
Submitted:
26 September 2023
Posted:
11 October 2023
You are already at the latest version
Abstract
Penile augmentation using filler injections is a growing trend; however, the foreign body reaction can cause complications such as ulcer and necrosis of the penis, which can requires reconstruction. The existing method of reconstruction of the penis focused on filling the deficit. We report a case involving a scrotal flap and autologous augmentation using a de-epithelialization technique for a soft tissue defect caused by delayed infection after a penile filler injection. The defect was reconstructed and an augmentation effect was achieved. The patient was a 41-year-old man who received an injection of Aquafilling® (Biomedica, Prague, Czech Republic) 7 years previously and developed a delayed infection. After debridement, the penile defect spanned the entire shaft, and the circumference of the penis was 7.5 cm. Using a bilateral scrotal flap technique, the inferior margins of both flaps were rolled inward after de-epithelialization to achieve autologous augmentation. No infection or flap necrosis occurred during the 3-month follow-up period after surgery. Additionally, the penis circumference was expanded to 12 cm, and the patient indicated that he was very satisfied with the result. This surgical technique can be widely applied as treatment for penile defects.
Keywords:
Penis
; Infections
; Surgical flaps
; Reconstructive surgical procedures
1. Introduction
Many men want to enlarge their penis size to increase their self-esteem and improve their ability to satisfy their sexual partners [1]. To enlarge the circumference of the penis, methods such as dermal grafting involving the groin, injectable fillers, prosthesis use, and reconstruction can increase the circumference from 0 to 4.9 cm [2]. Most men who undergo these procedures have physiologically normal penises; however, they want to enlarge their penis size for cosmetic and psychological reasons [3]. Penile augmentation is considered controversial, and there is no unanimously approved method of this type of augmentation [4]. Additionally, it may cause complications, such as asymmetry, subcutaneous nodules, ulcers, necrosis, erectile dysfunction, and decreased sensation [5].
Furthermore, penile augmentation procedures may lead to penile ulcer or necrosis and can require reconstructive surgery [6]. Local flaps may be a beneficial for tissue reconstruction according to the like-with-like principle [7]. However, reconstruction may not fulfill the needs of patients who want to enlarge their penis size. We introduce a technique involving a bilateral scrotal flap for skin defects caused by delayed infection after penile enlargement that can produce an enlargement effect.
This study was performed in accordance with the principles of the Declaration of Helsinki. The patient provided written informed consent for the publication and use of his images.
2. Case Description
A 41-year-old man without a specific medical history underwent a penile injection of Aquafilling® (Biomedica, Prague, Czech Republic) 7 years previously. No problems occurred immediately after the procedure; however, 7 years after the procedure, penile pain, swelling, fever, and pus developed. A delayed infection caused by the penile filler injection was considered (Figure 1A), and the patient underwent foreign body removal and antibiotic treatment for 4 weeks. After foreign body removal and debridement, the skin and soft tissue defects of the penis were observed (Figure 1B).
Surgery was performed using a single stage. The patient was administered general anesthesia upon request. The fibrotic tissue was removed using Versajet (Smith and Nephews, London, UK) and Metzenbaum scissors. After additional debridement, the penile defect had a circumference of 7.5 cm and a length of 5 cm over the entire shaft, and its depth reached the subcutaneous tissue level. The length of the flaccid penis was 7 cm.
