
Submitted:
11 October 2023
Posted:
11 October 2023
You are already at the latest version
Abstract
Introduction. Congenital muscular torticollis (CMT) is an asymmetrical head positioning resulting from structural changes in the sternocleidomastoid muscle (SCM) that occurs early in a child’s development period or due to perinatal trauma. Children with CMT exhibit a marked imbalance in tension between the SCMs. When the clinical picture is typical, an ultrasound scan is performed to reveal characteristic lesions, such as tissue fibrosis or post-traumatic changes. Early diagnosis of CMT in newborns and implementation of treatment offer the chance of a complete cure. Torticollis treatment aims to rebuild the SCM's normal function by restoring its anatomical length, normal cervical spine mobility and muscle flexibility to enable regular head movements. Surgical treatment is performed when conservative methods fail to improve the patient’s condition. Indications for surgery include marked shortening of the SCM, persistent fibrosis in the muscle, constant head and facial asymmetry, and rotation or lateral flexion in the cervical spine restricted by > 15°. After hip dislocations and foot deformities, pediatric orthopedics addresses torticollis as the third most common congenital anomaly. Aim. This study was a retrospective analysis of 111 children diagnosed and treated due to CMT. Methods. The following were determined: the relationship between the side of CMT location and the type of delivery (cc vs. natural), between the body weight at birth and the side of CMT location, between the extent of SCM thickening and the type of delivery, and the incidence of CMT depending on the order of delivery. Results and conclusions. The analysis showed that CMT was more common in boys 61(54%) than in girls 51(46%), which may be related to the greater birth weight in boys. Of the pediatric patients with CMT, 76% were primiparous. More often, children born via natural delivery had left-sided torticollis with a more significant broadening of the SCM on ultrasound scans than right-sided torticollis. Theories of torticollis development pathophysiology should be deepened, systematized, and further researched.
Keywords:
torticollis
; sternocleidomastoid muscle
; children
; perinatal risk factors
1. Introduction
Congenital muscular torticollis (CMT) is an inborn defect that involves forced and asymmetrical head positioning due to the shortening of the sternocleidomastoid muscle (SCM), most frequently unilaterally [1]. Muscle shortening is accompanied by typical morphological lesions (tissue fibrosis) as observed on ultrasonography. It can occur during prenatal development or due to perinatal trauma. Fibrotic changes result in SCM shortening and secondary mobility restriction in the cervical spine. Figure 1 shows that the infant's head tilts toward the contracted muscle and rotates the opposite side. Two types of torticollis are distinguished: the first resulting from intrauterine fetal malposition and the second following perinatal trauma accompanied by a hematoma within the SCM [2]. Bilateral torticollis is a rare type of CMT [3,4]. After hip dislocations and foot deformities, congenital torticollis is the third most common congenital anomaly among newborns and infants. Some authors prove that torticollis coexists with hip dysplasia [5,6]. Early diagnosis of CMT in newborns and implementation of treatment offer the chance of a complete cure [7]. The initiation of physiotherapy in the first few months of life contributes to the rapid regression of torticollis symptoms. CMT treatment can be conservative or surgical, depending on severity. Delayed diagnosis is accompanied by the head and cervical spine region asymmetry. Asymmetrical loads on the hip and pelvic joints can result in remote deformities. The consequences of untreated torticollis include craniofacial deformity, malocclusion, visual defects, and abnormal cervical spinal curvature [8].
1.1. Aetiology
CMT type I
Type I CMT is caused by fetal malposition [1,9]. During pregnancy, the fetal head and neck position can result in selective damage to one of the SCMs. Damage mechanisms include local crushing and ischemia, which lead to degenerative changes. Factors contributing to fetal malposition may include limited intrauterine space or low amniotic fluid levels. CMT is often observed in infants in a breech position and in primiparas, especially in cases of insufficient amniotic fluid and mechanical pressure of the uterine walls on the fetus [10]. Tissue ischemia results in muscle edema and subsequent degenerative changes, ultimately leading to muscle fibrosis.
CMT type II
CMT type II is a torticollis resulting from perinatal injury. This occurs most commonly during breech delivery or when there is a disproportion between the size of the fetus and the birth canal. Some authors believe that abnormal head tilt may cause injury to the mother’s womb due to muscle changes. The tilted head prevents proper entry into the birth canal, which causes muscle injury [11]. Other authors believe that the injury to the muscle may be due to excessive twisting of the head during its evacuation when the muscle fibers are torn, and a hematoma is formed, which subsequently undergoes resorption and fibrosis [12]. Sanerkin and Edwards supported the trauma theory and argued that traumatic and ischemic factors act simultaneously on the SCM muscle during labor. The muscle is likely stretched and locally crushed at birth, eventually leading to fibrosis [13]. However, most authors have stressed that the full pathomechanism remains unknown.
1.2. Epidemiology
The prevalence of CMT in European countries is estimated to range from 0.3% to 1.5% [14,15,16,17], whereas, in Asian countries, it ranges from 0.0084% to 3.92% [18,19]. According to Noga, congenital muscular torticollis is diagnosed in 3-5 out of 1,000 newborns [20]. At the Rehabilitation Department of the Children’s Hospital in Warsaw, Poland, from 2000 to 2018, infants with CMT accounted for 4.7% of all children aged 0–3 years receiving care.
