
Submitted:
11 October 2023
Posted:
12 October 2023
You are already at the latest version
Abstract
Despite Vitamin B12's recognized importance for the nervous system, there's still a lack of research on the association between Vitamin B12 and sleep, especially in primary care settings. We assessed Vitamin B12 levels in adult primary health care users and investigated correlations with sleep quality, insomnia and sleepiness. In this cross-sectional study, 512 consecutive participants were included. Information regarding anthropometrics, socio-demographics, and medical history was obtained. The Epworth Sleepiness Scale (ESS), Athens Insomnia Scale (AIS), and Pittsburg Sleep Quality Index (PSQI) were used to quantify excessive daytime sleepiness (EDS), insomnia symptoms, and sleep quality, respectively. Median Vitamin B12 was 342 (266, 446) pg/mL. After adjustments, Vitamin B12 levels<342 pg/mL showed significant associations with insomnia symptoms [OR (95% CI) 2.434 (1.331–4.452), p=0.004], especially in elderly, non-obese and female participants, with EDS only in obese participants [OR (95% CI) 3.996, (1.006-15.876), p=0.039]. Nonetheless, there was no significant association between B12 levels and poor sleep quality (OR 1.416, 95% CI 0.678-2.958, p=0.354). In conclusion, our results show that lower Vitamin B12 was associated with insomnia symptoms and sleepiness in specific groups of participants. However, further research with objective measurements of sleep is crucial to assess the relationship between sleep and Vitamin B12.
Keywords:
sleep disorders
; primary care
; vitamin B12
; insomnia symptoms
; excessive daytime sleepiness
; sleep quality
1. Introduction
Sleep health involves a complex sleep and wakefulness pattern that is tailored to individual, social, and environmental demands, with the goal of enhancing physical and mental well-being [1]. However, prior research has indicated that a significant proportion of the general population experience sleep impairment, including insufficient sleep duration, prolonged sleep latency, frequent and prolonged nocturnal awakenings, and other sleep disruptions [2-6]. Sleep impairment over time has been associated with a variety of health conditions, including metabolic and cardiovascular diseases, cancer, depression as well as greater risk of mortality [7-11]. In light of the unfavorable outcomes of sleep impairment, it is crucial to identify and explore the potential associated modifiable factors.
Recently, there has been a growing interest in the importance of diet and nutrition in relation to sleep impairment. Evidence suggests that there is a reverse connection between dietary or serum macro and micronutrients levels and sleep disturbances [12-14]. More specifically, macronutrients appear to play a role in modulating neurotransmitter levels and impacting intrinsic sleep mechanisms, ultimately influencing sleep patterns [15, 16]. Moreover, micronutrients may impact the activity of presynaptic neurons or the synthesis of sleep-regulating neurotransmitters, including serotonin, N-methyl-d-aspartate (NDMA) glutamate, and melatonin [16, 17, 18]. However, the clinical relevance of micronutrients to sleep health has received less attention, and findings regarding some micronutrients, such as B12, remain inconsistent [19].
Vitamin B12, also known as cobalamin, is a vital vitamin for the nervous system that cannot be synthesized by the body and must be obtained through dietary consumption [20]. It seems to play a crucial role in melatonin synthesis which regulates sleep rhythms with the potential to improve the sleep-wake cycle [18]. Therefore, it is a micronutrient worth considering when examining modifiable factors that are linked to sleep disturbances. However, there are few studies exploring the relationship between serum vitamin B12 and sleep health [19, 21,22]. Despite the lack of conclusive evidence in earlier studies [18, 23, 24, 25], more recent research points toward a negative correlation between serum vitamin B12 levels and sleep duration [21, 26]. Moreover, most of the research has predominantly focused on the correlation between B12 and the duration of sleep, and, overall, there is a scarcity of information regarding the impact of B12 on the quality of sleep, symptoms of insomnia, and sleepiness.
The aforementioned findings require more investigation, especially for populations without pertinent data, like Greece. Therefore, we hypothesized that vitamin B12 levels are associated with sleep quality, insomnia symptoms and daytime sleepiness. To test this hypothesis, we assessed serum Vitamin B12 levels in adult primary health care users in Crete, Greece and investigated possible correlations with socio-demographic factors, co-morbidities, sleep quality, insomnia symptoms and daytime sleepiness, after considering other confounders.
2. Materials and Methods
2.1. Patients
In this single-center, cross-sectional study, patients aged ≥ 18 years were consecutively approached by General Practitioners (GPs) during their regular consultations at four public primary health care practices (one organized health center and three satellite practices) located in rural and semi-urban areas, in the region of Crete over a 3-year period (2019–2022). Exclusion criteria included a history of current infectious diseases, gastrointestinal reabsorption disorders, bariatric surgery, pregnant or breastfeeding women, diagnosed sleep disorders or on sleep medication, intake of vitamin B12 supplements or medications with known effects on serum vitamin B12 levels. Ethical approval was provided by the Health Regional Administration (DYPE) of Crete Scientific Board Ethics Committee (protocol number 23542/06-12-2017) and the patients gave written informed consent.