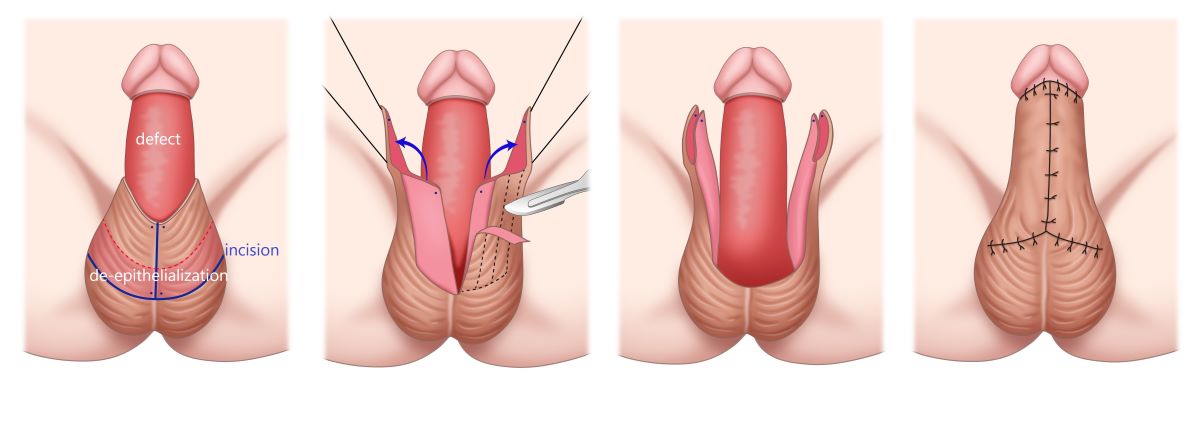
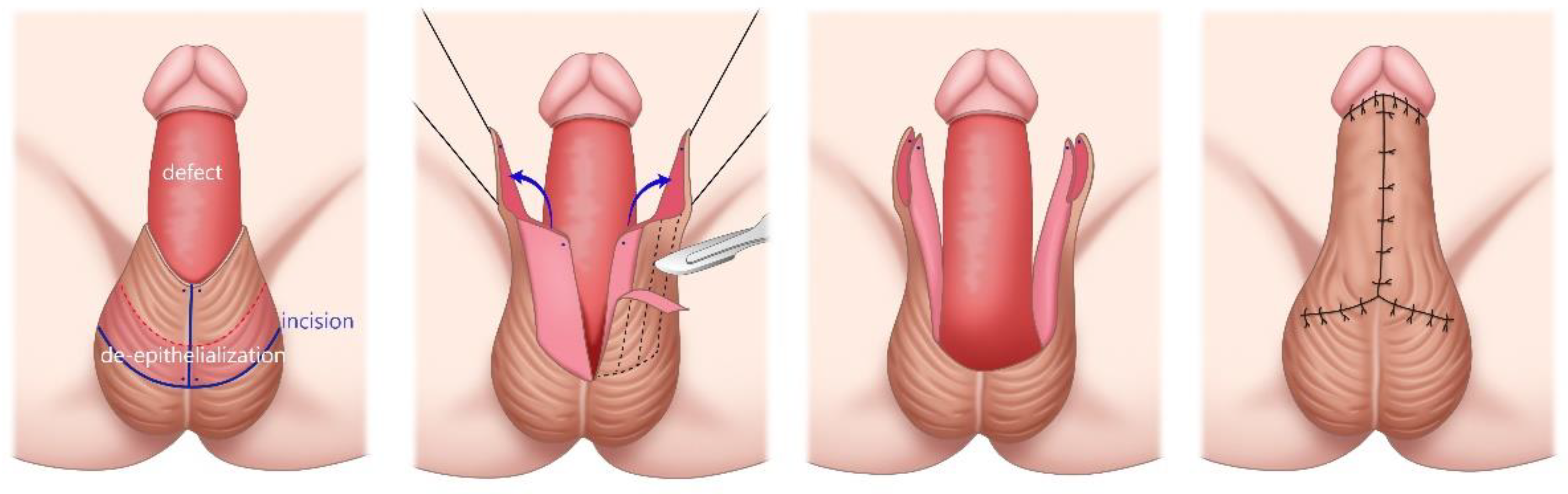
We designed an external pudendal artery-based bilateral scrotal flap to cover shaft defects. The pedicle base of the bilateral flap was designed to have a length of 5 cm and width of 9 cm. Furthermore, 4 cm of the inferior margin of the bilateral flap was designed as the de-epithelialization zone for augmentation (Figure 2A). Two rectangular flaps were carefully dissected in the subfascial plane while preserving Buck’s fascia and the dorsal neurovascular bundle of the penis.