1.3. Clinical presentation
An asymmetrical head position is characteristic of infants with CMT. The head was tilted laterally on the side of the shortened muscle and rotated with a slight extension toward the opposite side. In some cases, the flattening of the newborn skull is noticeable in the parieto-occipital region. This deformity is caused by pressure on the lambdoid suture at the end of pregnancy. Asymmetry within the trunk region is also observed. A child positions the trunk in a “C” shape, with the pelvis positioned obliquely.
Figure 1.
Characteristic asymmetrical head and trunk position in a “C” shape and oblique pelvic position during supination. Left-sided CMT.
Figure 1.
Characteristic asymmetrical head and trunk position in a “C” shape and oblique pelvic position during supination. Left-sided CMT.

Figure 2.
Characteristic asymmetrical head and trunk position in a “C” shape and oblique pelvic position in pronation. Left-sided CMT.
Figure 2.
Characteristic asymmetrical head and trunk position in a “C” shape and oblique pelvic position in pronation. Left-sided CMT.

Children with CMT exhibit a marked imbalance in tension between SCM muscles. On the torticollis side, the tension is excessive, whereas on the opposite side, the muscle fibers are stretched and weakened. In the case of CMT, the thickening and tension of the SCM muscle become palpable as early as between the second and third weeks of age. Thickening is usually observed in the central olive-shaped muscle. The palpable thickening of the SCM belly was firm, spindle-shaped, painless, and covered with healthy skin. It was most frequently located in the middle or lower third of the CMT (Figure 3). Thickening reaches its maximum size at three or four weeks of age [20]. In CMT, the range of cervical spinal mobility is typically normal. When secondary contracture of the SCM muscle occurs, examination reveals rotation restriction in the direction opposite to that of the torticollis. What is typical of CMT is the flattening of the skull in the parieto-occipital region [5,8]. This deformity is caused by pressure on the lambdoid suture at the end of pregnancy. Longer-lasting torticollis is characterized by changes that occur outside the cervical spine region. As the child grows, flattening of the parieto-occipital region and hair loss become noticeable, indicating that the deformity has persisted for a long time. Facial asymmetry also occurs over time and becomes more pronounced as children age. The face was shortened and diminished in longitudinal dimension along the forehead-chin axis on the torticollis side. In the transverse dimension, the face is widened along the nose-ear axis.
The contracted muscle is firm and tense in infants over five months, with either a narrow or wide fiber course. Occasionally, muscle fibers split peripherally into two tense bands. After age, deformities within the head and spine regions began to exacerbate. During this period, a child can move toward the torticollis, which cannot be observed in newborns; however, this movement is usually restricted. An asymmetrical head position can lead to an abnormal bite and visual development [21]. Forced misalignment of the eyeballs results in incorrect perception and processing of images [5]. The spine deforms as the cervical vertebrae adapt to flexion and become wedge-shaped [22].
Figure 4.
Head and facial asymmetry in an infant with left-sided CMT. Flattening the head in the parietal region, shortening the face on the torticollis side in the longitudinal dimension along the chin-forehead axis, narrowing the eye fissure, lowering the forehead on the torticollis, and enlarging the cheek on the unaffected side.
Figure 4.
Head and facial asymmetry in an infant with left-sided CMT. Flattening the head in the parietal region, shortening the face on the torticollis side in the longitudinal dimension along the chin-forehead axis, narrowing the eye fissure, lowering the forehead on the torticollis, and enlarging the cheek on the unaffected side.

1.4. Radiological image
The correct diagnosis of torticollis requires further examination. In cases of typical CMT, comparative ultrasound scans of both SCMs were performed. Ultrasound examination may reveal changes in the structure of the SCM in the form of muscle thickening, fibrosis, or hematoma. This image confirms the diagnosis of the muscular origin of torticollis [18,23]. Diagnosis requires classical cervical spine radiology in the posteroanterior and lateral projections when clinical imaging indicates abnormalities in the skeletal system. In case of discordance between the clinical symptoms and the additional examination results, an extension of diagnostics should include a computed tomography scan or magnetic resonance imaging.
1.5. Treatment
The treatment of torticollis aims to restore the normal function of the SCM by means of the following: restoring the anatomical length of the SCM muscle, restoring normal mobility of the cervical spine, achieving the muscle’s flexibility to enable normal movements of the head and
Restoring symmetry within the head and trunk regions. Most commonly, treatment begins with the implementation of nonsurgical methods. To date, no improvement has been recognized as the most effective method. Therapy aims to achieve flexibility, correct the length of the SCM muscle, and eliminate its thickening. The treatment results included symmetry within the head and trunk regions and normal psychomotor development for the calendar age. Surgical treatment is performed when conservative treatment fails. The essence of surgical treatment is to remove fibrosis and lengthen the SCM.
