
Submitted:
14 October 2023
Posted:
17 October 2023
You are already at the latest version
Abstract
Dual antiplatelet therapy (DAPT), comprising aspirin and a P2Y12 receptor inhibitor, is the cornerstone of post-percutaneous coronary intervention treatment to prevent stent thrombosis and reduce the risk of adverse cardiovascular events. The selection of an optimal DAPT regimen, considering the interplay of various antiplatelet agents, patient profiles, and procedural characteristics, remains an evolving challenge. Traditionally, a standard duration of 12 months has been recommended for DAPT in most patients. While contemporary guidelines provide general frameworks, DAPT modulation with longer or shorter treatment courses followed by aspirin or P2Y12 inhibitor monotherapy are evolving towards an individualized strategy to optimize the balance between efficacy and safety. This review comprehensively examines the current landscape of DAPT strategies after coronary stenting, with a focus on emerging evidence for treatment individualization.
Keywords:
dual antiplatelet therapy
; Percutaneous coronary intervention
; acute coronary syndrome
; bleeding risk
; tailored therapy
1. Introduction to the Rationale of Antiplatelet Therapy after Coronary Stenting
Percutaneous coronary intervention (PCI), especially with the availability of new drug-eluting stents (DES) technologies and new devices and drugs, has revolutionized the management of coronary artery disease (CAD) by providing effective revascularization and improving clinical outcomes [1,2,3,4,5,6]. Despite these achievements, CAD still represents the leading cause of mortality in developed countries [7,8] and the outcome is still unsatisfactory in high-risk patients [9,10,11]. Therefore, large attention has been paid so far to the identification of new risk factors [12,13,14,15] and implementation of primary and secondary prevention [16,17,18,19]. Antiplatelet therapies represent a key stone in secondary cardiovascular prevention. In fact, dual antiplatelet therapy (DAPT), comprising aspirin and a P2Y12 receptor inhibitor, is a cornerstone therapy in both elective and Acute Coronary syndromes (ACS) patients treated by PCI and stenting, to prevent both stent thrombosis (ST) and ischemic events of other vascular segments [16], as it is well known that platelet adhesion, activation, and aggregation play a pivotal role in vascular thrombosis [20].
Aspirin is still widely considered the “primary agent” for the treatment of acute or chronic coronary syndrome to which additional antiplatelet drugs are added when more intense antithrombotic effect is needed (Figure 1). Its antithrombotic action is based on the acetylation of the platelet’s cyclooxygenase (COX) [21], inhibiting the thromboxane A2 pathway. The interaction of ADP with the platelet P2Y12 receptor, is another essential part of the platelet’s activation process, causing enhanced platelet’s degranulation and thromboxane production, and prolonged platelets aggregation [22]. The inhibition of the P2Y12 pathway, prevents the binding of ADP to the receptor, attenuating platelets aggregation. In patients with acute coronary syndrome (ACS) or undergoing PCI for chronic coronary syndrome (CCS), DAPT has consistently shown to reduce recurrent major adverse cardiovascular events (MACE) compared to aspirin monotherapy [23,24].
However, the anti-thrombotic benefits of DAPT are counterbalanced by an increase in bleeding, which is directly related to the duration and intensity of the antiplatelet regimen, and significantly impact mortality with similar time-dependency of myocardial infarction [25]. Hence, determining the optimal duration and selection of antiplatelet agents for DAPT is of upmost importance to optimize clinical outcomes and remains a subject of ongoing investigation and clinical debate [26,27]. Recent studies have challenged the traditional notion of a one-size-fits-all approach, suggesting that individualized treatment strategies based on patient-specific factors and procedural characteristics may be necessary to select treatment [28]. Nowadays, the number of options to personalize DAPT treatment is vast, and are increasingly endorsed by international guidelines, leveraging on the modulation of DAPT duration (i.e., short vs. longer treatment courses) [29], DAPT components in term of P2Y12 inhibitor type (i.e., potent vs. non-potent P2Y12 inhibitor), and dosage [30]. The aim of this review aim is to summarize the evidence that, throughout the years, established the current options for DAPT modulation after PCI.
2. Dual Antiplatelet Therapy and Choice of the P2Y12 Inhibitor
The CURE trial [16] established clopidogrel as the standard of care for DAPT after ACS or PCI. This was a randomized, double-blind, placebo-controlled trial testing the safety and efficacy of clopidogrel (loading dose of 300 mg, followed by 75 mg per day) in patients with ACS. The study primary outcome, a composite of death from cardiovascular causes, nonfatal myocardial infarction, or stroke, was reduced by 20% in the clopidogrel group (9.6% vs 11.4%). This was mainly driven by a 23% reduction of recurrent myocardial infarction (MI). Compared to placebo, DAPT with clopidogrel increased the risk of major bleedings (requiring the transfusion of 2 or more units of blood) by 38% (gastrointestinal and at the sites of the arterial puncture), and need for transfusion by 30%, with no excess of fatal or life-threatening bleeding [31].
Additional large trials conducted in the setting of ACS have shown the superiority of both prasugrel (TRITON-TIMI 38 trial, among those undergoing invasive treatment) [32] and ticagrelor (PLATO trial) [33] as compared to clopidogrel in ischemic endpoints, despite higher risk of bleedings (Figure 2).
Currently approved oral P2Y12 inhibitors could be classified based on the pharmacological class into thienopyridines (clopidogrel and prasugrel) and non-thienopyridines (ticagrelor). A more clinical classification is based on the potency and consistency of platelet inhibition in potent (prasugrel, ticagrelor) and non-potent (clopidogrel) agents [34].
In brief, the current choice of P2Y12 inhibitor for DAPT is mainly based on the clinical presentation: current guidelines recommend using a potent P2Y12 inhibitors (prasugrel or ticagrelor) on top of aspirin in patients undergoing PCI for ACS if there aren’t any contraindications or the patient has not a high bleeding risk [35]. As the efficacy of clopidogrel is hampered by the slow and variable transformation of the prodrug to active metabolites, the highest thrombotic risk associated with an acute presentation require a more intense antithrombotic treatment [36,37]. In turn, in patient with chronic coronary syndrome (CCS), clopidogrel is the P2Y12 inhibitor of choice, unless additional high ischemic risk characteristics are present.
3. Optimal DAPT Duration
3.1. 12Months DAPT
In the last ten years there has been a great number of studies exploring optimal duration of DAPT followed by a single antiplatelet agent. Initially the recommended duration for DAPT after coronary stenting was 1-6 months [38]. This treatment window was non-randomly tested in the studies that compared drug-eluting stents (DES) with bare metal stents (BMS). The mean follow-up time for clopidogrel based DAPT in the PCI CURE trial was 8 months [16]. The evidence of an increased risk of late and very late ST after first-generation DES lead to a more cautious approach with extension of DAPT well beyond 12 months after implantation [39,40,41,42]. Based on the available evidence, consensus-based guidelines recommended a minimum of 12 months of DAPT in this setting [43]. However, the introduction of safer stent platforms [44,45] progressively showed that DAPT duration could be safely shortened [46]. The main reason to strike an optimal duration of DAPT is to reasonably balance the risk of ischemic and bleeding events, both impacting prognosis, and both opposingly affected by the duration of antithrombotic therapy. In this context, clinical trials comparing 3 or 6 months of DAPT to 12 months found no difference in ischemic events, with improved safety after short-term DAPT [47].
3.2. Prolonged (>12 months) DAPT
DESs reduced the rate of restenosis as compared with bare-metal stents, however there was an initial concern that first-generation DESs may be associated with an additional risk of late and very-late ST [48]. In addition, beyond stent-related events, ischemic events unrelated to the treated plaque may also occur, which support the potential for prolonged antiplatelet therapy as a secondary prevention strategy [49,50].
Among the others, patients with MI have heightened platelet activation and aggregation compared with patients with CCS, leading to a higher predisposition to atherothrombosis [51,52,53], and it may persist for years afterwards [54,55,56]. Hence, these patients may benefit more intensive antiplatelet therapies following PCI.
The DAPT study was a multicenter randomized trial that enrolled patients treated with DAPT after PCI with DES. At 12 months, patients who had no MACE or cerebrovascular event, repeat revascularization, or moderate or severe bleeding and had been adherent to thienopyridine therapy were randomized to continue thienopyridine or to placebo for another 18 months, to compare 12 months strategy vs 30 months strategy. The coprimary efficacy end points (the cumulative incidence of definite or probable ST and the composite of death, MI, or stroke) were significantly lower in the group that continued thienopyridine (0.4% vs 1.4% for stent thrombosis; 4.3% vs 5.9% for MACCE) and was consistent across stent type and thienopyridine drug used. However, prolonged DAPT lead to a significantly higher rate of bleeding, and all-cause mortality was increased by 36% in the prolonged DAPT group [57]. Importantly, most of the benefit observed with a prolonged DAPT treatment was observed among patients presenting with a MI [58,59].
Ticagrelor, when added to aspirin after an ACS, reduces the rate of major adverse CV events as compared with clopidogrel. However, patients who had a MI, who are at higher risk for recurrent ischemic events, could benefit from a prolonged DAPT with Ticagrelor.
The Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54 (PEGASUS-TIMI 54) trial, a randomized, double-blind, placebo-controlled clinical trial, tested long-term DAPT with ticagrelor, evaluating 2 different doses: 90 mg twice daily and 60 mg twice daily. The patients were considered eligible if had a spontaneous MI 1 to 3 years before, were at least 50 years of age, and had one of the following additional high-risk features: age of 65 years or older, diabetes mellitus (DM) requiring medication, a second prior spontaneous MI, multivessel coronary artery disease, or chronic renal dysfunction. They were randomized in a 1:1:1 ratio to receive ticagrelor orally at a dose of 90 mg twice daily, ticagrelor orally at a dose of 60 mg twice daily, or placebo. The median time from the MI (53.6% of them were STEMI) to randomization was 1.7 years. The two ticagrelor doses, reduced, as compared with placebo, the rate of CV death, MI, or stroke, but increased the rate of bleeding (even TIMI major bleeding, bleeding leading to transfusion, and bleeding leading to discontinuation of the study drug). Ultimately, the overall risk to benefit trade-off was improved with the ticagrelor 60mg bid dose, which lead to the final approval of this drug-dose with the new indication for extended DAPT [60].
Udell et al. conducted a meta-analysis of 6 RCTs on secondary prevention including 33 435 patients with prior-MI randomized to extended DAPT beyond 1 year or standard DAPT for 12 months. Extended DAPT beyond 1 year resulted in a 22% relative and 1.1% absolute risk reduction for major adverse CV events over a mean 31 months of follow-up with a 0.8% absolute increase in the risk of major bleeding, but without significant excess of ICH or fatal bleeding and no significant differences on non-CV causes of death. Importantly, extended DAPT was associated to a significant reduction of CV mortality [61].
Taken this into consideration, extended DAPT appears an attractive approach in patients with prior MI and low risk for bleeding. Whether the type of P2Y12i may be associated with a different impact on the overall long-term outcomes is not well established [62].
3.3. Short (1 or 3 or 6-months) DAPT
A short DAPT strategy of less than 12 months after coronary stent implantation has been compared to the standard of care (i.e., 12 months DAPT) in several RCTs, generally testing non-inferiority for ischemic events and superiority for bleeding.
The EXCELLENT trial (A Comparison of Xience/Promus Versus Cypher in Reducing Late Loss After Stenting) aimed to assess the effectiveness of a short-term DAPT strategy (6 months). A total of 1443 patients were randomly assigned in a 2 × 2 factorial design according to the type of stent (EES vs SES) and the duration of DAPT (6 vs 12 months). One of the points of the study was to determine if the short-term DAPT strategy was not inferior to the standard care concerning the occurrence of cardiac death, MI, or ischemia-driven target vessel revascularization (TVR). The primary end point is in-stent late loss at 9 months for comparison of type of stent, and the coprimary end point is target vessel failure (TVF) at 12 months for comparison of DAPT duration. The results indicated that the six-month DAPT strategy was non-inferior to the standard care. Additionally, although there was a numerical increase in TIMI major and minor bleeding in the 12-month group, this difference was not statistically significant (HR 0.40; 95% CI: 0.13–1.27; p = 0.12) [63].
