
Submitted:
13 October 2023
Posted:
17 October 2023
You are already at the latest version
Abstract
Introduction: Dengue is a mosquito transmitted arboviral infection. In dengue fever spontaneous bleeding in different parts of body occurs; but spontaneous bleeding into rectus muscle leading to haematoma formation is rare.
Case Presentation: A 72-year-old hypertensive female presented with high grade intermittent fever with chills and rigors for last four days. She was diagnosed to have dengue fever (NS1Ag -Reactive) on the day before admission. At admission, on examination she was found to be have dehydration. Immediately she was put on IV fluids, antiemetics and other supportive therapy. At admission she had low platelets, low haemoglobin, total leucocyte counts, with raised liver enzymes. On day 3 of illness, she had significant drop of haematocrit with low blood pressure and subsequently she managed with packed red blood cell (PRBC) transfusion. But on 9th day of illness, she has severe right iliac fossa pain mimicking acute appendicitis. CECT of abdomen showed soft tissue lesion in right lower abdomen (Inflammatory/ hematoma along rectus sheath) which was managed conservatively as per surgical opinion. 10 days past discharge she had no pain in right iliac fossa and size of hematoma was significantly reduced.
Discussion: In dengue fever, hematoma can be formed any vulnerable part in the but there are only a few cases reported to be having rectus sheath hematoma. Rectus sheath hematoma (RSH) has been mistaken for many acute abdominal diseases like- acute appendicitis. Our case mimicked acute appendicitis and managed conservatively with IV fluids, analgesics, Blood transfusion as it fits into RSH type II.
Conclusion: It is important to be vigilant in the patients who presents with abdominal pain in severe dengue cases. Prompt imaging in relevant areas could make the diagnosis and father treatment possible.
Keywords:
Dengue fever
; Rectus sheath hematoma
; surgical emergency
; acute appendicitis
Background
Dengue is a mosquito transmitted arboviral infection, which has become a disease of public health concern globally. It usually presents as fever with myalgia, body ache may often be complicated by bleeding, shock, organ involvement. Majority of patients present with fever, flu like symptoms, constitutional symptoms and some forms of plasma leakage. However, reports of dengue cases with organ involvement in the form of hepatitis, kidney injury, myocarditis, encephalitis, pancreatitis, acute respiratory distress syndrome (ARDS) are on the rise and this is called expanded dengue syndrome (EDS).(1) There has been reports of spontaneous bleeding in different parts of body but spontaneous bleeding into rectus muscle leading to haematoma formation is rare.(2) We report an interesting case of spontaneous rectus sheath haematoma leading to severe right iliac fossa pain mimicking acute appendicitis which was formed during the recovery phase of dengue haemorrhagic fever (DHF).
Case presentation
A 72-year-old hypertensive female resident of Kolkata, West Bengal, India, presented with high grade intermittent fever with chills and rigors for last four days. She also had severe muscle pain, body ache, nausea and vomiting associated with fever. She was unable to eat or drink due to the illness. She did not have any cough, shortness of breath, urinary symptoms, altered bowel habits. She was on telmisartan 40 mg and hydrochlorothiazide 12.5 mg for control of hypertension. She was diagnosed to have dengue fever (NS1Ag -Reactive) on the day before admission. At admission, on examination she was found to be have dehydration, mild pallor, BP- 110/70 mm of Hg, Pulse- 122/min (regular), temperature- 102.6⁰F, SpO2- 98% @ room air, alert, co-operative, chest- bilateral vesicular breath sounds, CVS- S1, S2 audible, Tender 2 cm hepatomegaly below right costal margin, no free fluid. Immediately she was put on IV fluids (volume calculated according to Holliday-Segar formula), antiemetics and other supportive therapy. At admission she had low platelets, low haemoglobin, total leucocyte counts, with raised liver enzymes. Serial blood parameters are mentioned in Table 1.