After transposition of the both elevated flaps, the inner 4-cm edge of the bilateral flap was de-epithelialized and rolled inward to achieve the augmentation effect (Figure 3). The entire circumference of the shaft was completely covered with the bilateral scrotal flap (Figure 2B,C). A silastic drain (3ea) was placed to prevent hematoma. The donor site was primarily closed. Dressing was performed using fluffy gauze for the penile shaft and scrotum.
Three months after surgery, no skin necrosis or infection was observed at the surgical site. After surgery, the penile shaft had a circumference of 12 cm and length of 6.5 cm. The patient complained of a slight pulling discomfort during erection, and the recovery of sensation was less than before surgery. There was no pain or pressure after surgery, and there were no complaints about penile hair distribution, which is one of the disadvantages of the scrotal flap. The patient rated his satisfaction level as “very satisfied.”
3. Discussion
To the best of our knowledge, this is the only reported case involving a bilateral scrotal flap and autologous augmentation using a de-epithelialization technique for a penile defect caused by delayed infection after an injection of Aquafilling®. Pedro reported various scrotal flap methods for resurfacing the penis (scrotal flap, bilateral scrotal flap, and apron flap), but only the functional effect of defect reconstruction was mentioned; the augmentation effect was not reported [8].
Injectable fillers for the penis have not been approved by the United States Food and Drug Administration, and there are no reviews regarding the complications of penile fillers in the literature. According to the study by Namgoong [9], Aquafilling® is a hydrophilic gel that was originally developed as a dermal facial filler in 2005; however, it is also used for breast and buttock augmentation. According to the study by Shin [10], Aquafilling® comprises 0.9% sodium chloride solution (98% of the total volume) and cationic copolyimide (2% of the total volume).; it provides stable results for 8 to 10 years. Aquafilling® is a popular option that is commonly used for penile enlargement; however, there are still insufficient reports about its complications.
According to the range of penile dimensions of Chinese adult male patients, the average flaccid penile length and circumference are 8.1 cm and 8.0 cm, respectively [11]. Our patient had a penile length and circumference of 6.5 cm and 12 cm, respectively, after surgery. He reported that his results were “very satisfactory.” Until recently, the aesthetic results of penile reconstruction have been interpreted as secondary to functional results [12]. However, our new surgical technique is effective and advantageous because it provides high patient satisfaction in terms of both functional and cosmetic outcomes.
In this case, the penile defect was caused by a delayed infection that occurred after the filler injection. Penile defects can be caused by various factors, including trauma, carcinoma, infection, burns, or iatrogenic causes (such as excessive surgical resection during circumcision) [13]. Our technique can be applied for a variety of cases, including infections caused by fillers. However, more attention should be focused on thorough infection control before flap surgery.
Our findings require validation by studies involving larger patient groups and long-term monitoring. Late surgical complications, such as scarring, erectile dysfunction, and infection, should be verified by long-term follow-up. Three months after surgery, the patient experienced a slight pulling discomfort during erection, and penile sensation was slightly lower than before surgery. Additional long-term follow-up will be needed for this. This method may be suitable for patients who want a large enlargement effect. Each individual may have different degrees of desired enlargement effect, and it is necessary to accurately confirm the patient's needs before surgery.
4. Conclusions
This was a rare case of skin necrosis resulting from a delayed infection after penile augmentation with Aquafilling® that was reconstructed using a bilateral scrotal flap with autologous augmentation. Our technique could be a useful option for a variety of penile defects because it allows not only reconstruction but also cosmetic augmentation. Additionally, because the demand for penile augmentation using fillers is increasing, early recognition and appropriate management of penile filler infections are necessary.
Author Contributions
Conceptualization, W.P.; validation; B.M., H.S. and W.P ; investigation, B.M., H.S. and W.P.; writ-ing—original draft preparation, B.M. and W.P.; writing—review and editing, B.M. and W.P.; visualization, B.M.; su-pervision, W.P; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
This study was performed in accordance with the recommendations of the Institutional Review Board of Gil Medical Center, Gachon Univercity (Incheon, Republic of Korea) (IRB No. GBIRB2023-353).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflict of interest.
