
Submitted:
19 October 2023
Posted:
19 October 2023
You are already at the latest version
Abstract
Abstract: Background: The periodization of physical exercise to optimize the objectives is common in competitive sports, however physical exercise programs for the older adults do not usu-ally present periodization in their programming, they are limited to carrying out similar sessions throughout the program. Methods:137 people over 60 years old performed a physical exercise program, 71 people participated in a multicomponent non-periodized program as the Control Group (CG) and 66 people participated in a program periodized in blocks as the Experimental Group (EG). The block periodization program was oriented to the development of strength, and was carried out in 86 sessions three times per week during a period of 8 months. Anthropometric assessments were made using: weight, height, BMI and electrical bioimpedance; and functional evaluations through standardized tests: SPPB, TUG, handgrip and two-minute stair test. Results: After the intervention, the EG presents significant improvements in the TUG, in the weight and in the BMI. On the other hand, the CG presents significant improvements in fat weight, in BMI and in the 2-minute stair test. The SPPB did not present changes after the intervention. Conclusion: The periodization of physical exercise for older adults does not have a significant impact on the functional capacity in this population group.
Keywords:
physical activity
; older adults
; periodized training
1. Introduction
Physical exercise is a key factor in health and its benefits for the elderly population have been widely documented, and the WHO[1] includes it in its health recommendations. Physical exercise programs for older adults are widely spread and a wide variety of physical activities are offered.
Physical exercise must be carried out on a regular basis, continued over time and applying long-term programs. For this reason, medium and long-term goals must be established to enhance the beneficial effects of physical exercise and avoid the harmful ones.
Sports periodization is defined as the "intentional sequencing of different training units so that the athlete can achieve the desired state and planned results" [2]. Sports periodization has been used since 1950 in high-performance sports to ensure that all the sessions aid in reaching the goal, however, if we look at studies of physical exercise for older adults, it is not usual for an evolution of the program to be collected over a medium and long term.
Periodized physical exercise is common in other groups [3,4], while in the elderly population models based on the ACSM [5] indications for strength training are usually presented.
For example, a season of a professional athlete lasting between 9 and 12 months is usually periodized, during which he has moments of evaluation through competitions and a rest period. Similarly, many physical exercise programs for older adults are developed with a duration of 8 to 9 months, or even shorter, followed by a rest period that usually coincides with the summer period. Given the similarity of months dedicated in both high-performance sport and exercise for older adults, the idea arises to apply medium-term planning methods for sports, micro cycles, mesocycles, and macrocycles, to an older adult population.
For this reason, this study compares a block periodization model against a non-periodized model, in order to find out if there are differences between both models and whether periodization could present better results. The block periodization model groups sessions, with similar physical and technical objectives, during a determined period of time, creating a progression in the physical capacity of the subjects, reaching a maximum point of fitness in a specific time. This model creates three types of blocks: one focused on the volume of work performed, a second directed at the intensity with which the exercise is performed, and the last one focused on whether the exercises are related to what is going to be evaluated.
In addition, the periodization in blocks has focused on strength training, so that it is related to the periodization presented by the ACSM[5]. The non-periodized model is based on the Geriatric Revitalization Program (PReGe) of the University of Salamanca, which is oriented towards multi-component physical development, with a low or medium intensity session structure, widely proven during the years of the programs existence
2. Materials and Methods
Participants
The study included 137 people over 60 years of age, of both sexes, independent, autonomous and non-institutionalized, from the municipality of Salamanca (Spain). Participation is voluntary via registration with the Salamanca City Council in the Geriatric PReGe, developed by the Faculty of Nursing and Physiotherapy of the University of Salamanca since 1991. The PReGe is carried out in groups in different spaces of the city. The exclusion criteria are: having a percentile lower than 15 in the two-minute stair test together with a relative contraindication or physical limitation; that there is an absolute contraindication for physical exercise; present a pathology that does not allow the normal development of the program; and not carry out the evaluations. They are distributed in CG (Control Group) and EG (Experimental Group )through cluster sampling. The EG is made up of 70 people, of which 4 were excluded according to criteria, who carried out a program of physical exercise, structured in blocks and oriented to the development of strength. The CG is made up of 88 people, of whom 17 were excluded according to criteria.
