
Submitted:
12 September 2024
Posted:
13 September 2024
You are already at the latest version
Abstract
Health and social needs exist along a dynamic continuum. Recognizing that health status is inextricably impacted by social determinants of health, community paramedicine has opportunities and a responsibility to reduce inequities. The objective of this scoping review was to investigate peer-reviewed and grey literature to explore how community paramedicine supports community needs along a health and social continuum. We conducted a scoping review of English language literature using the JBI Scoping Review methodology. We searched CINAHL, EMBASE, MEDLINE, Google Scholar, and organisational websites. 30 peer-reviewed and 13 grey literature articles met inclusion criteria. The findings describe the ways community paramedicine models evolved from minimising system pressures on emergency health services to addressing health and social needs. A key recommendation across the literature was the need to meaningfully engage communities early in program development to understand how best to implement and co-design integrated service models addressing specific community needs, though there was a lack of evidence to guide this approach. There is a notable lack of evidence pertaining to optimising technologies in program design and implementation. Results highlight opportunities to determine best practices for conducting holistic community needs assessments that include equitable stakeholder engagement and enhancing education to prepare paramedics for expanded roles. Community paramedicine provides opportunities to better meet the needs of structurally marginalised communities. There is a social responsibility and opportunity to engage communities to co-design service delivery, advance paramedic education, and enhance interprofessional collaboration to better support community needs and generate upstream solutions for individuals and communities
Keywords:
paramedic
; community paramedicine
; social needs
; health equity
Introduction
Paramedic practice is continuously evolving and innovating, expanding across healthcare settings as paramedicine continues to establish itself as an essential part of an integrated healthcare model.[1] There is ample opportunity to explore current paramedicine systems to guide future direction for progress and innovation. One example of a more recent innovation in paramedicine includes paramedics in expanded roles, such as extended care and community paramedics.[2] Community paramedicine has evolved from initiatives to reduce the burden on emergency health services and reduce emergency department admissions to programs that use “paramedics to provide immediate or scheduled primary, urgent, and/or specialized healthcare to vulnerable patient populations by focusing on improving equity in healthcare access across the continuum of care.” [3]. A recent international consensus defines community paramedics as practitioners who provide “person-centred care in a diverse range of settings that address the needs of the community. Their practice may include the provision of primary health care, health promotion, disease management, clinical assessment and needs-based interventions. They should be integrated with interdisciplinary healthcare teams which aim to improve patient outcomes through education, advocacy and health system navigation.”[4]
A person receiving healthcare is always immersed in a mix of health and social contexts [5,6]. Moreover, everyone is born into and exists within a health and social continuum [6]. This dynamic continuum means that increases in health incidences may be related to unmet social needs; while those with social privileges and adequate support may experience less frequent or severe health incidences [5,6,7]. Individual and population health is impacted by broad factors, with complex implications dependent on social determinants and economic environments, physical environments, and individuals’ behaviours and inherent characteristics throughout a lifetime [6]. The concept of the health and social continuum illustrates that health and social factors are inextricably connected [5,6].
The social determinants of health (SDH) describe specific social and economic factors that determine health status [6]. These relate to an individual’s position in society and expand beyond individual characteristics to include unearned advantages (i.e., privileges) and unearned disadvantages (i.e., discrimination, structural marginalisation). Experiences of discrimination, racism and trauma, both historical and contemporary, are important social determinants of health that disproportionately impact groups such as Indigenous Peoples, gender and/or sexually diverse individuals, and racialized populations [6,7,8,9].
This means that when paramedics respond to address an individual’s health needs, they also regularly encounter social aspects requiring assessment and care. Community paramedics are uniquely positioned to encounter individuals needing care in their homes and communities, and therefore have access to important information about a person’s environmental, social, and cultural contexts that other health professionals are not directly privy to. The primary health concern may be why paramedics are called to deliver health care - but the health problem may in fact be an outcome of unmet social needs.
Given the historical focus of community paramedicine programs towards meeting healthcare needs, we focused this scoping review on community needs along a health and social continuum. We centred our focus on social needs within the determinants of health, such as poverty, social isolation, culture, and access to health and social services.
Objective
The objective of this scoping review was to identify how community paramedicine supports community needs along a health and social continuum, with a key focus on research implications and how this may inform future practice and health service development [10,11]. We sought to answer the following research questions formulated using the population, concept, context (PCC) framework:
P – people with social needs
C – community paramedicine
C – social determinants of health (health/social continuum)
1) How does community paramedicine support social needs along a health and social continuum?
2.) What current opportunities and gaps exist in the literature regarding community paramedicine support social needs?
3.) What are the implications of this research for paramedicine?
A scoping review was considered the most appropriate approach to map the literature in the community paramedicine, identify concepts, gaps, and sources of evidence to inform policy, practice, and research [11]. In addition, we sought to identify available evidence - initial searches suggested minimal published literature in the field of community paramedicine, and we recognized the value of grey literature in accurately mapping this field. We narrowed the research focus to community paramedicine due to the increasing ways these programs are expanding services within communities, including program development targeting specific structurally marginalised populations and community needs [12].
Conceptual Framework
Prioritising equity and accountability of the profession, Tavares et al., identified paramedic roles at the individual practitioner-level [13], and further outlined principles and enabling factors to lead the progression of the paramedicine profession at the system-level [14]. While all concepts within these complementary studies intersect, the systems level principles of health care along a health and social continuum and social responsiveness, and the enactment by individual practitioners in their role as health and social advocates provides the conceptual lens from which we approached this work [13].
Language
In the context of this review, when the authors state ‘community needs’ we mean both health and social care needs, recognizing that health status is inextricably impacted by social determinants of health. We recognize the importance and evolution of language in accurately describing populations and their intersectional positions in society [15,16]. Therefore, we endeavour to use language within this manuscript that identifies the structural and systemic factors determining societal hierarchies and their inherent power imbalances. We use language such as oppressed, marginalised, and under-resourced to reflect the ways dominant groups determine socioeconomic policies and constructs that oppress some, while privileging others. Populations are not inherently vulnerable, rather vulnerability is an outcome of systemic and structural discrimination, being under-resourced and therefore, marginalised [16]. All people, communities and population groups are equal in value and worth. We use this intentional language to point to the systems of oppression resulting in marginalised outcomes rather than misidentifying certain populations themselves as possessing deficit(s).
Methods
We conducted the scoping review according to the JBI Scoping Review Guidance [17] and reported according to the PRISMA Extension for Scoping Reviews [18]. We conducted a preliminary search of Google Scholar, MEDLINE, and JBI Evidence Synthesis for duplicative efforts and we did not identify any current or in-progress systematic or scoping reviews on the topic.
Protocol
We registered the protocol with the Open Science Framework (https://osf.io/2d9j6/) in April 2023. There are several differences between the protocol and the completed study, and we report these here for transparency. A librarian was unavailable to assist in developing the search strategy due to time constraints and availability. There are slight differences in the search queries conducted based on results from initial searches in each database (see next section). The search strategy was adapted for each information source (see Online Resource 1). We elected to perform a 100% quality check of extracted data over a 20% check - all extracted data were checked for accuracy by one author (AB) who did not partake in the data extraction. As per JBI Scoping review methodology, we did not conduct a quality assessment.
Identification of Relevant Studies
The search strategy targeted peer-reviewed and non-peer reviewed literature. Only articles published at the time of the review were included. We conducted an initial search of Google Scholar and MEDLINE to inform our search strategy. The text words contained in the titles and abstracts of relevant articles (e.g., terms for community paramedicine, health and social continuum, and social needs), and the index terms for these articles were used to refine the search strategy.
We searched CINAHL, MEDLINE, and EMBASE in March and April 2023. Grey literature searches were guided by the CADTH Grey Matters toolkit, limited to primary sources identified through the International Roundtable on Community Paramedicine website (http://ircp.info), Google Scholar and Google [19]. Any reports identified through grey literature searches that were previously identified through database searches were excluded to avoid duplication. We also performed citation searching of the final included studies identified from databases using ‘citationchaser’ software [20].
Study Selection
Studies of any design (including reviews, editorials, and commentaries) were selected if they discussed how community paramedicine supports community needs along a health and social continuum and were published in English. We did not have access to translation resources. (Note that further JBI guidance on this issue is in development at the time of writing this study). Articles were excluded if their primary focus was outside the context of community paramedicine, if they did not address community health and social needs, if they described an economic or geospatial analysis or a study protocol, or if they were available as abstract only (e.g., conference abstracts). We included reviews to ensure that we were able to map the existing literature in a meaningful way.
