
Submitted:
18 October 2023
Posted:
19 October 2023
You are already at the latest version
Abstract
Introduction: The transcranial direct current stimulation (tDCS) is a promising technique for brain modulation after cerebrovascular accident (CVA). This treatment modality has been previously studied in the recovery of patients. The aim of this review is to analyze the evidence in the ap-plication of tDCS in the recovery of gait disturbance in stroke patients. Methods: This review was conducted according to the recommendations of the PRISMA statement. Three different elec-tronic databases were searched for relevant results: PubMed, Scopus, and Cochrane. We included reviews and meta-analyses that only considered randomized controlled trials (RCTs) that inves-tigated the effects of transcranial direct electrical stimulation, in combination or not with other physiotherapy treatment, on gait recovery. Results: Thirteen studies with a total of 195 RCTs were included. Data on population, outcome measures, protocols and outcomes were extracted. The Amstar-2 scale and the GRADE system of certainty of evidence were used. Only one study re-ceived high certainty of evidence, 5 received low certainty of evidence and 7 received critically low certainty of evidence. Conclusions: Although the tDCS produces positive changes in gait recovery in spatio-temporal parameters, mobility, endurance, strength and motor function, there is insuf-ficient evidence to recommend this treatment.
Keywords:
Physiotherapy
; neurorehabilitation
; gait
; transcranial electrical stimulation
; stroke
; non-invasive stimulation techniques
1. Introduction
Stroke is one of the leading causes of disability in the world and most survivors have limitations in mobility and gait [1]. Gait performance is considered an indicator of health and quality of life in people who have suffered a stroke [2], because gait performance is linked to the development of activities of daily living and community participation. Therefore, it is considered one of the most important objectives in the recovery of stroke survivors [3,4].
In recent years, numerous techniques have attempted to address gait impairments in stroke survivors from different approaches. Some of these techniques, such as percutaneous nerve electrostimulation, virtual reality, biofeedback using electromyography, neurophysiological approaches, or the use of auditory signals during gait re-education, have been classified by The America Stroke Association as level IIb-B evidence, indicating an unestablished recommendation and conflicts in evidence [5].
Non-invasive brain stimulation (NIBS) includes several techniques developed to achieve neuromodulation of the brain. It has its origins in the 1980s with the application of current to healthy subjects, which was a revolution compared to direct brain stimulation [6].. Two main techniques are described: magnetic fields and electrical stimulation. Transcranial electrical stimulation (TES) involves the application of a weak electrical current to the scalp, powered by batteries and connected to an anode and a cathode. Its effect lies in the modulation of the polarization of cell membranes, and it is voltage dependent [7,8]. The most popular type of TES is the tDCS [8]. The long-term effects of transcranial electrical stimulation are commonly defined by two concepts: long-term potentiation (LTP), related to neural excitation, and long-term depression (LTD), related to neural inhibition [9]. Both, which are a synaptic mechanism of plasticity, are related to the stimulation protocol; thus, the anode is more related to LTP effects, while the cathode is more related to LTD effects [10]. Their application is usually 1-2 mA and the duration of the treatment is between 10-30 minutes [11].
The key to the application of these techniques is the durability of the effects after treatment, which are associated with repeated stimulation in short periods of time, increasing the benefits and prolonging neuroplasticity. However, although the application of tDCS has a modulating effect at the cortical level that seems to favour the patient’s recovery and is associated with benefits in certain pathologies, there is a lack of evidence to support the use of these techniques for the recovery of gait in neurological patients [5]. This could be due to possible differences in application protocols, as factors such as electrode size, connector position and the conductivity of the different electrode materials, including saline concentration and conductive gel, could affect the results obtained [7].
Several reviews have attempted to answer the evidence of tDCS application for gait recovery in stroke patients [4,12,13,14,15,16,17,18,19,20,21,22,23,24]. However, the variability of the protocols and the heterogeneity of the outcome measures make it difficult to interpret the results. Other authors have attempted to synthesise and address the evidence for these protocols for the recovery of upper limb function [25] , however, no review of systematic reviews and meta-analyses for gait recovery has been conducted to allow the generation of evidence based tables and clinical recommendations. Therefore, an onverview of systematic reviews and meta-analyses is needed to summarise the effect of the application of tDCS in post-stroke patients for gait recovery, through the description of evidence based tables that facilitate the clinical recommendation of the different applications of this technique, using the GRADE method.
2. Materials and Methods
2.1 Database Search Strategy
The following databases were searched on 21 March 2023: PubMed, Scopus, and Cochrane Database of Systematic Reviews. The search terms used were: “stroke”, “cerebrovascular accident”, “apraxia of gait”, “gait disorder”, “gait dysfunction”. A combination of these and similar terms was performed using the Boolean operators AND and OR. We did not search the grey literature, as we aimed for studies that had been previously screened by reviewers. We also did not consult with experts in the field, conference abstracts, dissertations or reports not published on personal websites. The review protocol was registered with PROSPERO (CRD42021237915).