Study Design
Two assessments are carried out, one prior to the intervention (E1) and another at the end of the intervention (E2). The assessment consists of anamnesis, anthropometric assessment and functional assessment. Anthropometric assessment consists of measuring weight using a scale (PPW3300/01, from Bosch – Germany), foot size by stadiometer (SECA 213 from SECA GMHB & Co – Germany), Body Mass Index (BMI), and the percentage of body fat assessed by electrical bioimpedance (OMROM BF 300 – Japan). The functional assessment consists of the Short Physical Performance Battery (SPPB), which includes assessment of bi-standing balance, semi-tandem and tandem, displacement of 4 meters and strength of the lower limb in which the participants were instructed to get up and sit down as quickly as possible from a chair five times without using the arms; the Timed Up & Go test in which the participants had to get up from a chair, move to a mark located 3 meters and return to sit in the chair; the Handgrip test (JAMAR Plus+ from Performance Health – USA) and the two-minute Staircase of the senior fitness test [6], in which the participants had to alternately raise knees to hip height for two minutes. The evaluations are carried out by physiotherapists and a physical educator, and the intervention by physiotherapists.
Two groups are proposed, an EG with periodized intervention and a CG without periodization. The periodization of the EG is adjusted to three blocks per grouping and in turn 4 groupings of blocks (Figure 1) were made; with a total of 86 sessions of 50 minutes for 8 months, with three sessions a week. The first block of each group was oriented to volume, the second to intensity, and the third to exercises similar to the tests contained in the evaluations. The session had a classic warm-up structure, with low-intensity, low-impact joint mobility exercises, the main part, with submaximal strength and resistance-strength exercises, and a return to calm, with low-impact, low-intensity aerobic resistance exercises . For the CG, the intervention consisted of a PreGe [7] based on multicomponent physical exercise with protocolization of the session. The session includes static stretching, easy walking or running, breathing exercises, dynamic stretching and muscle strength exercises, easy walking or running, hydration, coordination and balance, easy walking or running, relaxed breathing and hydration. A total of 86 sessions of 50 minutes are carried out for 8 months. The intervention of both groups was approved for Bioethics Committee of University of Salamanca.
Statistical Analysis
The statistical analysis has been carried out using the SPSS Statistics v.24 program. The means, median, variance, standard deviation, minimums and maximums are obtained and the Kolmogorov-Smirnov normality test (Lillefors correction) is performed, obtaining an abnormal distribution. Homogeneity between groups is analyzed using the Krustal-Wallis H test. The analysis of the pre- and post-intervention differences used the Wilconxon signed-rank test, also analyzing through age ranges of under 75 years, between 75 and 85 years and over 85 years. Due to the non-homogeneity between groups, an ANCOVA was carried out on the covariates of sex and age. A confidence interval of 95% has been taken.
3. Results
The results were analyzed based on the baseline after 86 sessions of intervention (Table 1 and Table 2), diving the population into three age ranges: under 75 years (eTable 1 for EG and eTable 2 for CG), between 75 and 85 years (eTable 3 for EG and eTable 4 for CG), and over 85 years (eTable 5 for EG and eTable 6 for CG).
The CG presents a significant reduction in weight (p=0) and in its fat weight (p<0.005). While the EG presents a significant weight reduction (p<0.005). The results of both groups improve significantly in the BMI. The calculation made by the fat percentage analysis system does not detect variation in the fat percentage in the EG.
The results in the balance tests of the SPPB do not show a deterioration or an improvement after the intervention, both in the case of the CG and the EG. The 4m displacement time of the SPPB does not show significant losses or improvements in the groups. The SPPB lower limb strength test does not show significant variations in the CG and EG. The strength of the upper limb present significant differences after the intervention in the EG. The 2-minute stair test presents better results in GE but without statistical significance, while the CG presents significant improvement in results after the intervention (p<0.005). In the Up & Go test, the EG has presented a significant improvement (p<0.005), while the CG does not present a change after the intervention. It should be noted that the <75 years of the CG present a significant improvement in the 2-minute stair test. In people in the range of 75-85 years, the CG presents a significant improvement in the 2-minute stair test, while the EG presents a significant improvement in the Up & Go test.
Regarding the >85 years, the CG presents a significant improvement in the Up & Go, like the EG, in addition the EG presents a significant improvement in the strength of the left upper limb.
4. Discussion
The periodization models of physical exercise derived from high level competition sports are difficult to adapt to the characteristics of the elderly population, so it was decided to experiment with a physical exercise program with a long history, the Geriatric Revitalization Program ( PReGe), and a widely contrasted sports training model, the ATR, with the aim of discovering if the latter could provide additional benefits to the study population that participated in the traditional program.
Regarding the results of the anthropometric variables, the BMI presents an improvement from the result of E-1 to E-2, framing both results in the overweight condition of the BMI classification [8], in both the CG and in the EG. After the intervention, both the EG and the CG, in all age groups, present a reduction in BMI, as has been seen in other studies that relate physical exercise to BMI [9,10].
