
Submitted:
17 October 2023
Posted:
18 October 2023
You are already at the latest version
Abstract
Objectives: Non-adhesive gel-like embolic materials (NAGLEMs) are becoming increasingly dominant in the endovascular treatment of hypervascularised formations in the head and neck due to a combination of their key properties. The main advantages include their lack of adhesion, effective distribution and penetration through pathological vessels, and crucially, their controlla-bility during the process. Our assigned duty was to scrutinise the literature and assess the efficacy and outcomes of administering NAGLEMs, in comparison to other embolizing substances (name-ly, coils, glue, and particles), among patients treated at our clinic. The procedures involved ana-lyzing the technical aspects, efficiency, and safety of endovascular therapy applied to two catego-ries of hypervascular pathological anomalies, surgically managed from 2015 to 2023. Arteriove-nous malformations (AVMs) located in the head, neck, and paragangliomas with jugular/carotid body localization are combined by intense shunting blood flow and shared requirements for em-bolizates used in endovascular treatment (such as penetration, distribution, delayed polymeriza-tion and controllability). An analysis of the literature was also conducted. Results showed 18 pa-tients diagnosed with neck paragangliomas of the carotid body and jugular type. Five patients with arteriovenous malformation (AVM) of the face and neck were included, consisting of 16 fe-males and 7 males with an average age of 55 ± 13 years. Endovascular procedures were conduct-ed using NAGLEMs (ONYX (Medtronic), SQUID (Balt), and PHIL (Microvention)) and dimethyl sulfoxide (DMSO)-compatible balloon catheters. All patients achieved complete or partial embo-lization of hypervascularized formations using one or more stages of endovascular treatment. Additionally, three AVMs of the face and two paragangliomas of the neck were surgically ex-cised following embolization. In other instances, formations were not deemed necessary to be re-moved. The patients' condition upon discharge was assessed by the modified Rankin Scale (mRs) and rated between 0 and 2. Conclusion: Currently, NAGLEMs are predominantly used to treat hypervascularized formations in the neck and head due to their fundamental properties. These properties include a lack of adhesion and a delay in predictable polymerization (after 30-40 minutes). NAGLEMs also exhibit excellent distribution and penetration throughout the vascular bed of the formation. Adequate controllability of the process is largely achieved through the pres-ence of embolism forms of different viscosity, as well as excellent X-ray visualization.
Keywords:
embolic agent
; ONYX
; SQUID
; PHIL
; vascular malformations
; paragangliomas
1. Introduction
The field of vascular neurosurgery has been transformed by the advent of non-adhesive gel-like embolic materials (NAGLEMs) [1]. New treatments for patients with cerebral pathology [2,3,4] and hypervascular formations in the head and neck, specifically paragangliomas and arteriovenous malformations (AVMs), have arisen. The emergence of these non-adhesive compositions is due to the elimination of the shortcomings associated with earlier generations of embolising agents [1]. NAGLEMs, due to their fundamental properties, are becoming increasingly prevalent in the endovascular treatment of hypervascular formations in the head and neck region. Their primary advantages include lack of adhesion, effective distribution and penetration through the pathological formation vessels, and, crucially, adequate process controllability [1]. In this article, we have analysed the characteristics of different embolising agents that were employed prior to the introduction of NAGLEMs. Subsequently, we will make a direct comparison between NAGLEMs and these agents, taking into account evidence from worldwide literature and our own investigations. We aim to address why NAGLEMs are the preferred choice for treating hypervascularised diseases of the head and neck using intravascular treatment. This location for the pathological process was not chosen arbitrarily. This is because, in addition to neurosurgeons, specialists in maxillofacial [5], plastic [6], vascular [7] and radiosurgery [8] also deal with this condition. This site, where there can be hypervascularised pathological masses, often poses a challenge in terms of treatment tactics.
2. Results
2.1. Patient Population
In our clinics, specifically the North-Western district scientific and clinical center named after L. G. Sokolov Federal Medical and Biological Agency & Almazov National Research Medical Center in St. Petersburg, Russia in St. Petersburg, Russia, we performed operations on 23 patients with hypervascularised masses in the region of the head and neck between November 2015 and May 2023. Eighteen patients were diagnosed with paragangliomas; 7 (30.4%) had carotid body type while 11 (47.8%) had jugular type. Five (21.7%) patients had arteriovenous malformations in their face and neck. Among the patients, 16 (69.6%) were females and 7 (30.4%) were males. In six patients (26.1%), our clinic attempted embolization with non-gel-like embolic agents prior to treatment. However, only partial embolization was observed in all cases. Four patients (17.4%) received microsurgical removal of the mass after embolisation. The demographic data and treatment characteristics of patients in both groups are available in Table 1.
NAGLEMs (ONYX (Medtronic), Squid (Balt) and PHIL (Microvention)) were used. Embolization of the masses was achieved using balloons that are compatible with dimethyl sulfoxide (DMSO) to prevent the embolic agents from migrating into the main vessels. Therefore, the technique was effective in avoiding the risk of migration.
Squid was used in 11 out of 23 cases, Onyx in 8 out of 23 and Phil in only one patient.
The average embolisation time was 97 ± 28 (M ± SD) minutes (min 60, max 170). Complete embolization was defined as filling the vascular network of the mass by 100%, while subtotal embolization was defined as 85-99% filling of the vascular network. All 23 cases demonstrated either total or subtotal filling of the vascular network, with 17 neoplasms (73.9%) and 6 subtotals (26.1%) completely turned off. 100% complete AVMs were turned off in all 5 cases, and para-gangliomas were turned off in 12 out of 18 cases (66%). All patients underwent MRI in the early postoperative period.
The mRS scores at discharge were: 0 in 11 patients, 1 in 10 patients, and 2 in 2 patients. As follows from Table 1, the group of patients with AVMs of the face and neck (n=5) was significantly younger (p = 0.033) (method used: Fisher's F-criterion) and the mean age of patients in this group was 42 ± 6 (M ± SD). In this group, embolisation attempts with other non-gel-like agents (cyanoacrylates, alcohol and spirals) were significantly (p = 0.004) (method used: Pearson's Chi-square) more frequent (Figure 1).
Despite this, this group significantly (p = 0.035) (method used: Kraskell-Wallis Criterion) required less time to administer NAGLEMs, averaging 70 min (Me) (Figure 2).
In all cases in this group total embolization of AVM was performed using DMSO compatible baloons. mRS in this group, both at the time of admission and at the time of discharge, the average was 0 (Ме).
The group of paragangliomas (n=18) included patients of an older age, in this group in only 66.7% cases (n=12) we managed to achieve total shutdown mainly in the carotid body type subtype. In this group in 2 cases coils were used together with NAEM to occlude a large feeding vessel and reduce the bloodflow. In 11.1% of cases, due to the inability to conduct a balloon catheter along convoluted afferents, a Headway microcatheter was used for distal cath-eterization. In the same group, there is a single (4.3%) complication detected by us on magnetic resonance imaging (MRI) in the form of a small area of cerebral ischemia, clinically asymptomatic.
2.2. Illustrative Cases
As a demonstration, we present three clinical cases that most clearly demonstrate the advantages of NAGLEMs compared to other embolic agents.
Case #1
A 35-year-old male patient was admitted to the clinic with complaints on a cosmetic defect in the lower lip area. He has been ill since birth, 18 years ago he was diagnosed with AVM of the lower lip and microsurgical removal was performed. Over the past three years, the growth of formation has been noted. Angiography revealed a relapse of arteriovenous malformation with afferents from the left facial artery (Figure 3). In three years, he underwent sever-al stages of treatment: endovascular embolization with gelatin sponge and embolization with pure ethanol, without effect. The patient underwent endovascular embolization of the AVM of the lower lip with 5 ml of non-adhesive composition Onyx-18. Arteriovenous malformation was shut down totally (Figure 4, Figure 5 and Figure 6). The patient was directed to the next stage of surgical treatment – AVM removal by cosmetic surgeons (Figure 7). mRs score at discharge – 1.
Case #2
A 48-year-old male patient was admitted to the clinic with complaints of a subcutaneous volume formation in the lower jaw area on the left. Earlier in another clinic, an attempt was made to embolize AVM using microcoils. Angiography was performed - filling of the AVM of the soft tissues of the face in the area of the angle of the lower jaw on the left was noted. The presence of separable coils in the afferent from the previous operation was noted, however, the AVM was filled through the coils (Figure 8 and Figure 9). Total embolization of the AVM of the face soft tissues with 7.5 ml of non-adhesive composition Onyx-18 was performed. Arteriovenous malformation was totally shut down (Figure 10). There were no complications. mRs score at discharge – 0.
Case #3
A 58-year-old male patient was admitted to the clinic complaining of a palpable formation in the left submandibu-lar region. When angiogaphywas performed, the filling of the vascular network of the tumor of the left submandib-ular region from the branches of the left occipital artery, as well as the muscular branches of the left vertebral artery was noted (Figure 11). The patient underwent intravascular embolization of paraganglioma with 7.5 ml of non-adhesive composition Onyx-18 (Figure 12 and Figure 13). The vascular network of the paragangliomawas switched off subtotally (Figure 14). There were no complications. mRs score at discharge – 1.
3. Discussion
To date, the following materials are used in the endovascular treatment of hypervascularized formations of the head and neck: micro-spirals, polyvinyl alcohol-based particles, cyanoacrylate-based adhesives and NAGLEMs.
Intravascular embolization of hypervascularized formations of the head and neck in the vast majority of cases is used as a preparatory stage before microsurgical removal, thereby reducing the risks of intraoperative hemorrhagic com-plications, as well as increasing the radicality of the formations removal [9]. The method of preoperative embolization consists in filling of the vascular network of the formation with an embolizing agent in order to stop the blood flow through the main afferents of the formation to facilitate its surgical removal. Due to the presence of a highly developed network of vessels in such formations, the main aim of embolization is to fill the entire volume of the vascular network as much as possible. Most vividly in our series this was demonstrated by the Face AVMs group and case #1. It was the adequate total filling of the entire AVM that allowed the complete removal of the hypervascularized formation and only NAGLEMs were able to cope with this task, previous attempts were unsuccessful. An unfilled part of the vascular network leads to the development of collateral blood flow, thereby increasing the risks of surgical complications, and may probably become a predictor of relapse [3,10]. (An unfilled part of the vascular network of the formation, with insufficient penetration of embolizate into the small vessels of the formation, increases the risks of intraoperative complications, and also leads to the development of collateral blood flow, thereby being a predictor of relapse). Due to the insufficient amount of scientific justification, embolization has not yet been considered as the final method of treatment, however, there are investigations showing the effectiveness of such interventions in high-risk patients [11] Case #2 demonstrated the possibility of total shutdown of the AVM without subsequent removal, i.e. embolization in this case was an independent adequate method of treatment. Previous attempts at embolization with coils also did not lead to filling of the entire vascular network, which NAGLEMs subsequently coped with.
The process of successful embolization of hypervascularized formations depends on many factors, such as the experi-ence of the surgeon, the somatic status of the patient, competent anesthesia manual, equipment of the operating room, but, above all, on the properties of embolizing agents. Currently, there are no randomized studies comparing various embolizing agents in the treatment of hypervascularized formations of the head and neck, however, re-views and articles appear that allow assessing the effect of the properties of agents on the clinical outcome [10].
