
Submitted:
16 October 2023
Posted:
17 October 2023
You are already at the latest version
Abstract
ABSTRACT: Objectives: Oncostatin M (OSM), a member of the interleukin (IL)-6 family of cytokines, is known to elicit pathogenic effects involving disruption of the epithelial barrier function as a part of immunological response networks. It is not yet known how these integrated cytokine signals influence inflammation and other physiological processes in the pathology of chronic rhinosinusitis (CRS). We investigated the expression and distribution of OSM and OSM receptor (OSMR) in sinonasal specimens of CRS patients, and we compared the results with a panel of inflammatory cytokine levels and clinical features. Materials and Methods: We classified CRS patients as eosinophilic (ECRS, n=36) or non-eosinophilic (non-ECRS, n=35) based on the Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) phenotypic criteria, and we compared their cases with those of 68 non-CRS subjects. We also examined stimulatory effects of OSM on the expression levels of cytokine receptors by using the human bronchial epithelium cell line BEAS-2B. Results: An RT-PCR showed that the OSM mRNA levels were significantly increased in the ethmoid sinus mucosa of the CRS patients. The OSM mRNA levels were positively correlated with those of TNF-α, IL-1β, IL-13, and OSMR-β. In BEAS-2B cells, OSM treatment induced significant increases in the OSMR-β, IL-1R1, and IL-13Ra mRNA levels. Conclusions: Our findings indicate that OSM is involved in the pathogenesis of CRS in both type 1 and type 2 inflammation, suggesting the OSM signaling pathway as a potential therapeutic target for modulating epithelial stromal interactions.
Keywords:
paranasal sinus
; chronic rhinosinusitis
; CRS
; epithelial cell
; eosinophil
; oncostatin M
; OSM
; OSM receptor
; OSMR
1. Introduction
Chronic rhinosinusitis (CRS) is a disease characterized by symptomatic inflammation of the sinus mucosa lasting >12 weeks, as confirmed by endoscopy and/or imaging. CRS is classified into two types: type 2, mainly associated with a Th2 immune response, and non-type 2, characterized by a prevalence of type 1 and type 3 inflammation [1,2,3,4,5]. Eosinophilic chronic rhinosinusitis (ECRS) constitutes a subgroup of chronic rhinosinusitis with nasal polyps (CRSwNP) and is characterized by severe eosinophil infiltration. Pathological analyses of ECRS revealed a predominance of type 2 inflammation (3, 6, 7).
Oncostatin M (OSM) is a member of the interleukin (IL)-6 family of cytokines, which includes IL-11, IL-31, and leukemia inhibitory factor (LIF) [8]. OSM has been shown to be expressed by many cell types of the hematopoietic lineage, including T cells, neutrophils, macrophages, and eosinophils [9]. OSM is not known to be expressed by epithelium, fibroblasts, or smooth muscle, all of which express the two forms of the OSM receptor (OSMR) [10]. Individuals with CRS have been reported to have elevated levels of OSM in nasal polyp tissue, and OSM was shown to reduce the barrier function of the nasal mucosa [11]. Higher concentrations of OSM in sputum have been described in asthmatic patients with irreversible airflow obstruction [12,13]. In lung tissue, OSM has been found to increase airway hyper-responsiveness and cause eosinophilia [14]. It is not yet clear how OSM is involved in the development of CRS, however.
We conducted the present study to determine whether OSM is involved in the pathogenesis of CRS. We focused on the association between OSM and cytokines, specifically examining the relationship between OSM and type 1 and type 2 inflammatory cytokines. The role of OSM in the pathogenesis of CRS is also discussed.
2. Materials and Methods
2.1. Study design
This was a case-control study of 71 CRS patients who underwent endoscopic sinus surgery. The diagnosis of sinus disease was based on the patient's history, clinical symptoms, endoscopic findings, and computed tomography (CT) imaging. Patients with a previous sinus surgery were excluded. None of the patients had received topical or systemic steroids for ≥4 weeks prior to the surgery. The CT images were accessed by radiological grading using the Lund-Mackay system [15]. The diagnosis of allergic rhinitis was based on the patient's clinical history, presence of nasal symptoms together with positive nasal eosinophils, and positive allergen-specific IgE antibodies. We classified the CRS patients into ECRS and non-ECRS phenotypes based on the Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) scoring system. The scores include four items: bilateral sinus disease with ethmoid sinus dominant, the presence of nasal polyps, the degree of eosinophilia in peripheral blood, and a mucosal eosinophil count ≥70/high-power field (HPF) [7]. Sixty-eight patients without sinus infection who underwent endonasal surgery served as controls. All control subjects had paranasal sinus mucosa of normal appearance and normal radiological findings.
2.2. Quantitative RT-PCR analysis
Mucosal specimens were obtained from the ethmoid sinus, nasal polyps (if any), and the inferior turbinate at the time of surgery. When CRS was present bilaterally, specimens were taken from both sides. The specimens were divided and either immersed in RNAlater™ solution (Thermo Fisher Scientific, Waltham, MA, USA) for reverse transcription-polymerase chain reaction (RT-PCR) or fixed in 4% paraformaldehyde for immunohistochemistry. A quantitative PCR analysis was performed on an ABI Prism 7300 system (Applied Biosystems, Foster City, CA) as described [16]. Cellular RNA was isolated using RNeasy mini-kits (Qiagen, Valencia, CA). Total RNA was then reverse transcribed to cDNA using a high-capacity RNA-to-cDNA kit (Applied Biosystems) according to the manufacturer’s instructions. Gene expressions were measured on a real-time PCR system using TaqMan Gene Expression Assays (Thermo Fisher Scientific). PCR primers that are specific for OSM (Hs00171165_m1), OSMR β chain (Hs00384276_m1), tumor necrosis factor-alpha (TNF-α) (Hs99999043_m1), IL1-β (Hs01555410_m1), IL-1 receptor (Hs00991010_m1), IL-4 receptor-α (Hs00965056_m1), IL-13 (Hs00174379_m1), IL-13 receptor-α (Hs00609817_m1), and Gap43 (Hs00967138_m1) were used (Thermo Fisher Scientific). Primers for GAPDH (Hs02786624_g1) were used as a reference. Amplifications of the PCR products were quantified by the number of cycles, and the results were analyzed using the comparative cycle threshold (Ct) method (2−ΔΔCt). The quantities of target gene expression are presented as relative ratios compared to the expression of the reference gene (ratio: target gene/GAPDH expression).