Body weight presents a significant reduction in both groups, up to almost 2 kg of difference. On the contrary, the study by Ruiz-Montero [11] observed that weight was maintained or even increased in older adults with a 24-week program of aerobic Pilates, the same as Villareal[12] who concluded that physical exercise should be accompanied by a caloric restriction diet so that there is a reduction in weight. The Waters[13] review suggests that weight loss through physical exercise in people over 65 years of age is possible if accompanied by a change in lifestyle. It should be taken into account that the process of muscle atrophy accelerates after the age of 50, and can reach a loss of 30% of the muscle mass from the age of 80[14], and can influence our evaluation, the older a study population is, the more it will affect. The sarcopenia process can be retained or slowed down by strength training, with the EG model being the most beneficial for treating the pathology [15].
The results obtained in the reduction of fat weight in the sample have already been described previously in various studies; physical activity enables the control and reduction of adipose levels [16,17]. The CG model presents a significant reduction of the results in fat weight. The EG, for its part, presents a statistically significant reduction in weight and does not present differences in fat weight. From which we can conclude, that the EG model is not recommended for the maintenance of lean mass, since a decrease in total body weight has been observed, but without a decrease in fat mass.
The results of the SPPB balance assessment tests did not show any variation in either of the two groups (CG and EG) participating in this study, while previous PReGe studies did show improvements in balance [18], although others studies suggest that specific programs to improve balance[19] should be implemented to achieve positive results. The studies consulted [20,21] suggest that multicomponent physical exercise models improve the results in the lower limb strength test, but, paradoxically, those that have a more significant impact on the strength component present more modest results or show that there is no variation. Multicomponent physical exercise programs have been presented as a method to improve handgrip strength [22]. The CG presents good results in the hand grip strength test (handgrip), since it maintains the values after the intervention, which is relevant from the point of view of avoiding the deterioration inherent to aging. It is noteworthy that it is the EG that presents significant improvements in the handgrip test after the intervention in those over 85 years of age. The results obtained in the two-minute stair test vary according to age stratification, but studies such as those by Michael [23], Taguchi [24] and Severinsen[25] suggest that physical exercise programs present improvements in the aerobic tests. Severinsen[25] indicates that in physical exercise programs with a high predominance of strength work, specific tasks are required to improve in the six-minute walk test.
The results of our study suggest that the two models of physical exercise (CG and EG) are useful for the elderly population to maintain physical and functional capacity, since no negative evolution is observed in the tests carried out. For its part, a multicomponent physical exercise model appears to be more suitable for improving aerobic capacity. On the other hand, the strength-oriented physical exercise model presents a better result in strength-velocity, evaluated through the TUG, mainly in the group over 75 years of age.
Interventions that do not propose standardized planning present the effects produced by physical exercise at a random point within the program and not within the end of a cycle, as is the case with a periodized program, making it difficult to compare the results of one intervention or another. The EG planning model of our study does not conform to the classic methods of periodization of physical exercise in the elderly (linear, non-linear, and unplanned)[26]. For this reason we have not found published studies that fit models similar to ours.
The SPPB semi-tandem and feet together tests did not change after the intervention. The tandem test does not present significant variations in either of the two groups, however, it maintains the results obtained over time, this being positive for the study population. The systematic review by Latham et al. [19] indicates that physical exercise programs, focused mainly on the development of strength, do not have a significant influence on the results obtained in balance. Hafström [27] verified that in eight weeks there could be an improvement in balance with a proposal similar to the CG, while other research suggests that multicomponent groups only affect dynamic balance [28] . The study by Patil [29] with 409 women between 70 and 80 years old, presents similar results, mainly in the SPPB, in his proposal of 12 months of physical exercise similar to the CG. The review by Cadore and Rodríguez Mañas [30] also concluded that physical exercise improves balance, but that it is mainly the multicomponent programs that present said improvements in this aspect and that specific exercises should be included to improve this quality. The EG has not presented notable variations in the results of the balance assessments in our study, but it has shown a positive impact by maintaining the results over time. As previously mentioned, the implementation of a physical exercise program relevant to strength training, regardless of the periodization chosen, is not the model indicated for improving balance [31,32].
