
Submitted:
16 October 2023
Posted:
17 October 2023
You are already at the latest version
Abstract
Background: Neonatal transportation of sick newborns is a major predictor of outcome. Prompt identification of the sickest newborns allows immediate corrective intervention and outcome optimization. Multiple severity scores were developed, however an optimal score has not yet been identified. Aim: To identify a rapid, accurate, and easy to perform score predictive for neonatal mortality in outborn neonates. Material and methods: All neonates, irrespective of gestational age, admitted by transfer in our level III regional neonatal unit between 01.01.2015 and 31.12.2021 were included. Infants with congenital critical abnormalities were excluded. Sick neonatal score (SNS) was calculated and compared between survivors and non-survivors. Gestational age (GA), birth weight (BW), gender, Apgar score, place of birth, time between delivery and admission (AT), early onset sepsis were collected from medical records and compared between study groups. Subgroup analysis was performed based on gestational age (preterm versus term infants). A new score was elaborated, including GA, BW, and AT, namely MSNS-AT score, to further improve mortality prediction. The main outcomes were mortality prediction using SNS and MSNS-AT score. Univariable and multivariable analysis, including Cox regression, were performed using SPSS Statistic 22.0. P-value was considered statistically significant if <0.05, 95% confidence intervals, odds ratio and hazard ratios were calculated were appropriate. Results: A total of 418 outborn infants were admitted during study period; 15 infants were excluded due to critical congenital defects. Out of 403 outborn infants, 217 born prematurely (53.8%), 224 males (55.6%), 20 died (4.96%). Compared to the survivors, the non-survivor neonates had significantly lower GA, BW, and SNS score (p<0.05), although only SNS score remained significantly lower in all subgroups (preterm vs term infants). A SNS score ≤8 was associated with mortality both in the whole study group and in subgroups (p<0.001). Time to admission was significantly associated with increased mortality rate in the whole group (p<0.05) and in preterm infants but not in term ones (p>0.05). In univariable and multivariable Cox regression models, MSNS-AT score, with a cut-off optimal value of ≤10 was more precise in predicting mortality compared to SNS (AUC 0.735 vs. 0.775) when applied to the entire group, had a lower accuracy in the term infants (AUC 0.765 vs 0.809) and a better accuracy the preterm infants group (AUC 0.885 vs. 0.810). Conclusions: The MSNS-AT score – calculated by adding GA, BW, and AT to the SNS score - significantly improved mortality prediction at admission in the whole study group as compared to SNS score. The best accuracy prediction of MSNS-AT score was observed in preterm infants suggesting that, besides GA and BW, TA may be decisive for the outcome of outborn preterm infants. Further studies are necessary to confirm the predictive value of MSNS-AT score and to identify variables that can improve its value in term infants without affecting the simplicity, ease, and rapidity of the scoring system.
Keywords:
newborn
; outborn
; sick neonatal score
; mortality
; neonatal transportation
; scoring system
1. Introduction
One of the targets of World Health Organization (WHO)’s Millennium Development Goal (MDG) is the reduction of the under-five years of age mortality by two thirds [1]. Neonatal mortality represents a significant part of under-five mortality, reducing neonatal mortality rate is a key factor for reaching the MGD goal as a recent WHO report underlines that neonatal mortality rate, both globally and in Romania, did not show a similar significant decline as global child mortality from 2015 to 2019 [2].
Neonatal mortality rate is an important indicator of health and economical status of a nation [3]. Most neonatal deaths occur within the first 7 days of life. Delayed neonatal transportation and inefficient care during transfer are significant risk factors for neonatal mortality [4,5,6]. Neonatal transportation of sick newborns is a major predictor of outcome. This fact is often neglected in low- and middle-income countries [6,7], as it is in Romania. In utero transportation of high-risk pregnancies according to regionalization of the maternal and neonatal care is the safest option for both maternal and neonatal outcomes [8,9,10,11]. Unfortunately, preterm delivery and delivery of sick neonates are not always easy to anticipate and will continue to occur at lower level institutions and even at home. Efforts to improve neonatal stabilization pre-transport, neonatal care during transport, and the neonatal transport system itself - organization, training, equipment - are challenging in many countries. Outborn neonates are facing significantly higher morbidity and mortality rates [8,11,12].
Early recognition of sick neonates, optimal resuscitation if needed, prompt recognition and immediate competent interventions are needed to treat hypoglycaemia, seizures, and respiratory distress, prevention and treatment of hypothermia, hypoxia, hypotension, adequate monitoring before and during neonatal transport, and rapid transfer are extremely important for optimization of neonatal outcome [5,8,9,13,14,15,16]. A regionalized, specialized neonatal transport system may reduce neonatal complications and improve survival rates [11,14,17,18]. For many years now, clinicians have tried to evaluate the outborn infants at admission in order to identify and promptly address all complications that may impact their prognosis as the severity of the disease was described as an important prediction factor for mortality in newborn infants [19,20,21]. Severity scores were developed accordingly, including clinical and laboratory parameters, with different utilities and results in predicting mortality and morbidity rates [22]. Also, not all these scores can be applied in resource-limited areas. However, an optimal score has not yet been identified, and it may still be challenging to do so. This is because the validation of these scores has not shown the same level of sensitivity and specificity across various neonatal populations, regions, countries, and units. Additionally, there are many organizational differences between national maternal and neonatal care, regionalization, and neonatal transport systems [5,23,24,25]. An ideal score – or predictive model for the severity of the disease - should be easy, applicable early after admission, needing a minimum of invasive procedures, reproducible, with a good ability to predict mortality and specific morbidities and to discriminate between neonates with different outcomes [9,21,22,25,26,27,28]. Also, these predictions allow better planning and usage of resources of care, improvements of neonatal care before and during transport, cost analysis, evaluation of the care quality, comparisons between neonatal units, research, and parental counselling [22,25,26,27,28,29].
Organization of the Romanian neonatal transport system started in 2004, immediately after regionalization of the maternal and neonatal care in 2002, but still lacks, in many parts of the country, trained, specialized staff and special equipment. Considering the improved rates of survival at lower gestational ages, and insufficient number of beds in neonatal intensive care units (NICU), we face a continuous need for better critical neonatal care as survival is not anymore the ultimate goal of NICU care. Based on a prospective cohort, using the sick neonatal score (SNS) [14,30], and statistical models, the aim of our study was to identify a rapid and easy to perform score predictive for neonatal mortality in newborns submitted to our unit after delivery.
2. Materials and Methods
The study included all neonates (N = 418), irrespective of gestational age, admitted by transfer in level III regional neonatal unit of the Clinical County Emergency Hospital Sibiu, Romania between 01.01.2015 and 31.12.2021. Newborns with critical congenital defects (N = 15) were excluded. Neonatal and NICU charts were used to extract data. Sick neonatal score was calculated for every newborn using the criteria suggested by Rathod et al. [30] (Table 1) but using the first blood glucose and rectal temperature at admission. We also collected data as regards gestational age (defined using either the best obstetrical estimate based on first trimester ultrasound, or the date of the last menstrual cycle), birth weight, gender, the time between delivery and arrival to our unit (in hours), Apgar score at 1 minute, diagnosis of early onset sepsis, and place of birth (defined home delivery, delivery at level I, II, or III neonatal units). Per protocol unit, all these data must be completed by physicians in neonatal records. Outborn infants (403 included in the final analysis) were classified into two groups – survivors and non-survivors - according to the primary outcome, mortality. Subgroup analyses were performed, as the study group was also classified according to gestational age in preterm (N = 217) and term infants (N = 186), respectively. All the collected variables, including SNS score, were compared between infants who survived at discharge from the maternity hospital and those who died.
Prematurity was defined as birth occurring before completing 37 weeks of gestation. Blood glucose levels were measured using a blood gas analyzer. The first reading was used to calculate the SNS. An electronic thermometer was used to measure rectal temperature at admission. Respiratory effort and capillary refill time evaluated, scored, and noted by physicians at admission were used for SNS calculation; heart frequency and peripheral oxygen saturation were read and registered on pulse oximeter also at admission, in room air. Non-invasive mean blood pressure measurement was measured upon admission and used for SNS calculation.
Since most of the continuous variables didn’t have normal distribution they were presented both as median (and standard deviation) and as median (interquartile range) but compared with the Mann-Whitney U test. Spearman’s coefficient of correlation was used to highlight relationships between variables. Categorical variables were presented as counts (percentages) and compared with Pearson chi-square test. Receiver’s operating characteristics (ROC) curves were used to calculate the area under the curve (AUC) for each independent continuous variable and to establish optimal cut-off points. They are presented along with their sensitivity and specificity values. Survival analysis was conducted using Kaplan-Meyer curves, which consisted of presenting the survival curves and rank log-rank test, and through univariable and multivariable Cox proportional hazards model (Cox regression). In order to evaluate the goodness-of-fit for each model and to establish hierarchies we saved the hazard function for each Cox regression model performed and tested if the hazard probabilities match the outcome by running the ROC curves. The AUC of each model was indicative for its accuracy in outcome prediction. Confidence intervals of 95% were presented for AUC, and hazard ratios (HR). P value <0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS version 22.0.
