter air transport training program; E2: Postmortem - Performance of air transportation duties.
Table 3.
Doctor Helicopter Air Transport Business Training Program (Dr. HTTP).
| Day | Session | Topics | Contents | Minutes | Progress | Methods |
|---|---|---|---|---|---|---|
| 1 day Tea |
1 | Orientation and Safety Eduation |
[Training Program Information] ⦁ Training objectives and methods ⦁ About the instructor ⦁ An introduction to course delivery ⦁ Introduction to the Dr. Helicopter business overview |
30* | Online | Lectures |
| [Safety training and infection control] ⦁ Introduction to Dr. Helicopter Guidelines ⦁ An Introduction to Aeronautical Physiology for Drone ⦁ Managing medical devices to prevent infectious diseases ⦁ Onsite infection control to prevent infectious diseases ⦁ Managing boarding of asymptomatic (suspected) patients to prevent infectious diseases | ||||||
| 2 | Dispatch steps Ⅰ |
[Dispatch Simulation 1. Dispatch Reception]. ⦁ Scenario provision Virtual scenario provision Learners write down the dispatch receipt Instructors provide feedback on the receipt records written by learners (whether all necessary elements for dispatch reporting have been understood) ⦁ Guidance on dispatch request receipt and points to note during dispatch |
50* | off Line |
Team Activities |
|
| 3 | Dispatch steps Ⅱ |
[Dispatch Simulation 2. Preparation for Treatment: Medications and Medical Equipment] ⦁ Gathering medications and medical equipment for the dispatch phase at the hospital based on a secondary scenario ⦁ Receive feedback from instructors and peers on their performance* |
50* | off Line |
Team Activities | |
| 4 |
On-site medical care Ⅰ |
[Learning about key boarding patient populations (1)]: Primary boarding patient population 1. severe trauma 2. acute cerebral hemorrhage 3. acute stroke 4. acute myocardial infarction 5. other emergency-like symptoms (Shock, respiratory problems) Provide a standardized care manual (classroom) |
30 | Online | Lecture | |
| 5 |
On-site medical care Ⅱ |
[Learning about key boarding patient populations (2)] ⦁ Q&A and feedback for online courses ⦁ Role as a prehospital emergency care provider* |
30 | off Line |
Lecture | |
| 6 | Field boarding and transport | [Learning about on-site boarding] ⦁ Learn about movement considerations for patient boarding: Practice lifting and moving patients ⦁ Share patient transfer stories ⦁ Guide what to expect when transferring patients |
50* | off Line |
Team Activities Lecture |
|
| 7 | Patient Takeover |
[Performance Assessment: Emergency Medical Helicopter Simulation] ⦁ Conduct performance assessments to evaluate the learner's performance by conducting a dispatch-to-handoff phase. ⦁ Rubrics to help instructors evaluate observations, and worksheets to encourage learners to self-assess. ⦁ Instructor-observed assessment during performance and, for learners, self-assessment after performance is complete |
50 | off Line |
Perform Evaluation |
|
| 8 | Flight Exit |
[End of Operation and Reflection] ⦁ Documentation and recordkeeping for the end of life phase ⦁ How to Use the Flight Management System ⦁ Create and submit an action plan based on your instructor's observations and self-assessment. ⦁ Full discussion and lecture evaluations |
50 | off Line |
Team Activities |
Note: Offline training location: W University Hospital Doctor's Helicopter Mooring; *(Boldly) Modified and supplemented the contents of Prototype Ⅱ.
Table 4.
Common audience characteristics (N=11).
| Variables | Categories | N (%) | M±SD |
| Gender | Male | 5 (45.5) | |
| Femal | 6 (54.5) | ||
| Age (years) | 28.91±4.35 | ||
| Occupation | Nurse | 4(36.4) | |
| First Aid | 7 (63.6) | ||
| Education | Bachelor of Science | 6 (54.5) | |
| Bachelor's | 3(27.3) | ||
| Master of Arts Award | 2(18.2) | ||
| Total Clinical Experience (months) | 53.73±50.51 | ||
| Emergency Department Clinical Experience (months) | 43.82±30.32 | ||
| HEMS* Training Needs | Yes | 11(100) |
Note: HEMS represents helicopter emergency medical service.
Table 5.
Subjective job performance for air transportation work (N=11).