Our study does not present a statistically significant evolution in the 4-meter walk test in any of the groups, but it maintains the results avoiding the deterioration caused by age. In most cases, the difference between the mean of E-1 and E-2 is tenths or hundredths of a second, these differences could be due to the observation of the evaluator and therefore in future studies, it should be collected using electronic systems, such as photoelectric cells. The improvement of gait speed by a multicomponent low-intensity physical exercise program, such as that of the CG, is presented in different studies, such as the review and meta-analysis carried out by Hortobàgyi [33]. The study by VanSwearingen et al. [34] with 47 participants with a mean age of 77.2 years concluded that a multicomponent training presents improvements in movement speed, but better results are presented with a program more focused on gait re-education. Studies suggest that the development of force through non-linear periodization models allows improvements in short-distance displacement [35,36]. Our study points to a maintenance of walking speed capacity in short distance through a force-oriented ATR periodization. Bårdstu et al. [37] in a study with 104 participants, observed a stabilization of the results of gait speed in 20 meters in the group oriented to strength training after 8 months of the program. As previously indicated, Severinsen [25] considers it necessary to include specific gait activities to improve this indicator, while Cadore [30] does not consider it necessary to include this type of exercise to improve gait speed.
In our study, the lower limb strength test, corresponding to the SPPB, did not present significant variations, the same as in the 4-meter test. However, there are studies [38,39] where multicomponent physical exercise models do present improvements in lower limb strength. The study conducted by Oreskà et al[21] with 19 65-year-old subjects (±3.62) obtained significant improvements in the results obtained by a multicomponent exercise program. The lower limb strength test tends to be used as a means to analyze power, which is why it is usually used in studies that include a program aimed at developing strength [40]. The results obtained in these studies may be derived from the fact that the sample was sedentary, while our population has been participating in PReGE over the years. The study by Bårdstu [37], cited above, concluded that a strength-oriented physical exercise program presented a significant improvement in lower extremity strength tests, although Cadore et al[30] concluded that the use of a multicomponent or force model is indifferent to present an improvement in lower extremity strength. On the other hand, the ATR approach of the EG of this study is positive in lower extremity strength, since it maintains the results, although other studies present improvements in the mean results of this test[41]. On the other hand, Conlon et al[42] point out that the use of a block, or linear periodization model does not make a difference to the study result in this test.
Studies that present multicomponent programs have shown positive results in the assessment of upper limb strength [37,38]. In the present work, the results obtained by the CG are maintained after the intervention, avoiding the deterioration caused by age. Training models focused on strength have been shown to be effective in improving the results in the upper limb test[42]. Our study confirms that a strength-oriented program, such as the EG, allows maintaining and even presenting a tendency to improve the average results in the upper limb, although it does not present a significant difference.
The CG presents a positive evolution in the two-minute stair test. Lichtenstein et al[43] concluded in a study with 27 people that a multicomponent intervention presented better results than a traditional strength program, as can be seen in other studies[44]. The update carried out by Cadore and Izquierdo[45] suggests that the programs focused on the development of strength and aerobic capacity are the ones that present the best results in tests to assess aerobic capacity in a submaximal exercise such as the test of the 2 minute stair. Murlasits and Reed[46] hypothesize that nonlinear strength-oriented training does not affect the results of a test such as the 6-minute walk, or failing that, the two-minute stair test, as has been observed in the EG of this study.
Lacroix[47] and Zhuang[48] found that a multicomponent physical exercise program such as that of the CG improves the results in the TUG test. In our study, the CG does not present better results, but maintains them, this is relevant to avoid deterioration in the population studied. The TUG presents a statistically significant improvement in the EE, as observed by Coelho-Júnior et al[49] in a study with 45 women (60-79 years old), where the use of a DUP periodization model for 23 weeks decreased the completion time of the test by more than 50%. The significant improvement in this population is noteworthy, mainly in those over 85 years of age, taking into account that these programs are aimed at maintaining or avoiding physical deterioration.
The effects of the different interventions must be taken as independent, since there is no homogeneity in E-1 and therefore the groups are not comparable among themselves. The results obtained in our study, as Strohacker[50] already observed, do not allow us to definitively confirm that block planning is more effective than a non-periodized model.
The multicomponent program has presented an improvement in aerobic capacity, as well as in body weight and fat weight, while the periodization program for strength training presents improvements in strength-speed, an indicator for the prevention of falls.
5. Conclusions
We cannot conclude that a periodized intervention in blocks is more effective than a non-periodized intervention, but rather that, as has been widely documented, physical exercise, in any of its proposed forms, is beneficial for older adults, since it improves or maintains functional capacity. However, periodization makes it possible to improve the efficiency of physical exercise programs for older adults, providing them with a progression.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, eTable 1, eTable 2, eTable 3, eTable 4, eTable 5, eTable 6.