The PRODIGY (PROlonging Dual antIplatelet treatment after Grading stent-induced intimal hYperplasia study) trial was a 4:2 randomized open-label clinical trial that evaluated the efficacy and the safety of prolonged DAPT with clopidogrel as P2Y12 inhibitor, randomly allocating patients (predominantly presenting with ACS) to treatment with four coronary stents (BMS, paclitaxel-eluting stent, E-ZES, everolimus-eluting stent) and two DAPT duration strategies (6 vs 24 months’ DAPT). The study showed no differences in the primary efficacy endpoint of death, MI, and stroke between 6 and 24 months DAPT, and, as expected, among the patients receiving 24-months DAPT, there was a risk of type 2, 3 or bleeding events two-folds greater than the group receiving 6-months DAPT (HR 2.17, 95% CI 1.44-3.22; p=0.00018) [64]. Results remained largely consistent in multiple subgroups [65,66,67].
The REDUCE trial, randomized 1,496 ACS patients treated with COMBO stent to 3 or 12 months of DAPT. The composite primary study endpoint of all-cause mortality, MI, ST, stroke, target vessel revascularization and bleeding at 12 months was similar in the two groups, reaching prespecified non-inferiority (8.2% vs 8.4%, pnon-inferiority<0.001). However, numerically higher rates of mortality and ST in the three-month DAPT group were observed [68]. The non-inferiority of 3 vs 12 months DAPT was confirmed in several high-risk subgroups [69,70,71].
3.4. Individualization Of DAPT Duration Based on Ischemic And Bleeding Risk
The optimal DAPT strategy, that maximize the efficacy and the safety of the treatment, balancing ischemic and bleeding risk, should be individual and selected based on patient’s and procedural characteristics (Figure 3) [72,73,74].
The clinical presentation (ACS vs CCS) at the time of PCI is an important feature that influences the patient’s mortality risk (ranging between 0.36% in CCS and 4.78% in high-risk STEMI patients), and the risk of recurrent ischemic events [75,76]. Clinical presentation in the setting of an all-comer PCI population is also a treatment modifier of DAPT duration after coronary stenting. Costa et al. conducted an analysis of the PRODIGY (Prolonging DualAntiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia Study) trial, a study designed to compare 6- or 24-month DAPT regimens in patients treated with PCI and receiving a balanced mixture of stents with varying anti-intimal hyperplasia potency and belonging to both first and second generation DES. It showed the lack of ischaemic benefit in favour of a 24-month course of DAPT, in both CCS and ACS patients. Both in CCS and ACS patients the rate of bleeding was higher in the 24-month DAPT arm, with a greater magnitude in patients presenting with CCS. In terms of NACE rates, after excluding BARC 2 bleeding, appeared a numerical increase of NACE in CCS patients only, with interaction testing providing consistent borderline results in the 24-months DAPT arm. So, this analysis suggested that clinical presentation is a treatment modifier with respect to the value of prolonged vs. shortened DAPT duration [67].
In the DAPT trial, a randomized double-blind, placebo-controlled trial comparing 30 versus 12 months of dual antiplatelet therapy after coronary stenting, 30-month DAPT compared with 12-month treatment significantly reduced definite or probable ST both in patients with MI (0.5 vs 1.9%; p= 0.001) and without MI (0.4 vs 1.1%; p= 0.001) (Pint = 0.69). Yet, the reduction of MACCE from longer DAPT was greater for patients with MI (3.9 vs 6.8%; p \ 0.001) than patients without MI (4.4 vs 5.3%; p = 0.08) at the time of presentation, with a positive interaction testing (Pint = 0.03). Of 11,648 randomized patients (9961 treated with drug-eluting, 1687 with bare metal stents), 3,576 (30.7%) presented with MI. Importantly, longer DAPT was associated with a significant increase in all- cause death among patients presenting without MI (2.1 vs 1.5%; p = 0.04) [57].
The ischemic risk after PCI is also associated to several anatomical or procedural characteristic. This is why they have been consistently considered important elements to be taken into account for decisions around DAPT duration [77,78]. The complexity of a PCI can be quantified using previously validated and guideline-endorsed criteria: PCI with ≥3 stents implanted and 3 ≥ lesions and/or coronary vessels treated; and/or bifurcation with 2 stents implanted, total stent length >60 mm, and/or treatment of a chronic total occlusion (CTO). In these patients, long-term DAPT (≥12 month) compared with a short period of DAPT (three or six months), significantly reduced the risk of cardiac ischemic events [79].
Even the localization of the coronary artery stenosis should be considered a treatment modifier for DAPT duration, as suggested by Costa et al. in a retrospective analysis of the PRODIGY trial. In patients with a lumen stenosis of at least 30% on angiography, appraised by visual estimation, of the Left main or the proximal LAD twenty-four DAPT regimen, compared to six-month DAPT significantly reduced the rate of definite, probable, or possible ST. A consistent trend towards interaction between CAD location and DAPT duration was also noted for the composite of CV death and MI. The 24-month DAPT regimen remained associated with possible benefits in patients with LM/pLAD lumen narrowing irrespective of whether a stent was or was not implanted in these segments or whether patients presented with acute coronary syndrome [80].
In a patient-level meta-analysis from six RCTs (N = 9577) investigating DAPT durations (12 vs 6 months) after coronary stenting, 17.5% of patients had at least one of the characteristics of complex PCI (three-vessel PCI, and/or an implantation of three or more coronary stents, and/or three or more coronary lesions, and/or bifurcation stenting, i.e., bifurcation technique using stents in both the main and the side branch, and/or a final total stent length 60 mm, and/or treatment of a CTO). In this group, long DAPT compared with short DAPT reduced the adjusted MACCE rate (unadjusted event rates: 4.0 vs 6.0%; adjusted HR 0.56, 95% CI 0.35–0.89), whereas no benefit for a longer treatment was observed in the non-complex PCI group (2.5 vs 2.6%; adjusted HR 1.01; 95% CI 0.75–1.35) (Pint = 0.01). The magnitude of benefit in favor of long DAPT was directly and positively related to the number of complex PCI factors [81].
Concomitant high bleeding risk can mitigate the benefit from a longer DAPT regimen in patients undergoing a complex PCI. In an analysis that included 14,963 patients from 8 randomized trials, long-term DAPT in non-HBR patients reduced the ischemic events in both complex and noncomplex PCI, but not among HBR (PRECISE-DAPT > 25) patients, regardless of complex PCI features [82].
3.5. Optimal DAPT Duration in HBR Patients
The optimal duration of DAPT in high bleeding risk patients (HBR) has been recently explored. DAPT leads to a significant increase of the rate of major bleeding, associated with greater risks of adverse cardiac outcomes. Major bleeding is associated with an immediate and sustained increased risk of mortality, similar or greater than recurrent MI, easily offsetting the benefit of its ischemic protection. Roughly one out of three patients undergoing PCI is at HBR (i.e., patients with older age, low hemoglobin level, thrombocytopenia, renal insufficiency, cancer, a prior stroke, and a bleeding history) [25]. HBR features are also associated with an increased ischemic risk. These patients are considered to be at double-sided risk: high risk for bleeding, and high risk for recurrent ischemic or thrombotic events, that’s why weighing in ischemic and bleeding risk to decide the optimal DAPT strategy is a challenge for the clinician [83].
The current guidelines endorse the use of a standardized tool, the predicting bleeding complications in patients undergoing stent implantation and subsequent DAPT therapy (PRECISE-DAPT) score for bleeding risk stratification [84]. The PRECISE-DAPT score was developed to predict the bleeding risk in patients undergoing PCI and, therefore, a DAPT regimen. This score is based on five features clinical and laboratoristic features: age, white blood cell count, hemoglobin level, creatinine clearance, and history of spontaneous bleeding. Patients with a score of ≥25 are at a high risk of bleeding, indicating that the DAPT duration should be shorter (3 to 6 months) than that in patients with a score of < 25. To derive and validate the score, Costa et al., pooled 14 963 patients treated with DAPT after coronary stenting from eight multicentre randomized clinical trials. Using Cox proportional hazards regression, predictors of TIMI major or minor bleeding were identified, and based on them, a numerical score was developed. A derivation cohort of patients was used to assess the predictive performance of the score and it was validated in validation cohorts of patients from the PLATO trial (n=8595) and BernPCI registry (n=6172). In patients identified at high risk (score ≥25), a longer DAPT duration significantly increased bleeding, but not in those with lower risk profiles [85]. Multiple external validations of this prediction tool have been presented largely confirming the score discriminative ability [86,87].
A simplified version of the score, the 4-item PRECISE-DAPT, lacking white blood cells count, has been studied to know if it has potential to guide DAPT. In an analysis carried out in a pooled dataset of 5 randomized studies and including more than 10,000 patients, it showed that it may be useful to support clinical decision-making for DAPT duration [88].
The Academic Research Consortium for High Bleeding Risk (ARC-HBR), a collaboration of leading research organizations, regulatory authorities, and physician-scientists from the United States, Asia, and Europe focused on PCI–related bleeding, elaborated a standardized definition of HBR patients, based on review of the available evidence. Twenty clinical criteria were identified as major or minor by the consensus. Patients are considered to be at HBR if at least 1 major or 2 minor criteria are met. The coexistence of numerous numbers of risk factors is associated with a linear increase in risk of BARC 3 to 5 bleeding. Multiple external validations of this classification have been recently published [89].
The optimal DAPT duration for limiting bleeding risk while not reducing ischemic protection, was investigated in the MASTER DAPT trial. MASTER-DAPT was the first randomized trial to demonstrate that among HBR patients undergoing coronary stenting with a bioresorbable polymer-based sirolimus-eluting stent, abbreviating DAPT to 1 month was non-inferior to a standard DAPT for 6 months or more in terms of NACE, or major adverse cardiac or cerebral events, and superior in terms of major or clinically relevant non-major bleeding (MCRB). The trial enrolled patients, regardless their clinical presentation, that had undergone successful PCI with implantation of a biodegradable-polymer sirolimus-eluting stent (Ultimaster, Terumo), at HBR. Patients had to be free from ischemic and active bleeding events at the moment of the randomization. They were randomly assigned to an abbreviated DAPT regimen (i.e., stopped DAPT after 30 days and continued SAPT; abbreviated-therapy group) or to standard DAPT regimen (i.e., 6 months after the index procedure; standard-therapy group). The aim of the trial was to test whether the abbreviated dual antiplatelet therapy, was noninferior in terms of net adverse clinical events (NACE), major adverse cardiac or cerebral events (MACCE), and superior with regard to major or clinically relevant bleeding, compared to standard regimen. The trial showed that in patients at high risk for bleeding, the discontinuation of DAPT at a median of 34 days after PCI led to a reduction of the incidence of major or clinically relevant non-major bleeding (6.5% in the abbreviated-therapy group and 9.4% in the standard-therapy group) and was noninferior with regard to NACE and MACCE compared to standard treatment [90].
The XIENCE 28 and XIENCE 90 studies, were two prospective, single-arm studies, that compared 1 month DAPT regimen (XIENCE 28) and 3 months DAPT regimen (XIENCE 90), in patients HBR undergone successful PCI with a Xience stent implanted, a durable polymer everolimus-eluting stent, with 12-months DAPT, testing the hypothesis that would be non-inferior in terms of ischemic events and superior with respect to bleeding events. A total of 3652 patients, free from MI, repeat coronary revascularization, stroke, or ST, were randomized to 1 month (1605) or 3 months (2047) DAPT. Patients that presented with STEMI, or with a left ventricular ejection fraction < 30% were excluded. Most of the patients continued with ASA after DAPT discontinuation. The primary study endpoint was all-cause death or all MI, the secondary endpoints were BARC 2-5 bleeding and definite/probable ST. The studies present limitations inherent to the non-randomized design. A short DAPT regimen of 1 or 3 months resulted non-inferior with respect to ischemic outcomes, had similar rates of clinically relevant (BARC 2-5) bleeding, with a significant reduction in major (BARC 3-5) bleeding and a very low incidence of stent thrombosis [91,92].
