
Submitted:
11 October 2023
Posted:
12 October 2023
You are already at the latest version
Abstract
We present here a case of complex uterine anomaly – Obstructed HemiVagina with Ipsilateral Renal Agenesis (OHVIRA), also known as Herlyn-Werner-Wunderlich syndrome in a 13-year-old girl with the history of recurrent urinary tract infections (rUTI). In emergency room, trans-abdominal sonography revealed ovarian cyst and renal agenesis, without any suspicion of vaginal obstruction. This led to delay in the diagnosis of this uncommon anomaly. Finally, MRI findings confirmed the presence of OHVIRA syndrome.
As the congenital anomalies of kidney and urinary tract (CAKUT) are in almost one third of cases associated with genital malformations, urologist should carefully search for patients with rUTI. The patient underwent simultaneous laparoscopy and vaginoscopy, what was in our opinion the most appropriate therapeutic decision. In this article we are also going to discuss the role of laparoscopy in the management of OHVIRA syndrome as well as other surgical techniques described in the literature.
Keywords:
obstructed vagina
; OHVIRA syndrome
; recurrent urinary tract infections (rUTI)
; congenital anomalies of kidney and urinary tract (CAKUT)
; renal agenesis
; laparoscopic surgery in female adolescents
Introduction
Congenital anomalies of kidney and urinary tract (CAKUT) are in almost one third of cases associated with genital malformations [1,2]. Prevalence of CAKUT has a high range in pediatric population (3.5% to 43%) and this cluster of disorders represents the most frequent cause of chronic kidney disease (CKD) in children [3]. Indeed, these disorders may predispose to recurrent urinary tract infections (rUTI) resulting in kidney impairment [4]. Uterus didelphys with obstructed hemivagina (OHVIRA) may cause acute abdomen, rUTI, and this condition may be associated to CAKUT [5]. Therefore, OHVIRA should be considered in young females with these symptoms and CAKUT.
Currently, the management of OHVIRA is still debated. Although many ideas for OHVIRA management have been suggested delayed diagnosis is still an obliquitous problem. In this article, we present a problem-solving flowchart and other methods that could help professionals in their practice. Several operative techniques for OHVIRA management have been reported, such as puncture of vaginal wall, single-stage vaginoplasty, mini-laparotomy even with unilateral hysterectomy [6]. However, evidence regarding the most effective therapeutic option is scant. Moreover, some authors have also questioned the diagnostic role of laparoscopy, that is still under debate [7].
We report a case of a young women with OHVIRA associated to CAKUT and conditioning rUTI and pain. This case emphasizes that uterus didelphys with obstructed hemivagina (OHVIRA) should be considered in the differential diagnosis of adolescent girls presenting with acute abdomen, rUTI and CAKUT. Furthermore, we reviewed the most used surgical procedures for these conditions.
Case report
We report the case of a 13-year-old girl who presented with acute abdominal pain and UTI. Hematuria was not present. The patient had a history of rUTIs occurred six times in the last year, with urine cultures were positive for more than 105 colony-forming units (CFU)/mL of Escherichia coli (E coli). The young women complained rUTI despite courses of antibiotics had been administered (Cefuroxime 2x1 500 mg iv.).
The patient attained menarche 6 months previously, reporting of back and lower abdominal pain and UTI, of 1 week's duration. She had regular menstrual cycles, every 30 days, lasting -3 to -4 days.
Abdominal ultrasonography (US) [Figure 1] revealed the right renal agenesis and suspicion of right ovarian cyst. Due to elevated tumor markers (Ca-125/ROMA Index), the patient was referred to laparotomy. Urgent urological consultation excluded any urological cause and indicated on gynecological background of symptoms. Sudden vaginal bleeding led to expand investigations and the patient was admitted by tertiary referral hospital.
Particular image examination were performed at the Department of Gynecology, Endocrinology and Gynecologic Oncology of University hospital.
On admission, because of the patient’s severe pain, the examination under general anesthesia and dorsal lithotomy position with virgin-size speculum revealed a single normal vagina and one cervix. Bulging vaginal wall on the right side was also found. Unfortunately, the attempt to puncture a thick vaginal wall to relieve patient’s symptoms, failed in obtaining its drainage. MRI [Figure 2, Figure 3] provided correct diagnosis of both CAKUT and OHVIRA syndrome, being crucial for patient’s management and short and long-term follow-up. A rare congenital urogenital anomaly - uterus didelphys with obstructed hemivagina and ipsilateral renal agenesis (OHVIRA), known in the literature as Herlyn-Werner-Wunderlich (HWW) syndrome, was the final diagnosis.
According to the literature, we considered hemivaginal septal resection and anastomosis between the obstructed hemivagina and the normal vagina. However, escalating abdominal symptoms prompted us to perform laparoscopy simultaneously.
Family History
Medical, family, and psychosocial history of the patient including genetic information revealed no history of renal abnormalities.
Preoperative Management
Pre-operative management included psychological counselling of the patient and her family regarding treatment options, with detailed description of planned surgical approach. Before completion of the whole examinations, patient was given oral combined estrogen- progestin pill to block recurrent uterine blood flow, which could intensify abdominal symptoms.
Surgical Technique
The patient underwent combined laparoscopy and vaginoscopy. There was clinical evidence to suspect adnexal torsion and hematosalpinx, hence the laparoscopy was performed simultaneously. Vaginoscopy was done and with the help of resectoscope, a vertical incision was given and vaginal septum was excised and vaginal opening was extended. Intraoperative abdominal sonography was done for the appropriate evaluation of the place of resection [Figure 4, Figure 5.] Concomitant laparoscopy allowed abdominal cavity inspection and spontaneous drainage of hematosalpinx and hematometra was observed [Figure 6, Figure 7, Figure 8, Figure 9 and Figure 10]. Intravaginal catheter was placed for seven days to prevent early vaginal stenosis.
Follow- Up
The patient came for the health check in after one week and was followed up for prevention of the complications like vaginal stenosis and recurrence of obstruction. Hormonal therapy with combined estrogen-progesterone pill was administered to avoid heavy period and possible inflammation which could accelerate stenosis process. At 6 months follow-up, the patient was free from vaginal stenosis, rUTI and recurrence obstruction. We obtained written parental permission to present this case study.
Figure 1.
Ultrasound from extern hospital, when the diagnosis of hematocolpos was mistaken as ovarian cyst (black arrow). Double uterus was not recognized (white arrow).
Figure 1.
Ultrasound from extern hospital, when the diagnosis of hematocolpos was mistaken as ovarian cyst (black arrow). Double uterus was not recognized (white arrow).
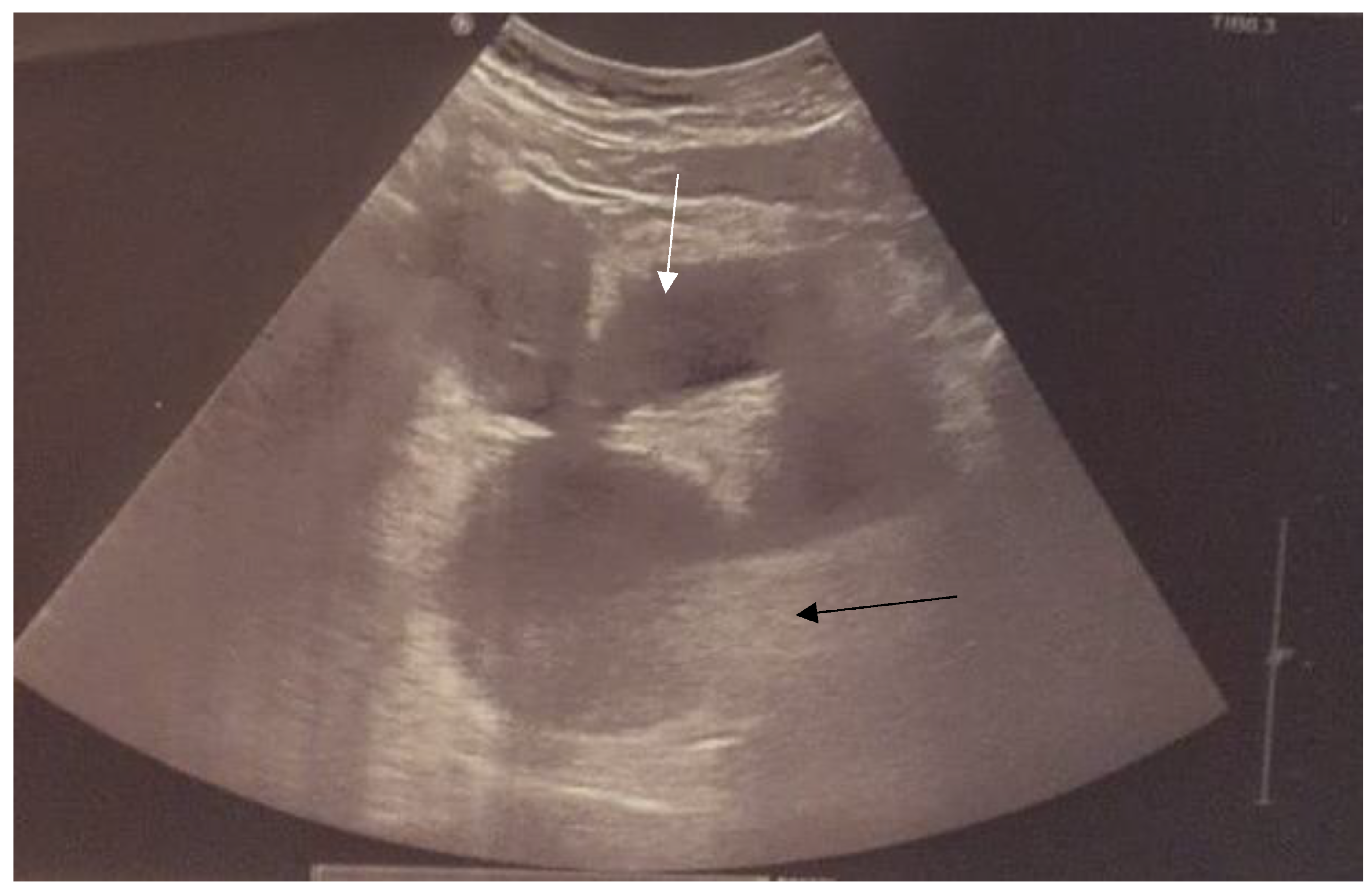
Figure 2.
