
Submitted:
11 October 2023
Posted:
12 October 2023
You are already at the latest version
Abstract
A total of 137 HCC patients treated with atezolizumab plus bevacizumab from October 2020 to September 2022 were enrolled. The median overall survival (OS) and progression-free survival (PFS) from the beginning of atezolizumab plus bevacizumab was 21.1 months (range, 18.8 months-not reached) and 10.5 months (range, 8.2‒12.1 months), respectively. Fifty patients were diagnosed with progressive disease after atezolizumab plus bevacizumab. Of this group, 24 patients were administered lenvatinib, and the median OS and PFS from the beginning of lenvatinib were 15.3 months (range, 10.3 months-not reached) and 4.0 months (range, 2.5‒6.4 months), respectively. The objective response rates based on response evaluation criteria in solid tumors (RECIST) criteria version 1.1 and modified RECIST were 33.3% and 54.2%, respectively. On multivariate analysis, Child-Pugh class A (hazard ratio 0.02, 95% confidence interval (CI) 0.02‒0.76, p = 0.02) and intrahepatic tumor occupancy rate <50% (hazard ratio <0.01, 95% CI 0.003‒0.35, p <0.01) were the significant factors for OS. There were some frequent adverse events (AEs) in patients treated with lenvatinib such as hypertension, fatigue, anorexia, proteinuria, and so on, but none directly caused death. In conclusion, lenvatinib after atezolizumab plus bevacizumab for unresectable HCC should be considered an effective treatment option.
Keywords:
hepatocellular carcinoma
; unresectable
; atezolizumab plus bevacizumab
; lenvatinib
1. Introduction
Primary liver cancer is the sixth most diagnosed cancer worldwide and hepatocellular carcinoma (HCC) accounts for more than 90% of primary liver cancers [1]. In Japan, the treatment strategy for HCC depends on the Japan Society of Hepatology (JSH) HCC Guidelines 2021 published by the JSH. The treatment algorithm is based on liver function, metastasis, vascular invasion, tumor number, and tumor size. Systemic therapy is the cornerstone of management for patients with advanced and unresectable HCC who are not suitable for locoregional therapies, such as surgical resection or radiofrequency ablation. Until 2018, the only systemic therapy for unresectable HCC was sorafenib, a tyrosine kinase inhibitor (TKI) [2], but several phase III trials recently resulted in the approval of multiple drug therapies [3-6]. The REFLECT trial was a phase III clinical trial evaluating the noninferiority of lenvatinib to sorafenib in first-line treatment of unresectable HCC. The primary endpoint of overall survival (OS) was noninferiority, and the secondary endpoints of progression-free survival (PFS), time to progression, and objective response rate (ORR) were significantly better for lenvatinib [3].
Since 2020, atezolizumab plus bevacizumab was positioned as a first-line systemic drug therapy for unresectable HCC because it significantly prolonged OS and PFS compared with sorafenib in the IMbrave 150 trial [7]. At American Society of Clinical Oncology-Gastrointestinal (ASCO-GI) 2021, an updated analysis of the IMbrave150 trial reported OS of 19.2 months and PFS of 6.9 months. The establishment of second-line therapy after atezolizumab plus bevacizumab combination therapy is an urgent issue. However, the time is short since the benefit of atezolizumab plus bevacizumab combination therapy was demonstrated, and the development of second-line therapy for unresectable HCC has been conducted in patients who failed first-line sorafenib therapy. Thus, an effective regimen after atezolizumab plus bevacizumab combination therapy has not been established at present.
In this report, the effectiveness of lenvatinib as second-line therapy after atezolizumab plus bevacizumab is demonstrated.
2. Materials and Methods
2.1. Patients
The flow chart of this study is shown in Figure 1. There were 137 patients treated with atezolizumab plus bevacizumab for unresectable HCC from October 2020 to September 2022 at Hiroshima University Hospital and affiliated hospitals. First, their patient records were examined, and the clinical data obtained at the start of atezolizumab plus bevacizumab were collected. In addition, OS and PFS from the beginning of atezolizumab plus bevacizumab were evaluated.
Next, patients were selected to evaluate lenvatinib after atezolizumab plus bevacizumab. Of the 137 patients, 87 patients were interrupted for the following reasons: 9 patients were diagnosed as having complete response (CR), 11 patients had adverse events (AEs), 10 patients showed decreased performance status, 9 patients had decreased liver function, 7 patients did not wish to be treated, and 5 patients dropped out because of other diseases. Thirty-six patients continued atezolizumab plus bevacizumab. Fifty patients were diagnosed as having progressive disease (PD), and of them, 23 patients were treated by other treatments: 19 with transcatheter arterial chemo embolization, 2 with radiation, and 1 with ramucirumab, and 1 had peritoneal seeding. Three patients opted for best supportive care. A total of 24 patients treated with lenvatinib after atezolizumab plus bevacizumab were evaluated. Clinical characteristics and therapeutic response, including OS, PFS, and the ORR, univariate and multivariate analyses of lenvatinib for OS, and AEs, were analyzed retrospectively.
2.2. Treatment Regimens
Regarding atezolizumab plus bevacizumab, patients received 1200 mg of atezolizumab plus 15 mg of bevacizumab per kilogram of body weight, intravenously every 3 weeks. For lenvatinib, patients received full dose (12 mg/day for body weight ≥60 kg, 8 mg/day for body weight < 60 kg) until withdrawal of consent, death, disease progression, worsening of liver function, or unacceptable toxicity.
2.3. Efficacy Assessment
To determine the patients’ response to treatment, dynamic computed tomography (CT) or magnetic resonance imaging was performed every 1‒3 months, and serum alpha-fetoprotein (AFP) and des-gamma-carboxyprothrombin (DCP) levels were also measured every 1-3 months. Treatment response was assessed by a hepatologist and a radiologist according to response evaluation criteria in solid tumors (RECIST) criteria version 1.1 and modified RECIST (mRECIST) [8] with four response categories: CR, partial response (PR), stable disease (SD), and PD. The ORR was defined as the sum of the patients who attained CR and those who attained PR, and the disease control rate (DCR) was defined as the sum of ORR and SD. The DCR and the ORR were determined by with the best response recorded from the beginning of treatment until disease progression or recurrence occurred. Treatment-related AEs were assessed according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0.
2.4. Statistics
OS and PFS were calculated by the Kaplan-Meier method and analyzed by the log-rank test. OS and PFS were assessed by calculating from the dates of treatment initiation to the date of the last follow-up or death and the date of recurrence, respectively. A Cox proportional hazards model was used to analyze the factors contributing to OS and PFS. A p-values of <0.05 were considered statistically significant. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Japan), which is a graphical user interface for R (The R Foundation for Computing, version 3.4.1).
3. Results
3.1. Patients’ Background Characteristics and Outcomes from the Beginning of Atezolizumab Plus Bevacizumab
The patients’ background characteristics at the beginning of atezolizumab plus bevacizumab are shown in Table 1. The median age was 75 years (range, 47‒92 years); 107 were males, and 30 were females. The etiologies of liver cirrhosis were hepatitis B virus in 15 (10.9%), hepatitis C virus in 48 (35.0%), hepatitis B virus and hepatitis C virus in 2 (1.5%), and non-B, non-C viral in 72 (52.6%) patients. The Child-Pugh scores were 5 and 6 in 84 (61.3%) and 53 (38.7%) patients, respectively. The modified albumin-bilirubin (mALBI) grades were 1, 2a, and 2b in 52 (38.0%), 45 (32.8%), and 40 (29.2%), respectively. Relative tumor volume <50% and ≥50% was seen in 130 (94.9%) and 7 (5.1%) patients, respectively. The median size of the liver tumor was 28 mm (range, 0‒220 mm). The HCC stages were II, III, IVa, and IVb in 33 (24.1%), 50 (36.5%), 22 (16.1%), and 32 (23.4%) patients, respectively. Barcelona Clinic Liver Cancer (BCLC) stages were A, B, and C in 8, 63, and 66 patients, respectively. The median AFP was 18.1 ng/ml (range, 1.2‒63,642 ng/ml). The median DCP was 236 mAU/ml (range, 11‒197,680 mAU/ml). The median observation period on atezolizumab plus bevacizumab was 11.7 months (range, 1‒28 months).