The review process consisted of title and abstract screening followed by full-text review. A screening form was developed by the primary author (TL) in Covidence (Veritas Health, Melbourne, Australia) and reviewed by both co-authors (JB and AB) [21]. We tested a sample of abstracts prior to screening for sensitivity. Two of the authors (TL and JB) independently screened titles and abstracts. Conflicts were resolved by AB and criteria were refined until we reached agreement. In the second step, two of the authors (TL and JB) independently assessed the full texts of screened articles to determine if they met the criteria. Conflicts were resolved by AB.
Data Charting
Data were extracted by a single reviewer (TL), using a data extraction form created by the primary researcher (TL), informed by the JBI Scoping Review Guidance (see Online Resource 2) [21]. All extracted data (100%) were checked for accuracy by one author (AB) who did not partake in the data extraction. Data extracted included article title, author name and year of publication, country of study, study design, study aim/objective, program setting and type, referral source, health and social needs assessment and education, key findings, discussion, conclusions about community paramedicine supporting health and social needs, and inductive categorisation. We exported the extracted data into Excel 365 (Microsoft, Redmond, WA) for analysis.
Collating, Summarising, and Reporting Results
We used the extracted data to report on the review findings. We used descriptive statistics to report the occurrence of PCC elements. We performed a descriptive qualitative content analysis via basic-level inductive coding to explore and report qualitative data [17]. Two authors (TL and AB) performed this independently in Covidence and resolved any disagreements via discussion. Informed by the WHO Operational framework for monitoring social determinants of health equity [22], codes were deductively grouped to facilitate data summary, reporting, and discussion.
Trustworthiness and Rigour
We ensured trustworthiness of our findings via several means [23]. Data were extracted directly to Excel to reduce transcription errors. We performed multiple comprehensive searches of the literature, and an inductive approach to content analysis to ensure credibility and confirmability. We ensured transferability by including global literature, with no time limitations to account for varying contexts. We ensured dependability by publishing a protocol, ensuring a clear audit trail, and having multiple authors review data during the study. We did not evaluate included studies for quality as per the JBI Scoping Review methodology [21].
Ethics Approval
This scoping review of literature did not involve any human participants or data not already made available on a public platform and therefore no ethics approval was required.
Results
Identification of Potential Studies
Databases and citation searching yielded 1475 records (CINAHL: 135, Embase: 891, Medline: 370, citation searching: 79) which resulted in the removal of 380 duplicates. We screened the remaining 1095 abstracts (see Figure 1).
Full-text screening led to the inclusion of 30 peer-reviewed and 13 grey literature articles (n = 43). The majority of studies were from Canada (n = 19), followed by the USA (n = 17), Australia (n = 5) and the Republic of Ireland (n = 2) (see Table 1).
The methodology utilised most frequently in the peer-reviewed articles was editorials (n = 8), followed by qualitative analysis (n = 6), case reports (n = 5), systematic reviews (n = 3), cohort studies (n = 2), case control study (n = 1), comparative case study (n = 1), cross-sectional analysis (n = 1), diagnostic test accuracy study (n = 1), root cause analysis (n = 1), and quantitative analysis (n = 1). Full study characteristics can be found in Online Resource 3.
Most studies were published in the last decade. In 2022, the most studies were conducted (n = 10), with an observed increase in studies produced since 2020 (see Table 1, Figure 2 and Online Resource 3). The program settings identified were predominantly urban (n = 18). When a program model was indicated, the literature mainly focused on home-visits (n = 22).
Just as health status must be considered along a health and social continuum, we applied a systems-thinking lens as a sensitising approach to understanding community paramedicine within broader health and social structures of society [24]. Systems, broadly described, are an organised assembly of components [25,26]. Systems thinking includes the complex dynamics within social systems, where outcomes must be explored and explained considering relationships between components and their environments, within a system [27]. We structured the codes and findings within the review according to the six categories of the WHO social determinants of health equity framework [22]: Economic security and equality, Education, Physical environment, Social and community context, Health behaviours, and Health care. (see Figure 3 and Table 2). We next highlight key findings from the included studies.
Economic Security and Equality
People experiencing poverty and/or housing insecurity were identified as key populations facing structural barriers to health and wellness in 28 (65%) of the studies [28,29,30,31,32]. Access to safe employment was featured as a barrier to sustainable income in 17 (40%) of reviewed studies [1,33,34,35,36]. While childcare is a consideration for many in the workforce, this potential employment limitation was only amplified in one reviewed study [37]. With community paramedics well-positioned to care for people in their own living environments, the basic need of food security was identified as a social determinant of health in 20 (47%) of studies [38]. When caring for individuals with complex health conditions, it was recognized that “individuals with low incomes are more likely to lack health insurance and have unmet medical needs, including care coordination and access to primary care” [35]. People receiving community paramedic care in outreach programs tended to experience socio-economic insecurity relating to their lack of current employment, health insurance, among other external factors [36]. While living location is addressed under physical environment, Cockrell explored the intersection of rural living as a factor in economic security, stating that “rurality alone does not equate to higher morbidity and mortality rates, but rather exacerbates socioeconomic disadvantage, decreased access to healthcare, occupational risk and environmental hazards. Rural populations are more likely to be exposed to greater risk factors and, on average, have lower levels of education, lower incomes, and reduced access to healthcare services” [34]. Home visit programs demonstrated that community paramedicine programs have capacity to support chronic disease management by focusing on identification of social determinants of health, such as economic support [39,40,41]
Education
The foundation of education as a determinant of health was explored in 30 (70%) studies. Amidst limitations from low health literacy and the complexities of system navigation, community paramedics’ role in care coordination arose as a key aspect of support provided by various program models [28,33,42,43,44,45]. Capabilities for community paramedics to address health needs was demonstrated in reports that paramedics are perceived as trusted health professionals engaged in health promotion and education during home-visits and outreach, and is evident where care coordination and system navigation is a program feature [29,35,36,44,46,47,48,49,50,51]. Programs proved adaptive when ad hoc response was required in instances of crisis, and included supporting persons impacted by flooding disasters and the COVID-19 pandemic [46,52]. Evaluation outcomes beyond health system utilisation were lacking in the literature.
Physical Environment
41 (95%) studies revealed health and social implications relating to individuals’ physical environments. A total of 22 studies (51%) featured home-visit program models, while 11 studies (25.5%) described programs that adapted to create outreach services, specifically addressing the needs of people experiencing homelessness [28,29,32,36,50]. Other programs established clinics within shelters and paramedic specialist units tasked to inner-city areas with high rates of people who are unhoused [28,31,32]. One jurisdiction in the USA leveraged technology by trialling GPS-based mobile health interventions to facilitate care coordination and health education for people experiencing homelessness [29]. For those housed, but facing challenges of low income, community paramedics acted as advocates, facilitating connections and referrals to community resources such as meals, employment and financial services [37,43,46,51,53]. For example, community paramedics identified that food insecurity was more prevalent for older adults living in community [38].
Contemporary healthcare services and record-keeping requires access to reliable internet, email, and mobile devices, yet only three studies (7%) explicitly explored this as an aspect of healthcare. Telemedicine and virtual care were described as features of community paramedicine models [35,46]. When testing a GPS-based mobile health intervention, in addition to providing reminders for medications and appointments, unhoused participants indicated regular access to a cell phone increased their ability to maintain personal safety and social connections [29]. Conversely, lacking access to internet services, digital devices, and durable medical equipment were identified as barriers to health [41]. The COVID-19 pandemic identified the capacity of community paramedicine to innovate programs by leveraging technology to facilitate patient monitoring and virtual visits [46]. Using technology to optimise collaboration between caregivers, interprofessional health providers and community services has given community paramedics a means to address inequities in accessing health care and social services [29,46]. This has been particularly beneficial in addressing gaps in community needs and service access for under-resourced populations who disproportionately faced inequities prior to the pandemic, such as unhoused and Indigenous Peoples in Canada [46]. However, included studies failed to describe strategies to optimise technologies and it remains unclear who is responsible for sourcing and maintaining devices used to facilitate care. There was also a lack of evidence exploring community paramedicine’s role in preventing and addressing climate change and its broad implications for health and healthcare.
