
Submitted:
18 October 2023
Posted:
19 October 2023
Read the latest preprint version here
Abstract
The anterior cruciate ligament (ACL) injury in the knee is one of the most frequent injuries in the biomechanical environment during jumping exercises; however, repeated jumping, like jumping rope, has not been reported to have a significant impact on the ACL injury. Because of this, this study aimed to compare and examine any potential biomechanical risk factors that can arise during various jumping rope activities, including the basic bounce (BB), forward-backward jump (FB), side-to-side jump (SS), and high knee jump (HK). Thirty participants were recruited. A motion capture system was used to obtain synchronized kinematic and kinetic data for four different jumping rope techniques. The OpenSim modeling system was used to determine the biome-chanical knee factors. The paired samples t-test was used to compare the mean difference in each jumping rope technique of initial contact (IC) and maximum knee flexion (MKF), and a one-way ANOVA was used to compare the mean difference between four different jumping rope techniques in the IC-MKF phase. Between IC and MKF, knee flexion angle, moment, joint ground reaction forces (GRF), and muscle forces of four jumping rope techniques were significantly different (p <.05). Also, in the IC-MKF phase, knee flexion angle and knee extension moment; HK was lower than others; vertical GRF; HK and FB were higher than others; anteroposterior, mediolateral GRF, and muscle forces; SS was higher than others (p <.05). Depending on the jumping rope techniques, the lower knee flexion angle in HK, the higher knee vertical GRF in HK and FB, the higher knee extension moment, anteroposterior, mediolateral GRF, and muscle forces on SS could be a pos-sibility of ACL injury risk compared to others. Therefore, it is recommended that SS be used in risk assessment of ACL in future studies, and BB will be suitable for normal people in daily exercises or will be the alternative intervention program for knee rehabilitation with the lowest risk of injury.
Keywords:
jumping rope exercises
; ACL
; OpenSim
; knee joint
; biomechanics
; modeling system
1. Introduction
Anterior cruciate ligament (ACL) injury in the knee is one of the most common injuries in sports and worsens the quality of life. In sports injuries, more than 30% had injuries related to the knee joint and approximately 20% of knee joint injuries had injuries on ACL [36]. Most ACL injuries occur when a sudden change in acceleration, deceleration, landing, or pivoting maneuvers is repeatedly performed. These injuries are also known as the injuries that occur without physical contact between athletes, which are called non-contact ACL injuries [8].
Several studies have investigated the mechanism of ACL injuries usually occur in landing, jumping, plant-and-cut, and twisting actions during specific tasks to understand the behavior of non-contact ACL injuries [4,60]. Jumping and landing are two common basic motions in everyday life and sports [20]. The previous study reported that overly small knee or hip flexion, overly large knee extension moment, valgus angle, and moment might be leading causes of ACL injuries [38,50]. Also, the previous study suggests that biomechanics in the sagittal plane are the major mechanism that can lead to ACL loading injuries [19]. Further, muscle reaction forces such as high quadriceps muscle force and low hamstring muscle contraction force can also contribute to ACL injury during jumping and landing tasks performance [12,18]. Sports exercises that include jumping can cause an ACL injury due to the large impact loads on the lower extremities taken during jumping, such as basketball and volleyball [3]. It has been reported that the landing phase of a single-leg jump is considered one of the most stressful activities [57] and a danger factor for knee injury, especially in the ACL [49]. A shallow knee angle typically refers to the degree of flexion in the knee joint during certain movements or exercises. In the context of jumping, it means that the knees are not bent enough, resulting in less shock absorption and stability during landing. This kind of landing phase is usually accompanied by a shortening of the quadriceps muscle, especially at shallow knee flexion (less than 40–60 degrees of knee flexion), which may put more tension on the ACL [6,37] and can made ACL rupture [37]. However, in the study of lower repeated landings and jumping, such as jumping rope, there is no direct scientific evidence suggesting that jumping rope has a direct relationship between knee shallow angles and knee risk factors. However, some general observations and considerations about the potential impact of jumping rope on knee angles, jumping impact, and knee risk factors such as weak muscle, imbalance, and improper biomechanics can be explored.
Jumping rope exercise is one type of plyometric exercise in which a person must jump, bounce, or skip repeatedly while a length of rope is swung over and under the lower limb, both ends held in the hands of the jumper, or alternately, and is one of the most popular in daily exercises [1] since it is a convenient exercise that can be done everywhere, does not require a lot of equipment, and is easily learned without special training [39]. Jumping rope has been long practiced as an exercise to promote health and fitness [40]. It can play a vital skill component in many sports and recreational activities to improve physical fitness, enhance cardiac-circulatory compatibility, improve endurance and flexibility, agility, bone mass, postural control, and muscle strength [46]. It is also usually used in schools of physical education, athletic events, and for training in sports activities like boxing, running, taekwondo, and etc. [15,56]. Additionally, besides these basic rope jump, various types of jumping rope, such as alternate jump, bell jump (front to back), skier’s jump (side to side), double bounce, cross over, etc. [17], are performed in training sports exercises to improve the sports skill plays for various purposes.
There are some studies that report the effects of vertical jumping and landing as the same types of jumping rope exercises. An analysis of the difference in jumping rope motion between single-under and double-under jumping movements using both feet in adult male jump-rope leaders has reported that double-under jumps utilize a greater range of motion in the lower limb and produce more ground reaction force [31]. The reported study on the fatigue effect of young people during a 3-minute alternating jump using a rating of perceived exertion (RPE) reported that the joint angle and joint space in the lower limb were associated with fatigue [26]. High velocity and high jumping may increase lower extremity loading to cause injuries [9,25]. But the reported study in repeated and lower jumping like jumping rope has not reported the effects in terms of biomechanics risk factors in the knee joint so well.
Simulation technology like a musculoskeletal modeling system (MMS) is a method that play an essential role in complex biomechanical problems [54]. The main advantage of MMS are method is non-invasive and can demonstrate reliable results [30]. Previous studies used a combination of musculoskeletal modeling techniques and motion capture data to predict the effects inside the body and biomechanics risk factors under different postures and activities like a normal walking, sitting to standing, squatting, landing, and drop jumping [32,42,52]. Many studies have showed that the simulation optimization method of the OpenSim musculoskeletal numerical simulation systems is superior to traditional inverse dynamics or mathematical methods [53,59]. However, since various studies have reported biomechanics risk factors for the knee joint using MMS, studies of the effects and biomechanics risk factors during lower repeated jumps like jumping rope may give a better understanding of the mechanics of jumping and landing. Therefore, the purpose of this study is to investigate and compare the possible biomechanics risk factors that can occur during the different types of jumping rope exercises including basic bounce (BB), forward-backward jump (FB), side-to-side jump (SS), and high knee jump (HK). The musculoskeletal modeling with inverse dynamic analysis together with motion capture data was used in this study. Accordingly, we hypothesized that the differences in the knee angle, moment, knee joint ground reaction forces, and muscle forces of four jumping rope techniques.
2. Materials and Methods
This study was conducted and approved by Dong-A University Institutional Review Board (IRB) for the Use and Protection of Human Subjects (2-1040709-AB-N-01-202112-HR-086-04).
a). Participants
A healthy 30 participants (male 22, female 8) participated in this study. The participants in this study were: 1) healthy and uninjured; and 2) experienced jumping rope activity. Participants in this study were not included if they: 1) had a specific condition or undergone surgery within the past six months; or 2) were currently experiencing lower muscular pain or damage that may affect this study. However, because of the COVID-19 pandemic, the total number of participants was reduced to 20 (male 16, female 4). Before the study, all participants had been given written information about the objectives and methods of the study and had been required to read and sign the consent form. After that, the participants' demographic characteristics were corrected as follows Table 1.
b). Experiment process
Twenty-eight 14-mm infrared reflective markers were placed on each participant to characterize the anatomical bone landmarks on both sides of the participant’s body. Anatomical bone landmarks included the acromion, sternum, anterior superior iliac spine, sacrum, upper thigh, mid-thigh, rear thigh, femur lateral epicondyle, femur middle epicondyle, upper shank, mid-shank, rear shank lateral ankle, first metatarsophalangeal joint, fifth metatarsophalangeal joint, and heel, as shown in Figure 1. The markers were placed on bilateral bone landmarks to ensure the complete capture of the participant’s movement. The methodology of placing markers was primarily based on a guide in Visual3D motion analysis software (Visual3D, C-Motion, Inc., United States). The motion capture system QTM Qualisys Track Manager (Qualisys AB, Gothenburg, Sweden) with 16 high-speed infrared cameras (200 Hz, Miqus QTM, Gothenburg, Sweden) was used to capture the trajectories of markers during the four different jumping rope techniques. Two fully integrated three-dimension force platforms (1000 Hz, Kistler Group, Winterthur, Switzerland) were synchronized and used to capture the dynamic ground-reaction force signal with a motion capture system.