Figure 2 shows OS and PFS from the beginning of atezolizumab plus bevacizumab. The median survival time (MST) was 21.1 months (95% confidence interval [CI], 18.8 months – not reached). The median PFS was 10.5 months (95% CI, 8.2 months – 12.1 months).
3.2. Patients’ Background Characteristics and Outcomes after Progression on Atezolizumab Plus Bevacizumab
Patients’ background characteristics at the time of diagnosis of progressive disease on atezolizumab plus bevacizumab are shown in Table 2. Systemic therapies after atezolizumab plus bevacizumab were lenvatinib (n=24) and ramucirumab (n=1).
Figure 3 shows post progression survival with atezolizumab plus bevacizumab. The median survival time was 12.5 months (95% CI, 9.3 months – not reached).
The patients’ background characteristics at the beginning of lenvatinib after atezolizumab plus bevacizumab are shown in Table 3. The Child-Pugh grades were A and B in 18 (75%) and 6 (25%) patients, respectively. The mALBI grades were 1, 2a, 2b, and 3 in 8 (33.3%), 6 (25%), 7 (29.2%), and 3 (12.5%) patients, respectively. The median time from the last atezolizumab plus bevacizumab to lenvatinib administration was 17 days.
Figure 4 shows OS and PFS of lenvatinib after progressive disease on atezolizumab plus bevacizumab. MST was 15.3 months (95% CI, 10.5 months – not reached), and median PFS was 4.0 months (95% CI, 2.5‒6.4 months).
3.3. Antitumor Response to Lenvatinib Administration Following Atezolizumab Plus Bevacizumab.
Table 4 shows the radiological responses to lenvatinib assessed according to the RECIST criteria version 1.1 and mRECIST. Eight (33.3%) patients achieved PR, 10 (41.7%) SD, and 5 (20.1%) developed PD, with an ORR of 33.3% and DCR of 75.0%. On the other hand, using the mRECIST criteria, 1 (4.2%) patient achieved CR, 12 (50.0%) patients achieved PR, 6 (25.0%) patients had SD, and 4 (16.7%) patients developed PD, with an ORR of 54.2% and DCR of 79.2%. It was not possible to evaluate RECIST and mRECIST in one patient because CT was not performed.
3.4. Prognostic Factors for OS and PFS on Lenvatinib
Table 5 shows the prognostic factors for OS in patients on lenvatinib with progressive disease after first-line atezolizumab plus bevacizumab. On univariate analysis, factors contributing to OS on lenvatinib were the Child-Pugh class and the intrahepatic tumor occupancy rate. On multivariate analysis, the following were independent factors contributing to OS on lenvatinib: Child-Pugh class A (hazard ratio [HR], 0.14; 95% CI, 0.02–0.76; p = 0.02) and intrahepatic tumor occupancy rate less than 50% (HR, 0.03; 95% CI, 0.003–0.35; p < 0.01).
OS on lenvatinib by Child-Pugh class was 17.5 months with class A and 10.5 months with class B, and that by intrahepatic tumor occupancy rate was 17.5 months with less than 50% and 5.6 months with greater than or equal to 50% (Figure 5).
On the other hand, there were no significant prognostic factors for PFS on lenvatinib on univariate or multivariate analysis.
3.5. Treatment-Related Toxicities
Table 6 shows the AEs of lenvatinib after atezolizumab plus bevacizumab. AEs were observed in all patients. The most common AE was hypertension (15 patients, 62.5%), which was easily treated with antihypertensive therapy. Fatigue was the second most common AE (14 patients, 58.3%). Anorexia (45.8%), diarrhea (41.7%), proteinuria (29.2%), and hand-foot syndrome (29.2%) were also observed. Although there were some patients who had grade 3 or 4 AEs, no patients died because of AEs.
4. Discussion
In the present study, the efficacy of lenvatinib as second-line therapy after atezolizumab plus bevacizumab for patients with unresectable HCC was examined. The American Society of Clinical Oncology (ASCO) guidelines state that second-line treatment with TKIs such as sorafenib, lenvatinib, cabozantinib, and regorafenib may be feasible after first-line atezolizumab plus bevacizumab therapy, but the level of evidence for such treatment is low [9]. The ASCO guidelines state that the choice of second-line therapy should be based on patient and clinician preference, comorbidities, general condition, and benefit of therapy. The European Society for Medical Oncology clinical practice guideline recommends sorafenib, lenvatinib, regorafenib, cabozantinib, and ramucirumab all side by side as second-line therapy after atezolizumab plus bevacizumab combination therapy [10]. The American Association for the Study of Liver Diseases has a flowchart showing atezolizumab plus bevacizumab as first-line therapy, sorafenib and lenvatinib as second-line therapy, and regorafenib, cabozantinib, and ramucirumab as third-line therapy [11]. Clinical practice guidelines for hepatocellular carcinoma of The Japan Society of Hepatology (4th JSH-HCC guidelines) listed atezolizumab plus bevacizumab as first-line, sorafenib and lenvatinib as second-line, and regorafenib, cabozantinib, and ramucirumab as third-line. In addition, in the 2021 edition of the JSH-HCC guidelines, the combination of atezolizumab plus bevacizumab was selected as the first-line therapy, and sorafenib, lenvatinib, regorafenib, cabozantinib, and ramucirumab were all treated in parallel as second-line therapies. All guidelines have in common the recommendation of sorafenib or lenvatinib as first-line therapy and regorafenib, cabozantinib, or ramucirumab as second-line or later therapy when the combination of atezolizumab plus bevacizumab is difficult to use due to autoimmune disease or other reasons.
Recently, network analyses of OS and PFS have been reported for various molecular-targeted agents (MTAs) and immune checkpoint inhibitors (ICIs) for unresectable HCC, by first-line and second-line treatment [12,13]. However, there have been no randomized, controlled trials in patients after atezolizumab plus bevacizumab, and given that the REFLECT trial comparing sorafenib and lenvatinib was a non-inferiority trial, it is considered that sorafenib, lenvatinib, regorafenib, cabozantinib, and ramucirumab in patients with AFP >400 ng/ml are all candidate second-line therapies.
Although there is no established evidence for second-line therapy after first-line atezolizumab plus bevacizumab combination therapy for unresectable HCC, the present study showed the efficacy and safety of subsequent systemic therapy in patients who progressed on first-line atezolizumab-bevacizumab. In the present study, the response rate to lenvatinib was 33.3% by RECIST and 54.2% by mRECIST in the 24 patients. Although PFS was 4.0 months, OS after atezolizumab plus bevacizumab was 15.3 months. In the REFLECT trial, the ORR of lenvatinib by mRECIST was 40.6%, and the median OS was 13.6 months, so the present results showed better outcomes. On multivariate analysis, the patients with good liver function before lenvatinib after atezolizumab plus bevacizumab and those with low intrahepatic tumor volume showed significant differences, contributing to the good therapeutic effect of lenvatinib after atezolizumab plus bevacizumab. Therefore, it is important to be careful not to decrease liver function with atezolizumab plus bevacizumab. In addition, the therapeutic effect of lenvatinib after atezolizumab plus bevacizumab was found to be good when the tumor occupied a small percentage of the liver. Regarding AEs, hypertension, fatigue, anorexia, diarrhea, proteinuria, and hand-foot syndrome were seen in the present study, and they were similar to the side effects seen in the REFLECT study. Therefore, it was found that the AEs of lenvatinib after atezolizumab plus bevacizumab were comparable to those of lenvatinib alone.