Social and Community Context
A total of 35 studies (81%) highlighted the negative impact of social isolation on health, particularly for older adults in both urban and rural settings [33,34,38,43,45,46,49,53,54,55,56,57,58]. Community paramedicines’ ability to address social isolation was evident in programs that used combinations of home-visits and clinics. When these models were embedded in social housing and supportive living sites, they were also well-positioned to address poverty, food insecurity and isolation of older adults [33,38,55]. The proximity that community paramedics have to individuals’ home and work life enables them to assess for harmful physical environments like elder abuse and intimate partner violence. While individuals and communities are not inherently vulnerable, groups made vulnerable due to cultural isolation and systemic and structural inequities such as discrimination on the basis of age, gender, sexuality, race, culture, refugee or immigration status, and incarceration were identified as populations that community paramedics encounter [1,37,41,46,59]. There were no data indicating the ways in which community paramedics are trained to consider inequities due to structural and systemic discrimination in their approach.
Health Behaviours
In 28 studies (65%), the intersection of mental health and substance use were predominant factors in those receiving community paramedicine services. Community paramedics encounter a high proportion of individuals with complex health, including mental health needs, that could benefit from further integration of care [40,60]. In response to high health system utilisation by people experiencing homelessness, and building on proven effectiveness of mobile outreach, an innovative “City Centre Team” (CCT) was created in a major Canadian city to focus care needs on people who are unhoused with a high prevalence of substance use [28,30,47]. Evaluation demonstrated the capability of community paramedicine to address health and social needs of people experiencing homelessness by using interdisciplinary and interprofessional collaboration and communication across community, social, and health services. Similar mobile outreach models have proved beneficial in other major cities across Canada and the USA, while other jurisdictions provide mental health care via community clinics [31,32,43,54,55]. Langabeer et al., highlighted that individuals who use substances often avoid seeking treatment, further reinforcing the benefits of outreach models in bringing care to people who use drugs in communities [36]. Considering the high instance of substance use-related calls, community paramedicine’s role in harm reduction strategies was not well explored in the included studies. In addition, while community paramedicine is rapidly expanding, initiatives to address mental health needs remain fragmented and there is a greater need for advocacy and attention to the social, economic and policy levels upstream of the point of individual crisis [60].
Health care
Access to health and social services was the predominant issue addressed in studies included in this review, with 42 of 43 (98%) included studies addressing community needs within this category. The disparity of workforce and subsequent service provision in rural contexts was a common challenge motivating both community-initiated and system-initiated community paramedicine development in remote and rural settings [34,46,59,61]. Risk of readmission post-discharge was found to increase when individuals met challenges managing existing chronic conditions due to lack of access to medications combined with low health literacy [42,62]. For many individuals, outreach community paramedicine programs served as a source and bridge to care that would otherwise be inaccessible [28,29,31,33,36,45,46,50]
Community Needs Assessment
A total of 36 studies (84%) reported on models of service delivery. In addition to outlining the service models, studies discussed the need for programs to be designed around community needs [2,28,48,51,59]. There was alignment across studies recommending engaging caregivers, broader stakeholders, and community members early when designing needs-based programming. Studies shared consensus on the priority to develop community needs approaches that are person-centred, incorporate co-design, and consider the complex barriers to health and social care in structurally oppressed populations [1,2,37,40,46,59,60,63].
Social Needs Education
Paramedics received additional education focused on SDH in 24 of the included studies (56%), while Logan identified the benefit of paramedics receiving cross-training as Community Health Workers (CHW) [48]. Community paramedics are described as collaborating with allied health professional, social and community groups, amplifying the necessity of integrated and collaborative approaches to bolster the supports required to address social needs in community care planning. Leyenaar identified that community paramedicine patients demonstrated higher proportions of complex care needs, including chronic disease and mental health needs, when compared to respective home care and community services support clients [40]. Education has been identified as a key enabler to advancing community paramedicine and meeting such complex needs. While community paramedicine education and training was found to be diverse in allowing learning to address patient needs along a health and social continuum, the optimal prerequisite education and experience requirements for roles practising in community paramedicine was unclear.[2,64]
Discussion
This scoping review aimed to explore how community paramedicine supports community needs along a health and social continuum and to identify gaps and opportunities for future research. We identified 43 articles from four countries published between 2003 and 2023. Our findings demonstrate that community paramedicine has evolved and is continuing to innovate to support community needs through a variety of program models across various settings.
Community paramedicine continues to expand in the United Kingdom, the Republic of Ireland, Finland, Australia, New Zealand, Canada and the USA [2,12,55,56,58,65]. This model of care is rapidly evolving in response to ageing populations and to address gaps in primary care [2,57,58]. Expansion of the paramedicine specialty has been largely motivated by health system utilisation measures, where emergency department avoidance and readmission is a key driver [2,55,56,58]. Recognizing the benefits to optimising service utilisation, attention should be called to including additional indicators such as healthcare experiences, outcomes, and improved social support. Where paramedic practice has traditionally taken a reactive and pathogenic approach to healthcare delivery, Cockrell advances the benefit of applying a salutogenic approach where care focuses on supporting health and well-being rather than factors that cause disease [34]. Programs are engaging with this concept in increasingly proactive ways, such as recognizing and targeting social needs as key determinants of health [1,41,66]. Community paramedicine has potential to enable values-based care models by integrating services with primary health and social services to reduce barriers for structurally marginalised populations [51,53,67,68].
Advances in technology enable innovations in healthcare to bridge access to service gaps, including telehealth, remote patient monitoring and virtual care, particularly in response to the COVID-19 pandemic [33,46,55]. Despite this, the evidence fails to provide guidance on optimal approaches to leveraging technologies in coordinating and supporting care. Recommendations exist to develop standards for virtual care, social media use, and enhancing cross-jurisdiction communications to rapidly coordinate during crisis response [69,70]. This will also require developing standards for data stewardship in program evaluation, quality improvement, and research [71]. There is a need to engage health systems planners to determine the most appropriate responsibility for sustainably sourcing, maintaining and the ongoing education necessary to optimise technology in paramedic care.
There were benefits observed when paramedics integrated the extension of person-centred palliative approaches to care into the home, and thereby optimising quality of life along the trajectory of illness [72]. Within an Indigenous community in the remote north of Canada, community paramedicine could address many health and social service gaps [3,59]. Authors cautioned against a one-size-fits-all approach and highlighted the need for programs to better address the needs of communities by including relevant program indicators [2,3,28,59]. A key recommendation across the literature was the need to meaningfully engage broader partners and communities early in program planning to understand how best to co-design and implement an integrated service model that addresses the specific needs of each community [2,28,34,48,59,60]. There were also cautions that focusing on increasing access to health and social services provided by the state-only risks further embedding settler colonialism in health and social equity efforts[73]. This requires paramedicine leaders to critically examine whose voices and perspectives are included at decision-making tables and whose are not. This reinforces the necessity to further study and incorporate equitable practices for community and stakeholder engagement and apply learnings from others when assessing community need [48,51,59].
The move towards tertiary education for community paramedicine specialisation in some jurisdictions provides greater opportunities for interprofessional learning to prepare paramedics as integrated members of the primary and greater healthcare team [2,12,34,65,74]. While studies mentioned additional paramedic training on SDH, what this training entailed was unclear or implicit, and inconsistencies in this requirement across studies indicate opportunity to enhance this education to better prepare paramedics to respond to the complexities of care within the health and social continuum [2,74]. Educators and program developers should expand beyond paramedicine to examine what can be learned from other professions in addressing equity along a health and social continuum. Paramedicine will reciprocally benefit from partnering, mentorship and collaboration with broad health and social professionals [68].
While some studies in this review targeted social needs, few programs appeared to examine the implications of intersectionality and structural competency on health and social inequities [1,60,63]. This intentionality was applied in a study that examined women’s experiences participating in a community paramedic program, where participants reported an overall reduction in barriers to care that specifically prioritised women’s health needs [44]. Evidence shows workforce diversity gaps have a direct effect on care and outcomes, revealing that practitioners employed in more homogeneous environments possess greater risk of providing inequitable care [75,76,77,78,79]. Community paramedicine should lead responsibly by applying knowledge in the provision of intersectionality and structural competency to workforce recruitment strategies, practitioner education and systems-level planning [9,15,16,80,81]. A core tenet of community paramedicine is cultivating trusting relationships, and while paramedics are generally perceived as trusted health professionals, there is an opportunity to examine how program planning and implementation can be optimised by recruiting practitioners who represent and reflect the cultures of the communities served [48,75,82].