3. Results
3.1. Group and subgroup analysis
The study group consisted of 418 newborns submitted to our unit during the study period; 15 of them were excluded from the analysis since they had been transferred due to severe congenital abnormalities; 224 (55.6%) males; 20 neonates died before discharge (4.96%). The number of transfers decreased significantly after 2017 and is presented in Figure 1. The baseline characteristics of the study group and subgroups based on gestational age are presented in Table 2.
At first, we wanted to validate SNS in our cohort, not only to the entire cohort but also in subgroups based on gestational age, and the results are presented in Table 3 and Table 4. A comparison between the baseline characteristics of the survivors and non-survivors showed that infants that died had significantly lower gestational age, birth weight, and SNS scores when the analysis was performed for the entire group and for the preterm infants group (Table 3). In the meantime, we used Mann-Whitney T to verify associations between the collected variables identified in the literature as important factors predictive of mortality rate: gestational age, birth weight, time duration between birth and admission to our unit, birth asphyxia (as reflected by an Apgar score at 1 minute), and early onset sepsis diagnosis (Table 4). All comparisons were performed in search of variables with the most significant impact on mortality in our population. The study found that mortality rates were significantly linked to gestational age and birth weight for the overall group, but not for preterm and term infants separately. Time of admission was a significant factor for mortality in both preterm infants and the overall group, while a lower Apgar score at 1 minute and a lower SNS score were significantly associated with mortality across all groups. (Table 3, 4). No associations were found for gender, Apgar score <3 at 1 minute, and early sepsis (Table 4). Most of the infants who died, especially premature infants, were transferred from level II neonatal units (Table 5).
3.2. SNS score to predict mortality
A ROC curve was performed to establish cut-off points for the time duration between birth and admission, which was found to be significantly associated with mortality. The area under the curve (AUC) was 0.664, p = 0.013. The optimal cut-off point for the time to admission variable was 6.5 hours (sensitivity 85%, specificity 54%). Consequently, the patients were separated into two groups based on the cut-off point and a Kaplan Meyer curve and a log test were done; these tests showed significant differences in survival between newborns admitted before and after 6.5 hours after birth (log-rank test: that χ2=16.395; p<0.001) (Figure 2A). Univariable and multivariable Cox regression indicated that time to admission over 6.5 hours (hazard ratio (HR): 14.009; CI 95%: 3.794-51.724; p<0.001) and SNS score (HR: 0.664, CI 95%: 0.574-0.769; p<0.001) are predictive for mortality outcome; adjustments for birth weight and gestational age were made in multivariable analysis. When time to admission was added to the SNS score in multivariable Cox regression we concluded that death HR became more accurate (AUC 0.808 vs 0.717)(Figure 2B). These results encouraged us to include time to admission in a modified scoring system, along with gestational age and birth weight, in our attempt to improve the mortality prediction in our population and settings.
3.3. Use of an improved SNS score for predicting mortality
In order to evaluate the inclusion of time-to-admission on survival rates we tried to modify SNS score to include the three variables with significant impact on mortality in our study group. We classified patients into three different groups based on the time-to-admission value: patients admitted in less than 6 hours after birth were classified as early admitted; patients admitted between 6-12 hours were considered intermediately admissions and those admitted after ≥12 hours were late admissions. Kaplan-Meyer curve and log-rank test showed significant differences in survival between these groups (χ2(2) =14.679; p=0.001). A scoring system was established for each of these groups based on the results of Cox regression coefficients. Compared with the intermediate group (6-12 hours), patients early admitted had a 1,347 higher survival rate, while compared to late admissions (≥13 hours.) survival rate was 3.278. Therefore, in the new scoring system, time-to-admission was grated 3 points for early admission, 1 point for intermediate admission, and 0 points for admissions after 13 hours. Additionally, we added gestational age and birth weight into the scoring system, using the same evaluation as in the Modified SNS (Table 6). Consecutively, we calculated a Modified SNS-Admission Time score (MSNS-AT score) for all our patients by adding the values for the three new variables to SNS scores. Ultimately, we compared the performance of MSNS-AT score with the SNS scoring system for the entire group and for subgroups based on gestational age.
The mean MSNS-AT score (SD) was 13.6 (3.3) in preterm infants, 16.7 (2.4) in term infants, and 15.0 (3.3) for the entire study group. A significantly higher median MSNS-AT score (interquartile range) was found in preterm infants and in the entire group that survived as compared to those who died (14.0 (2.9) vs. 7.2 (2.0); p <0.001 and 15.3 (3.0) vs. 9.5 (4.1); p <0.001 respectively). The difference had limited significance in term infants (16.8 (2.4) vs. 14.8 (2.5); p = 0.050). Mann-Whitney U test showed a significant association of MSNS-AT with mortality only in preterm infants (median score 14, IQR 11-16; p = 0.042 in preterm infants; median 17 (IQR 15-18 in term infants, and 16 (13-17) in the whole group, p>0.50 for both). However, an MSNS-AT score ≤10 demonstrated a statistically significant association with risk of death in the subgroups and in the entire group when survivors were compared to non-survivors: an MSNS-AT score ≤10 was found in 21 survivors (10.3%) vs. 14 non-survivors (100%) in the preterm infants (p<0.001); in 3 survivors (1.7%) vs 1 non-survivor (16.7%) in the term infants group (p = 0.003; OR 9.1 [95%CI 1.25-61.13]), and in 24 survivors (6.3%) and 15 non-survivors (75%) in all patients (p<0.001, OR 28.0 [10.7-72.89]).
The performance of the two scoring systems – SNS and MSNS-AT – was assessed by comparing the hazard probabilities of each multivariable model containing the scoring variable as a component and additional variables – gestational age, birth weight, time from birth to admission, Apgar score < 3 at 1 minute, early onset sepsis. Hazard probabilities were compared with ROC and accuracy was determined by AUC for each model (Table 7). We found that our modified scoring system is more precise in predicting mortality compared to SNS (AUC 0.735 vs. 0.775) when applied to the entire group, irrespective of gestational age, and had a lower accuracy in the term infants (AUC 0.765 vs 0.809). The best accuracy for the prediction of mortality was found for both scoring systems in the preterm infants group but, again, the MSNS-AT score performed better than the SNS score (AUC 0.885 vs. 0.810) (Figure 3A–C).
3.4. Evaluation of mortality risk with MSNS-AT score
In order to evaluate the risk of death using the MSN-AT score, we classified our patients based on the value of their MSNS-AT score. The first group had MSNS-AT scores ≤7, the second one comprised patients with scores between 8 and 15, and the last group had MSNS-AT scores ≥16 points. The Kaplan-Meyer curve was used to highlight differences in survival rates between groups. Significant survival disparities were found between the three groups classified according to MSNS-AT score (log-rank test: χ2(2) =58.390; p<0.001). Multivariable Cox regression showed that each group had a different risk of death, with the third group (MSNS-AT≥16) having the smallest risk of mortality (Figure 4). Cox proportional hazards model showed that compared with the third group, the second one (MSNS-AT 8-15) had higher mortality (HR: 3.607; CI 95%: 1.023-14.653; p=0.048) and the first group (MSNS-AT ≤7) has the highest mortality rate (HR: 47.120; CI 95%: 9.593-231.459; p<0.001); adjustments for birthweight, gestational age, time to admission, Apgar score at 1 minute, Apgar score under 3 and early onset sepsis were made in multivariable analysis (Table 8).
4. Discussion
One of the objectives of the World Health Organization's (WHO) Millennium Development Goal (MDG) is to reduce under-five mortality by two-thirds. This includes a significant reduction in neonatal mortality, as it accounts for a large portion of under-five mortality. Despite the fact that global child mortality rates decreased by almost 50% between 2000 and 2019, the neonatal mortality rates did not decline as much, according to a recent report. In Romania, the neonatal deaths declined from 884 (815-953) in 2015 to 690 (556-842) in 2019, the neonatal mortality rate reported in 2019 being 3.98 while the goal for 2030 is set at 3.17 [2]. Neonatal mortality is a serious concern as it reflects the health and economic status of a nation [3].