Author Contributions
Conceptualization, Alejandro Moreno-Mateos, Antonio Sánchez Muñoz and Carlos Moreno Pascual; Formal analysis, Alejandro Moreno-Mateos; Funding acquisition, Fausto Barbero Iglesias; Investigation, Alejandro Moreno-Mateos; Methodology, Alejandro Moreno-Mateos, Fausto Barbero Iglesias and Antonio Sánchez Muñoz; Project administration, Fausto Barbero Iglesias and Carlos Moreno Pascual; Resources, Fausto Barbero Iglesias and Carlos Moreno Pascual; Software, Alejandro Moreno-Mateos; Supervision, Fausto Barbero Iglesias and Carlos Moreno Pascual; Writing – original draft, Alejandro Moreno-Mateos; Writing – review & editing, Alejandro Moreno-Mateos and Yurena Gutiérrez Díaz.
Funding
This research was funded by Older Adults department of Salamanca City Council.
Institutional Review Board Statement
The study was approved by the Ethics Committee of University of Salamanca (Salamanca, Spain) (#444 18 December 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour at a Glance., 2020.
- Issurin V. Entrenamiento deportivo. Periodización en bloques. 3o edición. Badalona: Paidotribo, 2017.
- Heilbronn BE, Doma K, Gormann D et al. Effects of periodized vs. nonperiodized resistance training on army-specific fitness and skills performance., 2019. [CrossRef]
- Mattocks KT, Dankel SJ, Buckner SL et al. Periodization: What Is It Good For? [CrossRef]
- American College of Sports Medicine. Progression models in resistance training for healthy adults. Med Sci Sports Exerc 2009;41:687–708. [CrossRef]
- Rikli R, Jones J. The Senior Fitness Test. 2nd ed. Human Kinetics, 2012.
- Calvo-Arenillas JI, Parente T, Nobre J et al. Calidad de vida inicial de una muestra de mujeres mayores participantes en un programa de revitalización geriátrica. Psicología de La Salud y Promoción de La Calidad de Vida. Vol 15. Andavira, 2013.
- World Health Organization. Obesity : Preventing and Managing the Global Epidemic : Report of a WHO Consultation. World Health Organization, 2000.
- Jack Rejeski W, Brubaker PH, Goff DC et al. Translating weight loss and physical activity programs into the community to preserve mobility in older, obese adults in poor cardiovascular health. Arch Intern Med 2011;171:880–6.
- Swartz A, Strath S, Parker S et al. Ambulatory Activity and Body Mass Index in White and Non-White Older Adults. J Phys Act Health 2007;4:294–304. [CrossRef]
- Ruiz-Montero PJ, Castillo-Rodriguez A, Mikalački M et al. 24-weeks pilates-aerobic and educative training to improve body fat mass in elderly serbian women. Clin Interv Aging 2014;9:243–8. [CrossRef]
- Villareal DT, Chode S, Parimi N et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med 2011;364:1218–47. [CrossRef]
- Waters DL, Ward AL, Villareal DT. Weight loss in obese adults 65 years and older: A review of the controversy. Exp Gerontol 2013;48:1054–61. [CrossRef]
- Isidro Donate F. La sarcopenia y la mejora de la capacidad funcional del adulto mayor. Innovación e Investigación En Actividad Física y Deporte Para Mayores. Vol 8. Área de Gobierno y Servicios a la Ciudadanía. Delegación de Educación, Juventud y Deportes. Servicio de Deportes. Diputación de Málaga, 2020, 101–11.
- Borst SE. Interventions for sarcopenia and muscle weakness in older people. Age Ageing 2004;33:548–55. [CrossRef]
- Sedlmeier AM, Baumeister SE, Weber A et al. Relation of body fat mass and fat-free mass to total mortality: Results from 7 prospective cohort studies. Am J Clin Nutr 2021;113:639–46. [CrossRef]
- Alcazar J, Rodriguez-Lopez C, Ara I et al. Force-velocity profiling in older adults: An adequate tool for the management of functional trajectories with aging. Exp Gerontol 2018;108:1–6. [CrossRef]
- Méndez-Sánchez R. Evaluación y análisis de la eficacia del trabajo de flexibilidad de la cadena miofascial recta posterior y del equilibrio sobre el alcance funcional como predictor de caídas en personas mayores que realizan Revitalización Geriátrica. 2014. [CrossRef]
- Latham NK, Anderson CS, Lee A et al. A Randomized, Controlled Trial of Quadriceps Resistance Exercise and Vitamin D in Frail Older People: The Frailty Interventions Trial in Elderly Subjects (FITNESS). J Am Geriatr Soc 2003;51:291–9. [CrossRef]
- Meereis Lemos ECW, Guadagnin EC, Mota CB. Influence of strength training and multicomponent training on the functionality of older adults: Systematic review and meta-analysis. Revista Brasileira de Cineantropometria e Desempenho Humano 2020;22:1–20.