Before the experiment, each participant was well instructed on the performance assessment, and the four different jumping rope exercises were completed randomly: (1) Basic Bounce (BB): the participant was instructed to jump up and down while holding the rope’s handles in each of their hands. stand on tiptoes, slightly bending the knee, and push off with their feet. (2) forward-backward jump (FB): the process was similar to BB, with the jump to the front and back while spinning the rope. (3) side-to-side jump (SS); the process was similar to BB, with a change in direction to slide movement to the left and right while spinning the rope. (4) High knee jump (HK): jump up and down by alternately lifting one leg approximately 60 degrees as shown in Figure 2. Participants were instructed to jump by slightly bending their knees, and their heels could not touch the ground during landing. All the participants were asked to warm up in each self-selected activity for 5 minutes before the experiment started and practice performing jumping rope until they became familiar with the test movements and process. The experiment was performed for each technique for 30 seconds with barefoot, controlled by a metronome speed of 135 bpm, followed by a 5-minute rest period. A complete jump for each jumping rope technique was acceptable when the participant jumped without falling or losing balance. Further, the test was invalid if (1) their feet did not land on force platforms, (2) a rope fell out while jumping, or (3) they lost their balance while jumping or landing. A flowchart of this study is shown in Figure 3.
c). Primary data process
The kinematics and kinetics data of the experiment were filtered using a low-pass filter (Butterworth 4th order) and run with a cutoff frequency of 10 Hz for the motion capture system and 100 Hz for the force signal in the QTM software. The 10 seconds of each experiment's data from the dominant leg of the participants were analyzed. Knee kinematics and kinetics data from this experiment were stored in.c3d (coordinate 3D) file format and exported for use in the biomechanical data analysis.
d). Biomechanical data analysis
This study used a simplified generic musculoskeletal template model, Gait2392, in OpenSim (OpenSim 4.3, Stanford, California, United States), with 12 bony segments, 92 muscles, and 23 degrees of freedom [59]. This study mainly focused on the risk factors for knee joint variables in the four different jumping rope techniques. The dependent variables were chosen and analyzed. They were the knee flexion angle, the knee extension moment, knee joint ground reaction forces and muscle forces from the initial contact (IC) point to the maximum knee flexion (MKF) point, as shown in Table 2. Also, the duration from IC to MKF (IC-MKF phase) was selected and analyzed in this study. The muscle forces calculated in this study are as follows: Quadriceps femoris (rectus femoris, vastus lateralis, vastus medialis and vastus intermedius) and Hamstring (biceps femoris and semitendinosus).
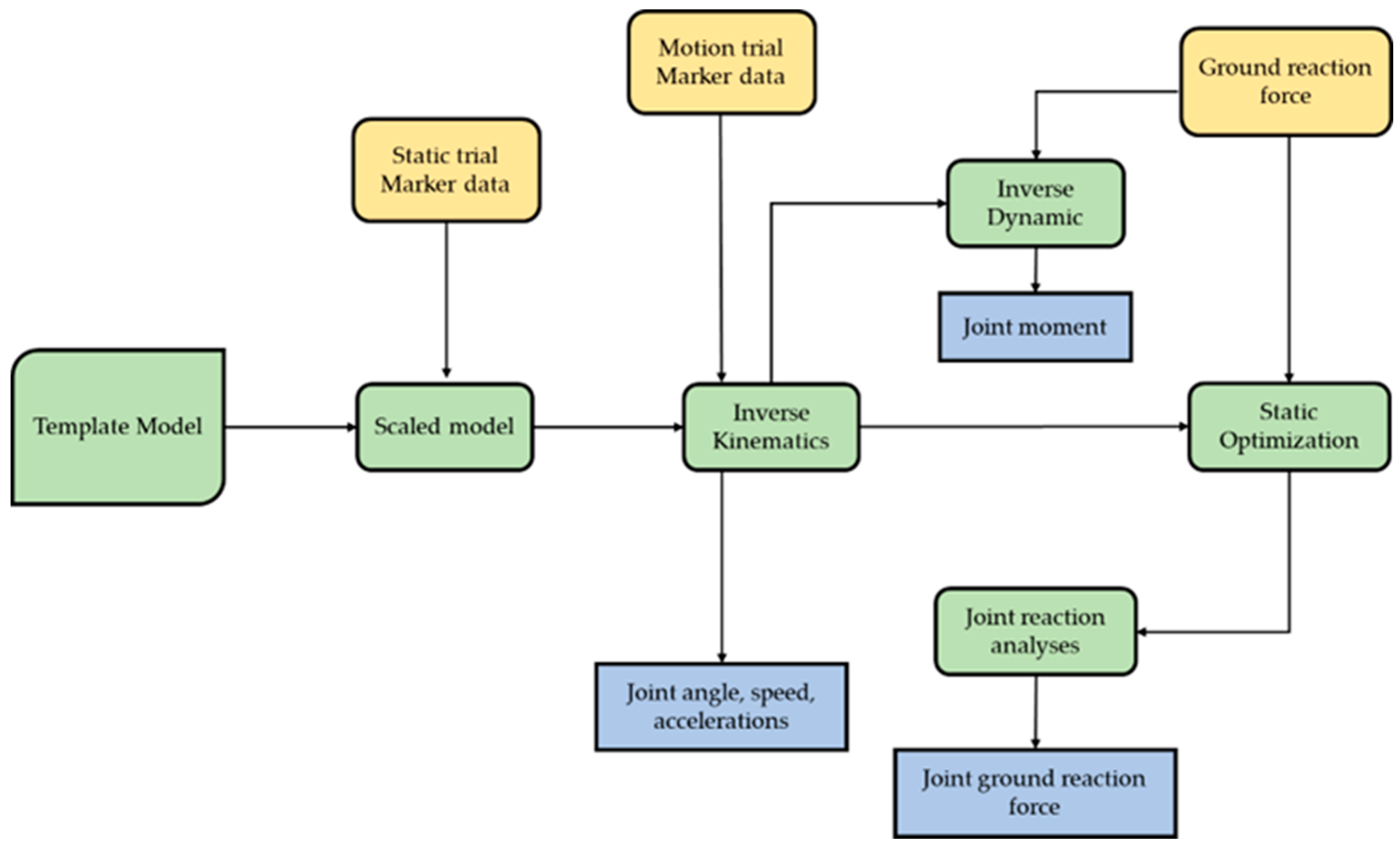
Before simulation, the.c3d file format was converted into specific files for use in OpenSim. A.trc (track row column) file is used to specify the positions of markers placed on a subject, and a.mot (motion) file consists of motion, joint angle, and ground reaction force. These files were created from.c3d files using the MOtoNMS Matlab toolbox (MATLAB R2018a, The MathWorks, MA, United States). After that, the musculoskeletal model was scaled to generate the anthropometry, and the inverse kinematics (IK) were calculated through OpenSim. Also, the inverse simulation of the four different jumping rope techniques was achieved through OpenSim residual reduction algorithms (RRA), static optimization, and the joint reaction analysis tool, which were used to calculate the dependent variables while time was used as the independent variable, as shown in Figure 3.
Figure 3.
