
Submitted:
13 October 2023
Posted:
16 October 2023
You are already at the latest version
Abstract
Melasma is a common skin disorder of acquired hyperpigmentation that appears commonly on the face. Although asymptomatic, melasma causes psychosocial and emotional distress. This study aimed to assess melasma's severity on people with darker skin types, evaluate the effects of melasma on the Quality of Life (QoL), and establish QoL predictors in affected individuals. This was a cross-sectional analytic study that enrolled 150 patients who were diagnosed with melasma from three private dermatology clinics in Durban, South Africa. The severity of melasma and QoL were measured using a Melasma Area and Severity Index (MASI) score, and Melasma Quality of Life scale (MELASQoL), respectively. The factors associated with impaired QoL were also explored using the multivariate method and stepwise regression analysis. MASI score of Masi (β = 0.209, t = 2.628, p < .010), involvement of cheeks (β = -0.268, t = -3.405, p <.001), level of education (β = -0.159, t = -2.029, p =.044) and being menopausal (β = -0.161, t = -2.027, p =.045) were found to be predictors of QoL. A regression model to predict MELASQoL given these four predictors was developed. The significance of the equation can allow remote scoring of MELASQoL based on the four variables.
Keywords:
Melasma
; Pigmentation
; Darker skin type
; Fitzpatrick skin types IV-VI
; Quality of life
1. Introduction
The skin is the most extensive organ of the human body, and it serves the most important function as a protective organ from the environment [1,2]. Healthy skin is essential so that homeostasis can run normally and also to prevent various disorders and diseases [1,2], therefore, the impact of skin conditions on well-being is proportional to their visibility [3]. The most common complaints dermatologists deal with are premature aging, acne, and pigmentary disorders including melasma [4,5].
Melasma is a common dyschromia, mainly found in women between Fitzpatrick skin types IV-VI [6,7,8]. Melasma prevalence varies across the globe. Its prevalence as a multifactorial disorder has ranged from 1% in the population as a whole to 9–50% in populations at higher risk [9]. This broad variance in prevalence has been attributed primarily to differences in ethnicity and levels of sun exposure among population groups living in different geographic regions. A study by Walker et al. suggests that in 546 dermatological patients in Nepal, melasma was the most common pigmentary disorder and the fourth most common dermatosis [10]. The Arab population in Saudi Arabia had a prevalence of 2.9%, whereas Arabs in America had a prevalence of 13.4–15.5% [11,12]. There was an 8.2% prevalence among 1,000 Latino patients [13], similarly, 8.8% of the Latino population in Texas had melasma, while 4.0% reported a history of it [14]. A prevalence of 1.5% was noted in Ethiopia [15] while in South Africa, dyschromias, including melasma, are the 3rd most prevalent dermatologic diagnosis in Durban [16].
Melasma is often associated with a variety of factors such as sun exposure, genetics, sex steroids (pregnancy and oral contraceptives), drugs, or cosmetics [6,7,17,18,19]. It is caused by melanocytic hypertrophy and hyperfunction of the epidermal-melanic unit [20]. Some studies have revealed that the pathology of melasma points to more heterogeneous pathogenesis involving interactions between keratinocytes, mast cells, gene regulation abnormalities, neovascularization, and disruption of the basement membrane [19,21,22]. Due to this complex pathogenesis, melasma is difficult to target and likely to recur after treatment. Oral therapies (tranexamic acid, glutathione), procedural interventions (chemical peels, microneedling, lasers, and lights), and topical therapies (tretinoin, hydroquinone, triple combination) are helpful, however, they are not suitable for all skin types due to undesired side effects, and suboptimal results, more especially when dealing with darker skin types (Fitzpatrick skin types IV-VI) [8,23].
Although asymptomatic, melasma as a facial disorder affects the appearance of facial skin aesthetically and can reduce a person’s confidence, resulting in a low quality of life for the patient [6,7]. Hence, personal and socioeconomic factors have been shown to have an impact on health-related QoL [24]. Quality of life (QoL) is defined as the ability to perform daily activities appropriate to a person’s age and plays a significant role in society [6,25]. The World Health Organization (WHO), describes quality of life as an individual’s perceptions of their position in life within their cultural context, value systems, expectations, goals, morals, and concerns [6,25,26,27].
The Melasma Quality of Life scale (MELASQoL) is one of the validated dermatology-specific instruments used to assess the impact of melasma on health-related quality of life (HRQoL) and has been established through clinical studies and validated in several languages [26,28,29,30]. The MELASQoL questionnaire comprises a 10-item questionnaire, based on SKINDEX-16 [29] and is used in numerous countries [6,28,31,32,33]. However, no evidence shows it has been fully explored in clinical practice in South Africa. With an emphasis on people with darker skin types, the aim of this study is to comprehensively understand melasma by achieving the following objectives:
- Assess the severity of melasma,
- Evaluate the impact of melasma on the QoL of affected patients,
- Identify predictors of QoL through stepwise regression analysis.
Although it may be possible for a clinician to get an overall view of a patient’s QoL by asking a single question, the use of a more detailed questionnaire provides much richer detail that allows the clinician to address both specific problems experienced by a patient and to identify which aspects of the patient’s life are most severely affected by their disease. Intervention can therefore be directed more appropriately [34].
To the best of our knowledge, no studies have been conducted in South Africa on this important topic. We believe findings from this study will play a major role in informing dermatologists in their clinical decision-making on a routine basis. Hence, measuring QoL can help enhance patient care by identifying the need for supportive interventions and also help to track the improvement of patient HRQoL as well as influence healthcare policy.
2. Materials and Methods
2.1. Study design and setting
We conducted a cross-sectional survey among adult patients aged 18 and above, with darker skin types, diagnosed with facial melasma. The survey was conducted from three private dermatology clinics (Heritage House-Musgrave, Multimedics-Umhlanga, and Durdoc-Durban CBD) in Durban.
2.2. Study population
We conducted a cross-sectional survey among adult patients aged 18 and above, with darker skin types, diagnosed with facial melasma. The survey was conducted from three private dermatology clinics (Heritage House-Musgrave, Multimedics-Umhlanga, and Durdoc-Durban CBD) in Durban.
2.3. Sample size and sampling techniques
We enrolled 150 respondents from three privately owned dermatology clinics. The survey was administered to patients in English, either online or face-to-face by a trained multilingual interviewer. All the surveys that were filled in manually were uploaded by trained data capture personnel. The respondents to be interviewed in the selected skin clinics were chosen using non-probability sampling (including convenience and purposive sampling). Patients were provided with information about the nature of the study and were only recruited after informed consent was received. They were assured that their anonymity and confidentiality would be maintained.
2.4. Data collection
Data were collected between March and December 2022. At enrolment, all patients filled out a clinical survey form to obtain information on their demographics age, gender, marital status, family history, sites of involvement as well as the use of cosmetics or other treatment alternatives that they had been using for melasma. All the patients were examined by a board-certified dermatologist. Patients were examined to identify the distribution of melasma which was divided into three regions: centrofacial (cheeks, forehead, upper lip, nose, and chin); mandibular (ramus of the mandible), and malar (cheeks and nose). In addition, data on the disease chronicity, cosmetic usage, aetiological factors including occupation, sun exposure, use of sunscreen, pregnancy history, use of hormone replacement therapy (HRT) amongst postmenopausal women, oral contraceptives use, and any other associated conditions with onset of melasma, were collected. The MELASQoL questionnaire (Table 1) was administered to respondents to measure their QoL.
This was done by adding up the components of the MELASQoL scale. Lowest score i.e., 1 point for each 7 factors equals 7. Or if the respondent scored 10 for each factor, the MELASQOL would be 70 as per the developers of the MELASQOL instrument. The severity of melasma was graded based on MASI (Table 2).
2.6. Statistical analysis
Data were collected, processed, and analyzed using SPSS version 28 software. Descriptive statistics on continuous data were conducted whilst frequencies were reported for categorical variables. A Pearson correlation matrix was used to establish the presence of multicollinearity between predictor variables. Despite the application of stepwise regression being considered crude by most statisticians, it is still widely reported in the literature and remains an invaluable tool in evaluating predictors [35]. A stepwise regression was performed to establish statistically significant predictors of QoL. Before the stepwise regression, the variables were evaluated for the presence of multicollinearity. High correlation values between predictors lead to redundancy and may markedly influence the model’s predictive value. As a guideline, any correlation value with an absolute value greater than 0.700 should be removed from a regression model.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Study Respondents Characteristics
This study enrolled a total of 150 respondents of either sex. The mean age of the respondents was 47.30 years (SD = 10.21). The majority (n = 143, 95%) were female while the remaining were males (n = 7, 8%). One hundred and fourteen (76%) of the participants were black African, 13 (9%) Indians and 23 (15%) were of mixed ancestry. Perceived causes of melasma included numerous triggers as illustrated in Figure 1 below. A few respondents did not know what caused their melasma.