2.3. Immunohistochemistry
The primary antibodies used were anti-human OSMR β mouse monoclonal antibody (#SC-271695; Santa Cruz Biotechnology, Dallas, TX) and anti-human GAP43 rabbit polyclonal antibody (#16971-1-AP; Proteintech, Rosemont, IL). Cryostat sections (approx. 5 μm thick) were immersed in 3% H2O2 for 10 min for endogenous peroxidase deactivation and blocked with 10% goat serum in phosphate-buffered saline (PBS) containing 0.1% Tween 20 for 1 hr at room temperature (RT). The slides were then incubated overnight at 4℃ with the primary antibodies. Staining and detection were performed according to the manufacturer’s instructions (Histofine Simple Stain kit; Nichirei Biosciences, Tokyo). Sections were counterstained with hematoxylin. Control specimens with IgG1 isotype control were used to verify that the nonspecific binding was not detectable. Consecutive sections were routinely stained with hematoxylin-eosin (HE) for the assessment of mucosal pathology and the degree of eosinophil infiltration.
2.4. Culture of human bronchial epithelial cells
Human bronchial epithelial cells (BEAS-2B) were purchased from KAC Co. (Kyoto, Japan). The cells were cultured in bronchial epithelial cell growth medium (BEGM™ BulletKit™; Lonza, Walkersville, MD) under serum-free conditions in a 5% CO2 incubator at 37℃. The medium was changed every 2–3 days. After the cells reached 80%–90% confluence, subcultures were performed and then used for the experiments.
2.5. Data analysis
The power and sample size calculations for the study design were performed based on data from a report of the OSM expression in CRS patients [11]. The G*power program ver. 3.1.9.6 was used for estimation (https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower.html, accessed Oct. 13, 2023). For multiple comparisons, a screening of the data for differences was first carried out using the Kruskal-Wallis test. If the analysis gave a significant result, a further comparison was done by the Mann-Whitney U-test for the between-group analysis. Fisher’s exact test was used to compare qualitative data. Correlation coefficients were calculated by the Spearman method. Probability (p)-values <0.05 were considered significant.
All procedures in this study complied with the ethical standards expressed in the Helsinki Declaration. The study protocol was approved by the Institutional Review Board of the Hiroshima University School of Medicine (approval no. E2014-9136). Written informed consent was obtained from all patients prior to their participation.
3. Results
3.1. Background and characteristics of the ECRS and non-ECRS subjects
The background and clinical characteristics of the study population are summarized in Table 1. We divided the 71 CRS patients into ECRS (n=36) and non-ECRS (n=35) groups based on the JESREC criteria. There were no significant age, gender, body mass index (BMI), or smoking-history differences between the patient groups or between these two groups and the controls (n=20). The ECRS group showed significant differences compared to the non-ECRS and control groups in the asthma complication rate, blood eosinophil count, tissue eosinophil count, and CT score. The non-ECRS group showed significant differences in the tissue eosinophil count and CT score compared to the control group.
3.2. Target gene expressions in sinonasal mucosa
3.2.1. Comparison of OSM and OSMR mRNA expressions between the controls and CRS patients
We classified the ethmoid sinus mucosa and nasal polyp (NP) samples obtained at surgery into a control group and a CRS group, and we conducted an RT-PCR analysis to determine the mRNA expression levels of OSM and OSMR-β. The results showed that both OSM and OSMR-β transcripts were predominantly increased in both CRS groups (Figure 1a,b). A similar analysis was performed for the inferior turbinate mucosa; no significant between-group differences were observed. We further subdivided the surgical specimens of the CRS patients into those of the non-ECRS and ECRS patients and compared the mRNA expression levels of OSM and OSMR-β based on phenotype differences. The results showed that OSM was predominantly increased at the ethmoid sinus mucosa in the ECRS group compared to the controls (Figure 2a). No significant differences in the expression of OSMR-β were identified in the ECRS group, but the non-ECRS group showed a predominant increase in the ethmoid sinus mucosa compared to the control group (Figure 2b).
We also observed a significant increase in OSM mRNA levels in the ethmoid sinus and NP mucosa in the ECRS group compared to the control group. In contrast, there was a significant increase in OSMR-β mRNA in the ethmoid sinus mucosa of the non-ECRS group compared to the control group. No significant difference in OSM mRNA levels was observed between the ECRS and control groups.
3.1.2. Correlation with inflammatory cytokines
We further assessed the mRNA expression levels of TNF-α, IL-13, IL-1β, and GAP43 sampled from the same surgical specimens and conducted a correlation analysis to assess possible associations between these cytokines and OSM and OSMR-β (Figure 3). We observed an intimate positive correlation between OSM and OSMR-β (r=0.5215). Additionally, OSM exhibited significant positive correlations with IL-1β (r=0.5591) and IL-13 (r=0.4525). As for OSMR-β, positive correlations were also observed with TNF-α (r=0.5108) and IL-1β (r=0.526). These results indicate that the augmented mRNA levels of OSM and OSMR-β were associated with both type 1 and type 2 inflammation-related cytokines, suggesting that OSM may play a role in both type 1 and type 2 inflammation pathways.
3.3. Immunohistochemical observation
Since transcriptional changes in OSM were associated with CRS pathology and clinical manifestations, we next examined the sinus tissue distribution of OSMR and Gap43 proteins in representative cases. In the non-ECRS group, intense inflammatory cell infiltration with neutrophils and lymphocytes dominated the ethmoid mucosa on conventional histological examination. By contrast, dense eosinophil infiltration was observed in the ECRS group. Representative immunohistological images of OSMR and Gap43 expression in ethmoid sinus mucosa sampled from CRS patients are shown in Figure 4. Basal cell layers of ethmoid sinus epithelial cells and some mesenchymal cells in the submucosal layer were stained positively for OSMR. Positive Gap43 immunoreactivity was localized mainly with nerve bundle fibers in the submucosal area.
3.4. Changes in receptor expression upon OSM stimulation in human airway epithelial cells
Because IL-1β and IL-13 showed significantly positive correlations with OSM in sinonasal specimens, we next examined alterations in the cytokine receptor expressions after stimulating BEAS-2B cells with OSM at 100 ng/mL for various durations (pretreatment, 1 hr, 3 hr, and 6 hr). The mRNA levels of IL-4Rα, IL-13RA1, IL-1R1, and OSMR-β were then measured by RT-PCR. The mRNA expression levels of all examined receptors exhibited a time-dependent increase when the human airway epithelial cells were stimulated with OSM (Figure 5).