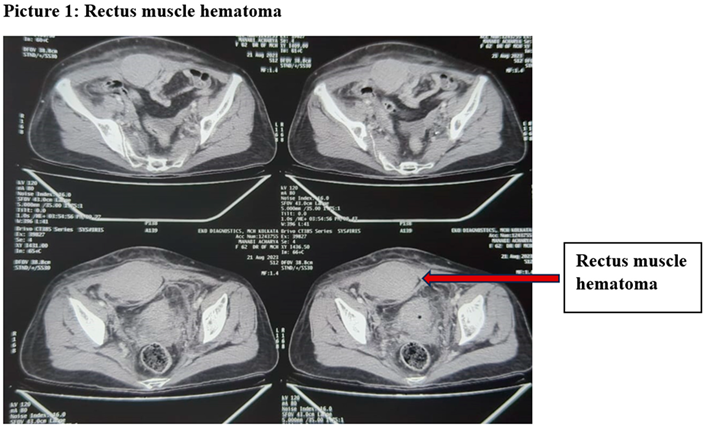
On day 3 of illness, she had significant drop of haematocrit with low blood pressure (90/60 mm of Hg). So, she was immediately transfused packed red blood cell (PRBC). Her Blood culture, urine cultures were showing no growth. Malaria was not found in peripheral blood smear and on Day 7 of illness her Dengue IgM was reactive. After the initial hypotension and drop in haematocrit she continued to have low haemoglobin (7~8 gm/dl) with normal blood pressure (without antihypertensives). Initially she complained of severe nausea and vomiting due to raised liver enzymes. But on 9th day of illness, she has severe right iliac fossa pain mimicking acute appendicitis with continued nausea. There was no history of trauma during this period also. At that time her stool occult blood test was strongly positive. Immediately surgical opinion was sought for this new onset abdominal pian and as acute appendicitis was the primary differential diagnosis, she was again started on IV fluids, Ceftriaxone, IV metronidazole and other supportive therapy. CECT of abdomen showed soft tissue lesion in right lower abdomen (? Inflammatory/? hematoma along rectus sheath). [Picture 1].
After that antibiotics were discontinued in view of normalised total leucocyte and absence of fever. After 2~3 days of conservative management she was stable with mild tender right iliac fossa mass. On surgical opinion she was discharged with a device to do a follow up ultrasonography. 10 days past discharge she had no pain in right iliac fossa and size of hematoma was significantly reduced (from 11 cm X 3 cm to 4 cm X 2 cm) on sonography. On Follow up after 15 days she had no right iliac fossa pain or mass felt. On ultrasonography also there was very minimal hematoma.
Discussion
Rectus sheath hematoma (RSH) usually presents as bleeding within the rectus abdominis muscle sheath. This is commonly be caused by ruptured epigastric vessels or a tear of the rectus muscle.(3) Usual known risk factors of spontaneous RSH are female gender, pregnancy, obesity, anticoagulant drugs, abdominal straining, severe vomiting, and intractable cough. (4) Complications in patients with DHF in the form of bleeding usually a result from the combination of thrombocytopenia, increased vascular fragility, increased fibrinolysis, pro-coagulation and anticoagulation factors imbalance.(5) In critical stage of DHF there is defervescence of fever and higher degree of plasma leakage and low platelet count, which in some cases may lead to circulatory failure or bleeding complications.(6) We did an extensive literature review of spontaneous hematoma in dengue fever which is shown in Table 2.
We can see from this literature review that maximum cases were reported from South East Asia as dengue fever mostly endemic here. There were slightly more males than females who had this spontaneous hematoma in different parts of the body in dengue fever. Age group was more in younger population. Majority had no co-morbidities. Hematoma can be formed any vulnerable part in the but there are quite a few cases reported to be having rectus sheath hematoma. Also, RSH did not need any surgical intervention; though splenic hematoma mostly managed with splenectomy. There were few mortalities when patient presented with cerebral or splenic hematomas.