Most respondents (61%) had no family history of melasma, while the remaining (39%) had a relative who suffered from melasma. Most people (41%) had their mother suffering from melasma, followed by their sibling (sister), aunt, cousin then lastly uncle, and brother. Some respondents (35%) had suffered from melasma for five years, while the majority of the respondents had experienced melasma in the past six months. Most respondents (61%) had used some form of traditional intervention e.g., turmeric powder paste, red ochre soil, or bark paste to treat their melasma while the remaining (39%) indicated that they had used only dermatological treatment interventions. The most common area (40%) of melasma was on the cheeks, followed by the forehead sides of the face, jawline, and nose respectively.
3.2. Descriptive Analysis of the Dependent and Predictor Variables
The mean and standard deviations of the respondent’s responses are shown in Table 3. These statistics describe all the variables of the sample population. Twenty-eight predictor variables were assessed.
These included the number of children (Kids), number of skin products used (Makeup), their age (Age), the Melasma Severity Index (Masi), time spent in the sun per day (SunOften), the sun protection factor used (spf), time spent in the sun (SunExposure), how long they have suffered with melasma (HowLongSuffer), how long they have been treated for it (TreatLongTreat), the number of triggers (Triggers), how often they play outdoor sport (SportOften), their gender (Gender), level of education (Educ), whether they use sun protection (SunPrt), whether they consulting a doctor (Doctor), they understood the meaning of the word “Melasma” (Word), they are diagnosed as suffering from the condition (Suffer), the location on the condition (Forehead), (Cheeks), (Jawline), (Nose), (Sides), whether they are receiving treatment (Treatment), whether they are using plant-based remedies (Plants), whether they had family members also suffering from the condition (Family), whether they played sport (Sport), whether they were menopausal (Menopause) and whether they were on hormone replacement therapy (HRT).
Table 4 illustrates the frequencies of these key categorical variables. Of particular significance in both Table 5 and Table 6, is that respondents have a relatively high MELASQoL score (M = 56.29, SD = 7.35), they are mainly women (95%), have had children (M = 2.10, SD = 1.13) and are middle-aged score (M = 47.30, SD = 10.21). However, only 10% reported that they are menopausal.
3.3. Severity of Melasma Index (MASI)
Based on 150 observations, a descriptive analysis was performed on the MASI index. The mean MASI index score was 40.62 (SD = 4.87) with scores ranging from 31.00 to 48.00. The kurtosis value of -1.03 indicated a modestly platykurtic distribution, indicating fewer outliers than a normal distribution. The skewness value of -0.18 indicated a minor leftward bias, indicating a slightly negative skewness. The analysis also computed a confidence level of 95.0% (CI = 0.786) for the estimated population mean based on the sample data (Table 5).
These findings provide a descriptive summary of the MASI index, highlighting the mean level, variability, and distribution of the scores. Figure 2 below also shows their respective frequency distributions (histograms).
3.4. QoL (MELASQoL)
Table 6 shows the 10 themes tested in the survey that constitute the respondents’ MELASQoL scores when summed together. For all ten themes, the frequency distributions are negatively skewed i.e., long tails to the left. This implies that respondents indicated that they were affected by melasma irrespective of their underlying melasma conditions, severity, outdoor behaviours, or demographics. These distributions indicate that even when the severity of melasma was low (MASI), and irrespective of which ethnic group or gender, their quality of life (MELASQoL) was still affected by melasma. The Variance Inflation Factor (VIF) was also used to determine the presence of multicollinearity. Table 6, therefore, shows that the presence of multicollinearity is not a concern.
3.5. Stepwise Regression Analysis
The MELASQoL score of respondents was predicted using a multivariate regression analysis that considered all the 28 independent variables relevant to the primary research question i.e., predicting the MELASQoL score of a melasma patient. Before being used in regression analysis, the majority of the independent variables had to be recorded because they were categorical variables.
Categories were dummy coded as “0” or “1”. Depending on whether they fall under a particular category or not, people were assigned a code of “0” or “1”. These categories were explicitly defined as mutually exclusive. For example, if a respondent did not use sun protection, this response would be coded “0”. If they did use sun protection, the response was coded “1”. The coding did not allow for any overlapping responses. The frequency of these dummy predictor variables is shown in Table 6.
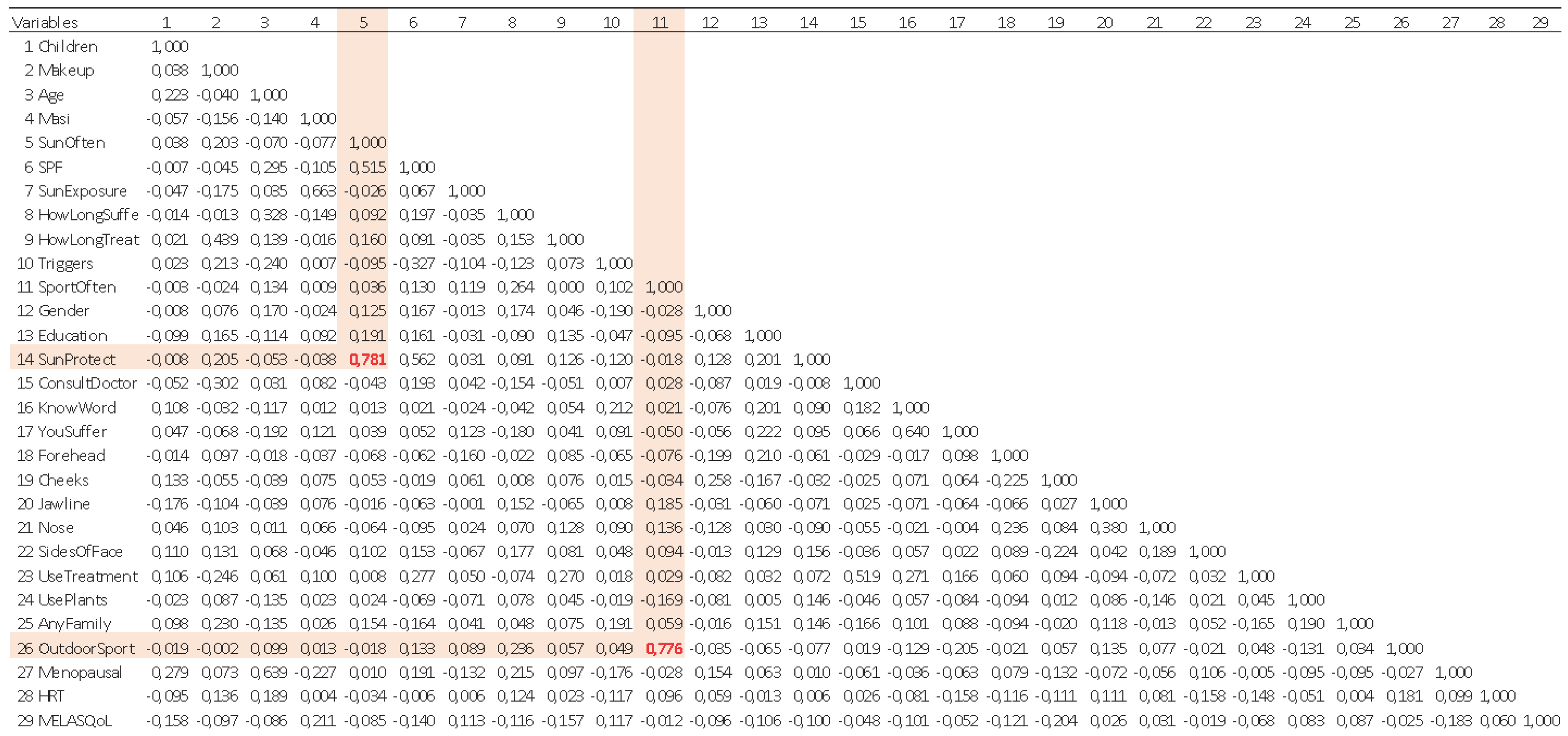
The stepwise regression method was used to build the regression model in SPSS version 28. Starting with all 28 predictor variables in the study question, this method includes removing each variable one at a time. Four variables had a Pearson correlation coefficient with absolute values greater than 0.700. These variables were: sun exposure and use of sun protection with a correlation coefficient of 0.781, and sport participation and outdoor sport participation with a correlation coefficient of 0.776. These variables were however not removed, but rather allowed the stepwise regression algorithm to include or exclude them objectively. The correlation matrix is reflected in Table 7.
Table 8 shows that the stepwise regression produced four statistically significant models and the increasing value of R2 and falling standard errors with successive inclusion of the independent variables from Model 1 (with MASI only) to Model 4 (with predictors MASI, Cheeks, Education, and Menopausal). R2 improved from 0.044 in Model 1 to 0.145 in Model 4. Model 4 produced the highest R2 and Adjusted R2 of 0.145 and 0.122, respectively, with the lowest standard error of the estimate (SE = 6.889).
Notwithstanding this low R2 value, different authors, depending on inter alia the regression model and other factors such as the context of the study, have different opinions concerning the informational utility derived from the use of R2. Falk and Miller, 1992 [36] suggested that for the variance explained of a specific endogenous construct to be judged appropriate, R2 values should be equal to or more than 0.10. Cohen 1988 [37] proposed the following R2 values for endogenous latent variables: 0.26 (substantial), 0.13 (moderate), and 0.02 (weak). Whilst Chin, 1998 [38] suggested R2 values of 0.67 (substantial), 0.33 (moderate), and 0.19 (weak) for endogenous latent variables. An R2 of 0.145 illustrates the dire need to research this topic more in the future to refine the explanatory power of future regression models.