4. Discussion
Chronic rhinosinusitis (CRS) is a prevalent condition characterized by symptomatic inflammation of the sinonasal mucosa persisting for >12 weeks, as confirmed by endoscopic examination and/or imaging studies. CRS is categorized into type 2 CRS, which is primarily associated with the Th2 immune response, and non-type 2 CRS, characterized by the prevalence of type 1 and type 3 inflammation [1,2,3,4,5]. Type 2 CRS involves crucial contributions from Th2 cytokines such as IL-4, IL-5, and IL-13, which are produced by Th2 cells, ILC2 cells, and mast cells. Conversely, non-type 2 CRS is marked by elevated levels of IFN-γ, IL-1β, IL-6, IL-8, and IL-17, along with the accumulation of Th1 and Th17 cells.
Eosinophilic chronic rhinosinusitis (ECRS) constitutes a subgroup within chronic rhinosinusitis with nasal polyps (CRSwNP) and is characterized by severe eosinophilic infiltration. This condition poses a significant challenge, as demonstrated by the findings of the JESREC Study [7]. Pathological analyses of ECRS revealed a predominant type 2 inflammation [3,6]. In contrast to non-ECRS patients, individuals with ECRS typically exhibit a poor response to both medical and surgical treatments.
OSM (oncostatin M) is a member of the IL-6 family of cytokines, and it exerts potent effects on stromal cell behavior in various tissues and organs. It is expressed and produced by multiple cell types within the hematopoietic lineage, including T cells, neutrophils, mast cells, macrophages, and eosinophils [9,18].
Human OSM signaling occurs through two receptors. The type I receptor is a heterodimer consisting of leukemia inhibitory factor receptor (LIFR) and gp130, and the type II receptor is a heterodimer composed of OSM receptor beta (OSMRβ) and gp130 [19]. In both scenarios, OSM initially binds to gp130 with low affinity, but effective signaling requires the subsequent recruitment of LIFR or OSMR, leading to the formation of high-affinity competent trimers [10]. In adult tissues, LIFR is expressed at low levels in a variety of epithelial, hematopoietic, and mesenchymal cell types and is not typically associated with pathological processes. In contrast, type II OSMR is highly expressed in numerous non-hematopoietic mesenchymal cells, including fibroblasts, endothelial cells, smooth muscle cells, osteoblasts, and adipocytes. OSMR is also present in hepatocytes, mesothelial cells, glial cells, and epithelial cells in various organs [20,21]. Due to the fact that the expression of LIFR is not commonly linked with pathological processes, studies of OSM often emphasize the crucial roles played by OSMR, rather than LIFR, in mediating OSM biology.
Increased OSM expression has been associated with inflammatory processes leading to barrier dysfunction in dermal and mucosal organs such as the skin, lungs, and intestines. Elevated levels of OSM in nasal polyp tissues of patients with CRS have been encountered, and OSM has been reported to diminish the barrier function of the nasal mucosa [11]. Therapeutic interventions aimed at preventing barrier dysfunction or restoring the barrier once it is compromised could thus potentially be effective in treating inflammatory diseases in human airways, including asthma, CRS, and allergic rhinitis. Targeting OSM may prove beneficial in both non-ECRS and ECRS cases, where barrier dysfunction is sensitive to immune responses. The present study was designed to investigate whether controlling the activation of OSM could be a strategy to enhance and restore polarized and organized epithelial function. As of this writing, no published study has explored the interplay between OSM function and the development of CRS with varying phenotypes in a Japanese population.
Our present analyses revealed that the levels of both OSM and OSMR-β were elevated in surgical specimens obtained from CRS patients. When categorized by the disease groups, the OSMR-β level was predominantly increased in the non-ECRS group, and the OSM level was predominantly increased in the ECRS group. Consistent with earlier findings, both OSM and OSMR-β were found to be heightened in the paranasal sinus mucosa of the present patients diagnosed with CRS. A significant correlation was also observed between each cytokine and OSM as well as OSMR-β. Specifically, the OSM level was correlated with IL-1β and IL-13, while OSMR-β was correlated with TNF-α.
An earlier study revealed that in the context of type 1 inflammation, OSM enhances the expression of OSMR and IL-1R1 in synovial fibroblasts, thereby amplifying the pathological effects of both OSM and IL-1 in rheumatoid arthritis (RA) [22]. In patients with RA, in line with these in vitro discoveries, it was reported that an intra-articular overexpression of OSM along with TNF-α or OSM and IL-1β leads to more extensive joint destruction compared to the impact of any single cytokine alone [23]. Regarding type 2 inflammation, earlier studies have documented heightened levels of OSM in sinus tissue from patients with allergic rhinitis and in the sputum of asthmatic individuals who exhibited irreversible airflow obstruction [12,13]. Additionally, elevated levels of OSM have been observed in nasal polyps from CRS patients, as well as in tissue biopsies and induced sputum from asthmatic patients. Biopsies from patients with eosinophilic esophagitis (EoE) showed increased OSM levels compared to controls [11,24]. In a mouse model, an intratracheal administration of adenovirus that expressed OSM was shown to be sufficient to induce robust type 2 inflammation in the lungs, even without a specific antigen challenge [25].
Those findings indicated that OSM is involved in both type 1 and type 2 inflammation. In our present study, OSM showed correlations with cytokines related to both type 1 and type 2 inflammation. Moreover, we explored the impact of OSM on airway epithelial cells under inflammatory conditions in humans, such as CRS. When BEAS-2B cells were stimulated with OSM and subjected to a gene expression analysis by RT-PCR, notable and temporal increases in the expression levels of IL-13RA1, IL-4Rα, and IL-1R1 were observed.
In summary, our results suggest that OSM levels are increased in the nasal mucosa of CRS patients and are associated with both type 1 and type 2 inflammation OSM was also reported to disrupt nasal mucosal barrier function [11]. Notably, the anti-OSMR-β antibody vixarelimab (KPL-716) is currently undergoing clinical trials as a treatment for nodular prurigo (ClinicalTrials.gov Identifier: NCT03816891) [26]. As our understanding of OSM's role in the pathogenesis of CRS deepens, there is optimism for the development of new therapeutic options for this prevalent disorder.