Conservative treatment
Proper physiotherapeutic management offers the possibility of a complete cure, provided that the therapy is implemented in the initial months of the infant’s life [24,25]. The most common management options include forced passive stretching of the shortened muscle and massage of the SCM [24]. These procedures aim to lengthen the affected muscles, achieve flexibility, and eliminate muscle thickening. Parental education plays a vital role in treatment. Parents learn to care for their child properly: to position, stimulate, carry, change, and feed the child. Correctional positioning of the newborn in pronation, with head rotation toward the torticollis side, was applied. This position was intended to correct SCM deformities. Parents are also taught to provide massages under home conditions. A cervical collar can maintain passive correction and outcomes achieved from exercises (Fig.3). The physiotherapeutic methods most commonly applied in CMT treatment include the NDT-Bobath and Vaclav Vojta’s methods [16].
Figure 5.
A child with right-sided CMT wearing a cervical collar.

Botulinum toxin type A (BTX-A)
In CMT, an indication for treatment using botulinum toxin type A (BTX-A) is a firm, shortened muscle that has failed to be corrected using the abovementioned methods [26,27]. Oleszek applied BTX-A to infants aged 6–18 months with CM when the physiotherapy was insufficient. Following the application of BTX-A, 74% of the infants showed improvement, 19% discontinued treatment, and 7% showed no improvement [28]. Collins also administered botulinum toxin injections to 8-month-old infants for whom therapy was proven ineffective [28]. There are reports in the literature on the effectiveness of BTX-A injections as a complementary measure to physiotherapy for treating refractory torticollis. Joyce stressed that, in many cases, the application of botulinum toxin can prevent the need for surgical intervention, but only in a situation where the SCM muscle is not fibrotic [26]. The side effects following administration of the product were mild and transient. However, Collins believed that the effectiveness of BTX-A is low and that further research needs to be conducted on the safety of botulinum toxin injections administered to infants with CMT [27].
Surgical treatment
Surgical treatment is performed when conservative methods fail to improve the condition. Indications for surgery include marked shortening of the SCM muscle, persistent muscle fibrosis, persistent head and facial asymmetry, and rotation or lateral flexion in the cervical spine region restricted by > 15° [27,29]. Most authors believe that surgery should be performed around one year of age. Surgical intervention is not indicated earlier, as most changes (approximately 90%) tend to regress after nonsurgical treatment. However, if surgery is postponed, asymmetry in the head position can lead to a sideways spine curvature [31]. However, some authors recommend performing surgery before one year of age to prevent skull deformities [31,32]. However, according to Shima, early surgery can create problems in postoperative wound management because of the easier formation of hematomas and the increased prevalence of infection in younger children. Certain authors indicate that age from 1 to 4 years is optimal for surgical intervention [33].
Figure 6.
Types of surgery used to treat children with CMT.
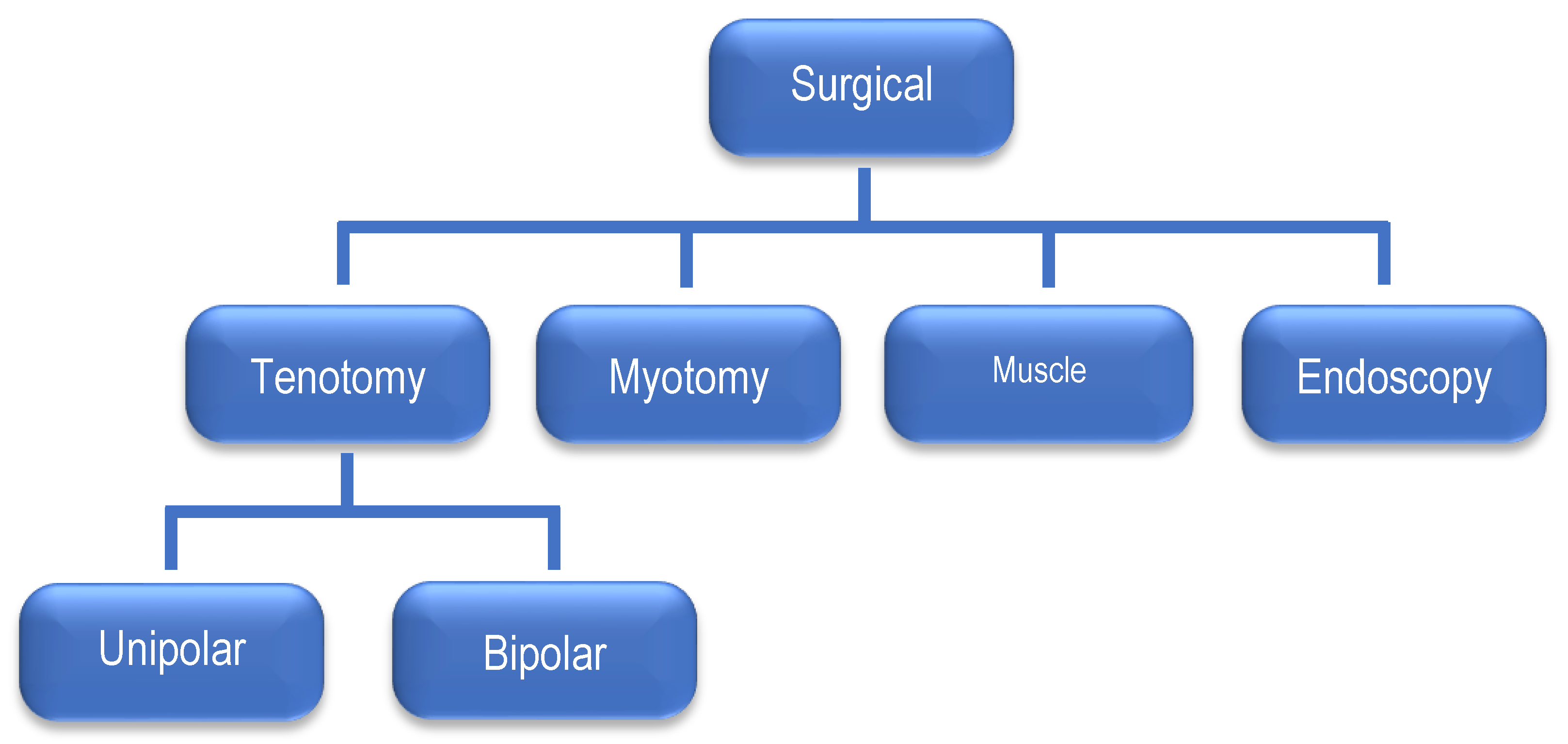