MRI presents hematocolpos (blue arrow) and hydrometrocolpos in right uterus (white arrow).
Figure 2.
MRI presents hematocolpos (blue arrow) and hydrometrocolpos in right uterus (white arrow).
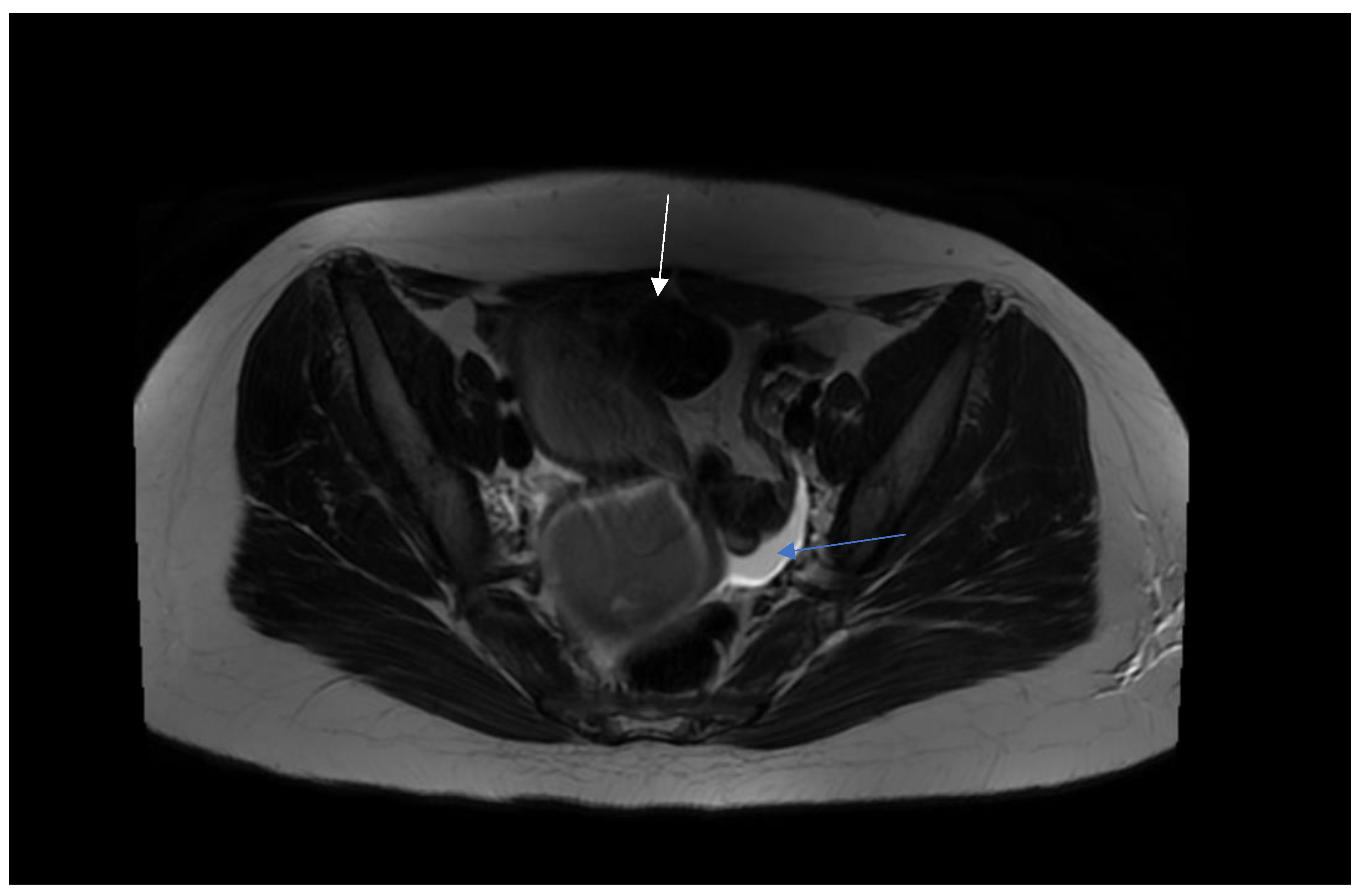
Figure 3.
MRI presents hematocolpos ( blue arrow) and left healthy uterus (white arrow).
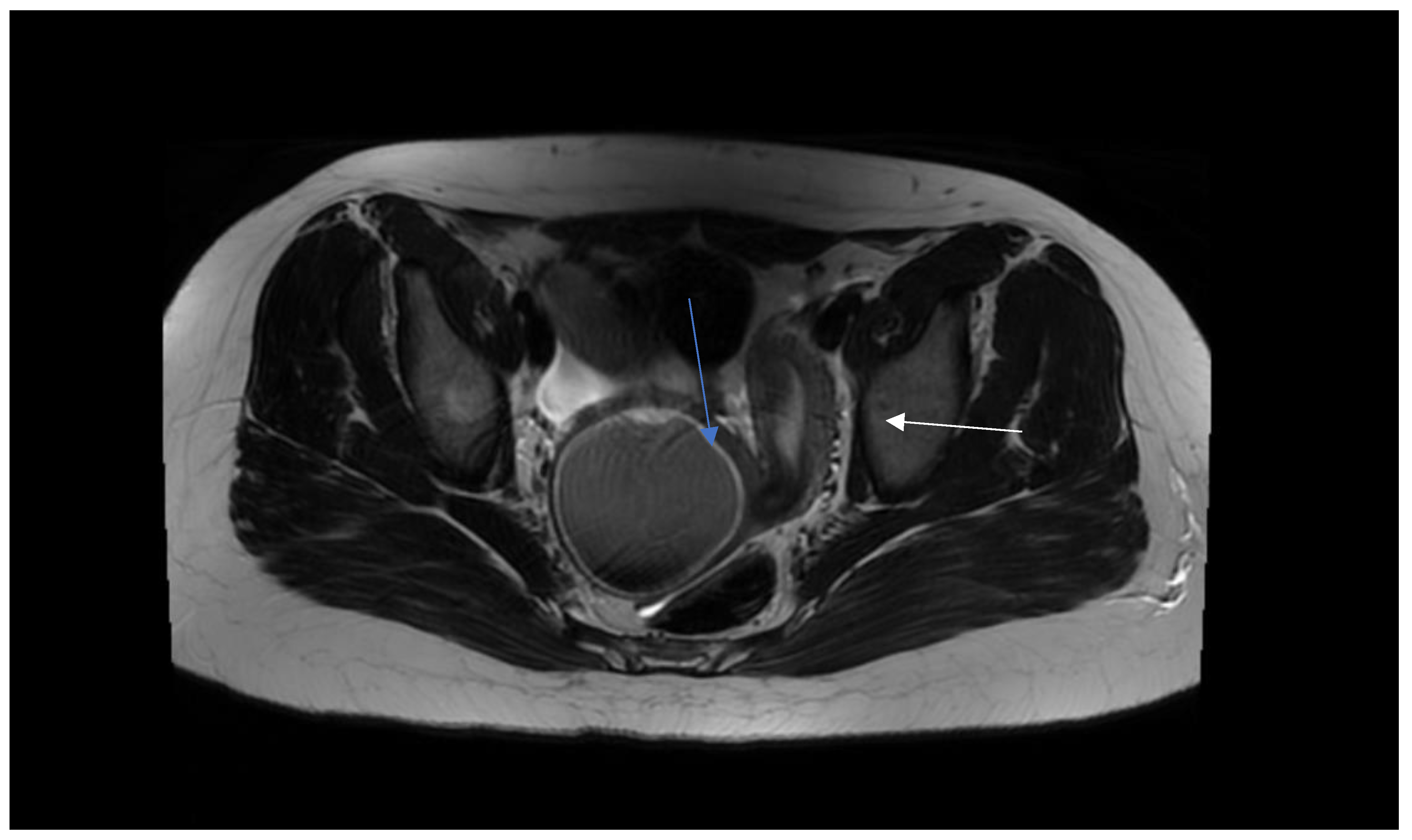
Figure 4.