Schematic of the OpenSim simulation process.
e). Statistical analysis
The biomechanical parameters of the lower limbs from four different jumping rope techniques were analyzed in SPSS (Version 27.0, IBM Corp., Armonk, NY, United States). The variables of this study are shown in Table 2.
All of the data were tested for normality and equal variance before analysis. The paired samples t-test was used to compare the mean difference in each jumping rope technique of IC and MKF, and an analysis of variance (one-way ANOVA) was used to compare the mean difference between four different jumping rope techniques in the IC-MKF phase. The post-hoc comparison was performed by the Tukey test of mean values, and the significant difference level was set at =.05 for all analyses.

Table 2.
Independent and dependent variables.
| Variables | ||
|---|---|---|
| IV | Jumping rope exercise | BB |
| HK | ||
| FB | ||
| SS | ||
| DV | Kinematics | Knee flexion (degree) |
| Knee moment (%BWm) | ||
| Kinetics | Knee joint GRF (%BW) | |
| Muscle forces (%BW) | ||
| IV, independent variables; DV, dependent variables; BB, basic bounce; HK, high knee jump; FB, forward-backward jump; SS, side-to-side jump; BW, body weight; BWm, Body weight∙hegiht(meter) | ||
3. Results
The paired samples t-test showed that the mean difference between IC and MKF in each jumping rope technique was significant. These results showed that differences in MKF had significant effects on the dependent variables (knee flexion angle, knee flexion moment, knee joint GRF and muscle forces) compared with IC (p < .05), as shown in Table 3. In BB and HK, knee flexion angle, vertical GRF (vGRF), and anteroposterior GRF (aGRF) had a significant difference, and knee extension moment in HK had a significant difference compared with IC (p < .05). In FB and SS, knee flexion angle, knee extension moment, and vertical GRF had a significant difference compared with IC (p < .05). Also, quadriceps muscle forces were significantly higher in all jumping rope techniques compared with IC. (p < .05).
As shown in Table 4, one-way ANOVA showed the mean difference between four different jumping rope techniques in the IC-MKF phase. The knee flexion angle and knee moment of the BB and HK were significantly lower than FB and SS (p < .05). In knee joint GRF, the vGRF of BB was significantly lower than that of HK, FB, and SS (p < .05). The aGRF of SS was significantly higher than BB and HK, and BB and HK were also significantly higher than FB (p < .05). Mediolateral GRF (mGRF) of BB, HK, and FB was significantly higher than SS (p < .05). While quadricep and hamstring muscle forces in SS was higher than others (p < .05).
4. Discussion
The objective of this study was to investigate and compare the possible biomechanical risk factors that can occur during different types of jumping rope exercises. This study used commonly used variables, including knee flexion angle and knee moments, as the kinetic variables of interest [24,47]. Also, to investigate a better understanding of knee injury factors, the evaluated knee joint GRF and muscle forces using musculoskeletal modeling processes at specific events was also chosen as the variables of interest [55]. We first hypothesized that the differences in the knee angle, moment, knee joint GRF, and muscle forces of the four different jumping rope exercises should be found in this study, and the results of this study partly agree with the hypotheses.
The risk factors for ACL injury are mainly reported with a small knee flexion angle or a large knee extension moment in the sagittal plane [4]. The risk factors for ACL injury are mainly reported with a small knee flexion angle or a large knee extension moment in the sagittal plane [4]. A previous study showed that the ACL loading will decrease with the increase in knee flexion angle in knee motion [16]. In addition, the increase in knee flexion angle while landing helps absorb some of the energy and effectively reduces the risk of ACL injury [18,24], thus reducing the risk of an ACL injury. In our study, a one-way ANOVA showed differences between the knee flexion angle and knee extension moment of four different jumping rope exercises. This study found that the knee flexion angle increased during the four different types of jumping rope at the MKF point. Additionally, a shallow angle of knee flexion of less than 40–60 degrees during landing may stress the ACL and increase the incidence of ACL rupture [6]. This study demonstrated that the participants experienced a greater decrease in knee flexion angle in the HK than other jumping rope techniques during the landing process, which means knee extension was increasing. Thus, the decreased knee flexion angle in HK is possible to increase the knee injury and could be a risk factor for a higher ACL load than other jumping rope techniques [16]. In addition, the increase in knee flexion angle while landing helps absorb some of the energy and effectively reduces the risk of ACL injury [18,24], thus reducing the risk of an ACL injury. In our study, a one-way ANOVA showed differences between the knee flexion angle and knee extension moment of four different jumping rope exercises. This study found that the knee flexion angle increased during the four different types of jumping rope at the MKF point. Additionally, a shallow angle of knee flexion of less than 40–60 degrees during landing may stress the ACL and increase the incidence of ACL rupture [6]. This study demonstrated that the participants experienced a greater decrease in knee flexion angle in the HK than other jumping rope techniques during the landing process, which means knee extension was increasing. Thus, the decreased knee flexion angle in HK is possible to increase the knee injury and could be a risk factor for a higher ACL load than other jumping rope techniques.
The knee extension moment refers to the rotation force (or torque) around the knee that pushes it to straighten or extend. The high knee extension moment of the landing process might lead to knee over-extension or hyper-extension, which can increase the strain on the ACL and significantly increase the ACL load [35]. In this study, the knee extension moment of the BB, HK, and FB was lower than that of the SS, which could be a risk factor that increases the ACL load in the four different jumping rope techniques in the landing process and can lead to an ACL injury. Some studies suggest that the risk factors measured in the sagittal plane, such as the angle and moment of the knee joint in landing, can cause a higher ACL load during the landing position [27]. The higher knee extension moment in the IC-MKF phase was similar to the phenomenon described by Kar et al. [28]. This phenomenon describes that the risk factors measured in the sagittal plane are associated with a high ACL load and are significantly higher than those measured in the frontal plane. As previously reported, the ACL load will be effectively reduced when the knee flexion angle exceeds around 50°, and this study showed that none of the four jumping rope techniques had a maximum knee flexion angle exceeding 50°. Thus, each decrease in the knee flexion angle could be a factor in the knee injury, and a higher ACL load is possible to occur [22]. Thus, the factors measured in the sagittal plane, such as the knee flexion and extension moment, are possible primary risk factors for ACL injury.
Previous studies have demonstrated that decreases in knee flexion angle could contribute to increased asymmetries at the knee joint if the magnitude of the knee joint GRF was decreased at the same time [23,47]. The size and direction of the GRF can directly affect the knee moment. Thus, decreased knee joint GRF was a mechanical representation of a decreased knee extension moment [23]. In this study, it was found that the knee joint vGRF (positive, upward; negative, downward) in the sagittal plane was higher for HK, FB, and SS than BB. The higher knee joint vGRF in HK, FB, and SS may be due to these three jumping rope techniques, which require more movement and reach the maximum vertical jump height immediately after landing. The knee joint helps to absorb and transmit the vertical forces from the foot upwards to the hip and the rest of the body. During activities like running or jumping, the knee flexes during landing to help absorb the shock from vGRF. Excessive vGRF or lack of proper shock absorption can lead to overuse injuries in the knee, such as patellofemoral pain syndrome or osteoarthritis [43,58,60]. Theoretically, except for the BB, the other three jumping rope techniques need to jump in different directions. Also, depending on the nature of the single-leg landing and double-leg landing jump tasks [48]. A double-leg landing jump task allows participants to use inter-limb compensation strategies that have the potential to increase limb asymmetries, while in a single-leg landing jump task, participants are only able to use inter-joint compensation during the jump task. The more different direction landing tasks were more effective on knee kinematics and kinetics than static landing tasks. Also, it will lead to both inter-limb and inter-joint compensation, and more loads might contribute to the high knee injury. In addition, the inherent factors that caused the decreased knee flexion moment could be deficits in dynamic strength, muscle inhibition, altered neuromuscular function, or fear, which can cause the decreased knee joint angle, decreased knee moment, and effect on the knee joint vGRF [5].