2.2. Demographic Characteristics
The collected data included anthropometric parameters, such as age, gender, height, weight, body mass index (BMI), details of co-morbidities, smoking history and alcohol intake. The Epworth Sleepiness Scale (ESS) was utilized to assess subjective excessive daytime sleepiness (EDS)[27]. The scale measures from 0 to 24 and a value less than or equal to 10 is considered normal. The evaluation of insomnia was performed utilizing the Athens Insomnia Scale (AIS), an 8-item self-assessment psychometric instrument, that has been employed as a means to assess the severity of insomnia [28]. The range of total scores falls between 0 and 24, and insomnia is indicated by a total score of 6 or above. Pittsburgh Sleep Quality Index (PSQI), a 19-item self-rated questionnaire, was employed to assess sleep quality. It evaluates subjective sleep quality and quantity, sleep habits that impact quality, and sleep disturbances occurrence in adults over a 1-month period. A global score of 6 or higher indicates poor sleep (range 0-21) [29].
2.3. Vitamin B12 Measurement
Serum samples for Vitamin B12 levels were obtained. Blood samples were taken after at least 8 hr of fasting, they were immediately centrifuged (3000 rpm for 10 min), and the serum obtained had been frozen at -80C until processing. Serum vitamin B12 levels was measured using the Alinity i system (Abbott Laboratories, Chicago, IL, USA) chemiluminescent microparticle immunoassay (CMIA) analyzer. For this study, the data on serum vitamin B12 levels were divided into two groups based on the median value of its measurement.
2.4. Statistical Analysis
Results are presented as mean ± standard deviation (SD) for continuous variables if normally distributed and as median (25th-75th percentile) if not. Qualitative variables are presented as absolute number (percentage). For comparisons between groups, a two-tailed t-test for independent samples (for normally distributed data) or a Mann–Whitney U test (for non-normally distributed data) was utilized for continuous variables and the chi-square test for categorical variables. Logistic regression analysis was applied to examine the effect of vitamin B12 levels on co-morbidities, sleepiness, sleep quality and insomnia symptoms, after controlling for potential explanatory variables, including age, gender, BMI, smoking status, co-morbidities, marital, educational status, menopausal status and alcohol intake. We checked multicollinearity among the predictors using collinearity statistics to ensure that collinearity between predictor variables was in the acceptable range as indicated by the tolerance value variance inflation factor. For the purpose of this analysis, the term cardiovascular disease, used as predictor in logistic regression models, referred to any of the following conditions: coronary disease, atrial fibrillation cerebrovascular disease and heart failure. Age was considered continuously and categorically, as age groups of 18–59 and >60 years, BMI was also considered continuously and categorically, as BMI groups of <30 and ≥30 kg/m2. Results were considered significant when p values were < 0.05. Data were analyzed using SPSS software (version 25, SPSS Inc, Chicago, IL).
3. Results
3.1. Study Population
Following the screening process, a grand total of 512 participants (whose average age was 64 years and of which 35% were male) were deemed eligible and subsequently included in the study, as depicted in Figure 1. Among the participants, 27% reported excessive daytime sleepiness (ESS≥11), while 40% experienced insomnia symptoms (AIS≥6) and 37% had poor sleep quality (PSQI≥6). The median level of Vitamin B12 was 342 (266, 446) pg/mL and there was no statistically significant difference observed between genders (349 vs 326, p=0.108). Participants were divided into two groups based on the median value of Vitamin B12: those with B12 levels below (<) 342 pg/mL, recognized as low levels and those with (≥) 342 pg/mL levels, recognized as normal levels.
Table 1 displays the baseline characteristics of the study population, stratified by Vitamin B12 status. Patients with low Vitamin B12 levels did not exhibit any notable differences in baseline characteristics compared to those without low levels, including age, gender, menopausal status, BMI, comorbidities, and smoking status (all p >0.05).
3.2. Vitamin B12 Correlations with Sleep Quality, Daytime Sleepiness, and Insomnia Symptoms
Table 2 and Figure 2 demonstrate differences in questionnaires scores between people with low Vitamin B12 levels and those without. The groups showed no significant variation in ESS score (6 vs 6, p=0.908) or excessive daytime sleepiness (ESS>10) (25 vs 22%, p=0.636). The PSQI score failed also to exhibit any significant differences between the groups (5 vs 4, p=0.286). Additionally, the difference in the percentage of people with PSQI≥6 between the groups was not statistically significant (37 vs 32, p=0.286).
On the other hand, individuals with low levels of Vitamin B12 exhibited a greater AIS score, albeit statistically insignificant, compared to those who didn't (5 vs 4, p=0.419). However, there was a significant difference between the two groups regarding the percentage of people with AIS≥6 (49 vs 34%, p=0.035). Besides, the study revealed that participants who experienced insomnia symptoms had a notably lower level of vitamin B12 compared to those who did not report such symptoms (310 vs 354, p=0.03).
Table 3, Table 4 and Table 5 show multiple stepwise logistic regression analysis of the relationship between excessive daytime sleepiness (EDS), sleep quality and insomnia symptoms and various independent variables, after multiparametric adjustments for age, gender, obesity, co-morbidities and marital, educational, menopausal and smoking status. The prevalence of EDS was significantly predicted by obesity and male gender in the population studied (Table 3). Although low Vitamin B12 levels did not have a significant predictive value for EDS, there was a significant correlation between low Vitamin B12 levels and EDS in obese patients (BMI≥30) (OR = 3.996, 95% CI = 1.006-15.876, p=0.039).