The method of embolization of hypervascularized formations using microcoils solely is not used, since they can oc-clude only the proximal part of the afferents, while maintaining the filling of the main internal network of the hy-pervascularized formationby the collateral blood flow. There are few reports on the use of microcoils in preoperative embolization of paragangliomas and AVMs of soft tissues of the head. The main described advantage of preopera-tive embolization with microcoils is the ability of palpatory detection of them during surgery and the absence of risks of distal embolism [12], among disadvantages there is a high cost of microcoils [13]. To our opinion, microcoils alone (without NAGLEMs) cannot be used for embolization due to the preservation of blood flow through smaller afferents and microcirculatory network, which was well demonstrated by the AVMof the face group and in case#2.
The method of embolization by particles based on polyvinyl alcohol is based on the gradual introduction of a pre-pared solution of particles of different sizes from 100 to 1000 microns into the vascular network of the neoplasm, from smaller to larger [14].When using this technique, it is almost never possible to embolize the vascular network completely, even with an-giographically complete shutdown of blood flow in the formation, it is necessary to remember about smaller vessels where particles cannot get due to their size [15]. That is the reason why collaterals begin to form, through which the blood supply of the formation continues [16]. According to Pauw BK et al. recanalization of paragangliomas of the jugular foramen area reaches 30% already 9 days after embolization with PVA particles [17].
During embolization, it is necessary to take into account the presence of potentially dangerous anastomoses between ICA and ECA, as well as ECA and VA to prevent undesirable phenomena due to accidental migration of particles. Since PVA particles are X-ray negative, delivery is carried out with an iodine-containing contrast agent [18]. Therefore, after contrast elimination, it is impossible to estimate the pools of probable random migrations [15].
The lack of control of distal embolism, the high frequency of recanalization after embolization, reduced penetration into the tissue (compared with liquid embolizing agents) suggest that the spectrum of application of PVA particles in surgery of hypervascularized formations should be significantly narrowed.
Cyanoacrylate-based adhesives were the first from liquid embolic agents to appear [19]. Rapid polymerization of cyanacrylates (from a few seconds) is the main problem of this group of embolizing agents when filling the vascular network of hypervascularized formations. Often the embolizate does not have time to fill the vascular network of the formation completely before its polymerization [1]. The amount of lipiodol mixed with cyanoacrylate directly affects the polymerization rate, therefore, the degree of dilution is determined by the blood flow rate and the depth to which the penetration of glue is desirable [20]. As a final result, embolization of hypervascularized formations by cyanoacrylates leads to their continued growth due to collaterals located distal to the afferents turned off by glue, and, thus, a dissonance is formed between the absence of afferent vessels available for further embolization and the extensive vascular network of hypervascular-ized formation formed. This was demonstrated in our both groups (both with facial AVM and with paragangliomas) where previous embolizations with cyanoacrylates did not lead to any result. In such situation, there are no emboli-zation possibilities and the treatment of such formations passes to microsurgeons, while the risks of intraoperative bleeding remain. For many years before the advent of non-adhesive compositions, cyanoacrylates remained the only available liquid embolic agents in the treatment of hypervascularized formations of the head and neck.
NAGLEMs (ONYX, SQUID, PHIL) are widely used for intravascular embolization of hypervascularized formations. All of the above NAGLEMs have certain potential advantages and disadvantages. Despite the structural differences, ONYX, Squid and PHIL have similar properties. All three non-adhesive compositions clog blood vessels as a result of “precipitation”, this mechanism is often compared to the solidification of a lava flow [1]. ONYX and Squid consist of three components: EVOH copolymer (ethylene and vinyl alcohol copolymer), micronized tantalum powder and DMSO. Tantalum powder provides the compositions with radiopacity. PHIL consists of two copolymers, polylactide-co-glycolide and polyhydroxyethylmethacrylate, as active components, DMSO and triiodphenol (iodine compounds), the latter covalently bound to two copolymers, which ensures the radiopacity of the agent. DMSO is used as a solvent in all three agents. While cyanoacrylates polymerize over a period of several seconds to several minutes, in non-adhesive compositions, the polymerization mechanism can take up to 30-40 minutes, depending on the size of the embolized blood vessels and the speed of blood flow in them. This aspect provides more controlled embolization, longer injection time and, consequently, better penetration and filling of the target formation, but also contributes to undesirable diffusion into normal arteries. A significant difference between SQUID and ONYX is the smaller size of tantalum powder granules [2,4]. The smaller size of tantalum granules is aimed at increasing the uniformity of radiopacity and improving visibility with longer injections [21].
Compared to ONYX and SQUID, PHIL flows forward more like a column rather than like the above behavior with precipitation from outside to inside. PHIL has a fairly high embolic capacity. Compared to SQUID 18 and Onyx 18, smaller volumes of PHIL are required for the same degree of embolization [19]. All three agents have several versions of different viscosities in their lines (ONYX18, ONYX20 and ONYX34, SQUID12 and SQUID18, PHIL25 PHIL30 PHIL35), which significantly expands the boundaries of their use. De-pending on the speed of the shunting process, the volume of formation, it is possible to select the necessary version of the embolizing agent, which will provide faster and more effective penetration into the target vascular network [19]. In our series detailing the treatment of patients with hypervascularised masses, we were able to develop the concept of curative embolisation through the use of NAGLEM distal penetration into the smallest vessels, along with the distribution of non-adhesive embolytes throughout the tumour stroma. This approach is further exemplified in Case #3 where (Figure 12, Figure 13 and Figure 14) demonstrate its success. This endovascular embolization served as a standalone treatment since the vasculature was entirely disconnected, and the paraganglioma did not necessitate any additional removal.
4. Conclusions
The benefits of using NAGLEMs in treating hypervascularized head and neck neoplasms currently stem from their key characteristics: non-adhesiveness and delayed, predictable polymerization (takes place after 30-40 minutes), efficient dispersion and infiltration through the neoplasm's vascular-distal duct, manageable process control mainly due to the range of embolization viscosities, and outstanding X-ray visualization. Currently, NAGLEMs are the sole effective embolic agents for fully and adequately occluding the vascular bed of hypervascular volumetric masses, taking into consideration all of these characteristics.
5. Materials and Methods
5.1. Study Design
This is a case–control, non-randomized study. The case series was designed to evaluate the effectiveness and results of the use of these NAGLEMs in treatment of patients in our clinic and compare with other emboliс agents. The study was conducted at the North-Western district scientific and clinical center named after L. G. Sokolov Federal Medical and Biological Agency & Almazov National Research Medical Center in St. Petersburg, Russia. Patients were enrolled in the study from November 2015 to May 2023.
We analyzed the technical features, effectiveness and safety of endovascular treatment of two groups of hypervascularized pathological formations localized in the soft tissues of the head and neck in 23 patients operated from 2015 to 2023. The age of the patients ranged from 29 to 76 years and averaged 55 ± 13 (M ± SD) years. In technical features, the type of Squid embolizing agent was evaluated in 12 cases (52.2%), Onyx – in 8 (34.8%), Phil – in 1 (4.3%) or a combination of Onyx+Squid – in 2 (8.7%), the type of delivery microcatheter , of which 91.3% prevailed (n=21) DMSO-compatible balloon catheters Scepter C, XC (Microvention) and microcatheters Headway (Microvention) 8,7% (n=2), respectively. The effec-tiveness was assessed based on the degree of shutdown of the vascular network of formations (total shutdown was achieved in 73.9% (n=17) cases, and subtotal 26.1% (n=6)) and the outcome on the mRs scale, the average of which was 1. Safety was assessed by the presence of complications that developed in 1 case (4.3%), changes in postopera-tive MRI that was performed in all patients at the time of discharge from the clinic.
5.2. NAGLEMs embolization technique
Embolization was carried out according to the following method. After performing angiography in standard projec-tions, afferents to the formation were determined, blood flow was assessed along the anterior and posterior commu-nicant arteries. A DMSO-compatible microcatheter or balloon catheter was inserted into the identified afferents and microangiography was performed, with an assessment of the so-called dangerous anastamoses. Then, through the same catheters and balloons for the delivery of NAGLEMs, embolization of hypervascularized formations was car-ried out with NAGLEMs injection to achieve maximum distal penetration. In cases where only DMSO-compatible microcatheters were used, surgical intervention was lengthened due to the time required for formation due to reflux and the formation of a proximal "plug". In one case coils were used according to the “Pressure Cooker Technique” de-scribed earlier for AVM of the brain [22] . In some cases, a DMSO compatible balloon catheter was installed to protect against cerebral vascular embolism in the internal carotid artery. After the introduction of NAGLEMs, a control angiography was performed, in which the degree of embolization was assessed.
5.3. Statistical analysis
Statistical analysis was carried out using the StatTech v. 3.1.10 program (developed by Stattech LLC Russia).
Quantitative indicators were evaluated for compliance with the normal distribution using the Shapiro-Wilk criterion (with the number of subjects less than 50) or the Kolmogorov-Smirnov criterion (with the number of subjects more than 50).
Quantitative indicators having a normal distribution were described using arithmetic averages (M) and standard deviations (SD), the boundaries of the 95% confidence interval (95% CI).
In the absence of a normal distribution, quantitative data were described using the median (Me) and the lower and upper quartiles (Q1 – Q3).
Categorical data were described with absolute values and percentages. Comparison of the two groups by a quantita-tive indicator having a normal distribution, provided that the variances are equal, was performed using the Student's t-test.
Comparison of three or more groups by a quantitative indicator having a normal distribution was performed using one-factor analysis of variance, a posteriori comparisons were carried out using the Tukey criterion (provided that the variances are equal).
The comparison of the two groups by a quantitative indicator, the distribution of which differed from the normal one, was performed using the Mann-Whitney U-test.
Comparison of three or more groups by a quantitative indicator, the distribution of which differed from the normal one, was performed using the Kraskel-Wallis criterion, a posteriori comparisons were performed using the Dunn criterion with the Hill correction.
The comparison of percentages in the analysis of four-field conjugacy tables was performed using the exact Fisher criterion (with values of the expected phenomenon less than 10).
The comparison of percentages in the analysis of multipole conjugacy tables was performed using Pearson's chi-square criterion. The direction and closeness of the correlation between the two quantitative indicators were assessed using Spearman's rank correlation coefficient (with a distribution of indicators other than normal). A predictive mod-el characterizing the dependence of a quantitative variable on factors was developed using the linear regression method.
The construction of a predictive model of the probability of a certain outcome was carried out using the logistic re-gression method. A measure of certainty indicating the part of the variance that can be explained by logistic regres-sion was the Nigelkirk coefficient R2.
A full statistical analysis can be seen in the Supplementary Materials.
To assess the diagnostic significance of quantitative signs in predicting a certain outcome, the method of analysis of ROC curves was used. The separating value of the quantitative attribute at the cut-off point was determined by the highest value of the Yuden index. An analysis of the available literature was also performed. The Pubmed library was searched for articles using following key-words: "AVM of the head and neck, embolization of extracranial AVMs, embolization of paragangliomas, embolic agent". Criteria for articles inclusion: a series of patients with hypervas-cularized formations of the head and neck and the use of embolizing agents in their treatment. The exclusion criteria were: percutaneous embolization. A total of 7 articles were selected [14,23,24,25,26,27,28].