Intraoperative abdominal sonography and puncture of hematocolpos (white arrow).
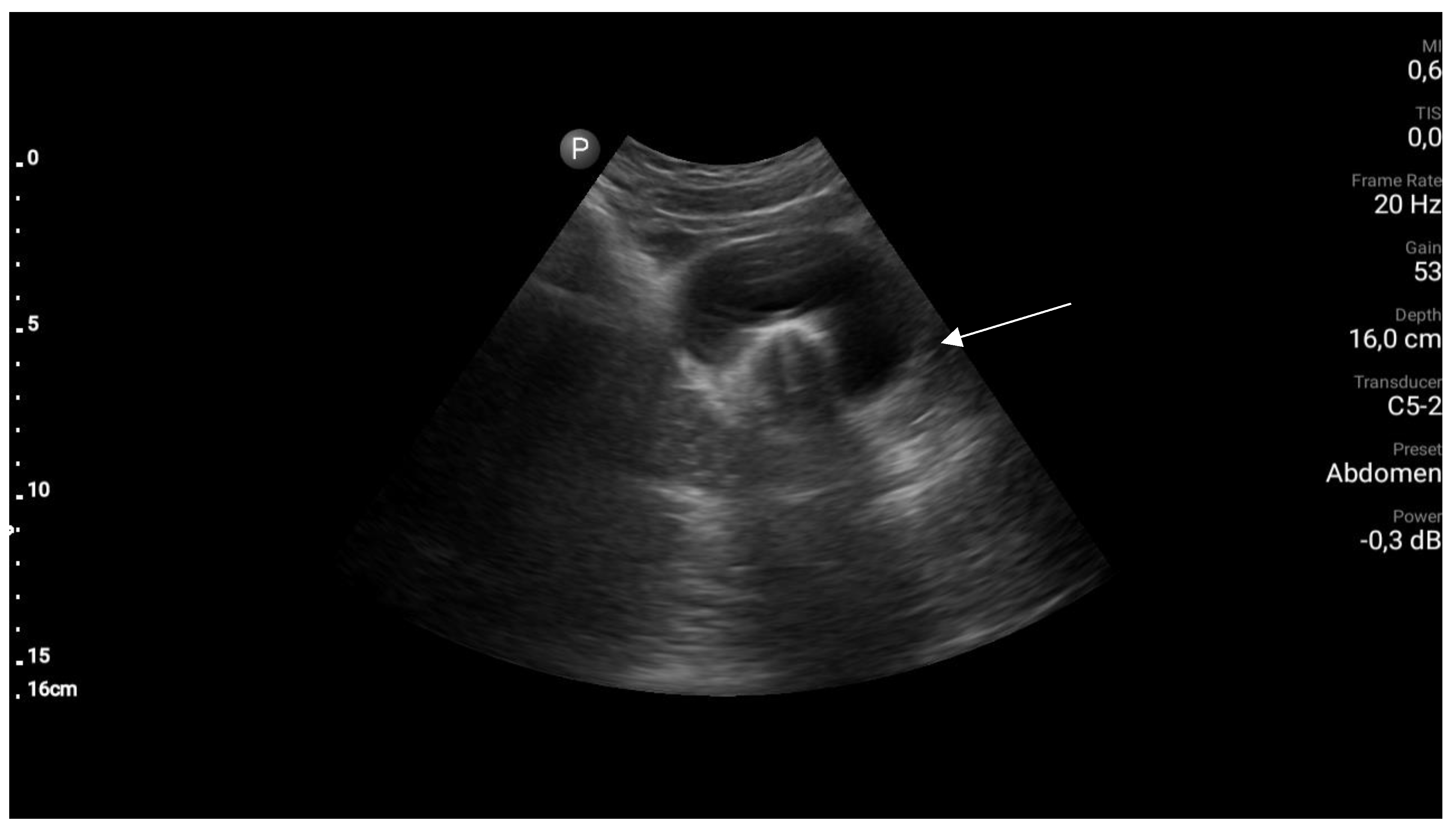
Figure 5.
Intraoperative abdominal sonography and drainage of hematocolpos.
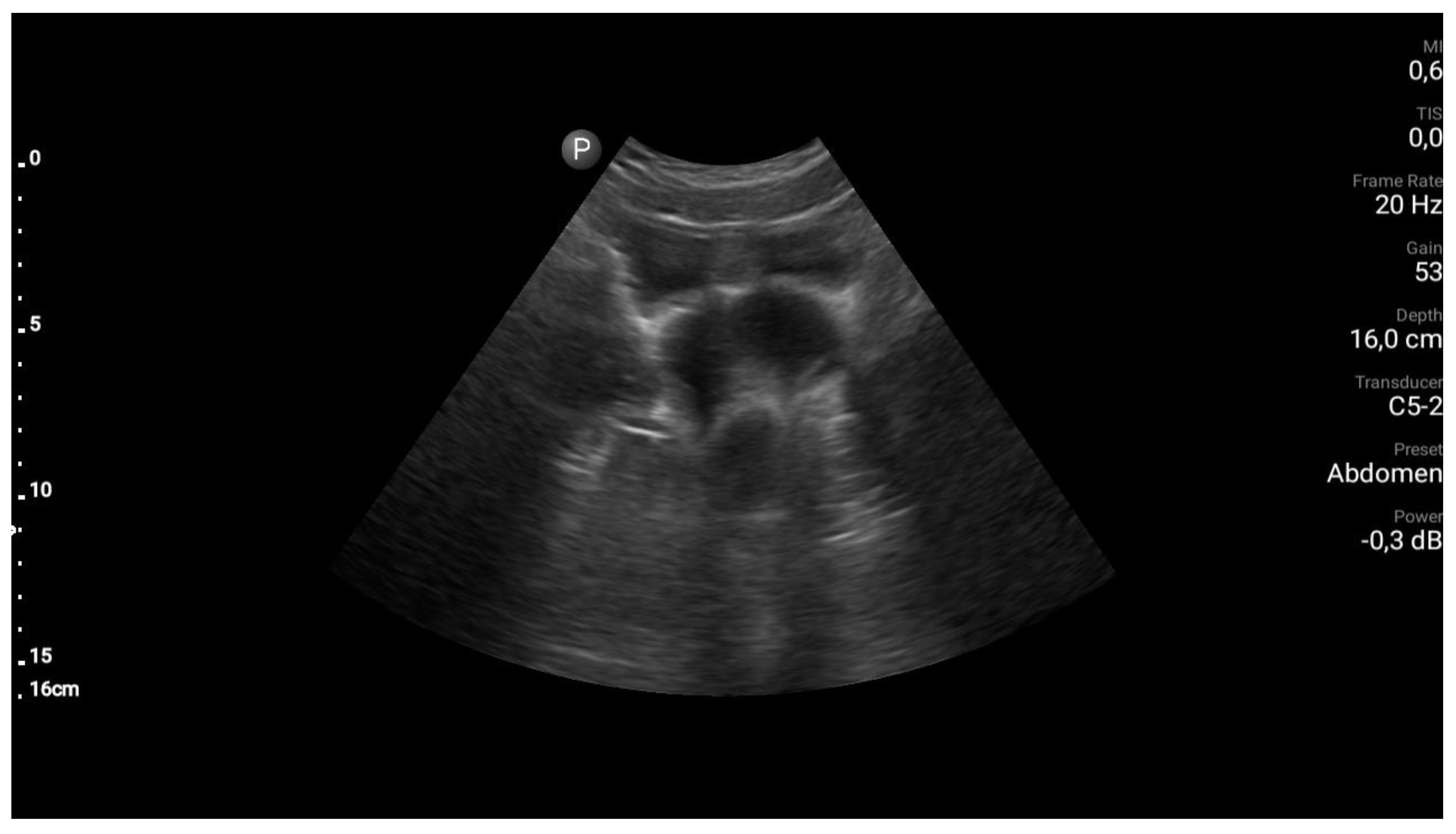
Figure 6.