Finally, as evidenced by this review, community paramedicine is rapidly evolving to provide responsive and integrated healthcare to communities. However, as Ford-Jones cautions - paramedics face tensions between implementing beneficial practice in response to unmet social needs, and the need to influence policymakers within health and non-health professions [60]. Paramedics must take appropriate action at the public policy level to develop evidence-informed, upstream solutions to address broader determinants of health in sustainable ways [60,83]. Training paramedics to address increasing mental health needs is not a viable option to address the intersectional and structural barriers that must be addressed via broader policy [34,36,48,60]. Acknowledging that political and socioeconomic factors are key determinants of health, there is a need for paramedicine broadly to determine roles in health and social advocacy to influence policy that commits to health equity and justice, for all [13,14,73,80,81].
Future Directions
While our findings demonstrate that community paramedicine has evolved to support community health and social needs through a variety of program models across various settings, gaps exist for future research in community paramedicine. Future studies should aim to contribute trustworthy quantitative, qualitative, and mixed-methods evidence to this growing body of literature. For example, guided by the principles of patients and their communities first and social responsiveness, it is paramount to ensure community paramedicine program design is needs-based [14,81]. It is important to determine key elements to inform a framework guiding community needs assessments. To address healthcare inequities that are a result of system-centred programming, those developing community paramedicine must commit to co-designing service models, specifically including perspectives from structurally marginalised groups [30,59,84]. Considering an intersectional lens, paramedicine leaders will require guidance on how to engage in equitable stakeholder engagement, including amplifying voices of people receiving care and their caregivers. Community paramedicine leaders and strategists should seek to identify transferable strategies from outside paramedicine and health-adjacent professions and seek opportunities to integrate care to optimise initiatives addressing healthcare along a health and social continuum. These intersecting areas of study opportunities need to be thoroughly explored and strategies implemented in ongoing effort to eliminate health outcome gaps.
Limitations
Despite efforts to be comprehensive, we may have missed relevant studies in this review. Areas where communities are leading development of community-led paramedicine programs to address local needs may not have published or reported work for inclusion. We acknowledge that the inclusion of English-only papers risks overlooking potential studies of expanded paramedic roles or community paramedicine programs in countries or jurisdictions where English is not the primary language.
Conclusion
Health system and resource utilisation remains a predominant motivator behind developing community paramedicine programs. Community paramedicine programs support community health and social needs through a variety of service models. As paramedicine program models evolve to address the needs of under-resourced and marginalised populations, system designers need to engage in community needs assessments to co-design service delivery. Better understanding of community needs will help to enhance paramedic education and engage interprofessional collaboration to best support individuals and communities. Paramedicine leaders, including paramedics themselves, have a social responsibility to advocate for and implement integrated approaches to service delivery and care that addresses the needs of the person receiving care and their communities in ways that consider the complex intersections of health and social conditions to optimise health equity and justice [1,13,14,63,75].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
TL: conceptualization (lead); methodology (lead); formal analysis (lead); writing – original draft (lead); writing – review and editing (supporting). JB: formal analysis (supporting); writing – review and editing (equal). AB: conceptualization (supporting); methodology (supporting); writing – original draft (supporting); formal analysis (supporting); writing – review and editing (lead); Supervision (lead).
Data Availability Statement
Search results and screening information can be obtained from the corresponding author.
Preprint
The findings of this study were previously made available as a preprint. Lunn, T.; Bolster, J.; Batt, A. Community Paramedicine Supporting Community Needs: A Scoping Review. Preprints 2023, 2023100999. https://doi.org/10.20944/preprints202310.0999.v2 [86]
Acknowledgements
We acknowledge this collaborative research was conducted on colonised Indigenous lands now referred to as Canada. We reside on traditional lands belonging to the Tla’amin Nation, Williams Treaty and Treaty 20 Michi Saagiig territory and in the traditional territory of the Michi Saagiig and Chippewa Nations, Métis Region 6, and Tk’emlups te Secwépemc in the traditional and unceded territory of the Secwépemc. These lands are home to the many diverse First Nations, Inuit, and Métis Peoples whose ancestors have stewarded this land since time immemorial [9,85].
Statements and Declarations
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author(s) received no financial support for the research, authorship, and/or publication of this article. This scoping review of literature did not involve any human participants or data not already made available on a public platform and therefore no ethics approval was required.
References
- Allana, A., & Pinto, A. (2021). Paramedics Have Untapped Potential to Address Social Determinants of Health in Canada. Healthcare Policy | Politiques de Santé, 16(3), 67–75. https://doi.org/10.12927/hcpol.2021.26432.
- Shannon, B., Eaton, G., Lanos, C., Leyenaar, M., Nolan, M., Bowles, K.-A., … Batt, A. (2022). The development of community paramedicine; a restricted review. Health & Social Care in the Community, 30(6), e3547–e3561. https://doi.org/10.1111/hsc.13985.
- CSA Group. (2017). CAN/CSA Z1630:17 Community paramedicine: Framework for program development. Toronto: CSA Group.
- Shannon, B., Baldry, S., O’Meara, P., Foster, N., Martin, A., Cook, M., … Miles, A. (2023). The definition of a community paramedic: An international consensus. Paramedicine, 20(1), 4–22. https://doi.org/10.1177/27536386221148993.
- Essington, T., Bowles, R., & Donelon, B. (2018). The Canadian Paramedicine Education Guidance Document. Ottawa: Paramedic Association of Canada.
- World Health Organization. (2008). Closing the gap in a generation: health equity through action on the social determinants of health - Final report of the commission on social determinants of health. Geneva: World Health Organization. Retrieved from https://www.who.int/publications-detail-redirect/WHO-IER-CSDH-08.1.
- Porroche-Escudero, A. (2022). Health systems and quality of healthcare: bringing back missing discussions about gender and sexuality. Health Systems, 1–7. https://doi.org/10.1080/20476965.2022.2096487.
- IISD. (2023, June 7). Who Is Being Left Behind in Canada? International Institute for Sustainable Development. International Institute for Sustainable Development. Retrieved March 31, 2023, from https://www.iisd.org/articles/insight/who-being-left-behind-canada.
- Truth and Reconciliation Commission of Canada. (2015). Honouring the truth, reconciling for the future: summary of the final report of the Truth and Reconciliation Commission of Canada. Retrieved from http://epe.lac-bac.gc.ca/100/201/301/weekly_acquisition_lists/2015/w15-24-F-E.html/collections/collection_2015/trc/IR4-7-2015-eng.pdf.
- Arksey, H., & O’Malley, L. (2005). Scoping studies: towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616.
- Munn, Z., Peters, M. D. J., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18(1), 143. https://doi.org/10.1186/s12874-018-0611-x.
- Shannon, B., Batt, A. M., Eaton, G., Bowles, K.-A., & Williams, B. (2021). Community Paramedicine Practice Framework Scoping Exercise. Retrieved from https://www.phecit.ie/Custom/BSIDocumentSelector/Pages/DocumentViewer.aspx?id=oGsVrspmiT0dOhDFFXZvIz0q5GYO7igwzB6buxHEgeAwoe6hhx3Qzd%252fCRqybt66szE0PsYSC8wDndnJ4ZZBtixIuvZKX1%252f4wN58oIZl8uwPebsYwRo0IvX6hVCWn5T8FxWsBQJfWSaVSf%252bRJ%252b80BMTb0c8d%252b63Hj.
- Tavares, W., Bowles, R., & Donelon, B. (2016). Informing a Canadian paramedic profile: framing concepts, roles and crosscutting themes. BMC Health Services Research, 16(1), 477. https://doi.org/10.1186/s12913-016-1739-1.
- Tavares, W., Allana, A., Beaune, L., Weiss, D., & Blanchard, I. (2021). Principles to Guide the Future of Paramedicine in Canada. Prehospital Emergency Care, 1–11. https://doi.org/10.1080/10903127.2021.1965680.
- Cho, S., Crenshaw, K. W., & McCall, L. (2013). Toward a Field of Intersectionality Studies: Theory, Applications, and Praxis. Signs: Journal of Women in Culture and Society, 38(4), 785–810. https://doi.org/10.1086/669608.
- Nixon, S. A. (2019). The coin model of privilege and critical allyship: implications for health. BMC Public Health, 19(1), 1637. https://doi.org/10.1186/s12889-019-7884-9.
- Peters, M. D., Godfrey, C., McInerney, P., Munn, Z., Tricco, A. C., & Khalil, H. (2024). 10. Scoping reviews. In E. Aromataris, C. Lockwood, K. Porritt, B. Pilla, & Z. Jordan (Eds.), JBI Manual for Evidence Synthesis. JBI. https://doi.org/10.46658/JBIMES-24-09.