Furthermore, we also estimated knee joint aGRF (positive, anterior; negative, posterior) and mGRF (positive, media; negative, lateral) throughout the jumping rope exercise. For aGRF, this force plays a role in forward and backward directions. During landing, if the foot strikes the ground with a forward motion, an aGRF will be generated to resist the forward motion of the foot and lower leg [7,51]. In this study, SS has a higher aGRF on the anterior side than other jumping rope exercises. The aGRF might be increasing due to decreased knee flexion angles [7,45]. An aggressive or large aGRF combined with a forceful contraction of the quadriceps muscle can produce an anterior shear force on the tibia. Essentially, this force attempts to slide the tibia forward in relation to the femur, which is called anterior tibia translation [51]. ACL primarily serves to resist anterior tibial translation [21]. Thus, if the aGRF on the anterior side surpasses the ACL’s capacity to resist, it can lead to an ACL tear from overstretching [7,21,51]. Therefore, the decrease in knee flexion could contribute to an increase in knee momentum asymmetry, which may increase the risk of knee injury during jumping and landing tasks [7].
For mGRF, in this study, we also found that the SS has a higher lateral mGRF than other jumping rope exercises. The previous study demonstrated the high values of lateral mGRF due to the mechanics of subtalar pronation to transmit and dampen the impact forces to the lower extremity during jumping tasks [41]. Knee joint ligaments inside, like the ACL and MCL, help stabilize and resist the leg against side-to-side forces and excessive movement during a change of direction rapidly or landing from a jump. The excessive use of mGRF can lead to weak stabilization mechanisms in the knee, which can lead to injuries like ACL tears [29]. In addition, the high impact lateral mGRF on the lateral side may lead to overpronation in the ankle [44]. Since overpronation in the ankle can lead to tibial internal rotation, valgus angle and moment can occur and cause higher ACL loading during the jumping process [28]. The ACL load will increase if the knee valgus is increasing, and the increased knee valgus angle poses a significant risk of ACL injury [27,28].
Furthermore, the higher stress or strain loading on the ACL depends on muscle forces [34]. Previous studies have shown that the knee extension moment caused by quadriceps contraction could increase the anterior tibial shear force, increasing the ACL load and injury risk [10]. In this study, the highest knee extension moment and muscle forces in quadriceps were found in the SS, followed by the FB, HK, and BB. The neuromuscular control strategy may be the cause of the increased knee extension moment and quadriceps femoris muscle forces observed in the SS. The SS requires more space between itself and the force plates and, immediately after landing, reaches its maximum vertical jump height [14]. Theoretically, jumping and landing, which require more movement, should produce larger quadriceps muscle forces, which increase the tibial anterior shear force and force the tibia forward relative to the femur. If not adequately resisted, it can lead to anterior tibial translation, increase strain in the ACL, and cause injury [13,14]. ACL load caused by quadriceps muscles can decrease when the knee flexion angle reaches up to 45 degrees and may have no impact when it exceeds 60 degrees [38]. Also, it can be related to hamstring muscle contraction. Studies have shown that the posterior shear forces in the tibia from hamstring muscle contraction can reduce the load on the ACL when the knee flexion angle is greater than 22 degrees [2]. In our study, the knee flexion angle was greater than 22 degrees in all four different jumping rope techniques. SS shows higher hamstring muscle forces related to higher knee flexion that can increase the activation level of the hamstring muscles [11]. Increased knee flexion angle on landing induces more hamstring contractions to participate in coordination [33], which effectively reduces ACL tension, decreasing the risk of ACL injury. Therefore, a high knee flexion angle while landing effectively resists the forces from quadriceps muscle contraction. At the same time, the coordinated contraction from the hamstring muscle may reduce the ACL load, reducing the risk of ACL injury.
In our study, we can assume that different techniques can demonstrate the knee joint risk factor for different reasons. This study showed that SS demonstrated a higher knee extension moment, knee joint aGRF, mGRF, and quadriceps muscle forces that can increase the ACL load and lead to an ACL injury than other jumping rope techniques. Also, HK demonstrated a smaller knee flexion in the IC, MKF, and IC-MKF phases. HK and FB demonstrated a high knee joint vGRF, while BB showed the lowest in all of the variables compared to other jumping rope techniques. Following the results, it can be assumed that the relatively unnatural jumping and landing action may increase the risk of ACL injury.
The use of male and female participants, which may have an effect on biomechanical factors from physiology, neuromuscular control mechanisms, and landing protection awareness during jumping assessments, challenges a limitation to this study. The participants may be affected by the metronome's speed level, which may be faster or slower than the participants' potential and result in an abnormal jump pattern. Additionally, there aren't many research on the knee during the exercise of jumping rope to compare with this one. In order to avoid or analyze external factors like gender or level of speed, height, or patterns condition with can directly influences to the study in the future, it is recommended that the study of the jumping rope task and landing process be taken into consideration. The outcomes of this study provided a better understanding of the behavior of the knee joint loading mechanism. Further, it could benefit from studies relevant to sports science, injury prevention, rehabilitation, and athletic training programs related to the knee joint.
5. Conclusions
This study indicated differences in knee flexion angle, knee flexion moment, and knee joint GRF between the four jumping rope exercises. However, knee flexion angle, knee extension moments, and knee joint vertical GRF are critical factors for knee injuries that can lead to an ACL injury. This study found that the risk of injury is lower in BB than in HK, FB, and SS. SS demonstrated the highest knee extension moment, knee joint aGRF, mGRF, and quadriceps muscle forces compared to other jumping rope techniques. Also, HK demonstrated a smaller knee flexion angle. HK and FB demonstrated high knee joint vGRF. Therefore, depending on the jumping rope techniques, it is recommended that use SS in future studies in risk assessment of ACL. Naturally jumping and landing jumping rope techniques like BB have shown a lower risk of injury than other techniques, which can lower knee joint and ACL injuries, and it may be suitable for normal people in exercises or for the rehabilitation program.
Author Contributions
Conceptualization, J.S. and H.J.; methodology, J.S.; software, J.S.; validation, J.S. and H.J.; formal analysis, J.S.; investigation, J.S.; resources, J.S.; data curation, J.S.; writing—original draft preparation, J.S. and H.J.; writing—review and editing, J.S. and H.J.; visualization, J.S.; supervision, H.J.; project administration, H.J.; funding acquisition, H.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guideline of the Declaration of Helsinki, and approved by the Institutional Review Board of Dong-A University (2-1040709-AB-N-01-202112-HR-086-04).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are available if there is justified research interest.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abou Elmagd, M., Benefits, need and importance of daily exercise. Int. J. Phys. Educ. Sports Health, 2016. 3(5): p. 22-27.
- Afsar, E., et al., Use of the finite element analysis to determine stresses in the knee joints of osteoarthritis patients with different Q angles. Journal of the Brazilian Society of Mechanical Sciences and Engineering, 2017. 39: p. 1061-1067. [CrossRef]
- Agel, J., T. Rockwood, and D. Klossner, Collegiate ACL injury rates across 15 sports: national collegiate athletic association injury surveillance system data update (2004-2005 through 2012-2013). Clinical journal of sport medicine, 2016. 26(6): p. 518-523. [CrossRef]
- Alazzawi, S., et al., Management of anterior cruciate ligament injury: pathophysiology and treatment. British Journal of Hospital Medicine, 2016. 77(4): p. 222-225. [CrossRef]
- Ardern, C.L., et al., Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. British journal of sports medicine, 2011. 45(7): p. 596-606. [CrossRef]
- Bakker, R., et al., Effect of sagittal plane mechanics on ACL strain during jump landing. Journal of Orthopaedic Research, 2016. 34(9): p. 1636-1644. [CrossRef]
- Baumgart, C., et al., Do ground reaction forces during unilateral and bilateral movements exhibit compensation strategies following ACL reconstruction? Knee Surgery, Sports Traumatology, Arthroscopy, 2017. 25: p. 1385-1394. [CrossRef]
- Boden, B.P., et al., Mechanisms of anterior cruciate ligament injury. 2000, SLACK Incorporated Thorofare, NJ. p. 573-578. [CrossRef]
- Boden, B.P. and F.T. Sheehan, Mechanism of non-contact ACL injury: OREF Clinical Research Award 2021. Journal of Orthopaedic Research®, 2022. 40(3): p. 531-540. [CrossRef]
- Boden, B.P., et al., Non-contact ACL injuries: mechanisms and risk factors. The Journal of the American Academy of Orthopaedic Surgeons, 2010. 18(9): p. 520.