Author Contributions
Conceptualization, C.I. and S.T.; methodology, S.T.; validation, T.H. and T.U.; formal analysis, C.I. and S.T.; investigation, C.I., Y.O., T.K. (Takashi Kakimoto), T.K. (Tomohiro Kawasumi) K.T. and M.N.; resources, S.T. and T.I.; data curation, T.I.; writing—original draft, C.I. and Y.O.; writing—review and editing, S.T., T.H., and T.U.; visualization, C.I.; supervision, S.T. and A.T.; project administration, S.T.; funding acquisition, C.I. and S.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded partly by a grant from the Japan Society for the Promotion of Science KAKENHI (No. 22K09668), a Health Labor Sciences Research grant (H30-Nanchitou (Nan)-Ippan-016), and the Society for Promotion of International Oto-Rhino-Laryngology (SPIO) Japan, SODA TOYOJI SPIO Research Grant 2022 (No. SR22001). funding.
Institutional Review Board Statement
This study was performed in accordance with the Declaration of Helsinki, with approval from the Institutional Review Board at the Hiroshima University School of Medicine (approval no. Hi-136-4; approval date: 2 November 2022).
Informed Consent Statement
Written informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
We thank Kaoru Shingai for technical assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kato, A.; Peters, A.T.; Stevens, W.W.; Schleimer, R.P.; Tan, B.K.; Kern, R.C.; Endotypes of chronic rhinosinusitis: Relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy 2022, 77, 812-826. [CrossRef]
- Tomassen, P.; Vandeplas, G.; Van, Z.T.; Cardell, L.O.; Arebro, J.; Olze, H.; Förster, R.U.; Kowalski, M.L.; Olszewska, Z.A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immunol. 2016, 137, 1449-1456. PMID: 26949058 . [CrossRef]
- Ishino, T.; Takeno, S.; Takemoto, K.; Yamato, K.; Oda, T.; Nishida, M.; Horibe, Y.; Chikuie, N.; Kono, T.; Taruya, T.; et al. Distinct Gene Set Enrichment Profiles in Eosinophilic and Non-Eosinophilic Chronic Rhinosinusitis with Nasal Polyps by Bulk RNA Barcoding and Sequencing. Int. J. Mol. Sci. 2022, 23, 10 5653. [CrossRef]
- Xu, Z.; Huang, Y.; Delemarre, T.; Cavaliere, C.; Zhang, N.; Bachert, C. Advances in chronic rhinosinusitis in 2020 and 2021. J. Allergy Clin. Immunol. 2022, 149, 854-866. [CrossRef]
- Kato, A.; Schleimer, R.P.; Bleier, B.S. Mechanisms and pathogenesis of chronic rhinosinusitis. J. Allergy Clin. Immunol. 2022, 149, 1491-1503. [CrossRef]
- Fujieda, S.; Imoto, Y.; Kato, Y.; Ninomiya, T.; Tokunaga, T.; Tsutsumiuchi, T.; Yoshida, K.; Kidoguchi, M.; Takabayashi, T.; Eosinophilic chronic rhinosinusitis. Allergol. Int. 2019, 68, 403-412. [CrossRef]
- Tokunaga, T.; Sakashita, M.; Haruna, T.; Asaka, D.; Takeno, S.; Ikeda, H.; Nakayama, T.; Seki, N.; Ito, S.; Murata, J.; et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: the JESREC Study. Allergy 2015, 70, 995-1003. doi: 10.1111/all.12644. PMID: 25945591.
- Rose, T.M.; Bruce, A.G. Oncostatin M is a member of a cytokine family that includes leukemia-inhibitory factor, granulocyte colony-stimulating factor, and interleukin 6. Proc. Natl. Acad. Sci. USA. 1991, 88(19), 8641-5. [CrossRef]
- Tamura, S.; Morikawa, Y.; Miyajima, A.; Senba, E. Expression of oncostatin M in hematopoietic organs. Dev. Dyn. 2002, 225, 327-31. [CrossRef]
- Gearing, D.P.; Comeau, M.R.; Friend, D.J.; Gimpel, S.D.; Thut, C.J.; McGourty, J.; Brasher, K.K.; King, J.A.; Gillis, S.; Mosley, B.; et al. The IL-6 signal transducer, gp130: an oncostatin M receptor and affinity converter for the LIF receptor. Science 1992, 255, 1434-1437. [CrossRef]
- Pothoven, K.L.; Norton, J.E.; Hulse, K.E.; Suh, L.A.; Carter, R.G.; Rocci, E.; Harris, K.E.; Shintani-Smith, S.; Conley, D.B.; Chandra, R.K. Oncostatin M promotes mucosal epithelial barrier dysfunction, and its expression is increased in patients with eosinophilic mucosal disease. J. Allergy Clin. Immunol. 2015, 136, 737-746.e4. [CrossRef]
- Simpson, J.L.; Baines, K.J.; Boyle, M.J.; Scott, R.J.; Gibson, P.G. Oncostatin M (OSM) is increased in asthma with incompletely reversible airflow obstruction. Exp. Lung Res. 2009, 35, 781-94. [CrossRef]