The occurrence of insomnia symptoms was found to be linked with female gender, hypertension, and insufficient Vitamin B12 levels (Table 4). Further analysis on subgroups that were stratified by gender, age and BMI indicated that low vitamin B12 levels were significantly associated with insomnia symptoms only in the subgroup of elderly (age group >60 years), (OR = 3.197, 95% CI = 1.495-6.836, p=0.003), females (OR = 2.549, 95% CI = 1.257-5.169, p=0.009) and non-obese subjects (BMI group<30) (OR = 2.955, 95% CI = 1.386-6.300, p=0.005).
There was no correlation found between vitamin B12 levels and poor sleep quality (Table 5), even after controlling for confounding factors. Furthermore, subgroup analyses based on gender, age, and BMI failed to reveal any significant associations.
4. Discussion
Our study aimed to investigate the potential correlation between Vitamin B12 levels and subjective sleep symptoms as assessed by ESS, AIS, and PSQI questionnaires. We found that low vitamin B12 levels were associated with a 2.4-times risk increase of insomnia symptoms and the association was significantly persisted in the older, females and non-obese subjects. Furthermore, in obese subjects a significant association of excessive daytime sleepiness and low vitamin B12 levels was noted.
Despite the acknowledged significance of vitamin B12 for the nervous system and the risks of its deficiency, there remains an insufficiency of research on the relationship between Vitamin B12 and sleep disorders, including the specific blood level thresholds that could trigger such disorders. The existing studies which have focused primarily on the relationship between micronutrients and sleep duration, have yielded inconsistent results regarding the impact of vitamin B12 on sleep patterns [19]. Initially, studies did not report any significant or conclusive impact of Vitamin B12 on the duration and phase of nocturnal sleep [18, 23, 24], except for Mayer et al [25], who observed a stimulating effect of Vitamin B12 supplementation associated with decreased sleep. Subsequent research indicated that there is a potential negative correlation between serum Vitamin B12 concentrations and the duration of sleep [21, 26].
The available evidence regarding the correlation of levels of Vitamin B12 and the likelihood of experiencing symptoms of insomnia is even more limited. Using data from 2459 adults and conducting cross-sectional surveys of the health and nutritional status of the American population, the National Health and Nutrition Examination Surveys (NHANES) study has concluded that Vitamin B12 levels and the duration of sleep are inversely associated [21]. Nevertheless, no association was observed between Vitamin B12 and symptoms of insomnia in this population. However, one must bear in mind that insomnia was assessed using only one question requiring a yes or no response. Similarly, in a subsequent study that examined 575 patients over the age of 65 from a geriatric population, no significant difference was found between levels of serum Vitamin B12 and the severity of insomnia assessed by The Insomnia Severity Index (ISI) [31]. In our study, a 2.4-fold increase in the odds ratio for insomnia symptoms was observed in individuals with low Vitamin B12 levels, demonstrating a significant association between the two. These findings appear to align with a previous investigation involving 355 Arabian female students, which discovered a negative association between serum Vitamin B12 levels and sleep latency. Participants in the same study exhibiting higher serum Vitamin B12 levels ranging from 333.1–482.2 also reported a decreased use of sleep medication [22]. In addition, a lower intake of Vitamin B12 seemed to be associated with a delayed sleep-wake rhythm [26] and a higher prevalence of insomnia symptoms, assessed by Insomnia Screening Questionnaire [32]. The crucial function of B12 in sleep latency is reinforced by a previous study that examined the impact of Vitamin B12 supplementation on the sleep-wake cycle of individuals with delayed sleep phase syndrome, showing a significant temporary improvement in the supplemented group [24]. The therapeutic benefits of Vitamin B12 supplementation in sleep-wake disorder management were also suggested by Maeda et al., who noted its role in regulating circadian rhythms [33].
On the other hand, our findings contradict those of a recent study involving 418 Chinese participants with type 2 diabetes, which identified an independent positive association between Vitamin B12 levels and insomnia symptoms, as assessed by AIS, after controlling for confounding variables [34]. Our speculation is that this discrepancy may have arisen partly due to variations in race/ethnicity. A recent investigation supports this assertion, revealing that a combination of genetic and acquired/environmental factors contribute to the ethnic differences in serum Vitamin B12 levels [35]. Additionally, Chinese participants demonstrate a higher probability of suffering from insufficient sleep (<6 hours) and lower occurrences of insomnia symptoms and daytime sleepiness when compared to Whites [36].
Interestingly, the association of B12 and insomnia symptoms was more pronounced in elderly, females, and non-obese participants. Despite the lack of explanation currently, it is plausible that Vitamin B12 affects sleep in distinct ways for both older and younger adults, due to the notable changes in sleep structure with aging. Variances in circadian phase, light responsiveness, and clock gene expression identified between older and younger adults [37] could lead to a different reaction to Vitamin B12.