Regionalization of maternal and neonatal care and in-utero transportation of high-risk pregnancies to neonatal units with adequate resources and experience is the safest option for the best outcome both for mothers and newborns [6,7,8,9,10,11]. However, preterm births and delivery of sick infants are not always predictable and these situations will continue to occur worldwide at lower-level institutions and even at home. It is estimated that in 50% of the high-risk pregnancies in utero transportation is practically impossible [1]. On the other hand, 40% of neonatal deaths occur in the first day of life [30] and 75% in the first 7 days of life [27,31]. Delayed neonatal transfer, inadequate stabilization before transport, and deficient care during transportation are recognized as important risk factors for neonatal mortality and morbidity [5,6,32]. Experts consider neonatal transport between medical institutions as part of neonatal intensive care and a major outcome predictor for sick neonates [33]. Early recognition of sick neonates, optimal resuscitation if needed, prompt recognition and treatment of hypoglycaemia, seizures, and respiratory distress, prevention of hypothermia, hypoxia, hypotension, adequate monitoring before and during neonatal transport, rapid transfer are often challenging but extremely important for optimization of neonatal outcomes [5,8,9,13,14,15,16,30,34]. Efforts to improve neonatal stabilization pretransport, neonatal care during transport, and the neonatal transport system itself - organization, training, equipment - are challenging in many countries but mandatory for decreasing neonatal morbidity and mortality rates as data in the literature shows that outborn neonates are facing significantly higher morbidity and mortality rates [8,11,12]. Also, the regionalized, specialized neonatal transport system can reduce neonatal complications and improve survival rates [11,14,17,18]. However, neonatal transport of sick neonates is often neglected in low- and middle-income countries [7], as it is in Romania.
Regionalization of maternal and neonatal care started in Romania in 2002 with a first normative act establishing the criteria differentiating between level I, II, and III (the highest) maternity hospitals [35,36]. In 2004, the Romanian Ministry of Health issued another order for experimental organization of three specialized neonatal transportation units [36,37]. Criteria for regionalization of maternal and neonatal care were changed through normative governmental normative acts in 2009, and 2011, and another change is pending final approval by the end of this year [38]. For the future, five levels of maternity hospitals have been proposed. Neonatal transport has been neglected, so a new norm has been implemented stating that each level III unit may have a special neonatal ambulance. This comes with special financial support from the National Recovery and Resilience Plan. In 2011, the Romanian Association of Neonatology developed a national guideline for pre-transport stabilization and transport of newborns [36]. According to current regulations, level I neonatal units must transfer all infants with a birth weight less than 2500g, even healthy ones and all sick infants, to higher levels. Level II units can care for infants with a birth weight greater than 1500g and/or a gestational age greater than 32 weeks, as long as they do not require mechanical ventilation or other invasive procedures. All other newborns must be transferred to level III units [35,39]. Our study group included 403 neonates after the exclusion of 15 infants submitted for severe congenital abnormalities, a rather large group of patients compared to most of the studies searching or evaluating a scoring system for the severity of the disease [20,26,27,28,29,30,40,41,42,43]. Out of the 403 infants in the study group, 217 were preterm infants (53.8%); 20 of the infants died, the fatality rate being 4.96%. Our maternity unit, part of an emergency county hospital, has been a level III regional maternal-neonatal unit since 2002, receiving between 70-90 outborn infants/year from one level II maternity hospital, 6 level I units, and after-delivery at home. The furthest inferior level I canter is situated at 161 km, a trip of around 2 and a half hour by car. As shown in Figure 1, a significant drop in the number of submissions occurred after 2017, mostly due to an increased number of in-utero transfers. Increased awareness of high-risk pregnancies and its potential effects on maternal and neonatal outcomes leading to increased addressability of pregnant women directly to our center is another possible explanation. Covid-19 restrictions may have been added in 2020 and 2021.
Many authors [22,30,43,44,45,46] evaluated scoring systems separately for term and preterm infants, as gestational age and birth weight are recognized factors with significant impact on neonatal mortality. We had done the same, performing all the analysis on the entire group and in two subgroups based on gestational age – preterm and term infants. Some similarities and differences were noted starting the analysis of the baseline characteristics (Table 2): boys were slightly overrepresented in all three groups (over 50%), the proportions of infants with Apgar score <3 at 1 minute were almost equal in the groups, and most of the infants from each category were transferred from level I units. A subsequent diagnosis of early-onset sepsis was more often seen in term infants as compared to preterm ones (40.3% vs. 17.1%), preterm infants were more rapidly transferred as compared to term infants (mean duration 17.3±65.0 vs. 27.0±32.4 hours), and death occurred more often in preterm infants (6.5% vs. 3.2%)(Table 2). Based on the regionalization of maternal and neonatal care, it is common for preterm infants to be taken to higher-level neonatal units. Since many of these infants face challenges transitioning to life outside the womb, this outcome is not surprising. Additionally, the delayed appearance of sepsis symptoms in term infants may be another explanation (also for delayed referral of term infants) but we did not collect data on transfer reasons and why term infants were transferred later than preterm infants.
Starting the 1990s, clinicians have struggled to find an objective, rapid tool to evaluate the severity of the disease in newborns, especially in outborn infants, as the severity of the disease was described as an important factor for neonatal morbidity and mortality [19,20,21,22] and neonatal transfer after delivery was found as a risk factor for increased morbidity and mortality in outborn infants as compared to inborn infants [12,32,47,48,49,50,51,52]. Many severity system scorings were developed, some based on clinical knowledge, some based on strong statistical associations between different clinical and laboratory variables and outcomes. A number of problems have been cited related to almost all the scoring systems existing at this moment in relation to what is expected from an ideal severity score. A perfect severity score, or predictive model for the severity of a disease, should be easily defined and applicable soon after admission. It should require minimal invasive procedures, be reproducible, and have a solid ability to predict mortality and specific morbidities. Additionally, it should be able to distinguish between neonates with varying outcomes [21,22,25,26,27,28,34]. All such scoring systems need accurate validation in reasonably large data sets, calibration, tests for their discrimination capacity (scores with AUC >0.8 are useful in practice), reproducibility, and capacity to avoid biases [25]. Scores such as CRIB, CRIB II, SNAP, SNAP-PE, SNAP II, SNAPPE II, TISS and NTISS, NICHHD, NMPI, NBRS, TOPS, TRIPS, MINT, Prem or Berlin score, Sinkin score are complex scores, with different power to predict mortality, either comprising multiple parameters, either designed for a specific population (eg. preterm infants) or special situation [3,9,11,19,20,22,25,35,36,43,44,45,46,50,51,52,53,54,55]. We had chosen the sick neonate score (SNS) score, a score initially developed by Hermansen in 1994 [42] and modified by Rathod et al [30] since this score was validated both in high-income countries and in a resource-limited countries [30,42] and, after exclusion of pH and partial oxygen pressure from Hermansen score, didn’t need any invasive procedure. Also, in many studies a SNS score ≤8 has been validated as a cut-off value for predicting mortality [29,30,56]. We calculated the SNS score (Table 2) using rectal temperature instead of axillary temperature since it is more accurate. The mean values of SNS score were comparable between study groups (10.0±2.6 in preterm infants, 11.8±2.2 in term infants, and 10.8±2.6 in the whole group). Significantly lower SNS scores were found when we compared the survivors and non-survivors in all study groups (comparison of median (IQR) values in Table 4; all p<0.05) but the SNS cut-off value ≤8 was associated with death only in preterm infants and the entire study groups (Table 5). We believe that the nonsignificant association of this cut-off value in term infants is due to the low number of term infants who died.
The next step was finding new variables easy to use for the SNS score in order to improve its ability to predict mortality in all neonatal populations. Lower gestational age and birth weight were repeatedly demonstrated as associated with an increased risk of death, therefore we used them for the development of a new scoring system, the same as other authors [5,26,27,28,57]. Gender, early onset sepsis diagnosis, and asphyxia (defined as an Apgar score <3/1 minute) showed no association with mortality (p>0.05) in statistics (Table 4 and Table 5). A clinical observation during the years was that infants submitted rapidly after delivery have a better course, therefore we tried to statistically analyse the prediction power of time to admission upon the mortality rate and the statistical analysis confirmed: time to admission was significantly associated with mortality in preterm infants and in the whole group (Table 4) and a duration of 6.5 hours between birth and admission into our unit had an AUC of 0.664, p 0.013, the sensitivity of 85% and specificity of 54% in predicting mortality (Figure 2). Mori et al. found that neonatal transport duration over 90 minutes is associated with a two times higher risk of death [58]. A new scoring model was designed (Table 6) using the SNS score and new variables; gestational age, birth weight, and time to admission, and we named it MSNS-AT. Evaluation of MSNS-AT scores in our study groups was encouraging. MSNS-AT score ≤10 demonstrated a statistically significant association with risk of death in the subgroups and in the entire group, was found in 21 survivors (10.3%) vs. 14 non-survivors (100%) in the preterm infants (p<0.001); in 3 survivors (1.7%) vs 1 non-survivor (16.7%) in the term infants group (p = 0.003; OR 9.1 [95% CI 1.25-61.13]), and in 24 survivors (6.3%) and 15 non-survivors (75%) in all patients (p<0.001, OR 28.0 [95% CI 10.7-72.89]). The results are comparable with those using MSNS to predict mortality. Padar et al [26] found that a cut-off value of 10 predicted mortality with a sensitivity of 88.24%, and sensibility of 92.5% in 248 neonates evaluated at birth and at 24 hours of life. A mean score of 9.11 was found in non-survivors as compared to 12.9 survivors in a group of 71 newborns of which 80% were term infants in a study published by Reddy et al [27]. A bigger study performed by Mansoor et al [57], including 585 neonates, both inborn and outborn infants, found a mean score of 8.2±2.96 in deceased newborns vs. 13.1±2.4 in survivors, while the cut-off value of 10 had 90% sensitivity and 88% specificity for predicting mortality. The same cut-off value predicted death with 85.9% sensitivity and 51.1% specificity in another recent study of 355 neonates but identified that better prediction of mortality can be done using a cut-off value of 8 [28]. Adding time to admission to our score, we expected that the mean MSNS-AT would be higher compared to MSNS but we still found significant differences in the score between survivors and non-survivors in preterm infants and for the entire group; 14.0±2.9 vs. 7.2±2.0; p <0.001 and 15.3±3.0 vs. 9.5±4.1; p <0.001 respectively. Limited significance was found in term infants (16.8±2.4 vs. 14.8± 2.5; p = 0.050), probably because most term infants arrived significantly later at our unit.