2.2. Eligibility Criteria
- Type of studies: This study only includes systematic reviews (with or without meta-analysis) that analysed randomised controlled trials due to their methodological quality. Published from 2015 to 2022. Only titles written in English and Spanish were considered.
-
Type of participants:
- ○
- Subjects diagnosed with an ischaemich or haemorrahagic stroke.
- ○
- Adults, over 18 years of age.
- ○
- Acute, sub-acute or chronic stroke.
- Type of intervention: we included studies in which the interventions involved tDCS, whether administered alone or in combination with another form of treatment and compared to another form of physical therapy, or placebo. We excluded papers that did not define interventions or multi-therapies and also any pharmacological treatment (e.g., botulinum toxin).
- Type of outcome measures: studies quantitatively assessing gait pattern (three-dimensional instrumental analysis systems), gait speed, functional mobility, endurance, motor function and muscle strength.
2.3. Study Selection and Data Extraction
The method of data collection was based on the Cochrane Handbook of Systematic Reviews of Interventions. Review Manager 5 software (RevMan 2020) was used for review writing [26].
Two reviewers screened the title, abstract and full texts independently for the inclusion of all systematic reviews potentially identified in the search. Differences were resolved by discussion, or, if necessary, consultation of a third team member.
Two authors independently extracted data from the reviews using a predefined data extraction form. Where outcome information was unclear or missing, the individual published file was accessed for further details.
2.4. Methodological Assessment and Evaluation of the Quality of Evidence
No reassessment was performed on the studies included in the reviews; however, the quality of the studies was reported according to the assessment of the author of each review. This information was subtracted during data collection and extraction.
The methodological quality of each systematic review was assessed using AMSTAR 2 (A Messurement Tool to Assess Systematic Review). Based in 16 items, this tool assesses the methodology used in a systematic review. Each item is rated as “yes” (clearly done), “no” (clearly not done), “cannot be answered”, or “not applicable”. Finally, the studies are classified according to their confidence. “High”, the SR has no weaknesses. “Medium”, no critical weaknesses, but some non-critical weaknesses. “Low”, some critical weaknesses. “Critically Low”, more than one critical weakness.
We assessed the quality of evidence for our primary endpoint, the evidence for the use of tDCS for gait training in stroke patients, using GRADE. We used the recommendation methods described in chapter 12, section 8.a of the Cochrane handbook [27], using GRADEproGDT software. All decisions to downgrade the quality of studies were justified by comments, so that the reader can understand the decisions and agree or disagree.
3. Results
3.1. Selection of Studies
A total of 47 studies were found, duplicates were removed leaving a total of 21 articles. Studies were screened by title and abstract to check that they met the previously established inclusion criteria. Finally, 13 reviews were included [4,12,13,14,15,18,19,20,21,22,23,24,28] with a total of 195 randomised controlled trials (RCT) included. The selection process is shown in the flow chart (Figure 1) with a list of excluded studies, reasons, and funding (Table S1).
3.2. Methodological Quality Assessment
The results of the methodological assessment of the included systematic reviews/meta-analyses are shown in Table 2. Only one study was rated with “High” confidence [12], although, it did not justify the study design decision. While 7 studies were rated with “Critically Low” confidence [4,14,18,20,21,22,28], the remaining 5 studies were classified with “Low” confidence. [13,15,19,23,24].
3.3. Assessing the Quality of Evidence
The results of the evidence assessment of the included systematic reviews/meta-analyses are shown in Table S1. The following outcomes of interest were broken down: gait speed, functional mobility, endurance, motor function and muscle strength.
3.4. Summary of Results
The characteristics of the included studies are summarised in Table 3. Of the 13 included studies, we found 8 meta-analyses [4,12,14,18,20,21,22,28] and 5 systematic reviews [13,15,19,23,24]. All articles defined the intervention as applying tDCS in combination with another physiotherapy treatment (treadmill, walking assistance robot, conventional physiotherapy, etc.) or alone. The control group received a placebo stimulation treatment in combination or not with physiotherapy, or a different stimulation protocol.
The outcome measures described by the reviews were organised as follows: spatiotemporal parameters of gait [4,13,14,15,18,19,20,21,23,24,28] functional mobility [4,13,14,15,18,19,20,21,23,24] gait endurance [4,13,15,18,19,20,21,23,24] motor function [17,19,24,28] muscle strength [4,12,13,14,24] and lower limb functionality [12,22].
3.4.1. Effect of tDCS in Combination with Physiotherapy on Spatiotemporal Parameters.
The outcome measures described for this outcome were 10MWT (10 Meter walk test), quantitative analysis using technological systems and gait cadence. For gait speed, the meta-analyses by Li et al. [4], Vaz et al. [14], Tien et al. [18] and Dong et al. [21] found no significant improvements in their meta-analyses.