Author Contributions
Conceptualization, A.P. (Andrey Petrov), A.I. and U.S.; data curation, US, A.P.(Andrey Petrov), A.I. and A.P. (Anna Petrova); formal analysis, E.K., N.T. and A.P. (Anna Petrova); investigation, A.P. (Andrey Petrov), A.P. (Anna Petrova) and A.I.; methodology, L.R.; project administration, A.I., U.S.. and A.P. (Andrey Petrov); supervision, L.R. and A.P. (Andrey Petrov); writing—original draft, A.P. (Andrey Petrov), E.K, N.T. and A.I.; writing—review and editing, L.R., A.P. (Andrey Petrov), A.I. and U.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
References
- Pal, A.; Blanzy, J.; Gómez, K.J.R.; Preul, M.C.; Vernon, B.L. Liquid Embolic Agents for Endovascular Embolization: A Review. Gels 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- Petrov, A.; Ivanov, A.; Rozhchenko, L.; Petrova, A.; Bhogal, P.; Cimpoca, A.; Henkes, H. Endovascular Treatment of Chronic Subdural Hematomas through Embolization: A Pilot Study with a Non-Adhesive Liquid Embolic Agent of Minimal Viscosity (Squid). J Clin Med 2021, 10, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Petrov, A.E.; Rozhchenko, L.V.; Ivanov, A.A.; Bobinov, V.V.; Henkes, H. The First Experience of Endovascular Treatment of Chronic Subdural Hematomas with Non-Adhesive Embolization Materials of Various Viscosities: Squid 12 and 18. Voprosy neirokhirurgii imeni N.N. Burdenko 2021, 85, 80. [Google Scholar] [CrossRef]
- Petrov, A.; Ivanov, A.; Dryagina, N.; Petrova, A.; Samochernykh, K.; Rozhchenko, L. Angiogenetic Factors in Chronic Subdural Hematoma Development. Diagnostics (Basel) 2022, 12, 2787. [Google Scholar] [CrossRef] [PubMed]
- Cortivo, F.D.; Diallo, R.; Preudhomme, R.; Coulibaly, A.; Salami, A.; Benateau, H. Exclusive Surgical Approach for Facial Arteriovenous Malformations in Precarious Conditions. J Stomatol Oral Maxillofac Surg 2022, 123, e549–e555. [Google Scholar] [CrossRef]
- Pedreira, R.; Lopez, J.; Ostrander, B.T.; Pearl, M.; Puttgen, K.; Tekes, A.; Dorafshar, A.H. An Interdisciplinary Approach to Treatment of Adult Facial Arteriovenous Malformations: A Review of the Literature and A Single Institution’s Experience With “Late” Surgical Resection and Aesthetic Reconstruction. J Craniofac Surg 2019, 30, 1635–1639. [Google Scholar] [CrossRef]
- Zheng, L.; Su, L.; Wang, D.; Wang, Z.; Wen, M.; Yang, X.; Han, Y.; Li, X.; Fan, X.; Tao, X. Ethanol Embolization of Lingual Arteriovenous Malformations: Positive Experience in 52 Patients during 11 Years. J Vasc Surg 2020, 72, 651–657. [Google Scholar] [CrossRef]
- Garg, K.; Singh, M. Role of Stereotactic Radiosurgery in Skull Base Paragangliomas - A Narrative Review. Neurol India 2023, 71, S153–S160. [Google Scholar] [CrossRef]
- Li, N.; Wan, Y.; Chen, W.; Yang, J.; Chang, G.; Huang, Y. Beneficial Effects of Preoperative Superselective Embolization on Carotid Body Tumor Surgery: A 13-Year Single-Center Experience. Front Oncol 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Graham, N.J.; Smith, J.D.; Else, T.; Basura, G.J. Paragangliomas of the Head and Neck: A Contemporary Review. Endocrine oncology (Bristol, England) 2022, 2, R153–R162. [Google Scholar] [CrossRef] [PubMed]
- Kocur, D.; Ślusarczyk, W.; Przybyłko, N.; Hofman, M.; Jamróz, T.; Suszyński, K.; Baron, J.; Kwiek, S. Endovascular Approach to Glomus Jugulare Tumors. Pol J Radiol 2017, 82, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Janakiram, T.N.; Nadakkavukaran, J.; Bhatia Sharma, S.; Sathyanarayanan, J.D. A Hybrid Approach Towards Successful Resection of a Huge Carotid Body Paraganglioma Using Coil Embolization and Traditional Surgical Techniques. Indian J Otolaryngol Head Neck Surg 2019, 71, 136–139. [Google Scholar] [CrossRef]
- Cvjetko, I.; Erdelez, L.; Podvez, Z.; Buhin, M.; Vidjak, V.; Borovecki, A.; Cvjetko, T.; Grsic, K. Coil Embolization and Surgical Removal of Carotid Body Paraganglioma. J Craniofac Surg 2013, 24, e242–e245. [Google Scholar] [CrossRef] [PubMed]
- White, J.B.; Link, M.J.; Cloft, H.J. Endovascular Embolization of Paragangliomas: A Safe Adjuvant to Treatment. J Vasc Interv Neurol 2008, 1, 37–41. [Google Scholar]
- Helal, A.; Vakharia, K.; Brinjikji, W.; Carlson, M.L.; Driscoll, C.L.W.; Van Gompel, J.J.; Link, M.J.; Cloft, H. Preoperative Embolization of Jugular Paraganglioma Tumors Using Particles Is Safe and Effective. Interv Neuroradiol 2022, 28, 145–151. [Google Scholar] [CrossRef]
- Valavanis, A. Preoperative Embolization of the Head and Neck: Indications, Patient Selection, Goals, and Precautions. AJNR Am J Neuroradiol 1986, 7, 943–952. [Google Scholar] [PubMed]
- Pauw, B.K.H.; Makek, M.S.; Fisch, U.; Valavanis, A. Preoperative Embolization of Paragangliomas (Glomus Tumors) of the Head and Neck: Histopathologic and Clinical Features. Skull Base Surg 1993, 3, 37–44. [Google Scholar] [CrossRef]
- Fang, Q.R.; He, X.Y.; Li, X.F.; Zhang, X.; Chen, M.; Li, H.; Li, W.; Wang, Z.Q.; Duan, C.Z. Comparative Efficacy of Glubran and Polyvinyl-Alcohol Particles in the Embolization of Meningiomas. Int J Neurosci 2016, 126, 1112–1119. [Google Scholar] [CrossRef]
- Vollherbst, D.F.; Chapot, R.; Bendszus, M.; Möhlenbruch, M.A. Glue, Onyx, Squid or PHIL? Liquid Embolic Agents for the Embolization of Cerebral Arteriovenous Malformations and Dural Arteriovenous Fistulas. Clin Neuroradiol 2022, 32, 25–38. [Google Scholar] [CrossRef]
- Zaki Ghali, M.G.; Kan, P.; Britz, G.W. Curative Embolization of Arteriovenous Malformations. World Neurosurg 2019, 129, 467–486. [Google Scholar] [CrossRef]
- Mason, J.R.; Dodge, C.; Benndorf, G. Quantification of Tantalum Sedimentation Rates in Liquid Embolic Agents. Interv Neuroradiol 2018, 24, 574–579. [Google Scholar] [CrossRef]
- Chapot, R.; Stracke, P.; Velasco, A.; Nordmeyer, H.; Heddier, M.; Stauder, M.; Schooss, P.; Mosimann, P.J. The Pressure Cooker Technique for the Treatment of Brain AVMs. Journal of Neuroradiology 2014, 41, 87–91. [Google Scholar] [CrossRef]
- Kalani, M.Y.S.; Ducruet, A.F.; Crowley, R.W.; Spetzler, R.F.; McDougall, C.G.; Albuquerque, F.C. Transfemoral Transarterial Onyx Embolization of Carotid Body Paragangliomas. Neurosurgery 2013, 72, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Case, D.; Folzenlogen, Z.; Rochon, P.; Kumpe, D.; Roark, C.; Seinfeld, J. Embolization of Head and Neck Vascular Malformations Using Serial Arterial Embolization Followed by Dominant Arterial Embolization with Two Microcatheter Technique. J Vasc Interv Neurol 2018, 10, 47–51. [Google Scholar]
- Lilje, D.; Wiesmann, M.; Hasan, D.; Ridwan, H.; Hölzle, F.; Nikoubashman, O. Interventional Embolization Combined with Surgical Resection for Treatment of Extracranial AVM of the Head and Neck: A Monocentric Retrospective Analysis. PLoS One 2022, 17, e0273018. [Google Scholar] [CrossRef]
- Michelozzi, C.; Januel, A.C.; Cuvinciuc, V.; Tall, P.; Bonneville, F.; Fraysse, B.; Deguine, O.; Serrano, E.; Cognard, C. Arterial Embolization with Onyx of Head and Neck Paragangliomas. J Neurointerv Surg 2016, 8, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Catapano, J.S.; Almefty, R.O.; Ding, D.; Whiting, A.C.; Pines, A.R.; Richter, K.R.; Ducruet, A.F.; Albuquerque, F.C. Onyx Embolization of Skull Base Paragangliomas: A Single-Center Experience. Acta Neurochir (Wien) 2020, 162, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Wang, D.; Han, Y.; Wang, Z.; Zheng, L.; Fan, X. Absolute Ethanol Embolization of Infiltrating-Diffuse Extracranial Arteriovenous Malformations in the Head and Neck. Eur J Vasc Endovasc Surg 2015, 50, 114–121. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Analysis of Embolisation by other agents conditioning on Groups.