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., … Straus, S. E. (2018). PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850.
- Grey Matters: a practical tool for searching health-related grey literature | CADTH. (n.d.). Retrieved June 11, 2023, from https://www.cadth.ca/grey-matters-practical-tool-searching-health-related-grey-literature.
- Haddaway, N. R., Grainger, M. J., & Gray, C. T. (2021, February 16). citationchaser: An R package and Shiny app for forward and backward citations chasing in academic searching. Zenodo. https://doi.org/10.5281/zenodo.4543513.
- Peters, M. D. J., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., … Khalil, H. (2020). Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis, 18(10), 2119–2126. https://doi.org/10.11124/JBIES-20-00167.
- World Health Organization. (2024). Operational framework for monitoring social determinants of health equity. Geneva, Switzerland: World Health Organization. Retrieved from https://www.who.int/publications-detail-redirect/9789240088320.
- Thomas, E., & Magilvy, J. K. (2011). Qualitative Rigor or Research Validity in Qualitative Research. Journal for Specialists in Pediatric Nursing, 16(2), 151–155. https://doi.org/10.1111/j.1744-6155.2011.00283.x.
- Batt, A. M., Williams, B., Brydges, M., Leyenaar, M., & Tavares, W. (2021). New ways of seeing: supplementing existing competency framework development guidelines with systems thinking. Advances in Health Sciences Education. https://doi.org/10.1007/s10459-021-10054-x.
- Friedman, B. (1997). Systems theory. In Theories and practice in social work (In J. Brandall., pp. 3–17). The Free Press.
- Sturmberg, J. P. (2007). Part 1 clinical application. Australian Family Physician, 36(3), 170–173.
- Kannampallil, T. G., Schauer, G. F., Cohen, T., & Patel, V. L. (2011). Considering complexity in healthcare systems. Journal of Biomedical Informatics, 44(6), 943–947. https://doi.org/10.1016/j.jbi.2011.06.006.
- Taplin, J., Dalgarno, D., Smith, M., Eggenberger, T., & Ghosh, S. M. (2023). Community paramedic outreach support for people experiencing homelessness. Journal of Paramedic Practice, 15(2).
- Moczygemba, L. R., Thurman, W., Tormey, K., Hudzik, A., Welton-Arndt, L., & Kim, E. (2021). GPS Mobile Health Intervention Among People Experiencing Homelessness: Pre-Post Study. JMIR mHealth and uHealth, 9(11), e25553. https://doi.org/10.2196/25553.
- Taplin, J. G., Barnabe, C. M., Blanchard, I. E., Doig, C. J., Crowshoe, L., & Clement, F. M. (2022). Health service utilization by people experiencing homelessness and engaging with community paramedics: a pre–post study. Canadian Journal of Emergency Medicine, 24(8), 885–889. https://doi.org/10.1007/s43678-022-00387-w.
- Ridgeway, J. L., Wissler Gerdes, E. O., Zhu, X., Finnie, D. M., Wiepert, L. M., Glasgow, A. E., … McCoy, R. G. (2023). A Community Paramedic Clinic at a Day Center for Adults Experiencing Homelessness. NEJM Catalyst, 4(4). https://doi.org/10.1056/CAT.22.0300.
- Stickler, Z. R., Carlson, P. N., Myers, L., Schultz, J. R., Swenson, T., Darling, C., … McCoy, R. G. (2021). Community Paramedic Mobile COVID-19 Unit Serving People Experiencing Homelessness. The Annals of Family Medicine, 19(6), 562–562. https://doi.org/10.1370/afm.2709.
- Ruest, M. (2016). County of Renfrew Paramedic Service Resilience Program Contribution to the Health Promotion Strategies that Address the Inequities Associated with Social Isolation of Seniors in the County of Renfrew. Canadian Paramedicine, 39(3).
- Cockrell, K. R., Reed, B., & Wilson, L. (2019). Rural paramedics’ capacity for utilising a salutogenic approach to healthcare delivery: a literature review. Australasian Journal of Paramedicine, 16. https://doi.org/10.33151/ajp.16.635.
- Georgiev, R., Stryckman, B., & Velez, R. (2019). The Integral Role of Nurse Practitioners in Community Paramedicine. The Journal for Nurse Practitioners, 15(10), 725–731. https://doi.org/10.1016/j.nurpra.2019.07.019.
- Langabeer, J. R., Persse, D., Yatsco, A., O’Neal, M. M., & Champagne-Langabeer, T. (2021). A Framework for EMS Outreach for Drug Overdose Survivors: A Case Report of the Houston Emergency Opioid Engagement System. Prehospital Emergency Care, 25(3), 441–448. https://doi.org/10.1080/10903127.2020.1755755.
- Thomas-Henkel, C., & Schulman, M. (n.d.). Screening for Social Determinants of Health in Populations with Complex Needs: Implementation Considerations.
- Pirrie, M., Harrison, L., Angeles, R., Marzanek, F., Ziesmann, A., & Agarwal, G. (2020). Poverty and food insecurity of older adults living in social housing in Ontario: a cross-sectional study. BMC Public Health, 20(1), 1320. https://doi.org/10.1186/s12889-020-09437-3.
- Swayze, D. (2017). The Community Paramedicine Approach to the Opioid Epidemic. JEMS: EMS, Emergency Medical Services - Training, Paramedic, EMT News. Retrieved from https://www.jems.com/mobile-integrated-healthcare/the-community-paramedicine-approach-to-the-opioid-epidemic/.
- Leyenaar, M. S., McLeod, B., Jones, A., Brousseau, A.-A., Mercier, E., Strum, R. P., … Costa, A. P. (2021). Paramedics assessing patients with complex comorbidities in community settings: results from the CARPE study. Canadian Journal of Emergency Medicine, 23(6), 828–836. https://doi.org/10.1007/s43678-021-00153-4.
- Naimi, S., Stryckman, B., Liang, Y., Seidl, K., Harris, E., Landi, C., … Gingold, D. B. (2023). Evaluating Social Determinants of Health in a Mobile Integrated Healthcare-Community Paramedicine Program. Journal of Community Health, 48(1), 79–88. https://doi.org/10.1007/s10900-022-01148-7.
- Sokan, O., Stryckman, B., Liang, Y., Osotimehin, S., Gingold, D. B., Blakeslee, W. W., … Rodriguez, M. (2022). Impact of a mobile integrated healthcare and community paramedicine program on improving medication adherence in patients with heart failure and chronic obstructive pulmonary disease after hospital discharge: A pilot study. Exploratory Research in Clinical and Social Pharmacy, 8, 100201. https://doi.org/10.1016/j.rcsop.2022.100201.
- Olynyk, C. (2010). Toronto EMS Community Paramedicine Program Overview 2010. Toronto, Canada. Retrieved from https://ircp.info/Portals/11/Downloads/Expanded%20Role/Toronto%20CREMS/Toronto%20EMS%20Community%20Paramedicine%20Program%20Overview%202010.pdf?ver=Vn9xFmVDYfFxk0pJG0QiFw%3d%3d.
- Schwab-Reese, L. M., Renner, L. M., King, H., Miller, R. P., Forman, D., Krumenacker, J. S., & DeMaria, A. L. (2021). “They’re very passionate about making sure that women stay healthy”: a qualitative examination of women’s experiences participating in a community paramedicine program. BMC Health Services Research, 21(1), 1167. https://doi.org/10.1186/s12913-021-07192-8.
- Pennel, C. L., Tamayo, L., Wells, R., & Sunbury, T. (2016). Emergency Medical Service-based Care Coordination for Three Rural Communities. Journal of Health Care for the Poor and Underserved, 27(4A), 159–180. https://doi.org/10.1353/hpu.2016.0178.
- Batt, A. M., Hultink, A., Lanos, C., Tierney, B., Grenier, M., & Heffern, J. (2021). Advances in Community Paramedicine in Response to COVID-19.
- Boland, L. L., Jin, D., Hedger, K. P., Lick, C. J., Duren, J. L., & Stevens, A. C. (2022). Evaluation of an EMS-Based Community Paramedic Pilot Program to Reduce Frequency of 9-1-1 Calls among High Utilizers. Prehospital Emergency Care, 1–8. https://doi.org/10.1080/10903127.2022.2086653.