A recent metanalysis of RCTs, searched studies comparing abbreviated (1 month) or short (3 months) with standard (≥6 months) DAPT in HBR patients (PRECISE-DAPT > 25) without indication for oral anticoagulation, to estimate the impact of this abbreviated DAPT regimens in this setting of patients. Articles were initially screened by title and abstract content. A total of 11 RCTs, including 9006 patients treated with PCI who were randomized to abbreviated (≤3 months) or standard (≥6 months) DAPT durations, and reporting outcome data for bleeding and ischemic endpoints at a minimum follow-up of 12 months after enrollment were included. A lower rate of major or clinically relevant non-major bleeding, major bleeding and CV mortality was registered with the abbreviated DAPT regimens, with no significant differences in terms of prevention of MACE, ST, and other ischemic events, irrespective of clinical presentation and P2Y12i used (Figure 4) [93].
The risk factors for both bleeding and ischemic events can intersect, leading to an ongoing debate regarding the most effective approach to reduce both types of events in this particular patient population. The OPT-BIRISK trial is a multicentre, double-blind, placebo-controlled superiority trial comparing clopidogrel monotherapy with DAPT, aspirin and clopidogrel, in patients with both high bleeding and ischaemic risk who have completed 9-12 months of DAPT post PCI for ACS. The primary endpoint of BARC 2, 3 or 5 bleeding and the key secondary endpoint of MACCE (a composite of all-cause mortality, MI, stroke or clinically driven revascularisation) were lower in the clopidogrel monotherapy arm, 2.5% vs. 3.3%, (HR 0.75, 95%CI 0.57-0.97, p=0.03) and 2.6%. vs 3.5%, (HR 0.74, 95%CI 0.57-0.96, p=0.02). The majority of patients enrolled in the study presented with unstable angina, which could potentially influence the observed outcomes. However, it’s important to consider that patients were not randomized into treatment groups until 9-12 months after undergoing PCI. This timing suggests that the patient population was transitioning toward the chronic phase within the spectrum of ACS/CCS [94].
3.6. Patients Treated on Long-Term OAC
The need for the association of antiplatelet and anticoagulant therapies is frequent, mostly in patients affected by atrial fibrillation that need thromboembolic prevention (AF) undergoing PCI or with concomitant ACS (condition that occurs in about 10% of cases of hospital admission for ACS) [95]. Anticoagulant therapy is inferior to antiplatelet therapy after stent implantation to prevent recurrent ischemic events and ST, on the other hand, antiplatelet therapy is inferior to anticoagulant therapy to prevent stroke and systemic embolism in patients with AF [96]. However, the combination of antithrombotic agents, triple therapy with oral anticoagulation and dual antiplatelet therapy (TAT), exposes the patient to an excessive bleeding hazard (3-4 times higher than the two treatments considered alone) [97]. Hence the patient needing long-term oral anticoagulation is considered HBR per se.
Considering that long term OAC therapy is mandatory in this setting, reducing DAPT duration has been widely explored in multiple clinical trials, testing the hypothesis of removing one antiplatelet agent early after stenting, downgrading TAT to a dual antithrombotic therapy (DAT) [98].
Several studies focused the attention on this clinical setting, studying the duration and the intensity of the antithrombotic treatment. Multiple trials evaluated, in patients with AF undergoing PCI, safety and efficacy of a DAT therapy approach with a NOAC compared with a triple antithrombotic therapy with a vitamin K antagonist [99,100].
The PIONEER AF-PCI trial, randomized 2124 patients affected by non-valvular AF treated with PCI, to receive DAT consisting of low-dose rivaroxaban (15 mg die) plus a P2Y12 inhibitor; very low-dose rivaroxaban (2.5 mg die) plus DAPT, or VKA plus DAPT. At 12 months, the study showed a lower rate of relevant bleeding in the groups not receiving a VKA, with the lowest rate in the low-dose rivaroxaban group (6.8% for rivaroxaban 15 mg + P2Y12i, 18.0% for rivaroxaban 2.5 mg + 26.7% for VKA + DAPT). Rates of ischemic events did not significantly differ in the three groups [99].
The AUGUSTUS trial, a randomized trial with 2:2 factorial design, enrolled 4614 patients with AF who had an ACS or had undergone PCI and were planning to take a P2Y12 inhibitor and randomized them to receive apixaban or a vitamin K antagonist and to receive aspirin or placebo for 6 months. AUGUSTUS is the first trial to test both the concept of OAC type and dual vs. triple therapy separately. At six-month follow-up, the primary endpoint, the rate of MCRB, was 10.5% of the patients receiving apixaban, as compared with 14.7% of those receiving a VKA. With respect to the second randomization, the primary endpoint occurred in 16.1% in the aspirin group, as compared to 9.0% in the placebo group (HR, 1.89; 95% CI, 1.59–2.24; p < 0.001). With respect to ischemic events, the rate was similar among patients treated with apixaban or VKA and also for patients randomized to aspirin or placebo. Ischemic stroke was significantly reduced by 50% among patients in the apixaban arm. In conclusion, in patients with AF and a recent ACS or PCI both dual therapy and apixaban were associated to a reduction of bleeding without an increase in ischemic events [101].
The impact of dual or triple therapy in HBR patients undergoing PCI has been evaluated in a subgroup analysis of the REDUAL PCI trial. In this study, DAT with dabigatran 110mg bid reduced bleeding risk in both patients at HBR and non-HBR. In turn, DAT with dabigatran 150mg compared to warfarin based TAT, reduced bleeding in non-HBR patients but not in HBR patients, with a trend towards less benefit in HBR patients [102].
Importantly, while most of the trials tested a DAT approach linked to NOAC and a TAT linked to VKA [103,104], it is important to unravel the true benefit associated to dual therapy beyond those given by a treatment with NOAC, which per se is associated to less bleeding compared to VKA. On this matter, Montalto et al. performed a systematic review evaluating randomized controlled trials comparing an abbreviated (4-6 weeks) or prolonged (>= 3 months) DAPT regimen in patients with OAC. Co-primary endpoints were MCRB and major bleeding, while the rate of MACE was endpoint for safety. Five studies were included, for a total of 7665 patients, 3843 treated with abbreviated DAPT and 3822 with prolonged DAPT. MCRB and major bleeding were lower with abbreviated DAPT [risk ratio (RR) 0.69 (0.52-0.91); P = 0.01 and 0.70 (0.52-0.95); P = 0.01, respectively] while the rate of MACE and other ischemic events (CV death, ST, MI) did not differ. Network meta-analysis showed that peri-procedural DAPT had the highest probability to be the best treatment in preventing MCRB and major bleeding when compared with both short and longer DAPT strategies [105].
4. Options for DAPT Discontinuation
After an initial period with DAPT, discontinuation of this regimen could be either followed by aspirin or P2Y12 inhibitor monotherapy. Multiple RCTs evaluated if a shorter term DAPT strategy for 6, 3 or even 1 months after DES implantation, followed by ASA monotherapy, was non-inferior to 12 months DAPT for ischemic endpoints while providing a reduction in bleeding events. More recently, a short DAPT strategy for 1-3 months followed by P2Y12 inhibitor monotherapy vs. standard DAPT was tested in multiple RCTs. Most of the patients in the P2Y12-inhibitor monotherapy arm of these trials were treated with ticagrelor. In a systematic review and individual participant data meta-analysis, Valgimigli et al. evaluated all randomised trials that compared P2Y12 inhibitor monotherapy after DAPT with DAPT among patients who underwent coronary revascularization. Among the 24,096 patients included, P2Y12i monotherapy was non-inferior to longer-term DAPT for the composite endpoint of all cause death, MI, and stroke throughout (2.95% vs. 3.27; P=0.005 for non-inferiority). This strategy also reduced the risk of BARC type 3 or type 5 bleeding among patients randomly allocated to P2Y12 inhibitor monotherapy [106]. Interestingly, these results were consistent also when higher risk patients treated with complex PCI were evaluated [107].
4.1. ASA Or P2Y12 Inhibitors for Long-Term Single Antiplatelet Therapy
While international guidelines endorse long-term treatment with aspirin in patients with prior ischemic events [108], which in practice often translate to a lifetime commitment to this therapy, whether P2Y12 inhibitor might represent a better option to the aspirin paradigm has been a matter of debate.
In the CAPRIE trial, that randomized patients with a recent ACS to clopidogrel vs. aspirin monotherapy, clopidogrel was associated to small but statistically significant 8.7% relative reduction of the primary ischemic endpoint compared to aspirin, with a favorable safety profile with less hemorrhagic events, especially gastrointestinal bleedings [109].
In a large systemic review and study level meta-analysis including 42,108 patients, Chiarito et al. observed that P2Y12 inhibitor monotherapy is associated with a modest significant reduction of the risk of MI compared with those who received aspirin (OR 0·81 [95% CI 0·66-0·99]; I2=10·9%) while the risk of stroke, all-cause death, vascular death and major bleeding did not differ between the two groups [110].
The HOST-EXAM trial (Harmonizing Optimal Strategy for Treatment of Coronary Artery Stenosis–Extended Antiplatelet Monotherapy) randomized patients who underwent uneventful DAPT for 12±6 months after PCI to discontinue DAPT continuing with either aspirin or clopidogrel. The study demonstrated that clopidogrel monotherapy was superior to aspirin monotherapy during the chronic maintenance period with regard to net adverse clinical events (5.7% vs. 7.7%, HR 0.73, 95%-CI: 0.59–0.90, P < 0.01) during the 24 months follow-up. The study extended follow-up also showed that clopidogrel monotherapy was associated with a 26% risk reduction of the primary end point, similar to the results during the in-trial period, with no difference in terms of all-cause death between aspirin and clopidogrel [111]. This randomized comparison importantly challenges the central role of aspirin in the long-term management of vascular disease patients.
Consistently, in a recent patient-level meta-analysis of 7 randomized trials and 24,325 patients Gragnano et al. compared P2Y12 inhibitor vs aspirin monotherapy in patients with established CAD.
The rate of the primary outcome, a composite of CV death, MI, and stroke, was lower with P2Y12 inhibitor monotherapy compared with aspirin over a 2 year follow-up, mainly driven by a significant reduction of MI (HR: 0.77; 95% CI: 0.66-0.90; P < 0.001), with similar rates of major bleeding and a more favorable net adverse clinical events profile in the P2Y12i group [112].
The SHARE (SHort-term Dual Antiplatelet Therapy After Deployment of BioabsoRbable Polymer Everolimus-Eluting Stent) trial, a study with the aim to compare the efficacy and safety of P2Y12 inhibitor monotherapy after 3 months of DAPT vs 12-month DAPT in patients treated with DES implantation. P2Y12i used were Clopidogrel for patients with CCS and Ticagrelor for patients with ACS. The study met the non-inferiority criteria for the primary outcome of NACE (a composite of MACCE and major bleeding) at 3 months, -0.44 % (95% CI, -1.19 to 0.32) P for noninferiority < 0.001, and 12 months, -0.93% (95% CI, -2.64 to 0.77) P for noninferiority < 0.001. The P2Y12i monotherapy also reduced the rate of major bleeding (0,2% vs 0,8%) [113].
4.2. Immediate DAPT Discontinuation after PCI, the No DAPT Strategy
With a trend towards exploring the feasibility of a progressively shorter DAPT after PCI with 6, 3 and even 1-month periods, the complete omission of aspirin immediately after PCI appears as a natural extension of the short-DAPT strategy.
This concept has been first studies in the ASET (Acetyl Salicylic Elimination Trial) a multicenter pilot study, of an aspirin-free prasugrel monotherapy strategy tested immediately after PCI in patients presenting with CCS undergoing non-complex PCI. The exploratory study design, based on a stop rule in case of more than 3 coronary ST were observed, showed that this strategy was feasible with no ST observed while ischemic events were rare [114].