Our investigation also revealed that vitamin B12 levels did not correlate with sleep quality as measured by PSQI in our cohort. These results are in agreement with prior current investigations conducted on Chinese individuals with type 2 diabetes [34], and female Arab students [22], wherein no correlation was found between serum Vitamin B12 levels and sleep quality, as assessed by PSQI. The NHANES study also did not identify a link between Vitamin B12 levels and metrics of sleep quality [21]. Additionally, 14 healthy adult participants did not exhibit any association between their serum Vitamin B12 levels and actigraphy-assessed sleep parameters before and two weeks after receiving 3mg/day cyanocobalamin supplementation [38]. Furthermore, research that has focused on the dietary intake of Vitamin B12 and its effect on sleep quality has yielded conflicting findings [39, 40]. A correlation was noted by Condo et al between Vitamin B12 consumption and improved sleep quality, evaluated by actigraphy in 32 female athletes at the elite level [39]. Conversely, Jahrami et al found a conflicting outcome, indicating a strong link between daily Vitamin B12 intake and lower sleep quality, evaluated by PSQI in 96 healthy individuals [40]. Given that these studies utilized methods to assess dietary intake as a means of measuring Vitamin B12 status, this may have resulted in an unreliable memory of individual dietary habits or errors in measurement, which could have influenced the final measurements of the aforementioned connections. As a result, more studies are warranted to explore the potential benefits of high serum levels or intake of Vitamin B12 on sleep quality.
To date, few data exist regarding Vitamin B12 status in the adult population and prevalence of EDS. According to our study, low levels of Vitamin B12 were not found to significantly predict EDS, which is consistent with prior studies including the NHANES study (n=2,459) [21] and also with studies that focused in elderly patients with chronic kidney disease (n=367) [41] and elderly patients with or without dementia (n=800) [42]. However, we found a significant correlation between low Vitamin B12 levels and EDS in obese participants. The exploration of a plausible association between low Vitamin B12 levels as a cause of EDS in obese population is constrained. Within the literature, a singular case is reported of an obese patient with obstructive sleep apnea (OSA) who experienced excessive daytime sleepiness (EDS) despite receiving optimal treatment and having a severe deficiency in Vitamin B12. The intake of Vitamin B12 supplements in this case proved to reverse EDS [43], which could imply that Vitamin B12 deficiency may play a role in causing daytime sleepiness.
The results from the current study have important implications for primary care health practice. Our study's overall sample revealed that a significant number of participants reported insomnia symptoms, poor sleep quality and EDS, indicating that primary care physicians encounter challenges in identifying and managing these disorders. Vitamin B12 levels <342 were identified as a significant predictor of a high AIS score, particularly in individuals over 60, females, and those who are not obese and also a significant predictor of high ESS score in obese subjects. Therefore, particularly within this subset of individuals, these Vitamin B12 levels may aid in distinguishing adults with a higher likelihood of developing insomnia and sleepiness later on.
It is plausible that several limitations might have affected our results. First, the cross-sectional design of our study precludes us from assigning causality to the associations between insomnia symptoms, excessive daytime sleepiness and Vitamin B12. Second, self-reported sleep measures were employed to determine sleep disorders, which may be affected by estimation bias, compared to more-objective measures such as actigraphy and polysomnography. Thirdly, we had to exclude patients with specific characteristics based on justified exclusion criteria to minimize potential bias in the study's findings. While we accounted for a significant number of relevant confounding variables, there is still the possibility of unmeasured confounders that might impact our results, such as dietary habits and stress levels. Nevertheless, no noteworthy dissimilarities are expected concerning dietary patterns, given that our research comprised only Cretan participants, dwelling in the same area, with similar dietary habits. Lastly, given that participants were residents of Crete (located in the southern region of Greece), the generalization of our conclusions to all Greek primary care users should be made with caution.
5. Conclusions