Left healthy uterus in laparoscopic view.
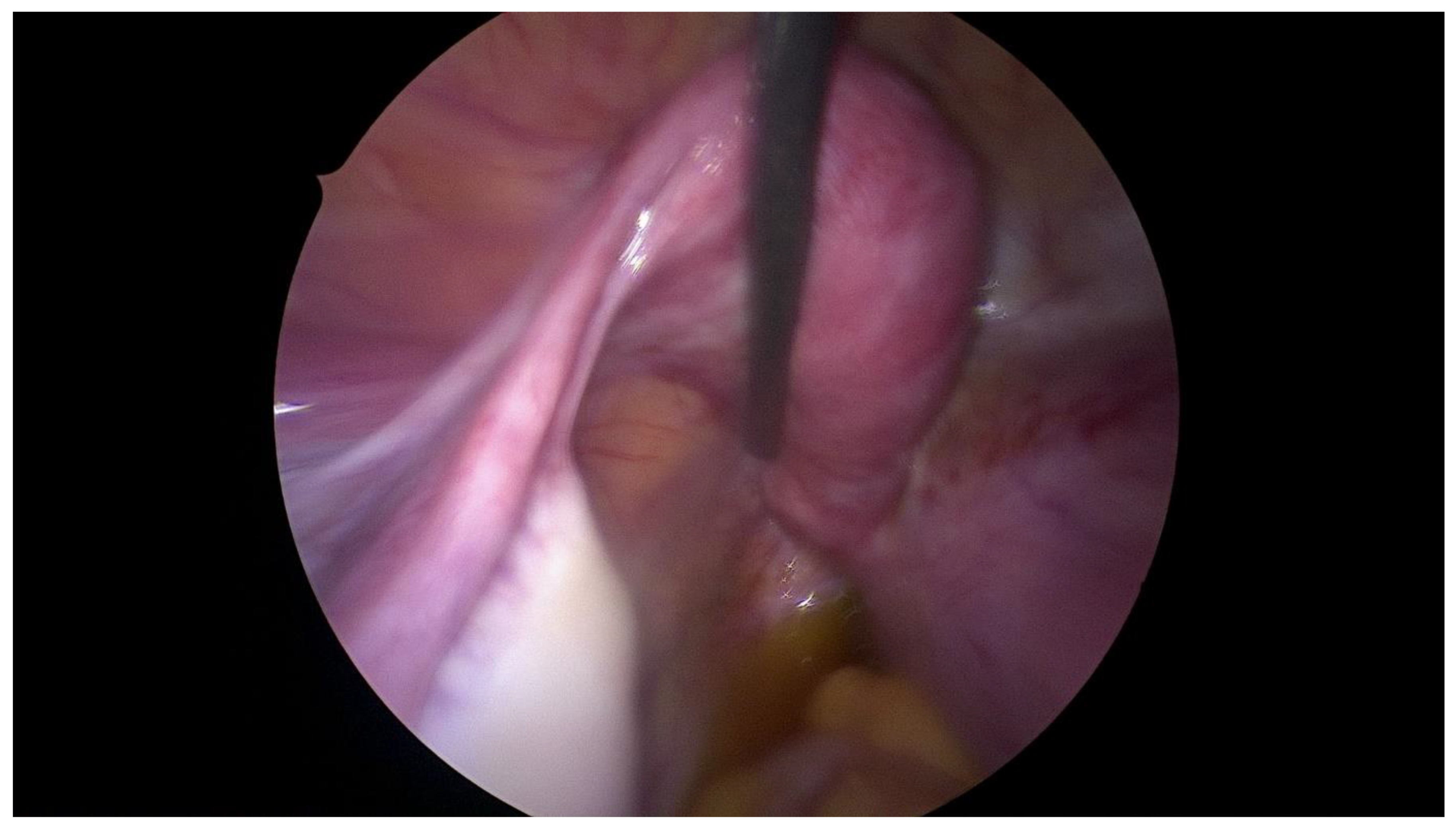
Figure 7.
Right uterus with hematometra in laparoscopic view.
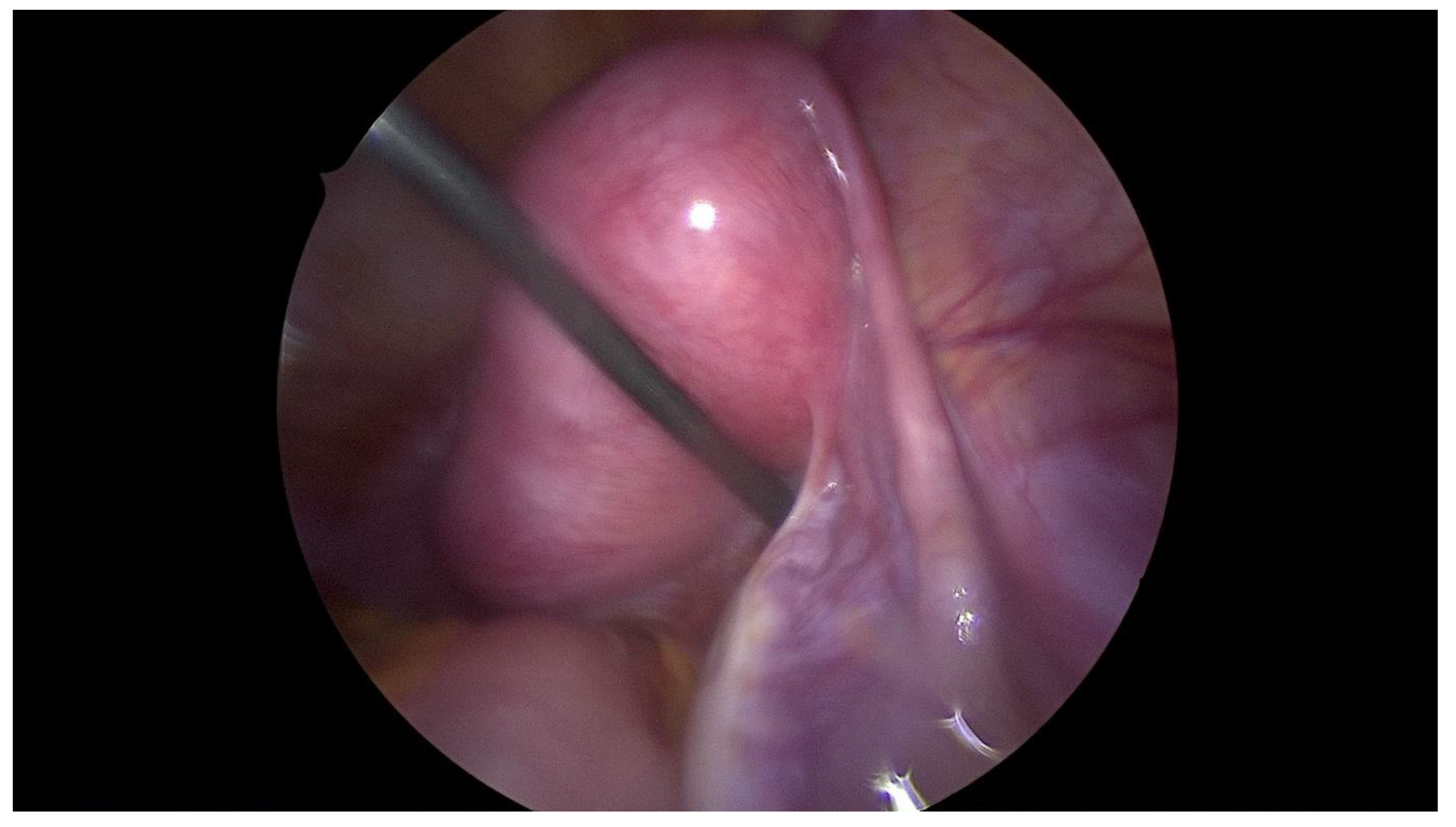
Figure 8.