One of the reasons why the combination of TKIs such as lenvatinib and ICIs such as atezolizumab plus bevacizumab are effective for HCC is due to VEGF inhibition. HCC is a hypervascular tumor and is known to express high levels of VEGF [14]. In addition, VEGF is known to be associated with immunosuppression in the tumor microenvironment during the cancer immune cycle, creating an environment in which CD8-positive (CD8+) T cells are ineffective [15,16]. Specifically, VEGF suppresses dendritic cell maturation and T cell activation in lymph nodes, inhibits CD8+ T cell infiltration into tumors, and differentiates and induces immunosuppressive cells such as regulatory T cells (Tregs). VEGF inhibition may release these factors, thereby creating an environment in which CD8+ T cells can exert their effects.
Abundant infiltration of CD8+ T cells in tumor tissue is considered important for ICIs to have a good therapeutic effect. It has also been reported that ICIs are less effective when there are many Tregs present that suppress the function of effector T cells such as CD8+ T cells, etc. To increase the efficacy of ICIs, it is important to balance the tumor microenvironment with a predominance of CD8+ cells over Tregs by inhibiting VEGF, as bevacizumab does. Similar to bevacizumab, lenvatinib is a multikinase inhibitor that targets not only VEGF receptors 1–3, but also fibroblast growth factor receptors 1–4, platelet-derived growth factor receptor alpha, rearranged during transfection, and KIT [17-20]. Therefore, the therapeutic effect of atezolizumab is expected to be enhanced by the VEGF inhibitory effect of lenvatinib.
It has been reported that a method to monitor the binding of anti-PD-1 antibodies to CD8+ T cells was found, and anti-PD-1 antibodies remains bound to CD8+ T cells for more than 20 weeks after patients stop treatments [21]. Therefore, it is assumed that the therapeutic effect of lenvatinib was added to the prolonged effect of the ICIs, and that it exerted its effect on immune cells and tumor cells.
Another reason why lenvatinib showed therapeutic efficacy after atezolizumab plus bevacizumab is that lenvatinib worked for ICI-refractory HCC. Factors that contribute to ICI refractoriness include Wnt/β-catenin signaling. It has been reported that HCC patients treated with ICIs was associated with lower DCR, shorter median PFS, and shorter median OS if they had altered activation of Wnt/β-catenin signaling [22]. On the other hand, it has been reported that Wnt/β-catenin mutations correlated with high expression of FGFR4, and lenvatinib was shown to be highly effective against HCC with high expression of FGFR4 with the ORR of 81% and PFS of 5.5 months, compared to the ORR of 31% and PFS of 2.5 months with low expression of FGFR4 [23,24]. There was a case report that described a patient with HCC with a β-catenin mutation, in whom lenvatinib after atezolizumab plus bevacizumab allowed the patient to progress to conversion surgery [25]. In addition, a case was reported in which a response to atezolizumab plus bevacizumab was achieved in the main intrahepatic tumor, but adrenal metastasis showed disease progression, and subsequent administration of lenvatinib resulted in shrinkage of the adrenal metastasis and conversion to surgery [26]. There have been reports of differences in responses to ICIs by organ [27], including other carcinomas [28], and future analysis of the efficacy of second-line therapy in patients with progression of extrahepatic lesions after ICIs as first-line therapy is also warranted.
Therefore, if the therapeutic effect of atezolizumab plus bevacizumab is judged to be poor, it may be better to change to lenvatinib immediately. As a way to examine the effects of atezolizumab plus bevacizumab at an early stage, there is a report that decreased AFP in unresectable HCC patients treated with atezolizumab plus bevacizumab at 3 weeks was identified as a factor predicting early tumor response [29]. This would help determine whether to continue atezolizumab plus bevacizumab at an early stage.
Recently, the results of phase III HIMALAYA trial which evaluated single tremelimumab, regular interval durvalumab (STRIDE) as first-line standard systemic therapy for unresectable HCC were published. As a result, STRAIDE showed significantly better efficacy compared to sorafenib [30]. Then, we have to consider whether to use STRIDE for second-line treatment of patients who received atezolizumab plus bevacizumab as first-line treatment. Although in other cancer types, in the treatment of renal cell carcinoma patients with disease progression during or after treatment with ICIs, the combination therapy with atezolizumab and cabozantinib as a TKI did not improve PFS or OS compared with cabozantinib alone and was associated with an increase in serious AEs [31]. Considering AEs, this may be a factor in the choice of treatment with lenvatinib and other TKIs as second-line therapy after atezolizumab plus bevacizumab.
The present study has two limitations. First, it was retrospective. Second, a selection bias could have existed because of the clinical observational nature of the study. Nevertheless, the usefulness of lenvatinib after atezolizumab plus bevacizumab was demonstrated. We believe that this information will be very useful for the systemic therapy of patients with unresectable HCC. Further accumulation of evidence is expected to establish an effective treatment regimen after atezolizumab plus bevacizumab combination therapy.
5. Conclusions
Lenvatinib after atezolizumab plus bevacizumab for unresectable HCC is a safe treatment and should be considered as an effective option that may provide a good prognosis for patients with good liver function and low intrahepatic tumor volume.
Author Contributions
Conceptualization, S.Y., T.K., Y.S., R.M., K.A., K.N., K.Y., S.U. and M.T.; Formal Analysis, S.Y.; Data Curation, S.Y., T.K., S.Y., Y.J., M.K., Y.S., R.M., K.A., K.N., K.Y., Y.F., S.U., H.F., A.O., T.N., E.M., D.M., M.T., Y.T., H.K., S.T., N.M., K.T. and S.O. Supervision, T.K. M.T. and S.O.; Writing—Original Draft, S.Y.; Writing—Review and Editing, T.K. and M.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Review Committee of Hiroshima University (approval ID E-2300 and E-1226) on 15 December 2020 and 5 July 2021. This was a retrospective analysis of records stored in a database. Official approval was received based on the Guidelines for Clinical Research issued by Japan’s Ministry of Health, Labour and Welfare.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all the study participants.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R. L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021, 71, 209-249.
- Llovet, J. M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J. F.; de Oliveira, A. C.; Santoro, A.; Raoul, J. L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008, 359, 378-390.
- Kudo, M.; Finn, R. S.; Qin, S.; Han, K. H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J. W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163-1173.
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y. H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56-66.
- Abou-Alfa, G. K.; Meyer, T.; Cheng, A. L.; El-Khoueiry, A. B.; Rimassa, L.; Ryoo, B. Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J. W.; et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med 2018, 379, 54-63.
- Zhu, A. X.; Kang, Y. K.; Yen, C. J.; Finn, R. S.; Galle, P. R.; Llovet, J. M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H. Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2019, 20, 282-296.
- Finn, R. S.; Qin, S.; Ikeda, M.; Galle, P. R.; Ducreux, M.; Kim, T. Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A. O.; et al., Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med 2020, 382, 1894-1905.
- Lencioni, R.; Llovet, J. M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis 2010, 30, 52-60.