Finally, the Durbin-Watson statistic is calculated to be 1.951 indicating the absence of autocorrelation. The ANOVA (Table 9) showed that all four models produced significance values less than 0.05 with the final model, Model 4, having an overall significance of F (4, 145) = 6.153 and p <.001.
Considering only Model 4, the final predictors are all statistically significant at a 0.05 level of significance i.e., MASI (β = 0.209, t = 2.628, p <.010), Cheeks (β = -0.268, t = -3.405, p <.001), Education (β = -0.159, t = -2.029, p =.044) and Menopausal (β = -0.161, t = -2.027, p =.045). Moreover, the sign of their standardized β-values was also evaluated. The sign of the MASI coefficient was positive (β = +0.209). Intuitively this makes sense in that a higher MASI score i.e., a high assessed severity of the respondent’s melasma should be positively correlated to a lower respondent’s QoL. The other three predictors have negative standardized β-values. The implication of this can be summarised as follows: Cheeks (β = -0.268), Education (β = -0.159), and Menopausal (β = -0.161).
Finally, the prediction of the MELASQoL score is described by the following equation based on the Stepwise Model 4 regression above:
| = | 51.730 | + | 0.315 Masi | - | 4.686 Cheeks | - | 4.148 Education | - | 2.519 Menopausal | ||
| se | = | (5.249) | (0.120) | (1.376) | (2.044) | (1.243) | r2 = 0.145 | ||||
|
t |
= |
(9.856) |
(2.628) |
(-3.405) |
(-2.029) |
(-2.027) |
F (4, 145) = 6.153 |
||||
| p < 0.001 | |||||||||||
| p | = | (< 0.001) | (.010) | (< 0.001) | (.044) | (.045) |
4. Discussion
This study assessed the impact of melasma on the QoL of patients with darker skin types using the MELASQoL scale and established predictors of MELASQoL using stepwise regression. The influence of melasma on patients’ QoL was reflected through both emotional distress and social life. Regarding their skin condition, respondents expressed dissatisfaction, despair, embarrassment, and depression. They revealed that it made them feel unattractive and that it had an impact on their social livelihoods. Melasma causes patients to feel unattractive to others and tends to decrease their desire to be around or interact with them. The reported epidemiologic characteristics of melasma patients in the current study were similar in some respects to those in previously reported factors [18,32,39,40,41].
Our results indicate that 89.33% of respondents use some form of sunscreen in their skincare routine while 10.67 used no sunscreen. A large proportion of respondents (92.48%) use sunscreen regularly but only once a day (92.48%), which may not be sufficient protection. This once-off sun protection application could be attributed to limited knowledge about the proper application of the sunscreen and its ability to protect against photo-pigmentation and the value of the SPF. Many people believe that higher SPF sunscreens provide adequate protection throughout the day [42]. Sunscreens must be applied in an amount of 2 mg/cm2 to provide the SPF stated on the container [43]. However, several studies have shown that consumers apply much less, only about a quarter (0.5 mg/cm2) of the recommended amount, therefore reapplication of sunscreen has been recommended to address these problems [43,44,45]. Furthermore, sweating, movement, and failure to reapply sunscreens at regular intervals all contribute to sunscreens performing poorly in the field when compared to their predicted efficacy in the laboratory [46,47]. It is important to disseminate the message that extreme caution is required in preventing the sun from aggravating melasma on the skin, which necessitates increased effort on the part of skin care specialists to educate and actively engage patients in effective sunscreen application.
Few respondents (10.67%), mainly women, indicated never using sunscreen. Based on given responses when they were asked to state the reasons for not using sun protection creams, the following are possible themes or reasons why women do not use sun protection cream:
- Cost: Some women do not use sun protection cream because they cannot afford it or believe it is too costly.
- Skin reactions: Some women experience skin reactions, irritation, or sensitivity to sun protection cream, which discourages them from using it.
- Appearance: Some women avoid using sun protection cream because they believe it makes their face look white or pale and “creates” pimples.
- No perceived need: Some women do not see the necessity of using sun protection cream, particularly if they spend most of their time indoors or do not spend much time in direct sunlight.
- Use of alternative products: A few women report using moisturizers or other products that have SPF as an alternative to dedicated sun protection cream.
- Efficacy concerns: A small number of women believe that sun protection cream is ineffective or does not work as advertised.
- Other reasons: Some women simply responded with “N/A” or “none”, indicating that they have no particular reason for not using sun protection cream, while others did not provide a reason at all.
Similar behaviors and attitudes concerning the use of sunscreens have been previously reported from respondents with the skin of colour [48,49]. Given the social-political background in South Africa, misconceptions about the use of sun protection still exist, and yet the literature demonstrates that all skin types need to be protected from solar Ultraviolet Radiation (UVR) [50,51]. Due to its geographic location, South Africa is a very hot country with daytime ambient temperatures that often exceed 35o C, the levels of ambient solar (UVR) throughout most of the year are high with the UV Index (UVI) being frequently extreme (11+ or > 6400 Jm-2/day) [52,53]. Hence, future interventions should incorporate components to effectively minimize barriers to sun protection and improve their self-efficacy in wearing sunscreen.
Respondents reported a family history of at least a first and second-degree relative suffering from melasma, suggesting a genetic predisposition as previously indicated in the literature [54,55]. Although men were the minority group (4.67%) in our study, they indicated similar effects of melasma as females. This finding is similar to previous reports that men are equally affected by melasma [41,54,56,57]. Aggravating and triggering factors (Table 3) were similar for both male and female respondents. A few respondents (39.33%) indicated that they use alternative or homemade interventions such as “mmemezi” bark, lemon and/or turmeric powder paste, and clays. The potential use of alternative treatments in managing uneven skin tone is gaining popularity as these treatments are perceived as being safe, affordable, and easily accessible and they provide protection from sun damage [23,58]. Most respondents (86%) reported that they go for professional-based treatments such as chemical peels. Multiple product use included both over-the-counter and prescribed creams such as hydroquinone, retinol, and vitamins like vitamin C and vitamin A. Majority of the respondents mentioned that they use specific brands such as Garnier, Eucerin, Dermalogica, and La Roche-Posay products, which are known for skin lightening. They also listed multiple products or treatments they use, often including a combination of creams, serums, and sunscreen. Most of these creams contain glycolic acid, anti-oxidants, and Vitamins C and E, which are common ingredients used for skin lightening [59,60,61].
The 4th model in the stepwise iteration produced MASI (β = 0.209, t = 2.628, p <.010), Cheeks (β = -0.268, t = -3.405, p <.001), Education (β = -0.159, t = -2.029, p =.044) and Menopause (β = -0.161, t = -2.027, p =.045) as statistically significant predictors of MELASQoL at a 0.05 level of significance. The R2 value was 0.145 implying that 14.5% of the changes in MELASQoL can be accounted for by these four independent variables. The overall model was found to be statistically significant with F (4, 145) = 6.153 and p <.001. During the stepwise regression, it was noted that a lot of predictors were dichotomous and typically these binary variables are mutually exclusive, and as such its standard practice to code as 0 or 1 [62,63,64]. Furthermore, it is good practice to check for multicollinearity so that the final model is parsimonious, hence a multicollinearity test was performed [65,66,67].
MELASQoL was created from questions more relevant to melasma-specific HRQoL issues, with a focus on the emotional and psychological aspects [29]. When compared to the DLQI and SKINDEX 16, MELASQoL was found to have high internal consistency, validity, and discriminatory power [28,29]. There is strong evidence that melasma can strongly affect quality of life [4,6,26,30,33,39,68]. Respondents reported a relatively high MELASQoL score (M = 56.29, SD = 7.35) indicating a significant influence of melasma on patients’ quality of life. Other studies in different countries have reported means of 55.00 ± 10.60 (Australia) [69], 44.4 ± 14.19 (Brazil) [32], 44.40 ± 14.90 (Brazil) [26], 42.49 (Spain) [30], 39.97 ±12.07 (Indonesia) [7] and 38.10 ± 16.60 (Korea) [70]. In all these studies, melasma is reported to cause frustration, embarrassment, and loss of confidence among respondents; furthermore, it makes them feel unattractive and it affects their relationships.
Other studies which analysed the relationship between the MASI and MELASQoL suggested that there is a statistically significant correlation between the two scores [6,28,30,31,70,71]. Hence, our study showed that MASI and MELASQoL scores were statistically correlated (R = 0.222) (Table 8). However, the contrary to this popular view, some studies have shown an unrelated or weak correlation between MASI and MELASQoL [7,32,33,39,69,72,73]. Thus, the relationship between the MASI and MELASQoL scores is mixed. Clinical severity should not be the only criterion used to assess the burden of patients’ skin conditions. The MASI score is based on “feelings”, and since they change according to the situation, “feelings” lack a clear criterion of evaluation. Even when melasma is not severe, it can cause emotional stress, potentially reducing patients’ quality of life.