RSH can be divided by the severity of haemorrhage as seen on CT scan. Type-I RSH are one sided hematoma contained only within the muscle. Type-II RSH is bilateral hematomas/ hematomas not contained within the muscle sheath. Type-III RSH is called when blood enters the pre-vesicular space or peritoneum. Usually type I & II RSH can be manged conservatively but type III usually needs surgery. Treatment of spontaneous RSH is generally conservative including resuscitation, correction of coagulopathy, analgesia and treatment of the underlying condition.(30) Interventional radiological intervention and embolization is preferred in cases of continued bleeding with surgery being considered as the last option.(31) RSH has been mistaken for many acute abdominal diseases like- acute appendicitis, dissecting abdominal aneurysm, cholecystitis and biliary colic, cholelithiasis, diverticular disease, peptic ulcer disease, acute gastritis, obstructed intestinal hernias. Our case mimicked acute appendicitis and managed conservatively with IV fluids, analgesics, Blood transfusion as it fits into RSH type II.
In conclusion, it is important to be vigilant in the patients who presents with abdominal pain or any neuro-deficit during convalescent phase of dengue fever. Because it could be a presenting symptom of spontaneous hematoma in different parts of the body. Prompt imaging in relevant areas could make the diagnosis and father treatment possible.
Funding
This case report did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kalayanarooj, S. Clinical Manifestations and Management of Dengue/DHF/DSS. TropMedHealth. 2011, 39 (4SUPPLEMENT), S83–S87. [Google Scholar] [CrossRef]
- de Azeredo, E.L.; Monteiro, R.Q.; de-Oliveira Pinto, L.M. Thrombocytopenia in Dengue: Interrelationship between Virus and the Imbalance between Coagulation and Fibrinolysis and Inflammatory Mediators. Yeh TM, editor. Mediators of Inflammation. 2015, 2015, 313842. [Google Scholar] [CrossRef]
- Aktürk, O.M.; Kayılıoğlu, S.I.; Aydoğan, İ.; Dinç, T.; Yildiz, B.; Cete, M.; et al. Spontaneous Rectus Sheath Hematoma: An Overview of 4-Year Single Center Experience. Indian J Surg. 2015, 77, 1219–1221. [Google Scholar] [CrossRef] [PubMed]
- Eckhoff, K.; Wedel, T.; Both, M.; Bas, K.; Maass, N.; Alkatout, I. Spontaneous rectus sheath hematoma in pregnancy and a systematic anatomical workup of rectus sheath hematoma: A case report. J Med Case Reports. 2016, 10, 292. [Google Scholar] [CrossRef]
- Wills, B.A.; Oragui, E.E.; Stephens, A.C.; Daramola, O.A.; Dung, N.M.; Loan, H.T.; et al. Coagulation Abnormalities in Dengue Hemorrhagic Fever: Serial Investigations in 167 Vietnamese Children with Dengue Shock Syndrome. CLIN INFECT DIS. 2002, 35, 277–285. [Google Scholar] [CrossRef]
- Martina, B.E.E.; Koraka, P. , Osterhaus ADME. Dengue Virus Pathogenesis: An Integrated View. Clin Microbiol Rev. 2009, 22, 564–581. [Google Scholar] [PubMed]
- Pahari, S.; Basukala, S.; Kunwar, P.; Thapa, K.; Khand, Y.; Thapa, O. Spontaneous splenic hematoma secondary to dengue infection: A rare case report. Annals of Medicine & Surgery. 2023, 85, 1030–1033. [Google Scholar]
- Kaushik, R.M.; Kumar, R.; Kaushik, M.; Saini, M.; Kaushik, R. Spontaneous spinal intradural hemorrhage in dengue fever: A case report. J Med Case Reports. 2022, 16, 213. [Google Scholar] [CrossRef] [PubMed]
- Corré, J.; Vally, S.; Boiron, P.; Bouillaud, Y.; Travers, J. Spontaneous coronary hematoma concomitant with myocarditis: The first report of double cardiac complication of dengue. ESC Heart Failure. 2023, 10, 1445–1448. [Google Scholar] [CrossRef]
- Siahaan, A.M.P.; Tandean, S.; Saragih, E.B.; Nainggolan, B.W.M. Spontaneous acute subdural hematoma in dengue fever: Case report and review of the literature. International Journal of Surgery Case Reports. 2022, 98, 107512. [Google Scholar] [CrossRef]
- Chang, C.Y. A Fatal Case of Dengue-Associated Hemophagocytic Lymphohistiocytosis and Retroperitoneal Hematoma in a Patient With Autoimmune Hemolytic Anemia. Cureus [Internet]. 2021 May 13. Available online: https://www.cureus.com/articles/58589-a-fatal-case-of-dengue-associated-hemophagocytic-lymphohistiocytosis-and-retroperitoneal-hematoma-in-a-patient-with-autoimmune-hemolytic-anemia (accessed on 9 September 2023).