- Gordan, J. D.; Kennedy, E. B.; Abou-Alfa, G. K.; Beg, M. S.; Brower, S. T.; Gade, T. P.; Goff, L.; Gupta, S.; Guy, J.; Harris, W. P.; et al. Systemic therapy for advanced hepatocellular carcinoma: ASCO Guideline. J Clin Oncol 2020, 38, 4317-4345.
- Vogel, A.; Martinelli, E., Updated treatment recommendations for hepatocellular carcinoma (HCC) from the ESMO Clinical Practice Guidelines. Ann Oncol 2021, 32, 801-805.
- Llovet, J. M.; Villanueva, A.; Marrero, J. A.; Schwartz, M.; Meyer, T.; Galle, P. R.; Lencioni, R.; Greten, T. F.; Kudo, M.; Mandrekar, S. J.; et al. Trial design and endpoints in hepatocellular carcinoma: AASLD Consensus Conference. Hepatology 2021, 73 Suppl 1, 158-191.
- Sonbol, M. B.; Riaz, I. B.; Naqvi, S. A. A.; Almquist, D. R.; Mina, S.; Almasri, J.; Shah, S.; Almader-Douglas, D.; Uson Junior, P. L. S.; Mahipal, A.; et al. Systemic therapy and sequencing options in advanced hepatocellular carcinoma: a systematic review and network meta-analysis. JAMA Oncol 2020, 6, e204930.
- Wang, D.; Yang, X.; Lin, J.; Bai, Y.; Long, J.; Yang, X.; Seery, S.; Zhao, H. Comparing the efficacy and safety of second-line therapies for advanced hepatocellular carcinoma: a network meta-analysis of phase III trials. Therap Adv Gastroenterol 2020, 13, 1756284820932483.
- Yao, D. F.; Wu, X. H.; Zhu, Y.; Shi, G. S.; Dong, Z. Z.; Yao, D. B.; Wu, W.; Qiu, L. W.; Meng, X. Y. Quantitative analysis of vascular endothelial growth factor, microvascular density and their clinicopathologic features in human hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int 2005, 4, 220-226.
- Morais, C., Sunitinib resistance in renal cell carcinoma. J Kidney Cancer VHL 2014, 1, 1-11.
- Teng, M. W.; Ngiow, S. F.; Ribas, A.; Smyth, M. J. Classifying cancers based on T-cell infiltration and PD-L1. Cancer Res 2015, 75, 2139-2145.
- Matsui, J.; Funahashi, Y.; Uenaka, T.; Watanabe, T.; Tsuruoka, A.; Asada, M. Multi-kinase inhibitor E7080 suppresses lymph node and lung metastases of human mammary breast tumor MDA-MB-231 via inhibition of vascular endothelial growth factor-receptor (VEGF-R) 2 and VEGF-R3 kinase. Clin Cancer Res 2008, 14, 5459-5465.
- Matsui, J.; Yamamoto, Y.; Funahashi, Y.; Tsuruoka, A.; Watanabe, T.; Wakabayashi, T.; Uenaka, T.; Asada, M. E7080, a novel inhibitor that targets multiple kinases, has potent antitumor activities against stem cell factor producing human small cell lung cancer H146, based on angiogenesis inhibition. Int J Cancer 2008, 122, 664-671.
- Yamada, K.; Yamamoto, N.; Yamada, Y.; Nokihara, H.; Fujiwara, Y.; Hirata, T.; Koizumi, F.; Nishio, K.; Koyama, N.; Tamura, T. Phase I dose-escalation study and biomarker analysis of E7080 in patients with advanced solid tumors. Clin Cancer Res 2011, 17, 2528-2537.
- Boss, D. S.; Glen, H.; Beijnen, J. H.; Keesen, M.; Morrison, R.; Tait, B.; Copalu, W.; Mazur, A.; Wanders, J.; O'Brien, J. P.; et al. A phase I study of E7080, a multitargeted tyrosine kinase inhibitor, in patients with advanced solid tumours. Br J Cancer 2012, 106, 1598-1604.
- Osa, A.; Uenami, T.; Koyama, S.; Fujimoto, K.; Okuzaki, D.; Takimoto, T.; Hirata, H.; Yano, Y.; Yokota, S.; Kinehara, Y.; et al. Clinical implications of monitoring nivolumab immunokinetics in non-small cell lung cancer patients. JCI Insight 2018, 3 (19), e59125.
- Harding, J. J.; Nandakumar, S.; Armenia, J.; Khalil, D. N.; Albano, M.; Ly, M.; Shia, J.; Hechtman, J. F.; Kundra, R.; El Dika, I.; et al. Prospective genotyping of hepatocellular carcinoma: clinical implications of next-generation sequencing for matching patients to targeted and immune therapies. Clin Cancer Res 2019, 25, 2116-2126.
- Yamauchi, M.; Ono, A.; Ishikawa, A.; Kodama, K.; Uchikawa, S.; Hatooka, H.; Zhang, P.; Teraoka, Y.; Morio, K.; Fujino, H.; et al. Tumor fibroblast growth factor receptor 4 level predicts the efficacy of lenvatinib in patients with advanced hepatocellular carcinoma. Clin Transl Gastroenterol 2020, 11, e00179.
- Tohyama, O.; Matsui, J.; Kodama, K.; Hata-Sugi, N.; Kimura, T.; Okamoto, K.; Minoshima, Y.; Iwata, M.; Funahashi, Y. Antitumor activity of lenvatinib (e7080): an angiogenesis inhibitor that targets multiple receptor tyrosine kinases in preclinical human thyroid cancer models. J Thyroid Res 2014, 2014, 638747.
- Johira, Y.; Kawaoka, T.; Kosaka, M.; Shirane, Y.; Miura, R.; Murakami, S.; Yano, S.; Amioka, K.; Naruto, K.; Ando, Y.; et al. Pathological complete response to lenvatinib after failure of atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. Liver Cancer 2022, 11, 174-177.
- Yano, S.; Kawaoka, T.; Johira, Y.; Miura, R.; Kosaka, M.; Shirane, Y.; Murakami, S.; Amioka, K.; Naruto, K.; Ando, Y.; et al. Advanced hepatocellular carcinoma with response to lenvatinib after atezolizumab plus bevacizumab. Medicine (Baltimore) 2021, 100, e27576.
- Lu, L. C.; Hsu, C.; Shao, Y. Y.; Chao, Y.; Yen, C. J.; Shih, I. L.; Hung, Y. P.; Chang, C. J.; Shen, Y. C.; Guo, J. C.; et al. Differential organ-specific tumor response to immune checkpoint inhibitors in hepatocellular carcinoma. Liver Cancer 2019, 8, 480-490.
- Müller, P.; Rothschild, S. I.; Arnold, W.; Hirschmann, P.; Horvath, L.; Bubendorf, L.; Savic, S.; Zippelius, A. Metastatic spread in patients with non-small cell lung cancer is associated with a reduced density of tumor-infiltrating T cells. Cancer Immunol Immunother 2016, 65, 1-11.
- Ando, Y.; Kawaoka, T.; Kosaka, M.; Shirane, Y.; Johira, Y.; Miura, R.; Murakami, S.; Yano, S.; Amioka, K.; Naruto, K.; et al. Early tumor response and safety of atezolizumab plus bevacizumab for patients with unresectable hepatocellular carcinoma in real-world practice. Cancers (Basel) 2021, 13, 3958.
- Abou-Alfa, G. K.; Chan, S. L.; Kudo, M.; Lau, G.; Kelley, R. K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.-K.; Dao, T. V.; Toni, E. N. D.; et al. Phase 3 randomized, open-label, multicenter study of tremelimumab (T) and durvalumab (D) as first-line therapy in patients (pts) with unresectable hepatocellular carcinoma (uHCC): HIMALAYA. J Clin Oncol 2022, 40 (4_suppl), 379-379.