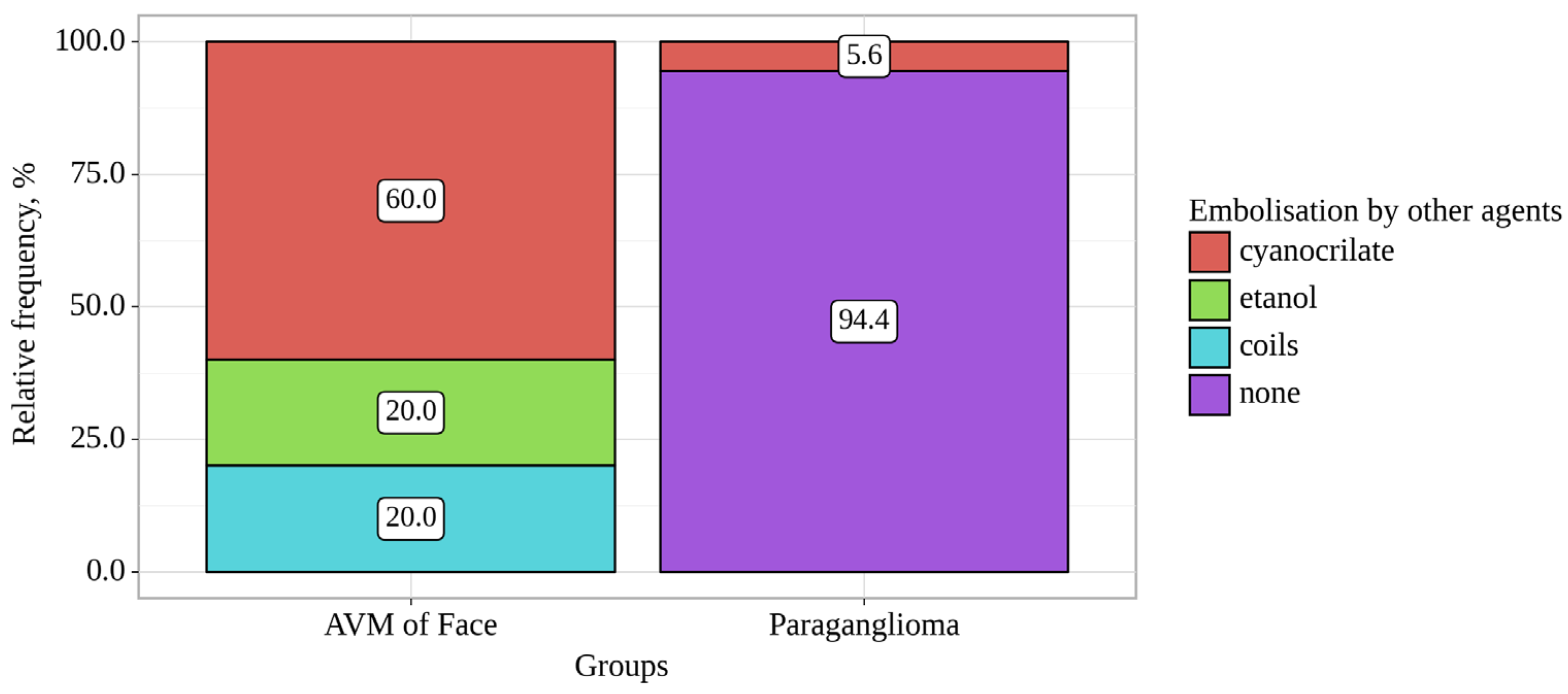
Figure 2.
Analysis of Time of embolisation conditioning on Groups.
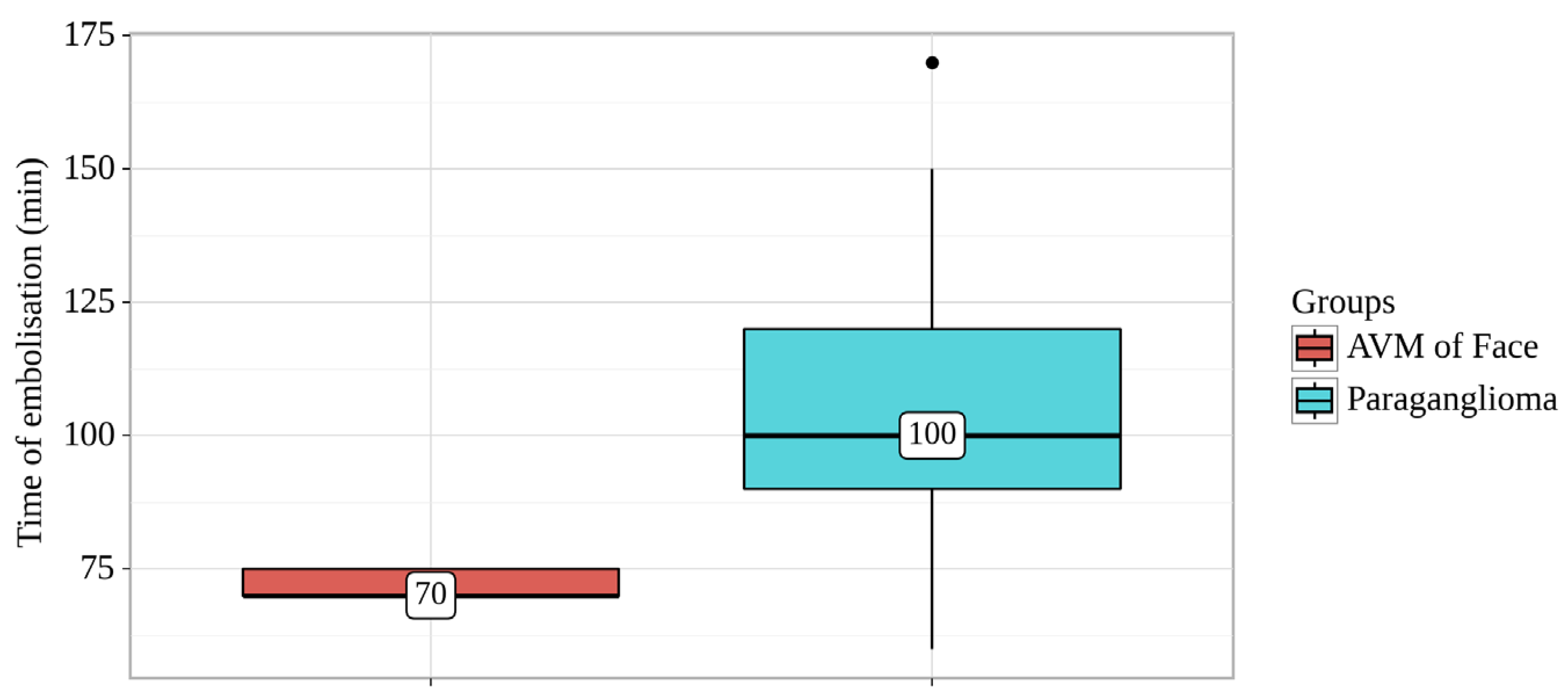
Figure 3.
Digital subtraction angiography from the facial arteries: a, b – straight and lateral projections on the left; c, d – straight and lateral projections on the right (white arrows indicate catheters at the ostium of the facial arteries, black long arrows indicate filling of the lower lip AVM, black short arrow indicates the afferent AVM from the left facial artery). There is filling of the AVM from the afferent from the left facial artery.
Figure 3.
Digital subtraction angiography from the facial arteries: a, b – straight and lateral projections on the left; c, d – straight and lateral projections on the right (white arrows indicate catheters at the ostium of the facial arteries, black long arrows indicate filling of the lower lip AVM, black short arrow indicates the afferent AVM from the left facial artery). There is filling of the AVM from the afferent from the left facial artery.
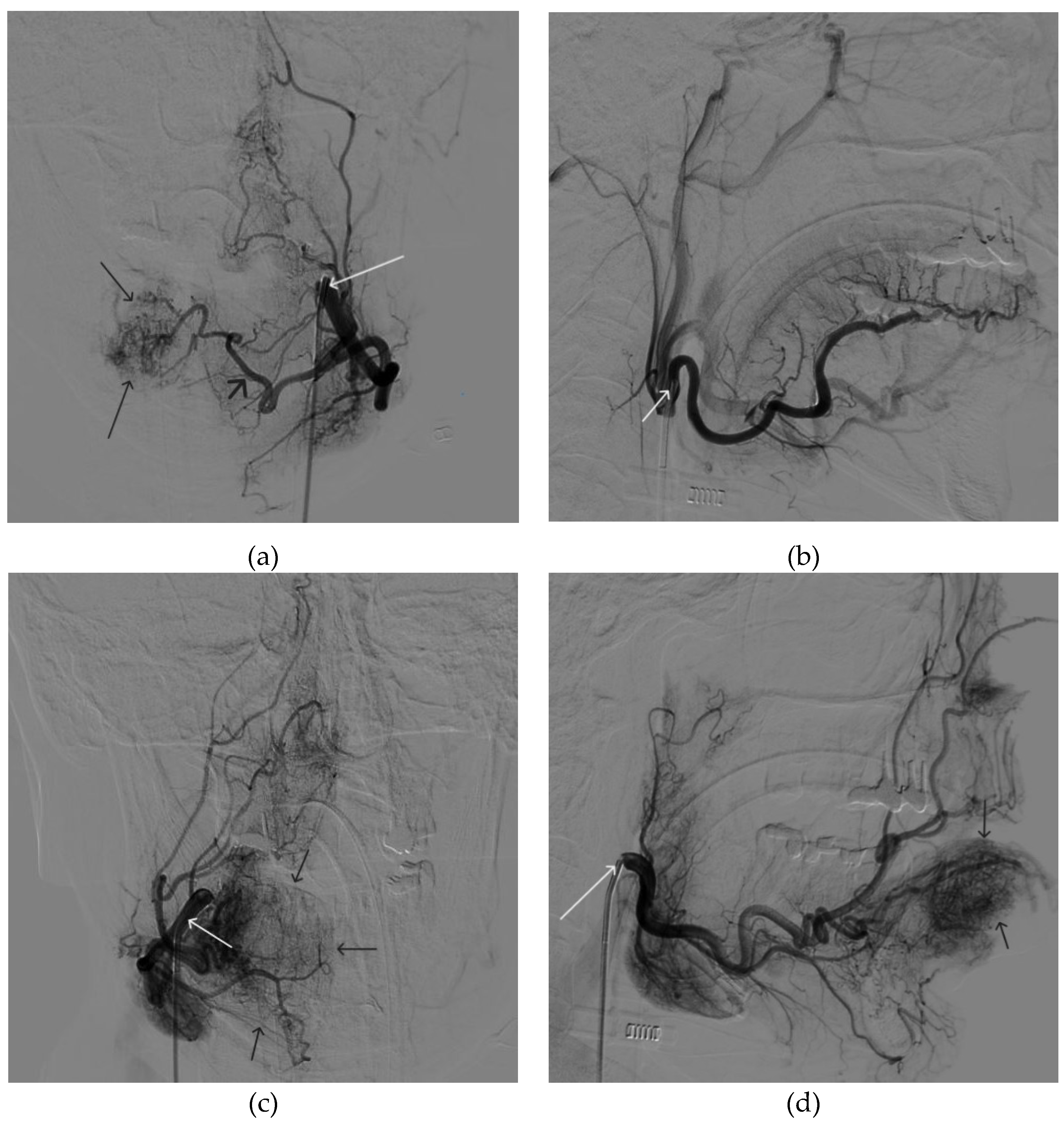
Figure 4.
The process of introducing Onyx-18 into the AVM of the lower lip (the white arrow indicates the microcatheter, the black arrow indicates the spread of embolizate along the vascular network of the formation).
Figure 4.
The process of introducing Onyx-18 into the AVM of the lower lip (the white arrow indicates the microcatheter, the black arrow indicates the spread of embolizate along the vascular network of the formation).