The most commonly performed surgeries are the tenotomies and myotomies of the SCM, whereas lengthening the scarred muscles is less common. Tenotomies are performed unipolar or, less commonly, by the subcutaneous method or with total exposure of tendon attachments. Unipolar tenotomy can be either upper or lower. Lower tenotomy is most widely applied and involves the release of the SCM muscle attachments on the clavicle and sternum. Upper tenotomy involves cutting the muscle near its attachment to the mastoid process. Bipolar tenotomy involves cutting the muscle near its attachment to the clavicle and sternum and near its attachment to the mastoid process. The bipolar method is used when the deformity is severe and cannot be corrected using the unipolar method. An incision was made on the wrinkled skin above the clavicle. Incisions in the clavicle or close proximity tend to widen and become unsightly. It is recommended that approximately 1 cm of the tendon be removed to prevent recurrence of deformity. A transverse myotomy was performed at the mid-length of the SCM. Muscle lengthening is carried out as the “Z” plasty technique [33,34]. Early postoperative complications include wound damage, hematoma formation, and superficial wound infections. However, late complications include scar disfigurement, scar tethering, and loss of SCM muscle contour [34]. The medical literature describes several endoscopic surgical techniques used to release the SCM. The advantages of endoscopy include its low invasiveness and minimal scarring [35]. Tang recommended endoscopic release of the SCM muscle in infants and children as young as six months of age [36]. Opinions in the literature on physiotherapeutic management after surgical treatment have been divided. Angoules believes that because recurrences occur in 1.2% of patients, an intensive physiotherapy program (including manual stretching of the SCM) is required [37]. Some authors recommend using hypercorrective head positioning after surgery, fixed with a plaster dressing, whereas others recommend a semi-rigid orthotic or cervical collar. Most authors agree with physiotherapy's advisability to remodel the cortical map's movement patterns after wound healing.
2. Materials and Methods
This study was based on a retrospective analysis of children with CMT treated at the Rehabilitation Department of Professor Jan Bogdanowicz Children’s Hospital in Warsaw, Poland, from 2000 to 2018.
2.1. Study group
The study group comprised 111 children, including 50 girls (46%) and 61 boys (54%). The group characteristics are presented in Table 1.
Thickening of the SCM was noted in all the children in the study group. Abnormal echogenicity of the SCM was diagnosed in 66 patients (76%), including 31 girls (36%) and 35 boys (40%); these changes were not noted in 21 patients (24%). The group comprised seven girls (8%) and 14 boys (16%). Of the 66 children with abnormal echogenicity, 38 had left-sided torticollis (58%), and 28 had right-sided torticollis (42%). Mobility was restricted to the cervical spine in 78 patients (70%).
In the study group, complications during delivery occurred in 35 children (33%); in 21 cases, the birth was via cesarean section (20%), ten births were via assisted natural delivery (9%), breech delivery was noted in three cases (3%), and bigeminal pregnancy was reported in one patient (1%).
2.2. The inclusion criteria for the analysis were as follows:
- 0 to 5 months of age, diagnosis of torticollis of muscular origin (bone lesions were excluded), informed and voluntary parental consent for their children’s participation in the study.
2.3. The following relationships were analyzed:
- between the side of the CMT location and the type of delivery (cc vs. natural), between body weight at birth and the side of the CMT location, between the extent of SCM muscle thickening and the type of delivery (cc vs. natural), if the incidence of CMT depends on the delivery order.
2.4. Statistical analysis
For statistical calculations, tests were applied depending on the distribution and variance homogeneity of the variables. Mann–Whitney non-parametric U tests were used when the distribution was not normal.