Finally, MSNS-AT score was tested for accuracy in all the study groups, adjusting for gestational age, birth weight, Apgar score <3, and early onset sepsis rate, and in comparison with SNS score (Table 7, Figure 3 and Figure 4) and we found that this new score has the better performance in predicting mortality vs. SNS score in the whole group, irrespective of gestational age (AUC 0.735 vs. 0.775) and performed even better in preterm infants (AUC 0.885 vs. 0.810). A lower accuracy was found in term infants (MSNS-AT AUC 0.765 vs. SNS AUC 0.809). Another analysis has shown that a cut-off value ≤7 accurately predicted death in 58.1% of the infants in the study group while only 1.4% of infants with values >16 have died.
Severity scores were developed accordingly, including clinical and laboratory parameters, with different utilities and results in predicting mortality and morbidity rates [22]. Also, not all these scores can be applied in resource-limited areas. Still, an ideal score was not identified and this may be difficult even now since validation of various scores hasn’t demonstrated the same sensibility and specificity in different neonatal populations, from different regions, countries, and neonatal units, with so many organizational differences between national maternal and neonatal care regionalization and neonatal transport systems [5,23,25]. Currently, no unique mathematical formula can completely capture the complex clinical neonatal process, regardless of the accuracy of the scoring system, according to some experts [5].
But these predictions allow better planning and usage of resources of care, improvements of neonatal care before and during transport, cost analysis, evaluation of the care quality, comparisons between neonatal units, research, and even parental counselling [8,22,25,26,27,28,29,53]. Therefore, clinicians, like us, will continue searching for the ideal scoring system, ideal at least for the population they have to care. We made efforts to find the best – in terms of accuracy - and easiest-to-apply scoring system for our population, based on our experience that preterm infants have to be considered and analyzed separately from term infants.
We acknowledge some limitations of our study. We didn’t evaluate the individual components of the SNS score as this was not the goal of our study. Instead, we plan to do so in a future study in which we plan to compare SNS scores before transfer and at arrival in our unit in order to evaluate pretransport stabilization and the quality of care during neonatal transport. Also, probably a higher number of patients would give increased statistical power to some of our comparisons and associations. The study period was quite long – 7 years – and protocols for stabilization and transport have been changed during this period, influencing the neonatal status at arrival in some of the newborns included in the study. We didn’t perform the yearly comparative analysis of the severity scores.
5. Conclusions
The MSNS-AT score – calculated by adding gestational age, birthweight, and time to admission to the SNS score - significantly improved mortality prediction at admission in the whole study group as compared to SNS score. We found, as other authors, that the predictive accuracy of the same score is different in term and preterm infants, suggesting that different scores have to be used for these categories of neonates. The best accuracy prediction of MSNS-AT score was observed in the group of preterm infants suggesting that, besides gestational and birth weight, time to admission may be decisive for the outcome of outborn preterm infants. Further studies are necessary to confirm the predictive value of MSNS-AT score and to identify variables that can improve its value in term infants without affecting the simplicity, ease, and rapidity of the scoring system. We are planning to validate the new score in a new, independent data set.
Based on a prospective cohort starting from the SNS score, and using statistical models we developed an MSNS-AT score with better predictive performance for mortality in outborn infants that may help us to better allocate all types of resources and to adjust care and treatment to optimize neonatal outcomes. The organization of the Romanian neonatal transport system started in 2004, immediately after regionalization of the maternal and neonatal care, trained, specialized staff and special equipment are limited or even lacking in many parts of the country. Considering the improved rates of survival at lower gestational ages, and the insufficient number of beds in neonatal intensive care units (NICU), we face a continuous need for better critical neonatal care as survival isn’t anymore the ultimate goal of NICU care.
Author Contributions
Conceptualization, M.L.O., I.C.M., R.G., and M.C; methodology, M.L.O., B.C., S.B.T, C.I. and A.G.B; software, D.A.T., I.A.R., S.B.T, and C.I.; formal analysis, M.L.O, A.G.B, R.G., and M.C.; investigation, B.C., D.A.T., I.A.R., and I.C.M; validation: B.C., D.A.T., I.A.R., S.B.T., C.I., I.C.M., A.G.B., M.C. and M.L.O.; resources, I.A.R.; data curation, M.L.O.; writing—original draft preparation, M.L.O., B.C., D.A.T., and I.A.R.; writing—review and editing, M.L.O., C.I., S.B.T., A.G.B, R.G.; supervision, M.O.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable due to retrospective design of the study. The publication of the research was approved by the Ethical, Medical Deontology, and Discipline Committee of the Clinical County Emergency Hospital Sibiu under the decision 22979/29.09.2023 as it was conducted in accordance with the Declaration of Helsinki for studies involving humans.
Informed Consent Statement
Written informed consent for publication was not obtained as the study design was retroepctive and participating patients cannot be identified.
Data Availability Statement
The data presented in this study are not publicly available due to institutional restrictions but are available upon reasonable request from the corresponding author.
Acknowledgments
The authors are grateful to Boris Kramer for his kind support in editing the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Standards For Improving Quality Of Maternal and Newborn Care in Health Facilities. World Health Organisation. 2016. Available online: http://www.who.int (accessed on 3 September 2023).
- GBD 2019 Under-5 Mortality Collaborators. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet. 2021, 398, 870–905. [Google Scholar] [CrossRef]
- Qu, W., Shen, Y., Qi, Y., Jiang, M., Zheng, X., Zhang, J., Wu, D., He, W., Geng, W., Hei., M. Comparison of four neonatal transport scoring methods in the prediction of mortality risk in full-term, out-born infants: a single-center retrospective cohort study. Eur J Pediatr. 2022, 181, 3005–3011.
- Neonatal Mortality-UNICEF Data. Available online: https://data. unicef.org/topic/child-survival/neonatal-mortality/ (accessed on 30 August 2023).
- Meshram, R.M., Nimsarkar, R.A., Nautiyal, A.P. Role of modified sick neonatal score in predicting the neonatal mortality at limited-resource setting of central India. J Clin Neonatol 2023, 12, 1–6. [CrossRef]
- Cavallin, F., Contin, A., Alfeu, N., Macmillian, B., Seni, A.H.A., Cebola, B.R., Calgaro, S., Putoto, G., Trevisanuto, D. Prognostic role of TOPS in ambulance-transferred neonates in a low-resource setting: a retrospective observational study. BMC Pregnancy Childbirth. 2022, 22, 726.
- Guidelines for Perinatal Care. American Academy of Pediatrics. Committee on Fetus and Newborn. Edited by American College of Obstetricians and Gynecologists. Committee on Obstetric Practice. 2012.
- Chang, A.S., Berry, A., Jones, L.J., Sivasangari, S. Specialist teams for neonatal transport to neonatal intensive care units for prevention of morbidity and mortality. Cochrane Database Syst Rev. 2015, 2015, CD007485.
- Chheda, A., Khadse, S., Valvi, C., Kulkarni, R., Hiremath, A. Importance of Temperature, Oxygen Saturation, Perfusion, Sugar (TOPS) Parameters and the Concept of TOPS Score for Neonatal Transport in India – A Pilot Project. Pediatric Oncall Journal. 2018, 15, 69–72.
- Amer, R., Moddemann, D., Seshia, M., Alvaro, R., Synnes, A., Lee, K.S., Lee, S.K., Shah, P.S.; Canadian Neonatal Network and Canadian Neonatal Follow-up Network Investigators. Neurodevelopmental Outcomes of Infants Born at <29 Weeks of Gestation Admitted to Canadian Neonatal Intensive Care Units Based on Location of Birth. J Pediatr. 2018, 196, 31–37.
- Whyte, H.E., Jefferies, A.L.; Canadian Paediatric Society, Fetus and Newborn Committee. The interfacility transport of critically ill newborns. Paediatr Child Health. 2015, 20, 265–275.
- Chen, W.H., Su, C.H., Lin, L.C., Lin, H.C., Lin, Y.J., Hsieh, H.Y., Sheen, J.M., Lee, C.T. Neonatal mortality among outborn versus inborn babies. Pediatr Neonatol. 2021, 62, 412–418.