- Logan, R. I. (2022). ‘I Certainly Wasn’t as Patient-Centred’: Impacts and Potentials of Cross-Training Paramedics as Community Health Workers. Anthropology in Action, 29(3), 14–22. https://doi.org/10.3167/aia.2022.290302.
- McManamny, T. E., Boyd, L., Sheen, J., & Lowthian, J. A. (2022). Feasibility and acceptability of paramedic-initiated health education for rural-dwelling older people. Health Education Journal, 81(7), 848–861. https://doi.org/10.1177/00178969221125622.
- Mund, E. (2016). Taking Care to the Streets. EMSWorld. Retrieved from https://lw.hmpgloballearningnetwork.com/site/emsworld/article/12179630/taking-mih-cp-care-to-the-streets.
- Rahim, F., Jain, B., Patel, T., Jain, U., Jain, P., & Palakodeti, S. (2022). Community Paramedicine: An Innovative Model for Value-Based Care Delivery. Journal of Public Health Management and Practice, Publish Ahead of Print. https://doi.org/10.1097/PHH.0000000000001683.
- Gainey, C. E., Brown, H. A., & Gerard, W. C. (2018). Utilization of Mobile Integrated Health Providers During a Flood Disaster in South Carolina (USA). Prehospital and Disaster Medicine, 33(4), 432–435. https://doi.org/10.1017/S1049023X18000572.
- Strum, R. (2015). Paramedics as Health Advocates. Canadian Paramedicine, 38(6).
- Newall, N. (2015). Who’s At My Door Project: How organizations find and assist socially isolated older adults (p. 44). Winnipeg, Manitoba: Centre on Aging. Retrieved from https://umanitoba.ca/centre-on-aging/sites/centre-on-aging/files/2021-02/centre-aging-research-publications-report-who%27s-at-my-door-project.pdf.
- Nolan, M., Hillier, T., & D’Angelo, C. (2012). Community Paramedicine in Canada. Retrieved from https://ircp.info/Portals/11/Downloads/Policy/Comm%20Paramedicine%20in%20Canada.pdf?ver=XJMZv0HNBUMEpxqc9etOFg%3d%3d.
- Raven, S., Tippett, V., Ferguson, J.-G., & Smith, S. (2006). An exploration of expanded paramedic healthcare roles for Queensland (p. 100). Queensland, Australia: Australian Centre for Prehospital Research. Retrieved from https://ircp.info/portals/11/downloads/expanded%20role/queensland%20expanded%20role.pdf.
- Hay, D., Varga-Toth, J., & Hines, E. (2006). Frontline Health Care in Canada: Innovations in Delivering Services to Vulnerable Populations (Rresearch Report No. F, 63) (p. 96).
- PHECC. (2020). The introduction of Community Paramedicine into Ireland. Retrieved from https://www.phecit.ie/Custom/BSIDocumentSelector/Pages/DocumentViewer.aspx?id=oGsVrspmiT0dOhDFFXZvIz0q5GYO7igwzB6buxHEgeDKMmmW%252fnE3lbsxRkYxd6aQYk7snfcymr0EG16DvMZvqmNsz5SqfTY2bCjDsrkmvfchr0f6fWdxsRfEpP0eHF2WFYnnA1HA6sq8buhbiuE7hUxFSMEFO%252btRyWB31RTiP1quSbFCsa%252bZGt6Ri4g1h1nnWZcXksZCSqw%253d.
- Ashton, C., & Leyenaar, M. S. (2019). Health Service Needs in the North: A Case Study on CSA Standard for Community Paramedicine. Canada: Canadian Standards Association. Retrieved from https://www.csagroup.org/wp-content/uploads/CSA-Group-Research-Health-Service-Needs-in-the-North-1.pdf.
- Ford-Jones, P. C., & Daly, T. (2022). Filling the gap: Mental health and psychosocial paramedicine programming in Ontario, Canada. Health & Social Care in the Community, 30(2), 744–752. https://doi.org/10.1111/hsc.13189.
- Misner, D. (2003). Community Paramedicine: A Part of an Integrated Health Care System. Retrieved from https://ircp.info/Portals/11/Downloads/Expanded%20Role/Community%20Paramedicine.pdf?ver=TfO8p2_1qDzq4LlLyNLlqA%3d%3d.
- Buitrago, I., Seidl, K. L., Gingold, D. B., & Marcozzi, D. (2022). Analysis of Readmissions in a Mobile Integrated Health Transitional Care Program Using Root Cause Analysis and Common Cause Analysis. Journal for Healthcare Quality, 44(3), 169–177. https://doi.org/10.1097/JHQ.0000000000000328.
- Hirello, L., & Cameron, C. (2021). Improving Paramedicine through Social Accountability. Canadian Paramedicine, 44(3). Retrieved from https://canadianparamedicine.ca/special-editions/.
- Chan, J., Griffith, L. E., Costa, A. P., Leyenaar, M. S., & Agarwal, G. (2019). Community paramedicine: A systematic review of program descriptions and training. CJEM, 21(6), 749–761. https://doi.org/10.1017/cem.2019.14.
- PHECC. (2022). Community Paramedicine in Ireland: a framework for the specialist paramedic. Retrieved from https://www.phecit.ie/Custom/BSIDocumentSelector/Pages/DocumentViewer.aspx?id=oGsVrspmiT0dOhDFFXZvIz0q5GYO7igwzB6buxHEgeDq00klOJxrAiwRg8WilA7iQpuh0JuuyxLZ%252fgoqHj9YAdVJBi%252feIjLQQQejAdgErxHc1gOlnYuCfGcZtM%252fFZTDuGELCeo4hOpwR2WpMNptaZMMl%252biPM01lTiSTAjYn0UiWidbzfXGJzNluN5VUHbqIsRWHtJZQ5aTg%253d.
- Agarwal, G., Lee, J., McLeod, B., Mahmuda, S., Howard, M., Cockrell, K., & Angeles, R. (2019). Social factors in frequent callers: a description of isolation, poverty and quality of life in those calling emergency medical services frequently. BMC Public Health, 19(1), 684. https://doi.org/10.1186/s12889-019-6964-1.
- Agarwal, G., & Brydges, M. (2018). Effects of a community health promotion program on social factors in a vulnerable older adult population residing in social housing. BMC Geriatrics, 18(1), 95. https://doi.org/10.1186/s12877-018-0764-9.
- Agarwal, G., Keenan, A., Pirrie, M., & Marzanek-Lefebvre, F. (2022). Integrating community paramedicine with primary health care: a qualitative study of community paramedic views. CMAJ Open, 10(2). https://doi.org/10.9778/cmajo.20210179.
- Bolster, J., Batt, A. M., & Pithia, P. (2022). Emerging Concepts in the Paramedicine Literature to Inform the Revision of a Pan-Canadian Competency Framework for Paramedics: A Restricted Review. https://doi.org/10.7759/cureus.32864.
- Batt, A. M., Bank, J., Bolster, J., & Pithia, P. (2023). Canadian Paramedic Landscape Review and Standards Roadmap. Toronto: CSA Group. Retrieved from https://www.csagroup.org/article/research/canadian-paramedic-landscape-review-and-standards-roadmap/.
- First Nation Information Governance Centre. (n.d.). OCAP Principles. The First Nations Information Governance Centre. Canada. Retrieved June 11, 2023, from https://fnigc.ca/.
- Rosa, A., Dissanayake, M., Carter, D., & Sibbald, S. (2022). Community paramedicine to support palliative care. Progress in Palliative Care, 30(1), 11–15. https://doi.org/10.1080/09699260.2021.1912690.
- Gebhard, A., McLean, S., & St Denis, V. (2022). White benevolence: racism and colonial violence in the helping professions. Canada: Fernwood Publishing Company.
- O’Meara, P., Ruest, M., & Stirling, C. (2014). Community Paramedicine: Higher Education as An Enabling Factor. Australasian Journal of Paramedicine, 11, 1–9. https://doi.org/10.33151/ajp.11.2.22.
- NAEMSE. (2023). NAEMSE Consensus Statement on Diversity, Equity, Inclusion, and Belonging. Prehospital Emergency Care. Retrieved from https://www.tandfonline.com/doi/pdf/10.1080/10903127.2023.2212753?download=true.
- Alsan, M., Garrick, O., & Graziani, G. (2019). Does Diversity Matter for Health? Experimental Evidence from Oakland. American Economic Review, 109(12), 4071–4111. https://doi.org/10.1257/aer.20181446.