In our study, four variables had Pearson correlation coefficients with absolute values greater than 0.700. These variables were: Sun exposure and use of sun protection with a correlation coefficient of 0.781, and sports participation and participation in outdoor sports with a correlation coefficient of 0.776. Also, a strong correlation between MASI and Sun Exposure, R = 0.663 (Table 8) was noted in our study. Jointly, studies provide evidence that excessive sun exposure contributes to melasma and therefore impacts the severity of melasma [74,75,76]. The excessive sun exposure from our study may have resulted from the participation in outdoor sports as well as insufficient sun protection application as indicated by the study respondents. Our study results showed that the MELASQoL score is impacted, so it was decided to not remove the variables and allow the stepwise regression algorithm to include or exclude them objectively. This decision was supported by the model’s collinearity statistics in Table 6. Myers [77] suggests that a tolerance value below 0.1 indicates a serious collinearity problem whilst Menard [78] recommends that a tolerance value less than 0.2 indicates a potential collinearity problem. Once again, as a rule of thumb, a tolerance of 0.1 or less is a cause for concern. Similarly, the Variance Inflation Factor (VIF) is also used for determining the presence of multicollinearity. Values of VIF exceeding 10 are often regarded as indicating multicollinearity Allison, 2001[79]. The rule of thumb is that VIF must be less than 5.0. As depicted in Table 6, the presence of multicollinearity is not a concern.
Using the stepwise regression model, the three MELASQoL predictors Cheeks (β = -0.268), Education (β = -0.159) and Menopausal (β = -0.161) have negative standardized β-values. The implication of this can be summarised as follows:
The value for Cheeks (β = -0.268), implied that the greater the prevalence of melasma on the malar area of the respondent, the lower their reported MELASQoL i.e., the higher their reported QoL. Previous research has identified the malar to be one of the most common patterns of melasma presentation [4,68,80,81,82,83]. In our study, we found that people who had a malar pattern of melasma reported that they were not negatively affected by melasma. Some studies have reported that the progression of the disease has no bearing on the quality of life [39,69,73]. Another reason could be that it is easier to cover melasma in the malar area with cosmetic camouflage [84,85,86].
The value for Education (β = -0.159), implied that the more educated the respondent, the higher the reported MELASQoL score i.e., lower QoL. This finding could be that in socially unequal societies like South Africa, educated people are more prominent in society, therefore meeting people in their qualified professions may make them feel negatively affected by their condition. Concerning the level of education, some studies have shown that people with a low level of education may have less information regarding disease prevention, are more likely to work in less qualified fields of work, more vulnerable to unprotected sun exposure, and may have less access to dermatologic care and may not afford costly treatments and make-up [30,40,71,87,88].
The value for Menopause (β = -0.161), when women are menopausal, the lower the MELASQoL score and the greater their overall quality of life. This finding may be attributed to a few suggestions. Firstly, it may be that due to their age, they have accepted the condition of their skin hence they have suffered for many years and therefore are no longer bothered. Another reason could be that they might have slowed down in pursuing careers where they have to meet new people. Scientifically, menopausal women produce significant amounts of oestrogen which is a known risk factor for melasma [30,89,90,91]. Thus, they may be aware of the implications of their hormone production stage and may attribute the severity of melasma.
Given the present study, it is evident that melasma has a significant negative impact on a patient’s QoL. The MELASQoL may not be an ideal tool to measure QoL as it mainly focuses on emotions, which makes the measurement subjective. Previously a more objective instrument that looks into the severity of melasma has been proposed. The new modified MASI (mMASI) score is based on the measurement of darkness and area of involvement in identifying melasma severity, since homogeneity is unreliable it has been removed from the new modified MASI score [92]. In assessing the severity of melasma, most authors have agreed that the mMASI score is reliable, accurate, and responsive to change. Furthermore, the mMASI score has been demonstrated to be easier to acquire and perform, as well as simpler to calculate, than the MASI score [93,94,95]. Thus, the mMASI score can successfully substitute the MASI score.
5. Conclusions
Melasma has a significant impact on a patient’s quality of life (QoL). In this study, we found that impairment of quality of life is greater irrespective of the underlying melasma conditions. Even when melasma is not severe, it can cause emotional stress, potentially reducing patients’ quality of life. Through the stepwise regression model, we distilled 4 key predictor variables out of 28 and developed a regression model to predict MELASQoL given these four predictors. The significance of the equation can allow e.g., remote scoring of MELASQoL based on the four variables, which could help customize the treatment intervention based on the forecasted score.
Author Contributions
Conceptualization, N.M.; methodology, N.M. and M.P.; software, M.P.; formal analysis, N.M and M.P.; investigation, N.M.; resources, N.C.D.; writing—original draft preparation, N.M.; writing—review and editing, N.M; M. P; M.U.M; P.P.; supervision, N.C. D; N.G; A.H.; funding acquisition, N.G. and N.M. All authors have read and agreed to the published version of the manuscript.
Funding
This work is based on research supported in part by the National Research Foundation of South Africa (Grant Number: 138179), the Department of Science and Innovation (DSI) “Cosmeceutical concepts and product development” project; the HWSETA bursary, and the Durban University of Technology Seed Funding grant.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the University of KwaZulu-Natal Biomedical Research Ethics Committee (UKZN BREC) (Protocol reference number: BREC/00002721/2021). The survey was conducted between March and December 2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Due to privacy, data is available on request from the first author.
Acknowledgments
The authors would like to thank all respondents for their enthusiastic participation in this study. We are thankful to Dr. Desmond Kuupiel for editing the manuscript. Our heartfelt gratitude goes to Heritage House, Multimedics as well as Durdoc centre practice staff for their administrative and technical support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dréno B, Araviiskaia E, Berardesca E, Gontijo G, Sanchez Viera M, Xiang L, et al. Microbiome in healthy skin, update for dermatologists. Journal of the European Academy of Dermatology and Venereology. 2016;30(12):2038-47. [CrossRef]
- Bodeker, G.; Ryan, T.J.; Volk, A.; Harris, J.; Burford, G. Integrative Skin Care: Dermatology and Traditional and Complementary Medicine. J. Altern. Complement. Med. 2017, 23, 479–486. [Google Scholar] [CrossRef]
- Resende, D.I.S.P.; Ferreira, M.S.; Lobo, J.M.S.; Sousa, E.; Almeida, I.F. Skin Depigmenting Agents in Anti-Aging Cosmetics: A Medicinal Perspective on Emerging Ingredients. Appl. Sci. 2022, 12, 775. [Google Scholar] [CrossRef]
- Siddiqui S, Qayyum M. Correlation between quality of life and clinical severity of melasma in Pakistani women: Maryam Qayyum, Saadiya Siddiqui, Mohsina, Mahmoona Ilyas, Atif Shahzad, Nadia Ali Zafar. Journal of Pakistan Association of Dermatologists. 2022;32(4):683-9.
- Amatya, B.; Jha, A.K.; Shrestha, S. Frequency of different types of facial melanoses referring to the Department of Dermatology and Venereology, Nepal Medical College and Teaching Hospital in 2019, and assessment of their effect on health-related quality of life. BMC Dermatol. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zeng, X.; Ying, J.; Cai, Y.; Qiu, Y.; Xiang, W. Evaluating the quality of life among melasma patients using the MELASQoL scale: A systematic review and meta-analysis. PLOS ONE 2022, 17, e0262833. [Google Scholar] [CrossRef] [PubMed]
- Jusuf NK, Putra IB, Mahdalena M. Is there a correlation between severity of melasma and quality of life? Open access Macedonian journal of medical sciences. 2019;7(16):2615.
- Mpofana, N.; Abrahamse, H. The Management of Melasma on Skin Types V and VI Using Light Emitting Diode Treatment. Photomed. Laser Surg. 2018, 36, 522–529. [Google Scholar] [CrossRef]
- Majid I, Aleem S. Melasma: Update on Epidemiology, Clinical Presentation, Assessment, and Scoring. Journal of Skin and Stem Cell. 2021;8(4).