- Mohan, K.R., Kumar, R. Study of indications, complications and outcomes of neonatal transport by a skilled team. Int J Contemp Pediatr. 2019, 6, 2402–2405. [CrossRef]
- Rathod, D., Adhisivam, B., Bhat, B.V. Transport of sick neonates to a tertiary care hospital, South India: condition at arrival and outcome. Trop Doct. 2015, 45, 96–99. [CrossRef]
- O'Brien, E.A., Colaizy, T.T., Brumbaugh, J.E., Cress, G.A., Johnson, K.J., Klein, J.M., Bell, E.F. Body temperatures of very low birth weight infants on admission to a neonatal intensive care unit. J Matern Fetal Neonatal Med. 2019, 32, 2763–2766. [CrossRef]
- Tay, V.Y., Bolisetty, S., Bajuk, B., Lui, K., Smyth, J.; the New South Wales and the Australian Capital Territory Neonatal Intensive Care Units' Data Collection. Admission temperature and hospital outcomes in extremely preterm infants. J Paediatr Child Health. 2019, 55, 216–223.
- Standards for improving quality of care for small and sick newborns in health facilities. Geneva: World Health Organization; 2020. Available online: https://creativecommons.org/licenses/by-nc-sa/3.0/igo (accessed on 3 September 2023).
- Stroud, M.H., Trautman, M.S., Meyer, K., Moss, M.M., Schwartz, H.P., Bigham, M.T., Tsarouhas, N., Douglas, W.P., Romito, J., Hauft, S., Meyer, M.T., Insoft, R. Pediatric and neonatal interfacility transport: results from a national consensus conference. Pediatrics 2013, 132, 359–366.
- Das, R.R., Sankar, J., Sankar, M.J. Sick Neonate Score: Better than Others in Resource Restricted Settings? Indian J Pediatr. 2016, 83, 97–98. [CrossRef]
- Ravikumar, S.P., Kaliyan, A., Jeganathan, S., Manjunathan, R. Post-transport TOPS score as a predictive marker of mortality among transported neonates and its comparative analysis with SNAP-II PE. Heliyon. 2022, 8, e10165. [CrossRef]
- Chellani, H., Arya, S. Scoring Tools to Predict Neonatal Mortality: Where Do We Stand Today? Indian J Pediatr. 2023, 90, 323. [CrossRef]
- Garg, B., Sharma, D., Farahbakhsh, N. Assessment of sickness severity of illness in neonates: review of various neonatal illness scoring systems. J Matern Fetal Neonatal Med. 2018, 31, 1373–1380. [CrossRef] [PubMed]
- Lee, K.S. Neonatal transport metrics and quality improvement in a regional transport service. Transl Pediatr. 2019, 8, 233–245. [Google Scholar] [CrossRef]
- Adhisivam, B. Clinical Scores for Sick Neonates. Indian J Pediatr. 2023, 90, 324–325. [Google Scholar] [CrossRef] [PubMed]
- Dorling, J.S., Field, D.J., Manktelow, B. Neonatal disease severity scoring systems. Arch Dis Child Fetal Neonatal Ed. 2005, 90, F11–F16. [CrossRef] [PubMed]
- Padar, C., Rajan, A., Shriyan, A., Oommen, R.A. Modified Sick Neonatal Score and Delta: Modified Sick Neonatal Scores As Prognostic Indicators in Neonatal Intensive Care Units. Cureus. 2022, 14, e28414.
- Reddy, P., Gowda, B.R. A. A Study of the Prediction of Mortality in a Tertiary Care Hospital Using the Modified Sick Neonatal Score (MSNS): An Observational Cross-Sectional Study. Cureus. 2023, 15, e38484.
- Shivaramakrishnababji, N., Rajesh, C., Mekala, A., Siddani, B.R. Validation of modified sick neonatal score, a simple clinical score for assessment of severity of illness and outcome in new-borns for resource poor settings. Int J Contemp Pediatr 2022, 9, 53–57.
- Agrawal, J. Sick Neonate Score: Role in Predicting Neonatal Mortality. Clinics Mother Child Health. 2020, 17, 355. [Google Scholar]
- Rathod, D., Adhisivam, B., Bhat, B.V. Sick Neonate Score--A Simple Clinical Score for Predicting Mortality of Sick Neonates in Resource Restricted Settings. Indian J Pediatr. 2016, 83, 103–106. [CrossRef] [PubMed]
- WHO. Newborn mortality. 2021. Available online: https://www.who.int/news-room/factsheets/detail/levels-and-trends-in-child-mortality-report-2021 (accessed on 12 August 2023).
- Hirata, K., Ueda, K., Wada, K., Ikehara, S., Tanigawa, K., Kimura, T., Ozono, K., Iso, H; Japan Environment and Children’s Study Group. Long-term outcomes of children with neonatal transfer: the Japan Environment and Children's Study. Eur J Pediatr. 2022, 181, 2501–2511. [CrossRef]
- Ashokcoomar, P., Bhagwan, R. Towards a safer and more efficient neonatal transfer system in South Africa: A qualitative inquiry with ALS paramedics. Australasian Journal of Paramedicine 2021, 18, 1–9.
- Dempsey, E.M., Barrington, K.J. Evaluation and treatment of hypotension in the preterm infant. Clin Perinatol. 2009, 36, 75–85. [CrossRef]
- Ordinul Ministrului Sănătăţii şi Familiei nr. 910 privind criteriile de ierarhizare a secţiilor de spital de specialitate obstetrică, ginecologie şi neonatologie, publicat în Monitorul Oficial al României, 18.11.2002.
- Bivoleanu, A., Avasiloaiei, A., Voicilă, C., Stamatin, M., Stoicescu, S.M. Echilibrarea nou-născutului pentru transport și transportul neonatal, aprobat prin Ordinul Ministerului Sănătății 1232/2.08.2011, pulicat în Monitorul Oficial al României, Partea I, nr. 586/18.08.2011, Editura Alma Mater, Sibiu, 2011.
- Ordinul Ministrului Sănătăţii nr. 417 privind Înfiinţarea Unităţii de transport neonatal specializat, publicat în Monitorul Oficial al României, Partea I, nr. 349; 21.04.2004.
- Odinul Ministrului Sănătății privind aprobarea metodologiei şi criteriilor minime obligatorii de ierarhizare a structurilor de obstetrică-ginecologie, neonatologie şi pediatrie care asigură servicii de terapie intensivă pentru nou-născuți și pentru modificarea și completarea Ordinului ministrului sănătăţii nr. 323/2011 privind aprobarea metodologiei şi a criteriilor minime obligatorii pentru clasificarea spitalelor în funcţie de competenţă. Available online: https://www.ms.ro/ro/transparenta-decizionala/acte-normative-in-transparenta/ordin-privind-aprobarea-metodologiei-%C5%9Fi-criteriilor-minime-obligatorii-de-ierarhizare-a-structurilor-de-obstetric%C4%83-ginecologie-neonatologie-%C5%9Fi-pediatrie-care-asigur%C4%83-servicii-de-terapie-intensiv%C4%83-pentru-nou-n%C4%83scu%C8%9Bi/ (accessed on 25 September 2023).
- Ordinului Ministrului Sănătăţii nr. 323/18.04.2011 privind aprobarea metodologiei şi a criteriilor minime obligatorii pentru clasificarea spitalelor în funcţie de competenţă, publicat în Monitorul Oficial al României nr. 274/19.04.2011.
- Broughton, S.J., Berry, A., Jacobe, S., Cheeseman, P., Tarnow-Mordi, W.O., Greenough, A; Neonatal Intensive Care Unit Study Group. The mortality index for neonatal transportation score: a new mortality prediction model for retrieved neonates. Pediatrics. 2004, 114, e424–e428. [CrossRef]
- Mathur, N.B., Arora, D. Role of TOPS (a simplified assessment of neonatal acute physiology) in predicting mortality in transported neonates. Acta Paediatr. 2007, 96, 172–175. [CrossRef]
- Hermansen, M.C., Hasan, S., Hoppin, J., Cunningham, M.D. A validation of a scoring system to evaluate the condition of transported very-low-birthweight neonates. Am J Perinatol. 1988, 5, 74–78. [CrossRef] [PubMed]
- Dorling, J.S., Field, D.J. Value and validity of neonatal disease severity scoring systems. Arch Dis Child Fetal Neonatal Ed. 2008, 93, F80–F82.
- Ray, S., Mondal, R., Chatterjee, K., Samanta, M., Hazra, A., Sabui, T.K. Extended Sick Neonate Score (ESNS) for Clinical Assessment and Mortality Prediction in Sick Newborns referred to Tertiary Care. Indian Pediatr. 2019, 56, 130–133. [CrossRef]
- Dammann, O., Shah, B., Naples, M., Bednarek, F., Zupancic, J., Allred, E.N., Leviton, A; ELGAN Study Investigators. Interinstitutional variation in prediction of death by SNAP-II and SNAPPE-II among extremely preterm infants. Pediatrics. 2009, 124, e1001–e1006. [CrossRef]
- Cole, T.J., Hey, E., Richmond, S. The PREM score: a graphical tool for predicting survival in very preterm births. Arch Dis Child Fetal Neonatal Ed. 2010, 95, F14–F19. [CrossRef]
- Helenius, K., Longford, N., Lehtonen, L., Modi, N., Gale, C; Neonatal Data Analysis Unit and the United Kingdom Neonatal Collaborative. Association of early postnatal transfer and birth outside a tertiary hospital with mortality and severe brain injury in extremely preterm infants: observational cohort study with propensity score matching. BMJ. 2019, 367, l5678.