This strategy was also recently studied in ACS patients in the OPTICA and MACT trial which resembled the study design of the ASET [115,116]. In this latter trial which was also the only one to include STEMI patients, two ST were observed all in this higher risk group, which raise concern regarding early de-escalation of treatment in patients at particularly high ischemic risk such as STEMI patients [115,116,117].
The recent STOPDAPT-3 trial compared an aspirin free strategy with prasugrel monotherapy at a dose of 3.75 mg/day with a DAPT prasugrel based strategy (Aspirin 81-100 mg/day and prasugrel 3.75 mg/day) in patients undergoing PCI or ACS. 75% of the patients enrolled presented with ACS. The prasugrel monotherapy was not superior to DAPT for major bleeding events (BARC 3 or 5) and, although cardiovascular events met criteria for noninferiority, they were higher in the monotherapy group at 30 days. These results indicates that a a strategy of de-escalation immediately post-PCI is not beneficial and could in fact be harmful, particularly among ACS patients [118].
However, while the no DAPT strategy appeared feasible and could represent a solution for patients at extremely HBR or truly intolerant to aspirin, larger randomized studies are needed before broader clinical implementation.
5. Conclusions
DAPT has been the cornerstone of treatment after coronary stenting and secondary prevention after an ACS. Individualize antiplatelet therapy after stenting represents an opportunity to balance ischemic and bleeding risk especially in higher risk patients. Procedural complexity, patient characteristics and bleeding risk collectively shape the decision-making process surrounding DAPT. The quest for a ‘one-size-fits-all’ regimen is progressively supplanted by the recognition of a nuanced, patient-centered approach.
Author Contributions
Conceptualization—writing—original draft preparation—review and editing, G.C.; conceptualization—writing—original draft preparation—review and editing, F.C.; writing—review and editing, G.D.L.; review and editing, V.G.; review and editing, M.G.; review and editing, E.S.; review and editing, A.Ma.; review and editing, L.T.; review and editing, S.C.; review and editing, G.D.B.; review and editing, A.M; review and editing, E.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Conflicts of Interest
Mattia Galli declares to have received speaker fees from Terumo. The other authors declare no conflicts of interest.
References
- Van Zandvoort, L.J.C.; Ali, Z.; Kern, M.; Van Mieghem, N.M.; Mintz, G.S.; Daemen, J. Improving PCI Outcomes Using Postprocedural Physiology and Intravascular Imaging. JACC Cardiovasc. Interv. 2021, 14, 2415–2430. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on Myocardial Revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Shiomi, H.; Kozuma, K.; Morimoto, T.; Kadota, K.; Tanabe, K.; Morino, Y.; Tamura, T.; Abe, M.; Suwa, S.; Ito, Y.; et al. Ten-year Clinical Outcomes from a Randomized Trial Comparing New-generation Everolimus-eluting Stent versus First-generation Sirolimus-eluting Stent: Results from the RESET Extended Study. Catheter. Cardiovasc. Interv. 2023, ccd.30791. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Smits, P.; Hofma, S.H.; Di Lorenzo, E.; Vlachojannis, G.J.; Van’T Hof, A.W.J.; Van Boven, A.J.; Kedhi, E.; Stone, G.W.; Suryapranata, H. Everolimus Eluting Stent vs First Generation Drug-Eluting Stent in Primary Angioplasty: A Pooled Patient-Level Meta-Analysis of Randomized Trials. Int. J. Cardiol. 2017, 244, 121–127. [Google Scholar] [CrossRef]
- De Luca, G.; Suryapranata, H.; Stone, G.W.; Antoniucci, D.; Tcheng, J.E.; Neumann, F.-J.; Bonizzoni, E.; Topol, E.J.; Chiariello, M. Relationship Between Patient’s Risk Profile and Benefits in Mortality From Adjunctive Abciximab to Mechanical Revascularization for ST-Segment Elevation Myocardial Infarction: A Meta-Regression Analysis of Randomized Trials. J. Am. Coll. Cardiol. 2006, 47, 685–686. [Google Scholar] [CrossRef]
- Secco, G.G.; Ghione, M.; Mattesini, A.; Dall’Ara, G.; Ghilencea, L.; Kilickesmez, K.; De Luca, G.; Fattori, R.; Parisi, R.; Marino, P.N.; et al. Very High-Pressure Dilatation for Undilatable Coronary Lesions: Indications and Results with a New Dedicated Balloon. EuroIntervention 2016, 12, 359–365. [Google Scholar] [CrossRef]
- Silverio, A.; Di Maio, M.; Citro, R.; Esposito, L.; Iuliano, G.; Bellino, M.; Baldi, C.; De Luca, G.; Ciccarelli, M.; Vecchione, C.; et al. Cardiovascular Risk Factors and Mortality in Hospitalized Patients with COVID-19: Systematic Review and Meta-Analysis of 45 Studies and 18,300 Patients. BMC Cardiovasc. Disord. 2021, 21, 23. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Forouzanfar, M.H.; Moran, A.E.; Barber, R.; Nguyen, G.; Feigin, V.L.; Naghavi, M.; Mensah, G.A.; Murray, C.J.L. Demographic and Epidemiologic Drivers of Global Cardiovascular Mortality. N. Engl. J. Med. 2015, 372, 1333–1341. [Google Scholar] [CrossRef]
- De Luca, G.; Dirksen, M.T.; Spaulding, C.; Kelbæk, H.; Schalij, M.; Thuesen, L.; Van Der Hoeven, B.; Vink, M.A.; Kaiser, C.; Musto, C.; et al. Impact of Diabetes on Long-Term Outcome After Primary Angioplasty. Diabetes Care 2013, 36, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; Revaiah, P.C.; Ninomiya, K.; Masuda, S.; Kotoku, N.; Kageyama, S.; Onuma, Y.; Morel, M.A.; Garg, S.; Feldman, T.; et al. 10 Years of SYNTAX. JACC Asia 2023, 3, 409–430. [Google Scholar] [CrossRef]
- Sterling, L.H.; Fernando, S.M.; Talarico, R.; Qureshi, D.; Van Diepen, S.; Herridge, M.S.; Price, S.; Brodie, D.; Fan, E.; Di Santo, P.; et al. Long-Term Outcomes of Cardiogenic Shock Complicating Myocardial Infarction. J. Am. Coll. Cardiol. 2023, 82, 985–995. [Google Scholar] [CrossRef]
- Verdoia, M.; Schaffer, A.; Barbieri, L.; Aimaretti, G.; Marino, P.; Sinigaglia, F.; Suryapranata, H.; De Luca, G. Impact of Diabetes on Neutrophil-to-Lymphocyte Ratio and Its Relationship to Coronary Artery Disease. Diabetes Metab. 2015, 41, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Makris, A.; Barkas, F.; Sfikakis, P.P.; Liberopoulos, E.; Filippatos, T.D.; Ray, K.K.; Agouridis, A.P. Lipoprotein(a), Interleukin-6 Inhibitors, and Atherosclerotic Cardiovascular Disease: Is There an Association? Atheroscler. Plus 2023, 54, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rizzacasa, B.; Amati, F.; Romeo, F.; Novelli, G.; Mehta, J.L. Epigenetic Modification in Coronary Atherosclerosis. J. Am. Coll. Cardiol. 2019, 74, 1352–1365. [Google Scholar] [CrossRef] [PubMed]
- Novara Atherosclerosis Study Group (NAS); De Luca, G.; Verdoia, M.; Cassetti, E.; Schaffer, A.; Cavallino, C.; Bolzani, V.; Marino, P. High Fibrinogen Level Is an Independent Predictor of Presence and Extent of Coronary Artery Disease among Italian Population. J. Thromb. Thrombolysis 2011, 31, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.R.; Yusuf, S.; Peters, R.J.; Bertrand, M.E.; Lewis, B.S.; Natarajan, M.K.; Malmberg, K.; Rupprecht, H.-J.; Zhao, F.; Chrolavicius, S.; et al. Effects of Pretreatment with Clopidogrel and Aspirin Followed by Long-Term Therapy in Patients Undergoing Percutaneous Coronary Intervention: The PCI-CURE Study. The Lancet 2001, 358, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Castellano, J.M.; Pocock, S.J.; Bhatt, D.L.; Quesada, A.J.; Owen, R.; Fernandez-Ortiz, A.; Sanchez, P.L.; Marin Ortuño, F.; Vazquez Rodriguez, J.M.; Domingo-Fernández, A.; et al. Polypill Strategy in Secondary Cardiovascular Prevention. N. Engl. J. Med. 2022, 387, 967–977. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Angiolillo, D.A.; Galli, M.; Collet, J.-P.; Kastrati, A.; O’Donoghue, M.O. Antiplatelet Therapy after Percutaneous Coronary Intervention. EuroIntervention 2022, 17, e1371–e1396. [Google Scholar] [CrossRef] [PubMed]
- Patrono, C.; García Rodríguez, L.A.; Landolfi, R.; Baigent, C. Low-Dose Aspirin for the Prevention of Atherothrombosis. N. Engl. J. Med. 2005, 353, 2373–2383. [Google Scholar] [CrossRef] [PubMed]
- Fontana, P.; Dupont, A.; Gandrille, S.; Bachelot-Loza, C.; Reny, J.-L.; Aiach, M.; Gaussem, P. Adenosine Diphosphate–Induced Platelet Aggregation Is Associated With P2Y 12 Gene Sequence Variations in Healthy Subjects. Circulation 2003, 108, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Giustino, G.; Mehran, R.; Dangas, G.D.; Kirtane, A.J.; Redfors, B.; Généreux, P.; Brener, S.J.; Prats, J.; Pocock, S.J.; Deliargyris, E.N.; et al. Characterization of the Average Daily Ischemic and Bleeding Risk After Primary PCI for STEMI. J. Am. Coll. Cardiol. 2017, 70, 1846–1857. [Google Scholar] [CrossRef] [PubMed]
- Patrono, C.; Morais, J.; Baigent, C.; Collet, J.-P.; Fitzgerald, D.; Halvorsen, S.; Rocca, B.; Siegbahn, A.; Storey, R.F.; Vilahur, G. Antiplatelet Agents for the Treatment and Prevention of Coronary Atherothrombosis. J. Am. Coll. Cardiol. 2017, 70, 1760–1776. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Costa, F.; Lokhnygina, Y.; Clare, R.M.; Wallentin, L.; Moliterno, D.J.; Armstrong, P.W.; White, H.D.; Held, C.; Aylward, P.E.; et al. Trade-off of Myocardial Infarction vs. Bleeding Types on Mortality after Acute Coronary Syndrome: Lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) Randomized Trial. Eur. Heart J. 2016, ehw525. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Roffi, M.; Byrne, R.A.; Costa, F.; Valgimigli, M.; Task Force for the Management of Dual Antiplatelet Therapy in Coronary Artery Disease of the European Society of Cardiology (ESC); Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; et al. Case-Based Implementation of the 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease. Eur. Heart J. 2018, 39, e1–e33. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Costa, F.; Byrne, R.; Haude, M.; Baumbach, A.; Windecker, S. Dual Antiplatelet Therapy Duration after Coronary Stenting in Clinical Practice: Results of an EAPCI Survey. EuroIntervention 2015, 11, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Windecker, S.; Valgimigli, M. Dual Antiplatelet Therapy Duration: Reconciling the Inconsistencies. Drugs 2017, 77, 1733–1754. [Google Scholar] [CrossRef]