- Brazen, D.M., et al., The effect of fatigue on landing biomechanics in single-leg drop landings. Clinical Journal of Sport Medicine, 2010. 20(4): p. 286-292. [CrossRef]
- Carvalho, A., P. Mourão, and E. Abade, Effects of strength training combined with specific plyometric exercises on body composition, vertical jump height and lower limb strength development in elite male handball players: a case study. Journal of human kinetics, 2014. 41: p. 125. [CrossRef]
- Chen, L., et al., Effect of different landing actions on knee joint biomechanics of female college athletes: Based on opensim simulation. Frontiers in Bioengineering and Biotechnology, 2022. 10: p. 899799. [CrossRef]
- Cruz, A., et al., The effects of three jump landing tasks on kinetic and kinematic measures: implications for ACL injury research. Research in sports medicine, 2013. 21(4): p. 330-342. [CrossRef]
- Donath, L., et al., Effects of slackline training on balance, jump performance & muscle activity in young children. International journal of sports medicine, 2013: p. 1093-1098. [CrossRef]
- Donelon, T.A., et al., Biomechanical determinants of knee joint loads associated with increased anterior cruciate ligament loading during cutting: a systematic review and technical framework. Sports Medicine-Open, 2020. 6(1): p. 1-21. [CrossRef]
- Eler, N. and H. Acar, The Effects of the Rope Jump Training Program in Physical Education Lessons on Strength, Speed and VO 2 Max in Children. Universal Journal of Educational Research, 2018. 6(2): p. 340-345. [CrossRef]
- Etnoyer, J., et al., Instruction and jump-landing kinematics in college-aged female athletes over time. Journal of athletic training, 2013. 48(2): p. 161-171. [CrossRef]
- Fleming, B.C., et al., The effect of weightbearing and external loading on anterior cruciate ligament strain. Journal of biomechanics, 2001. 34(2): p. 163-170. [CrossRef]
- Fort-Vanmeerhaeghe, A., et al., Lower limb neuromuscular asymmetry in volleyball and basketball players. Journal of Human Kinetics, 2016. 50: p. 135. [CrossRef]
- Gardner, E.J., et al., Effect of anteromedial and posterolateral anterior cruciate ligament bundles on resisting medial and lateral tibiofemoral compartment subluxations. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 2015. 31(5): p. 901-910. [CrossRef]
- Gerritsen, K.G., A.J. van den Bogert, and B.M. Nigg, Direct dynamics simulation of the impact phase in heel-toe running. Journal of biomechanics, 1995. 28(6): p. 661-668. [CrossRef]
- Gokeler, A., et al., Abnormal landing strategies after ACL reconstruction. Scandinavian journal of medicine & science in sports, 2010. 20(1): p. e12-e19. [CrossRef]
- Hansberger, B.L., et al., Peak lower extremity landing kinematics in dancers and nondancers. Journal of athletic training, 2018. 53(4): p. 379-385. [CrossRef]
- Hong, Y.G., et al., The kinematic/kinetic differences of the knee and ankle joint during single-leg landing between shod and barefoot condition. International journal of precision engineering and manufacturing, 2014. 15: p. 2193-2197. [CrossRef]
- Jang, K.H., et al., Effects of skill level and feet width on kinematic and kinetic variables during jump rope single under. Korean J. Sport Biomech, 2017. 27(2): p. 99-108. [CrossRef]
- Kar, J. and P.M. Quesada, A numerical simulation approach to studying anterior cruciate ligament strains and internal forces among young recreational women performing valgus inducing stop-jump activities. Annals of biomedical engineering, 2012. 40: p. 1679-1691. [CrossRef]
- Kar, J. and P.M. Quesada, A musculoskeletal modeling approach for estimating anterior cruciate ligament strains and knee anterior–posterior shear forces in stop-jumps performed by young recreational female athletes. Annals of biomedical engineering, 2013. 41: p. 338-348. [CrossRef]
- Kim, C., et al., Effects of patellofemoral pain syndrome on changes in dynamic postural stability during landing in adult women. Applied Bionics and Biomechanics, 2022. 2022. [CrossRef]
- Kim, H.J., et al., Evaluation of predicted knee-joint muscle forces during gait using an instrumented knee implant. Journal of orthopaedic research, 2009. 27(10): p. 1326-1331. [CrossRef]
- Kim, Y. and D. Kim, A Comparative Analysis on the Kinematic and Ground Reaction Force Factors by Rope Skipping Types. Korea Society for Wellness, 2015. 10(2): p. 77-77.
- Konrath, J.M., et al., Estimation of the knee adduction moment and joint contact force during daily living activities using inertial motion capture. Sensors, 2019. 19(7): p. 1681. [CrossRef]
- Leppänen, M., et al., Stiff landings are associated with increased ACL injury risk in young female basketball and floorball players. The American journal of sports medicine, 2017. 45(2): p. 386-393. [CrossRef]
- Lim, Y.P., Y.-C. Lin, and M.G. Pandy, Effects of step length and step frequency on lower-limb muscle function in human gait. Journal of biomechanics, 2017. 57: p. 1-7. [CrossRef]
- Lohmander, L.S., et al., The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. The American journal of sports medicine, 2007. 35(10): p. 1756-1769.
- Majewski, M., H. Susanne, and S. Klaus, Epidemiology of athletic knee injuries: A 10-year study. The knee, 2006. 13(3): p. 184-188. [CrossRef]
- Maniar, N., et al., Muscle force contributions to anterior cruciate ligament loading. Sports Medicine, 2022. 52(8): p. 1737-1750. [CrossRef]
- Marieswaran, M., et al., A review on biomechanics of anterior cruciate ligament and materials for reconstruction. Applied bionics and biomechanics, 2018. 2018. [CrossRef]
- Miyaguchi, K., S. Demura, and M. Omoya, Relationship between jump rope double unders and sprint performance in elementary schoolchildren. The Journal of Strength & Conditioning Research, 2015. 29(11): p. 3229-3233. [CrossRef]
- Miyaguchi, K., H. Sugiura, and S. Demura, Possibility of stretch-shortening cycle movement training using a jump rope. The Journal of Strength & Conditioning Research, 2014. 28(3): p. 700-705. [CrossRef]
- Neal, B.S., et al., Foot posture as a risk factor for lower limb overuse injury: a systematic review and meta-analysis. Journal of foot and ankle research, 2014. 7: p. 1-13. [CrossRef]
- Niu, W., et al., Effect of dropping height on the forces of lower extremity joints and muscles during landing: a musculoskeletal modeling. Journal of Healthcare Engineering, 2018. 2018. [CrossRef]
- Norcross, M.F., et al., The association between lower extremity energy absorption and biomechanical factors related to anterior cruciate ligament injury. Clinical biomechanics, 2010. 25(10): p. 1031-1036. [CrossRef]
- Nur Saibah, G., Biomechanical investigation of individual with over-pronation and over-supination foot during walking/Nur Saibah Ghani. 2020, University of Malaya.
- Oberländer, K.D., et al., Altered landing mechanics in ACL-reconstructed patients. Medicine and science in sports and exercise, 2013. 45(3): p. 506-513. [CrossRef]
- Orhan, S., Effect of weighted rope jumping training performed by repetition method on the heart rate, anaerobic power, agility and reaction time of basketball players. Advance in Environmental Biology, 2013. 7(5): p. 945-951.