Double uterus. Right uterus with hematometra.
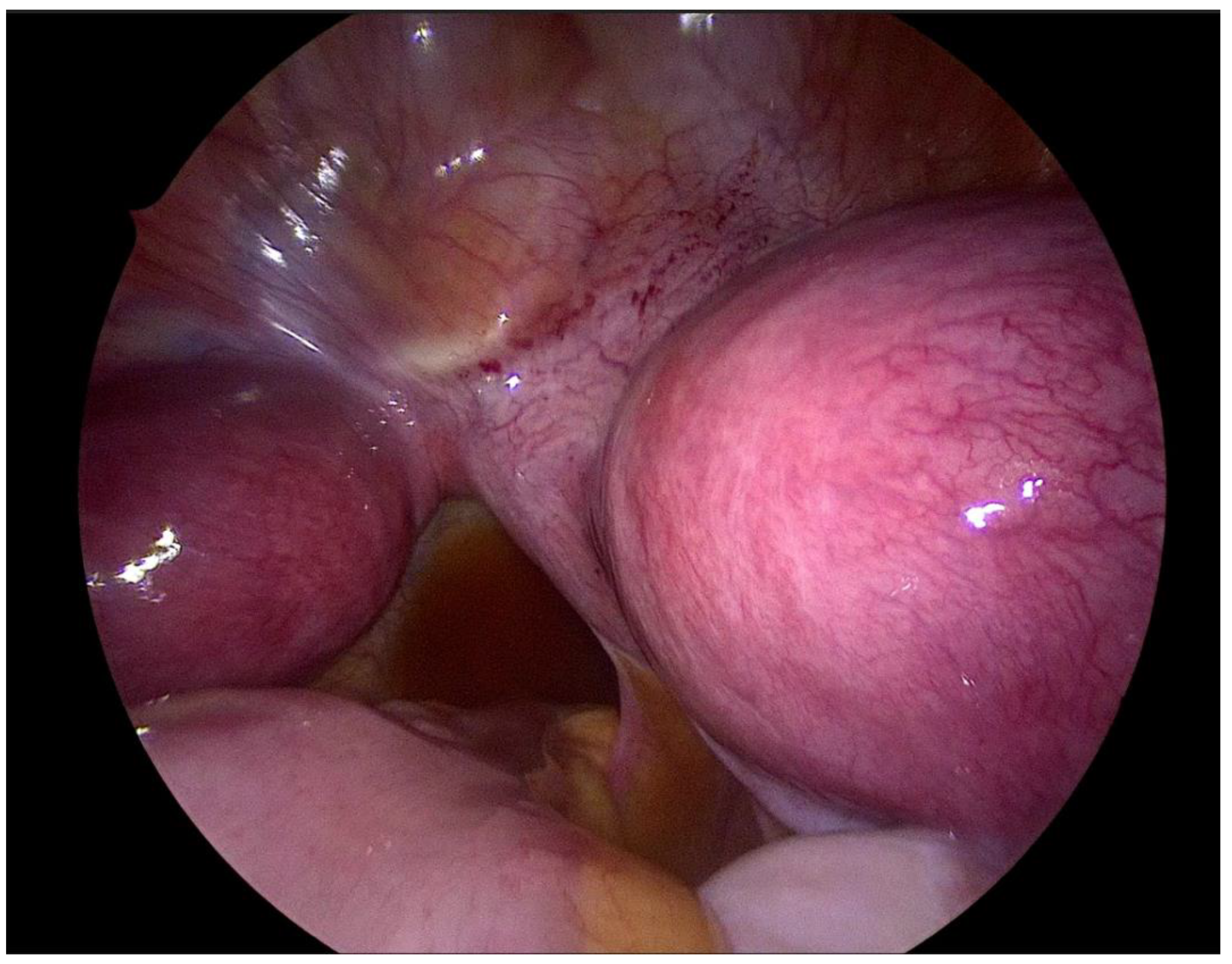
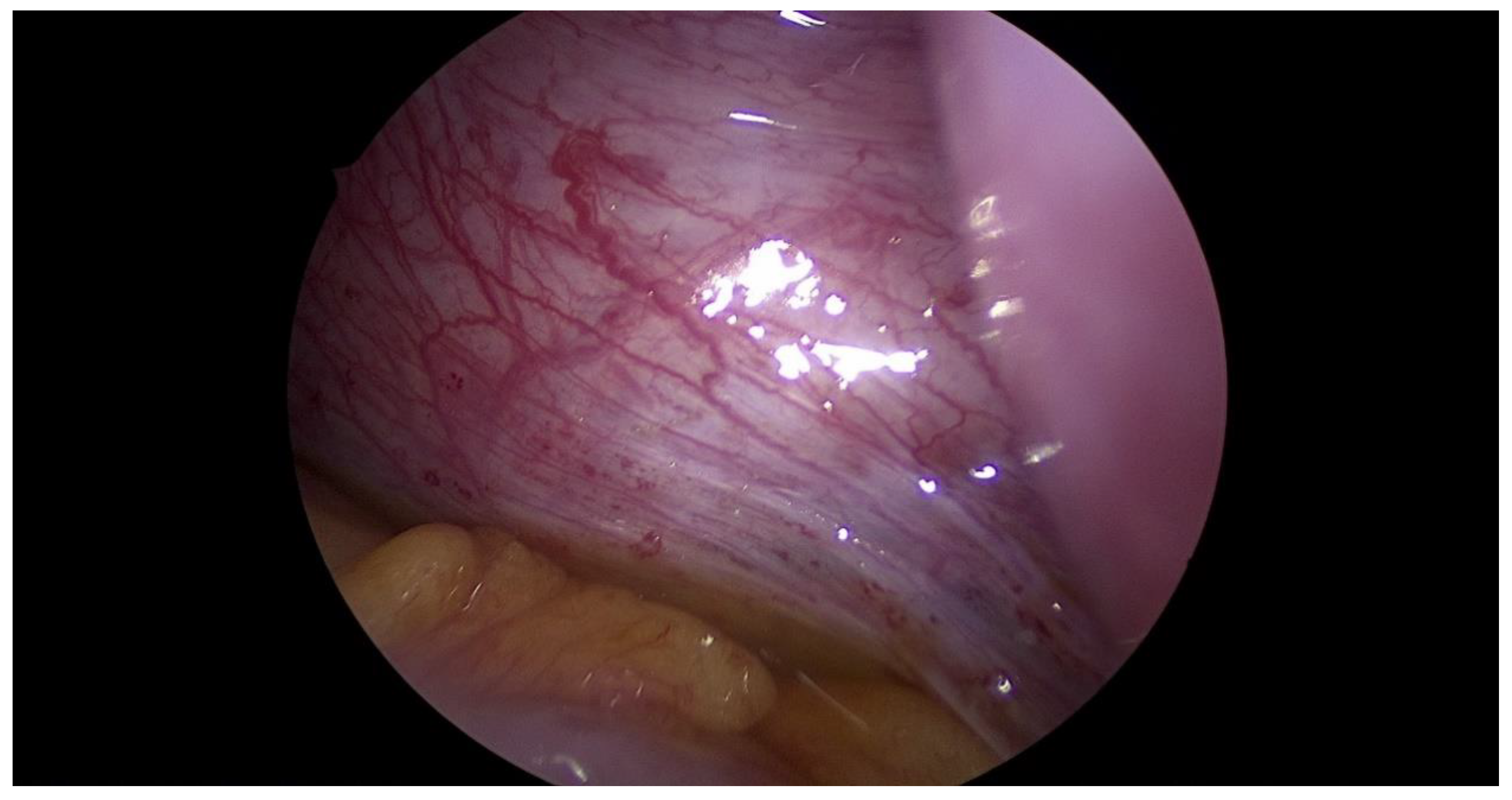
Figure 9.
Hematosalpinx of right fallopian tube.