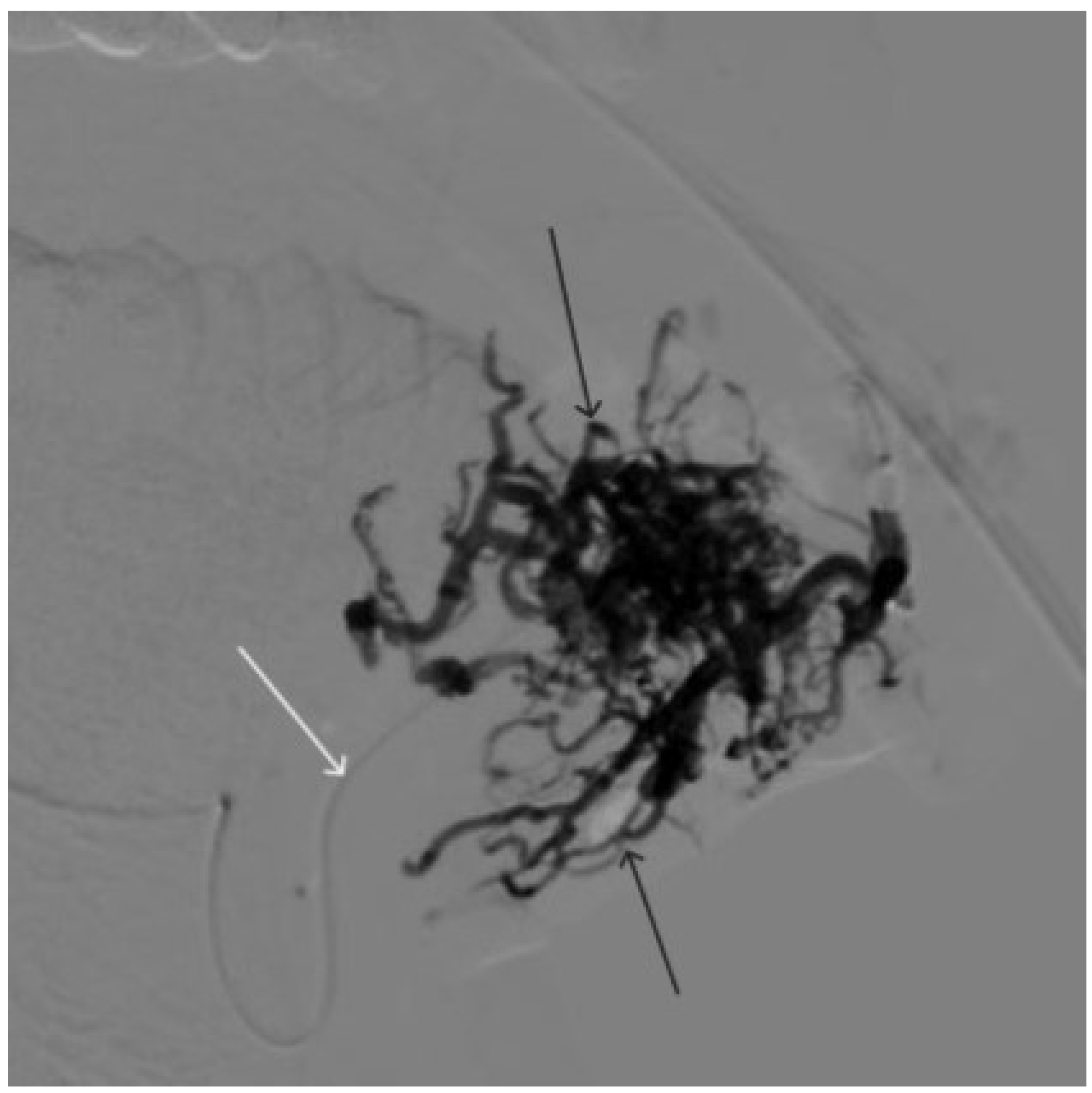
Figure 5.
X-ray in single shot mode. The NAGLEMs cast is visualized, filling the vascular network (the white arrow indicates the guiding catheter at the ostium of the left facial artery, the black arrow indicates the karst).
Figure 5.
X-ray in single shot mode. The NAGLEMs cast is visualized, filling the vascular network (the white arrow indicates the guiding catheter at the ostium of the left facial artery, the black arrow indicates the karst).
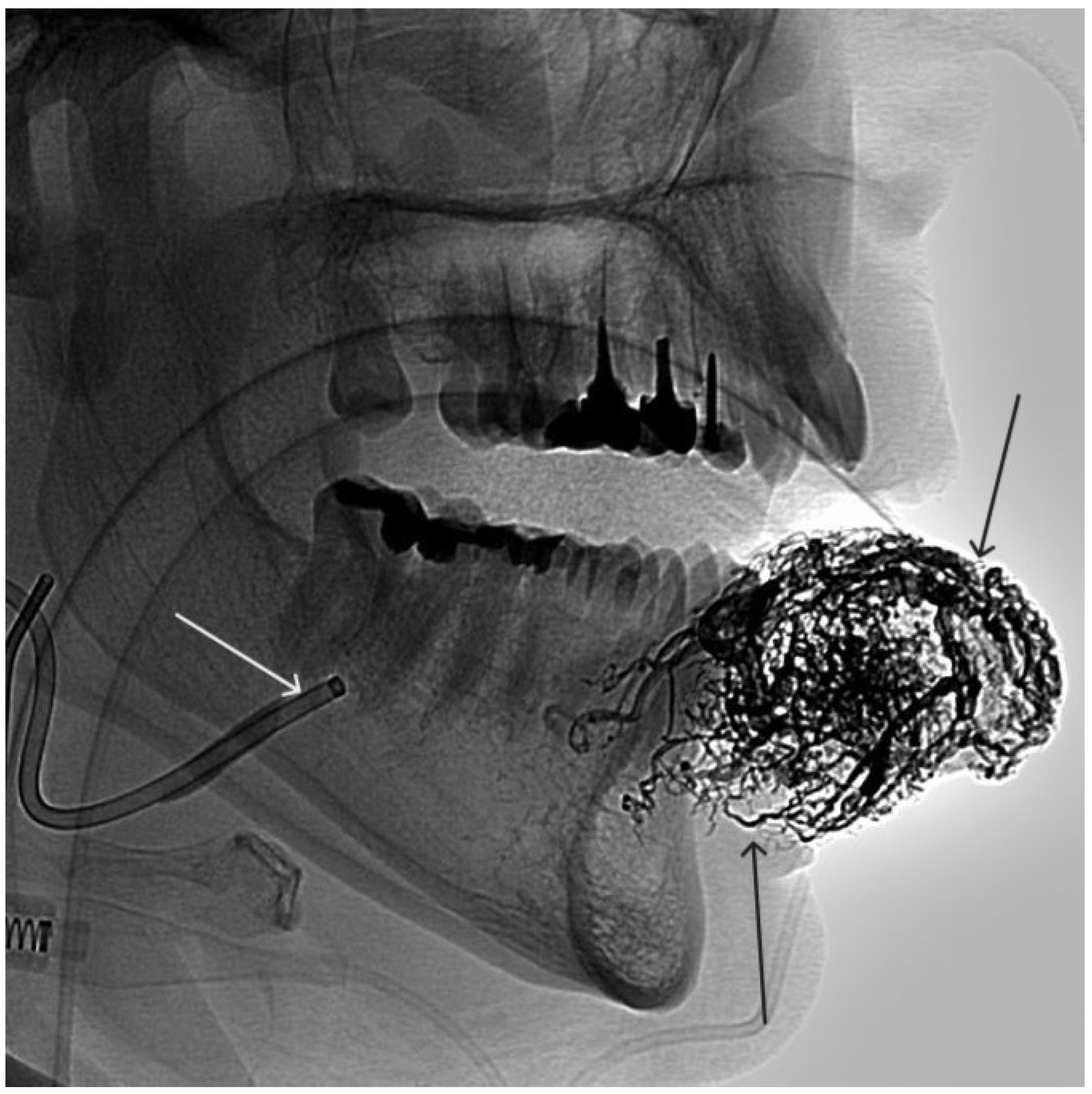
Figure 6.
Digital subtraction angiography from the right and left facial arteries: a - direct projection; b - lateral projection (white arrows indicate catheters at the ostium of the facial arteries, black arrows indicate embolizate karst). The absence of AVM contrast is noted.
Figure 6.
Digital subtraction angiography from the right and left facial arteries: a - direct projection; b - lateral projection (white arrows indicate catheters at the ostium of the facial arteries, black arrows indicate embolizate karst). The absence of AVM contrast is noted.
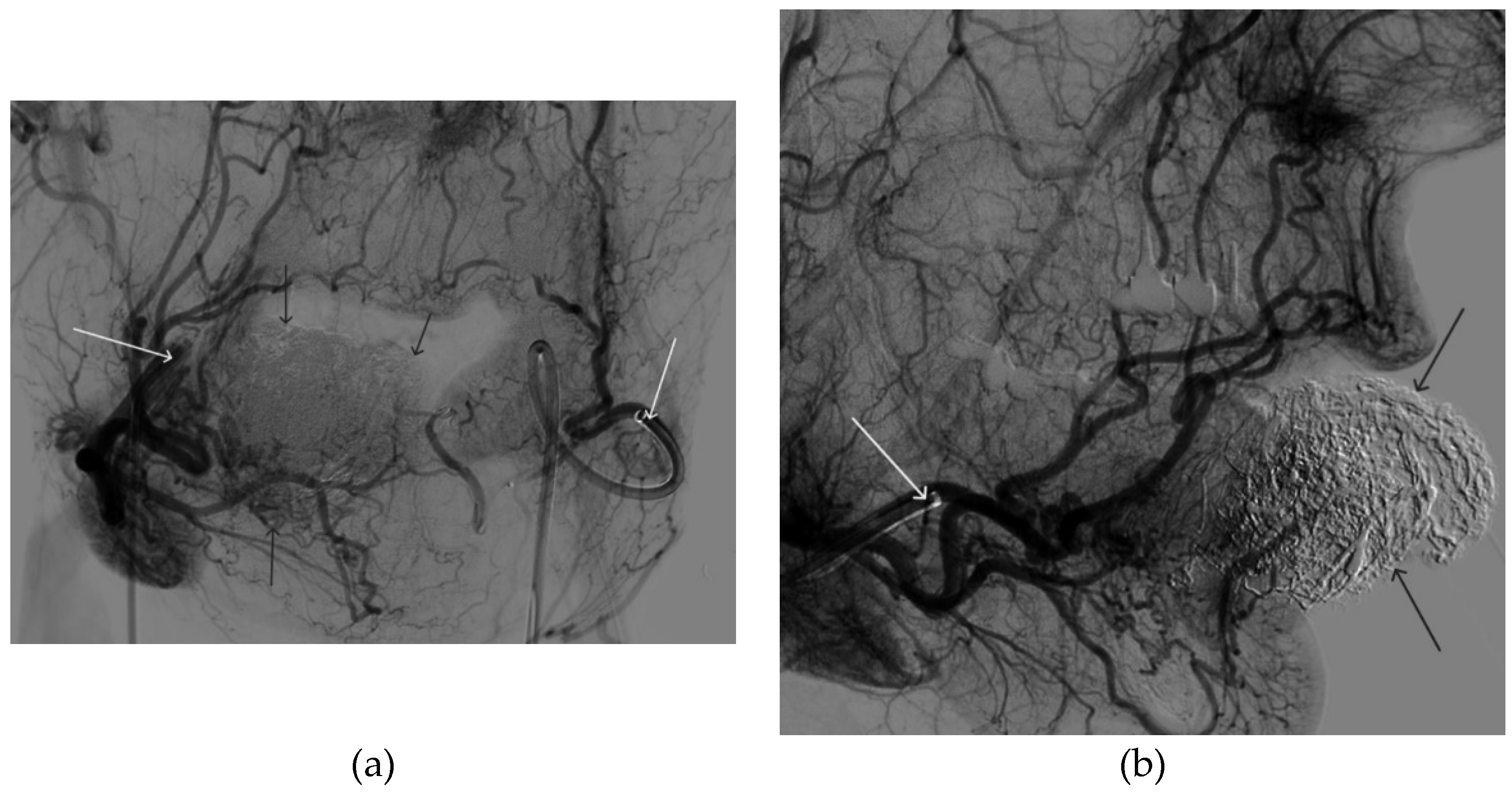
Figure 7.
a - The appearance of the AVM before embolization, b - the appearance of the AVM after embolization, c - the patient after surgical removal of the AVM.