- Crowe, R. P., Krebs, W., Cash, R. E., Rivard, M. K., Lincoln, E. W., & Panchal, A. R. (2020). Females and Minority Racial/Ethnic Groups Remain Underrepresented in Emergency Medical Services: A Ten-Year Assessment, 2008–2017. Prehospital Emergency Care, 24(2), 180–187. https://doi.org/10.1080/10903127.2019.1634167.
- Rosenkranz, K. M., Arora, T. K., Termuhlen, P. M., Stain, S. C., Misra, S., Dent, D., & Nfonsam, V. (2021). Diversity, Equity and Inclusion in Medicine: Why It Matters and How do We Achieve It? Journal of Surgical Education, 78(4), 1058–1065. https://doi.org/10.1016/j.jsurg.2020.11.013.
- Rudman, J. S., Farcas, A., Salazar, G. A., Hoff, J., Crowe, R. P., Whitten-Chung, K., … Joiner, A. P. (2023). Diversity, Equity, and Inclusion in the United States Emergency Medical Services Workforce: A Scoping Review. Prehospital Emergency Care, 27(4), 385–397. https://doi.org/10.1080/10903127.2022.2130485.
- Metzl, J. M., & Hansen, H. (2014). Structural competency: Theorizing a new medical engagement with stigma and inequality. Social Science & Medicine, 103, 126–133. https://doi.org/10.1016/j.socscimed.2013.06.032.
- Castillo, E. G., Isom, J., DeBonis, K. L., Jordan, A., Braslow, J. T., & Rohrbaugh, R. (2020). Reconsidering Systems-Based Practice: Advancing Structural Competency, Health Equity, and Social Responsibility in Graduate Medical Education. Academic Medicine, 95(12), 1817–1822. https://doi.org/10.1097/ACM.0000000000003559.
- Coletto, D. (2023, June 8). Canadians Are Ready for Paramedics to Do More in Healthcare: Abacus Data Poll. Retrieved June 9, 2023, from https://abacusdata.ca/pac-2023/.
- Allana, A., Tavares, W., Pinto, A. D., & Kuluski, K. (2022). Designing and Governing Responsive Local Care Systems – Insights from a Scoping Review of Paramedics in Integrated Models of Care. International Journal of Integrated Care, 22(2), 5, 1–19. https://doi. org/10.5334/ijic.6418.
- Taplin, J. G., Bill, L., Blanchard, I. E., Barnabe, C. M., Holroyd, B. R., Healy, B., & McLane, P. (2023). Exploring paramedic care for First Nations in Alberta: a qualitative study. CMAJ Open, 11(6), E1135–E1147. https://doi.org/10.9778/cmajo.20230039.
- Allan, B. (2015). First Peoples, Second Class Treatment. Toronto: Li Ka Shing Knowledge Institute. Retrieved from https://www.wellesleyinstitute.com/wp-content/uploads/2015/02/Summary-First-Peoples-Second-Class-Treatment-Final.pdf.
- Lunn, T., Bolster, J., & Batt, A. (2024, February 13). Community Paramedicine Supporting Community Needs: A Scoping Review. Preprints. https://doi.org/10.20944/preprints202310.0999.v2.
Figure 1.
PRISMA diagram. Generated at https://estech.shinyapps.io/prisma_flowdiagram/.
Figure 1.
PRISMA diagram. Generated at https://estech.shinyapps.io/prisma_flowdiagram/.
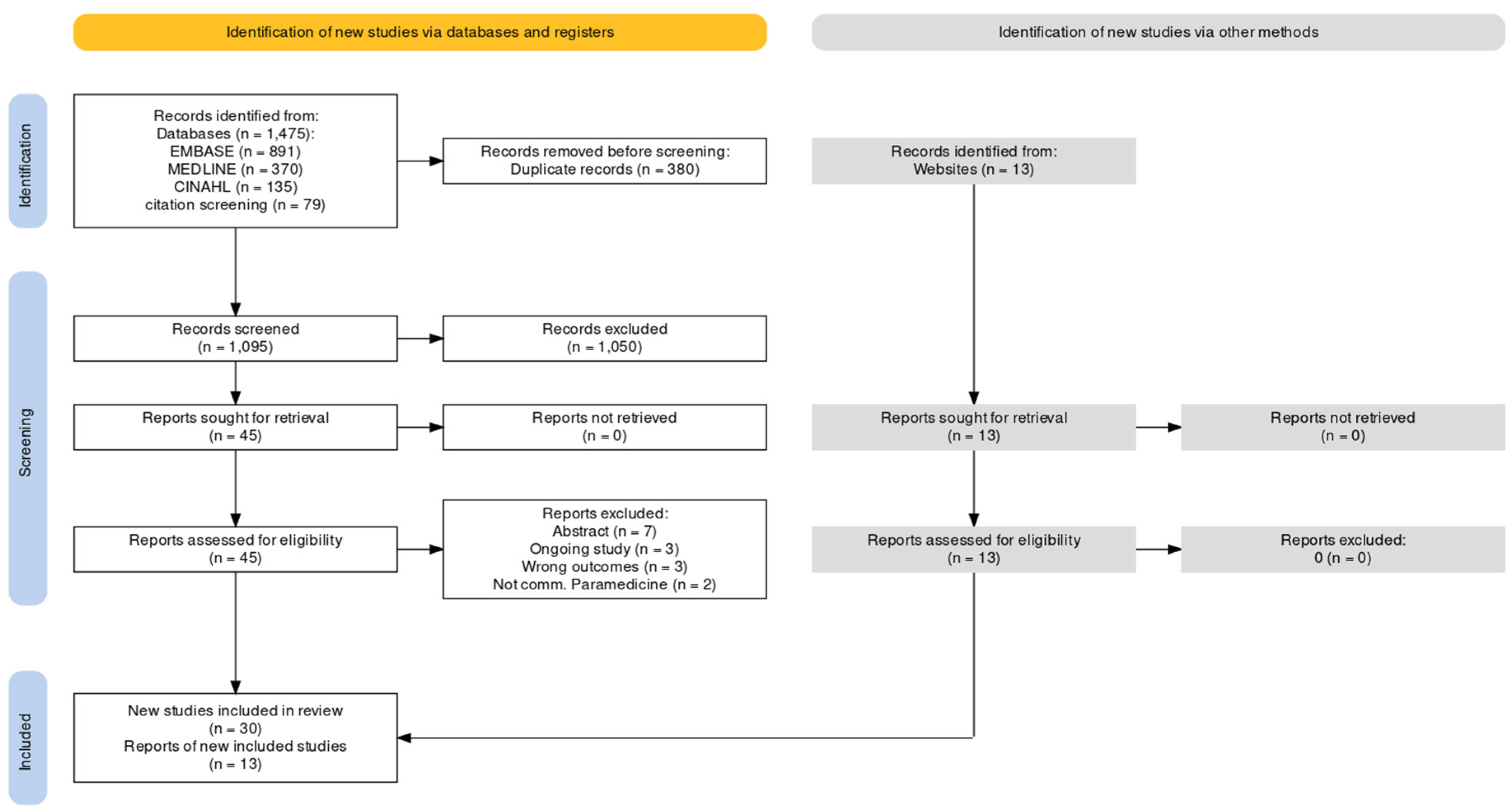
Figure 2.
Publications per year.