Mitsutake et al. [20] included both online and offline stimulation in their analysis. Only the online application showed a significant improvement over offline.
According to GRADE, the certainty of the evidence for these studies was classified as “low” and “very low”.
As for systematic reviews, Paz et al. [13] and Santos et al. [19] expressed significant improvements in walking speed (9.09%, p=0.046). For Navarro-López et al. [15] and Bressi et al. [24] there were no significant improvements in any of the included studies. For the review by Corominas-Teruel et al. [23] the results were presented as effect size. Only one study showed a large effect in this respect.
According to GRADE, they were classified as “low” and “very low” certainty (Table S2).
3.4.2. Effect of tDCS in Combination with Physiotherapy on Functional Mobility
The outcome measures were the TUG (Time up and go), the FAC (Functional ambulatory category), the RMI (Rivermead mobility index) and the Tinetti test. In the studies by Vaz et al. [14], Mitsutake et al. [20] and Dong et al. [21] found no significant improvements in their meta-analysis evaluated by FAC and TUG. Whereas Tien et al. [18], who found significant improvements describing FAC, RMI and TUG, found no significant differences with the Tinetti test. According to GRADE, the certainty of evidence was classified as “low” and “very low”. However, Li et al. [4] who were the only ones with a “moderate” certainty of evidence, showed significant improvements for functional mobility.
In terms of systematic reviews, studies find controversial results depending on the outcome measures used. It is noted that Paz et al. [13] Navarro-López et al. [15] Bressi et al. [24] and Santos et al. [19] do not provide sufficient evidence to recommend the use of tDCS for functional mobility.
For the review by Corominas-Teruel et al. [23], who evaluated the results using cohen’s d, also did not consider there was insufficient evidence for a treatment recommendation.
3.4.3. Effect of tDCS in Combination with Physiotherapy on Endurance
The outcome measure for this outcome was the 6MWT (6 Minute walking test). Li et al. [4], Tien et al. [18] and Dong et al. [21] reported no significant improvements in their meta-analyses.
Mitsutake et al. [20] included both online and offline application in their analysis. Only the online application showed significant improvements over the offline application. According to GRADE, the certainty of the evidence was classified as “low” and “very low”.
In terms of systematic reviews, the included studies show controversial results. Paz et al. [13], Navarro-López et al. [15], Santos et al. [19] and Bressi et al. [24] were not considered to show significant improvements in gait endurance. Corominas-Teruel et al. [23], who evaluated the results using cohen’s d, also did not have enough evidence to make a treatment recommendation. According to GRADE, the certainty of the evidence was classified as “low” and “very low” (Table S2).
3.4.4. Effect of tDCS in Combination with placebo On Motor Function
The outcome measure used for this outcome was the FMA-LE (Fugl-Meyer assessment lower extremity). Dong et al. [21] and Li et al. [16] reported no significant improvement. According to GRADE, the certainty of the evidence was classified as “low”.
The systematic review by Paz et al. [13], Navarro-López et al. [15], Santos et al. [19] and Bressi et al. [24] were not considered to have enough evidence to recommend the use of tDCS to improve motor function. According to GRADE, the certainty of the evidence was classified as “very low” (Table S2).
3.4.5. Effect of tDCS in Combination with Physiotherapy on Muscle strength
The outcome measures for this outcome were the MRC (Medical research council) and MI-LE (Motricity index lower extremity). Although Li et al. [4] reported significant improvements, Vaz et al. [14] did not report significant improvements for muscle strength. According to GRADE, the certainty of the evidence was classified as “low” and “very low”.
3.4.6. Effect of tDCS in Combination with Placebo on Lower Limb Function
Outcome measures for this outcome were spatiotemporal parameters (10MWT and cadence), endurance (6MWT), functional mobility (FAC, Tinetti and MI-LE), motor function (FMA) and balance (BBS). Elsner et al. [12], showed no significant improvements in either statistical analysis. Veldema et al. [22], performed a comparative meta-analysis of different stimulation protocols. They described a large effect in the application of tDCS in contralateral and bilateral hemispheres.
The certainty of the evidence was classified as “low” and “very low” (Table S2).
4. Discussion
This review has included 8 meta-analyses and 5 systematic reviews with the aim of assessing the quality of evidence regarding the application of tDCS in the recovery of gait in post-ACV patients. The evidence has been assessed using the AMSTAR-2 tools for risk of bias and GRADEpro for certainty of evidence. Outcome measures for lower limb recovery were extracted and classified as follows: spatiotemporal parameters (gait speed and cadence), functional mobility, endurance, muscular strength, motor function and lower limb functionality.
Although some studies have shown that tDCS improves significantly gait speed [20], functional mobility [4,13,18], muscle strength [4], endurance [20] and functionality of the lower limbs [22] compared to sham stimulation, and to the control group, the certainty of the evidence does not seem homogeneous to recommend the benefits of the application of tDCS.