- Orishimo, K.F., et al., Adaptations in single-leg hop biomechanics following anterior cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy, 2010. 18(11): p. 1587-1593. [CrossRef]
- Paterno, M.V., et al., Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. The American journal of sports medicine, 2010. 38(10): p. 1968-1978. [CrossRef]
- Peebles, A.T., et al., Using force sensing insoles to predict kinetic knee symmetry during a stop jump. Journal of Biomechanics, 2019. 95: p. 109293. [CrossRef]
- Rachmat, H., et al., In-situ mechanical behavior and slackness of the anterior cruciate ligament at multiple knee flexion angles. Medical engineering & physics, 2016. 38(3): p. 209-215. [CrossRef]
- Sanford, B.A., et al., Asymmetric ground reaction forces and knee kinematics during squat after anterior cruciate ligament (ACL) reconstruction. The Knee, 2016. 23(5): p. 820-825. [CrossRef]
- Schellenberg, F., et al., Evaluation of the accuracy of musculoskeletal simulation during squats by means of instrumented knee prostheses. Medical engineering & physics, 2018. 61: p. 95-99. [CrossRef]
- Seth, A., et al., OpenSim: Simulating musculoskeletal dynamics and neuromuscular control to study human and animal movement. PLoS computational biology, 2018. 14(7): p. e1006223. [CrossRef]
- SONG, H.-s., J.-g. QIAN, and X. TANG, Summary of software OpenSim with focus on its human motion modeling theory and application field. Journal of Medical Biomechanics, 2015: p. E373-E379.
- Stock, H., et al. Sagittal hip-knee coordination during a 45 degree cutting task. in ISBS-Conference Proceedings Archive. 2016.
- Trecroci, A., et al., Jump rope training: Balance and motor coordination in preadolescent soccer players. Journal of sports science & medicine, 2015. 14(4): p. 792.
- Wang, L.-I., The lower extremity biomechanics of single-and double-leg stop-jump tasks. Journal of sports science & medicine, 2011. 10(1): p. 151.
- Xu, D., et al., Single-leg landings following a volleyball spike may increase the risk of anterior cruciate ligament injury more than landing on both-legs. Applied Sciences, 2020. 11(1): p. 130. [CrossRef]
- Yu, J., et al. Human gait analysis based on OpenSim. in 2020 International Conference on Advanced Mechatronic Systems (ICAMechS). 2020. IEEE.
- Zahradnik, D., et al., Lower extremity mechanics during landing after a volleyball block as a risk factor for anterior cruciate ligament injury. Physical Therapy in Sport, 2015. 16(1): p. 53-58. [CrossRef]
Figure 1.
Schematic representation of the placement markers in the front, side, and back view of the marker set.
Figure 1.
Schematic representation of the placement markers in the front, side, and back view of the marker set.
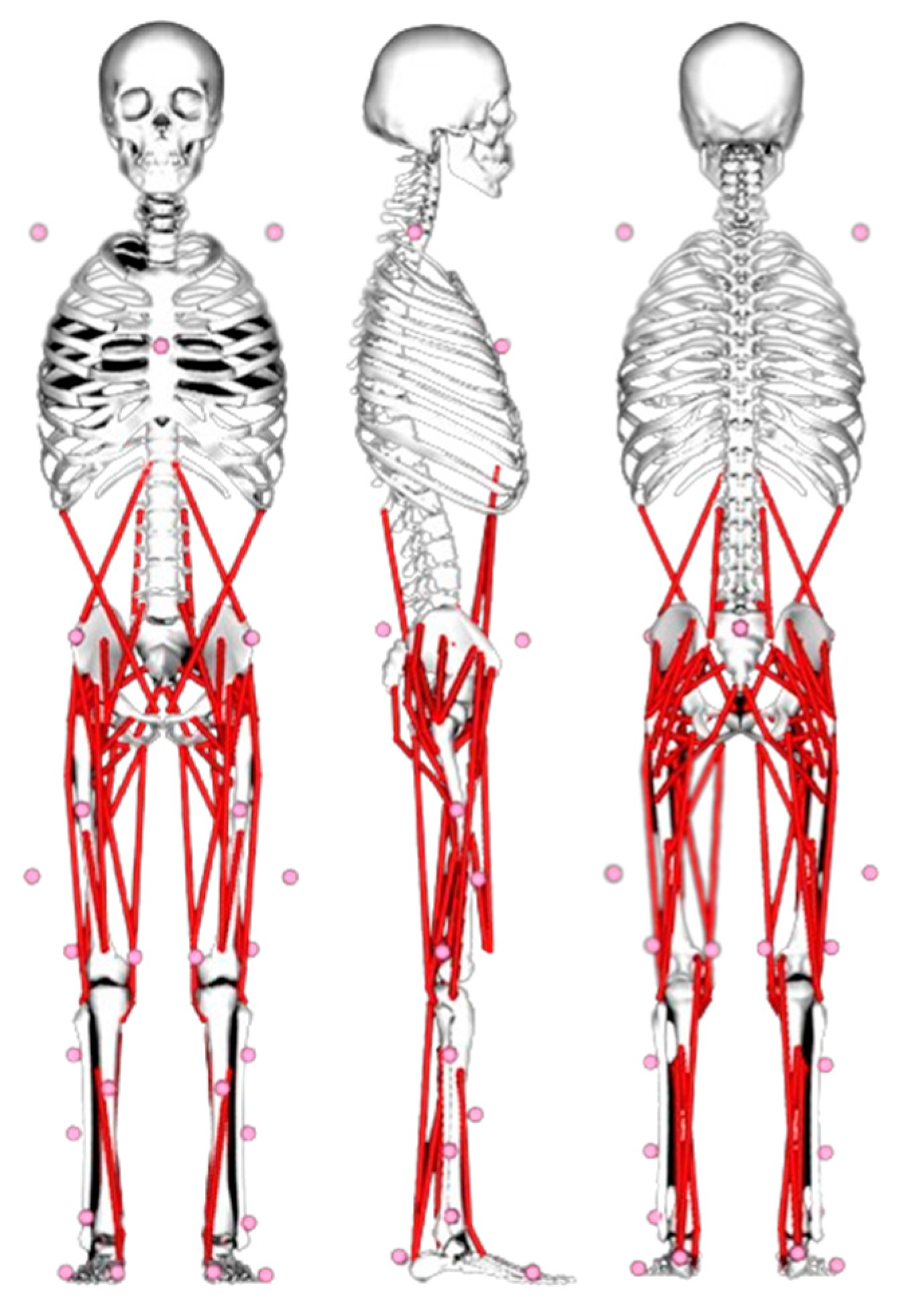
Figure 2.
Jumping rope techniques: (a) BB; (b) FB; (c) SS; (d) HK.