- Ungthammakhun, C.; Chueansuwan, W.; Changpradub, D. Dengue Hemorrhagic Fever Complicated with Spontaneous Rupture of the Spleen among Patients with Thalassemia and G6PD Deficiency: A Case Report. Arch Clin Med Case Rep [Internet]. 2021, 5. Available online: https://www.fortunejournals.com/articles/dengue-hemorrhagic-fever-complicated-with-spontaneous-rupture-of-the-spleen-among-patients-with-thalassemia-and-g6pd-deficiency-a-.html (accessed on 9 September 2023).
- Mushtaque, R.S.; Ahmad, S.M.; Mushtaque, R.; Baloch, S. A Curious Case of Dengue Fever: A Case Report of Unorthodox Manifestations. Case Reports in Medicine. 2020, 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Matthias, A.T.; Apsara, S.; Epa, A. A case report of dengue haemorrhagic fever complicated with psoas haematoma requiring blood transfusion. BMC Infect Dis. 2019, 19, 385. [Google Scholar] [CrossRef] [PubMed]
- Baruah, S.; Dubey, S.; Ghavghave, U.; Jha, A.N. Dengue Fever Presenting with Cervicodorsal Acute Spinal Spontaneous Subdural Hematoma—Case Report and Review of Literature. World Neurosurgery. 2019, 122, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Singh, R.; Ghosh, S.; Chawla, A. Unusual surgical emergency in a patient of dengue haemorrhagic fever: Spontaneous rectus sheath haematoma leading to abdominal compartment syndrome. BMJ Case Reports 2018, bcr-2018-225936. [Google Scholar] [CrossRef] [PubMed]
- Tamilarasan, V.; Chandra, M.R.K.R.; Mohan, B.V.M.; Kadambi, M. Vocal cord hematoma: An unusual complication of dengue fever. Egypt J Intern Med. 2018, 30, 168–169. [Google Scholar] [CrossRef]
- Anam, A.M.; Rabbani, R.; Shumy, F. Spontaneous calf haematoma in severe dengue. BMJ Case Reports. 2018, bcr-2017-222932. [Google Scholar] [CrossRef] [PubMed]
- Nelwan, E.J.; Angelina, F.; Adiwinata, R.; Matondang, S.; Andriono, P. Spontaneous rectus sheath hematomas in dengue hemorrhagic fever: A case report. IDCases. 2017, 10, 35–37. [Google Scholar] [CrossRef]
- Jayasinghe, N.S.; Thalagala, E.; Wattegama, M.; Thirumavalavan, K. Dengue fever with diffuse cerebral hemorrhages, subdural hematoma and cranial diabetes insipidus. BMC Res Notes. 2016, 9, 265. [Google Scholar] [CrossRef]
- Singh, J. Retroperitoneal Haematoma in a Patient with Dengue Haemorrhagic Fever: A Rare Case Report. JCDR [Internet]. 2016. Available online: http://jcdr.net/article_fulltext.asp?issn=0973-709x&year=2016&volume=10&issue=11&page=OD01&issn=0973-709x&id=8771 (accessed on 9 September 2023).