Figure 7.
a - The appearance of the AVM before embolization, b - the appearance of the AVM after embolization, c - the patient after surgical removal of the AVM.
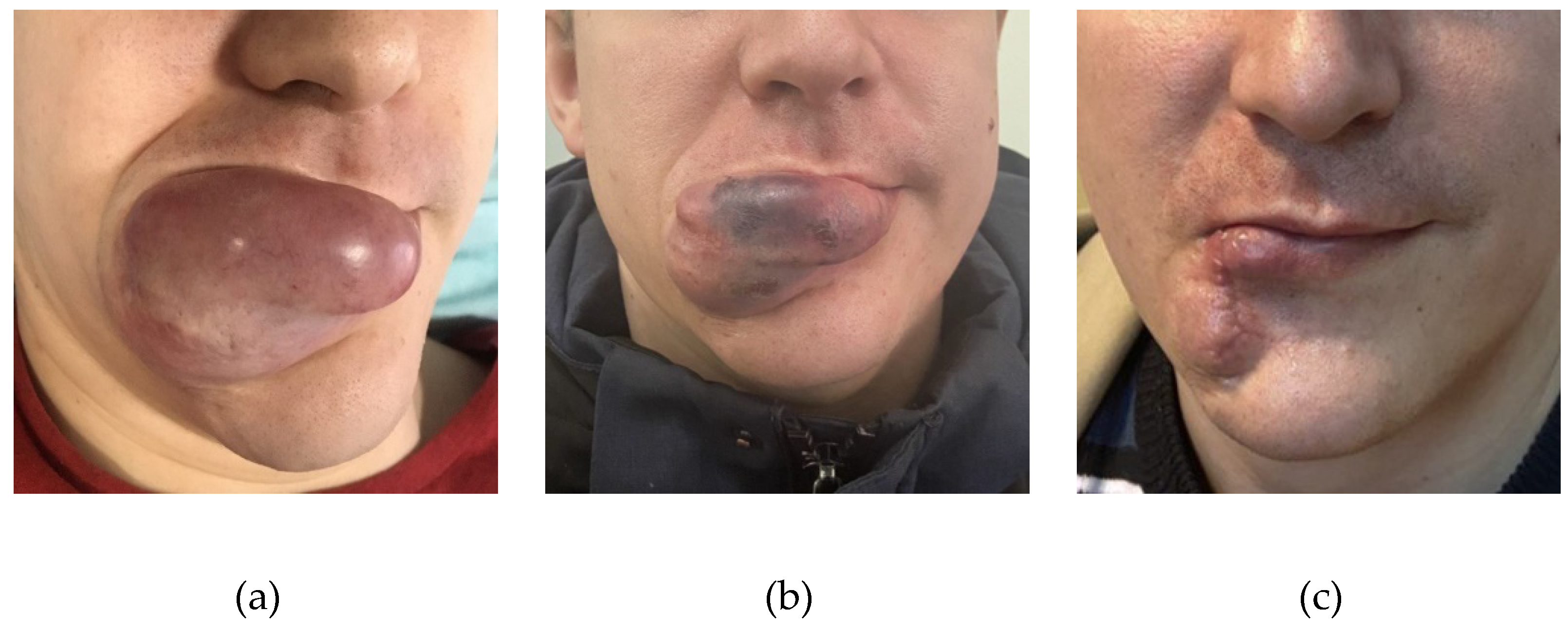
Figure 8.
Digital subtraction angiography from the left external carotid artery, direct projection (white arrow indicates catheter in the left external carotid artery, black arrows indicate contrast AVM.
Figure 8.
Digital subtraction angiography from the left external carotid artery, direct projection (white arrow indicates catheter in the left external carotid artery, black arrows indicate contrast AVM.
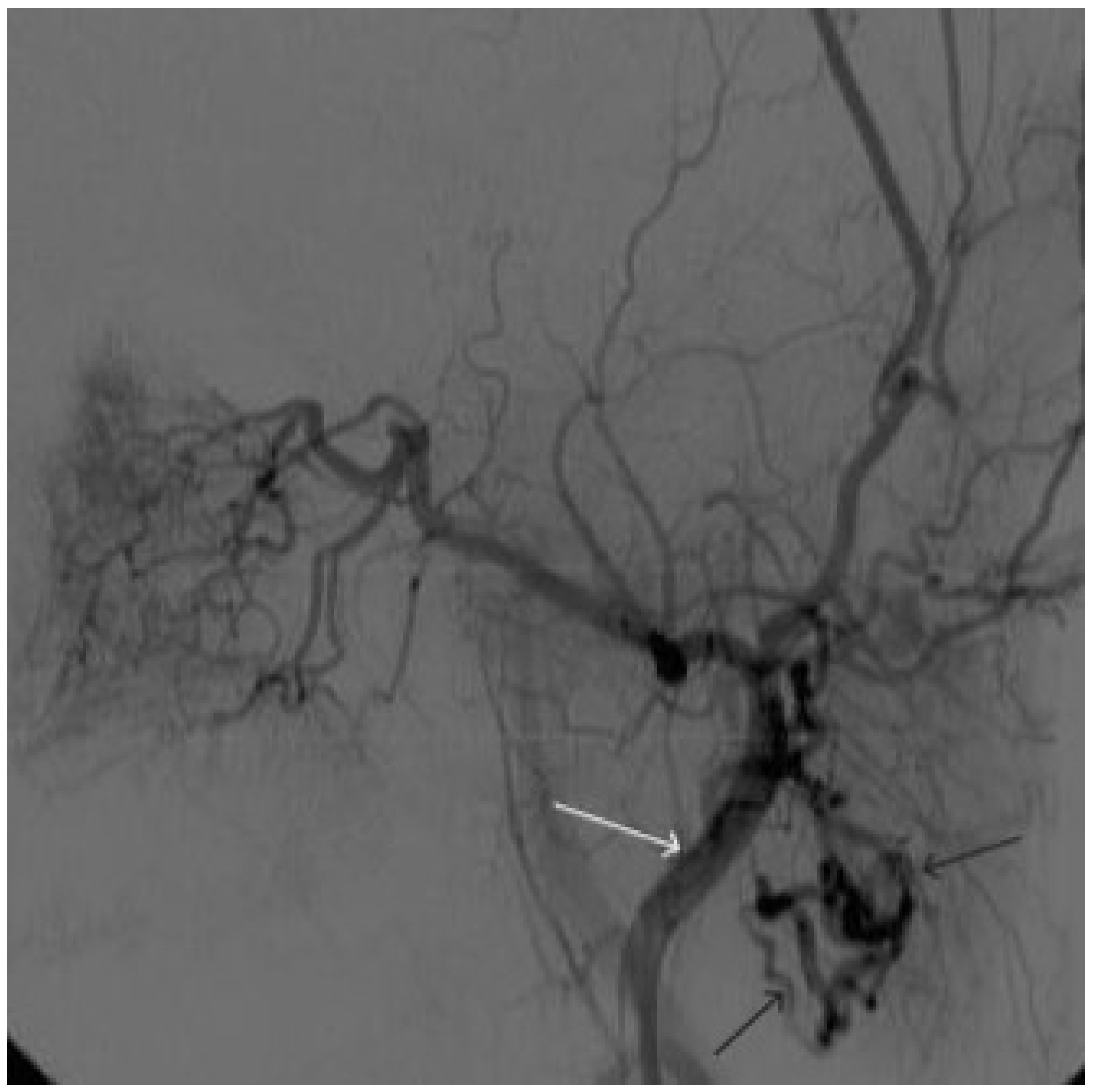
Figure 9.
X-ray, direct projection (the white arrow indicates a microcatheter in the left external carotid artery, the black arrows indicate a complex of microcoils from the previous stage of embolization.
Figure 9.
X-ray, direct projection (the white arrow indicates a microcatheter in the left external carotid artery, the black arrows indicate a complex of microcoils from the previous stage of embolization.
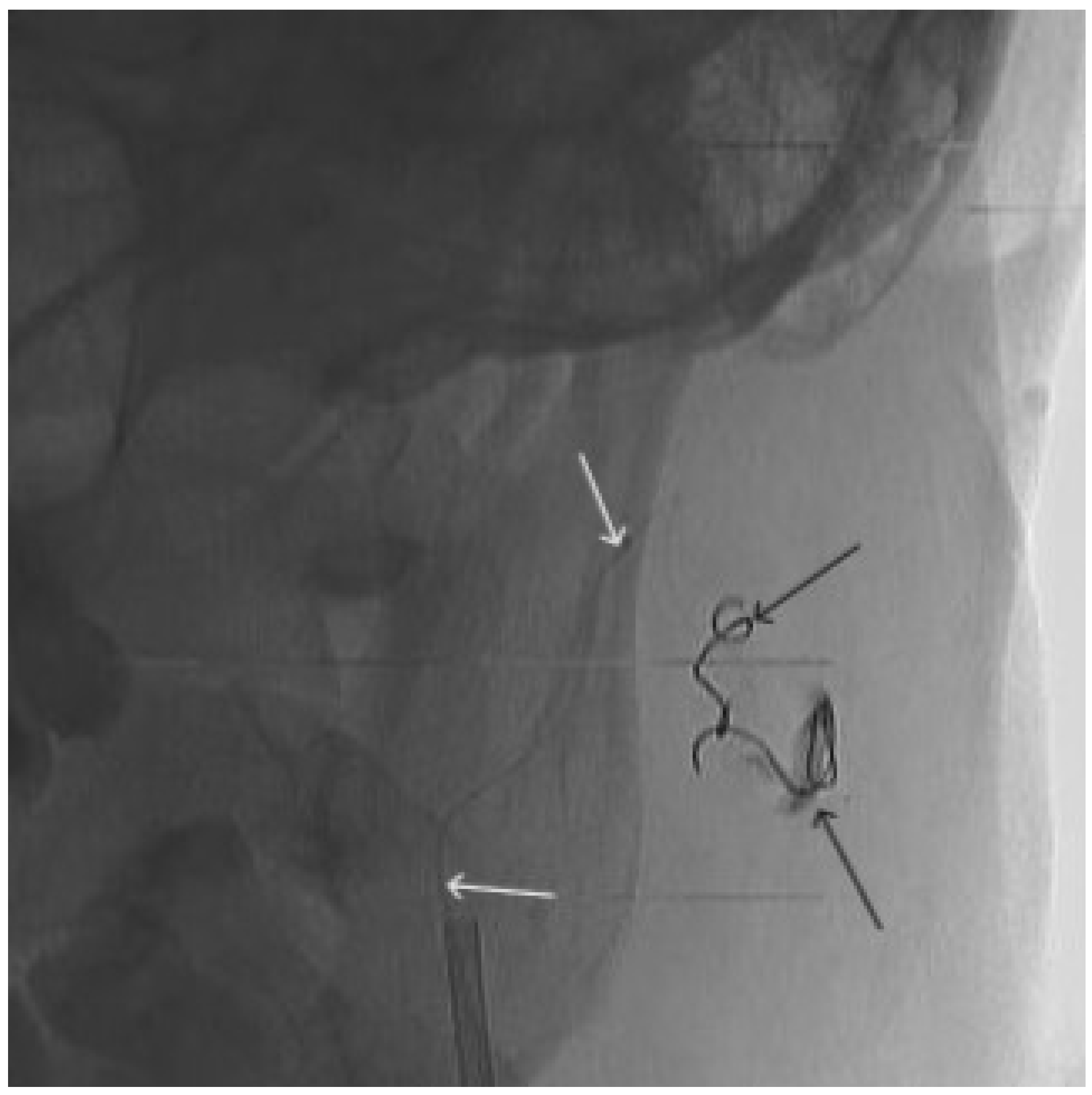
Figure 10.