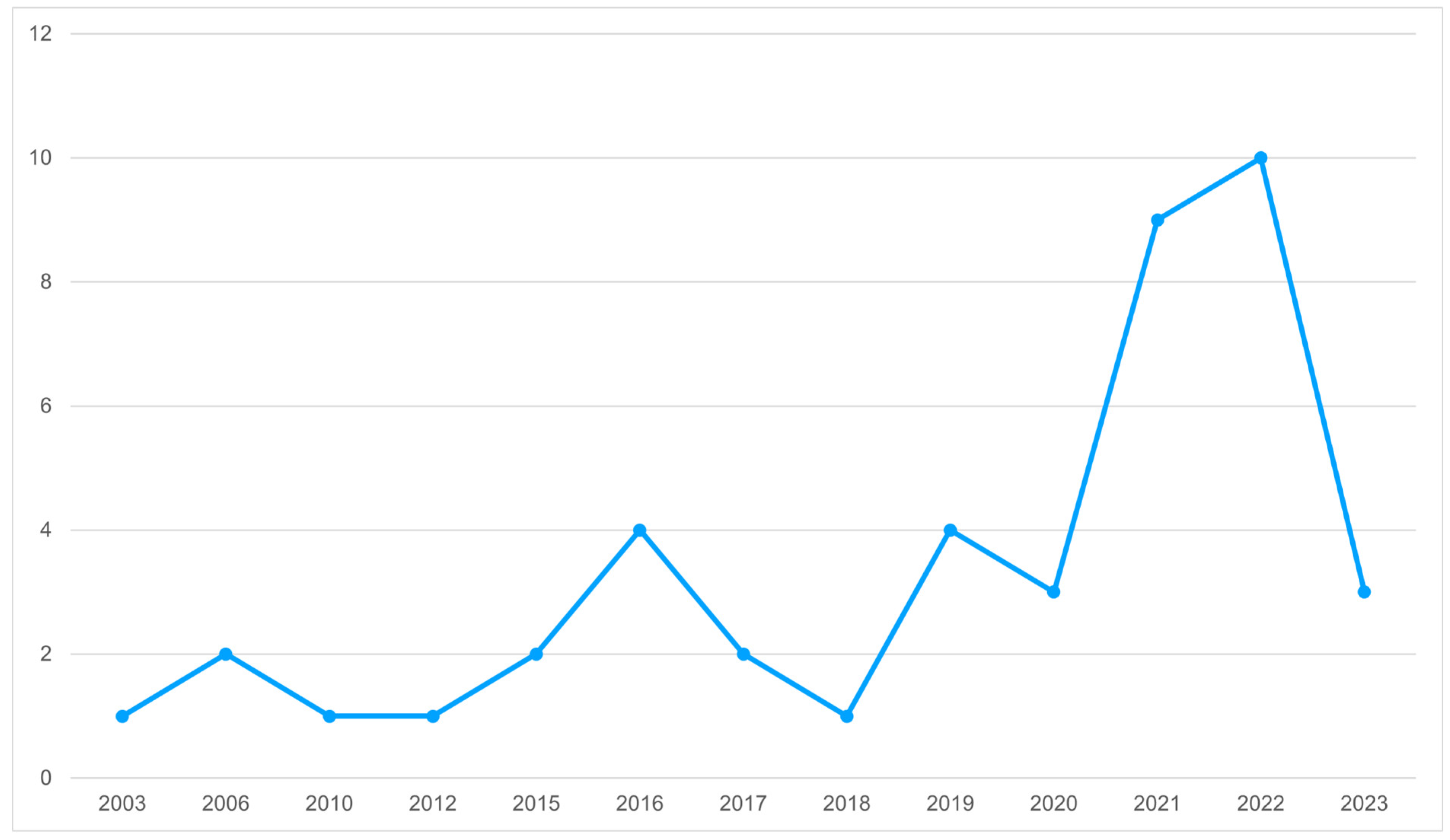
Figure 3.
Visual representation of community paramedicine supporting community needs.


Table 1.
Included studies (n=43).
| Author - Year | Location | Publication Title |
|---|---|---|
| Allana & Pinto 2021 | Canada | Paramedics Have Untapped Potential to Address Social Determinants of Health in Canada |
| Boland et al. 2022 | United States | Evaluation of an EMS-Based Community Paramedic Pilot Program to Reduce Frequency of 9-1-1 Calls among High Utilizers |
| Buitrago et al. 2022 | United States | Analysis of Readmissions in a Mobile Integrated Health Transitional Care Program Using Root Cause Analysis and Common Cause Analysis |
| Chan et al. 2019 | Canada | Community paramedicine: A systematic review of program descriptions and training |
| Cockrell et al. 2019 | Australia | Rural paramedics’ capacity for utilising a salutogenic approach to healthcare delivery: a literature review |
| Ford-Jones & Daly 2022 | Canada | Filling the gap: Mental health and psychosocial paramedicine programming in Ontario, Canada |
| Gainey et al. 2018 | United States | Utilization of Mobile Integrated Health Providers During a Flood Disaster in South Carolina (USA) |
| Georgiev et al. 2019 | United States | The Integral Role of Nurse Practitioners in Community Paramedicine |
| Hirello & Cameron 2021 | Canada | Improving Paramedicine Practice Through Social Accountability |
| Langabeer et al. 2020 | United States | A Framework for EMS Outreach for Drug Overdose Survivors: A Case Report of the Houston Emergency Opioid Engagement System |
| Leyenaar et al. 2021 | Canada | Paramedics assessing patients with complex comorbidities in community settings: results from the CARPE study |
| Logan 2022 | United States | ‘I Certainly Wasn’t as Patient-Centred’ Impacts and Potentials of Cross-Training Paramedics as Community Health Workers |
| McManamny et al. 2022 | Australia | Feasibility and acceptability of paramedic-initiated health education for rural-dwelling older people |
| Moczygemba et al. 2021 | United States | GPS Mobile Health Intervention Among People Experiencing Homelessness: Pre-Post Study |
| Mund 2016 | United States | Taking Care to the Streets |
| Naimi et al. 2023 | United States | Evaluating Social Determinants of Health in a Mobile Integrated Healthcare-Community Paramedicine Program |
| Pennel et al. 2016 | United States | Emergency Medical Service- based Care Coordination for Three Rural Communities |
| Pirrie et al. 2020 | Canada | Poverty and food insecurity of older adults living in social housing in Ontario: a cross-sectional study |
| Rahim et al. 2022 | United States | Community Paramedicine: An Innovative Model for Value-Based Care Delivery |
| Ridgeway et al. 2023 | United States | A Community Paramedic Clinic at a Day Center for Adults Experiencing Homelessness |
| Rosa et al. 2021 | Canada | Community paramedicine to support palliative care |
| Ruest 2016 | Canada | County of Renfrew Paramedic Service Paramedic Resilience Program Contribution to the Health Promotion Strategies that Address the Inequities Associated with Social Isolation of Seniors in the County of Renfrew |
| Schwab-Reese et al. 2021 | United States | “They’re very passionate about making sure that women stay healthy”: a qualitative examination of women’s experiences participating in a community paramedicine program |
| Shannon et al. 2022 | Australia | The development of community paramedicine; a restricted review |
| Sokan et al. 2022 | United States | Impact of a mobile integrated healthcare and community paramedicine program on improving medication adherence in patients with heart failure and chronic obstructive pulmonary disease after hospital discharge: A pilot study |
| Stickler et al. 2021 | United States | Community Paramedic Mobile COVID-19 Unit Serving People Experiencing Homelessness |
| Strum 2015 | Canada | Paramedics as Health Advocates: Populations of Low Social Determinants of Health |
| Swayze 2016 | United States | Chronic Disease Management for the Community Paramedic |
| Taplin et al. 2022 | Canada | Health service utilization by people experiencing homelessness and engaging with community paramedics: a pre–post study |
| Taplin et al. 2023 | Canada | Community paramedic outreach support for people experiencing homelessness |
| Newall 2015 | Canada | Who’s At My Door Project - How Organizations Find and Assist Socially Isolated Older Adults |
| Raven et al. 2006 | Australia | An exploration of expanded paramedic healthcare roles for Queensland |
| Thomas-Henkel & Schluman 2017 | United States | Screening for Social Determinants of Health in Populations with Complex Needs: Implementation Considerations |
| Olynyk 2010 | Canada | Community Referrals by EMS - an extension of service |
| Nolan et al. 2012 | Canada | Community Paramedicine in Canada |
| Misner 2003 | Canada | Community Paramedicine: A Part of an Integrated Health Care System |
| Hay et al. 2006 | Canada | Frontline Health Care in Canada: Innovations in Delivering Services to Vulnerable Populations |
| Ashton & Leyenaar 2019 | Canada | Health Services Needs in the North: a case study on CSA standard for community paramedicine |
| CSA Group 2017 | Canada | Community paramedicine: Framework for program development |
| Batt et al. 2021 | Canada | Advances in Community Paramedicine in Response to COVID-19 |
| PHECC 2020 | Ireland | The introduction of Community Paramedicine into Ireland |
| Shannon et al. 2021 | Australia | Community Paramedicine Practice Framework Scoping Exercise |
| PHECC 2022 | Ireland | Community Paramedicine in Ireland: a framework for the specialist paramedic |
Table 2.
Codes arranged by WHO Operational framework for monitoring social determinants of health equity.
Table 2.
Codes arranged by WHO Operational framework for monitoring social determinants of health equity.
| Framework category | Economic security and equality | Education | Physical environment | Social and community context | Health behaviours | Health care |
|---|---|---|---|---|---|---|
| Included codes |
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