Our results showed that lower Vitamin B12 levels were associated with higher risk of insomnia symptoms and EDS in specific subgroup of adult primary healthcare care users. Despite the need for additional work to elucidate the potential underlying mechanisms of these associations, low Vitamin B12 levels should be considered as a possible culprit in certain subpopulations of patients experiencing sleep disturbances. Further prospective studies are also needed to determine the accurate levels of Vitamin B12 for sleep health and the need for Vitamin B12 supplementation.
Author Contributions
Conceptualization, I.T. and S.S.; methodology, I.B. and E.L.; software, I.B..; validation, I.B. and I.T.; formal analysis, I.B.; M.L. and K.R.; investigation, M.L. and K.R..; writing—original draft preparation, I.B..; writing—review and editing, I.B.; S.S. and I.T.; supervision, I.T. and S.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Primary Health Care Centre of Kastelli Scientific Board Ethics Committee (protocol code 23542/06-12-2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Buysse, D.J. Sleep health: Can we define it? Does it matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef]
- Cho, Y.W.; Shin, W.C.; Yun, C.H.; Hong, S.B.; Kim, J.; Earley, CJ. Epidemiology of insomnia in Korean adults: prevalence and associated factors. J Clin Neurol 2009, 5, 20–23. [Google Scholar] [CrossRef]
- Hossain, J.L.; Shapiro, C.M. The prevalence, cost implications, and management of sleep disorders: an overview. Sleep Breath 2002, 6, 85–102. [Google Scholar] [CrossRef]
- Minowa, M.; Okawa, M. Uchiyama, M. Prevalence of sleep disturbance and hypnotic medication use in relation to sociodemographic factors in the general Japanese adult population. J Epidemiol 2000, 10, 79–86. [Google Scholar]
- Sutton, D.A.; Moldofsky, H. Badley, E.M. Insomnia and health problems in Canadians. Sleep 2001, 24, 665–670. [Google Scholar] [CrossRef]
- Wong, W.S.; Fielding, R. Prevalence of insomnia among Chinese adults in Hong Kong: a population-based study. J Sleep Res 2011, 20, 117–126. [Google Scholar] [CrossRef]
- Riemann, D.; Berger, M.; Voderholzer, U. Sleep and depression – results from psychobiological studies: an overview. Biol Psychol 2001, 57, 67–103. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Liao, D.; Pejovic, S.; Calhoun, S.; Karataraki, M.; & Bixler, E.O.; & Bixler, E. O. Insomnia with objective short sleep duration is associated with type 2 diabetes: a population-based study. Diabetes Care 2009, 32, 1980–1985. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Cooper, D.; D'Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Eur Heart J 2011, 32, 1484–1492. [Google Scholar] [CrossRef]
- Qin, Y.; Zhou, Y.; Zhang, X.; Wei, X.; He, J. Sleep duration and breast cancer risk: a meta-analysis of observational studies. Int J Cancer 2014, 134, 1166–1173. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, L.; Kalesan, B. Sleep duration and mortality: a systematic review and meta-analysis. J Sleep Res 2009, 18, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Afaghi, A.; O’Connor, H.; Chow, C.M. Acute effects of the very low carbohydrate diet on sleep indices. Nutr Neurosci 2008, 11, 146–154. [Google Scholar] [CrossRef]
- Grandner, M.A.; Jackson, N.; Gerstner, J.R.; Knutson, K.L. Sleep symptoms associated with intake of specific dietary nutrients. J Sleep Res 2014, 23, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Bertisch, S.M.; Sillau, S.; de Boer, I.H.; Szklo, M.; Redline, S. 25-Hydroxyvitamin D concentration and sleep duration and continuity: Multi-Ethnic Study of Atherosclerosis. Sleep 2015, 38, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Peuhkuri, K.; Sihvola, N.; Korpela, R. Diet promotes sleep duration and quality. Nutr Res 2012, 32, 309–319. [Google Scholar] [CrossRef]
- Ursin, R. Serotonin and sleep. Sleep Med Rev 2002, 6, 55–67. [Google Scholar] [CrossRef]
- Sowa-Kućma, M.; Legutko, B.; Szewczyk, B.; Novak, K.; Znojek, P.; Poleszak, E.; Papp, M.; Pilc, A.; Nowak, G. A ntidepressant-like activity of zinc: further behavioral and molecular evidence. J Neural Transm 2008, 115, 1621–1628. [Google Scholar] [CrossRef] [PubMed]
- Honma, K.; Kohsaka, M.; Fukuda, N.; Morita, N.; Honma, S. Effects of vitamin B12 on plasma melatonin rhythm in humans: increased light sensitivity phase-advances the circadian clock? Experientia 1992, 48, 716–720. [Google Scholar] [CrossRef]
- Ji, X.; Grandner, M.A.; Liu, J. The relationship between micronutrient status and sleep patterns: a systematic review. Public Health Nutr 2017, 20, 687–701. [Google Scholar] [CrossRef]
- Calderón-Ospina, C.A.; Nava-Mesa, M.O. B. Vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci Ther 2020, 26, 5–13. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Gamaldo, A.A.; Canas, J.A.; Beydoun, H.A.; Shah, M.T.; McNeely, J.M.; Zonderman, A.B. Serum nutritional biomarkers and their associations with sleep among US adults in recent national surveys. PLoS One 2014, 9, e103490. [Google Scholar] [CrossRef] [PubMed]
- Al-Musharaf, S.; Alabdulaaly, A.; Bin Mujalli, H.; Alshehri, H.; Alajaji, H.; Bogis, R.; Alnafisah, R.; Alfehaid, S.; Alhodaib, H.; Murphy, A.M.; Hussain, S.D.; Sabico, S.; McTernan, P.G.; Al-Daghri, N. Sleep quality is associated with vitamin B12 status in female Arab students. Int. J. Environ. Res. Publ. Health 2021, 18, 4548. [Google Scholar]