- Walker, S.; Shah, M.; Hubbard, V.; Pradhan, H.; Ghimire, M. Skin disease is common in rural Nepal: results of a point prevalence study. Br. J. Dermatol. 2007, 158, 334–338. [Google Scholar] [CrossRef] [PubMed]
- El-Essawi, D.; Musial, J.L.; Hammad, A.; Lim, H.W. A survey of skin disease and skin-related issues in Arab Americans. J. Am. Acad. Dermatol. 2007, 56, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Parthasaradhi, A.; Al Gufai, A.F.; H, A.; M, A.; A, A.; A, S.; M, A.; A, A.; N, M.; H, A.S. The pattern of skin diseases in Hail Region, Saudi Arabia. Ann. Saudi Med. 1998, 18, 558–561. [Google Scholar] [CrossRef]
- Tendero, M.P.A.; Romero, I.B.; Rincón, J.M.R.; Payá, J.S.; Costa, A.L.; Crespo, M.P.; Salvador, J.F.S. Dermatoses in Latin American immigrants seen in a tertiary hospital. Eur. J. Dermatol. 2009, 19, 157–162. [Google Scholar] [CrossRef]
- Werlinger, K.D.; Guevara, I.L.; González, C.M.; Rincón, E.T.; Caetano, R.; Haley, R.W.; Pandya, A.G. Prevalence of Self-diagnosed Melasma Among Premenopausal Latino Women in Dallas and Fort Worth, Tex. Arch. Dermatol. 2007, 143, 423–431. [Google Scholar] [CrossRef]
- Hiletework, M. Skin diseases seen in Kazanchis health center. . 1998, 36, 245–54. [Google Scholar] [PubMed]
- Dlova, N.C.; Akintilo, L.O.; Taylor, S.C. Prevalence of pigmentary disorders: A cross-sectional study in public hospitals in Durban, South Africa. Int. J. Women’s Dermatol. 2019, 5, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Sangha, A.M. Dermatological Conditions in SKIN OF COLOR-Melasma: Topical and Systemic Management. . 2022, 15, S17–S19. [Google Scholar] [PubMed]
- Tamega AdA, Miot H, Moço N, Silva M, Marques M, Miot L. Gene and protein expression of oestrogen-β and progesterone receptors in facial melasma and adjacent healthy skin in women. International Journal of Cosmetic Science. 2015;37(2):222-8.
- E Grimes, P.; Yamada, N.; Bhawan, J. Light Microscopic, Immunohistochemical, and Ultrastructural Alterations in Patients with Melasma. Am. J. Dermatopathol. 2005, 27, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Maranzatto CFP, Miot HA, Miot LDB, Meneguin S. Psychometrican analysis and dimensional structure of the Brazilian version of melasma quality of life scale (MELASQoL-BP). Anais brasileiros de dermatologia. 2016; 91: 422-8.
- Kim, E.H.; Kim, Y.C.; Lee, E.-S.; Kang, H.Y. The vascular characteristics of melasma. J. Dermatol. Sci. 2007, 46, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Torres-Álvarez, B.; Mesa-Garza, I.G.; Castanedo-Cázares, J.P.M.; Fuentes-Ahumada, C.B.; Oros-Ovalle, C.; Navarrete-Solis, J.; Moncada, B. Histochemical and Immunohistochemical Study in Melasma: Evidence of Damage in the Basal Membrane. Am. J. Dermatopathol. 2011, 33, 291–295. [Google Scholar] [CrossRef]
- Mpofana, N.; Chibi, B.; Visser, T.; Paulse, M.; Finlayson, A.J.; Ghuman, S.; Gqaleni, N.; Hussein, A.A.; Dlova, N.C. Treatment of Melasma on Darker Skin Types: A Scoping Review. Cosmetics 2023, 10, 25. [Google Scholar] [CrossRef]
- Jobanputra, R.; Bachmann, M.; MBChB, D.R.J.; MBChB, M.M.B. The effect of skin diseases on quality of life in patients from different social and ethnic groups in Cape Town, South Africa. Int. J. Dermatol. 2000, 39, 826–831. [Google Scholar] [CrossRef]
- Ali R, Aman S, Nadeem M, Kazmi AH. Quality of life in patients of melasma. Journal of Pakistan Association of Dermatologists. 2013;23(2):143-8.
- Cestari, T.; Hexsel, D.; Viegas, M.; Azulay, L.; Hassun, K.; Almeida, A.; Rêgo, V.; Mendes, A.; Filho, J.; Junqueira, H. Validation of a melasma quality of life questionnaire for Brazilian Portuguese language: the MelasQoL-BP study and improvement of QoL of melasma patients after triple combination therapy. Br. J. Dermatol. 2006, 156, 13–20. [Google Scholar] [CrossRef]
- Fleck M, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Application of the Portuguese version of the abbreviated instrument of quality life WHOQOL-bref. Revista de saude publica. 2000; 34: 178-83.
- Dogramaci AC, Havlucu DY, Inandi T, Balkrishnan R. Validation of a melasma quality of life questionnaire for the Turkish language: the MelasQoL-TR study. Journal of dermatological treatment. 2009;20(2):95-9.
- Balkrishnan, R.; Mcmichael, A.; Camacho, F.; Saltzberg, F.; Housman, T.; Grummer, S.; Feldman, S.; Chren, M.-M. Development and validation of a health-related quality of life instrument for women with melasma. Br. J. Dermatol. 2003, 149, 572–577. [Google Scholar] [CrossRef]
- Dominguez, A.R.; Balkrishnan, R.; Ellzey, A.R.; Pandya, A.G. Melasma in Latina patients: Cross-cultural adaptation and validation of a quality-of-life questionnaire in Spanish language. J. Am. Acad. Dermatol. 2006, 55, 59–66. [Google Scholar] [CrossRef]
- Sarkar, R.; Garg, S.; Dominguez, A.; Balkrishnan, R.; Jain, R.; Pandya, A. Development and validation of a Hindi language health-related quality of life questionnaire for melasma in Indian patients. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 16–22. [Google Scholar] [CrossRef]
- Freitag, F.; Cestari, T.; Leopoldo, L.; Paludo, P.; Boza, J. Effect of melasma on quality of life in a sample of women living in southern Brazil. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Misery, L.; Schmitt, A.; Boussetta, S.; Rahhali, N.; Taieb, C. Melasma: Measure of the Impact on Quality of Life Using the French Version of MELASQOL after Cross-cultural Adaptation. Acta Dermato-Venereologica 2010, 90, 331–332. [Google Scholar] [CrossRef] [PubMed]
- Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY. Translating the science of quality of life into practice: what do dermatology life quality index scores mean? Journal of Investigative Dermatology. 2005;125(4):659-64.
- Thayer, JD. Stepwise Regression as an Exploratory Data Analysis Procedure. 2002.
- Falk R, Miller N. A primer for soft modeling University of Akron Press. Akron, Ohio. 1992.
- Cohen J, Cohen P, West SG, Aiken LS. Applied multiple regression/correlation analysis for the behavioral sciences: Routledge; 2013.
- Chin, WW. Commentary: Issues and opinion on structural equation modeling. JSTOR; 1998. p. vii-xvi.
- Ikino, J.K.; Nunes, D.H.; Da Silva, V.P.M.; Fröde, T.S.; Sens, M.M. Melasma and assessment of the quality of life in Brazilian women. An. Bras. de Dermatol. 2015, 90, 196–200. [Google Scholar] [CrossRef] [PubMed]
- D’Elia MPB, Brandão MC, de Andrade Ramos BR, da Silva MG, Miot LDB, Dos Santos SEB, et al. African ancestry is associated with facial melasma in women: a cross-sectional study. BMC medical genetics. 2017;18: 1-7.
- Guinot, C.; Cheffai, S.; Latreille, J.; Dhaoui, M.; Youssef, S.; Jaber, K.; Nageotte, O.; Doss, N. Aggravating factors for melasma: a prospective study in 197 Tunisian patients. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 1060–1069. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Oh, B.H.; Lee, Y.W.; Choe, Y.B.; Ahn, K.J. The relation between the amount of sunscreen applied and the sun protection factor in Asian skin. J. Am. Acad. Dermatol. 2010, 62, 218–222. [Google Scholar] [CrossRef]
- Teramura, T.; Mizuno, M.; Asano, H.; Naito, N.; Arakane, K.; Miyachi, Y. Relationship between sun-protection factor and application thickness in high-performance sunscreen: double application of sunscreen is recommended. Clin. Exp. Dermatol. 2012, 37, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Diffey, BL. When should sunscreen be reapplied? Journal of the American Academy of Dermatology. 2001;45(6):882-5.
- Heerfordt, I.M.; Torsnes, L.R.; Philipsen, P.A.; Wulf, H.C. Photoprotection by sunscreen depends on time spent on application. Photodermatol. Photoimmunol. Photomed. 2017, 34, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Faurschou, A.; Wulf, H. The relation between sun protection factor and amount of suncreen applied in vivo. Br. J. Dermatol. 2007, 156, 716–719. [Google Scholar] [CrossRef]
- Petersen B, Wulf HC. Application of sunscreen− theory and reality. Photodermatology, photoimmunology & photomedicine. 2014 Apr;30(2-3):96-101.
- Seetan K, Shatanawi M, Ali A, Khamees Aa, Alsheikh A, Alawneh A, et al. Disease characteristics, determinants, and perception of use of sunscreen and sun-protective behaviors among patients of color with melasma: A cross-sectional study. Photodermatology, Photoimmunology & Photomedicine. 2022;38(5):495-500.
- Rigel, D.S.; Taylor, S.C.; Lim, H.W.; Alexis, A.F.; Armstrong, A.W.; Fuxench, Z.C.C.; Draelos, Z.D.; Hamzavi, I.H. Photoprotection for skin of all color: Consensus and clinical guidance from an expert panel. J. Am. Acad. Dermatol. 2021, 86, S1–S8. [Google Scholar] [CrossRef]
- Albrecht S, Jung S, Müller R, Lademann J, Zuberbier T, Zastrow L, et al. Skin type differences in solar-simulated radiation-induced oxidative stress. British Journal of Dermatology. 2019;180(3):597-603.