Digital subtraction angiography from the left external carotid artery, direct projection (white arrow indicates the left external carotid artery, black arrows indicate the boundaries of the filled AVM).
Figure 10.
Digital subtraction angiography from the left external carotid artery, direct projection (white arrow indicates the left external carotid artery, black arrows indicate the boundaries of the filled AVM).
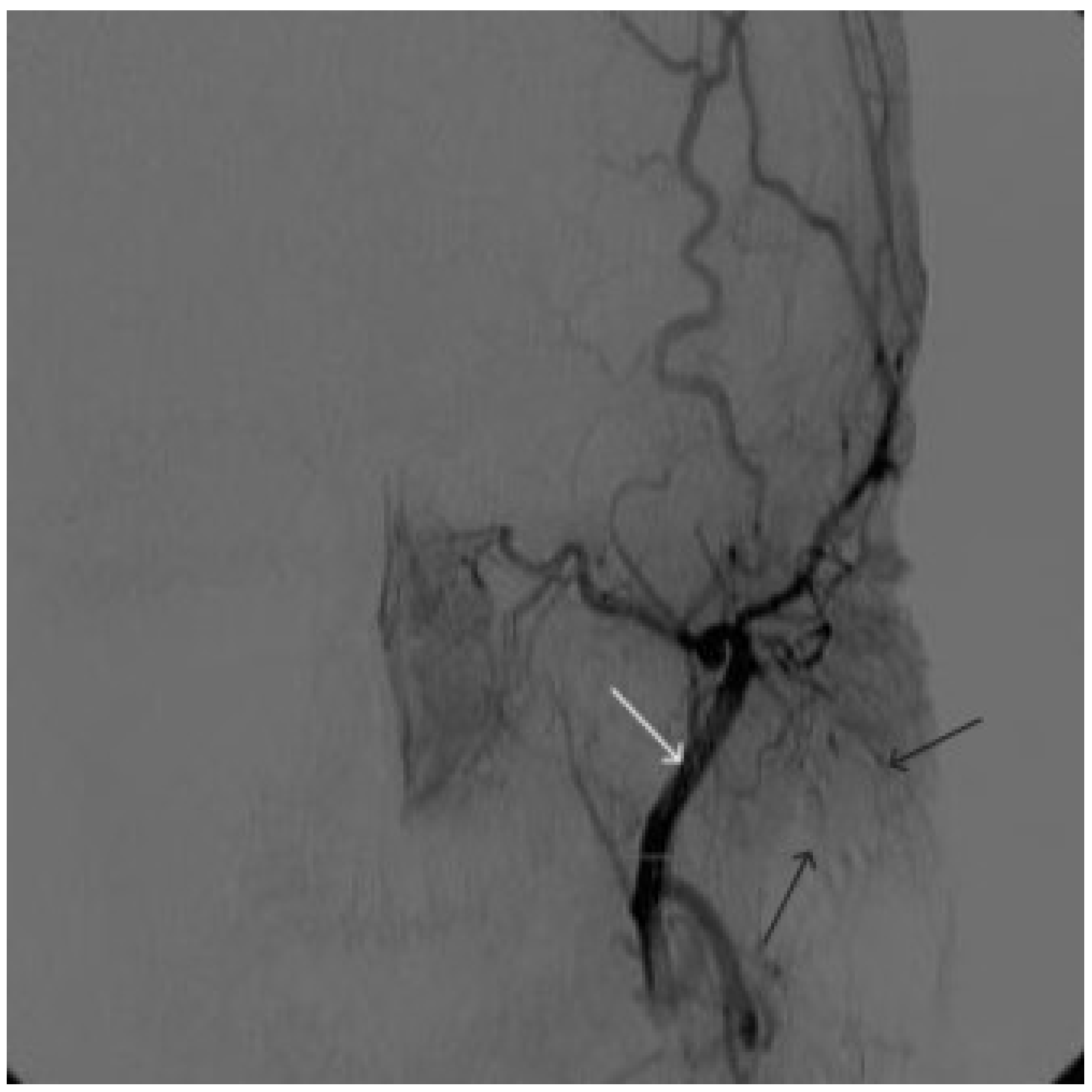
Figure 11.
Digital subtraction angiography from the left common carotid artery: a – direct projection, b - lateral projection (white arrows indicate the left internal carotid artery, long black arrows indicate the external carotid artery, short black arrows indicate the boundaries of the paraganglioma).
Figure 11.
Digital subtraction angiography from the left common carotid artery: a – direct projection, b - lateral projection (white arrows indicate the left internal carotid artery, long black arrows indicate the external carotid artery, short black arrows indicate the boundaries of the paraganglioma).
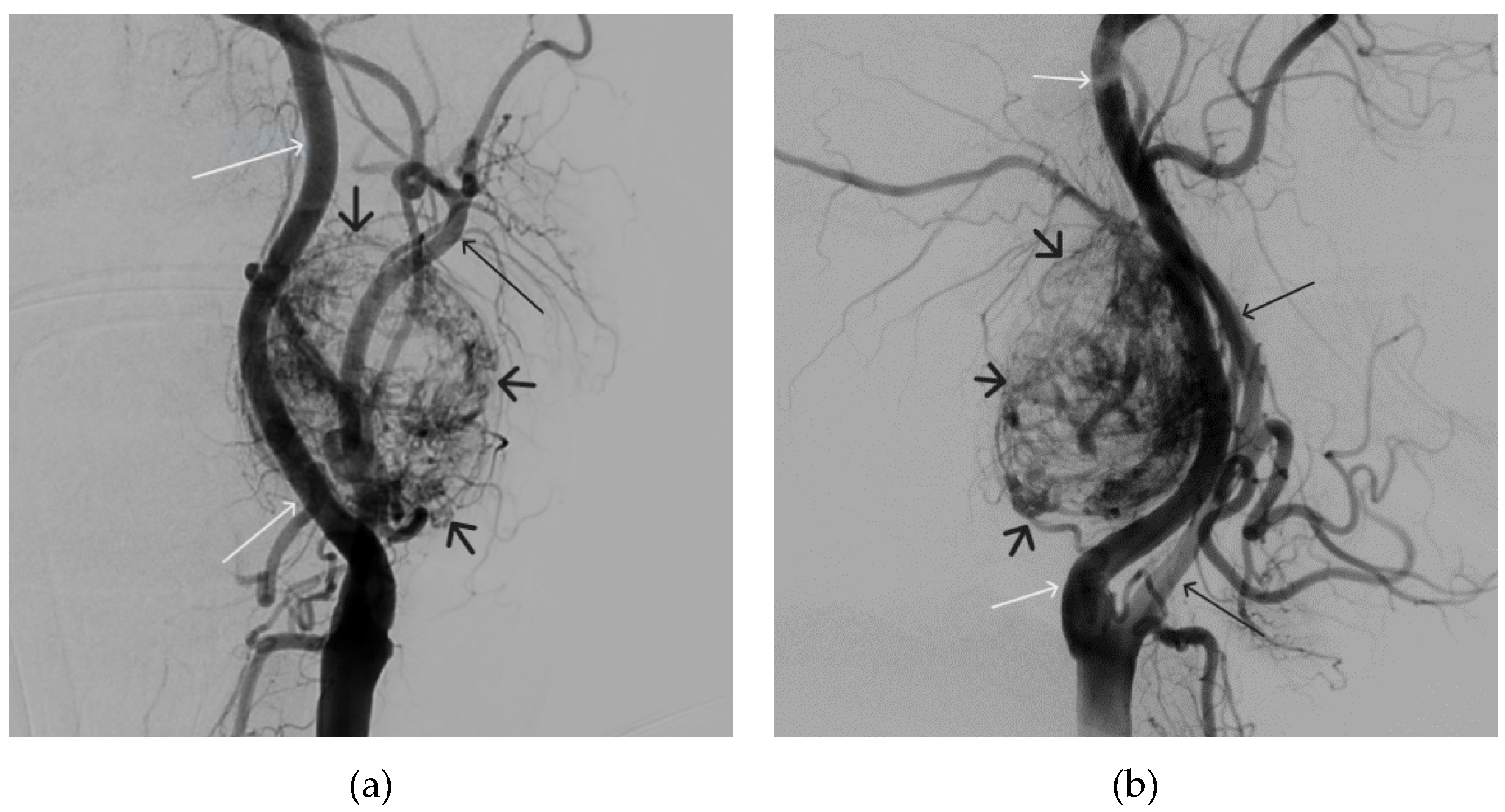
Figure 12.
Distribution of Onyx-18 along the vascular network of the paraganglioma: a – direct projection, b - lateral projection (white arrows indicate filling of the vascular network of the paraganglioma, black arrows indicate an inflated balloon in the left internal carotid artery).
Figure 12.
Distribution of Onyx-18 along the vascular network of the paraganglioma: a – direct projection, b - lateral projection (white arrows indicate filling of the vascular network of the paraganglioma, black arrows indicate an inflated balloon in the left internal carotid artery).