- Okawa, M.; Takahashi, K.; Egashira, K.; Furuta, H.; Higashitani, Y.; Higuchi, T.; Ichikawa, H.; Ichimaru, Y.; Inoue, Y.; Ishizuka, Y.; Ito, N.; Kamei, K.; Kaneko, M.; Kim, Y.; Kohsaka, M.; Komori, T.; Kotorii, T.; Matsumoto, M.; Mishima, K.; Mizuki, Y.; … Takahashi, S. Vitamin B12 treatment for delayed phase syndrome: a multicenter double-blind study. Psychiatry Clin Neurosci 1997, 51, 275–279. [Google Scholar] [CrossRef]
- Takahashi, K.; Okawa, M.; Matsumoto, M.; Mishima, K.; Yamadera, H.; Sasaki, M.; Ishizuka, Y.; Yamada, K.; Higuchi, T.; Okamoto, N.; Furuta, H.; Nakagawa, H.; Ohta, T.; Kuroda, K.; Sugita, Y.; Inoue, Y.; Uchimura, N.; Nagayama, H.; Miike, T.; Kamei, K. Double-blind test on the efficacy of methylcobalamin on sleep–wake rhythm disorders. Psychiatry Clin Neurosci 1999, 53, 211–213. [Google Scholar] [CrossRef]
- Mayer, G.; Kroger, M. Meier-Ewert, K. Effects of vitamin B12 on performance and circadian rhythm in normal subjects. Neuropsychopharmacology 1996, 15, 456–464. [Google Scholar] [CrossRef]
- Sato-Mito, N.; Shibata, S.; Sasaki, S.; Sato, K. Dietary intake is associated with human chronotype as assessed by both morningness–eveningness score and preferred midpoint of sleep in young Japanese women. Int J Food Sci 2011, 62, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test-retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J Psychosom Res 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Aparicio-Ugarriza, R.; Palacios, G.; Alder, M.; González-Gross, M. A review of the cut-off points for the diagnosis of vitamin B12 deficiency in the general population. Clin Chem Lab Med 2015, 53, 1149–1159. [Google Scholar] [CrossRef]
- Soysal, P.; Smith, L.; Dokuzlar, O.; Isik, A.T. Relationship Between Nutritional Status and Insomnia Severity in Older Adults. J Am Med Dir Assoc 2019, 20, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Zadeh, S.S.; Begum, K. Comparison of nutrient intake by sleep status in selected adults in Mysore, India. Nutr Res Pract 2011, 5, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Okamoto, N.; Nishimoto, M.; Hoshino, R.; Ohara, K.; Ohashi, Y.; Kawaguchi, K. A Multicenter Study of the Effects of Vitamin B12on Sleep-Waking Rhythm Disorders: In Shizuoka Prefecture. Psychiatry Clin. Neurosci 1992, 46, 229–230. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Liu, Z.; Yao, N.; Zhang, X.; Ge, Q. The independent association between vitamin B12 and insomnia in Chinese patients with type 2 diabetes mellitus: a cross-sectional study. Nutr Diabetes 2022, 12, 3. [Google Scholar] [CrossRef] [PubMed]
- O'Logbon, J.; Crook, M.; Steed, D.; Harrington, D.J.; Sobczyńska-Malefora, A. Ethnicity influences total serum vitamin B12 concentration: a study of Black, Asian and White patients in a primary care setting. J Clin Pathol 2022, 75, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, R.; Zee, P.; Lutsey, P.L.; Javaheri, S.; Alcántara, C.; Jackson, C.L.; Williams, M.A.; Redline, S. Racial/ethnic differences in sleep disturbances: the Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2015, 38, 877–888. [Google Scholar] [CrossRef]
- Duffy, J.F.; Zitting, K.M.; Chinoy, E.D. Aging and circadian rhythms. Sleep Med Clin 2015, 10, 423–434. [Google Scholar] [CrossRef]
- Channer-Wallen, T.; Dawson, P.; Thomas-Brown, P.G.; Gossell-Williams, M. Lack of association between serum vitamin B12 and nocturnal sleep parameters following cyanocobalamin supplementation in healthy adults. Heliyon 2022, 8, e08831. [Google Scholar] [CrossRef]
- Condo, D.; Lastella, M.; Aisbett,B. ; Stevens, A.; Roberts, S. Sleep duration and quality are associated with nutrient intake in elite female athletes. J Sci Med Sport 2022, 25, 345–350. [Google Scholar] [CrossRef]
- Jahrami, H.; Alekri, E.; BaHammam, A.S.; Alsalman, A.; Bragazzi, N.L.; Alhaj, O.; Saif, Z. The association between micronutrient status and sleep quality in patients with depression: a case-control study. Sleep Breath 2021, 25, 1571–1579. [Google Scholar] [CrossRef]
- Heybeli, C.; Soysal, P.; Oktan, M.A.; Smith, L.; Çelik, A.; Kazancioglu, R. Associations between nutritional factors and excessive daytime sleepiness in older patients with chronic kidney disease. Aging Clin Exp Res 2022, 34, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Koc Okudur, S.; Soysal, P. Excessive Daytime Sleepiness is Associated With Malnutrition, Dysphagia, and Vitamin D Deficiency in Older Adults. J Am Med Dir Assoc 2021, 22, 2134–2139. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, I.; Yingling, K.; Bukamur, H.; Abusnina, W. Vitamin B12 Deficiency: A Rare Cause of Excessive Daytime Sleepiness. J Clin Sleep Med 2019, 15, 1365–1367. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The flowchart of patients finally included.

Figure 2.
Comparison of questionnaires scores based on Vitamin B12 levels.