- Mpofana N, Ramhurry C. An Investigation into the effectiveness of light emitting diodes on treating melasma on skin type VI. American Journal of Dermatology and Venereology. 2014.
- Lucas, R.M.; Norval, M.; Wright, C.Y. Solar ultraviolet radiation in Africa: a systematic review and critical evaluation of the health risks and use of photoprotection. Photochem. Photobiol. Sci. 2015, 15, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.Y.; Norval, M.; Summers, B.; Davids, L.M.; Coetzee, G.; Oriowo, M. Solar ultraviolet radiation exposure and human health in South Africa: finding a balance. South Afr. Med J. 2012, 102, 665. [Google Scholar] [CrossRef] [PubMed]
- Sarkar R, Ailawadi P, Garg S. Melasma in men: A review of clinical, etiological, and management issues. The Journal of clinical and aesthetic dermatology. 2018;11(2):53.
- Handel, A.C.; Miot, L.D.B.; Miot, H.A. Melasma: a clinical and epidemiological review. An. Bras. de Dermatol. 2014, 89, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Vázquez M, Maldonado H, Benmamán C, Sanchez JL. Melasma in men: a clinical and histologic study. International journal of dermatology. 1988;27(1):25-7.
- Vachiramon V, Suchonwanit P, Thadanipon K. Melasma in men. Journal of Cosmetic Dermatology. 2012;11(2):151-7.
- Dlova, N.C.; Nevondo, F.T.; Mwangi, E.M.; Summers, B.; Tsoka-Gwegweni, J.; Martincigh, B.S.; Mulholland, D.A. Chemical analysis and in vitro UV-protection characteristics of clays traditionally used for sun protection in South Africa. Photodermatol. Photoimmunol. Photomed. 2013, 29, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Huh, C.-H.; Seo, K.-I.; Park, J.-Y.; Lim, J.-G.; Eun, H.-C.; Park, K.-C. A Randomized, Double-Blind, Placebo-Controlled Trial of Vitamin C Iontophoresis in Melasma. Dermatology 2003, 206, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Babbush, K.M.; Babbush, R.A.; Khachemoune, A. The Therapeutic Use of Antioxidants for Melasma. J. Drugs Dermatol. 2020, 19, 788–792. [Google Scholar] [CrossRef]
- Ismail ESA, Patsatsi A, Abd el-Maged WM, Nada EEDAeA. Efficacy of microneedling with topical vitamin C in the treatment of melasma. Journal of cosmetic dermatology. 2019;18(5):1342-7.
- Wolf, G.; Cartwright, B. Rules for coding dummy variables in multiple regression. Psychol. Bull. 1974, 81, 173–179. [Google Scholar] [CrossRef]
- Cohen, A. Dummy Variables in Stepwise Regression. Am. Stat. 1991, 45, 226. [Google Scholar] [CrossRef]
- Hardy, MA. Regression with dummy variables: Sage; 1993.
- Mansfield, E.R.; Helms, B.P. Detecting Multicollinearity. Am. Stat. 1982, 36, 158. [Google Scholar] [CrossRef]
- Alin, A. Multicollinearity. Wiley interdisciplinary reviews: computational statistics. 2010;2(3):370-4.
- Farrar, D.E.; Glauber, R.R. Multicollinearity in Regression Analysis: The Problem Revisited. Rev. Econ. Stat. 1967, 49, 92. [Google Scholar] [CrossRef]
- KrupaShankar, D.S.R.; Somani, V.K.; Kohli, M.; Sharad, J.; Ganjoo, A.; Kandhari, S.; Mysore, V.R.; Aurangabadkar, S.; Malakar, S.; Vedamurthy, M.; et al. A Cross-Sectional, Multicentric Clinico-Epidemiological Study of Melasma in India. Dermatol. Ther. 2014, 4, 71–81. [Google Scholar] [CrossRef]
- Anderson, L.; Rodrigues, M. Quality of life in a cohort of melasma patients in Australia. Australas. J. Dermatol. 2018, 60, 160–162. [Google Scholar] [CrossRef]
- Kim HY, Park GH, Park EJ, Kwon IH, Kim KH, Kim KJ. Usefulness of melasma quality of life scale (MELASQOL) when evaluating the quality of life in Korean melasma patients. Korean Journal of Dermatology. 2013:422-8.
- Pollo, C.F.; Miot, L.D.; Meneguin, S.; Miot, H.A. Factors associated with quality of life in facial melasma: a cross-sectional study. Int. J. Cosmet. Sci. 2018, 40, 313–316. [Google Scholar] [CrossRef]
- Kothari, P.; Sharma, Y.K.; Patvekar, M.; Gupta, A. Correlating impairment of quality of life and severity of melasma: A cross-sectional study of 141 patients. Indian J. Dermatol. 2018, 63, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Harumi, O.; Goh, C.L. The Effect of Melasma on the Quality of Life in a Sample of Women Living in Singapore. . 2016, 9, 21–4. [Google Scholar] [PubMed]
- Kwon, S.; Na, J.; Choi, J.; Park, K. Melasma: Updates and perspectives. Exp. Dermatol. 2018, 28, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Micek, I.; Pawlaczyk, M.; Kroma, A.; Seraszek-Jaros, A.; Urbańska, M.; Gornowicz-Porowska, J. Treatment of melasma with a low-fluence 1064 nm Q-switched Nd:YAG laser: Laser toning in Caucasian women. Lasers Surg. Med. 2021, 54, 366–373. [Google Scholar] [CrossRef]
- Dorgham, N.A.; Hegazy, R.A.; Sharobim, A.K.; Dorgham, D.A. Efficacy and tolerability of chemical peeling as a single agent for melasma in dark-skinned patients: A systematic review and meta-analysis of comparative trials. J. Cosmet. Dermatol. 2020, 19, 2812–2819. [Google Scholar] [CrossRef] [PubMed]
- Myers RH, Myers RH. Classical and modern regression with applications: Duxbury press Belmont, CA; 1990.
- Menard, S. Applied logistic regression analysis: Sage; 2002.
- Allison, PD. Logistic regression using SAS: Theory and application: SAS institute; 2012.
- Rathi, S.K.; Achar, A. Melasma: A clinico-epidemiological study of 312 cases. Indian J. Dermatol. 2011, 56, 380–2. [Google Scholar] [CrossRef]
- Moin, A.; Jabery, Z.; Fallah, N. Prevalence and awareness of melasma during pregnancy. Int. J. Dermatol. 2006, 45, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Gover, M.D.; Nouri, K.; Taylor, S. The treatment of melasma: A review of clinical trials. J. Am. Acad. Dermatol. 2006, 55, 1048–1065. [Google Scholar] [CrossRef] [PubMed]
- Tamega AdA, Miot L, Bonfietti C, Gige T, Marques MEA, Miot HA. Clinical patterns and epidemiological characteristics of facial melasma in Brazilian women. Journal of the European Academy of Dermatology and Venereology. 2013;27(2):151-6.
- Holme, S.; Beattie, P.; Fleming, C. Cosmetic camouflage advice improves quality of life. Br. J. Dermatol. 2002, 147, 946–949. [Google Scholar] [CrossRef]
- Ogbechie-Godec, O.A.; Elbuluk, N. Melasma: an Up-to-Date Comprehensive Review. Dermatol. Ther. 2017, 7, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Sheth VM, Pandya AG. Melasma: a comprehensive update: part II. Journal of the American Academy of Dermatology. 2011;65(4):699-714.
- Lynch, J.W.; Smith, G.D.; A Kaplan, G.; House, J.S. Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ 2000, 320, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Renzi, C.; Abeni, D.; Picardi, A.; Agostini, E.; Melchi, C.; Pasquini, P.; Puddu, P.; Braga, M. Factors associated with patient satisfaction with care among dermatological outpatients. Br. J. Dermatol. 2001, 145, 617–623. [Google Scholar] [CrossRef]
- Simpson, ER. Sources of estrogen and their importance. The Journal of steroid biochemistry and molecular biology. 2003;86(3-5):225-30.
- Koothirezhi R, Ranganathan S. Postmenopausal syndrome. 2020.
- Cario, M. How hormones may modulate human skin pigmentation in melasma: An in vitro perspective. Exp. Dermatol. 2019, 28, 709–718. [Google Scholar] [CrossRef]
- Pandya AG, Hynan LS, Bhore R, Riley FC, Guevara IL, Grimes P, et al. Reliability assessment and validation of the Melasma Area and Severity Index (MASI) and a new modified MASI scoring method. Journal of the American Academy of Dermatology. 2011;64(1):78-83. e2.
- Abou-Taleb, D.A.; Ibrahim, A.K.; Youssef, E.M.; Moubasher, A.E. Reliability, Validity, and Sensitivity to Change Overtime of the Modified Melasma Area and Severity Index Score. Dermatol. Surg. 2017, 43, 210–217. [Google Scholar] [CrossRef]
- Thng TGS, Chuah SY. The Scoring Aid: MASI and Modified MASI. Melasma and Vitiligo in Brown Skin. 2017:63-70. [CrossRef]
- Rendon M, Berneburg M, Arellano I, Picardo M. Treatment of melasma. Journal of the American Academy of Dermatology. 2006;54(5):S272-S81. [CrossRef]
Figure 1.