- Pal, S. K.; Albiges, L.; Tomczak, P.; Suárez, C.; Voss, M. H.; de Velasco, G.; Chahoud, J.; Mochalova, A.; Procopio, G.; Mahammedi, H.; et al. Atezolizumab plus cabozantinib versus cabozantinib monotherapy for patients with renal cell carcinoma after progression with previous immune checkpoint inhibitor treatment (CONTACT-03): a multicentre, randomised, open-label, phase 3 trial. Lancet 2023, 402, 185-195.
Figure 1.
Flow chart of patient selection in the study.
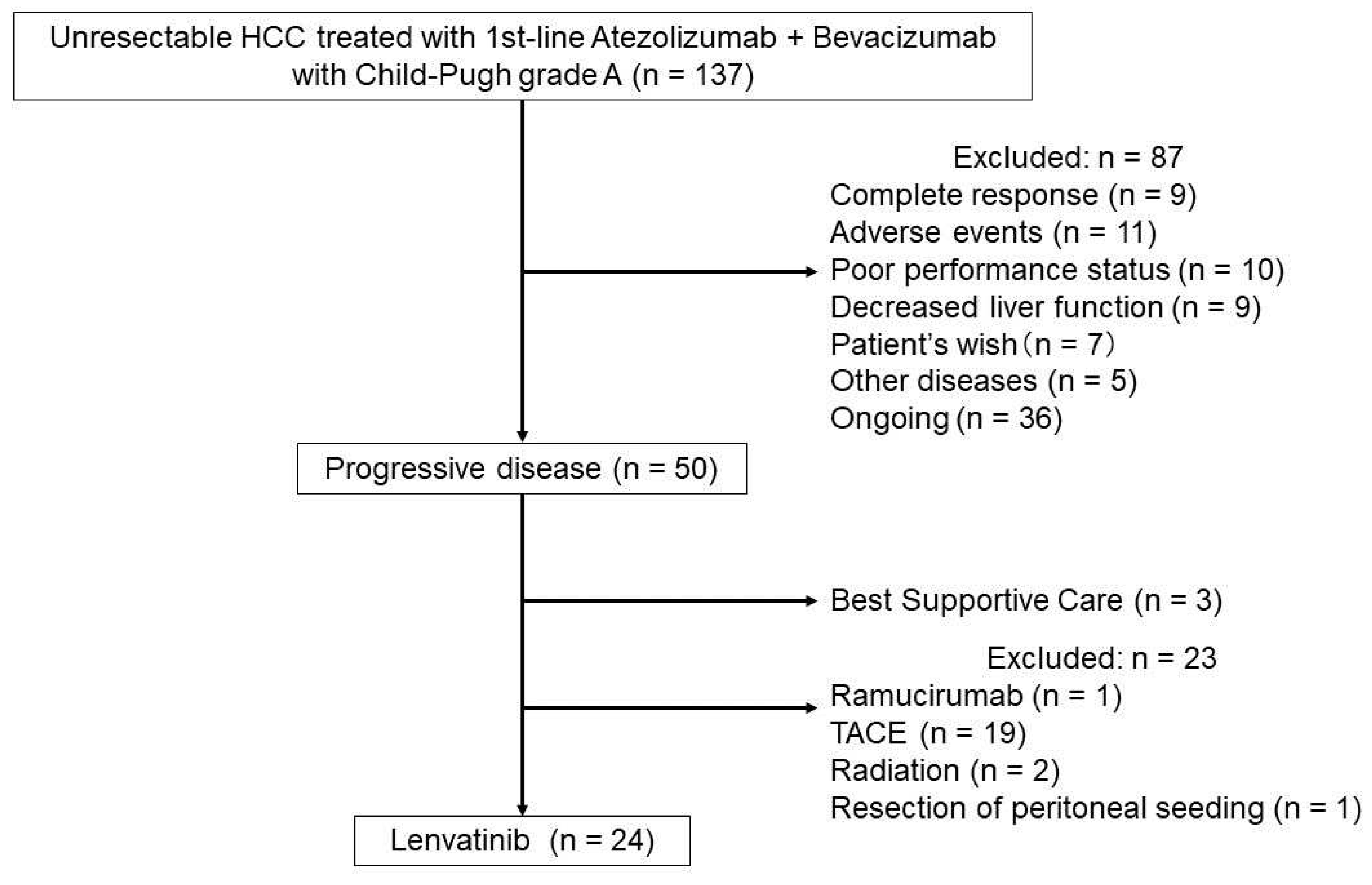
Figure 2.
Overall survival (OS) and progression-free survival (PFS) on atezolizumab plus bevacizumab. (a) OS (median survival time (MST), 21.1 months; 95% confidence interval (CI), 18.8 months–not reached). (b) PFS (median PFS, 10.5 months; 95% CI, 8.2–12.1 months).
Figure 2.
Overall survival (OS) and progression-free survival (PFS) on atezolizumab plus bevacizumab. (a) OS (median survival time (MST), 21.1 months; 95% confidence interval (CI), 18.8 months–not reached). (b) PFS (median PFS, 10.5 months; 95% CI, 8.2–12.1 months).
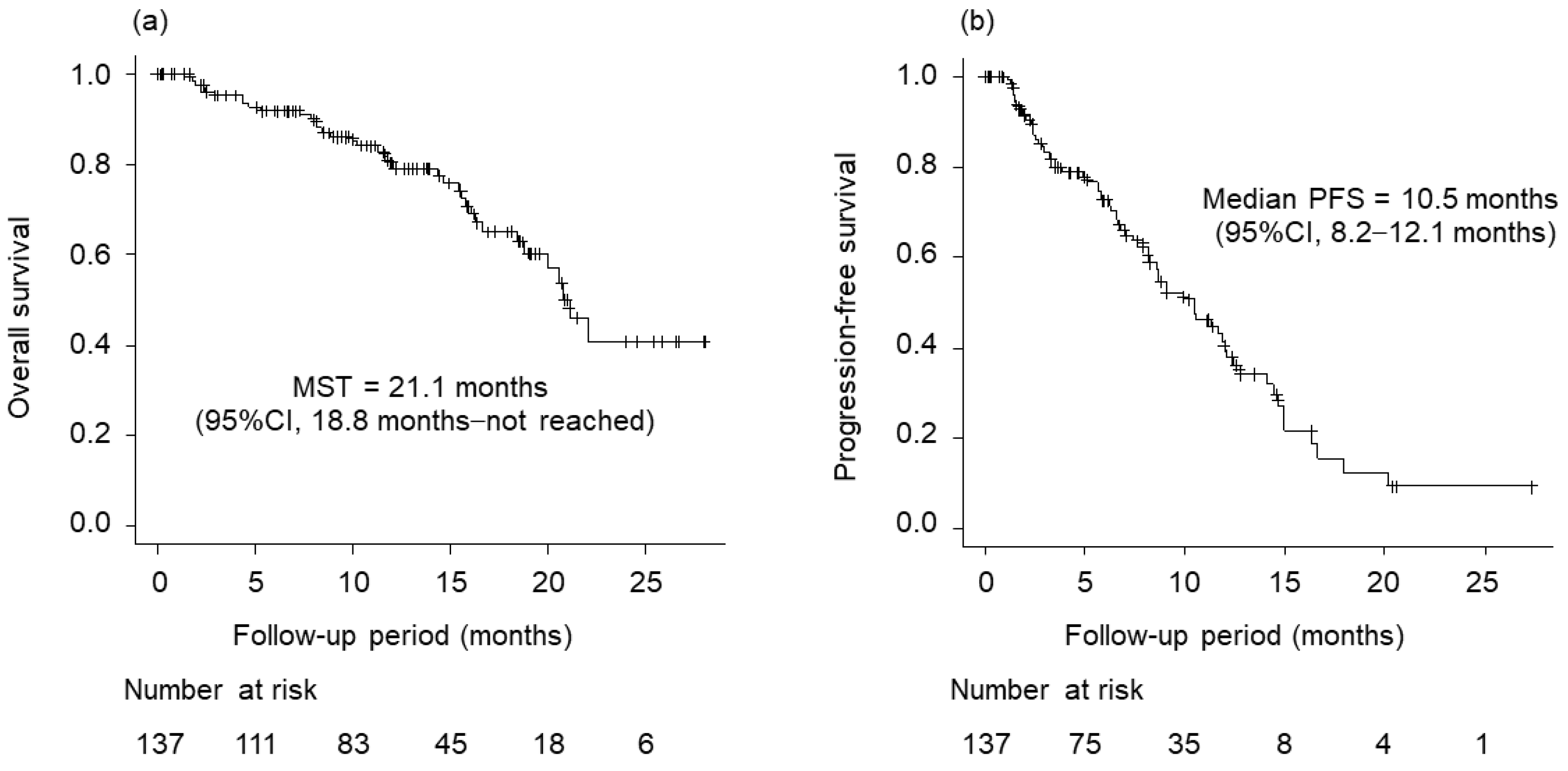
Figure 3.