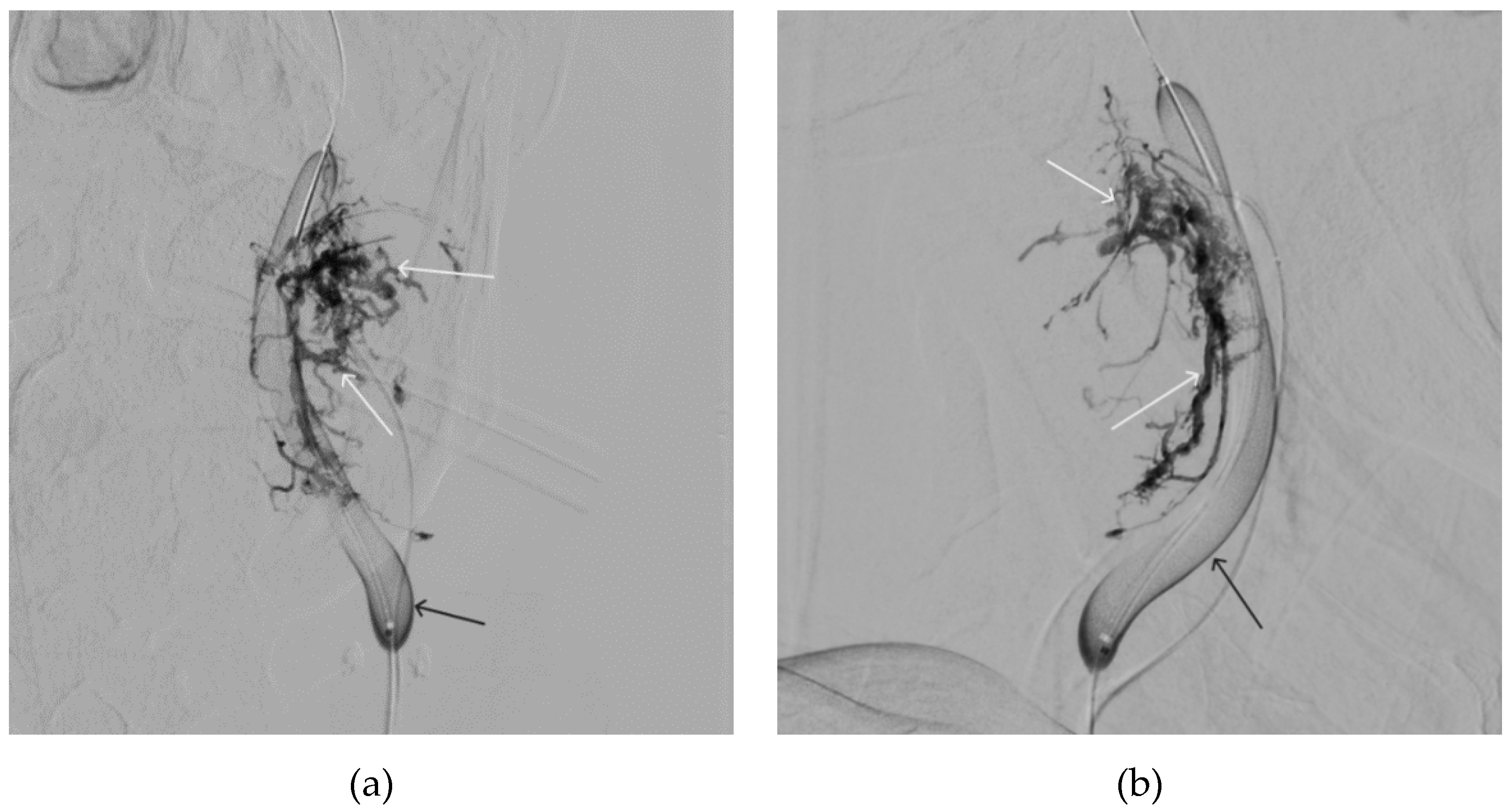
Figure 13.
X-ray in single shot mode. a, b and c – demonstrate gradual spreading of Onyx-18 (NAGLEMs cast) through the vascular network of the paraganglioma direct projections (black arrows indicate filling of the vascular network of the paraganglioma, white arrows indicate an inflated balloon in the left internal carotid artery).
Figure 13.
X-ray in single shot mode. a, b and c – demonstrate gradual spreading of Onyx-18 (NAGLEMs cast) through the vascular network of the paraganglioma direct projections (black arrows indicate filling of the vascular network of the paraganglioma, white arrows indicate an inflated balloon in the left internal carotid artery).
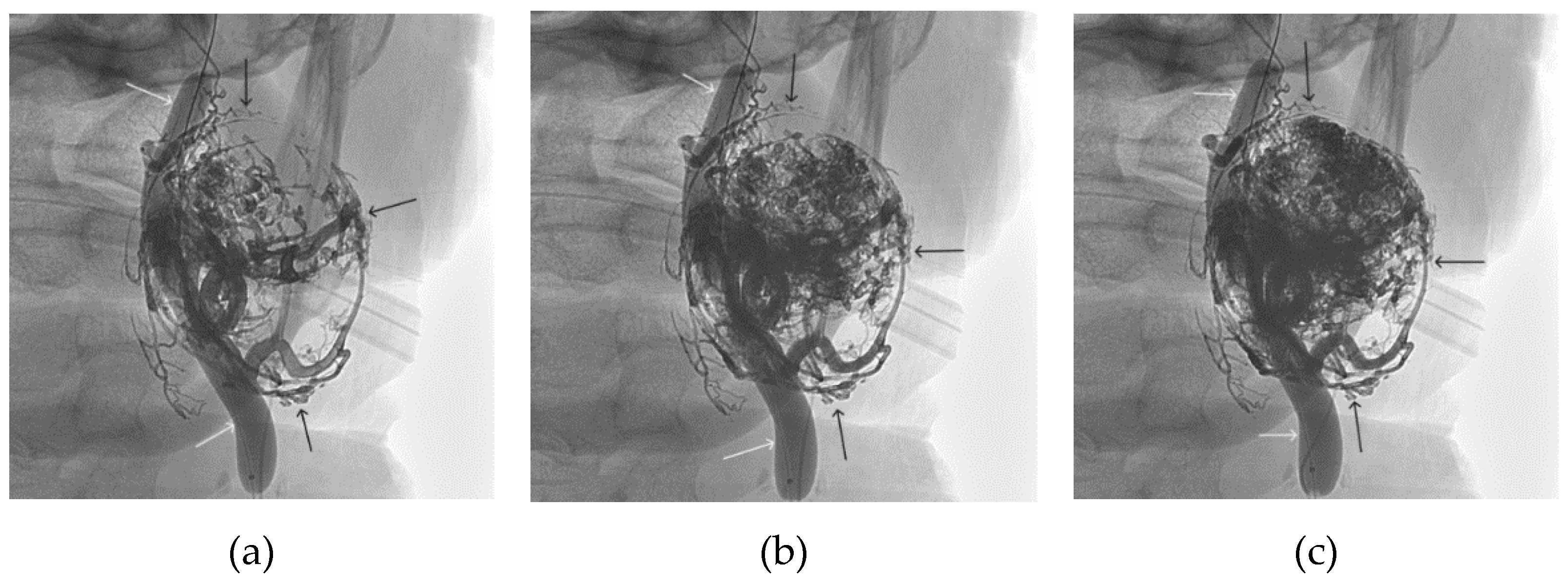
Figure 14.
Digital subtraction angiography from the left common carotid artery: a – direct projection, b - lateral projection (white arrows indicate the guiding catheter in the left external carotid artery, black arrows indicate the boundaries of the embolized paraganglioma).
Figure 14.
Digital subtraction angiography from the left common carotid artery: a – direct projection, b - lateral projection (white arrows indicate the guiding catheter in the left external carotid artery, black arrows indicate the boundaries of the embolized paraganglioma).
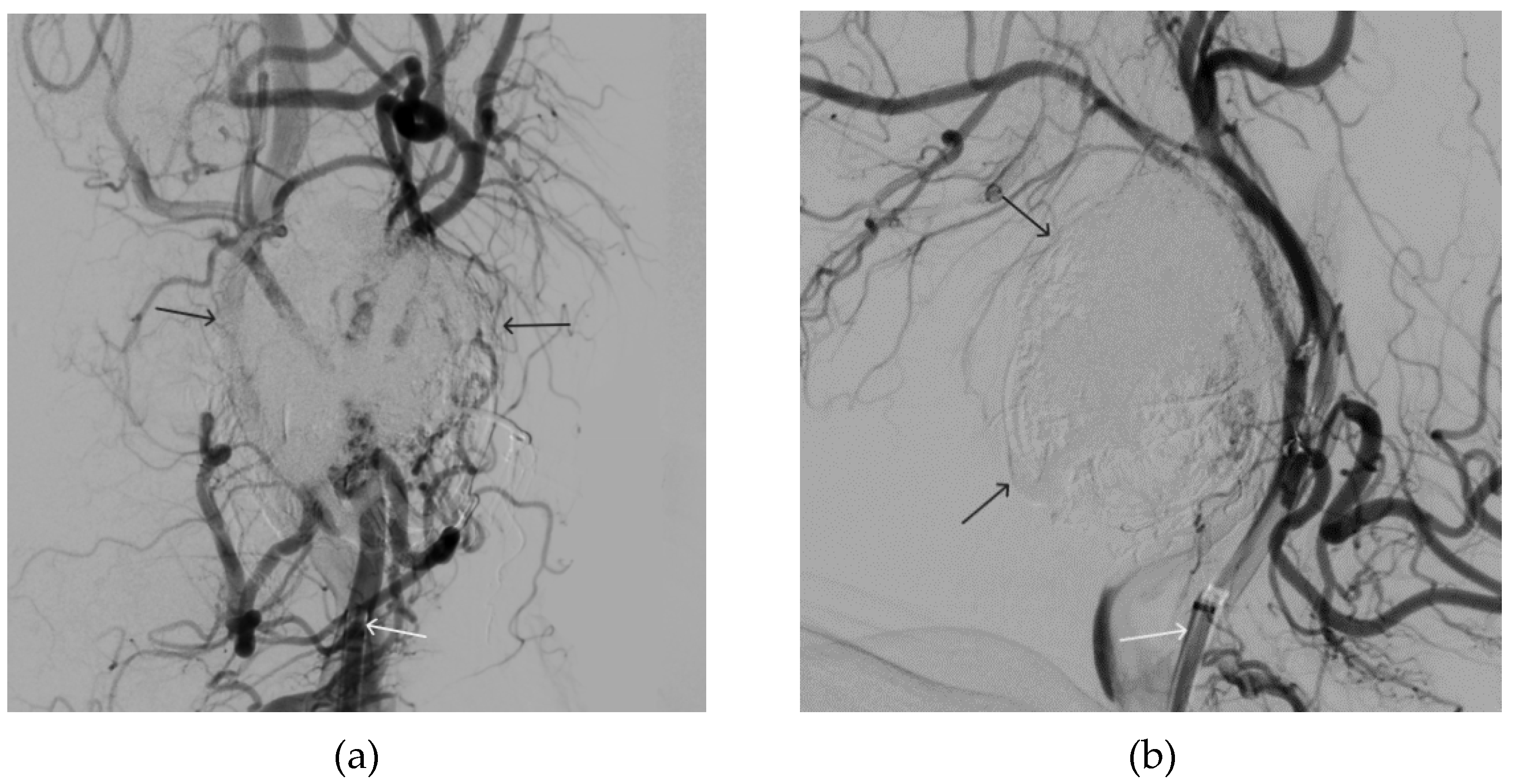

Table 1.
Summary of the demographic and treatment data of two patient groups treated by NAGLEMs embolisation.
Table 1.
Summary of the demographic and treatment data of two patient groups treated by NAGLEMs embolisation.
| Variables | Face AVMs (n=5) |
Paragangliomas (n=18) |
|---|---|---|
| Age (years), M ± SD | 42 ± 6 | 58 ± 12 |
| Sex (female/male) | 3/2 | 13/5 |
| Number of treatment stages (Me, Q₁ – Q₃) |
2, 2 - 2 | 1, 1 - 2 |
| Number of NAEM embolisation steps (Me, Q₁ – Q₃) |
1, 1 - 1 | 1, 1 - 2 |
| Open Surgical Interventions after embolization (%) | 3 (60,0 %) | 1 (5,6 %) |
| Coils while NAEM embolisation (%) | none | 2 (11,1 %) |
| Total embolisation (%) | 5 (100 %) | 12 (66,7 %) |
| Type of catheter (%) | Scepter C, XC (100 %) (Microvention) |
Scepter C, XC (88,9 %) Headway (11,1 %) (Microvention) |
| mRS before embolization Me, Q₁ – Q₃ |
0, 0 - 0 | 1, 0 - 1 |
| mRS at discharge Me, Q₁ – Q₃ |
0, 0 - 1 | 1, 0 - 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