- Sharma, A.; Bhatia, S.; Singh, R.; Malik, G. Dengue fever with rectus sheath hematoma: A case report. J Family Med Prim Care. 2014, 3, 159. [Google Scholar] [CrossRef]
- Waseem, T.; Latif, H.; Shabbir, B. An unusual cause of acute abdominal pain in dengue fever. The American Journal of Emergency Medicine. 2014, 32, 819–e3. [Google Scholar] [CrossRef]
- Mehtani, A.; Jha, A.; Kataria, H.; Jangira, V.; Shukla, A. Acute Compressive Ulnar Neuropathy in a Patient of Dengue Fever: An Unusual Presentation. Journal of Orthopaedic Case Reports. 2013, 3, 25–28. [Google Scholar] [CrossRef]
- Sarkar, J.; Mohan, C.; Misra, D.; Goel, A. Lingual hematoma causing upper airway obstruction: An unusual manifestation of dengue fever. Asian Pacific Journal of Tropical Medicine. 2011, 4, 412–413. [Google Scholar] [CrossRef] [PubMed]
- Mittal, M.; Jain, N. Subdural haematoma and axonal polyneuropathy complicating dengue fever. Case Reports. 2011, 2011(jun16 1), bcr1220103672–bcr1220103672. [Google Scholar] [CrossRef]
- Tong, P.; Yeoh, C.; Yong, E. Abdominal mass and a forgotten haemorrhagic fever. The Lancet. 2010, 376, 140. [Google Scholar] [CrossRef] [PubMed]
- Seravali, M.R.M.; Santos, A.H.G.D.; Costa, C.E.F.; Rangel, D.T.A.; Valentim, L.F.; Gonçalves, R.M. Spontaneous splenic rupture due to dengue fever: Report of two cases. Braz J Infect Dis. 2008, 12, 538–540. [Google Scholar] [CrossRef] [PubMed]
- Miranda, L.E.C.; Miranda, S.J.C.; Rolland, M. Case report: Spontaneous rupture of the spleen due to dengue fever. Braz J Infect Dis [Internet]. 2003, 7. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-86702003000600011&lng=en&nrm=iso&tlng=en (accessed on 9 September 2023).
- Liao, E.D.; Puckett, Y. A Proposed Algorithm on the Modern Management of Rectus Sheath Hematoma: A Literature Review. Cureus [Internet]. 2021. Available online: https://www.cureus.com/articles/75702-a-proposed-algorithm-on-the-modern-management-of-rectus-sheath-hematoma-a-literature-review (accessed on 9 September 2023).
- Won, D.Y.; Kim, S.D.; Park, S.C.; Moon, I.S.; Kim, J.I. Abdominal Compartment Syndrome Due to Spontaneous Retroperitoneal Hemorrhage in a Patient Undergoing Anticoagulation. Yonsei Med J. 2011, 52, 358. [Google Scholar] [CrossRef]

Table 1.
Treands of blood parameters day-wise with associated clinical events.