- Oreská Ľ, Slobodová L, Vajda M et al. Multimodal trainings of physical performance in elderly The effectiveness of two different multimodal training modes on physical performance in elderly. Eur J Transl Myol 2020;30:88–97.
- Labott BK, Bucht H, Morat M et al. Effects of Exercise Training on Handgrip Strength in Older Adults: A Meta-Analytical Review. Gerontology 2019;65:686–98. [CrossRef]
- Michael K, Goldberg AP, Treuth MS et al. Progressive adaptive physical activity in stroke improves balance, gait, and fitness: Preliminary results. Top Stroke Rehabil 2009;16:133–9. [CrossRef]
- Taguchi N, Higaki Y, Inoue S et al. Effects of a 12-month multicomponent exercise program on physical performance, daily physical activity, and quality of life in very elderly people with minor disabilities: An intervention study. J Epidemiol 2010;20:21–9. [CrossRef]
- Severinsen K, Jakobsen JK, Pedersen AR et al. Effects of resistance training and aerobic training on ambulation in chronic stroke. Am J Phys Med Rehabil 2014;93:29–42. [CrossRef]
- Moura BM, Ruas C V., Diefenthaeler F. Influence of Muscle Strength Gains on Functional Capacity Improvements following Resistance Training in Older Adults: A Linear Mixed Model Approach. Phys Occup Ther Geriatr 2020;39:113–28. [CrossRef]
- Hafström A, Malmström E-M, Terdèn J et al. Improved Balance Confidence and Stability for Elderly After 6 Weeks of a Multimodal Self-Administered Balance-Enhancing Exercise Program. Gerontol Geriatr Med 2016;2:1–13. [CrossRef]
- Liu CJ, Changa WP, De Carvalho IA et al. Effects of physical exercise in older adults with reduced physical capacity: Meta-analysis of resistance exercise and multimodal exercise. Int J Rehabil Res 2017;40:303–14. [CrossRef]
- Patil R, Uusi-Rasi K, Tokola K et al. Effects of a multimodal exercise program on physical function, falls, and injuries in older women: A 2-year community-based, randomized controlled trial. J Am Geriatr Soc 2015;63:1306–13. [CrossRef]
- Cadore EL, Rodríguez-Mañas L, Sinclair A et al. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuvenation Res 2013;16:105–14. [CrossRef]
- Latham NK, Anderson CS, Bennett DA et al. Progressive resistance strength training for physical disability in older people. Cochrane Database Syst Rev 2003. [CrossRef] [PubMed]
- Bulat T, Hart-Hughes S, Ahmed S et al. Effect of a group-based exercise program on balance in elderly. Clin Interv Aging 2007;2:655–60.
- Hortobágyi T, Lesinski M, Gäbler M et al. Effects of Three Types of Exercise Interventions on Healthy Old Adults’ Gait Speed: A Systematic Review and Meta-Analysis. Sports Medicine 2015;45:1627–43. [CrossRef]
- VanSwearingen JM, Perera S, Brach JS et al. Impact of exercise to improve gait efficiency on activity and participation in older adults with mobility limitations: A randomized controlled trial. Phys Ther 2011;91:1740–51. [CrossRef]
- Hayashida I, Tanimoto Y, Takahashi Y et al. Correlation between muscle strength and muscle mass, and their association with walking speed, in community-dwelling elderly Japanese individuals. PLoS One 2014;9:1–6. [CrossRef]
- Bray NW, Jones GJ, Rush KL et al. Multi-Component Exercise with High-Intensity, Free-Weight, Functional Resistance Training in Pre-Frail Females: A Quasi-Experimental, Pilot Study. Journal of Frailty and Aging 2020;9:111–7. [CrossRef]
- Bårdstu HB, Andersen V, Fimland MS et al. Effectiveness of a resistance training program on physical function, muscle strength, and body composition in community-dwelling older adults receiving home care: A cluster-randomized controlled trial. European Review of Aging and Physical Activity 2020;17. [CrossRef]
- Clemson L, Fiatarone M, Bundy A et al. Integration of balance and strength training into daily life activity to reduce rate of falls in older people (the LiFE study): randomised parallel trial. BMJ 2012;345:1–15. [CrossRef]
- Hagedorn DK, Holm E. Effects of traditional physical training and visual computer feedback training in frail elderly patients. A randomized intervention study. EUR J PHYS REHABIL MED 2010;46:159–68.