- Costa, F.; Valgimigli, M. The Optimal Duration of Dual Antiplatelet Therapy after Coronary Stent Implantation: To Go Too Far Is as Bad as to Fall Short. Cardiovasc. Diagn. Ther. 2018, 8, 630–646. [Google Scholar] [CrossRef]
- Capodanno, D.; Mehran, R.; Krucoff, M.W.; Baber, U.; Bhatt, D.L.; Capranzano, P.; Collet, J.-P.; Cuisset, T.; De Luca, G.; De Luca, L.; et al. Defining Strategies of Modulation of Antiplatelet Therapy in Patients With Coronary Artery Disease: A Consensus Document from the Academic Research Consortium. Circulation 2023, 147, 1933–1944. [Google Scholar] [CrossRef]
- Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N. Engl. J. Med. 2001, 345, 494–502. [CrossRef] [PubMed]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Schreuder, M.M.; Badal, R.; Boersma, E.; Kavousi, M.; Roos-Hesselink, J.; Versmissen, J.; Visser, L.E.; Roeters Van Lennep, J.E. Efficacy and Safety of High Potent P2Y 12 Inhibitors Prasugrel and Ticagrelor in Patients With Coronary Heart Disease Treated With Dual Antiplatelet Therapy: A Sex-Specific Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2020, 9, e014457. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the Management of Acute Coronary Syndromes. Eur. Heart J. 2023, ehad191. [Google Scholar] [CrossRef]
- Epstein, F.H.; Fuster, V.; Badimon, L.; Badimon, J.J.; Chesebro, J.H. The Pathogenesis of Coronary Artery Disease and the Acute Coronary Syndromes. N. Engl. J. Med. 1992, 326, 310–318. [Google Scholar] [CrossRef]
- Galli, M.; Ortega-Paz, L.; Franchi, F.; Rollini, F.; Angiolillo, D.J. Precision Medicine in Interventional Cardiology: Implications for Antiplatelet Therapy in Patients Undergoing Percutaneous Coronary Intervention. Pharmacogenomics 2022, 23, 723–737. [Google Scholar] [CrossRef]
- Kikkert, W.J.; Damman, P. Optimal Duration of Dual Antiplatelet Therapy for Coronary Artery Disease. Neth. Heart J. 2018, 26, 321–333. [Google Scholar] [CrossRef]
- De Luca, G.; Dirksen, M.T.; Spaulding, C.; Kelbæk, H.; Schalij, M.; Thuesen, L.; Van Der Hoeven, B.; Vink, M.A.; Kaiser, C.; Musto, C.; et al. Drug-Eluting vs Bare-Metal Stents in Primary Angioplasty: A Pooled Patient-Level Meta-Analysis of Randomized Trials. Arch. Intern. Med. 2012, 172. [Google Scholar] [CrossRef]
- McFadden, E.P.; Stabile, E.; Regar, E.; Cheneau, E.; Ong, A.T.; Kinnaird, T.; Suddath, W.O.; Weissman, N.J.; Torguson, R.; Kent, K.M.; et al. Late Thrombosis in Drug-Eluting Coronary Stents after Discontinuation of Antiplatelet Therapy. The Lancet 2004, 364, 1519–1521. [Google Scholar] [CrossRef]
- Joner, M.; Finn, A.V.; Farb, A.; Mont, E.K.; Kolodgie, F.D.; Ladich, E.; Kutys, R.; Skorija, K.; Gold, H.K.; Virmani, R. Pathology of Drug-Eluting Stents in Humans. J. Am. Coll. Cardiol. 2006, 48, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Camenzind, E.; Steg, P.G.; Wijns, W. A Cause for Concern. Circulation 2007, 115, 1440–1455. [Google Scholar] [CrossRef]
- Kolh, P.; Wijns, W.; Danchin, N.; Di Mario, C.; Falk, V.; Folliguet, T.; Garg, S.; Huber, K.; James, S.; Knuuti, J. Guidelines on Myocardial Revascularization. Eur. J. Cardiothorac. Surg. 2010, 38, S1–S52. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Sabate, M.; Kaiser, C.; Brugaletta, S.; De La Torre Hernandez, J.M.; Galatius, S.; Cequier, A.; Eberli, F.; De Belder, A.; Serruys, P.W.; et al. Effects of Cobalt-Chromium Everolimus Eluting Stents or Bare Metal Stent on Fatal and Non-Fatal Cardiovascular Events: Patient Level Meta-Analysis. BMJ 2014, 349, g6427–g6427. [Google Scholar] [CrossRef]
- Wijns, W.; Steg, P.G.; Mauri, L.; Kurowski, V.; Parikh, K.; Gao, R.; Bode, C.; Greenwood, J.P.; Lipsic, E.; Alamgir, F.; et al. Endeavour Zotarolimus-Eluting Stent Reduces Stent Thrombosis and Improves Clinical Outcomes Compared with Cypher Sirolimus-Eluting Stent: 4-Year Results of the PROTECT Randomized Trial. Eur. Heart J. 2014, 35, 2812–2820. [Google Scholar] [CrossRef]
- Capodanno, D.; Bhatt, D.L.; Gibson, C.M.; James, S.; Kimura, T.; Mehran, R.; Rao, S.V.; Steg, P.G.; Urban, P.; Valgimigli, M.; et al. Bleeding Avoidance Strategies in Percutaneous Coronary Intervention. Nat. Rev. Cardiol. 2022, 19, 117–132. [Google Scholar] [CrossRef]
- Benenati, S.; Galli, M.; De Marzo, V.; Pescetelli, F.; Toma, M.; Andreotti, F.; Bona, R.D.; Canepa, M.; Ameri, P.; Crea, F.; et al. Very Short vs. Long Dual Antiplatelet Therapy after Second Generation Drug-Eluting Stents in 35 785 Patients Undergoing Percutaneous Coronary Interventions: A Meta-Analysis of Randomized Controlled Trials. Eur. Heart J.-Cardiovasc. Pharmacother. 2021, 7, 86–93. [Google Scholar] [CrossRef]
- Mauri, L.; Hsieh, W.; Massaro, J.M.; Ho, K.K.L.; D’Agostino, R.; Cutlip, D.E. Stent Thrombosis in Randomized Clinical Trials of Drug-Eluting Stents. N. Engl. J. Med. 2007, 356, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Cutlip, D.E.; Chhabra, A.G.; Baim, D.S.; Chauhan, M.S.; Marulkar, S.; Massaro, J.; Bakhai, A.; Cohen, D.J.; Kuntz, R.E.; Ho, K.K.L. Beyond Restenosis: Five-Year Clinical Outcomes From Second-Generation Coronary Stent Trials. Circulation 2004, 110, 1226–1230. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Maehara, A.; Lansky, A.J.; De Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P.; et al. A Prospective Natural-History Study of Coronary Atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Trip, M.D.; Cats, V.M.; Van Capelle, F.J.L.; Vreeken, J. Platelet Hyperreactivity and Prognosis in Survivors of Myocardial Infarction. N. Engl. J. Med. 1990, 322, 1549–1554. [Google Scholar] [CrossRef]
- Gawaz, M.; Neumann, F.-J.; Ott, I.; Schiessler, A.; Schömig, A. Platelet Function in Acute Myocardial Infarction Treated With Direct Angioplasty. Circulation 1996, 93, 229–237. [Google Scholar] [CrossRef]
- Brandt, J.T.; Payne, C.D.; Wiviott, S.D.; Weerakkody, G.; Farid, N.A.; Small, D.S.; Jakubowski, J.A.; Naganuma, H.; Winters, K.J. A Comparison of Prasugrel and Clopidogrel Loading Doses on Platelet Function: Magnitude of Platelet Inhibition Is Related to Active Metabolite Formation. Am. Heart J. 2007, 153, e9–e66. [Google Scholar] [CrossRef]
- Alnasser, S.M.A.; Huang, W.; Gore, J.M.; Steg, Ph.G.; Eagle, K.A.; Anderson, F.A.; Fox, K.A.A.; Gurfinkel, E.; Brieger, D.; Klein, W.; et al. Late Consequences of Acute Coronary Syndromes: Global Registry of Acute Coronary Events (GRACE) Follow-Up. Am. J. Med. 2015, 128, 766–775. [Google Scholar] [CrossRef]
- Jernberg, T.; Hasvold, P.; Henriksson, M.; Hjelm, H.; Thuresson, M.; Janzon, M. Cardiovascular Risk in Post-Myocardial Infarction Patients: Nationwide Real World Data Demonstrate the Importance of a Long-Term Perspective. Eur. Heart J. 2015, 36, 1163–1170. [Google Scholar] [CrossRef]
- Crimi, G.; Leonardi, S.; Costa, F.; Adamo, M.; Ariotti, S.; Valgimigli, M. Role of Stent Type and of Duration of Dual Antiplatelet Therapy in Patients with Chronic Kidney Disease Undergoing Percutaneous Coronary Interventions. Is Bare Metal Stent Implantation Still a Justifiable Choice? A Post-Hoc Analysis of the All Comer PRODIGY Trial. Int. J. Cardiol. 2016, 212, 110–117. [Google Scholar] [CrossRef]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.-L.T.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef] [PubMed]
- Yeh, R.W.; Kereiakes, D.J.; Steg, P.G.; Windecker, S.; Rinaldi, M.J.; Gershlick, A.H.; Cutlip, D.E.; Cohen, D.J.; Tanguay, J.-F.; Jacobs, A.; et al. Benefits and Risks of Extended Duration Dual Antiplatelet Therapy After PCI in Patients With and Without Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2015, 65, 2211–2221. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Valgimigli, M. Impact of Clinical Presentation on Dual Antiplatelet Therapy Duration. J. Am. Coll. Cardiol. 2015, 66, 1203–1204. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Bhatt, D.L.; Cohen, M.; Steg, P.G.; Storey, R.F.; Jensen, E.C.; Magnani, G.; Bansilal, S.; Fish, M.P.; Im, K.; et al. Long-Term Use of Ticagrelor in Patients with Prior Myocardial Infarction. N. Engl. J. Med. 2015, 372, 1791–1800. [Google Scholar] [CrossRef] [PubMed]
- Udell, J.A.; Bonaca, M.P.; Collet, J.-P.; Lincoff, A.M.; Kereiakes, D.J.; Costa, F.; Lee, C.W.; Mauri, L.; Valgimigli, M.; Park, S.-J.; et al. Long-Term Dual Antiplatelet Therapy for Secondary Prevention of Cardiovascular Events in the Subgroup of Patients with Previous Myocardial Infarction: A Collaborative Meta-Analysis of Randomized Trials. Eur. Heart J. 2015, ehv443. [Google Scholar] [CrossRef]
- Costa, F.; Adamo, M.; Ariotti, S.; Navarese, E.P.; Biondi-Zoccai, G.; Valgimigli, M. Impact of Greater than 12-Month Dual Antiplatelet Therapy Duration on Mortality: Drug-Specific or a Class-Effect? A Meta-Analysis. Int. J. Cardiol. 2015, 201, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Park, K.W.; Yoon, J.-H.; Kim, J.-S.; Hahn, J.-Y.; Cho, Y.-S.; Chae, I.-H.; Gwon, H.-C.; Ahn, T.; Oh, B.-H.; Park, J.-E.; et al. Efficacy of Xience/Promus versus Cypher in REducing Late Loss after StENTing (EXCELLENT) Trial: Study Design and Rationale of a Korean Multicenter Prospective Randomized Trial. Am. Heart J. 2009, 157, 811–817. [Google Scholar] [CrossRef]
- Valgimigli, M.; Campo, G.; Monti, M.; Vranckx, P.; Percoco, G.; Tumscitz, C.; Castriota, F.; Colombo, F.; Tebaldi, M.; Fucà, G.; et al. Short- Versus Long-Term Duration of Dual-Antiplatelet Therapy After Coronary Stenting: A Randomized Multicenter Trial. Circulation 2012, 125, 2015–2026. [Google Scholar] [CrossRef]