- Kang, H.J.; Kang, J.S.; Lee, S.H.; Hwang, S.J.; Chae, S.W.; Woo, J.S.; Lee, H.M. Upregulation of oncostatin m in allergic rhinitis. Laryngoscope 2005, 115, 2213-6. [CrossRef]
- Fritz, D.K.; Kerr, C.; Fattouh, R.; Llop-Guevara, A.; Khan, W.I.; Jordana, M.; Richards, C.D. A mouse model of airway disease: oncostatin M-induced pulmonary eosinophilia, goblet cell hyperplasia, and airway hyperresponsiveness are STAT6 dependent, and interstitial pulmonary fibrosis is STAT6 independent. J. Immunol. 2011, 186(2), 1107-18. [CrossRef]
- Lund, V.J.; Kennedy, D.W. Quantification for staging sinusitis. The Staging and Therapy Group. Ann. Otol. Rhinol. Laryngol. Suppl. 1995, 167, 17‒21. [CrossRef]
- Takemoto, K.; Lomude, L.S.; Takeno, S.; Kawasumi, T.; Okamoto, Y.; Hamamoto, T.; Ishino, T.; Ando, Y.; Ishikawa, C.; Ueda, T. Functional Alteration and Differential Expression of the Bitter Taste Receptor T2R38 in Human Paranasal Sinus in Patients with Chronic Rhinosinusitis. Int. J. Mol. Sci. 2023, 24(5), 4499. [CrossRef]
- Asano, K.; Ueki, S.; Tamari, M.; Imoto, Y.; Fujieda, S.; Taniguchi, M. Adult-onset eosinophilic airway diseases. Allergy 2020, 75, 3087-3099. [CrossRef]
- Pothoven, K.L.; Schleimer, R.P. The barrier hypothesis and Oncostatin M: Restoration of epithelial barrier function as a novel therapeutic strategy for the treatment of type 2 inflammatory disease. Tissue Barriers 2017, 5, e1341367. [CrossRef]
- Jones, S.A.; Jenkins, B.J. Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer. Nat. Rev. Immunol. 2018, 18, 773-789. [CrossRef]
- Richards, C.D. The enigmatic cytokine oncostatin m and roles in disease. ISRN Inflamm. 2013, 2013, 512103. [CrossRef]
- West, N.R.; Owens, B.M.J.; Hegazy, A.N. The oncostatin M-stromal cell axis in health and disease. Scand. J. Immunol. 2018, 88, e12694. [CrossRef]
- Le Goff, B.; Singbrant, S.; Tonkin, B.A.; Martin, T.J.; Romas, E.; Sims, N.A.; Walsh, N.C. Oncostatin M acting via OSMR, augments the actions of IL-1 and TNF in synovial fibroblasts. Cytokine 2014, 68, 101-109. [CrossRef]
- Hui, W.; Rowan, A.D.; Richards, C.D.; Cawston, T.E. Oncostatin M in combination with tumor necrosis factor alpha induces cartilage damage and matrix metalloproteinase expression in vitro and in vivo. Arthritis Rheum. 2003, 48, 3404-18. [CrossRef]
- Pothoven, K.L.; Norton, J.E.; Suh, L.A.; Carter, R.G.; Harris, K.E.; Biyasheva, A.; Welch, K.; Shintani-Smith, S.; Conley, D.B.; Liu, M.C.; et al. Neutrophils are a major source of the epithelial barrier disrupting cytokine oncostatin M in patients with mucosal airways disease. J. Allergy Clin. Immunol. 2017, 139, 1966-1978.e9. [CrossRef]
- Fritz, D.K.; Kerr, C.; Fattouh, R.; Llop-Guevara, A.; Khan, W.I.; Jordana, M.; Richards, C.D. A mouse model of airway disease: oncostatin M-induced pulmonary eosinophilia, goblet cell hyperplasia, and airway hyperresponsiveness are STAT6 dependent, and interstitial pulmonary fibrosis is STAT6 independent. J. Immunol. 2011, 186, 1107-18. [CrossRef]
- Sofen, H.; Bissonnette, R.; Yosipovitch, G.; Silverberg, J.I.; Tyring, S.; Loo, W.J.; Zook, M.; Lee, M.; Zou, L.; Jiang, G.L.; et al. Efficacy and safety of vixarelimab, a human monoclonal oncostatin M receptor β antibody, in moderate-to-severe prurigo nodularis: a randomised, double-blind, placebo-controlled, phase 2a study. EClinicalMedicine 2023, 57, 101826. [CrossRef]
Figure 1.
Comparison of mRNA expression in sinus mucosa of the controls and all CRS patients detected by RT-PCR. (a) OSM and (b) OSMR-β mRNA levels were quantitatively normalized against GAPDH levels. *p<0.05, **p<0.01. Center lines: median values. Error bars: interquartile ranges.
Figure 1.
Comparison of mRNA expression in sinus mucosa of the controls and all CRS patients detected by RT-PCR. (a) OSM and (b) OSMR-β mRNA levels were quantitatively normalized against GAPDH levels. *p<0.05, **p<0.01. Center lines: median values. Error bars: interquartile ranges.
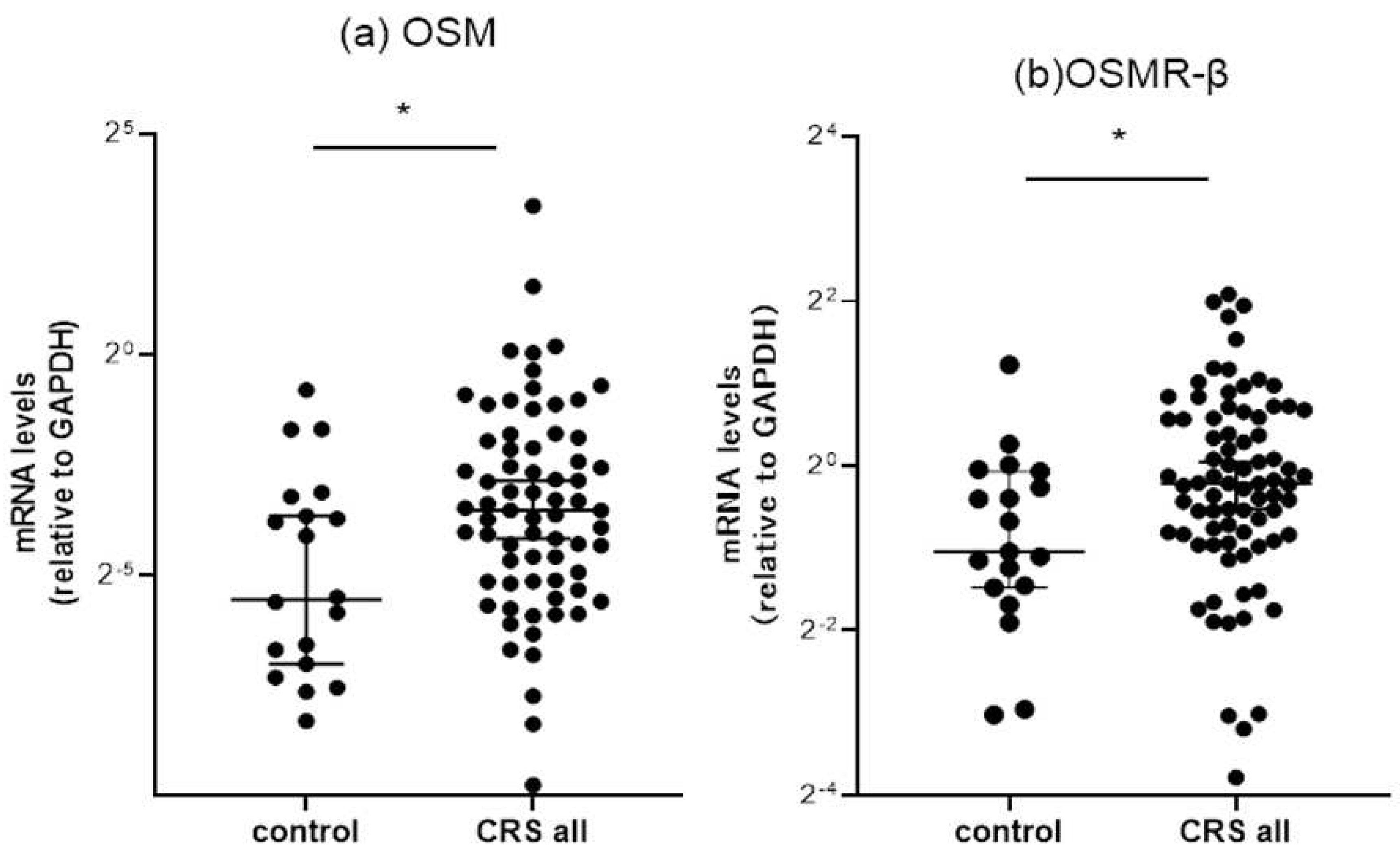
Figure 2.