2.5. Ethics
All the procedures performed in this study involving human participants conformed to the ethical guidelines of the 2013 Declaration of Helsinki, as reflected in a priori approval by the institution’s human research committee. They followed the Adapted Physical Activity (APA) Ethics Standard. The protocol was approved by the Institutional Review Board (IRB) and ethics committee (Military Medical Institute, Warsaw, Poland; number 124/WIM/2018). The written informed parental consent was waived due to the characteristics of the retrospective study. The verbal assent regarding their children's participation in the study was performed. The approval was obtained from an institutional research ethics committee before recruitment, and subjects received no payment for participating in this study. The experiment was conducted with the understanding of each patient’s parent.
3. Results
3.1. Relationship between the side of CMT location and the type of delivery
In 53 (91%) cases, left-sided torticollis occurred in children born via natural delivery, and only five cases (9%) were delivered via cc. However, right-sided torticollis occurred in 37 children (69%) born via natural delivery, and 16 (31%) were born via cc.
3.2. Relationship between the birth body weight and the location of CMT
The mean body weight at birth in children with left-sided CMT was 3,674 g, whereas it was 3,274 g for those with right-sided CMT.
3.3. Relationship between the extent of the SCM muscle thickening and the type of delivery (cc vs. natural)
The thickness of both SCM muscles was analyzed using ultrasonography. The difference in the thickness of both (right/left) SCM muscles was greater in children born via natural delivery and was 6.07 mm, on average. On average, the difference in the thickness of both SCM muscles in children born via cesarean section was 4.14 mm. The average width of the left SCM in left-sided torticollis in children born via natural delivery was 13.99 mm, whereas that of the right SCM in right-sided torticollis was 8.3 mm. Of the 57 cases of left-sided torticollis in the entire study group, abnormal SCM muscle structure was noted in 38 (67%). Muscle structure abnormalities were reported in 28 (42%) of 54 cases of right-sided torticollis. In children with abnormal SCM structures, the difference in the thickness of both muscles was greater than that in children with normal SCM structures (6.15 vs. 3.79).

Table 2.
Relationship between the side of CMT location, mean body weight at birth, and the type of delivery.
Table 2.
Relationship between the side of CMT location, mean body weight at birth, and the type of delivery.
| Natural delivery | Cesarian section | Mean body weight at birth | |
|---|---|---|---|
| L-sided torticollis | 91% | 9% | 3,674 |
| R-sided torticollis | 69% | 31% | 3,274 |
Table 3.
A comparison of the SCM muscle width in an ultrasound scan with the type of delivery, the number of births, sex, and the location of torticollis expressed in millimeters.
Table 3.
A comparison of the SCM muscle width in an ultrasound scan with the type of delivery, the number of births, sex, and the location of torticollis expressed in millimeters.
| Width of R-SCM [mm] | Width of L-SCM [mm] | Difference [mm] | |
|---|---|---|---|
| Natural birth | 8.30 | 13.99 | 6.07 |
| Cesarean section | 9.39 | 17.72 | 4.14 |
| 1st birth | 8.58 | 14.94 | 5.47 |
| Next birth | 8.30 | 14.00 | 6.35 |
| Boys | 8.40 | 14.56 | 5.86 |
| Girls | 8.67 | 14.92 | 5.44 |
| L-CMT | 4.93 | 10.69 | 5.76 |
| R-CMT | 11.22 | 5.61 | 5.61 |
3.4. Incidence of CMT depending on the order of delivery
Eighty-four participants (76%) were primiparous, including 41 girls (37%) and 43 boys (39%). Twenty-seven study participants (24%) were the offspring of multiparous women, including 11 girls (9%) and 16 boys (15%).
4. Discussion
CMT is a congenital condition that disturbs children’s global motor skills [5]. It is characterized by shortening and thickening of the SCM muscle, resulting in tilting the head to the side of the torticollis with rotation towards the opposite side. CMT can be accompanied by plagiocephaly, developmental dysplasia of the hip, brachial plexus trauma, and anomalies of the feet or lower limbs [1,8]. CMTs are most often located unilaterally and seldom bilaterally. Bilateral torticollis was not diagnosed in any of the 111 patients in the study group. According to the literature, CMT is slightly more common in boys than in girls [1,23,38]. A larger head circumference and greater body weight in boys may be risk factors. Petronic et al. reported a higher CTM in boys [14]. The current study also included more boys with CMT (61, 54%) than girls (n=51, 46%). Analysis of body weight at birth revealed that boys weighed more (3,632 g) than girls (3,299 g), which may explain the higher prevalence of CMT in boys. The results of a study by Kim proved that CMT is more frequently associated with the left SCM muscle [39]. In the study group, with a small difference, there were more cases of left-sided torticollis (n=57; 