- Fang, J.L., Mara, K.C., Weaver, A.L., Clark, R.H., Carey, W.A. Outcomes of outborn extremely preterm neonates admitted to a NICU with respiratory distress. Arch Dis Child Fetal Neonatal Ed. 2020, 105, 33–40. [CrossRef] [PubMed]
- Shipley, L., Gyorkos, T., Dorling, J., Tata, L.J., Szatkowski, L., Sharkey, D. Risk of Severe Intraventricular Hemorrhage in the First Week of Life in Preterm Infants Transported Before 72 Hours of Age. Pediatr Crit Care Med. 2019, 20, 638–644. [CrossRef] [PubMed]
- Jensen, E.A., Lorch, S.A. Effects of a Birth Hospital's Neonatal Intensive Care Unit Level and Annual Volume of Very Low-Birth-Weight Infant Deliveries on Morbidity and Mortality. JAMA Pediatr. 2015, 169, e151906. [CrossRef] [PubMed]
- Gupta, N., Shipley, L., Goel, N., Browning Carmo, K., Leslie, A., Sharkey, D. Neurocritical care of high-risk infants during inter-hospital transport. Acta Paediatr. 2019, 108, 1965–1971. [CrossRef]
- Redpath, S., Shah, P.S., Moore, G.P., Yang, J., Toye, J., Perreault, T., Lee. K.S; Canadian Neonatal Transport Network and Canadian Neonatal Network Investigators. Do transport factors increase the risk of severe brain injury in outborn infants <33 weeks gestational age? J Perinatol. 2020, 40, 385–393.
- Behera, B., Lal Meena, B. Outcomes of Sick Neonates Transported to a Tertiary Care Hospital by a Trained Team, in Northern India. Indian Journal of Neonatal Medicine and Research. 2021, 9, PO10–PO15.
- Behera, B., Archana, B.R. SNAPPE-II (Score for Neonatal Acute Physiology with Perinatal Extension-II) in Predicting Mortality and Morbidity in NICU. J Clin Diagn Res. 2015, 9, SC10–SC12.
- Morse, S., Groer, M., Shelton, M.M., Maguire, D., Ashmeade, T. A Systematic Review: The Utility of the Revised Version of the Score for Neonatal Acute Physiology Among Critically Ill Neonates. J Perinat Neonatal Nurs. 2015, 29, 315–344. [CrossRef] [PubMed]
- Fleisher, B.E., Murthy, L., Lee, S., Constantinou, J.C., Benitz, W.E., Stevenson, D.K. Neonatal severity of illness scoring systems: a comparison. Clin Pediatr (Phila). 1997, 36, 223–227. [CrossRef] [PubMed]
- Mansoor, K.P., Ravikiran, S.R., Kulkarni, V., Baliga, K., Rao, S., Bhat, K.G., Baliga, B.S., Kamath, N. Modified Sick Neonatal Score (MSNS): A Novel Neonatal Disease Severity Scoring System for Resource-Limited Settings. Crit Care Res Pract 2019, 2019, 9059073.
- Mori, R., Fujimura, M., Shiraishi, J., Evans, B., Corkett, M., Negishi, H., Doyle, P. Duration of inter-facility neonatal transport and neonatal mortality: systematic review and cohort study. Pediatr Int. 2007, 49, 452–458. [CrossRef]
Figure 1.
Representation of the number of transferred newborn infants during the study period.
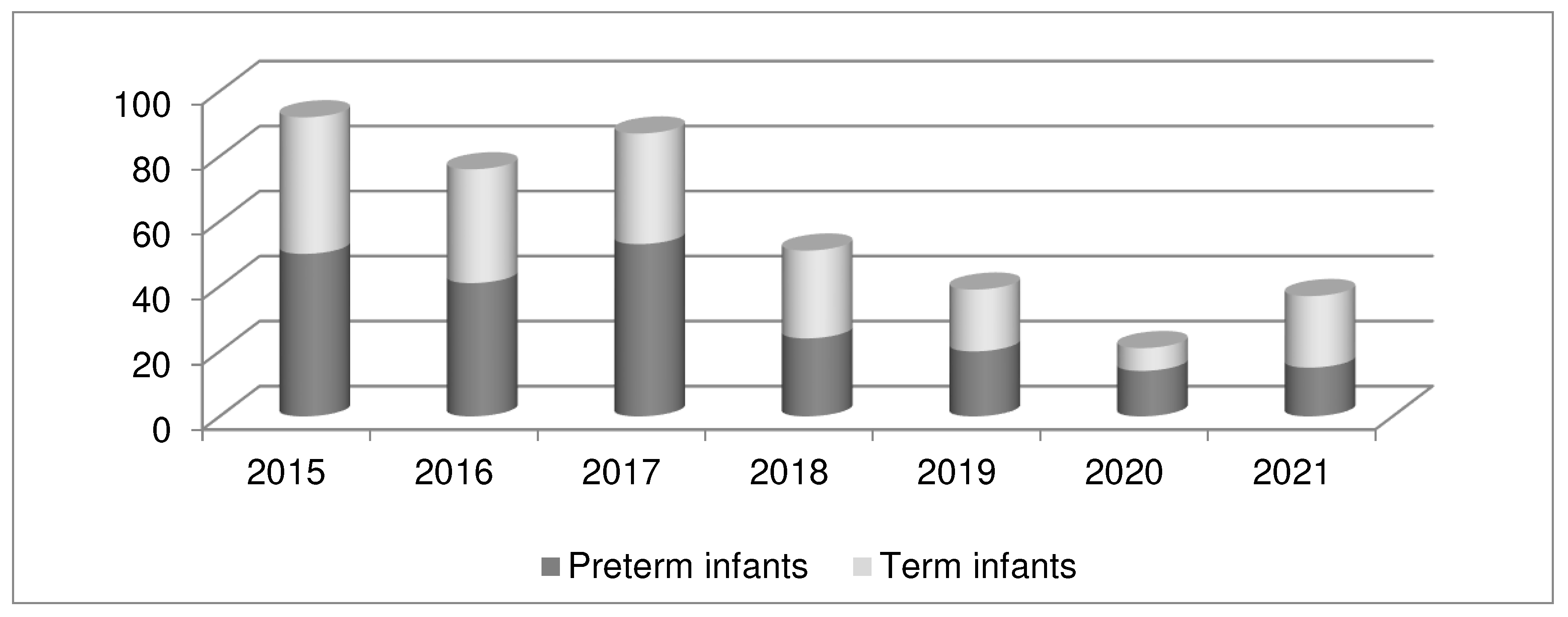
Figure 2.
A. Survival differences between newborns based on the time-to-admission period. B. Improvement of Hazard estimation by adding a time-to-admission variable to the SNS score regression model.
Figure 2.
A. Survival differences between newborns based on the time-to-admission period. B. Improvement of Hazard estimation by adding a time-to-admission variable to the SNS score regression model.