- Gargiulo, G.; Costa, F.; Ariotti, S.; Biscaglia, S.; Campo, G.; Esposito, G.; Leonardi, S.; Vranckx, P.; Windecker, S.; Valgimigli, M. Impact of Proton Pump Inhibitors on Clinical Outcomes in Patients Treated with a 6- or 24-Month Dual-Antiplatelet Therapy Duration: Insights from the PROlonging Dual-Antiplatelet Treatment after Grading Stent-Induced Intimal Hyperplasia StudY Trial. Am. Heart J. 2016, 174, 95–102. [Google Scholar] [CrossRef]
- Adamo, M.; Costa, F.; Vranckx, P.; Leonardi, S.; Navarese, E.P.; Garcia-Garcia, H.M.; Valgimigli, M. Does Smoking Habit Affect the Randomized Comparison of 6 versus 24-Month Dual Antiplatelet Therapy Duration? Insights from the PRODIGY Trial. Int. J. Cardiol. 2015, 190, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Vranckx, P.; Leonardi, S.; Moscarella, E.; Ando, G.; Calabro, P.; Oreto, G.; Zijlstra, F.; Valgimigli, M. Impact of Clinical Presentation on Ischaemic and Bleeding Outcomes in Patients Receiving 6- or 24-Month Duration of Dual-Antiplatelet Therapy after Stent Implantation: A Pre-Specified Analysis from the PRODIGY (Prolonging Dual-Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia) Trial. Eur. Heart J. 2015, 36, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Damen, S.A.; Camaro, C.; Benit, E.; Verdoia, M.; Rasoul, S.; Liew, H.B.; Polad, J.; Ahmad, W.A.; Zambahari, R.; et al. Final Results of the Randomised Evaluation of Short-Term Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome Treated with a New-Generation Stent (REDUCE Trial). EuroIntervention 2019, 15, e990–e998. [Google Scholar] [CrossRef]
- Vranken, N.P.A.; Rasoul, S.; Luijkx, J.J.P.; Pustjens, T.F.S.; Postma, S.; Kolkman, E.J.; Kedhi, E.; Rifqi, S.; Lee, M.K.Y.; Ebelt, H.; et al. Short-term Dual Antiplatelet Therapy in Diabetic Patients Admitted for Acute Coronary Syndrome Treated with a New-generation Drug-eluting Stent. Diabetes Metab. Res. Rev. 2022, 38, e3530. [Google Scholar] [CrossRef]
- Verdoia, M.; Suryapranata, H.; Damen, S.; Camaro, C.; Benit, E.; Barbieri, L.; Rasoul, S.; Liew, H.B.; Polad, J.; Ahmad, W.A.W.; et al. Gender Differences with Short-Term vs 12 Months Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome Treated with the COMBO Dual Therapy Stent: 2-Years Follow-up Results of the REDUCE Trial. J. Thromb. Thrombolysis 2021, 52, 797–807. [Google Scholar] [CrossRef]
- Kedhi, E.; Verdoia, M.; Suryapranata, H.; Damen, S.; Camaro, C.; Benit, E.; Barbieri, L.; Rasoul, S.; Liew, H.B.; Polad, J.; et al. Impact of Age on the Comparison between Short-Term vs 12-Month Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome Treated with the COMBO Dual Therapy Stent: 2-Year Follow-up Results of the REDUCE Trial. Atherosclerosis 2021, 321, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Ariotti, S.; Costa, F. Duration of Dual Antiplatelet Therapy after Drug-Eluting Stent Implantation: Will We Ever Reach a Consensus? Eur. Heart J. 2015, 36, 1219–1222. [Google Scholar] [CrossRef] [PubMed]
- Morici, N.; De Servi, S.; De Luca, L.; Crimi, G.; Montalto, C.; De Rosa, R.; De Luca, G.; Rubboli, A.; Valgimigli, M.; Savonitto, S. Management of Acute Coronary Syndromes in Older Adults. Eur. Heart J. 2022, 43, 1542–1553. [Google Scholar] [CrossRef] [PubMed]
- Montalto, C.; Crimi, G.; Morici, N.; Piatti, L.; Grosseto, D.; Sganzerla, P.; Tortorella, G.; De Rosa, R.; De Luca, L.; De Luca, G.; et al. Bleeding Risk Prediction in Elderly Patients Managed Invasively for Acute Coronary Syndromes: External Validation of the PRECISE-DAPT and PARIS Scores. Int. J. Cardiol. 2021, 328, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Campos, C.M.; Costa, F.; Garcia-Garcia, H.M.; Bourantas, C.; Suwannasom, P.; Valgimigli, M.; Morel, M.-A.; Windecker, S.; Serruys, P.W. Anatomic Characteristics and Clinical Implications of Angiographic Coronary Thrombus: Insights From a Patient-Level Pooled Analysis of SYNTAX, RESOLUTE, and LEADERS Trials. Circ. Cardiovasc. Interv. 2015, 8, e002279. [Google Scholar] [CrossRef] [PubMed]
- McAllister, K.S.L.; Ludman, P.F.; Hulme, W.; De Belder, M.A.; Stables, R.; Chowdhary, S.; Mamas, M.A.; Sperrin, M.; Buchan, I.E. A Contemporary Risk Model for Predicting 30-Day Mortality Following Percutaneous Coronary Intervention in England and Wales. Int. J. Cardiol. 2016, 210, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Zimarino, M.; Angiolillo, D.J.; Dangas, G.; Capodanno, D.; Barbato, E.; Hahn, J.-Y.; Giustino, G.; Watanabe, H.; Costa, F.; Cuisset, T.; et al. Antithrombotic Therapy after Percutaneous Coronary Intervention of Bifurcation Lesions. EuroIntervention 2021, 17, 59–66. [Google Scholar] [CrossRef]
- Giustino, G.; Costa, F. Characterization of the Individual Patient Risk After Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2019, 12, 831–834. [Google Scholar] [CrossRef]
- Caracciolo, A.; Mazzone, P.; Laterra, G.; Garcia-Ruiz, V.; Polimeni, A.; Galasso, S.; Saporito, F.; Carerj, S.; D’Ascenzo, F.; Marquis-Gravel, G.; et al. Antithrombotic Therapy for Percutaneous Cardiovascular Interventions: From Coronary Artery Disease to Structural Heart Interventions. J. Clin. Med. 2019, 8, 2016. [Google Scholar] [CrossRef]
- Costa, F.; Adamo, M.; Ariotti, S.; Ferrante, G.; Navarese, E.P.; Leonardi, S.; Garcia-Garcia, H.; Vranckx, P.; Valgimigli, M. Left Main or Proximal Left Anterior Descending Coronary Artery Disease Location Identifies High-Risk Patients Deriving Potentially Greater Benefit from Prolonged Dual Antiplatelet Therapy Duration. EuroIntervention 2016, 11, e1222–e1230. [Google Scholar] [CrossRef]
- Giustino, G.; Chieffo, A.; Palmerini, T.; Valgimigli, M.; Feres, F.; Abizaid, A.; Costa, R.A.; Hong, M.-K.; Kim, B.-K.; Jang, Y.; et al. Efficacy and Safety of Dual Antiplatelet Therapy After Complex PCI. J. Am. Coll. Cardiol. 2016, 68, 1851–1864. [Google Scholar] [CrossRef]
- Costa, F.; Van Klaveren, D.; Feres, F.; James, S.; Räber, L.; Pilgrim, T.; Hong, M.-K.; Kim, H.-S.; Colombo, A.; Steg, P.G.; et al. Dual Antiplatelet Therapy Duration Based on Ischemic and Bleeding Risks After Coronary Stenting. J. Am. Coll. Cardiol. 2019, 73, 741–754. [Google Scholar] [CrossRef]
- Costa, F.; Tijssen, J.G.; Ariotti, S.; Giatti, S.; Moscarella, E.; Guastaroba, P.; De Palma, R.; Andò, G.; Oreto, G.; Zijlstra, F.; et al. Incremental Value of the CRUSADE, ACUITY, and HAS-BLED Risk Scores for the Prediction of Hemorrhagic Events After Coronary Stent Implantation in Patients Undergoing Long or Short Duration of Dual Antiplatelet Therapy. J. Am. Heart Assoc. 2015, 4, e002524. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease Developed in Collaboration with EACTS. Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Van Klaveren, D.; James, S.; Heg, D.; Räber, L.; Feres, F.; Pilgrim, T.; Hong, M.-K.; Kim, H.-S.; Colombo, A.; et al. Derivation and Validation of the Predicting Bleeding Complications in Patients Undergoing Stent Implantation and Subsequent Dual Antiplatelet Therapy (PRECISE-DAPT) Score: A Pooled Analysis of Individual-Patient Datasets from Clinical Trials. The Lancet 2017, 389, 1025–1034. [Google Scholar] [CrossRef]
- Castelijns, M.C.; Hageman, S.H.J.; Teraa, M.; Van Der Meer, M.G.; Westerink, J.; Costa, F.; Ten Berg, J.M.; Visseren, F.L.J. External Validation of Bleeding Risk Models for the Prediction of Long-Term Bleeding Risk in Patients with Established Cardiovascular Disease. Am. Heart J. 2023, 260, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Munafò, A.R.; Montalto, C.; Franzino, M.; Pistelli, L.; Di Bella, G.; Ferlini, M.; Leonardi, S.; D’Ascenzo, F.; Gragnano, F.; Oreglia, J.A.; et al. External Validity of the PRECISE-DAPT Score in Patients Undergoing PCI: A Systematic Review and Meta-Analysis. Eur. Heart J. - Cardiovasc. Pharmacother. 2023, pvad063. [Google Scholar] [CrossRef]
- Costa, F.; Van Klaveren, D.; Colombo, A.; Feres, F.; Räber, L.; Pilgrim, T.; Hong, M.-K.; Kim, H.-S.; Windecker, S.; Steyerberg, E.W.; et al. A 4-Item PRECISE-DAPT Score for Dual Antiplatelet Therapy Duration Decision-Making. Am. Heart J. 2020, 223, 44–47. [Google Scholar] [CrossRef]
- Silverio, A.; Di Maio, M.; Buccheri, S.; De Luca, G.; Esposito, L.; Sarno, G.; Vecchione, C.; Galasso, G. Validation of the Academic Research Consortium High Bleeding Risk Criteria in Patients Undergoing Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis of 10 Studies and 67,862 Patients. Int. J. Cardiol. 2022, 347, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Frigoli, E.; Heg, D.; Tijssen, J.; Jüni, P.; Vranckx, P.; Ozaki, Y.; Morice, M.-C.; Chevalier, B.; Onuma, Y.; et al. Dual Antiplatelet Therapy after PCI in Patients at High Bleeding Risk. N. Engl. J. Med. 2021, 385, 1643–1655. [Google Scholar] [CrossRef]
- Valgimigli, M.; Cao, D.; Angiolillo, D.J.; Bangalore, S.; Bhatt, D.L.; Ge, J.; Hermiller, J.; Makkar, R.R.; Neumann, F.-J.; Saito, S.; et al. Duration of Dual Antiplatelet Therapy for Patients at High Bleeding Risk Undergoing PCI. J. Am. Coll. Cardiol. 2021, 78, 2060–2072. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Cao, D.; Makkar, R.R.; Bangalore, S.; Bhatt, D.L.; Angiolillo, D.J.; Saito, S.; Ge, J.; Neumann, F.-J.; Hermiller, J.; et al. Design and Rationale of the XIENCE Short DAPT Clinical Program: An Assessment of the Safety of 3-Month and 1-Month DAPT in Patients at High Bleeding Risk Undergoing PCI with an Everolimus-Eluting Stent. Am. Heart J. 2021, 231, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Montalto, C.; Branca, M.; Hong, S.-J.; Watanabe, H.; Franzone, A.; Vranckx, P.; Hahn, J.-Y.; Gwon, H.-C.; Feres, F.; et al. Dual Antiplatelet Therapy Duration after Percutaneous Coronary Intervention in High Bleeding Risk: A Meta-Analysis of Randomized Trials. Eur. Heart J. 2023, 44, 954–968. [Google Scholar] [CrossRef] [PubMed]
- Yaling Han Optimal AntiPlatelet Therapy for High Bleeding and Ischemic RISK Patients - OPT-BIRISK.; ESC Congress 2023 - Amsterdam, August 28 2023.