Post progression survival (PPS) with atezolizumab plus bevacizumab (median PPS, 12.5 months; 95% CI, 9.3–12.5 months).
Figure 3.
Post progression survival (PPS) with atezolizumab plus bevacizumab (median PPS, 12.5 months; 95% CI, 9.3–12.5 months).
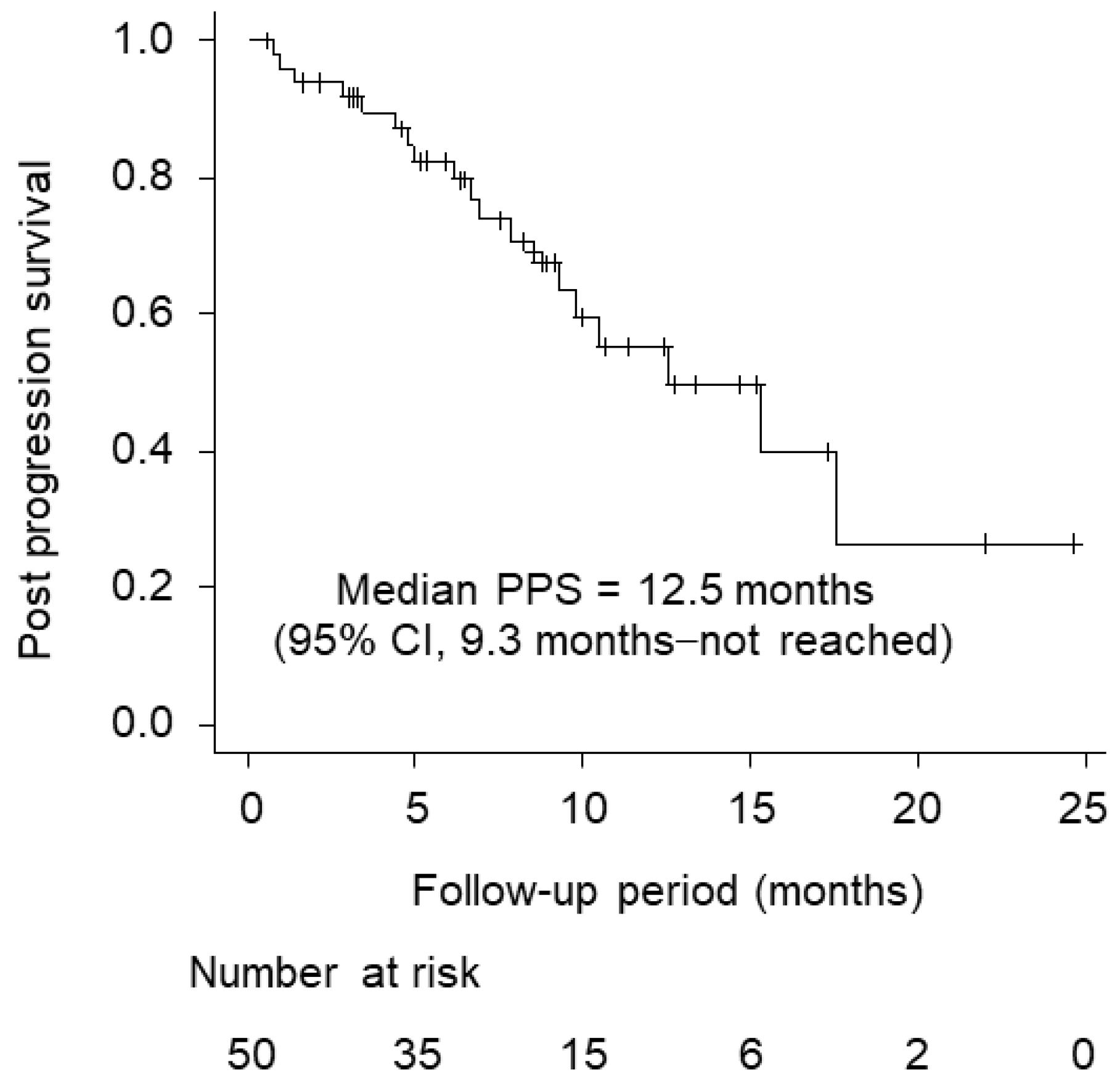
Figure 4.
Overall survival (OS) and progression-free survival (PFS) on lenvatinib after atezolizumab plus bevacizumab. (a) OS (median survival time (MST), 15.3 months; 95% confidence interval (CI), 10.5 months–not reached). (b) PFS (median PFS, 4.0 months; 95% CI, 2.5–6.4 months).
Figure 4.
Overall survival (OS) and progression-free survival (PFS) on lenvatinib after atezolizumab plus bevacizumab. (a) OS (median survival time (MST), 15.3 months; 95% confidence interval (CI), 10.5 months–not reached). (b) PFS (median PFS, 4.0 months; 95% CI, 2.5–6.4 months).