| Contents | M±SD | Z | p | |||
|---|---|---|---|---|---|---|
| Pre-Training | After Training | Difference | ||||
| 1 | I can conduct a questionnaire and physical examination based on the patient's primary symptoms. | 2.64±0.81 | 3.36±0.50 | -.72±0.78 | -2.30 | .021 |
| 2 | I can plan interventions appropriate to the patient's condition in air transport. | 2.36±0.51 | 3.27±0.47 | -.90±0.53 | -2.88 | .004 |
| 3 | I can execute pre-hospital care according to the intervention plan in air transport. | 2.64±0.81 | 3.09±0.54 | -.45±0.68 | -1.89 | .059 |
| 4 | I can evaluate the outcomes of interventions tailored to the patient's condition in air transport. | 2.45±0.69 | 3.09±0.70 | -.63±0.67 | -2.33 | .020 |
| 5 | I am able to consult and liaise with other healthcare teams during air transport operations. | 2.36±0.81 | 3.45±0.52 | -1.09±0.83 | -2.81 | .005 |
| 6 | I can establish and maintain cooperation with other healthcare teams in air transport. | 2.45±0.69 | 3.45±0.52 | -1.00±0.63 | -2.81 | .005 |
| 7 | I am able to hand over patient information during air transport. | 3.18±0.41 | 3.91±0.30 | -.72±0.46 | -2.83 | .005 |
| 8 | I can act as a researcher to build the scientific evidence base for pre-hospital care interventions. | 1.73±0.47 | 2.55±0.69 | -.81±0.75 | -2.46 | .014 |
| 9 | I can act as an educator in providing education to patients, communities, and other providers. | 2.27±0.79 | 2.82±0.75 | -.54±0.82 | -1.90 | .058 |
| 10 | I can continue to participate in the education and training of prehospital emergency care providers to maintain my expertise. | 2.64±0.67 | 3.36±0.67 | -.72±0.78 | -2.27 | .023 |
| 11 | I can collaborate with other agencies in air transport operations to ensure scene control, mass casualty triage, and resource utilization. | 2.18±0.75 | 3.09±0.70 | -.90±0.70 | -2.64 | .008 |
| 12 | I can act as an on-site expert in scene control, mass casualty triage, and resource utilization during air transport operations. | 2.73±1.20 | 2.82±0.75 | -.09±1.04 | -.31 | .763 |
| 13 | I can act as a counselor to enhance communication between agencies and facility personnel in air transport operations. | 2.82±0.87 | 3.36±0.67 | -.54±0.68 | -2.12 | .034 |
| 14 | I can collaborate with other healthcare providers to perform and improve the care provided to patients during air transport operations. | 2.45±0.82 | 3.18±0.60 | -.72±0.78 | -2.27 | .023 |
| 15 | I can act as an advocate to protect patient rights and promote recovery and health during air transport operations. | 2.27±0.79 | 2.82±0.75 | -.54±0.68 | -2.12 | .034 |
| Total Score | 37.18±8.34 | 47.63±7.20 | -10.45±6.68 | -2.94 | .003 | |
Table 6.
Objective job performance for air transportation work (N=11).
| Contents | M±SD | Z | p | |||
|---|---|---|---|---|---|---|
| Pre-Training | After Training |
Difference | ||||
| 1 | Gather patient information and confirm airworthiness. | 1.68±0.47 | 1.95±0.22 | -.27±0.55 | -2.12 | .034 |
| 2 | Share the decision to dispatch and prepare the necessary first aid kit and medical equipment. | 1.63±0.49 | 1.91±0.29 | -.27±0.45 | -2.44 | .014 |
| 3 | Use in-flight communications equipment to share additional information about the patient. | 1.00±0.87 | 1.23±0.69 | -.22±1.26 | -.86 | .390 |
| 4 | Share patient care plan and follow physician instructions. Perform preparatory procedures for patient care as directed by the physician. | 1.27±0.55 | 1.77±0.43 | -.50±0.74 | -2.67 | .008 |
| 5 | Select first aid kit and necessary medical equipment, safely transport to the patient. | 1.59±0.50 | 2.00±0.00 | -.40±0.50 | -3.00 | .003 |
| 6 | Check the patient's condition and apply medical treatment, utilizing medical equipment. | 1.72±0.46 | 1.86±0.35 | -.13±0.56 | -1.14 | .258 |
| 7 | Perform necessary treatments as directed by a physician. | 1.55±0.51 | 2.00±0.00 | -.45±0.50 | -3.16 | .002 |
| 8 | Collaborate with rescuers to move the patient to a mobile trolley (stretcher). | 1.50±0.51 | 1.96±0.22 | -.45±0.50 | -3.16 | .002 |
| 9 | Direct patient movement and determine direction of travel. | 1.13±0.64 | 1.77±0.53 | -.63±0.84 | -2.84 | .005 |
| 10 | Organize applied medical treatment and medical equipment to safely load the patient. | 1.55±0.51 | 1.91±0.29 | -.36±0.65 | -2.31 | .021 |
| 11 | Check for medical equipment and debris, organizing the medical equipment and first aid kit. | 1.09±0.97 | 1.27±0.55 | -.18±1.22 | -.79 | .426 |
| 12 | Check the patient's vital signs and consciousness and apply patient monitoring equipment. | 1.73±0.46 | 2.00±0.00 | -.27±0.45 | -2.45 | .014 |
| 13 | Implement patient safety measures and administer medical treatment using medical equipment. | 1.50±0.51 | 1.96±0.22 | -.45±0.59 | -2.89 | .004 |
| 14 | Perform necessary treatments as directed by the physician. | 1.68±0.47 | 1.95±0.22 | -.27±0.55 | -2.12 | .034 |
| 15 | Communicate patient status and continuously check for any additional changes. | 1.59±0.50 | 1.91±0.29 | -.31±0.56 | -2.33 | .020 |
| 16 | Safely move the patient using a stretcher and put away medical supplies and equipment. | 1.32±0.47 | 2.00±0.00 | -.68±0.47 | -3.87 | .000 |
| 17 | Provide basic patient information, including demographics, treatment, and current condition to emergency medical center staff. | 1.50±0.50 | 1.95±0.21 | -.45±0.50 | -3.16 | .002 |
| 18 | Access the flight management system and complete the air transport logbook. | 1.41±0.50 | 2.00±0.00 | -.59±0.50 | -3.61 | .000 |
| 19 | Check and replenish consumed medicines, medical supplies, and oxygen. | 1.46±0.51 | 1.95±0.22 | -.50±0.51 | -3.32 | .001 |
| 20 | Implement post-flight infection control and check the charging and operating status of medical equipment. | 1.54±0.51 | 2.00±0.00 | -.45±0.50 | -3.16 | .002 |
| Total Score | 29.81±2.63 | 37.72±1.49 | -7.91±3.99 | -2.94 | .003 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