51%) than right-sided torticollis (n=54; 49%). Boys more often had left-sided torticollis (58%), while in the group of girls, left-sided torticollis occurred in 24 out of 57 cases (42%). This is consistent with studies showing that right-sided torticollis is more common in girls [38]. The etiology of CMT remains unclear. Some researchers consider impaired blood supply to the SCM muscle resulting from vascular underdevelopment at early developmental stages, venous outflow obstruction, and secondary ischemia as the cause. An inadequate blood supply leads to degenerative changes and muscle fibrosis [10,40]. Most supporters of the ischemic theory agree that ischemia of the SCM results from a non-physiological position of the fetus resulting from intrauterine space restriction [40]. All children in the study group had thickening of the SCM muscle, with as many as 78 children (70%) in which mobility was restricted to the cervical spine region. The remaining 34 patients (30%) had no mobility restrictions in the cervical spine region. This appears to support Tachdjian, who proposed that changes in SCM resulted in its shortening [41]. According to this, CMT occurs due to intrauterine space restriction, and the ischemic theory appears most likely. This finding may be supported by the number of children (n=84, 76%) born during their first delivery in the study group. Since the average body weight at birth of children with CMT born in the first delivery was 3,464 g, it may be assumed that the children born in the first delivery could have had little space in the primipara’s womb.The neonatal positioning may be asymmetrical for primiparas, with the head tilted to the side, lateral rotation towards the opposite side, and the maxillary area tilted towards the shoulder. In the analyzed material, a significant relationship was observed between body weight at birth and the location of CMT (p=0.0001). The mean body weight at birth in children with left-sided CMT was 3,674 g, while that in children with right-sided CMT was 3,274 g. The analysis also demonstrated a significant relationship between birth weight and sex (p=0.0012). In the study group, boys had a greater body weight at birth than girls did. The mean body weights at birth were 3,632 g for boys and 3,299 g for girls. In the study group, there was a predominance of boys with left-sided torticollis, who were also more numerous in the more severe torticollis group. Therefore, it can be presumed that a more severe form of CMT most likely occurs in boys, most commonly in the left SCM. A statistically significant difference was observed in the study material between the extent of SCM thickening and the type of delivery (p=0.02). A greater difference in the width of both SCM muscles was noted in children born via natural delivery (average: 6.07 mm) than in those born via cesarean section (average: 4.14 mm). Of the 90 births via natural delivery in the study group, left-sided torticollis occurred in 52. Out of 21 births via cesarean section, left-sided torticollis occurred in only five cases. Therefore, 52 (91%) of the 57 patients with left-sided torticollis were delivered via natural labor. On ultrasound, an abnormal SCM structure occurred in 66 patients in the study group, with left-sided torticollis noted in 38 patients (58%). The abnormal left SCM width of cesarean children born via natural delivery was 13.99 mm, while the right muscle was 8.3 mm, on average. The greater width of the abnormal left SCM, demonstrated in the current study, appears to be consistent with reports made the formation of micro-traumas during labor conditional on SCM muscle shortening [42,43]. Therefore, children delivered via natural labor in the study group had left-sided torticollis with greater muscle broadening than those with right-sided torticollis. The current study showed that greater thickening of the left SCM could have developed during natural labor.
5. Conclusions
After hip dislocations and foot deformities, pediatric orthopedics addresses torticollis as the third most common congenital anomaly. Theories of torticollis development pathophysiology should be deepened, systematized, and further researched. Conducting observational and prospective studies on large patient groups to identify risk and prognostic factors is essential.
Our study shows that CMT occurs more commonly in boys (61; 54%) than in girls (51; 46%), which can be related to the greater body weight of boys at birth (average body weight at birth: boys, 3,632 g vs. girls, 3,299 g). Most children with CMT were primiparous (76% vs. 24%). More often, children born via natural delivery had left-sided torticollis with a more significant broadening of the SCM muscle on ultrasound scans than in right-sided torticollis.
Author Contributions
Conceptualization: P.J. and O.J.; Methodology: P.J.; Investigation: O.J.; Writing—original draft preparation: A. K-S. J.N..; Writing — review and editing: P.J.; J.N.; and K.Z.S. All the authors have read and agreed to the published version of the manuscript.