Brain reorganisation after stroke seems to be crucial to patient recovery [29], however, it has been observed that the healthy hemisphere may influence this reorganisation during the recovery period. Abnormalities are observed in the interhemispheric relationship to produce voluntary movement [30] and the reduced excitability of the injured hemisphere, particularly the primary motor cortex (M1), compared to the intact hemisphere. [31]. Also, some theories point to the influence of the intact hemisphere on affect, although this cannot be confirmed. Therefore, although tDCS techniques appear to be a useful tool for influencing factors related to corticospinal excitability of the injured hemisphere and recovery, the results seem to be inconclusive.
Previous authors have reviewed the evidence for these techniques in upper limb recovery [32,33], but there does not seem to be clear evidence of their influence on functional recovery. Whereas other authors have shown significant results in the application of tDCS for the prevention of falls and recovery of the lower limb [34]. This may be due to differences in the brain representation of the upper limbs compared to the lower limbs. It has been observed that the activation of mechanically similar joints does not follow the same patterns as would be expected, in fact, it is related to the task being performed. For example, in a brain image we can see that the contraction of the elbow follows a more lateralised pattern, while the contraction of the knee follows a more medial pattern. [35]. Therefore, tDCS techniques may give different results depending on the task targeted for recovery, as reflected in this gait study.
In this review, we found a large heterogeneity of findings suggesting that the application of tDCS could lead to improvements in gait, but not all results seem to be conclusive. This could be explained by differences in application protocols or sample size, as most of them include a small number of participants, even in combination with several studies. As for the outcome measures, there is a high heterogeneity in the management and statistical analysis of these data.
On the other hand, it is important to mention the differences in the application protocols for the different techniques. Regarding the application of tDCS, the intensity applied in the included studies ranges between 1-2.5 mA, although other authors have previously set the threshold for corticospinal excitation at 2 mA for the anode [36]. Another important factor is the application of unilateral or bilateral tDCS. Most of the included reviews involve studies where unilateral application (anode or cathode) is predominant for excitatory or inhibitory purposes. Although the benefit of unilateral application in post-ACV patients has been demonstrated [37], some reviews continue to include RCTs that perform bilateral application [4,15,18]. Finally, some studies differentiate between online delivery, which combines stimulation and some targeted activity simultaneously, and offline delivery, which performs pre-treatment stimulation. No direct benefits are observed for offline stimulation. [20].
This overview of systematic reviews and meta-analyses presents an update of the evidence on the application of tDCS for gait recovery. However, these results should be interpreted with caution due to some limitations in the review process. First, only studies published in any journal that were in English and/or Spanish were included. Second, an exhaustive search of the grey literature was not conducted. Third, the sample size in the included studies is too small to draw robust conclusions. Fourth, some reviews include studies with a high risk of bias, especially in randomisation and blinding of patients, therapists, and assessors.
5. Conclusions
This paper suggests that tDCS, in combination with other therapies, may help improve gait recovery in stroke patients. However, the results appear inconclusive, and the certainty of the evidence was classified as low and very low for most outcomes. Thus, the application of tDCS is classified as inconclusive, indicating that the review found low, very low or insufficient quality evidence for the effectiveness of the treatment.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Excluded studies; Table S2: Summary of the quality of evidence (GRADE).
Author Contributions
Conceptualization and methodology, software, investigation, resources, writing—original draft preparation, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wonsetler, E.C.; Bowden, M.G. A Systematic Review of Mechanisms of Gait Speed Change Post-Stroke. Part 1: Spatiotemporal Parameters and Asymmetry Ratios. Top Stroke Rehabil 2017, 24, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Ghai, S.; Ghai, I. Effects of (Music-Based) Rhythmic Auditory Cueing Training on Gait and Posture Post-Stroke: A Systematic Review & Dose-Response Meta-Analysis. Sci Rep 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Alingh, J.F.; Groen, B.E.; van Asseldonk, E.H.F.; Geurts, A.C.H.; Weerdesteyn, V. Effectiveness of Rehabilitation Interventions to Improve Paretic Propulsion in Individuals with Stroke – A Systematic Review. Clinical Biomechanics 2020, 71, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Fan, J.; Yang, J.; He, C.; Li, S. Effects of Transcranial Direct Current Stimulation on Walking Ability after Stroke: A Systematic Review and Meta-Analysis. Restor Neurol Neurosci 2018, 36, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association; 2016; Vol. 47, ISBN 0000000000000. [Google Scholar]