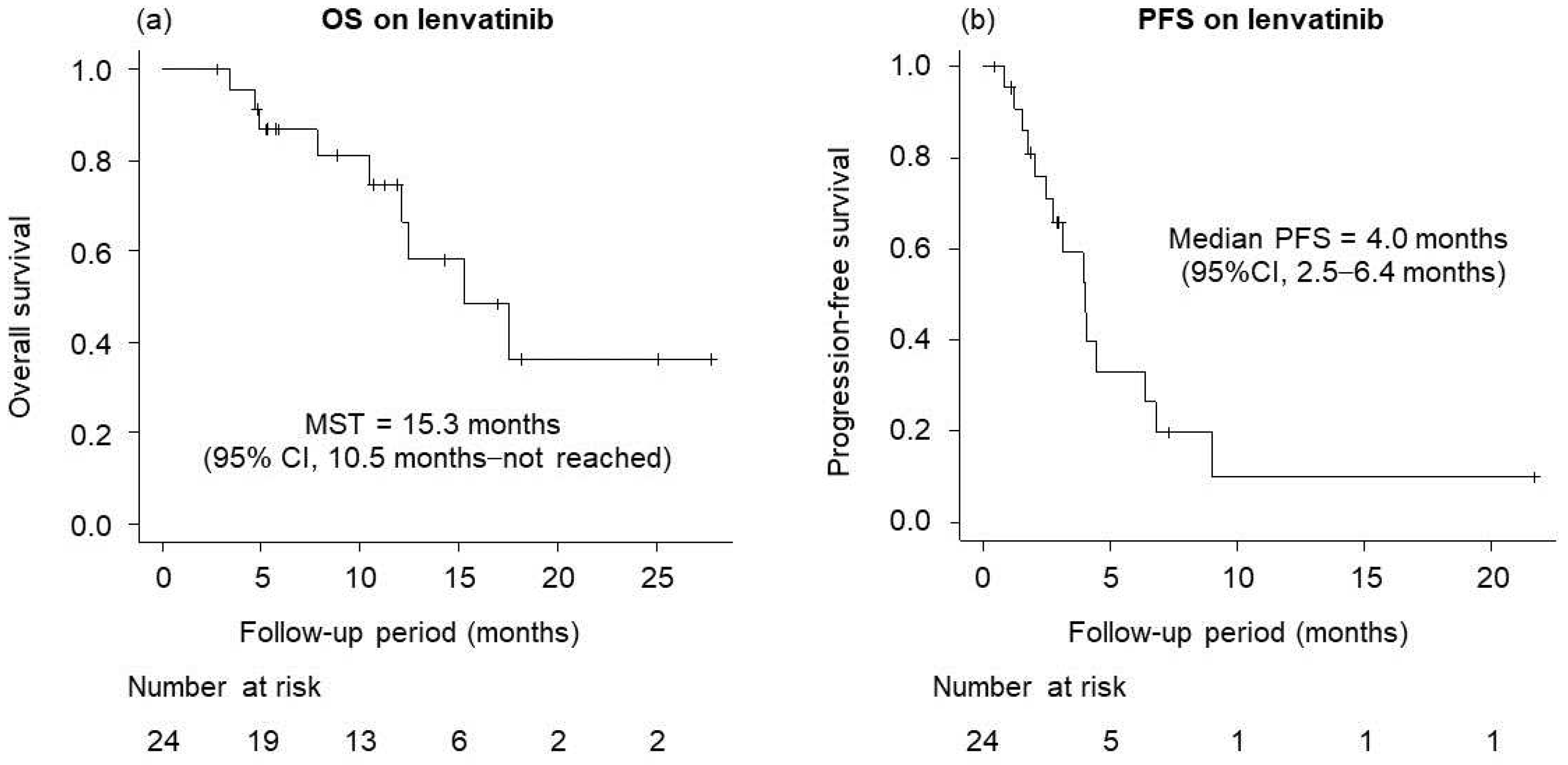
Figure 5.
Overall survival (OS) on lenvatinib after atezolizumab plus bevacizumab. (a) OS for the patients with Child-Pugh A is better than for those with Child-Pugh B (median OS 17.5 vs. 10.5 months, p = 0.022). (b) OS for the patients with a relative tumor volume (RTV) <50% is better than for those with an RTV ≥50% (median OS 17.5 vs. 5.6 months, p = 0.00028).
Figure 5.
Overall survival (OS) on lenvatinib after atezolizumab plus bevacizumab. (a) OS for the patients with Child-Pugh A is better than for those with Child-Pugh B (median OS 17.5 vs. 10.5 months, p = 0.022). (b) OS for the patients with a relative tumor volume (RTV) <50% is better than for those with an RTV ≥50% (median OS 17.5 vs. 5.6 months, p = 0.00028).
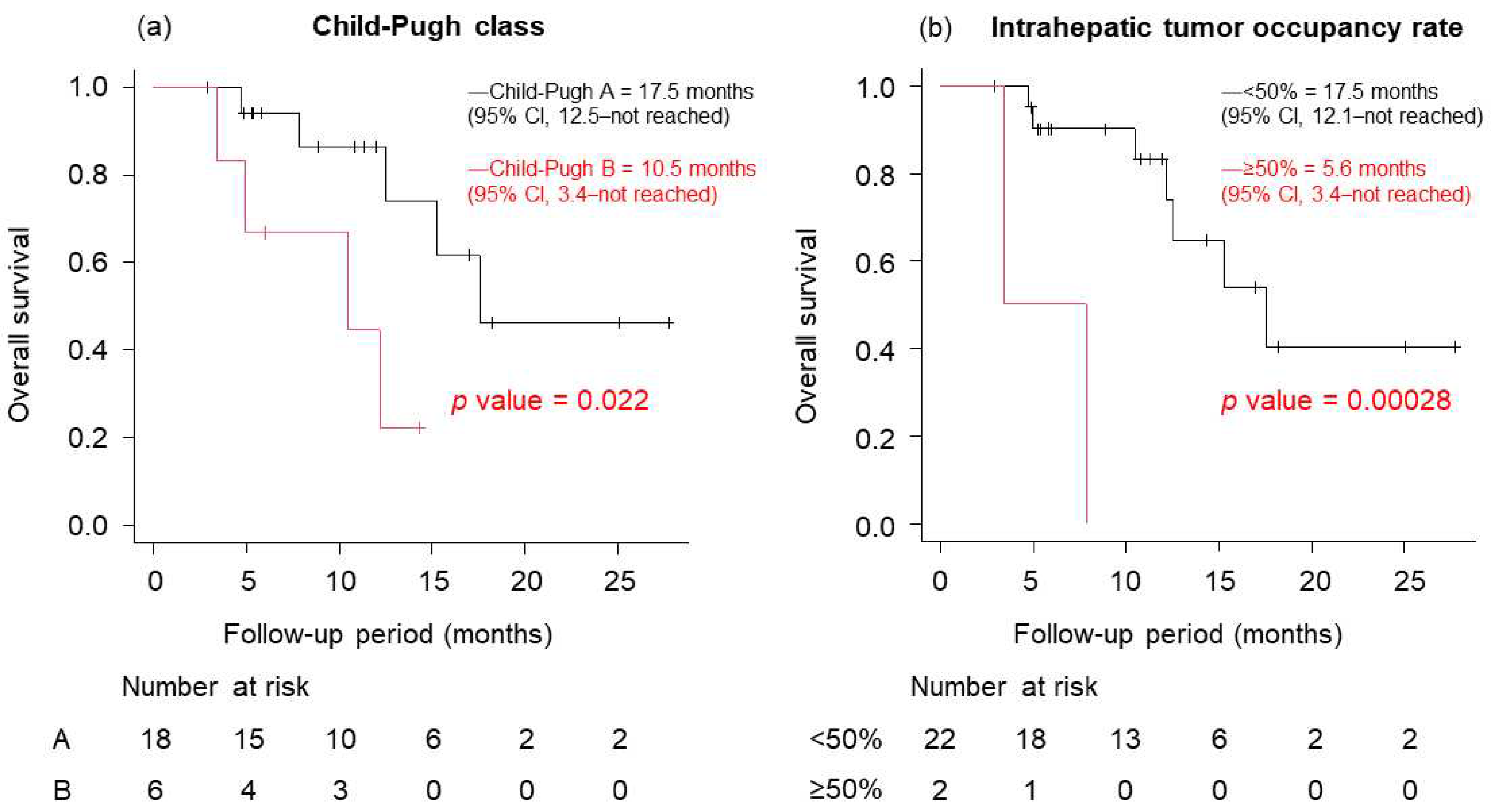

Table 1.