Funding
This study did not receive external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The project did not require registration. The datasets may be shared via correspondence with the authors upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Davids, J.R.; Wenger, D.R.; Mubarak, S.J. Congenital muscular torticollis: A sequela of intrauterine or perinatal compartment syndrome. J. Pediatr. Orthop. 1993, 13, 141–147. [Google Scholar]
- Sanerkin, N.G. Birth injury to the sternomastoid muscle. J. Bone Joint Surg. Br. 1966, 48, 441–447. [Google Scholar] [CrossRef]
- Matuszewski, L.; Pietrzyk, D.; Kandzierski, G.; Wilczynski, M. Bilateral congenital torticollis: A case report with 25 years of follow-up. J Pediatr Orthop B. 2017, 26, 585–588. [Google Scholar] [CrossRef]
- Babu, M.K.; Lee, P.; Mahadev, A.; Lee, E.H. Congenital bilateral sternocleidomastoid contracture: A case report. J. Pediatr. Orthop. B. 2009, 18, 145–147. [Google Scholar] [CrossRef]
- Kim, O.H.; Lee, S.W.; Ha, E.K.; Kim, J.H.; Jo, Y.H.; Rhie, S.; Han, M.Y.; Chae, K.Y. Neurodevelopmental outcomes and comorbidities of children with congenital muscular torticollis: Evaluation using the National Health Screening Program for Infants and Children database. Clin. Exp. Pediatr. 2022, 65, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Joiner, E.R.A.; Andras, L.M.; Skaggs, D.L. Screening for hip dysplasia in congenital muscular torticollis: Is physical exam enough? J Child Orthop 2014, 8, 115–119. [Google Scholar] [CrossRef]
- Carenzio, G.; Carlisi, E.; Morani, I.; Tinelli, C.; Barak, M.; Bejor, M.; Dalla Toffola, E. Early rehabilitation treatment in newborns with congenital muscular torticollis. Eur. J. Phys. Rehabil. Med. 2015, 51, 539–545. [Google Scholar] [PubMed]
- Yu, C.C.; Wong, F.H.; Lo, L.J.; Chen, Y.R. Craniofacial deformity in patients with uncorrected congenital muscular torticollis: An assessment from three-dimensional computed tomography imaging. Plast. Reconstr. Surg. 2004, 113, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.C.Y.; Tang, S.P.; Chen, T.M.; Wong, M.W.; Wong, E.M. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants - a study of 1,086 cases. J. Pediatr. Surg. 2000, 35, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Hardgrib, N. et al. Do obstetric risk factors truly influence the etiopathogenesis of congenital muscular torticollis? J. Orthop. Traumatol. Off. J. Ital. Soc. Orthop. Traumatol. 2017, 18, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Hulbert, K.F. Congenital torticollis. J. Bone Joint Surg. 1950, 32, 50–59. [Google Scholar] [CrossRef]
- Macdonald, D. Sternomastoid tumor and muscular torticollis. J. Bone Joint Surg. Br. 1969, 51, 432–443. [Google Scholar] [CrossRef]
- Sanerkin, N.G. Birth injury to the sternomastoid muscle. J. Bone Joint Surg. Br. 1966, 48, 441–447. [Google Scholar] [CrossRef]
- Kumar, N.; Mukherji, S. Congenital muscular torticollis. Annals of Maxillofacial Surgery 2013, 3, 198. [Google Scholar]
- Wei, J.L.; Schwartz, K.M.; Weaver, A.L.; Orvidas, L.J. Pseudotumor of Infancy and Congenital Muscular Torticollis: 170 Cases. The Laryngoscope 2001, 111, 688–695. [Google Scholar] [CrossRef]
- Jung, M.W.; Landenberger, M.; Jung, T.; Lindenthal, T.; Philippi, H. Vojta therapy and neurodevelopmental treatment in children with infantile postural asymmetry: A randomized controlled trial. J. Phys. Ther. Sci. 2017, 29, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Minghelli, B.; Vitorino, N.G.D. Incidence of congenital muscular torticollis in babies from southern Portugal: Types, age of diagnosis and risk factors. Int. J. Environ. Res. Public. Health. 2022, 19, 9133. [Google Scholar] [CrossRef]
- Cheng, J.C.Y.; Au, A.W.Y. Infantile torticollis: A review of 624 cases. J. Pediatr. Orthop. 1993, 14, 802–808. [Google Scholar] [CrossRef]
- Chen, M.M.; Chang, H.C.; Hsieh, C.F.; Yen, M.F.; Chen, T.H. Predictive Model for Congenital Muscular Torticollis: Analysis of 1021 Infants With Sonography. Arch Phys Med Rehabilit 2005, 86, 2199–2203. [Google Scholar] [CrossRef]
- Nogi, J. Wrodzony mięśniowy kręcz szyi. In: Pizzutillo P.: Ortopedia dziecięca. Czelej. Lublin 1997, 341-342.
- Rao, R.; Morton, G.V.; Kushner, B.J. Ocular torticollis and facial asymmetry. Binocul. Vis. Strabismus Q. 1999, 14, 27–32. [Google Scholar] [PubMed]
- Lee, J.Y.; Koh, S.E.; Lee, I.S.; Jung, H.; Lee, J.; Kang, J.I.; Bang, H. The cervical range of motion as a factor affecting outcomes in patients with congenital muscular torticollis. Ann. Rehabil. Med. 2013, 37, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.; Cheng, J.; Metreweli, C. Ultrasonography of congenital muscular torticollis. Pediatr. Radiol. 2005, 22, 356–360. [Google Scholar] [CrossRef]