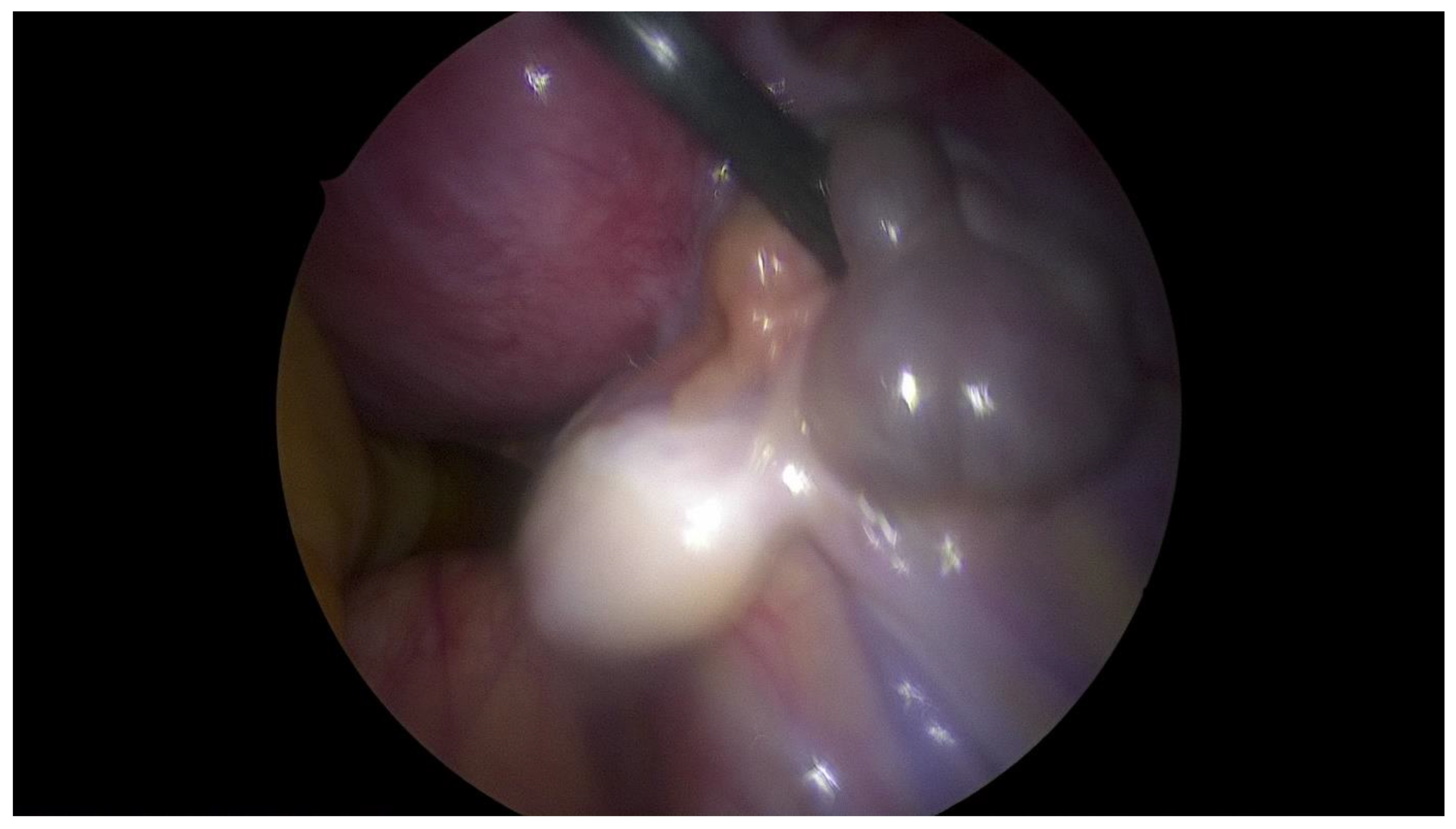
Figure 10.
Active endometriosis of peritoneum.
| Diagnostic and treatment flow-chart of OHVIRA syndrome |
|
Step 1. Preoperative management Patients age (mostly occurs in young females), accurate history: time of first period, gradually increased symptoms, the appearance of symptoms during menarche, symptoms increase with each subsequent period, recurrent UTI, urinary disorders [8,9]. Perform physical examination. Next to the transabdominal US, transperineal and transrectal US can be useful in emergency situations to accurately access the place of abnormality [10]. MRI imaging should be considered as "gold standard in the diagnostic process [11]. Plan of the surgery and step by step proceeding is important while operating patients with urogenital abnormalities. As interdisciplinary collaboration of urologist and gynecologist is often necessary to treat correctly these patients. |
|
Step 2. Preoperative management Preoperative counselling with patients, often with psychological assist is essential to support families. The information about future family planning and chanced of spontaneous pregnancy should be given precisely before the surgery [12]. However, hormonal therapy with continuous oral contraceptives should be considered in pre-operative management to give a time for preoperative preparation [13]. |
|
Step 3 Surgical management Surgery is necessary when acute abdominal symptoms are present. “Wait and see” approach is only possible when the clinical situation allows it. Perform laparoscopy and vaginoscopy in order to achieve the correct diagnosis and treat concomitant hematosalpinx and endometriosis [14]. Intraoperative US is helpful to evaluate the place of resection. Unnecessary lengthening the time to diagnosis, contributes to unindentent consequence. |
|
Step 4 Postoperative management The insertion of uterine catheter filled with saline into a place of stenosis allow to avoid the risk of possible restenosis [15]. Continuous oral contraceptives are recommended to avoid possible consequences like the risk of restenosis. |
|
Step 5 Postoperative management Pharmacological treatment with non-steroidal anti-inflammatory drugs (NSAIDS) should be avoided as they can cause the damage of renal structure [12]. |
|
Step 6 Follow- up At 6-12 month after the surgery, urologist re-counselling should be made to decide if the patient requires other imaging tests like uro-scintigraphy to evaluate the function of heathy kidney [2]. |
Figure 11.
Management flow-chart of patients with Obstructed HemiVagina with Ipsilateral Renal Agenesis (OHVIRA). Flowchart abbreviations : UTI- urinary tract infection, US-ultrasound.
Discussion
OHVIRA syndrome is a rare congenital urogenital anomaly derived from Mullerian tract abnormality [16]. The characteristic triad of this syndrome is didelphys uterus, obstructed hemivagina, and ipsilateral renal agenesis [16]. OHVIRA often accompanies with other anatomical disorders like longitudinal or transverse vaginal septum [17]. Also, renal agenesis, urinary retention or unexplained recurrent UTI’s should always awake surgeon’s attention for possible congenital anomalies. However, other accompanying renal anomalies, such as, renal dysplasia, a double collecting system, and ectopic ureter are possible, although only a limited number of such cases have been reported [18,19].
Symptoms like acute abdominal pain, dysmenorrhea, urinary disorders can mislead clinicians to make accurate diagnosis. Although rarely encountered, OHVIRA should be in the differential diagnosis of adolescent girls presenting with acute abdomen.
This case highlights the potential pitfalls and challenges in gynecologic surgery of adolescence. It also emphasizes that uterus didelphys with obstructed hemivagina (OHVIRA) should be considered in the differential diagnosis of adolescent girls presenting with acute abdomen, recurrent UTI and CAKUT [21]. We also aimed to highlight the role of detailed diagnostic process and correct management as crucial for the future family planning in OHVIRA patients.
Sometimes, a condition misinterpreted as dysmenorrhea and normal menstrual blood flow through the unobstructed hemivagina can delay reaching a correct diagnosis.1 Dysmenorrhea is reported by 30 – 90% of young female patients and "irregular menstrual bleeding" in up to 43% [22]. The presence of menarche does not mean that anatomical problem does not exist. Comprehensive interview with regard to medical history is an important part of diagnostic process. In the meanwhile, the first menstruation in our patient came from healthy uterus, which mislead the clinician to make a good diagnosis and excluded the anatomical cause of the symptoms.
Pelvic pain in young women adolescents is often a puzzle, and suspicion and knowledge about different causes are important for accurate diagnosis. As urogenital abnormalities are rare, they can be mistaken for ovarian cysts [23]. In our case second uterus was taken as ovarian cyst, what prolonged the diagnosis.
Recurrent UTI can be associated with specific women anomalies, but not - treated properly can lead to upper urinary tract infections like -glomerulo or – pyelonephritis [2,3,4,24]. Therefore, urinary tract disorders are usually a first sign of unrecognized urogenital tract disorders.
Often forgotten endometriosis in adolescence can provoke dysmenorrhea, chronic pelvic pain, and in consequence develop endometrial cysts, which could imitate large abdominopelvic masses [26].
Such abnormalities like vaginal septum, urogenital sinus, rudimentary horn, and other should be in mind when counselling a women adolescent with nonspecific symptoms. The need of precise follow up is necessary in patients with CAKUT, and it must be noted that renal agenesis and other could be associated with congenital anomalies of female reproductive organs [2].