| Day of illness | Sample | Hb (gm/dl) | Hct | TLC (/cmm) | Platelet count (/cmm) | SGPT (IU/l) | SGOT (IU/l) |
Phase /clinical events |
|---|---|---|---|---|---|---|---|---|
| Day 4 | Admission | 8.6 | 21.5 | 2,300 | 80,000 | 61 | 158 | Febrile Phase |
| Evening | 8.7 | 22.8 | 2,200 | 70,000 | - | - | ||
| Day 5 | Morning | 9.1 | 26.9 | 1,400 | 60,000 | 98 | 232 | Critical Phase |
| Evening | 9.1 | 25.0 | 1,200 | 69,000 | - | - | ||
| Day 6 | Morning | 9.4 | 28.4 | 1,700 | 30,000 | 176 | 548 | Critical Phase; Severe Nausea and Vomiting; 1 unit of PRBC given |
| Evening | 7.0 | 21.4 | 1,600 | 22,000 | - | - | ||
| Day 7 | Morning | 8.2 | 23.5 | 2,500 | 30,000 | 190 | 534 | Critical Phase; Nausea, vomiting present |
| Evening | 7.8 | 22.4 | 2,700 | 32,000 | - | - | ||
| Day 8 | Morning | 6.8 | 19.2 | 2,800 | 33,000 | 186 | 504 | Critical Phase ended; Nausea, vomiting present; 1 unit of PRBC given; Stool for OBT- strongly positive |
| Evening | 6.7 | 18.7 | 3,300 | 35,000 | - | - | ||
| Day 9 | Morning | 7.8 | 22.7 | 4,300 | 40,000 | 178 | 456 | Nausea, vomiting present; Severe RIF pain; 1 unit of PRBC given |
| Evening | 7.6 | 23.9 | 4,200 | 45,000 | - | - | ||
| Day 10 | Morning | 8.2 | 24.6 | 4,300 | 55,000 | 170 | 345 | Nausea, vomiting subsided, RIF pain continued |
| Evening | 8.0 | 25.8 | 4,700 | 76,000 | - | - | ||
| Day 11 | Morning | 7.6 | 23.7 | 5,800 | 90,000 | 134 | 235 | RIF pain continued, RIF tender mass felt; antibiotics and IV fluids started; 1 unit of PRBC given |
| Evening | 7.2 | 2.6 | 5,700 | 1,12,000 | - | - | ||
| Day 12 | Morning | 8.6 | 26.7 | 6,300 | 1,25,000 | 87 | 176 | RIF tender mass felt; 1 unit of PRBC given |
| Evening | 8.9 | 27.9 | 7,600 | 1,56,000 | - | - | ||
| Day 13 | Morning | 8.5 | 27.0 | 8,900 | 2,12,000 | 67 | 112 | Imaging showed right lower abdominal rectus muscle hematoma, 1 unit of PRBC given; antibiotics discontinued |
| Day 14 | Morning | 9.2 | 28.3 | 8,700 | 2,54,000 | 56 | 78 | Mild RIF tenderness; discharged |
Table 2.
Literature review of Spontaneous Hematoma in Dengue fever.
| Location | Sex | Age | Co-morbidities/ drugs | Presentation | Diagnosis | Treatment | Outcome | |
| Our case 2023 |
India | F | 72 | HTN | RIF pain; Recurrent Vomiting (dengue hepatitis) | RSH (CT scan) | Conservative | Survival |
| Pahari et al. 2023(7) | Nepal | M | 54 | Nil | Left upper abdominal pain | Splenic sub-capsular hematoma (CT scan) | Conservative | Death |
| Kaushik et al. 2022(8) | India | F | 48 | Nil | Acute onset paraplegia with bladder and bowel dysfunction and anaesthesia below the umbilicus | Compression of spinal cord due to intradural hematoma at the D7–D8 level (MRI) | Emergency D7–D8 laminectomy with excision of the clot and Dural repair |
Survival with residual neuro-deficit |
| Corré et al. 2022(9) | France | M | 33 | Nil | Chest pain | Coronary hematoma (angiography): Acute myocarditis (CMRI) | Conservative with dual antiplatelets | Survival |
| Siahann et al. 2022(10) | Indonesia | M | 65 | Nil | Altered consciousness and focal neuro- deficits | Subdural hematoma (CT scan) | Craniotomy | Survival |
| Chang et al. 2021(11) | Malaysia | F | 59 | DM | Hypotensive shock | Retroperitoneal hematoma (Ultrasonography) Associated with HLH and AIHA |
Conservative | Death |
| Ungthammakhun et al. 2021(12) | Thailand | M | 22 | Nil | Left upper abdominal pain | Splenomegaly with active contrast extravasation at spleen surrounded with hematoma, and generalized hemoperitoneum (CT scan) |
Splenectomy | Survival |