- De Caterina, R.; Agewall, S.; Andreotti, F.; Angiolillo, D.J.; Bhatt, D.L.; Byrne, R.A.; Collet, J.-P.; Eikelboom, J.; Fanaroff, A.C.; Gibson, C.M.; et al. Great Debate: Triple Antithrombotic Therapy in Patients with Atrial Fibrillation Undergoing Coronary Stenting Should Be Limited to 1 Week. Eur. Heart J. 2022, 43, 3512–3527. [Google Scholar] [CrossRef] [PubMed]
- Clopidogrel plus Aspirin versus Oral Anticoagulation for Atrial Fibrillation in the Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events (ACTIVE W): A Randomised Controlled Trial. The Lancet 2006, 367, 1903–1912. [CrossRef] [PubMed]
- Sørensen, R.; Hansen, M.L.; Abildstrom, S.Z.; Hvelplund, A.; Andersson, C.; Jørgensen, C.; Madsen, J.K.; Hansen, P.R.; Køber, L.; Torp-Pedersen, C.; et al. Risk of Bleeding in Patients with Acute Myocardial Infarction Treated with Different Combinations of Aspirin, Clopidogrel, and Vitamin K Antagonists in Denmark: A Retrospective Analysis of Nationwide Registry Data. The Lancet 2009, 374, 1967–1974. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Ten Berg, J.M.; et al. Optimal Antithrombotic Regimens for Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: An Updated Network Meta-Analysis. JAMA Cardiol. 2020, 5, 582. [Google Scholar] [CrossRef]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; Van Eickels, M.; et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.H.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef]
- Costa, F.; Valgimigli, M.; Steg, P.G.; Bhatt, D.L.; Hohnloser, S.H.; Ten Berg, J.M.; Miede, C.; Nordaby, M.; Lip, G.Y.H.; Oldgren, J.; et al. Antithrombotic Therapy According to Baseline Bleeding Risk in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: Applying the PRECISE-DAPT Score in RE-DUAL PCI. Eur. Heart J. -Cardiovasc. Pharmacother. 2022, 8, 216–226. [Google Scholar] [CrossRef]
- Andò, G.; Costa, F. Double or Triple Antithrombotic Therapy after Coronary Stenting and Atrial Fibrillation: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Cardiol. 2020, 302, 95–102. [Google Scholar] [CrossRef]
- Saglietto, A.; D’Ascenzo, F.; Errigo, D.; Leonardi, S.; Dewilde, W.J.; Conrotto, F.; Omedè, P.; Montefusco, A.; Angelini, F.; De Filippo, O.; et al. Antithrombotic Strategies in Patients Needing Oral Anticoagulation Undergoing Percutaneous Coronary Intervention: A Network Meta-analysis. Catheter. Cardiovasc. Interv. 2021, 97, 581–588. [Google Scholar] [CrossRef]
- Montalto, C.; Costa, F.; Leonardi, S.; Micari, A.; Oreglia, J.A.; Vranckx, P.; Capodanno, D.; Ten Berg, J.; Lopes, R.D.; Valgimigli, M. Dual Antiplatelet Therapy Duration after Percutaneous Coronary Intervention in Patients with Indication to Oral Anticoagulant Therapy. A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Heart J. -Cardiovasc. Pharmacother. 2023, 9, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Gragnano, F.; Branca, M.; Franzone, A.; Baber, U.; Jang, Y.; Kimura, T.; Hahn, J.-Y.; Zhao, Q.; Windecker, S.; et al. P2Y12 Inhibitor Monotherapy or Dual Antiplatelet Therapy after Coronary Revascularisation: Individual Patient Level Meta-Analysis of Randomised Controlled Trials. BMJ 2021, n1332. [Google Scholar] [CrossRef] [PubMed]
- Gragnano, F.; Mehran, R.; Branca, M.; Franzone, A.; Baber, U.; Jang, Y.; Kimura, T.; Hahn, J.-Y.; Zhao, Q.; Windecker, S.; et al. P2Y12 Inhibitor Monotherapy or Dual Antiplatelet Therapy After Complex Percutaneous Coronary Interventions. J. Am. Coll. Cardiol. 2023, 81, 537–552. [Google Scholar] [CrossRef]
- Marquis-Gravel, G.; Mehta, S.R.; Valgimigli, M.; Levine, G.N.; Neumann, F.-J.; Granger, C.B.; Costa, F.; Lordkipanidzé, M.; Roffi, M.; Robinson, S.D.; et al. A Critical Comparison of Canadian and International Guidelines Recommendations for Antiplatelet Therapy in Coronary Artery Disease. Can. J. Cardiol. 2020, 36, 1298–1307. [Google Scholar] [CrossRef]
- A Randomised, Blinded, Trial of Clopidogrel versus Aspirin in Patients at Risk of Ischaemic Events (CAPRIE). The Lancet 1996, 348, 1329–1339. [CrossRef] [PubMed]
- Chiarito, M.; Sanz-Sánchez, J.; Cannata, F.; Cao, D.; Sturla, M.; Panico, C.; Godino, C.; Regazzoli, D.; Reimers, B.; De Caterina, R.; et al. Monotherapy with a P2Y12 Inhibitor or Aspirin for Secondary Prevention in Patients with Established Atherosclerosis: A Systematic Review and Meta-Analysis. The Lancet 2020, 395, 1487–1495. [Google Scholar] [CrossRef]
- Kang, J.; Park, K.W.; Lee, H.; Hwang, D.; Yang, H.-M.; Rha, S.-W.; Bae, J.-W.; Lee, N.H.; Hur, S.-H.; Han, J.-K.; et al. Aspirin Versus Clopidogrel for Long-Term Maintenance Monotherapy After Percutaneous Coronary Intervention: The HOST-EXAM Extended Study. Circulation 2023, 147, 108–117. [Google Scholar] [CrossRef]
- Gragnano, F.; Cao, D.; Pirondini, L.; Franzone, A.; Kim, H.-S.; Von Scheidt, M.; Pettersen, A.-Å.R.; Zhao, Q.; Woodward, M.; Chiarito, M.; et al. P2Y12 Inhibitor or Aspirin Monotherapy for Secondary Prevention of Coronary Events. J. Am. Coll. Cardiol. 2023, 82, 89–105. [Google Scholar] [CrossRef]
- Pil-Ki Min P2Y12 Inhibitor Monotherapy vs DAPT after PCI with BP-EES: The SHARE Randomized Clinical Trial.; ESC Congress 2023 - Amsterdam, 26 August 2023.
- Kogame, N.; Guimarães, P.O.; Modolo, R.; De Martino, F.; Tinoco, J.; Ribeiro, E.E.; Kawashima, H.; Ono, M.; Hara, H.; Wang, R.; et al. Aspirin-Free Prasugrel Monotherapy Following Coronary Artery Stenting in Patients With Stable CAD. JACC Cardiovasc. Interv. 2020, 13, 2251–2262. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Jeong, Y.-H.; Yun, K.H.; Cho, J.Y.; Gorog, D.A.; Angiolillo, D.J.; Kim, J.W.; Jang, Y. P2Y12 Inhibitor Monotherapy Combined With Colchicine Following PCI in ACS Patients. JACC Cardiovasc. Interv. 2023, 16, 1845–1855. [Google Scholar] [CrossRef] [PubMed]
- Van Der Sangen, N.M.R.; Claessen, B.E.P.M.; Küçük, I.T.; Den Hartog, A.W.; Baan, J.; Beijk, M.A.M.; Delewi, R.; Van De Hoef, T.P.; Knaapen, P.; Lemkes, J.S.; et al. Single Antiplatelet Therapy Directly after Percutaneous Coronary Intervention in Non-ST-Segment Elevation Acute Coronary Syndrome Patients: The OPTICA Study. EuroIntervention 2023, 19, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Micari, A. Aspirin-Free Strategy After ACS Implementing Colchicine. JACC Cardiovasc. Interv. 2023, 16, 1856–1859. [Google Scholar] [CrossRef] [PubMed]
- Masahiro Natsuaki Short and Optimal Duration of Dual Antiplatelet Therapy After Everolimus-Eluting Cobalt-Chromium Stent-3 - STOPDAPT-3.; ESC Congress 2023 - Amsterdam, 26 August 2023.
Figure 1.
Antiplatelet therapy treatment pathways.
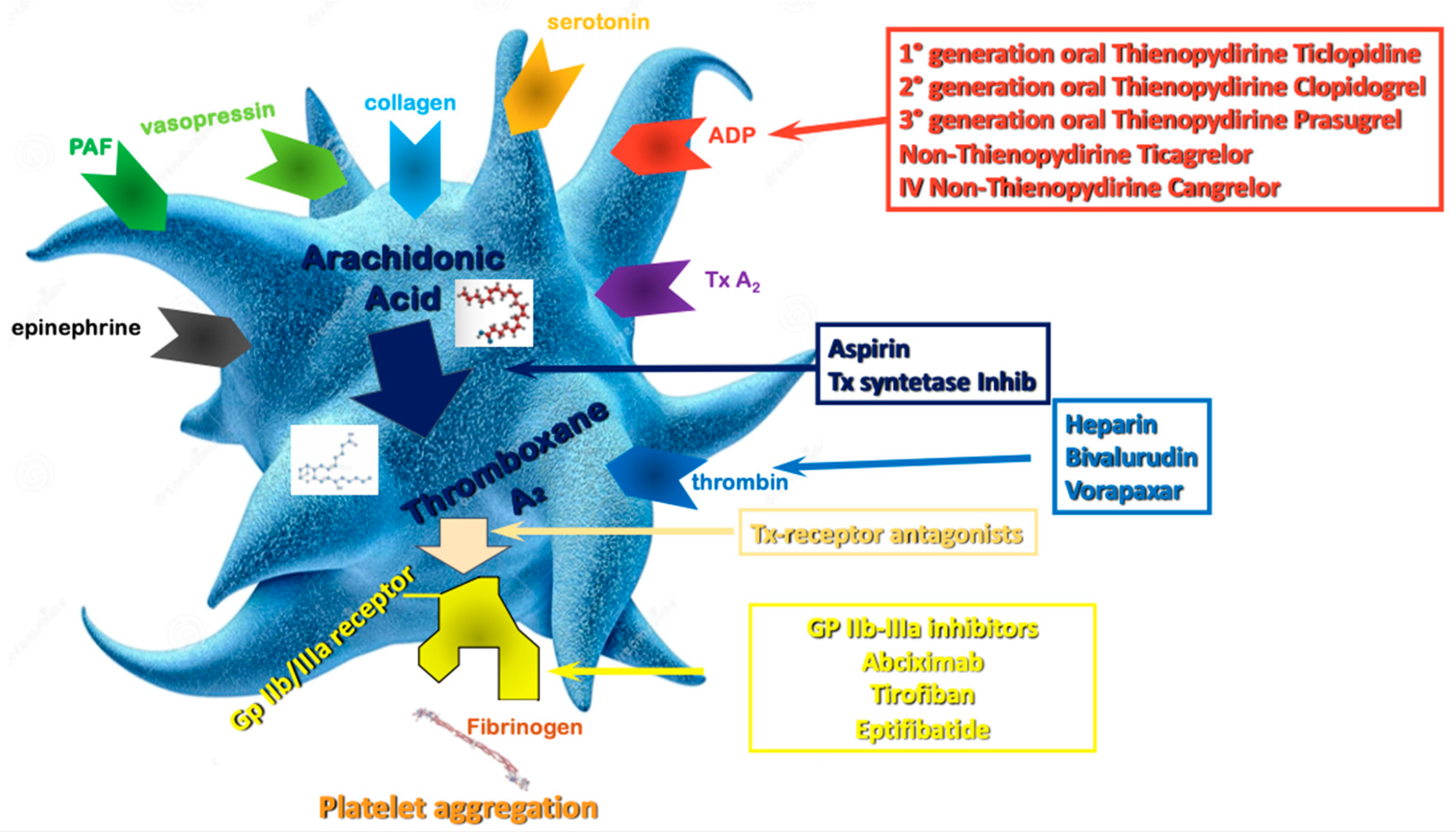
Figure 2.
Impact of potent vs. non-potent P2Y12 inhibitors in association with aspirin on non-CABG related TIMI major bleeding complications in patients with acute coronary syndromes. *Analysis restricted to patients < 75 years, without previous stroke, Weight > 60 kg.
Figure 2.
Impact of potent vs. non-potent P2Y12 inhibitors in association with aspirin on non-CABG related TIMI major bleeding complications in patients with acute coronary syndromes. *Analysis restricted to patients < 75 years, without previous stroke, Weight > 60 kg.