Background characteristics of all cases (n = 137).
| All (n = 137) | |
|---|---|
| Age, range, y | 75 (47–92) |
| Sex (male/female), n | 107/30 |
| Performance status (0/1/2), n | 113/18/6 |
| Etiology (HBV/HCV/HBV+HCV/NBNC), n | 15/48/2/72 |
| Child–Pugh score (5/6), n | 84/53 |
| mALBI grade (1/2a/2b), n | 52/45/40 |
| Relative tumor volume (<50%/≥50%), n | 130/7 |
| Size of main tumor, range, mm | 28 (0–220) |
| Microvascular invasion (absent/present), n | 112/25 |
| Extrahepatic metastasis (absent/present), n | 93/44 |
| HCC stage (II/III/IVa/IVb), n | 33/50/22/32 |
| BCLC stage (A/B/C), n | 8/63/66 |
| Serum alpha-fetoprotein, range, ng/ml | 18.1 (1.2–63642) |
| Serum des-gamma-carboxy prothrombin, range, mAU/ml | 236 (11–197680) |
| Observation period, range, months | 11.7 (1–28) |
Values represent medians (range) or numbers of patients. HBV—hepatitis B virus infection; HCV—hepatitis C virus infection; NBNC—non-B, non-C viral hepatitis; mALBI—modified albumin-bilirubin; HCC—hepatocellular carcinoma; BCLC—Barcelona Clinic Liver Cancer.
Table 2.
Background characteristics at the time of diagnosis of progressive disease on atezolizumab plus bevacizumab (n = 50).
Table 2.
Background characteristics at the time of diagnosis of progressive disease on atezolizumab plus bevacizumab (n = 50).
| n = 50 | |
|---|---|
| Sex (male/female), n | 41/9 |
| Performance status (0/1/2), n | 32/12/5 |
| Etiology (HBV/HCV/NBNC), n | 7/19/24 |
| Child–Pugh grade (A/B/C), n | 34/14/2 |
| mALBI grade (1/2a/2b/3), n | 12/10/23/5 |
| Relative tumor volume (<50%/≥50%), n | 45/5 |
| Size of main tumor, range, mm | 33 (0–170) |
| Microvascular invasion (absent/present), n | 35/15 |
| Extrahepatic metastasis (absent/present), n | 27/23 |
| HCC stage (II/III/IVa/IVb), n | 6/16/9/19 |
| BCLC stage (A/B/C), n | 3/15/32 |
| Serum alpha-fetoprotein, range, ng/ml | 105.3 (0.8–64620) |
| Serum des-gamma-carboxy prothrombin, range, mAU/ml | 2842.5 (22–247805) |
| Systemic therapy after atezolizumab plus bevacizumab | 25 (LEN 24, RAM 1) |
Values represent medians (range) or numbers of patients. HBV—hepatitis B virus infection; HCV—hepatitis C virus infection; NBNC—non-B, non-C viral hepatitis; mALBI—modified albumin-bilirubin; HCC—hepatocellular carcinoma; BCLC—Barcelona Clinic Liver Cancer; LEN—lenvatinib; RAM—ramucirumab.
Table 3.
Background characteristics at the beginning of lenvatinib after atezolizumab plus bevacizumab (n = 24).
Table 3.
Background characteristics at the beginning of lenvatinib after atezolizumab plus bevacizumab (n = 24).
| n = 24 | |
|---|---|
| Sex (male/female), n | 20/4/ |
| Performance status (0/1/2), n | 19/4/1 |
| Etiology (HBV/HCV/NBNC), n | 5/11/8 |
| Child–Pugh grade (A/B/C), n | 34/14/2 |
| mALBI grade (1/2a/2b/3), n | 8/6/7/3 |
| Relative tumor volume (<50%/≥50%), n | 22/2 |
| Size of main tumor, range, mm | 30 (0–120) |
| Microvascular invasion (absent/present), n | 16/8 |
| Extrahepatic metastasis (absent/present), n | 13/11 |
| HCC stage (II/III/IVa/IVb), n | 2/9/3/10 |
| BCLC stage (A/B/C), n | 8/16 |
| Serum alpha-fetoprotein, range, ng/ml | 140.5 (1.5–64620) |
| Serum des-gamma-carboxy prothrombin, range, mAU/ml | 2614 (25–214866) |
| Time to LEN administration after Atez+Bev, days | 17 (4–63) |
Values represent medians (range) or numbers of patients. HBV—hepatitis B virus infection; HCV—hepatitis C virus infection; NBNC—non-B, non-C viral hepatitis; mALBI—modified albumin-bilirubin; HCC—hepatocellular carcinoma; BCLC—Barcelona Clinic Liver Cancer; LEN—lenvatinib; Atez+Bev —atezolizumab plus bevacizumab.
Table 4.
Radiological response (n = 24).
| %(n) | RECIST 1.1 | mRECIST |
|---|---|---|
| CR | 0.0 (0) | 4.2 (1) |
| PR | 33.3 (8) | 50.0 (12) |
| SD | 41.7 (10) | 25.0 (6) |
| PD | 20.1 (5) | 16.7 (4) |
| N.E | 4.2 (1) | 4.2 (1) |
| ORR | 33.3 (8) | 54.2 (13) |
| DCR | 75.0 (18) | 79.2 (19) |
RECIST—response evaluation criteria in solid tumors; mRECIST—modified response evaluation criteria in solid tumors; CR—complete response; PR—partial response; SD—stable disease; PD—progressive disease; N.E—not evaluated; ORR—objective response rate; DCR—disease control rate.
Table 5.
Prognostic factors for overall survival in patients on lenvatinib with progressive disease after first-line atezolizumab plus bevacizumab (Cox hazards analysis).
Table 5.
Prognostic factors for overall survival in patients on lenvatinib with progressive disease after first-line atezolizumab plus bevacizumab (Cox hazards analysis).
| Variable | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| p value | HR | 95% CI | p value | ||
| Sex | Male | 0.13 | |||
| Etiology | Viral infection | 0.72 | |||
| Child–Pugh grade | A | 0.02 | 0.14 | 0.02 0.76 | 0.02 |
| Microvascular invasion | Absent | 0.63 | |||
| Extrahepatic metastasis | Absent | 0.37 | |||
| Relative tumor volume | <50% | <0.01 | 0.03 | 0.003 0.35 | <0.01 |
| Serum alpha-fetoprotein | <400 ng/ml | 0.40 | |||
| TACE/TAI combination | yes | 0.13 | |||
TACE—transcatheter arterial chemoembolization; TAI—transcatheter arterial infusion; HR—Hazard ratio; CI—confidence interval.
Table 6.
Adverse events associated with lenvatinib.
| Event %(n) | All Patients (n = 24) | |
|---|---|---|
| Any Grade | Grade 3 or 4 | |
| Hypertension | 62.5 (15) | 16.7 (4) |
| Fatigue | 58.3 (14) | 25.0 (6) |
| Anorexia | 45.8 (11) | 12.5 (3) |
| Diarrhea | 41.7 (10) | 4.2 (1) |
| Proteinuria | 29.2 (7) | 20.8 (5) |
| Hand-foot syndrome | 29.2 (7) | 0.0 (0) |
| Hypothyroidism | 20.8 (5) | 0.0 (0) |
| Renal dysfunction | 12.5 (3) | 4.2 (1) |
| Increased AST or ALT | 8.3 (2) | 0.0 (0) |
| Hoarseness | 8.3 (2) | 0.0 (0) |
| Thrombocytopenia | 8.3 (2) | 4.2 (1) |
| Interstitial pneumonia | 4.2 (1) | 0.0 (0) |
AST—aspartate aminotransferase; ALT—alanine aminotransferase.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



