Submitted:
20 October 2023
Posted:
20 October 2023
You are already at the latest version
Abstract
Current treatments in patients with pancreatic cancer offer limited benefits. In this report, we applied “alkalization therapy”, which was efficacious for other solid tumors at our clinic, to stage 4 pancreatic cancer patients, and investigated its effect on disease prognosis. Patients with metastatic pancreatic cancer who were treated at Karasuma Wada Clinic in Kyoto, Japan, between 2011 and 2022 were included in the study. All patients received alkalization therapy (combination of an alkaline diet, bicarbonate, and citric acid administration), alongside standard chemotherapy. Urine samples were collected to assess urine pH as a marker for whole-body alkalization. In the 98 patients analyzed, the median overall survival (OS) from the time of diagnosis was 13.2 months. Patients with a mean urine pH of 7.5 or greater had a median OS of 29.9 months, compared with 15.2 months for those with a mean urine pH of 6.5 to 7.5, and 8.0 months for those with a mean urine pH of less than 6.5, which suggests a trend of a longer OS in patients with a higher urine pH. Conclusions: Alkalization therapy may offer a viable approach to enhance the survival of stage 4 pancreatic cancer patients, who typically have an unfavorable prognosis.
Keywords:
Pancreatic cancer
; Cancer metabolism
; Alkalization therapy
; Tumor microenvironment
; Urine pH
1. Introduction
Pancreatic cancer is a devastating disease with a rapidly increasing incidence and a very high mortality rate. In Japan, the incidence rate is 34.8 per 100,000 population, and the 5-year relative survival rate is 8.5% [1]. Moreover, it is the fourth leading cause of cancer death in Japan [1]. Most patients with pancreatic cancer have local invasion and distant metastasis at the time of diagnosis, making curative resection impossible in many cases. Even if surgery is performed, the recurrence rate is high, and the prognosis is unfavorable. To overcome this situation, either the discovery of a clinically applicable method for detecting tumors at a resectable stage, or the establishment of an effective nonsurgical treatment to prevent tumor progression is needed, and to date, various studies have been conducted on these points. Among the currently available treatments, nonsurgical treatments, such as chemotherapy and radiotherapy have continued to provide some extension of survival time for pancreatic cancer patients, but the results are still not satisfactory.
We have been focusing on the tumor microenvironment (TME) surrounding malignant tumors as a possible therapeutic target. Our reasons are as follows: 1) Malignant tumors use glycolysis for their cellular metabolism, and release more protons into the extracellular space than normal cells, lowering the pH of the TME to acidic levels [2]. 2) The acidic TME attracts inflammatory cells that cause chronic inflammation, and creates a more favorable environment for tumor growth[3]. Based on these molecular and cell biological findings, we hypothesized that preventing malignant tumors from creating an acidic TME, and reversing it by raising the pH of the TME would inhibit tumor growth and decrease its resistance to anticancer drugs[4]. We then devised an original treatment method that we named “alkalization therapy”, which can be applied clinically based on this idea. “Alkalization therapy” is a simple therapy performed by shifting the patient’s diet to one that is expected to alkalize the whole body, and furthermore, its effect is enhanced by combining it with the administration of alkalizing agents, such as bicarbonate and citric acid[5,6,7]. We have obtained favorable results using alkalization therapy at our clinic in patients with various types of cancers, such as malignant lymphoma, gastric cancer, small cell lung cancer, and breast cancer[8,9] In addition, we previously conducted a study on patients with advanced pancreatic cancer at our clinic, and reported that the combination of chemotherapy and alkalization therapy showed a significant advantage over chemotherapy alone, with a median overall survival (OS) of 15.4 months (combination treatment group) vs. 10.8 months (chemotherapy alone group) (p < 0.005)[10].