- Michener, G.R.; Beecher, M.D.B.; Johnson, V.R.; Brooke, M. de L. Stimulation of the Cerebral Cortex in the Intact Human Subject. Nature 1980. [Google Scholar]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-Based Guidelines on the Therapeutic Use of Transcranial Direct Current Stimulation (TDCS). Clinical Neurophysiology 2017, 128, 56–92. [Google Scholar] [CrossRef] [PubMed]
- Polanía, R.; Nitsche, M.A.; Ruff, C.C. Studying and Modifying Brain Function with Non-Invasive Brain Stimulation. Nat Neurosci 2018, 21, 174–187. [Google Scholar] [CrossRef]
- Antal, A.; Luber, B.; Brem, A.K.; Bikson, M.; Brunoni, A.R.; Cohen Kadosh, R.; Dubljević, V.; Fecteau, S.; Ferreri, F.; Flöel, A.; et al. Non-Invasive Brain Stimulation and Neuroenhancement. Clin Neurophysiol Pract 2022, 7, 146. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Farahani, F.; Bikson, M.; Parra, L.C. Weak DCS Causes a Relatively Strong Cumulative Boost of Synaptic Plasticity with Spaced Learning. Brain Stimul 2022, 15, 57–62. [Google Scholar] [CrossRef]
- Kesikburun, S. Non-Invasive Brain Stimulation in Rehabilitation. Turk J Phys Med Rehabil 2022, 68, 1. [Google Scholar] [CrossRef]
- Elsner, B.; Kugler, J.; Pohl, M.; Mehrholz, J. Transcranial Direct Current Stimulation (TDCS) for Improving Activities of Daily Living, and Physical and Cognitive Functioning, in People after Stroke (Review). Cochrane Library 2020. [Google Scholar] [CrossRef]
- De Paz, R.H.; Serrano-Muñoz, D.; Pérez-Nombela, S.; Bravo-Esteban, E.; Avendaño-Coy, J.; Gómez-Soriano, J. Combining Transcranial Direct-Current Stimulation with Gait Training in Patients with Neurological Disorders: A Systematic Review. J Neuroeng Rehabil 2019, 16, 4–11. [Google Scholar] [CrossRef]
- Vaz, P.G.; Salazar, A.P. da S.; Stein, C.; Marchese, R.R.; Lukrafka, J.L.; Plentz, R.D.M.; Pagnussat, A.S. Noninvasive Brain Stimulation Combined with Other Therapies Improves Gait Speed after Stroke: A Systematic Review and Meta-Analysis. Top Stroke Rehabil 2019, 26, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Navarro-López, V.; Molina-Rueda, F.; Jiménez-Jiménez, S.; Alguacil-Diego, I.M.; Carratalá Tejada, M. Effect of Transcranial Direct Current Stimulation Combined with Rehabilitation on Gait Pattern, Balance, and Functionality in Stroke Patients: A Systematic Review. diagnostics 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Fan, J.; Yang, J.; He, C.; Li, S. Effects of Repetitive Transcranial Magnetic Stimulation on Walking and Balance Function after Stroke: A Systematic Review and Meta-Analysis; 2018; Vol. 97, ISBN 0000000000000. [Google Scholar]
- Tung, Y.C.; Lai, C.H.; Liao, C. De; Huang, S.W.; Liou, T.H.; Chen, H.C. Repetitive Transcranial Magnetic Stimulation of Lower Limb Motor Function in Patients with Stroke: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin Rehabil 2019, 33, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Tien, H.H.; Liu, W.Y.; Chen, Y.L.; Wu, Y.C.; Lien, H.Y. Transcranial Direct Current Stimulation for Improving Ambulation after Stroke: A Systematic Review and Meta-Analysis. International Journal of Rehabilitation Research 2020, 43, 299–309. [Google Scholar] [CrossRef]
- Santos, L.V.; Lopes, J.B.P.; Duarte, N.A.C.; Castro, C.R.A. de P.; Grecco, L.A.C.; Oliveira, C.S. TDCS and Motor Training in Individuals with Central Nervous System Disease: A Systematic Review. J Bodyw Mov Ther 2020, 24, 442–451. [Google Scholar] [CrossRef]
- Mitsutake, T.; Imura, T.; Hori, T.; Sakamoto, M.; Tanaka, R. Effects of Combining Online Anodal Transcranial Direct Current Stimulation and Gait Training in Stroke Patients: A Systematic Review and Meta-Analysis. Front Hum Neurosci 2021, 15, 1–12. [Google Scholar] [CrossRef]
- Dong, K.; Meng, S.; Guo, Z.; Zhang, R.; Xu, P.; Yuan, E.; Lian, T. The Effects of Transcranial Direct Current Stimulation on Balance and Gait in Stroke Patients: A Systematic Review and Meta-Analysis. Front Neurol 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Veldema, J.; Gharabaghi, A. Non-Invasive Brain Stimulation for Improving Gait, Balance, and Lower Limbs Motor Function in Stroke. J Neuroeng Rehabil 2022, 19. [Google Scholar] [CrossRef]
- Corominas-Teruel, X.; Mozo, R.M.S.S.; Simó, M.F.; Colomina Fosch, M.T.; Valero-Cabré, A. Transcranial Direct Current Stimulation for Gait Recovery Following Stroke: A Systematic Review of Current Literature and Beyond. Front Neurol 2022, 13. [Google Scholar] [CrossRef]
- Bressi, F.; Cinnera, A.M.; Morone, G.; Campagnola, B.; Cricenti, L.; Santacaterina, F.; Miccinilli, S.; Zollo, L.; Paolucci, S.; Di Lazzaro, V.; et al. Combining Robot-Assisted Gait Training and Non-Invasive Brain Stimulation in Chronic Stroke Patients: A Systematic Review. Front Neurol 2022, 13, 795788. [Google Scholar] [CrossRef] [PubMed]
- Lüdemann-Podubecká, J.; Bösl, K.; Nowak, D.A. Repetitive Transcranial Magnetic Stimulation for Motor Recovery of the Upper Limb after Stroke. Prog Brain Res 2015, 218, 281–311. [Google Scholar] [CrossRef] [PubMed]
- The cochrane collaboration Review Manager (RevMan) [Computer Program] 2020.