Number of times a trigger category was selected by the respondents.
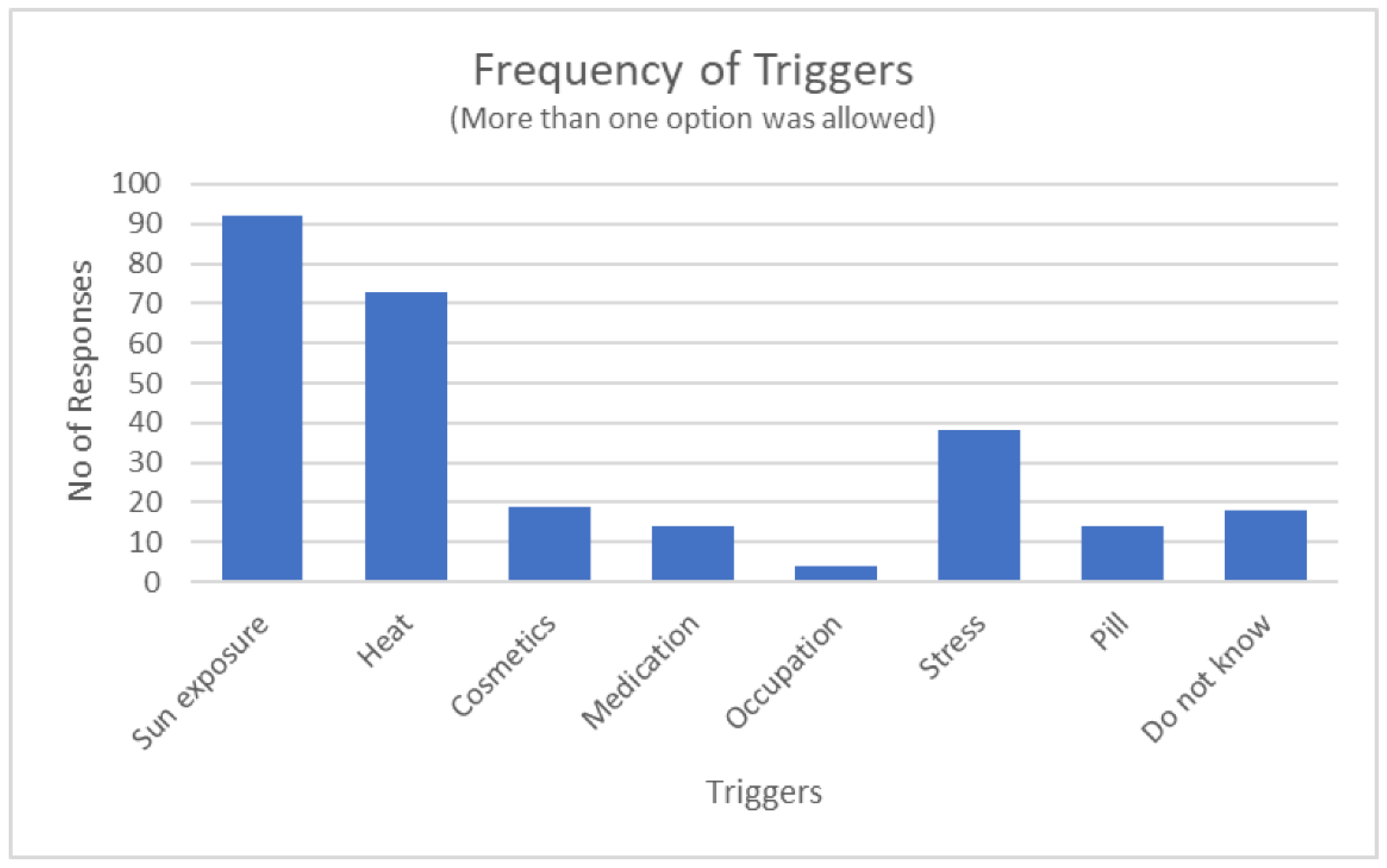
Figure 2.
Distribution of MASI scores.
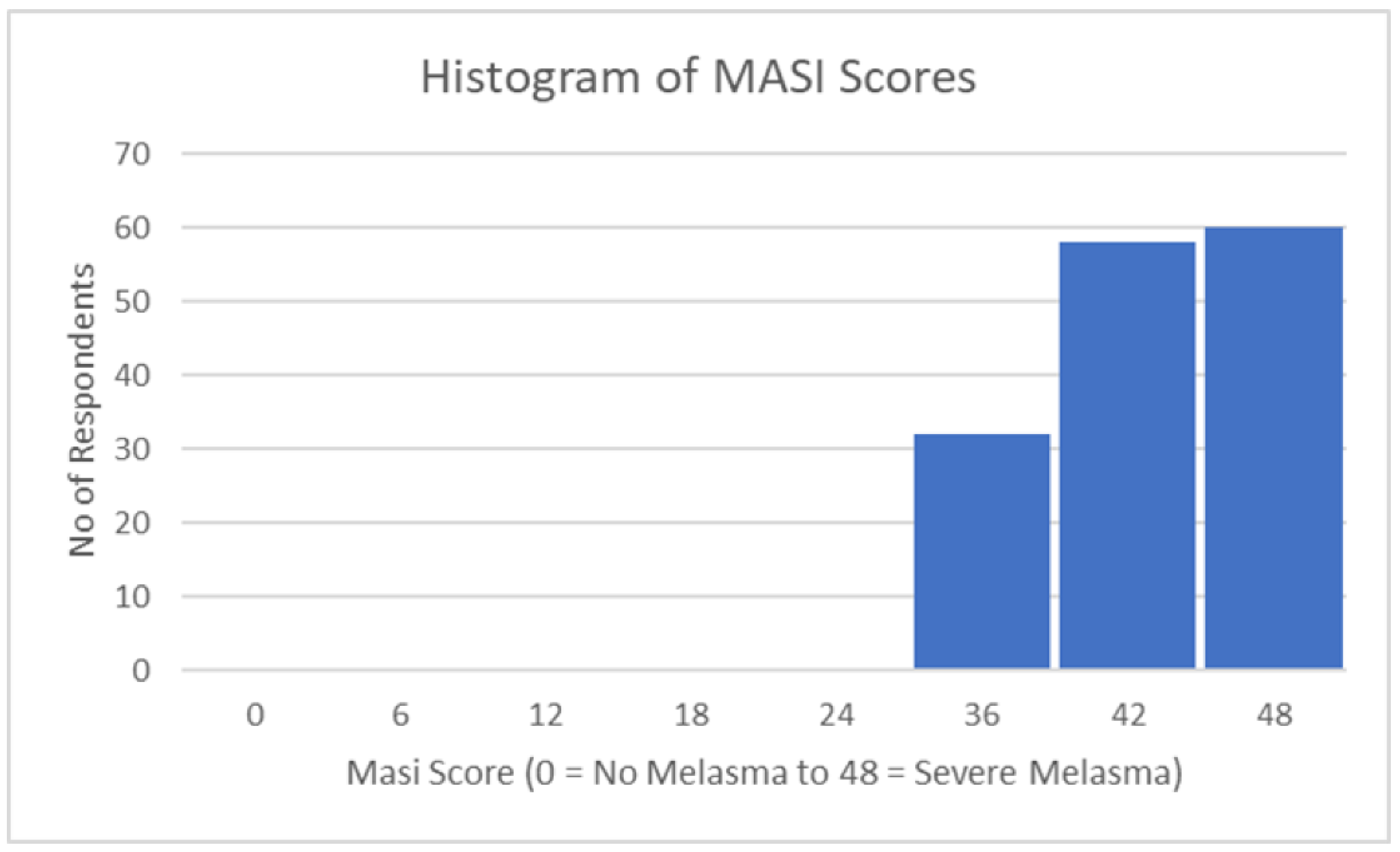

Table 1.
MELASQoL Scale
| On a Likert scale of 1 (not bothered at all) to 7 (bothered all the time), the subject rates how s/he feels about themselves: |
|
Likert scale numerical values: 1 (Not bothered at all); 2 (Not bothered);3 (Not bothered sometimes); 4 (Neutral); 5 (Bothered sometimes); 6 (Bothered most of the time);7 (Bothered all the time). The MELASQOL is scored from 7 to 70, with a higher score indicating worse melasma-related health-related quality of life.
Table 2.
Melasma Area Severity Index (MASI) grading scale parameters.
| Score | Darkness (D) | Homogeneity (H) | Area (A) |
|---|---|---|---|
| 0 | Absent | Minimal | No involvement |
| 1 | Slight | Slight | < 10% |
| 2 | Mild | Mild | 10-29% |
| 3 | Marked | Marked | 30-49% |
| 4 | Maximum | Maximum | 50-69% |
| 5 | 70-89% | ||
| 6 | 90-100% |
D=darkness, H=homogeneity, A=area, F=forehead, MR=right malar, ML=left malar, C= chin; MASI total score = 0.3A (f) [D(f) + H(f)] +0.3A (lm) [D(lm) + H (lm)] +0.3A (rm) [D(rm) + H (rm)] +0.1A (c) [D(c) + H(c)]; Values 0.3, 0.3, 0.3, and 0.1 are the respective percentage of the total facial area.