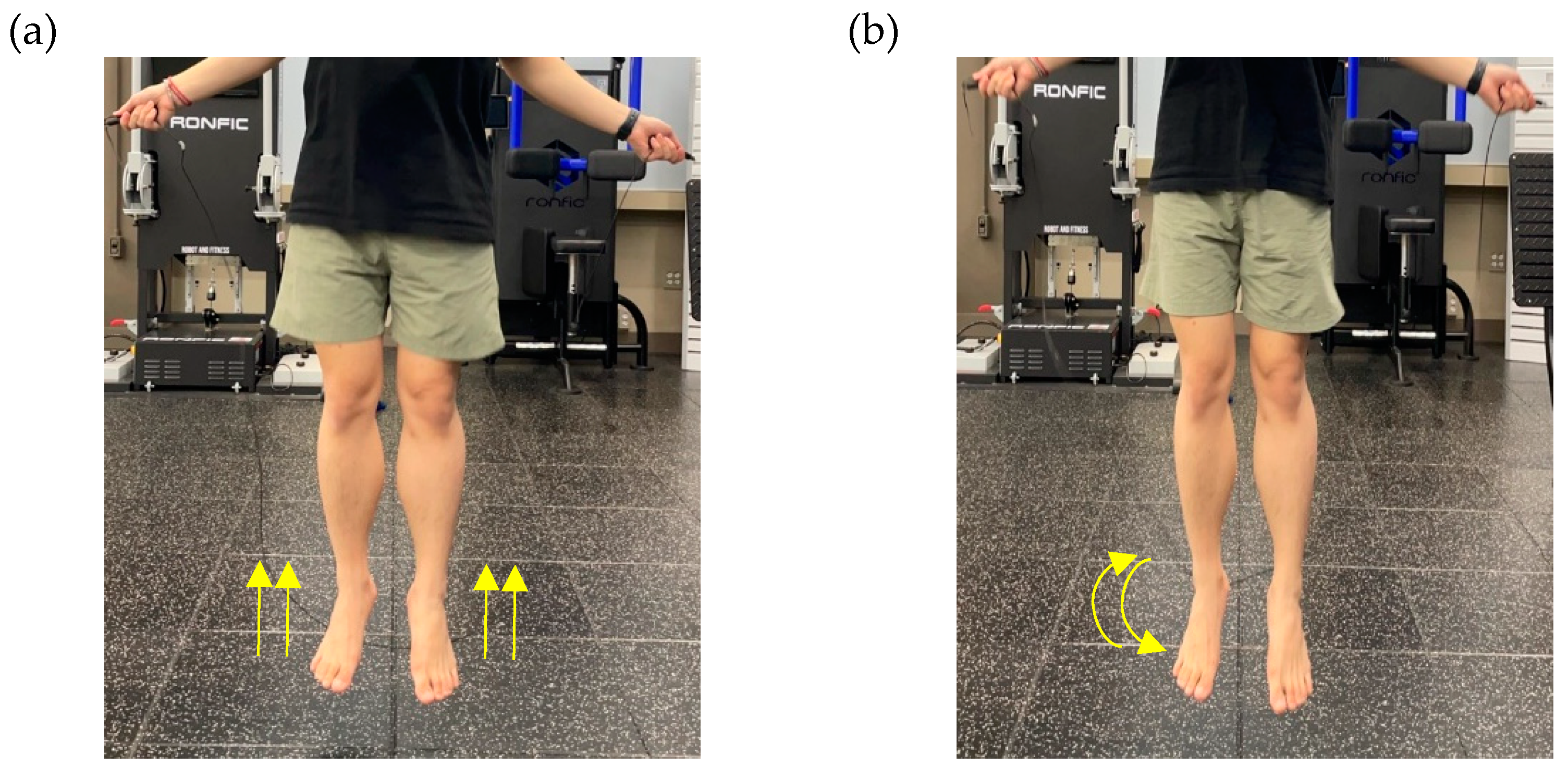
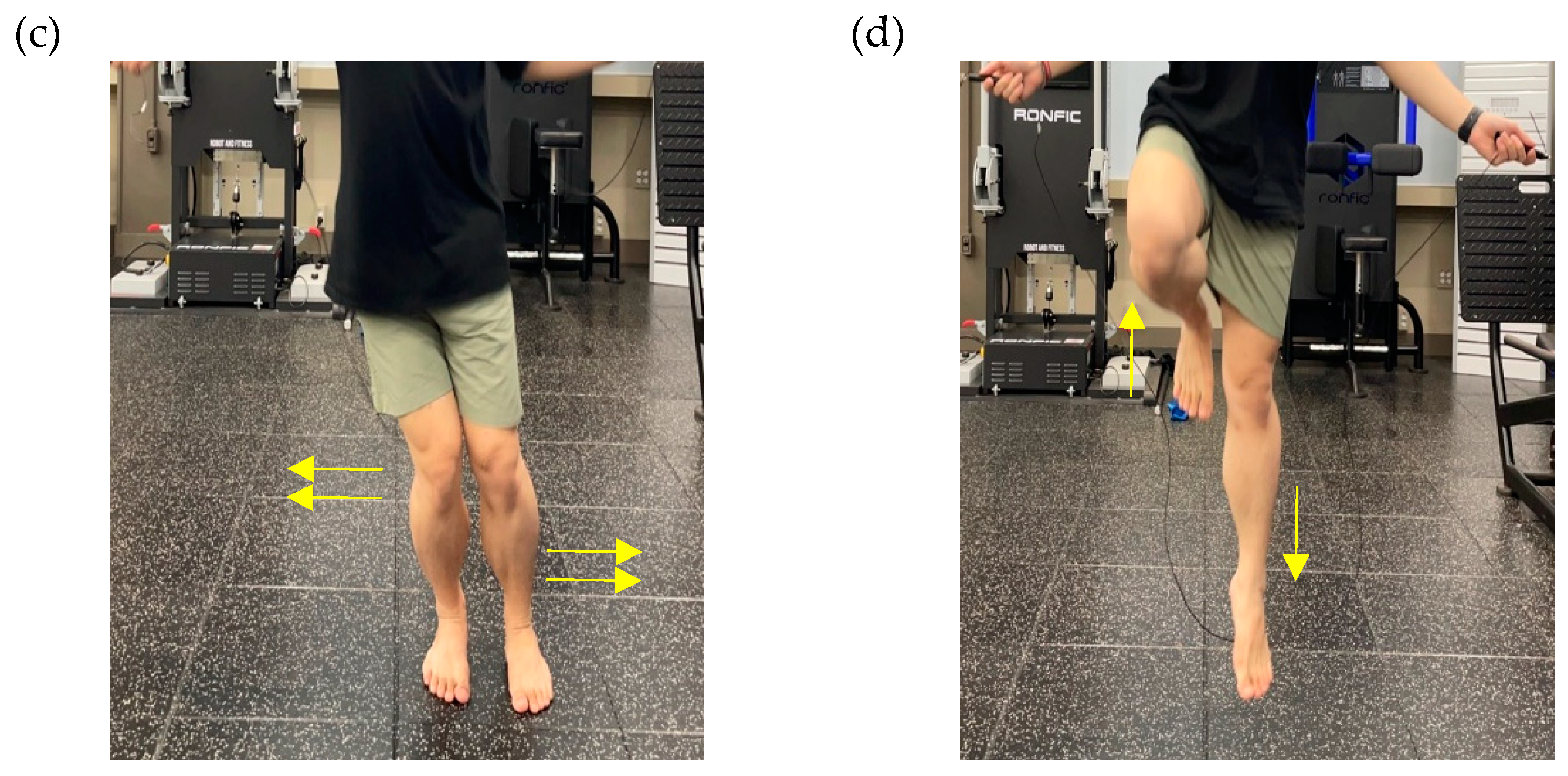
Figure 3.
Flowchart of this study.
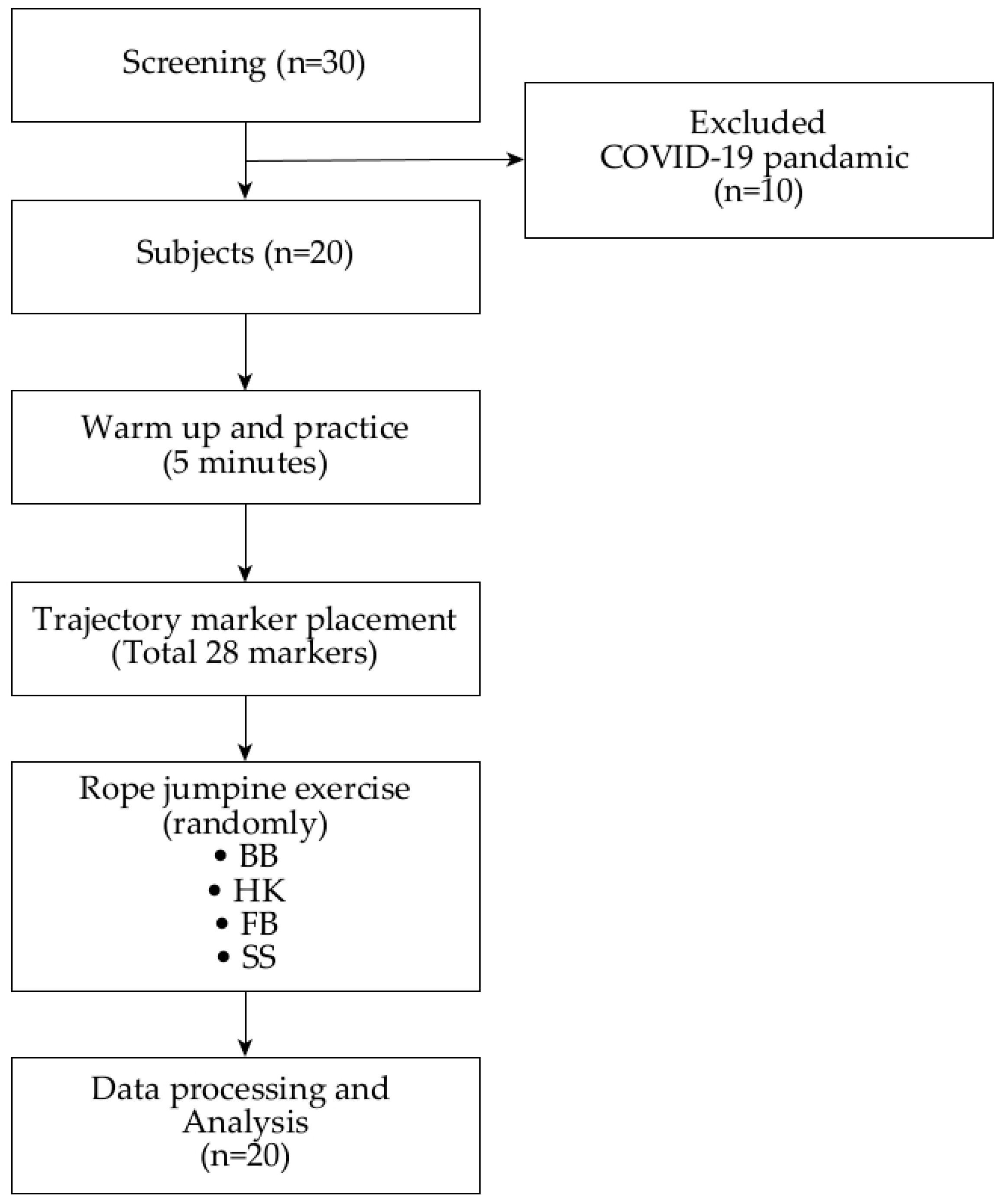
Table 1.