- Regterschot GRH, Folkersma M, Zhang W et al. Sensitivity of sensor-based sit-to-stand peak power to the effects of training leg strength, leg power and balance in older adults. Gait Posture 2014;39:303–7. [CrossRef]
- Fahlman MM, McNevin N, Boardley D et al. Effects of resistance training on functional ability in elderly individuals. American Journal of Health Promotion 2011;25:237–43. [CrossRef]
- Conlon JA, Newton RU, Tufano JJ et al. Periodization Strategies in Older Adults: Impact on Physical Function and Health. Med Sci Sports Exerc 2016;48:2426–36. [CrossRef]
- Lichtenstein E, Morat M, Roth R et al. Agility-based exercise training compared to traditional strength and balance training in older adults: A pilot randomized trial. PeerJ 2020:1–17. [CrossRef]
- Mahmoodi Z, Shabani R, Gholipour M. Eight Weeks of Exercise Training on 6MWT, Heart Function, and CHF Biomarker in Patients with Chronic Heart Failure. SN Compr Clin Med 2020;2:1453–61. [CrossRef]
- Cadore EL, Izquierdo M. How to simultaneously optimize muscle strength, power, functional capacity, and cardiovascular gains in the elderly: An update. Age (Omaha) 2013;35:2329–44. [CrossRef]
- Murlasits Z, Reed J. Muscular adaptations to periodized resistance-training in older adults. Sci Sports 2020;35:216–22. [CrossRef]
- Lacroix A, Kressig RW, Muehlbauer T et al. Effects of a supervised versus an unsupervised combined balance and strength training program on balance and muscle power in healthy older adults: A randomized controlled trial. Gerontology 2016;62:275–88. [CrossRef]
- Zhuang J, Huang L, Wu Y et al. The effectiveness of a combined exercise intervention on physical fitness factors related to falls in community-dwelling older adul. Clin Interv Aging 2014;9:131–40.
- Coelho-Júnior HJ, de Oliveira Gonçalvez I, Sampaio RAC et al. Periodized and non-periodized resistance training programs on body composition and physical function of older women. Exp Gerontol 2019;121:10–8. [CrossRef]
- Strohacker K, Fazzino D, Breslin WL et al. The use of periodization in exercise prescriptions for inactive adults: A systematic review. Prev Med Rep 2015;2:385–96. [CrossRef]
Figure 1.
Graph of volume, intensity and specific technique in block periodized.
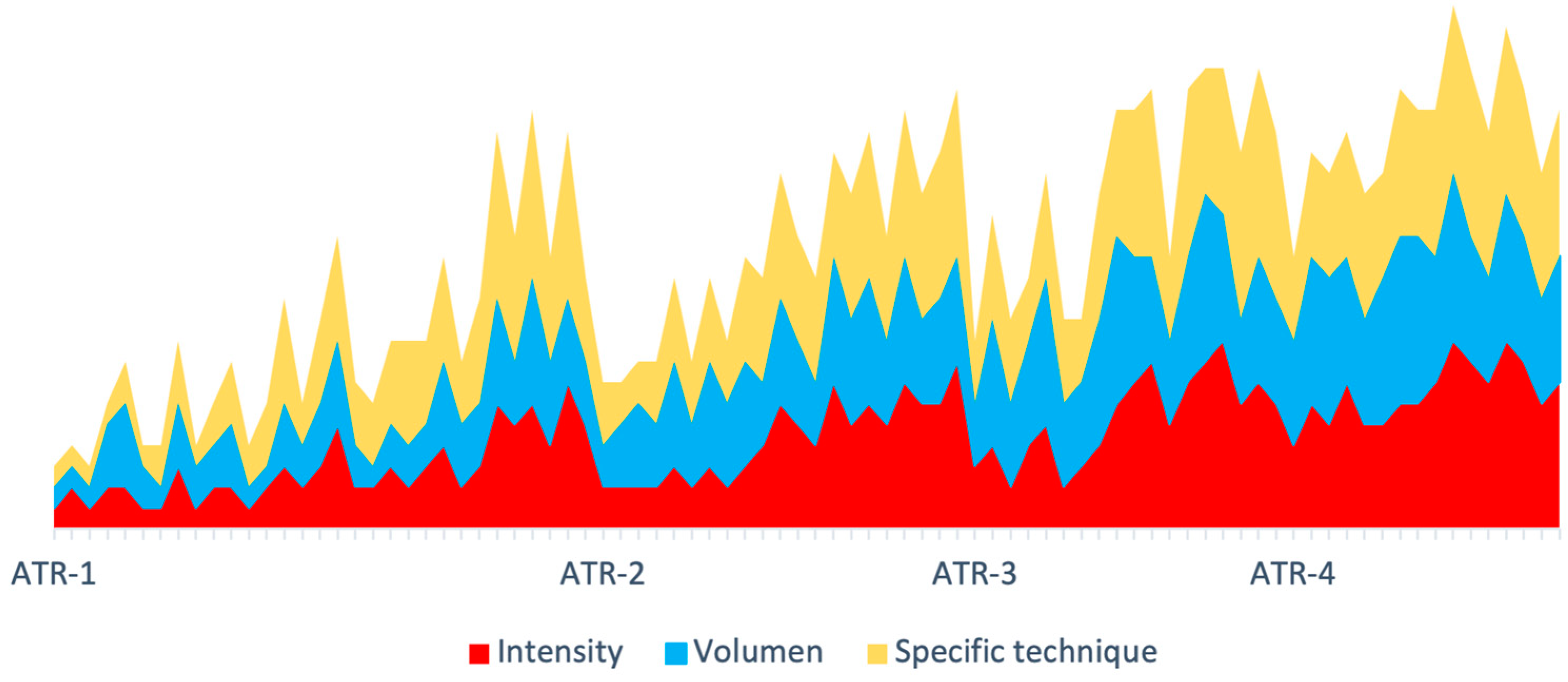

Table 1.