MRI imaging is the gold standard for diagnosis with higher sensitivity in detecting the uterine morphology and the continuity of the vagina when compared to ultrasonography [6]. MRI may be useful to obtain a proper diagnosis and to plan the most correct surgical strategy.
However, high cost and sometimes long waiting time for the result, constitutes the limits of this investigation. In this case, abdominal sonography, which was thought to be suitable for virgins, misled the radiologist and congenital abnormality was mistaken for ovarian cyst. Urogenital anomalies may be overlooked, because of rare prevalence of these conditions. Transrectal sonography is feasible when transvaginal method cannot be performed, though it can be helpful, is rarely accepted by the young patients [26]. In the literature of transperineal ultrasound has been reported as non-invasive tool that could be used for the detection and characterization of the vaginal and perineal masses [27]. Furthermore, in the evaluation of vaginal pathologies, the use of three-dimensional / four-dimensional ultrasound should be considered, given its high sensitivity and specificity. [28].
Gynecologic surgeons face many challenges when considering complex gynecologic surgery, especially in children. Anticipating the intraoperative risks and carefully step by step surgical plan should be an integral part of each procedure in children with congenital anomalies.
To date, several surgical techniques for OHVIRA management have been reported, such as puncture of vaginal wall, single-stage vaginoplasty, mini-laparotomy even with unilateral hysterectomy, using of a vaginal mold or stent [8,29]. Septum and vaginal trauma which is often occurred because of using retractors lead to searching for new methods that will allow to reduce such complications. According to data new “No-touch” technique is safe and effective, provides good visualization and help to protect septum from trauma. Authors also decline lower risk of vaginal stenosis, adhesions and postoperative pain [29]. Grünberger described a modification of surgical approach, which called Z-plasty [30]. Van Bijsterveldt et al. proposed combined abdominal-vaginal method that can be used in patients with a higher risk of restenosis after surgery. Layman modified previous author technique by using balloon catheter to provide traction of vagina which prevented vagina stenosis [31].
Uterus didelphys do not increase the risk of miscarriage or preterm delivery. Surgical intervention is mainly performed in patients with uterine septum through combination of laparoscopic and hysteroscopic surgery. After this procedure, there are significant benefits in reducing the frequency of infertility, recurrent pregnancy loss, and adverse pregnancy outcomes. However, none of the procedures proved to be superior [32]. Recognizing anatomical abnormalities before the surgery is important when counseling patients before taking them to the operating room.
It is technically difficult to puncture the thick fibrotic tissue of hemivaginal septum with a needle. Due to such proceeding we expose the patient to unnecessary interventions, like minilaparotomy. Therefore, we offered our patient intraoperative abdominal sonography to directly evaluate the accurate and safe place of puncture and septal resection.
Minimally invasive surgery has acquired more and more space in the surgical panorama. Furthermore, it has many advantages in adolescent gynecology. Some of the authors discussed the role of laparoscopy in management of OHVIRA [18,32,33]. In our opinion, concomitant laparoscopic approach allows us to particulate evaluate small pelvis.
Hydrometrocolpos and associated with OHVIRA recurrent blood flow can develop hematosalpinx and in consequence endometriosis [34]. During laparoscopy we observed the drainage of hematosalpinx, therefore the efficacy of our treatment was ‘under eye’ control. We have also found active endometriosis lesions, what confirmed that late recognition of OHVIRA can have serious consequences.
The necessity of unilateral hysterectomy of one uterus is questionable. First of all, such procedure is not a simple one in children. Another point is the future family planning in patients with congenital anomalies.
In contrast to other authors, we believe that concomitant laparoscopic surgery is necessary in the surgical approach in OHVIRA patients [18,32]. Not only for clarification of diagnosis but also for the evaluation of pelvis anatomy and potential consequences of unrecognized disease like hematosalpinx and endometriosis. Perhaps, preoperative evolution of Ca-125 marker indicated possible development of early endometriosis. Furthermore, laparoscopic surgery allows intraoperative observation of drainage from the uterus and efficacy of our treatment.
Because of the higher risk of vaginal restenosis in patients with OHVIRA syndrome, there is a strong need of long-distance follow-up in such patients. Sometimes surgical resection is necessary. Early postoperative management with antibiotics and oral contraceptive are necessary to avoid vaginal infection and future restenosis.
Urologists should be aware that congenital anomalies of kidney and urinary tract (CAKUT) are often associated with female genitourinary disorders [35,36]. To avoid detrimental consequences of unrecognized congenital disease, early diagnosis and interdisciplinary team collaboration is necessary. Assessment of the prevalence of associated malformations in CAKUT may be important as it helps clinicians to ascertain a general and renal prognosis for these patients. Follow up of OHVIRA requires prolonged monitoring of solitary kidney function and guidance enabling satisfactory sexual intercourse and delivery. Girls with renal agenesis should be carefully monitored for possible genital tract anomalies and, conversely, girls with vaginal or uterine anomalies should be monitored for renal malformations[37].
This study has some limitations. First, most reports related to OHVIRA comprise only individual cases, which is caused by the rarity of this disorder. Only some studies showed a larger number of cases. Also some data from medical history were missing or the value of medical images were poor.
The purpose of this study was to outline correct management pathway and surgical approach concerning OHVIRA, which could vary not only due to anatomical differences, but also due to medical advances and the possibility of delayed diagnosis.
Conclusion
OHVIRA conditions may be associated to rUTI and CAKUT [38]. A careful evaluation of urinary tract should be recommended in OHVIRA patients. Delayed diagnosis may result with retrograde tubal reflux and endometriosis. Combined management of laparoscopy and vaginoscopy should be considered in all female patients with suspicion of congenital abnormalities as standard procedure [39]. Unrecognized and not properly treated congenital malformations of the vagina, cervix, and uterus, although rare may have severe implications for future family planning in OHVIRA patients [32]. After surgery, adolescent patients should undergo regular follow-up visits in order to prevent an adhesion formation recurrence after vaginal septum resection.