Comparison of the mRNA expression in paranasal sinus mucosa from the controls, non-ECRS patients, and ECRS patients as detected by RT-PCR. (a) OSM and (b) OSMR-β mRNA levels were quantitatively normalized against GAPDH levels. *p<0.05, **p<0.01. Center lines: median values. Error bars: interquartile ranges.
Figure 2.
Comparison of the mRNA expression in paranasal sinus mucosa from the controls, non-ECRS patients, and ECRS patients as detected by RT-PCR. (a) OSM and (b) OSMR-β mRNA levels were quantitatively normalized against GAPDH levels. *p<0.05, **p<0.01. Center lines: median values. Error bars: interquartile ranges.
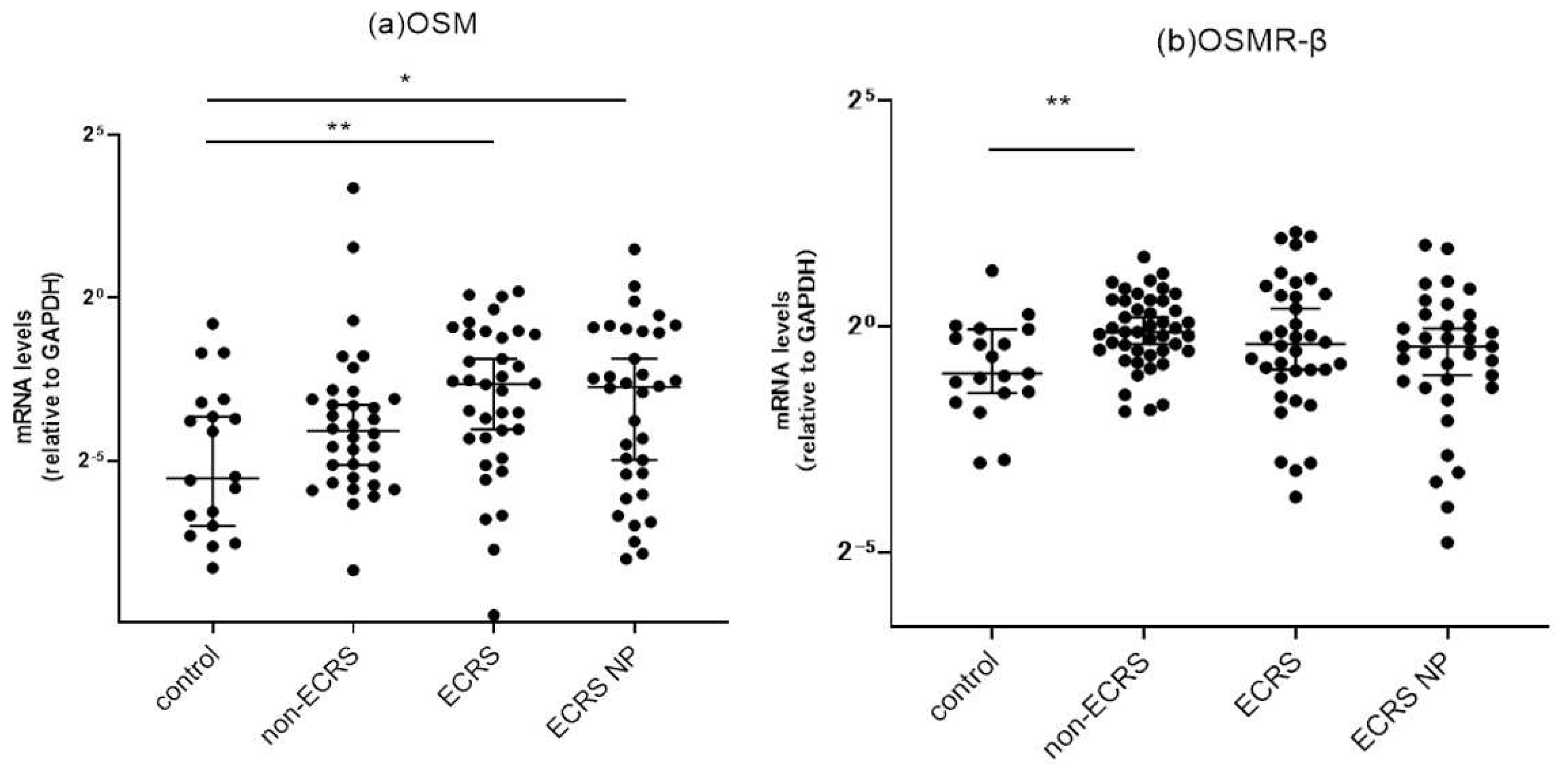
Figure 3.
(a–e) Correlation of mRNA expression levels between OSM and a panel of inflammatory cytokines in sinus mucosa from CRS patients. (f–j) Correlations of mRNA expression levels between OSMR-β and a panel of inflammatory cytokines in sinus mucosa from CRS patients.
Figure 3.
(a–e) Correlation of mRNA expression levels between OSM and a panel of inflammatory cytokines in sinus mucosa from CRS patients. (f–j) Correlations of mRNA expression levels between OSMR-β and a panel of inflammatory cytokines in sinus mucosa from CRS patients.