| Mushtaque et al. 2020(13) | Pakistan | M | 32 | Nil | Decreased power in bilateral lower limbs and pain in right leg |
Bilateral iliopsoas hematoma (CT scan) | Conservative | Survival |
| Matthias etal. 2019(14) | Sri Lanka | M | 28 | Nil | Left groin and inguinal region | Left psoas haematoma (Ultrasonography) |
Conservative | Survival |
| Baruah et al. 2018(15) | India | F | Not Mentioned | HTN, Bronchial Asthma, OSA | Acute quadriparesis with urinary incontinence | Cervicodorsal anterior epidural hematoma (MRI) | Surgical evacuation (durotomy) | Death |
| Ghosh et al. 2018(16) | India | F | 74 | HTN | Recurrent Vomiting | RSH (CT scan) | Surgical evacuation for Abdominal Compartment Syndrome | Survival |
| Tamilasran et al. 2018(17) | India | M | 36 | Nil | Sore throat | Hematoma involving both the vocal cords and immediate sub-glottis (Video Laryngoscopy) |
Conservative | Survival |
| Anam et al. 2017(18) | Bangladesh | M | 45 | Nil | Left calf swelling | Calf muscle hematoma (Ultrasonography) | Surgical evacuation via fasciotomy | Survival |
| Nelwan et al. 2017(19) | Indonesia | F | 58 | Nil | lower abdominal pain | RSH (Cullen’s sign + CT scan) | Conservative | Survival |
| Jayasinghe et al. 2016(20) | Sri Lanka | F | 24 | Nil | Headache, loss of consciousness, seizure | Intracranial haemorrhages and sub arachnoid haemorrhages (CT scan) |
Conservative as platelet count was 40,000/cmm | Death |
| Singh et al. 2016(21) | India | M | 30 | Nil | RIF pain | Intra-parenchymal haematoma in the liver with extension to right peritoneum and right psoas muscle haematoma |
Conservative | Survival |
| Sharma et al. 2014(22) | India | M | 40 | Nil | Severe pain in paraumbilical region, extending to right hypochondrium and lumbar regions |
RSH (CT scan) | Conservative | Survival |
| Waseem et al. 2014(23) | Pakistan | M | 55 | HTN, DM, Aspirin | Pain in right upper quadrant of abdomen | RSH (CT scan) | Surgical Evacuation | Survival |
| Mehtani et al. 2013 (24) | India | M | 36 | Nil | Right forearm pain with tingling and numbness along the distribution of ulnar nerve | Hematoma compressing ulnar neurovascular bundle (MRI) | Surgical evacuation | Survival with residual neuro-deficit |
| Sarkar et al. 2011(25) | India | M | Young | Nil | Inability to protrude his tongue and was unable to speak | Tongue- enlarged and swollen (Clinical) |
Conservative | Survival |
| Mittal et al. 2011(26) | India | F | 27 | Nil | Recurrent seizure | Bilateral subdural haematoma (MRI) | Conservative | Survival with residual neuro-deficit |
| Tong et al. 2010(27) | Republic of Singapore | F | 37 | Adenomyosis, OCP | RIF pain | RSH (CT scan), DVT (US doppler) | Conservative; Anti-coagulation after stabilisation | Survival |
| Seravali et al. 2008(28) | Brazil | M | 27 | Nil | Shock | Spleen congested with rupture of middle third and peri-splenic hematoma (Intra-operative) |
Splenectomy | Survival |
| Seravali et al. 2008(28) | Brazil | M | 20 | Nil | Left upper abdomen pain | Splenic hematoma (Ultrasonography) | Splenectomy | Survival |
| Miranda et al. 2003(29) | Brazil | M | 27 | Nil | Diffuse abdominal pain | Splenic hematoma (CT scan) | Splenectomy | Survival |
HTN- Hypertension; RIF- Right iliac fossa; RSH- Rectus sheath hematoma; CT scan- Computed tomography scan; MRI- Magnetic resonance imaging; CMRI- Cardiac Magnetic resonance imaging; HLH- Hemophagocytic Lymph histiocytosis; AIHA- Auto-immune haemolytic anaemia: DVT- Deep vein thrombosis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