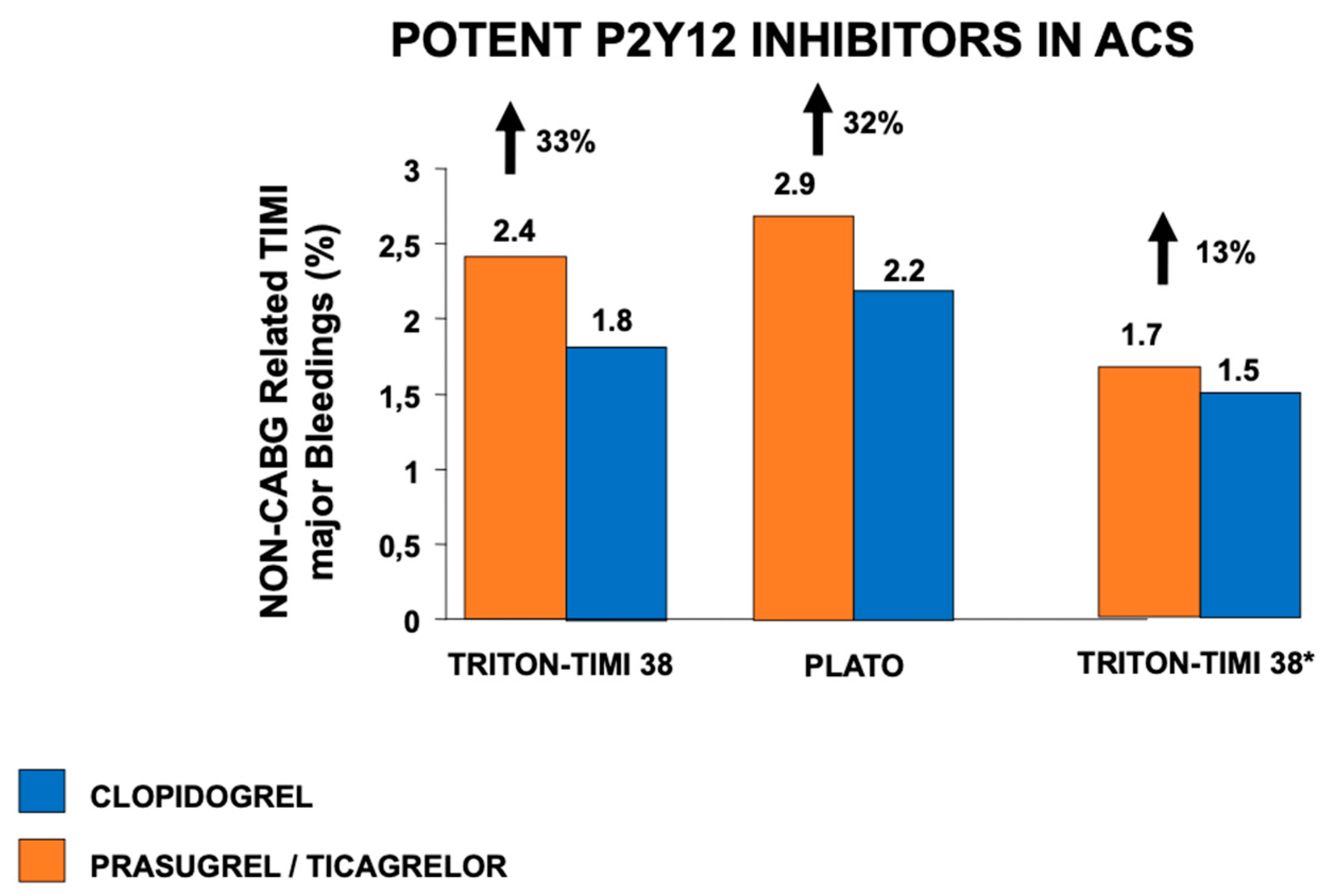
Figure 3.
Features informing individualization of antiplatelet therapy after percutaneous coronary intervention.
Figure 3.
Features informing individualization of antiplatelet therapy after percutaneous coronary intervention.
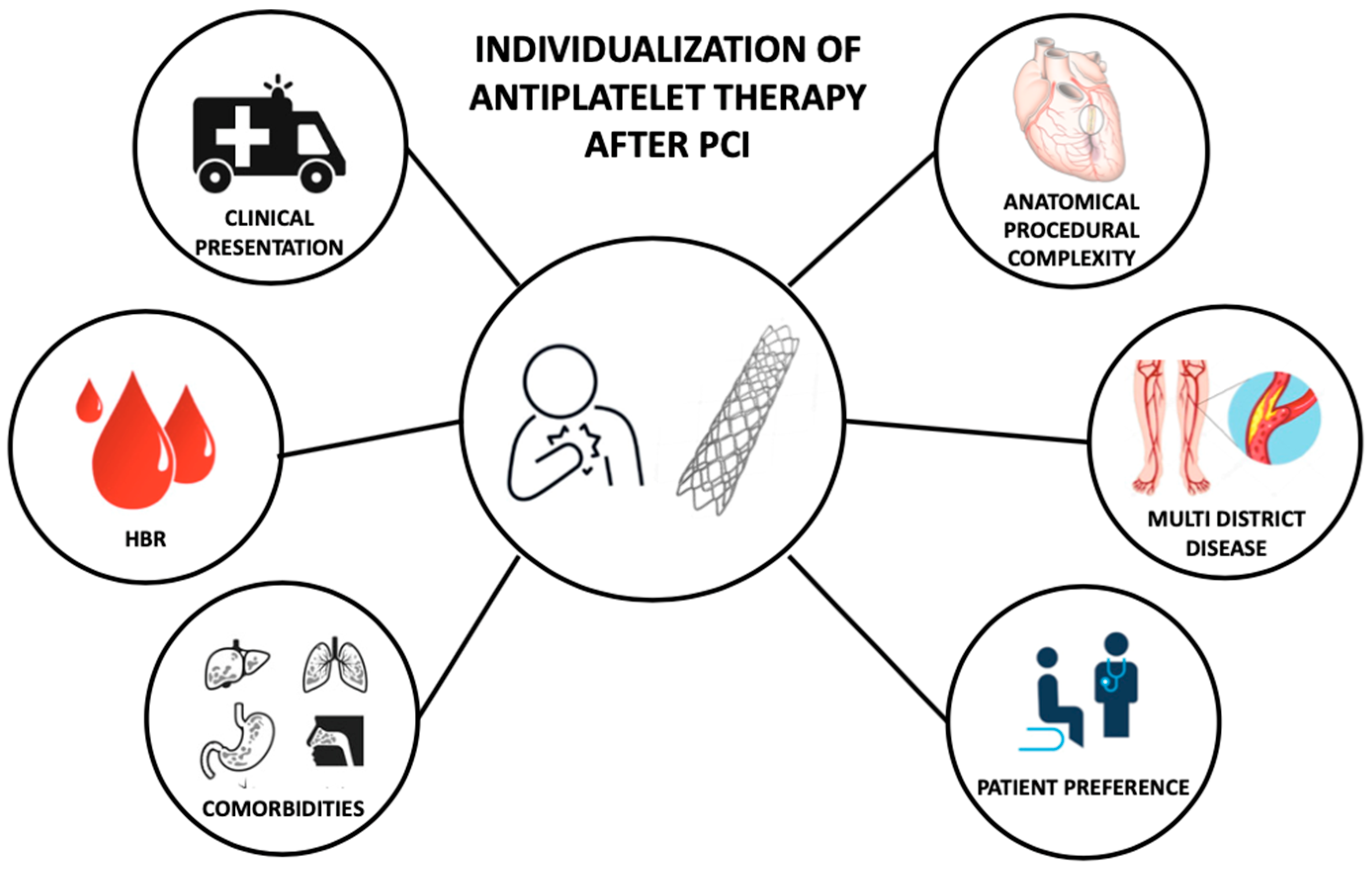
Figure 4.
Impact of abbreviated vs. standard dual antiplatelet therapy duration on clinical events in patients at high bleeding risk.
Figure 4.
Impact of abbreviated vs. standard dual antiplatelet therapy duration on clinical events in patients at high bleeding risk.
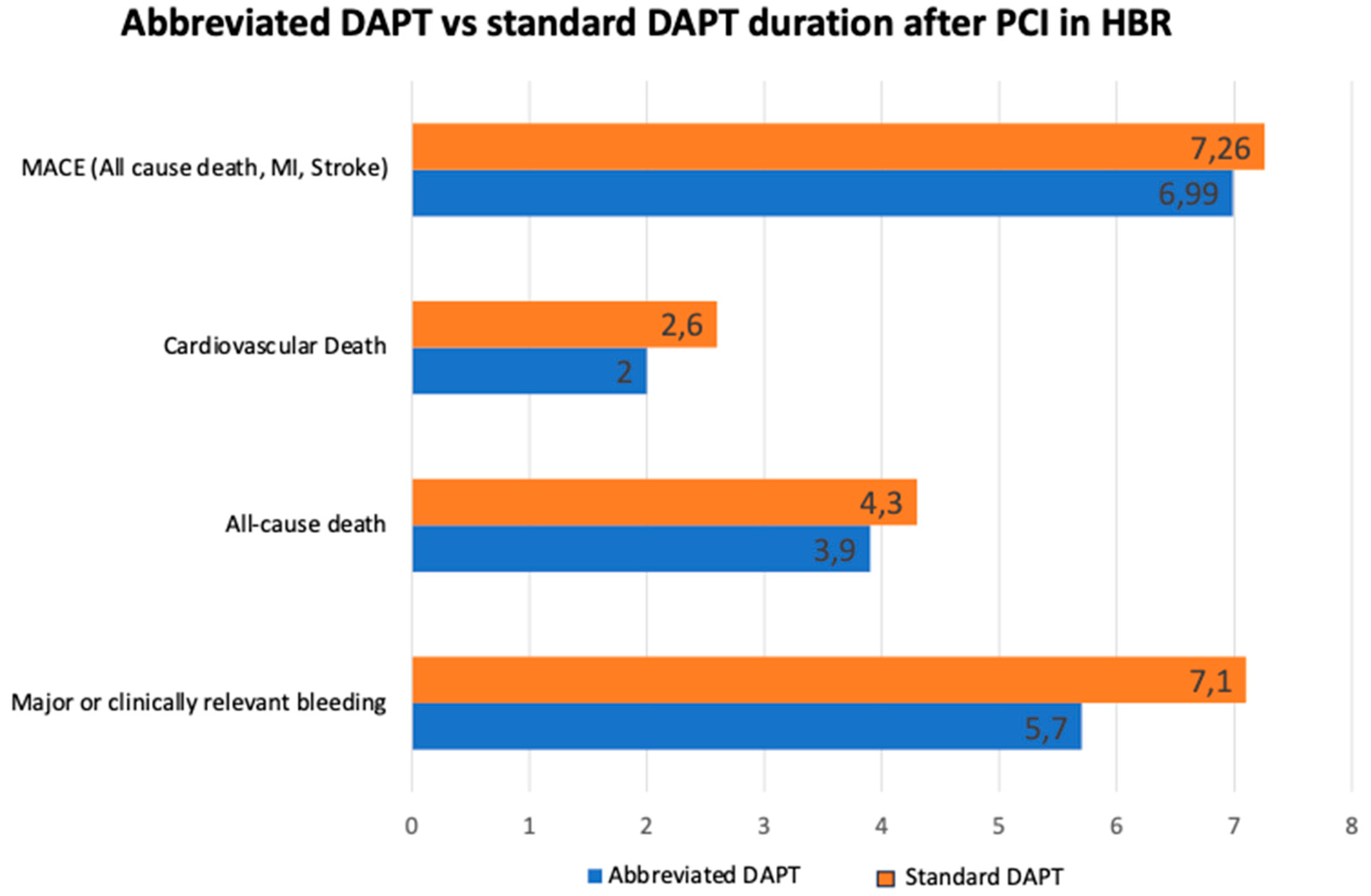
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