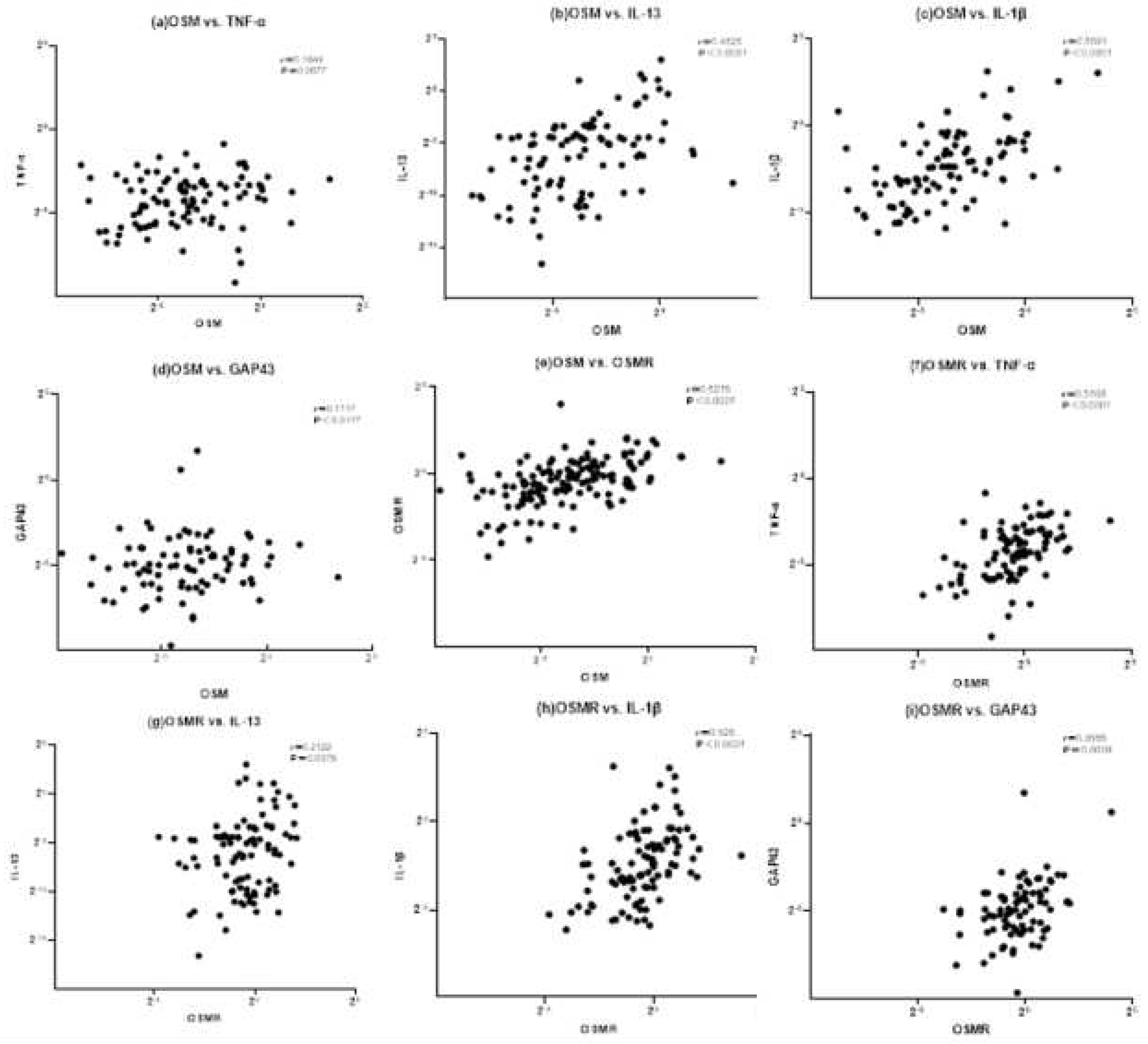
Figure 4.
Representative immunohistological images showing OSMR (a,b) and Gap43 (c) expression in ethmoid sinus mucosa sampled from CRS patients. Basal cell layers of ethmoid sinus epithelial cells and some mesenchymal cells in the submucosal layer stained positively for OSMR. Enlarged view of the intense cytoplasmic staining for OSMR in the basal cells (b, red arrowheads). Positive Gap43 immunoreactivity was localized mainly with nerve bundle fibers in the submucosal area (c, yellow arrowheads). Scale bar: 20 μm.
Figure 4.
Representative immunohistological images showing OSMR (a,b) and Gap43 (c) expression in ethmoid sinus mucosa sampled from CRS patients. Basal cell layers of ethmoid sinus epithelial cells and some mesenchymal cells in the submucosal layer stained positively for OSMR. Enlarged view of the intense cytoplasmic staining for OSMR in the basal cells (b, red arrowheads). Positive Gap43 immunoreactivity was localized mainly with nerve bundle fibers in the submucosal area (c, yellow arrowheads). Scale bar: 20 μm.