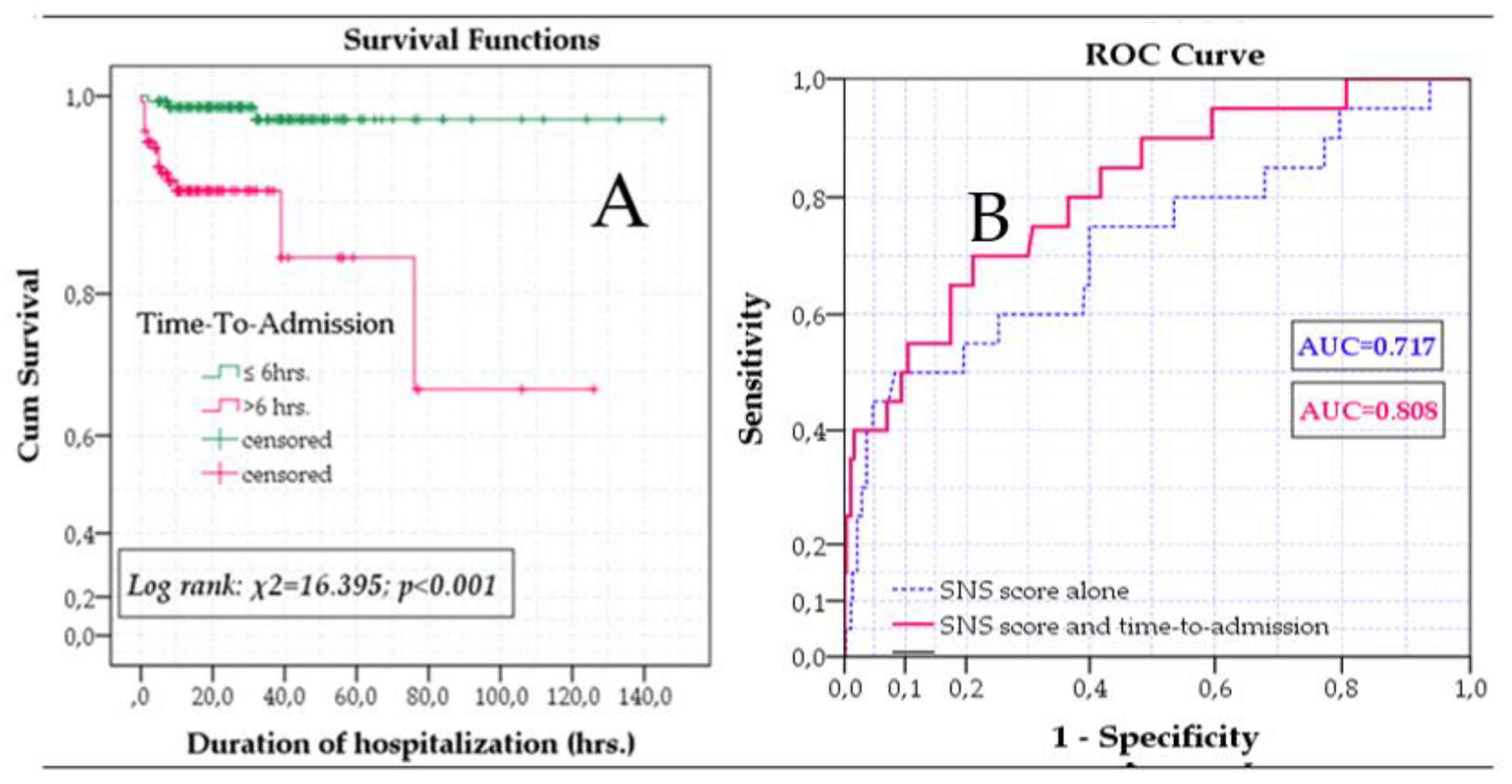
Figure 3.
Difference between the SNS score and the novel MSNS-AT score in our study groups: A. Term newborns; B. The entire group; C. Preterm infants.
Figure 3.
Difference between the SNS score and the novel MSNS-AT score in our study groups: A. Term newborns; B. The entire group; C. Preterm infants.
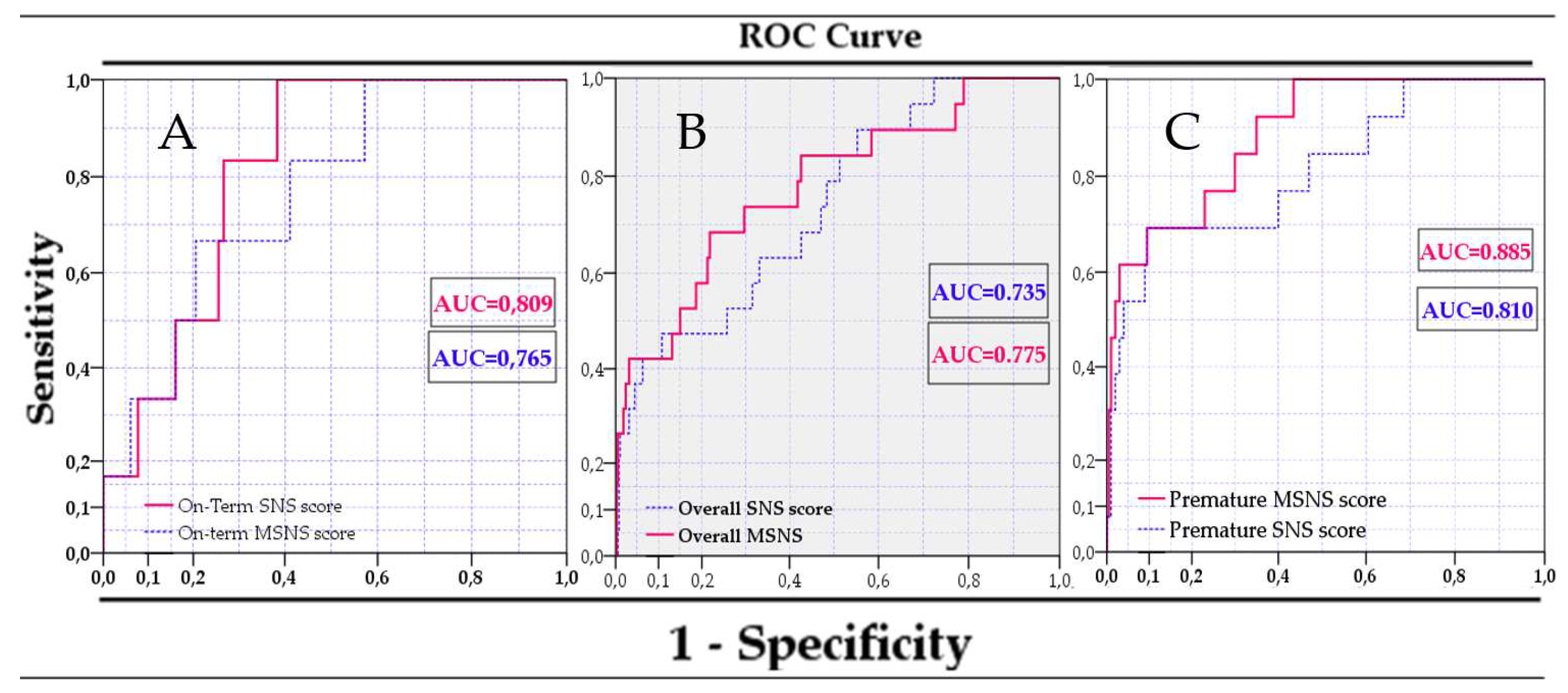
Figure 4.
Overall risk of mortality assessed with Modified MSNS-AT score.
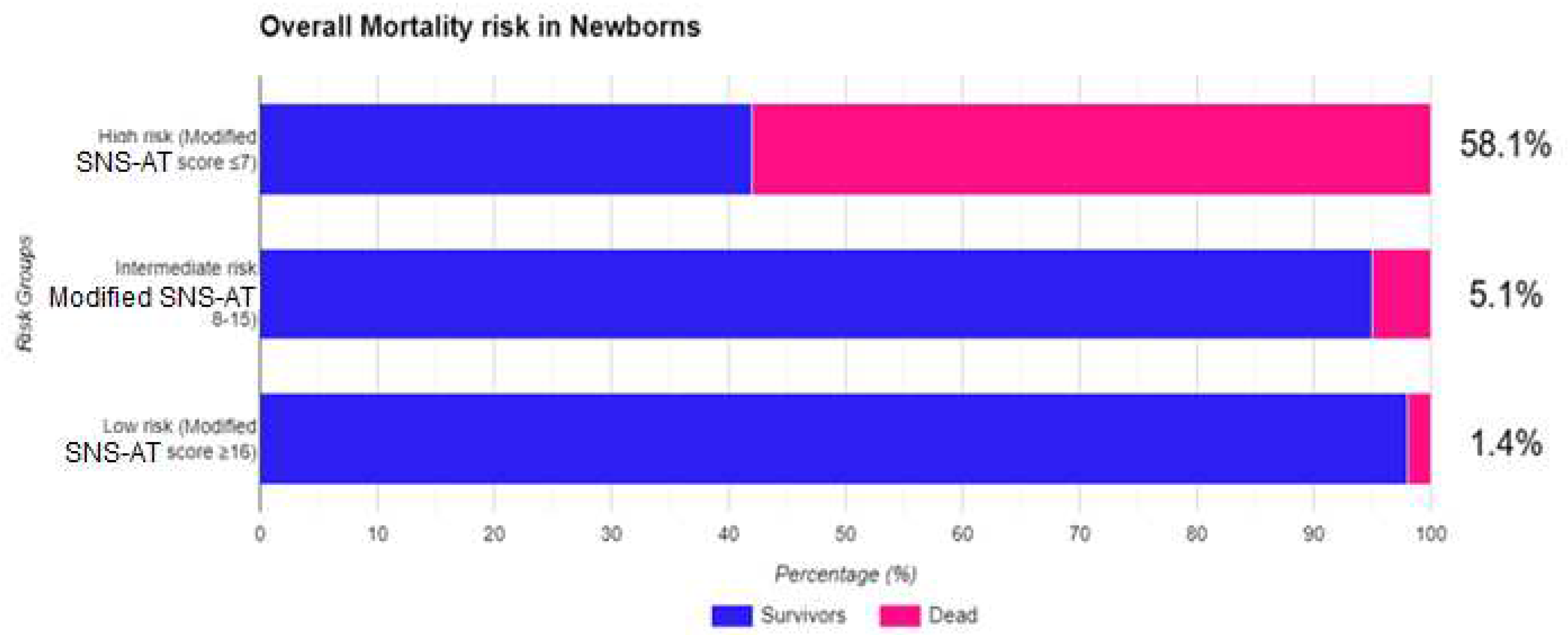

Table 1.