- Cheng, J.C.; Wong, W.M.; Tang, S.P.; Chen, T.M.; Shum, S.L.; Wong, E.M. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants. A prospective study of eight hundred and twenty-one cases. J. Bone Joint Surg. Am. 2001, 83, 679–687. [Google Scholar] [CrossRef]
- Carenzio, G.; Carlisi, E.; Morani, I.; Tinelli, C.; Barak, M.; Bejor, M.; Toffola, E. Early rehabilitation treatment in newborns with congenital muscular torticollis. Eur. J. Phys. Rehabil. Med. 2015, 51, 539–545. [Google Scholar]
- Joyce, M.B.; de Chalain, T.M. Treatment of recalcitrant idiopathic muscular torticollis in infants with botulinum toxin type A. J. Craniofac Surg. 2005, 16, 321–327. [Google Scholar] [CrossRef]
- Collins, A.; Jankovic, J. Botulinum toxin injection for congenital muscular torticollis presenting in children and adults. Neurology. 2006, 67, 1083–1085. [Google Scholar] [CrossRef] [PubMed]
- Oleszek, J.L.; Chang, N.; Apkon, S.D.; Wilson, P.E. Botulinum toxin type A in the treatment of children with congenital muscular torticollis. Am. J. Phys. Med. Rehabil. 2005, 84, 813–816. [Google Scholar] [CrossRef]
- Pan, P. The Transaxillary Subcutaneous Endoscopic Sternocleidomastoid Muscle Division as an Approach for the Surgical Treatment of Congenital Muscular Torticollis in Children. Indian. J. Otolaryngol. Head. Neck Surg. 2020, 72, 123–127. [Google Scholar] [CrossRef]
- Lee, Y.T.; Yoon, K.; Kim, Y.B.; Chung, P.W.; Hwang, J.H.; Park, Y.S.; Chung, S.H.; Cho, S.K.; Han, B.H. Clinical features and outcome of physiotherapy in early presenting congenital muscular torticollis with severe fibrosis on ultrasonography: A prospective study. J. Pediatr. Surg. 2011, 46, 1526–1531. [Google Scholar] [CrossRef]
- Yu, C.C.; Wong, F.H.; Lo, L.J.; Chen, Y.R. Craniofacial deformity in patients with uncorrected congenital muscular torticollis: An assessment from three-dimensional computed tomography imaging. Plast. Reconstr. Surg. 2004, 113, 24–33. [Google Scholar] [CrossRef]
- Sönmez, K.; Türkyılmaz, Z.; Demiroğulları, B.; Özen, I.; Karabulut, R.; Bağbancı, B.; Başaklar, A.; Kale, N. Congenital Muscular Torticollis in Children. ORL, 2005, 67, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Jang, H.P. Operative treatment of congenital torticollis. J. Bone Joint Surg. Br. 2008, 90, 934–939. [Google Scholar] [CrossRef]
- Cheng, J.C.Y.; Tang, S.P. Outcome of surgical treatment of congenital muscular torticollis. Clin. Orthop. Relat. Res. 1999, 362, 190–200. [Google Scholar] [CrossRef]
- Wang, J.; Wei, Q.; Liu, Y. Endoscopic release of congenital muscular torticollis with radiofrequency in teenagers. J. Orthop. Surg. Res. 2018, 13, 1–10. [Google Scholar] [CrossRef]
- Tang, S.T.; Yang, Y.; Mao, Y.Z.; Wang, Y.; Li, S.W.; Tong, Q.S.; Cao, G.Q.; Li, S. Endoscopic transaxillary approach for congenital muscular torticollis. J. Pediatr. Surg. 2010, 45, 2191–2194. [Google Scholar] [CrossRef]
- Angoules, A.; Boutsikari, E.; Latanioti, E. Congenital Muscular Torticollis: An Overview. J. Gen. Pract. 2013, 1, 105–109. [Google Scholar] [CrossRef]
- Petronic, I.; Brdar, R.; Cirovic, D.; Nikolic, D.; Lukac, M.; Janic, D.; Pavicevic, P.; Golubovic, Z.; Knezevic, T. Congenital muscular torticollis in children: Distribution, treatment duration and outcome. Eur. J. PhysRehabil Med. 2010, 46, 153–157. [Google Scholar]
- Kim, M.O.; Kim, S.J. Results of the conservative management in congenital muscular torticollis. J. Korean Acad. Rehabil. Med. 1992, 16, 42–50. [Google Scholar]
- Leibovitch, L.; Kuint, J.; Rosenfeld, E.; Schushan-Eisen, I.; Weissemann-Brenner, A.; Maayan-Metzger, A. Short-term outcome among term singleton infants with intrapartum oligohydramnios. Acta Paediatr. 2012, 101, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Tachdjian, Mihrano, O. Pediatric Orthopedic Surgery. W.B. Saunders Co. Phila. 1990, 1, 112–124. [Google Scholar]
- Özkan, E.; Özkan, M.; Isik, I. Evaluation of the clinical role of strain elastography in patients diagnosed with congenital torticollis. J. Diagn. Med. Sonogr. 2021, 37, 242–246. [Google Scholar] [CrossRef]
- Wójcicki, K.; Krieger, R.; Berry, A.; Reuther, W. Fibromatosis colli spuriously presenting as a retropharyngeal mass on cervical spine radiographs. Intern. Emerg. Med. 2015, 11, 277–279. [Google Scholar] [CrossRef] [PubMed]
Figure 3.
Noticeable thickening of the SCM muscle – left-sided CTM.

Table 1.
Study group characteristics.
| N (%) | Left-sided CMT | Right-sided CMT | Mean birth weight | Birth | Term of birth | |||
|---|---|---|---|---|---|---|---|---|
| cc | natural | pre | on time | |||||
| Boys | 61 (54%) | 33 | 28 | 3632 | 10 | 51 | 1 | 60 |
| Girls | 50 (46%) | 24 | 26 | 3299 | 11 | 39 | 5 | 45 |
| Total | 111 (100%) | 57 | 54 | 21 | 90 | 6 | 105 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