- Higgins, J. Manual Cochrane de Revisiones Sistemáticas de Intervenciones, Versión 5.1. 0. Manual Cochrane de Revisiones Sistemáticas de Intervenciones, versión 5.1.0, 2012; 1–639. [Google Scholar]
- Kuwahara, W.; Sasaki, S.; Yamamoto, R.; Kawakami, M.; Kaneko, F. The Effects of Robot-Assisted Gait Training Combined with Non-Invasive Brain Stimulation on Lower Limb Function in Patients with Stroke and Spinal Cord Injury: A Systematic Review and Meta-Analysis. Front Hum Neurosci 2022, 16. [Google Scholar] [CrossRef]
- Ward, N. Assessment of Cortical Reorganisation for Hand Function after Stroke. J Physiol 2011, 589, 5625. [Google Scholar] [CrossRef]
- Murase, N.; Duque, J.; Mazzocchio, R.; Cohen, L.G. Influence of Interhemispheric Interactions on Motor Function in Chronic Stroke. Ann Neurol 2004, 55, 400–409. [Google Scholar] [CrossRef]
- McDonnell, M.N.; Stinear, C.M. TMS Measures of Motor Cortex Function after Stroke: A Meta-Analysis. Brain Stimul 2017, 10, 721–734. [Google Scholar] [CrossRef]
- Hatem, S.M.; Saussez, G.; della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front Hum Neurosci 2016, 10, 1–22. [Google Scholar] [CrossRef]
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F. Interventions for Improving Upper Limb Function after Stroke. Cochrane Database of Systematic Reviews 2013, 2013. [Google Scholar] [CrossRef]
- Andrade, S.M.; Ferreira, J.J. de A.; Rufino, T.S.; Medeiros, G.; Brito, J.D.; da Silva, M.A.; Moreira, R. de N. Effects of Different Montages of Transcranial Direct Current Stimulation on the Risk of Falls and Lower Limb Function after Stroke. Neurol Res 2017, 39, 1037–1043. [Google Scholar] [CrossRef]
- Luft, A.R.; Smith, G. V.; Forrester, L.; Whitall, J.; Macko, R.F.; Hauser, T.K.; Goldberg, A.P.; Hanley, D.F. Comparing Brain Activation Associated with Isolated Upper and Lower Limb Movement across Corresponding Joints. Hum Brain Mapp 2002, 17, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, D.T.; Norton, J.A.; Roy, F.D.; Gorassini, M.A. Effects of Transcranial Direct Current Stimulation on the Excitability of the Leg Motor Cortex. Exp Brain Res 2007, 182, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Halakoo, S.; Ehsani, F.; Hosnian, M.; Zoghi, M.; Jaberzadeh, S. The Comparative Effects of Unilateral and Bilateral Transcranial Direct Current Stimulation on Motor Learning and Motor Performance: A Systematic Review of Literature and Meta-Analysis. Journal of Clinical Neuroscience 2020, 72, 8–14. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart (PRISMA).