Demographic characteristics of the participants.
| n | Age (year) | Height (cm) | Weight (kg) | BMI (kg/m2) |
|---|---|---|---|---|
| 20 | 26.40±2.59 | 173.50±4.30 | 83.40±17.56 | 27.60±5.19 |
| BMI, Body Mass Index | ||||
Table 3.
Statistic of knee variables between the IC and MKF of four different jumping rope techniques(mean ± SD).
Table 3.
Statistic of knee variables between the IC and MKF of four different jumping rope techniques(mean ± SD).
| Jumping rope Techniques | Variables | IC | MKF | Statistical |
|---|---|---|---|---|
| BB | Knee flexion (degree) | 26.62 ± 9.65 | 37.98 ± 8.62 | < .05 |
| Knee extension moment (%BWm) | 1.60 ± 0.70 | 1.90 ± 0.60 | ||
| Knee joint GRF (%BW) | ||||
| Vertical | -110.23 ± 20.93 | -125.67 ± 21.88 | < .05 | |
| Anteroposterior | 14.59 ± 4.28 | 11.62 ± 3.37 | < .05 | |
| Mediolateral | 7.28 ± 12.93 | 7.17 ± 13.56 | ||
| Muscle forces (%BW) | ||||
| Quadriceps | 209.64 ± 42.71 | 396.94 ± 78.09 | < .05 | |
| Hamstring | 49.15 ± 43.11 | 53.94 ± 40.18 | ||
| HK | Knee flexion (degree) | 22.37 ± 3.67 | 31.59 ± 3.65 | < .05 |
| Knee extension moment (%BWm) | 1.11 ± 0.56 | 2.06 ± 0.64 | < .05 | |
| Knee joint GRF (%BW) | ||||
| Vertical | -118.78 ± 30.65 | -165.91 ± 37.60 | < .05 | |
| Anteroposterior | 18.02 ± 15.34 | 20.53 ± 18.93 | < .05 | |
| Mediolateral | 4.76 ± 8.99 | 3.96 ± 10.35 | ||
| Muscle forces (%BW) | ||||
| Quadriceps | 404.18 ± 55.05 | 530.50 ± 93.59 | < .05 | |
| Hamstring | 49.25 ± 35.06 | 54.47 ± 38.07 | ||
| FB | Knee flexion (degree) | 38.26 ± 9.70 | 45.85 ± 9.82 | < .05 |
| Knee extension moment (%BWm) | 1.11 ± 0.61 | 2.21 ± 0.53 | < .05 | |
| Knee joint GRF (%BW) | ||||
| Vertical | -122.88 ± 21.01 | -163.10 ± 22.69 | < .05 | |
| Anteroposterior | -8.70 ± 12.47 | -8.85 ± 13.02 | ||
| Mediolateral | 6.14 ± 9.82 | 7.33 ± 11.21 | ||
| Muscle forces (%BW) | ||||
| Quadriceps | 431.89 ± 59.05 | 537.34 ± 89.36 | < .05 | |
| Hamstring | 83.67 ± 38.02 | 98.19 ± 42.22 | ||
| SS | Knee flexion (degree) | 35.89 ± 9.11 | 47.27 ± 9.71 | < .05 |
| Knee extension moment (%BWm) | 1.98 ± 0.73 | 2.68 ± 0.67 | < .05 | |
| Knee joint GRF (%BW) | ||||
| Vertical | -114.63 ± 25.20 | -163.15 ± 31.25 | < .05 | |
| Anteroposterior | 21.13 ± 5.66 | 24.51 ± 12.23 | ||
| Mediolateral | -6.22 ± 13.01 | -8.31 ± 13.09 | ||
| Muscle forces (%BW) | ||||
| Quadriceps | 532.53 ± 88.47 | 601.59 ± 93.81 | < .05 | |
| Hamstring | 94.40 ± 48.44 | 105.11 ± 38.89 | ||
| BB, basic bounce; HK, high knee jumping rope; FB, Forward-backward jumping rope, SS, Side-to-side jumping rope; GRF, Ground reaction force; BW, Body weight; BWm, Body weight∙hegiht(meter) | ||||
| * The mean difference is significant at the p < .05 | ||||
Table 4.
Statistic of knee variables from the IC-MKF phase of four different jumping rope techniques(mean ± SD).
Table 4.
Statistic of knee variables from the IC-MKF phase of four different jumping rope techniques(mean ± SD).
| Variable | BB | HK | FB | SS | Post-hoc |
|---|---|---|---|---|---|
| Knee flexion (degree) | 32.30 ± 9.01 | 26.98 ± 3.25 | 42.05 ± 9.55 | 41.58 ± 9.21 | BB,HK<FB,SS |
| Knee extension moment (%BWm) | 1.75 ± 0.48 | 1.59 ± 0.48 | 1.66 ± 0.46 | 2.33 ± 0.55 | BB,HK,FB<SS |
| Knee joint GRF (%BW) | |||||
| Vertical | -117.95 ± 20.17 | -142.35 ± 33.47 | -142.99 ± 20.49 | -138.89 ± 27.84 | BB>HK,FB,SS |
| Anteroposterior | 13.10 ± 3.50 | 19.28 ± 16.97 | -8.77 ± 12.63 | 22.82 ± 7.70 | SS>BB,HK>FB |
| Mediolateral | 7.22 ± 13.20 | 4.36 ± 9.59 | 6.74 ± 9.03 | -7.26 ± 12.61 | BB,HK,FB>SS |
| Muscle forces (%BW) | |||||
| Quadriceps | 303.29 ± 57.23 | 467.34 ± 68.62 | 484.61 ± 68.84 | 567.06 ± 89.12 | BB<HK,FB<SS |
| Hamstring | 51.54 ± 41.64 | 51.86 ± 36.56 | 90.93 ± 40.12 | 95.75 ± 43.66 | BB,HK<FB,SS |
| BB, basic bounce; HK, high knee jumping rope; FB, Forward-backward jumping rope, SS, Side-to-side jumping rope; GRF, Ground reaction force; BW, Body weight; BWm, Body weight∙hegiht(meter) | |||||
| * The mean difference is significant at the p < .05 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