References
- E Dillon, B.; Chama, N.B.; Honig, S.C. Penile size and penile enlargement surgery: a review. Int. J. Impot. Res. 2008, 20, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Guo, Y.; Luo, C.; Su, X. Preliminary Application of a Novel Autologous Scrotal Dartos Flap Method for Enlargement of Penile Girth in Men with Small Penis Syndrome. Plast. Reconstr. Surg. 2022, 150, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Vardi, Y. Is Penile Enlargement an Ethical Procedure for Patients with a Normal-Sized Penis? Eur. Urol. 2006, 49, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Austoni E, Guarneri A, Cazzaniga A. A new technique for augmentation phalloplasty: Albugineal surgery with bilateral saphenous grafts–Three years of experience. Eur Urol. 2002:42, 245–253. [CrossRef]
- Khor, N.W.M.; Dhar, A.; Cameron-Strange, A. The perils of penile enhancement: case report of a fulminant penile infection. BMC Urol. 2021, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- G. Garaffa, A. G. Garaffa, A. Abdel Raheem, D.J. Ralph An up-date on penile reconstruction Asian J. Androl. 2011 May; 13(3): 391–394.
- P. Pungrasmi, A. P. Pungrasmi, A. Chayasadom, A. Angspatt Anatomical and functional outcome after bilateral scrotal flap in penile reconstruction. Asian Biomedicine. 8: 2014 Feb;8(1), 2014. [Google Scholar]
- Faveret, P.L.S.; Santiago, F. Surgical Management of Penile Lesions Secondary to Foreign Body Reaction: A Case Report and Systematic Review. Aesthetic Surg. J. 2017, 38, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Namgoong, S.; Kim, H.-K.; Hwang, Y.; Shin, S.-H.; You, H.-J.; Kim, D.-W.; Kim, A.; Jung, S.P.; Yoon, E.-S. Clinical Experience with Treatment of Aquafilling Filler-Associated Complications: A Retrospective Study of 146 Cases. Aesthetic Plast. Surg. 2020, 44, 1997–2007. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Suh, J.S.; Yang, S.G. Correcting Shape and Size Using Temporary Filler after Breast Augmentation with Silicone Implants. Arch. Aesthetic Plast. Surg. 2015, 21, 124–126. [Google Scholar] [CrossRef]
- Chung KM, A Study on the Penile Size of Korea men. Korean J Urol. 1971 Dec;12(4):401-404.
- Kolehmainen, M.; Suominen, S.; Tukiainen, E. Pelvic, Perineal and Genital Reconstructions. Scand. J. Surg. 2013, 102, 25–31. [Google Scholar] [CrossRef] [PubMed]
- W.C. Ching, H.T. W.C. Ching, H.T. Liao, B.G. Ulusal, et al. Salvage of a complicated penis replantation using bi-pedicled scrotal flap following a prolonged ischemia time J. Plast. Reconstr. Aesthet. Surg., 2010 Aug;63(8):e639-43.
Figure 1.
Preoperative clinical image. The penile defect caused by a delayed infection that occurred 7 years after the filler injection. (A) Before and (B) after foreign body removal and initial debridement.
Figure 1.
Preoperative clinical image. The penile defect caused by a delayed infection that occurred 7 years after the filler injection. (A) Before and (B) after foreign body removal and initial debridement.

Figure 2.
Intraoperative clinical images. The penile defect is reconstructed using an external pu-dendal artery-based bilateral scrotal flap. (A) De-epithelization procedure. (B) The superior side and (C) inferior side after surgery.
Figure 2.
Intraoperative clinical images. The penile defect is reconstructed using an external pu-dendal artery-based bilateral scrotal flap. (A) De-epithelization procedure. (B) The superior side and (C) inferior side after surgery.

Figure 3.
Schematic diagram of the bilateral scrotal flap with autologous augmentation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