References
- Kagan, M.; Pleniceanu, O.; Vivante, A. The genetic basis of congenital anomalies of the kidney and urinary tract. Pediatr Nephrol. 2022, 37, 2231–2243. [Google Scholar] [CrossRef]
- Rodriguez, M.M. Congenital Anomalies of the Kidney and the Urinary Tract (CAKUT). Fetal Pediatr Pathol. 2014, 33, 293–320. [Google Scholar] [CrossRef]
- Capone, V.P.; Morello, W.; Taroni, F.; Montini, G. Genetics of Congenital Anomalies of the Kidney and Urinary Tract: The Current State of Play. Int J Mol Sci. 2017, 18, 796. [Google Scholar] [CrossRef]
- Salo, J.; Ikäheimo, R.; Tapiainen, T.; Uhari, M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011, 128, 840–847. [Google Scholar] [CrossRef]
- Van Dam, M.J.C.M.; Zegers, B.S.H.J.; Schreuder, M.F. Case Report: Uterine Anomalies in Girls With a Congenital Solitary Functioning Kidney. Front Pediatr. 2021, 9, 791499. [Google Scholar] [CrossRef]
- Gungor Ugurlucan, F.; Dural, O.; Yasa, C.; Kirpinar, G.; Akhan, S.E. Diagnosis, management, and outcome of obstructed hemivagina and ipsilateral renal agenesis (OHVIRA syndrome): Is there a correlation between MRI findings and outcome? Clin Imaging. 2020, 59, 172–178. [Google Scholar] [CrossRef]
- Sleiman, Z.; Wehbe, G.S.; Rassy, E.E.; Zreik, T.; Bitar, R.; Samaha, M.; et al. A novel surgical intervention for an uncommon entity: Laparoscopy-assisted resection of a vaginal septum in obstructed hemivagina and ipsilateral renal anomaly syndrome. J Laparoendosc Adv Surg Tech A. 2019, 29, 714–716. [Google Scholar] [CrossRef]
- Smith, N.A.; Laufer, M.R. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: Management and follow-up. Fertil Steril. 2007, 87, 918–922. [Google Scholar] [CrossRef]
- Kim, S.J.; Shim, S.Y.; Cho, H.H.; Park, M.H.; Lee, K.A. Prenatal Diagnosis of Fetal Obstructed Hemivagina and Ipsilateral Renal Agenesis (OHVIRA) Syndrome. Medicina (Kaunas). 2023, 59, 703. [Google Scholar] [CrossRef]
- Sijmons, A.; Broekhuizen, S.; van der Tuuk, K.; Verhagen, M.; Besouw, M. OHVIRA syndrome: Early recognition prevents genitourinary complications. Ultrasound. 2023, 31, 61–64. [Google Scholar] [CrossRef]
- Zhang, H.; Ning, G.; Fu, C.; Bao, L.; Guo, Y. Herlyn-Werner-Wun- derlich syndrome: Diverse presentations and diagnosis on MRI. Clin Radiol 2020, 75, 480–e17e25. [Google Scholar] [CrossRef]
- Gungor Ugurlucan, F.; Bastu, E.; Gulsen, G.; Kurek Eken, M.; Akhan, S.E. OHVIRA syndrome presenting with acute abdomen: A case report and review of the literature. Clin Imaging. 2014, 38, 357–359. [Google Scholar] [CrossRef] [PubMed]
- Cobec, I.M.; Rempen, A. OHVIRA-syndrome (Obstructed hemivagina with ipsilateral renal anomaly) as differential diagnosis of acute lower abdominal pain. Ann Ital Chir. 2023, 12, S2239253X23038720. [Google Scholar] [PubMed]
- Boyraz, G.; Karalo€k, A.; Turan, T.; et al. Herlyn-Werner- Wunderlich syndrome; laparoscopic treatment of obstructing longitudinal vaginal septum in patients with hematocolpos - a different technique for virgin patients. J Turk Ger Gynecol Assoc. 2020, 21, 303–304. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, M.; Zhang, Y.; Liu, H.; Yuan, P.; Peng, X.; et al. Proposal of the 3O (Obstruction, Ureteric Orifice, and Outcome) subclassification system associated with obstructed hemivagina and ipsilateral renal anomaly (OHVIRA). J Pediatr Adolesc Gynecol. 2020, 33, 307–313. [Google Scholar] [CrossRef]
- Mandava, A.; Prabhakar, R.R.; Smitha, S. OHVIRA syndrome (obstructed hemivagina and ipsilateral renal anomaly) with uterus didelphys, an unusual presentation. J Pediatr Adolesc Gynecol. 2012, 25, e23–e25. [Google Scholar] [CrossRef] [PubMed]
- Arakaki, R.; Yoshida, K.; Imaizumi, J.; Kaji, T.; Kato, T.; Iwasa, T. Obstructed hemivagina and ipsilateral renal agenesis (OHVIRA) syndrome: A case report. Int J Surg Case Rep. 2023, 107, 108368. [Google Scholar] [CrossRef]
- Gündüz, R.; Ağaçayak, E.; Evsen, M.S. OHVIRA syndrome presenting with acute abdomen findings treated with minimally invasive method: Three case reports. Acta Chir Belg. 2022, 122, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Prada Arias, M.; Muguerza Vellibre, R.; Montero Sánchez, M.; Vázquez Castelo JLArias González, M.; Rodríguez Costa, A. Uterus didelphys with obstructed hemivagina and multicystic dysplastic kidney. Eur J Pediatr Surg. 2005, 15, 441–445. [Google Scholar] [CrossRef]
- Gilsanz, V.; Cleveland, R.H.; Reid, B.S. Duplication of the müllerian ducts and genitourinary malformations. Part II: Analysis of malformations. Radiology. 1982, 144, 797–801. [Google Scholar]
- Zarfati, A.; Lucchetti, M.C. OHVIRA (Obstructed Hemivagina and Ipsilateral Renal Anomaly or Herlyn-Werner-Wunderlich syndrome): Is it time for age-specific management? J Pediatr Surg. 2022, 57, 696–701. [Google Scholar] [CrossRef]
- Karout, S.; Soubra, L.; Rahme, D.; Karout, L.; Khojah, H.M.J.; Itani, R. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Womens Health. 2021, 21, 392. [Google Scholar] [CrossRef]
- Bascietto, F.; Liberati, M.; Marrone, L.; Khalil, A.; Pagani, G.; Gustapane, S.; Leombroni, M.; Buca, D.; Flacco, M.E.; Rizzo, G.; Acharya, G.; Manzoli, L.; D'Antonio, F. Outcome of fetal ovarian cysts diagnosed on prenatal ultrasound examination: Systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2017, 50, 20–31. [Google Scholar] [CrossRef]
- Yu, J.-H.; Lee, S.-R.; Choi, H.; Kim, K.-S.; Kang, B.-M. A New Case of Herlyn–Werner–Wunderlich Syndrome: Uterine Didelphys with Unilateral Cervical Dysgenesis, Vaginal Agenesis, Cervical Distal Ureteral Remnant Fistula, Ureterocele, and Renal Agenesis in a Patient with Contralateral Multicystic Dysplastic Kidney. Diagnostics 2022, 12, 83. [Google Scholar]
- Benagiano, G.; Bianchi, P.; Guo, S.W. Endometriosis in adolescent and young women. Minerva ObstetGynecol. 2021, 73, 523–535. [Google Scholar] [CrossRef] [PubMed]
- Güdücü, N.; Sidar, G.; İşçi, H.; Yiğiter, A.B.; Dünder, İ. The utility of transrectal ultrasound in adolescents when transabdominal or transvaginal ultrasound is not feasible. J Pediatr Adolesc Gynecol. 2013, 26, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Kamal, E.M.; Lakhdar, A.; Baidada, A. Management of a transverse vaginal septum complicated with hematocolpos in an adolescent girl: Case report. Int J Surg Case Rep. 2020, 77, 748–752. [Google Scholar] [CrossRef]
- Kupesić, S.; Kurjak, A.; Skenderovic, S.; Bjelos, D. Screening for uterine abnormalities by three-dimensional ultrasound improves perinatal outcome. J Perinat Med. 2002, 30, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Subedi, J.; Zhang, A.; Johnson, G.; Zhao, X.; Xu, D.; Guan, X. Vaginoscopic Incision of Oblique Vaginal Septum in Adolescents with OHVIRA Syndrome. Sci Rep. 2019, 9, 20042. [Google Scholar] [CrossRef]
- Blanton, E.N.; Rouse, D.J. Trial of labor in women with transverse vaginal septa. Obstet. Gynecol. 2003, 101 (5 Pt 2), 1110–1112. [Google Scholar]
- Van Bijsterveldt, C.; Willemsen, W. Treatment of patients with a congenital transversal vaginal septum or a partial aplasia of the vagina. The vaginal pull-through versus the push-through technique. J. Pediatr. Adolesc. Gynecol. 2009, 22, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Kudela, G.; Wiernik, A.; Drosdzol-Cop, A.; Machnikowska-Sokołowska, M.; Gawlik, A.; Hyla-Klekot, L.; Gruszczyńska, K.; Koszutski, T. Multiple variants of obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome - one clinical center case series and the systematic review of 734 cases. J Pediatr Urol. 2021, 17, 653–e1. [Google Scholar] [CrossRef] [PubMed]
- Kriplani, A.; Dalal, V.; Kachhawa, G.; Mahey, R.; Yadav, V.; Kriplani, I. Minimally Invasive Endoscopic Approach for Management of OHVIRA Syndrome. J Obstet Gynaecol India. 2019, 69, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, S.K.; Misra, R.; Thukral, B.B.; Gupta, R. OHVIRA: Uterus didelphys, blind hemivagina and ipsilateral renal agenesis: Advantage MRI. J Hum Reprod Sci. 2012, 5, 67–70. [Google Scholar] [CrossRef]
- Samanta, A.; Rahman, S.M.; Vasudevan, A.; Banerjee, S. A novel combination of OHVIRA syndrome and likely causal variant in UMOD gene. CEN Case Rep. 2023, 12, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.S.; Stefanovici, C. Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) - A Fetal Autopsy Case. J Pediatr Adolesc Gynecol. 2022, 35, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Saleem, S.N. MR imaging diagnosis of uterovaginal anomalies: Current state of the art. Radiographics. 2003, 23, e13. [Google Scholar] [CrossRef]
- Kim, Y.N.; Han, J.H.; Lee, Y.S.; Lee, I.; Han, S.W.; Seo, S.K.; Yun, B.H. Comparison between prepubertal and postpubertal patients with obstructed hemivagina and ipsilateral renal anomaly syndrome. J Pediatr Urol. 2021, 17, 652–e1. [Google Scholar] [CrossRef]
- Paul, P.G.; Sudhakar, M.; Shah, M.; Chowdary, V.S.; Paul, G. Vaginoscopic Management of OHVIRA (Obstructive Hemivagina and Ipsilateral Renal Agenesis). J Minim Invasive Gynecol. 2023, 30, 361–362. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