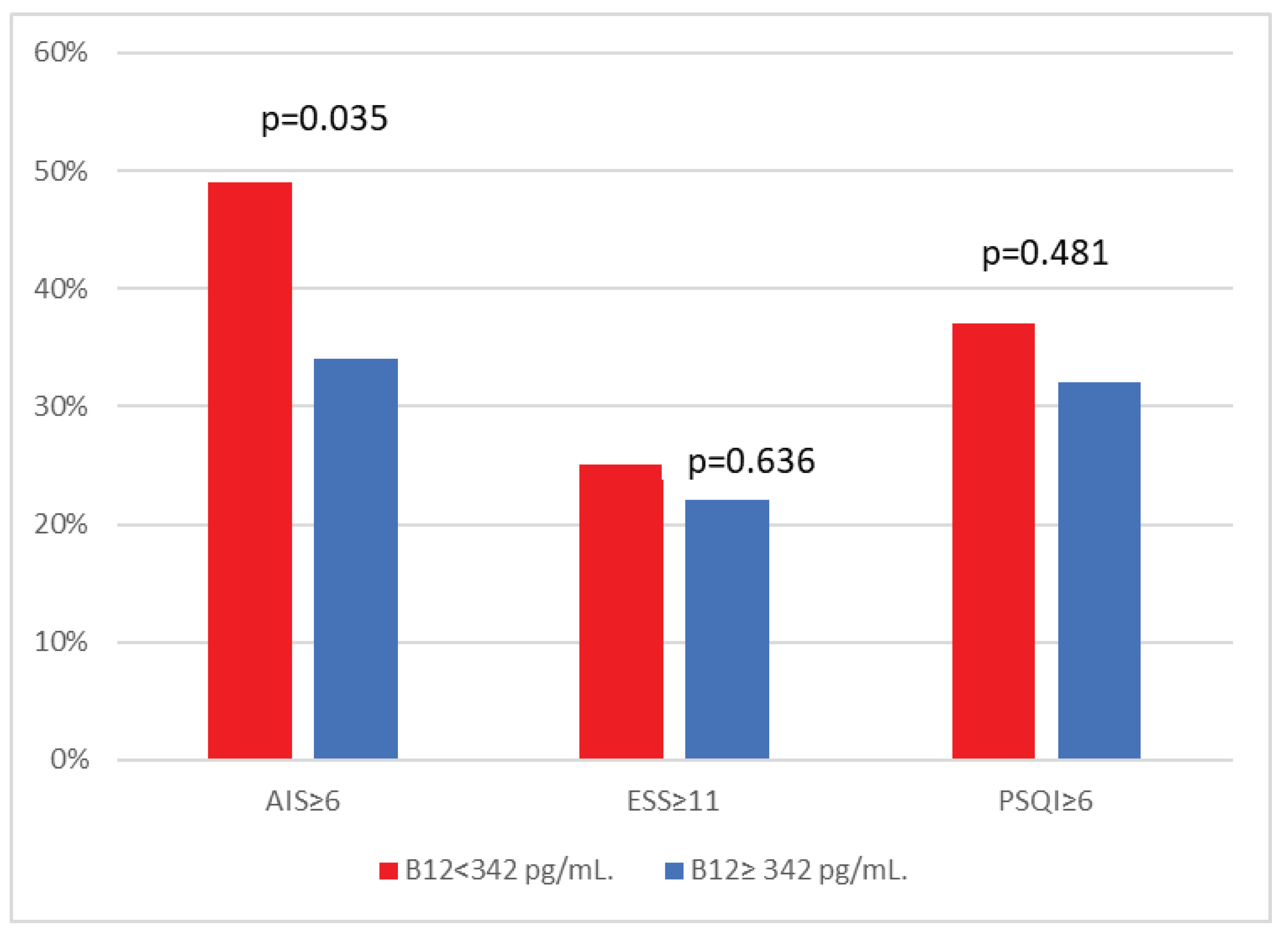

Table 1.
Clinical characteristics of the 512 primary care users according to Vitamin B12 status.
| Total population according to Vitamin B12 status |
||||
|---|---|---|---|---|
| Total population |
Vitamin B12 ≥342 pg/mL | Vitamin B12 <342 pg/mL | p-value | |
| N=512 | N=256 | N=256 | ||
| Demographics | ||||
| Gender, males (%) | 180 (35%) | 84 (33%) | 96 (38%) | 0.343 |
| Menopause (%) | 249 (75%) | 129 (75%) | 120 (75%) | 0.997 |
| Age, years | 64 ± 16 | 63 ± 16 | 65 ± 15 | 0.144 |
| Age ≥ 60 years | 323 (63%) | 151 (59%) | 172 (67%) | 0.160 |
| BMI (kg/m2) | 30 ± 16 | 30 ± 19 | 30 ± 11 | 0.903 |
| BMI≥30, n (%) | 168 (33%) | 84 (33%) | 84 (33%) | 0.966 |
| Smoking status | ||||
| Never, n (%) | 272 (53%) | 148 (58%) | 124 (49%) | |
| Current/, n (%) | 107 (21%) | 56 (22%) | 51 (20%) | |
| Former, n (%) | 133 (26%) | 51 (20%) | 82 (32%) | 0.066 |
| Co-morbidities | ||||
| Hypertension | 260 (51%) | 130 (51%) | 130 (51%) | 0.999 |
| Diabetes Type 2 | 97(19%) | 38 (15%) | 59 (23%) | 0.128 |
| Hyperlipidemia | 279 (55%) | 133 (52%) | 146 (57%) | 0.463 |
| COPD | 38 (7%) | 18 (7%) | 20 (8%) | 0.163 |
| Asthma | 20 (4%) | 15 (6%) | 5 (2%) | 0.136 |
| Coronary Artery Disease | 35 (7%) | 20 (8%) | 15 (6%) | 0.529 |
| Atrial fibrillation | 23 (5%) | 13 (5%) | 10 (4%) | 0.837 |
| Cerebrovascular Disease | 11 (2%) | 7 (3%) | 4 (1%) | 0.429 |
| Cardiovascular Disease | 74 (15%) | 43 (17%) | 31 (12%) | 0.216 |
| Depression (on medications) |
59 (11%) | 33 (13%) | 26 (10%) | 0.533 |
Data are presented as mean values ± SD or median (25th-75th percentile), unless otherwise indicated. BMI, Body mass index; COPD, Chronic obstructive pulmonary disease; Cardiovascular disease: Coronary heart disease or atrial fibrillation or cerebrovascular disease or heart failure.
Table 2.