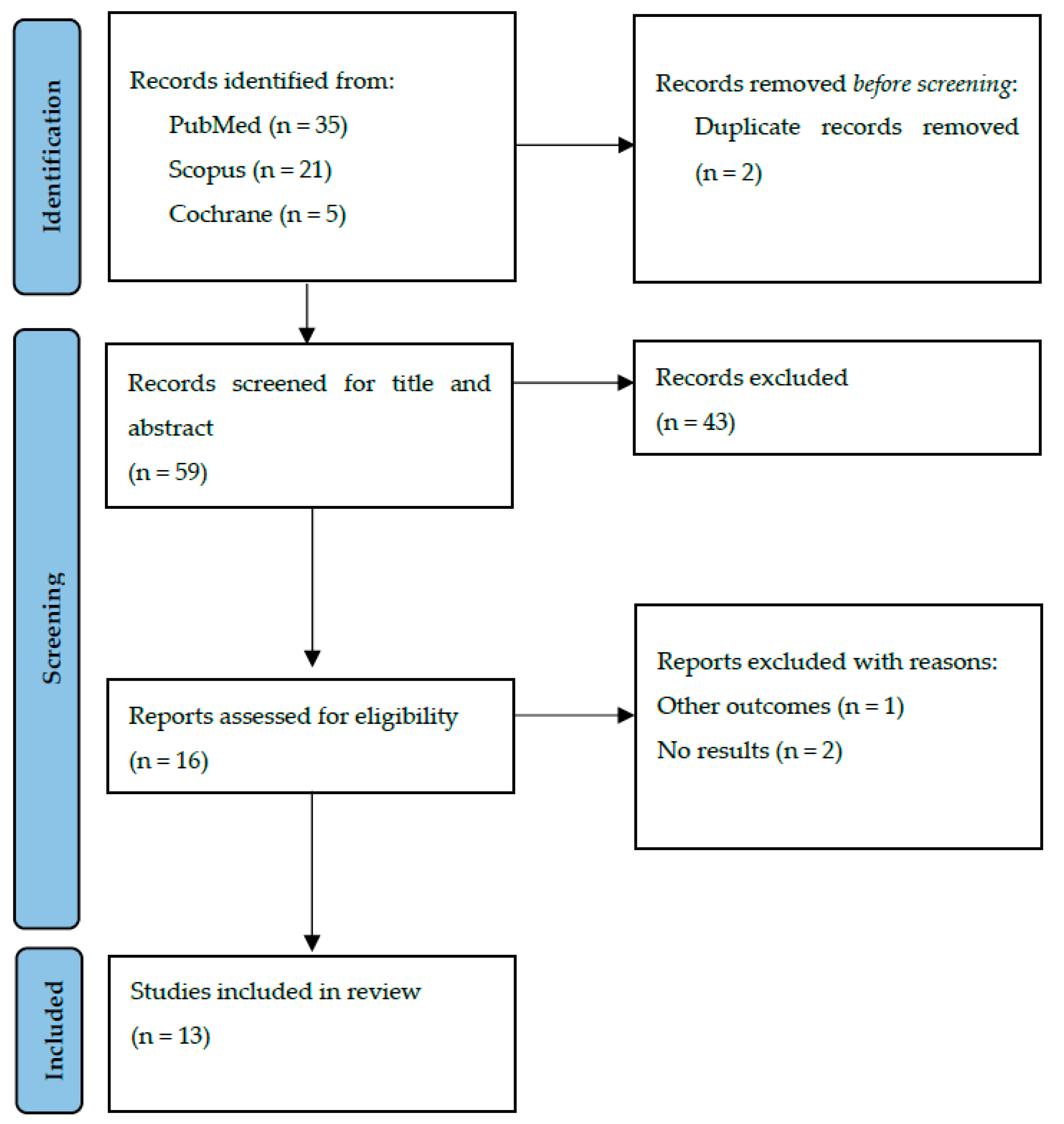

Table 1.
Full search strategy.
| PubMed Search |
|---|
| 2,(((stroke) AND (NIBS)) OR (tDCS)) AND (gait),Most Recent,"Meta-Analysis, Systematic Review, from 2016 - 2022","((((""stroke""[MeSH Terms] OR ""stroke""[All Fields] OR ""strokes""[All Fields] OR ""stroke s""[All Fields]) AND ""NIBS""[All Fields]) OR (""transcranial direct current stimulation""[MeSH Terms] OR (""transcranial""[All Fields] AND ""direct""[All Fields] AND ""current""[All Fields] AND ""stimulation""[All Fields]) OR ""transcranial direct current stimulation""[All Fields] OR ""tdcs""[All Fields])) AND (""gait""[MeSH Terms] OR ""gait""[All Fields])) AND ((meta-analysis[Filter] OR systematicreview[Filter]) AND (2016:2022[pdat]))" |
| Cochrane Search |
| "transcranial direct current stimulation":ti,ab,kw AND "stroke":ti,ab,kw |
| Scopus Search |
| stroke AND tdcs AND gait AND PUBYEAR > 2014 AND PUBYEAR < 2023 AND ( LIMIT-TO (DOCTYPE , "re")) AND (LIMIT-TO ( SUBJAREA, "HEAL")) |
Table 2.