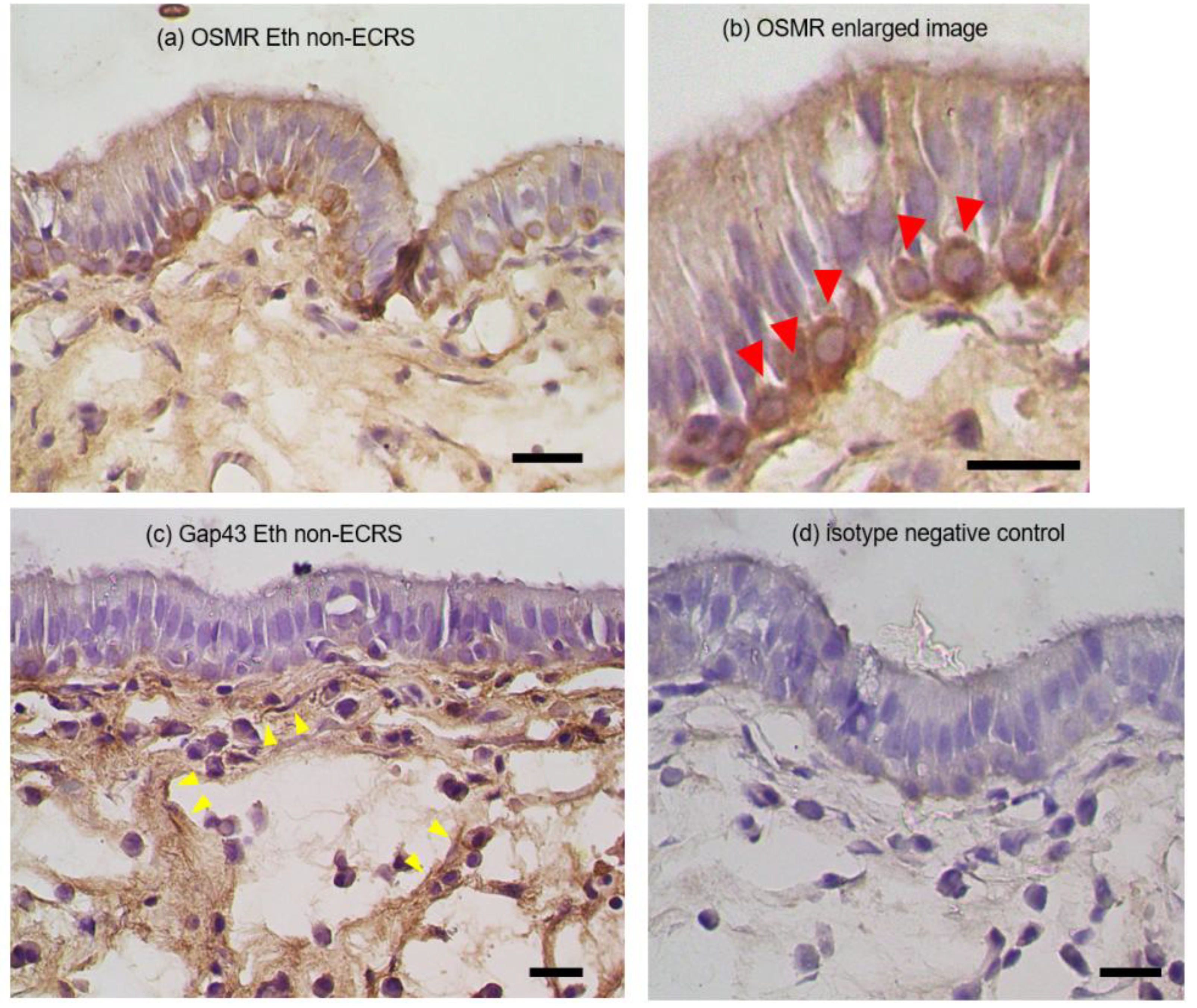
Figure 5.
Time course changes shown by RT-PCR in the mRNA expressions of (a) IL-4Rα, (b) IL-13RA1, (c) IL-1R1, and (d) OSMR-β over time following treatment with 100 ng/mL OSM.
Figure 5.
Time course changes shown by RT-PCR in the mRNA expressions of (a) IL-4Rα, (b) IL-13RA1, (c) IL-1R1, and (d) OSMR-β over time following treatment with 100 ng/mL OSM.
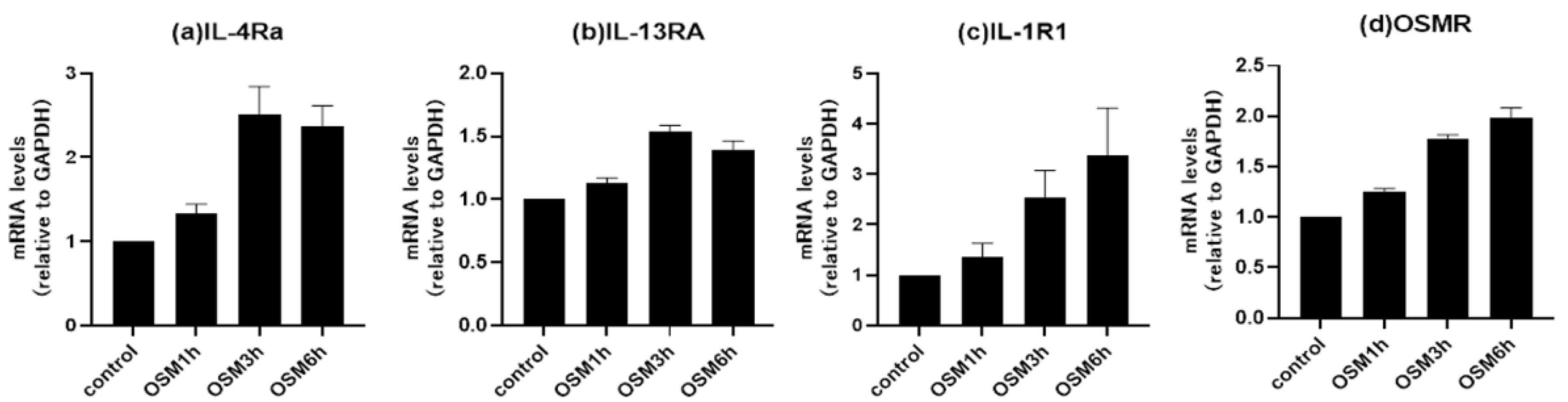

Table 1.
Background and clinical characteristics of the study population.
| controls | non-ECRS | ECRS | |
| Number (male/female) | 20 (6/14) | 35 (21/14) | 36 (18/18) |
| Age (mean±SD) | 49.6±15.6 | 51.5±15.4 | 54.5±10.2 |
| Allergic rhinitis (%) | 8 (53.3%) | 25 (71.4%) | 27 (75%) |
| BMI (kg/mm2) (mean±SD) | 22.4±4.2 | 23.3±3.8 | 22.6±3.6 |
| Bronchial asthma (%) | 1 (5%) | 5 (14.3%) | 17 (47.2%)**††† |
| Blood eosinophils (%) (median, range) | 2.5 (0.0-6.6) | 1.6 (0.0-20.0) | 6.8 (1.1-13.9)****††† |
| Tissue eosinophils (cells/HPF) (median, range) | 4.97 (0.0-23.0) | 7.3 (0.0-70.3) †† | 117.0 (4.0-383.3)****††† |
| CT score (mean±SD) | 2.45±4.24 | 7.7±5.2††† | 14.8±5.0****††† |
Data are mean ± standard deviation (SD), median (range), or number (%). **p<0.01, ****p<0.0001 vs. the other groups. †p<0.05, ††p<0.01, †††p<0.001 vs. the control. BMI: body mass index, ECRS: eosinophilic chronic rhinosinusitis, HPF: high-power field (x400), CT: computed tomography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