Table 3.
Descriptive statistics of the dependent and predictor variables.
| Variables | Notes | Mean | Std. Deviation |
|---|---|---|---|
| MELASQoL | Scale from 7 to 70 | 56.29 | 7.35 |
| Children | Number of children | 2.10 | 1.13 |
| Skin care regime | Total number of skin products used | 2.43 | 2.11 |
| Age | Years | 47.30 | 10.21 |
| MASI | MASI grading scale | 40.62 | 4.87 |
| Sun exposure | Times a day | 0.95 | 0.42 |
| SPF | Range from 4 to 100 | 45.09 | 27.64 |
| Sun exposure | Minutes per day | 113.00 | 47.33 |
| Duration of melasma | Years | 6.38 | 4.78 |
| Treatment duration | Months | 10.54 | 13.56 |
| Triggers | Total number of triggers | 1.81 | 0.72 |
| Sport participation | Number of days per week | 1.01 | 2.22 |
Table 4.
Frequency table of dummy regressor variables.
| Dummy Variables |
Frequency of “0” |
Percentage (%) |
Frequency of “1” |
Percentage (%) |
|
|---|---|---|---|---|---|
| Gender | 7 | 5% | 143 | 95% | |
| Education | 13 | 9% | 137 | 91% | |
| Use of sun protection | 16 | 11% | 134 | 89% | |
| Previously consulted with the Doctor | 20 | 13% | 130 | 87% | |
| Familiarity with the word melasma | 16 | 11% | 134 | 89% | |
| Suffers from melasma | 9 | 6% | 141 | 94% | |
| Forehead | 88 | 59% | 62 | 41% | |
| Cheeks | 34 | 23% | 116 | 77% | |
| Jawline | 116 | 77% | 34 | 23% | |
| Nose | 134 | 89% | 16 | 11% | |
| Sides of the face | 111 | 74% | 39 | 26% | |
| Current melasma treatment | 18 | 12% | 132 | 88% | |
| Use of plants as an alternative treatment | 91 | 61% | 59 | 39% | |
| Family history | 91 | 61% | 59 | 39% | |
| Participation in outdoor sport | 117 | 78% | 33 | 22% | |
| Post-menopausal | 101 | 67% | 49 | 33% | |
| HRT | 140 | 93% | 10 | 7% | |
Gender: 0 = Male, 1 = Female; Education: 0 = Uneducated, 1 = Educated; for the rest of the variables: 0 = No, 1 = Yes
Table 5.
Descriptive summary of the severity of melasma observed in the respondents.
| MASI Statistics | |
|---|---|
| Mean | 40.62 |
| Standard Error | 0.40 |
| Median | 40.00 |
| Mode | 40.00 |
| Standard Deviation | 4.87 |
| Sample Variance | 23.73 |
| Kurtosis | -1.03 |
| Skewness | -0.18 |
| Range | 17.00 |
| Minimum | 31.00 |
| Maximum | 48.00 |
| Sample size | 150 |
| Confidence Level (95,0%) | 0,786 |
Table 6.
Percentage of answers for each MELASQoL question from melasma patients (N = 150).
| MELASQoL | Likert Scalea | Descriptives | Frequency Distribution |
||||||||
| Questions on… | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Count | Mean | Stdev | |
| Appearance | 0 | 0 | 0 | 3 | 38 | 77 | 32 | 150 | 5,920 | 0,735 |  |
| Frustration | 0 | 0 | 0 | 4 | 37 | 77 | 32 | 150 | 5,913 | 0,748 | |
| Embarrassment | 0 | 0 | 2 | 7 | 40 | 70 | 31 | 150 | 5,807 | 0,862 | |
| Depressed | 0 | 0 | 1 | 5 | 44 | 79 | 21 | 150 | 5,760 | 0,754 | |
| Others | 0 | 0 | 0 | 7 | 39 | 82 | 22 | 150 | 5,793 | 0,742 | |
| Desire | 1 | 0 | 1 | 13 | 40 | 71 | 24 | 150 | 5,667 | 0,943 | |
| Affection | 1 | 0 | 1 | 13 | 44 | 66 | 25 | 150 | 5,647 | 0,953 | |
| Unattractive | 1 | 0 | 2 | 10 | 39 | 74 | 24 | 150 | 5,693 | 0,938 | |
| Unproductive | 1 | 1 | 1 | 21 | 37 | 70 | 19 | 150 | 5,520 | 1,018 | |
| Freedom | 1 | 0 | 1 | 11 | 41 | 76 | 20 | 150 | 5,660 | 0,901 | |
| a7-point Likert Scale ranging from 1 = “Not bothered at all” to 7 = “Constantly bothered”. | |||||||||||
Table 7.
Correlation matrix of predictor and dependent variables.Table 8. Stepwise regression model summary.
Table 7.
Correlation matrix of predictor and dependent variables.Table 8. Stepwise regression model summary.
| Model | R | R2 | Adjusted R2 | Std. Error | Durbin-Watson |
|---|---|---|---|---|---|
| 1 | ,211a | 0,044 | 0,038 | 7,210 | |
| 2 | ,305b | 0,093 | 0,081 | 7,047 | |
| 3 | ,348c | 0,121 | 0,103 | 6,962 | |
| 4 | ,381d | 0,145 | 0,122 | 6,889 | 1,951 |
| a Predictors: (Constant), MASI | |||||
| b Predictors: (Constant), MASI, Cheeks | |||||
| c Predictors: (Constant), MASI, Cheeks, Education | |||||
| d Predictors: (Constant), MASI, Cheeks, Education, menopausal | |||||
| e Dependent Variable: MELASQoL | |||||
Table 8.
Percentage of answers for each MELASQoL question from melasma patients (N = 150).
|
Table 9.
Analysis of the variance (ANOVA) of the four stepwise regression models.
| Modela | Sum of Squares | Df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|---|
| 1 | Regression | 357.63 | 1 | 357.630 | 6.880 | .010b |
| Residual | 7692.768 | 148 | 51.978 | |||
| Total | 8050.398 | 149 | ||||
| 2 | Regression | 749.586 | 2 | 374.793 | 7.546 | <.001c |
| Residual | 7300.812 | 147 | 49.665 | |||
| Total | 8050.398 | 149 | ||||
| 3 | Regression | 973.157 | 3 | 324.386 | 6.692 | <.001d |
| Residual | 7077.241 | 146 | 48.474 | |||
| Total | 8050.398 | 149 | ||||
| 4 | Regression | 1168.115 | 4 | 292.029 | 6.153 | <.001e |
| Residual | 6882.283 | 145 | 47.464 | |||
| Total | 8050.398 | 149 | ||||
| a Dependent Variable: MELASQoL | ||||||
| b Predictors: (Constant), MASI | ||||||
| c Predictors: (Constant), MASI, Cheeks | ||||||
| d Predictors: (Constant), MASI, Cheeks, Education | ||||||
| e Predictors: (Constant), MASI, Cheeks, Education, menopausal | ||||||
Table 10.
Regression coefficients.
| Model | Unstandardized Coefficients |
Std. Error |
Standardized Coefficients |
t-values | Significance | Collinearity Statistics | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | Beta | Tolerance | VIF | |||||||
| 1 | (Constant) | 43,376 | 4,960 | 8,745 | <,001 | |||||
| MASI | 0,318 | 0,121 | 0,211 | 2,623 | 0,010 | 1,000 | 1,000 | |||
| 2 | (Constant) | 45,356 | 4,900 | 9,257 | <,001 | |||||
| MASI | 0,343 | 0,119 | 0,227 | 2,886 | 0,004 | 0,994 | 1,006 | |||
| Cheeks | -3,872 | 1,378 | -0,221 | -2,809 | 0,006 | 0,994 | 1,006 | |||
| 3 | (Constant) | 48,710 | 5,086 | 9,577 | <,001 | |||||
| MASI | 0,370 | 0,118 | 0,245 | 3,132 | 0,002 | 0,983 | 1,017 | |||
| Cheeks | -4,391 | 1,383 | -0,251 | -3,175 | 0,002 | 0,964 | 1,037 | |||
| Education | -4,426 | 2,061 | -0,170 | -2,148 | 0,033 | 0,961 | 1,040 | |||
| 4 | (Constant) | 51,730 | 5,249 | 9,856 | <,001 | |||||
| MASI | 0,315 | 0,120 | 0,209 | 2,628 | 0,010 | 0,933 | 1,071 | |||
| Cheeks | -4,686 | 1,376 | -0,268 | -3,405 | <,001 | 0,953 | 1,049 | |||
| Education | -4,148 | 2,044 | -0,159 | -2,029 | 0,044 | 0,957 | 1,045 | |||
| Menopausal | -2,519 | 1,243 | -0,161 | -2,027 | 0,045 | 0,931 | 1,074 | |||
| a Dependent Variable: MELASQoL | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