Questionnaires scores of the 512 primary care users according to Vitamin B12 status.
| Total population according to Vitamin B12 status |
||||
|---|---|---|---|---|
| Total population |
Vitamin B12 ≥342 pg/mL | Vitamin B12 <342 pg/mL | p-value | |
| N=512 | N=256 | N=256 | ||
| Daytime sleepiness | ||||
| ESS | 6 (4, 10) | 6 (4, 10) | 6 (4, 10) | 0.908 |
| ESS≥11 (%) | 120 (23%) | 56 (22%) | 64 (25%) | 0.636 |
| Insomnia symptoms | ||||
| Athens Insomnia Scale Score | 5 (3,6) | 4 (3, 6) | 5 (3, 6) | 0.419 |
| Athens Insomnia Scale Score≥6 (%) | 212 (41%) | 87 (34%) | 125 (49%) | 0.035 |
| Sleep Quality | ||||
| PSQI | 5 (3, 6) | 4 (3, 6) | 5 (3, 6) | 0.286 |
| PSQI≥6 | 177 (35%) | 82 (32%) | 95 (37%) | 0.481 |
Data are presented as mean values ± SD or median (25th-75th percentile), unless otherwise indicated. ESS, Epworth Sleepiness Scale; PSQI, Pittsburgh Sleep Quality Index.
Table 3.
Multiple stepwise logistic regression analysis of the relationship between excessive daytime sleepiness (ESS≥11) and various independent variables.
Table 3.
Multiple stepwise logistic regression analysis of the relationship between excessive daytime sleepiness (ESS≥11) and various independent variables.
| B | S.E. | p-value | OR (95%CI) | |
| Males versus Females | 1.098 | 0.385 | 0.004 | 2.998 (1.410-6.374) |
| Age >60 years | -0.169 | 0.366 | 0.669 | 0.844 (0.388-1.835) |
| Body mass index≥30 | 0.759 | 0.342 | 0.027 | 2.135 (1.091-4.178) |
| Current/Former smoking | 0.362 | 0.397 | 0.362 | 1.436 (0.660-3.126) |
| Hypertension | 0.139 | 0.393 | 0.723 | 1.159 (0.532-2.484) |
| Diabetes type 2 | 0.443 | 0.429 | 0.302 | 1.557 (0.671-3.614) |
| Cardiovascular disease | -0.554 | 0.521 | 0.288 | 0.575 (0.207-1.597) |
| COPD | 0.189 | 0.546 | 0.729 | 1.208 (0.414-3.521) |
| Depression | -0.050 | 0.573 | 0.931 | 0.952 (0.310-2.924) |
| Vitamin B12 <342 | 0.101 | 0.517 | 0.762 | 1.106 (0.576-2.125) |
Table 4.
Multiple stepwise logistic regression analysis of the relationship between insomnia symptoms (AIS≥6) and various independent variables.
Table 4.
Multiple stepwise logistic regression analysis of the relationship between insomnia symptoms (AIS≥6) and various independent variables.
| B | S.E. | p-value | OR (95%CI) | |
| Females versus Males | 1.266 | 0.397 | 0.001 | 3.547 (1.630-7.718) |
| Age >60 years | -0.129 | 0.375 | 0.730 | 0.879 (0.422-1.831) |
| Body mass index≥30 | 0.073 | 0.318 | 0.818 | 1.076 (0.577-2.009) |
| Current/Former smoking | 0.227 | 0.356 | 0.523 | 1.255 (0.625-2.520) |
| Hypertension | 1.229 | 0.368 | 0.001 | 3.419 (1.661-7.035) |
| Diabetes type 2 | -0.467 | 0.424 | 0.270 | 0.627 (0.273-1.438) |
| Cardiovascular disease | 0.526 | 0.453 | 0.246 | 1.692 (0.696-4.112) |
| COPD | 0.133 | 0.603 | 0.826 | 1.142 (0.350-3.724) |
| Depression | -0.467 | 0.472 | 0.322 | 0.627 (0.249-1.579) |
| Vitamin B12 <342 | 0.890 | 0.308 | 0.004 | 2.434 (1.331-4.452) |
Table 5.
Multiple stepwise logistic regression analysis of the relationship between poor sleep quality (PSQI≥6) and various independent variables.
Table 5.
Multiple stepwise logistic regression analysis of the relationship between poor sleep quality (PSQI≥6) and various independent variables.
| B | S.E. | p-value | OR (95%CI) | |
| Females versus Males | 0.318 | 0.460 | 0.489 | 1.374 (0.558-3.384) |
| Age >60 years | 0.385 | 0.469 | 0.410 | 1.470 (0.588-3.679) |
| Body mass index≥30 | 0.305 | 0.424 | 0.471 | 1.357 (0.591-3.116) |
| Current/Former smoking | -0.624 | 0.424 | 0.141 | 0.536 (0.233-1.229) |
| Hypertension | 0.028 | 0.438 | 0.948 | 1.029 (0.436-2.430) |
| Diabetes type 2 | 0.275 | 0.522 | 0.599 | 1.316 (0.473-3.662) |
| Cardiovascular disease | 0.262 | 0.592 | 0.658 | 1.300 (0.408-4.144) |
| COPD | 1.307 | 0.767 | 0.089 | 3.693 (0.821-16.614) |
| Depression | 0.540 | 0.631 | 0.392 | 1.716 (0.498-5.918) |
| Vitamin B12 <342 | 0348 | 0.376 | 0.354 | 1.416 (0.678-2.958) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