Baseline and results of Experimental Group.
| Experimental Group | Baseline E1 (N=66) | Final E2 (N=66) | p-value | ||
|---|---|---|---|---|---|
| Characteristics | |||||
| % Women | 57,6% | ||||
| Age average (years) | 79,05 (,665) | ||||
| Antrhopometric | |||||
| Weight (kg) | 66,1197 (1,44618) | 65,5066 (1,47093) | ,005* | ||
| Height (cm) | 153,1839 (,88423) | ||||
| BMI (kg/m2) | 28,0404 (,46446) | 27,7773 (,48135) | ,005* | ||
| % Body Fat | 43,120 (,5818) | 43,331 (,5562) | ,425 | ||
| Fat weight (kg) | 28,507 (,6787) | 28,326 (,6986) | ,073 | ||
| Functional Test | |||||
| Tandem (sec) | 9,0420 (,35501) | 9,0830 (,41727) | ,313 | ||
| 4m Walking (sec) | 4,4861 (,20368) | 4,5279 (,20227) | ,100 | ||
| Strong leg (sec) | 10,0388 (,47834) | 9,7239 (,45389) | ,335 | ||
| Handgrip Right (kg) | 20,0102 (,76774) | 20,9091 (1,06854) | ,131 | ||
| Handgrip Left (kg) | 19,7488 (,00783) | 20,5010 (1,06425) | ,133 | ||
| Up & Go (sec) | 9,0815 (,38562) | 80,2424 (3,46875) | ,000* | ||
| 2’ Step (steps) | 78,5366 (3,48500) | 8,0203 (,38029) | ,706 | ||
Table 2.
Baseline and results of Control Group.
| Control Group | Baseline E1 (N=71) | Final E2 (N=71) | p-value | ||
|---|---|---|---|---|---|
| Characteristics | |||||
| % Women | 80,3% | ||||
| Age average (years) | 76,94 (,709) | ||||
| Antrhopometric | |||||
| Weight (kg) | 66,1197 (1,44618) | 67,0403 (1,26658) | ,000* | ||
| Height (cm) | 153,1839 (,88423) | ||||
| BMI (km/m2) | 28,0404 (,46446) | 28,8645 (,51849) | ,000* | ||
| % Body Fat | 43,120 (,5818) | 43,273 (,6348) | ,365 | ||
| Fat weight (kg) | 28,507 (,6787) | 29,102 (,7600) | ,004* | ||
| Functional Test | |||||
| Tandem (sec) | 9,0420 (,35501) | 8,8626 (,39385) | ,122 | ||
| 4m Walking (sec) | 4,4861 (,20368) | 4,2956 (,11002) | ,907 | ||
| Strong leg (sec) | 10,0388 (,47834) | 10,6081 (,33604) | ,132 | ||
| Handgrip Right (kg) | 20,0102 (,76774) | 19,6767 (,57739) | ,445 | ||
| Handgrip Left (kg) | 19,7488 (,00783) | 19,9279 (2,92586) | ,812 | ||
| Up & Go (sec) | 9,0815 (,38562) | 82,0930 (2,34953) | ,132 | ||
| 2’ Step (steps) | 78,5366 (3,48500) | 7,9272 (,17525) | ,000* | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