AMSTAR checklist.
| AMSTAR Checklist | Li et al. | De Paz et al. | Vaz et al. | Elsner et al. | Tien et al. | Santos et al. | Mitsutake et al. | Dong et al. | Navarro-López et al. | Veldema et al. | Corominas-Teruel et al. | Bressi et al. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| 2 | N | N | Y | Y | N | Y | Y | Y | N | N | Y | Y |
| 3 | N | N | N | N | N | N | N | N | N | N | N | N |
| 4 | PY | PY | PY | Y | N | PY | PY | PY | Y | PY | PY | PY |
| 5 | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| 6 | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| 7 | N | N | N | Y | N | N | N | N | PY | N | N | N |
| 8 | Y | Y | Y | Y | Y | Y | Y | PY | Y | Y | Y | Y |
| 9 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 10 | N | N | N | Y | N | N | N | N | N | N | N | N |
| 11 | Y | NA | Y | Y | Y | NA | Y | Y | NA | Y | NA | NA |
| 12 | Y | NA | N | Y | Y | NA | Y | Y | NA | Y | NA | NA |
| 13 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 14 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 15 | N | NA | N | Y | N | NA | N | N | NA | N | NA | NA |
| 16 | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Overall assessment | Critically low | Low | Critically low | High | Critically low | Low | Critically low | Critically low | Low | Critically low | Low | Low |
1= Question PICO; 2= Protocol registered prior to review; 3= Justification of the design of the studies included; 4= adequate literature search; 5= Selection of duplicate studies; 6= Duplicate data extraction; 7= Justification of excluded studies; 8= Adequate description of the studies included; 9=Risk of bias of individual included studies; 10= source of funding for the studies included; 11= Appropriate meta-analytical methods; 12= Risk of bias assessment on meta-analysis; 13= Consideration of the risk of bias in the interpretation of the results of the review; 14= Explanation of heterogeneity in results; 15= Assessment of the presence and impact of publication bias; 16= Conflict of interest.
Table 3.
Summary of included studies.
| Review | Data assessed as up to date | Population | Interventions | Comparison interventions | Outcomes for which data were reported | Review limitations |
|---|---|---|---|---|---|---|
| Li et al. (2018) [4] | April 2017 (English) | Post-stroke patients over 18 years of age |
tDCS:
|
Simulated treatment (complementary robot-assisted treatments, task-related training, robotic orthoses and conventional rehabilitation) |
|
|
| De Paz et al. (2019) [13] | 2018 | Patients diagnosed with a pathology of the central nervous system | tDCS applying anode in ipsilateral (affected) hemisphere (n=4). |
|
|
|
| Vaz et al. (2019) [14] | December 2018 | Subjects who have suffered an acute/subacute (less than six months) or chronic (more than six months) stroke. |
tDCS:
|
|
|
|
| Elsner et al. (2020) [12] | January 2019 (all languages) | Post-stroke patients over 18 years of age |
tDCS:
|
|
|
|
| Tien et al. (2020) [18] | January 2019 | Post-stroke patients over 18 years of age |
tDCS:
|
Simulated treatment of tDCS. |
|
|
| Santos et al. (2020) [19] | October 2018 | Children, adolescents, adults and older people who do not have a progressive central nervous system disease. | tDCS in combination with motor training. | Simulated treatment in combination with motor training. |
|
|
| Matsutake et al. (2021) [20] | 19 March 2021 | Patients diagnosed with haemorrhagic or ischaemic stroke with unilateral hemiplegia. They can walk without support and can maintain their weight and balance. |
tDCS:
|
Simulated tDCS treatment in combination with robot-assisted gait therapy or neuromuscular stimulation. |
|
|
| Dong et al. (2021) [21] | August 2020 | Patients who have been diagnosed with a stroke. | tDCS applying anode in ipsilateral hemisphere. | Simulated treatment of tDCS. |
|
|
| Navarro-López et al. (2021) [15] | March 2020 | Patients who have been diagnosed with a stroke. |
tDCS:
|
Simulated treatment of tDCS. |
|
|
| Veldema et al. (2022) [22] | 31 March 2021 | Patients diagnosed with stroke |
NIBS:
|
Simulated stimulation | Lower limb functionality (combining outcome measures of balance, gait and motor function). |
|
| Corominas-Teruel et al. (2022) [23] | 7 February 2022 | Patients who have suffered a stroke aged 18 years or older | tDCS. | Simulated stimulation alone or in combination with other therapies. |
|
|
| Bressi et al. (2022) [24] | 15 March 2021 | Patients over 18 years of age who have suffered a stroke in a chronic process (>6 months). | tDCS in combination with gait-assisted robot | Simulated stimulation |
|
|
tDCS= Transcranial Direct-Current Stimulation; rTMS= repetitive transcranial magnetic stimulation; NIBS= Non-invasive brain stimulation; iTBS= intermitent transcranial brain stimulation; tACS= transcranial alterning current stimulation; tsDCS= transcranial spinal direct current stimulation ; FAC= Functional Ambulatory Category; TUG= Time Up and Go; FMA= Fugl Meyer Assessment; mEFAP= modified Emory Functional Ambulatory Profile; 6MWT= 6 minutes walking test; 10MWT= 10 meters walking test; MAS= Modified Ashworth Scale; RMI= Rivermead Mobility Index; CT= conventional therapy; MI-LE= Lower limb Motricity Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