Sick neonatal score [30].
Table 1.
Sick neonatal score [30].
| Variables | Score | ||
|---|---|---|---|
| 0 | 1 | 2 | |
| Respiratory effort | Apnea or grunting | Tachypnea (>60/min) +/- retractions | Normal (40-60/min) |
| Heart rate | Bradycardia/ Asystole |
Tachycardia (>160/min) | Normal (100-160/min) |
| Mean blood pressure (mmHg) | <30 | 30-39 | >39 |
| Axillary temperature (0C) | <36 | 36-36.5 | 36.5-37.5 |
| Capillary filling time (s) | >5 | 3-5 | <3 |
| Random blood sugar (mg/dL) | <40 | 40-60 | >60 |
| SpO2 in room air (%) | <85 | 85-92 | >92 |
Table 2.
Baseline characteristics of the study group and subgroups.
| Preterm Infants (N 217) | Term Infants (N 186) |
All Infants (N 403) |
|
|---|---|---|---|
| Gestational age (weeks)(mean SD) | 35.56±2.87 | 38.73±1.31 | 35.40±3.83 |
| Birth weight (grams) (mean SD) | 1788.55±561.90 | 3119.30±631.25 | 2402.74±891.80 |
| Male gender (N/%) | 113/52.1 | 111/59.7 | 224/55.6 |
| Time to admission (hours) (mean SD) | 17.33±65.07 | 27.06±32.44 | 21,82±52.75 |
| Apgar score/1 min. (mean SD) | 6.60±2.12 | 7.30±2.32 | 6.92±2.24 |
| Apgar score< 3/1 min. (N/%) | 22/10.1 | 19/10.2 | 41/10.2 |
| Early onset sepsis (N/%) | 37/17.1 | 75/40.3 | 112/27.8 |
| Place of birth | |||
| Home (N/%) | 8/3.7 | 5/2.7 | 13/3.2 |
| Level I (N/%) | 125/57.6 | 126/67.7 | 251/62.3 |
| Level II (N/%) | 82/38.2 | 55/29.6 | 138/34.2 |
| Level III (N/%) | 1/0.5 | - | 1/0.2 |
| Death (N/%) | 14/6.5 | 6/3.2 | 20/5.0 |
| SNS score (mean SD) | 10.04±2.67 | 11.85±2.20 | 10.87±2.63 |
Table 3.
Comparison of baseline characteristics between survivors and non-survivors in the whole group and subgroups based on gestational age.
Table 3.
Comparison of baseline characteristics between survivors and non-survivors in the whole group and subgroups based on gestational age.
| Preterm Infants | Term Infants | ALL | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Survivors (mean/SD) |
Non-survivors (mean/SD) |
p* | Survivors (mean/SD) |
Non-survivors (mean/SD) |
p* | Survivors (mean/SD) |
Non-survivors (mean/SD) |
p* | |
| Gestational Age (weeks) | 32.7/2.7 | 30.7/4.4 | 0.007 | 38.7/1.3 | 38.3/1.2 | 0.457 | 35.5/3.7 | 32.9/5.1 | 0.003 |
| Birth weight (grams) | 1804/543 | 1557/767 | 0.112 | 3128/638 | 2853/261 | 0.295 | 2426/885 | 1946/889 | 0.010 |
| Sns score | 10.4/2.4 | 5.3/2.1 | <0.001 | 11.9/2.2 | 10.2/2.2 | 0.057 | 11.1/2.4 | 6.8/3.0 | <0.001 |
* Independent Samples T Test.
Table 4.
Association of tested variables with mortality in study groups.
| Preterm Infants (N 217) |
Term Infants (N 186) |
All Infants (N 403) |
||||
|---|---|---|---|---|---|---|
| Median (IQR) | p* | Median (IQR) | p* | Median (IQR) | p* | |
| Gestational age (weeks) | 36 (31-35) | 0.077 | 39 (38-39) | 0.525 | 36(33-39) | 0.026 |
| Birth weight (grams) | 1750 (1400-2162.5) |
0.164 | 3100 (2800-3422.5) |
0.135 | 2330 (1700-3100) |
0.032 |
| Time to admission (hours) | 4 (3-7) | <0.001 | 12.5 (5-36) | 0.343 | 6.0 (3-21) | 0.013 |
| Apgar score/1 min. | 7 (6-8) | <0.001 | 8 (6.75-9) | 0.038 | 7 (6-8.75) | <0.001 |
| Sns score | 11.0 (8-12) | <0.001 | 12.5 (10-14) | 0.038 | 11.0 (11-13) | <0.001 |
* Mann-Whitney U test.
Table 5.
Baseline characteristics and their association with mortality.
| Preterm Infants | Term Infants | ALL | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Survivors (N/%) |
Non-survivors (N/%) |
p-value |
OR (95%CI) |
Survivors (N/%) |
Non-survivors (N/%) |
p-value | OR (95%CI) |
Survivors (N/%) |
Non-survivors (N/%) |
p-value | OR (95%CI) |
|
| Male gender | 105/51.7 | 8/57.1 | 0.696 |
1.23(0.44-3.42) | 106/58.9 | 5/83.3 | 0.232 | 3.38(0.46-28.34) | 211/55.1 | 13/65.0 | 0.386 | 1.48(0.60-3.64) |
| Apgar score <3 | 20/9.9 | 2/15.4 | 0.529 | 1.65(0.34-7.99) | 19/10.6 | 0/0 | 0.404 | - | 39/10.2 | 2/10.5 | 0.995 | 1.03(0.23-4.65) |
| Early sepsis | 34/16.7 | 3/21.4 | 0.654 | 1.36(0.36-5.12) | 72/40.0 | 3/50.0 | 0.626 | 1.50(0.29-7.64) | 106/27.7 | 6/30.0 | 0.822 | 1.12(0.42-2.99) |
| Sns score≤8 | 48/23.6 | 14/100 | <0.001 | 1.29(1.13-1.48) | 18/10.0 | 1/16.7 | 0.598 | 1.80(0.20-16.27) | 66/17.2 | 15/75.0 | <0.001 | 14.41(5.06-41.02) |
| Place of birth home | 7/3.4 | 1/7.1 | 0.013 | - | 5/2.8 | 0/0 | 0.750 | 12/3.1 | 1/5.0 | 0.014 | - | |
| Level i | 123/60.6 | 2/14.3 | 122/67.8 | 4/66.7 | 245/64.0 | 6/30.0 | ||||||
| Level ii | 72/35.5 | 11/78.6 | 53/29.4 | 2/33.3 | 125/32.6 | 13/65.0 | ||||||
| Level iii | 1/0.5 | 0/0 | 0/0 | 0/0 | 1/0.3 | 0/0 | ||||||
Table 6.
Modified SNS-Admission Time score.
| 0 points | 1 points | 2 points | 3 points | |
| Gestational age (weeks) | <32 | 32-36 | ≥37 | - |
| Birth weight (g) | < 1500 | 1500-2499 | ≥2500 | - |
| Time from birth to admission (h) | ≥12 | 6-12 | - | <6 |
| Final MSNS-AT Score | Points granted on the above variables are added to the SNS score | |||
Table 7.
Accuracy of the two scoring systems for prediction mortality evaluated in study groups.
| Model | AUC | p-Value | 95% CI | |
|---|---|---|---|---|
| Lower | Upper | |||
| Sns score in term infants | 0.809 | 0.010 | 0.698 | 0.920 |
| Msns-at in term infants | 0.765 | 0.027 | 0.601 | 0.929 |
| Sns score in preterm infants | 0.810 | 0.000 | 0.676 | 0.945 |
| Msns-at in preterm infants | 0.885 | 0.000 | 0.800 | 0.970 |
| Sns score in all infants | 0.735 | 0.001 | 0.622 | 0.848 |
| Msns-at in all infants | 0.775 | 0.000 | 0.659 | 0.890 |
Table 8.
Cox proportional multivariable model with adjustments.
| Multivariable Cox Regression | p-Value | HR | 95.0% CI for HR | |
|---|---|---|---|---|
| Variables | Lower | Upper | ||
| Gestational age | 0.920 | 1.012 | 0.800 | 1.280 |
| Birthweight | 0.904 | 1.000 | 0.999 | 1.001 |
| Apgar 1 min. | 0.563 | 1.113 | 0.774 | 1.600 |
| Apgar <3 | 0.966 | 1.054 | 0.093 | 11.918 |
| Early sepsis | 0.871 | 0.917 | 0.322 | 2.610 |
| Time-to-admission | 0.575 | 1.001 | 0.997 | 1.006 |
| Msns-at ≥16 | <0.001 | |||
| Msns-at 8-15 | 0.048 | 3.607 | 1.023 | 14.653 |
| Msns-at ≤7 | <0.001 | 47.120 | 9.593 | 231.459 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