However, one problem is the method to evaluate whether or not “alkalization therapy” is actually contributing to increasing the pH of the TME. We previously reported the association between urine pH and antitumor effects, in our evaluation of the potential use of urine pH as an indicator of whether or not alkalization therapy is being performed adequately. In a study on patients with hepatocellular carcinoma, in which alkalization therapy was monitored by urine pH, we found that the median OS from the start of alkalization therapy in patients with a urine pH of 7.0 or greater was not reached (n = 12; 95% confidence interval (CI) = 3.0–not reached), which was significantly longer than that in patients with a pH of less than 7.0 (15.4 months; n = 17; 95% CI = 5.8–not reached, p < 0.05)[11].
In the present study, we applied “alkalization therapy”, which has shown favorable outcomes as an effective nonsurgical treatment for various solid tumors as well as advanced pancreatic cancer at our clinic, to a cohort of “stage 4” pancreatic cancer patients, and additionally investigated the effect of urine pH levels on prognosis improvement.
2. Patients and Methods
2.1. Study Design
This study was a retrospective analysis performed to assess the potential effects of alkalization therapy on patients with metastatic pancreatic cancer. The patients were treated at Karasuma Wada Clinic in Kyoto, Japan, between January 1, 2011, and April 30, 2022. Data were collected from the clinic’s medical records. All participants received alkalization therapy, which consisted of an alkalizing diet and the oral administration of alkalizing agents (bicarbonate and citric acid). Alkalization therapy was performed in conjunction with standard chemotherapies for pancreatic cancer. A flowchart of patient inclusion/exclusion is shown in Figure 1.
Flowchart showing the number of patients analyzed in this study. Of the 209 patients with pancreatic cancer who visited Karasuma Wada Clinic between January 2011 and April 2022, 131 were diagnosed as having stage 4 cancer. After excluding 21 patients who visited fewer than 3 times, and 12 patients for whom urine samples could not be collected, a total of 98 patients were included in the analysis
2.2. Alkalization Therapy
Alkalization therapy was defined by a combination of an alkaline diet and the oral administration of bicarbonate (3.0−5.0 g/day) and/or citric acid (3.0−6.0 g/day). The alkaline diet consists of a large amount of fruits and vegetables, and minimal amounts of meat and dairy products. Patients were guided to consume at least 400 g of fruits and vegetables daily, while avoiding meat and dairy products. Patients documented their meals for the initial 4 weeks of the diet. At each visit, a doctor or nurse reviewed the patients’ meal logs to ensure dietary adherence, and offered advice based on the meal logs. Ultimately, the final dietary choices were at the discretion of the patients.
2.3. Assessment Procedures
The median OS from the time of the initial diagnosis was calculated. Urine samples were collected during regular patient visits, which occurred at a minimum of once every 2 months and up to twice a month. The OS from the time of initial diagnosis was then compared among the following 3 groups: 1) patients with a mean urine pH of 7.5 or higher, 2) patients with a mean urine pH of 6.5 or higher but less than 7.5, and 3) patients with a mean urine pH of less than 6.5.
2.4. Statistical Analyses
For each patient, mean urine pH values were measured for all collected urine samples, from the patient’s initial visit to Karasuma Wada Clinic through to April 30, 2022. Standard deviations of the mean values in the dataset were also calculated. All p-values were 2-sided, and a p-value of less than 0.05 was considered to indicate a statistically significant difference between groups. All statistical procedures were performed using Easy R (version 1.61; Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical interface adapted from R (The R Foundation for Statistical Computing, Vienna, Austria)[12]
3. Results
3.1. Patient Characteristics
Between January 1, 2011, and April 30, 2022, 209 patients with pancreatic cancer visited Karasuma Wada Clinic. Of these, 131 patients were diagnosed as having stage 4 cancer. After excluding 21 patients who visited fewer than 3 times, and 12 patients for whom urine samples could not be collected, a total of 98 patients were included in the analysis (Figure 1). The cohort consisted of 53 men and 45 women. The mean age at their first visit to Karasuma Wada Clinic was 64.5 years, with a range of 27 to 88 years. All of the patients underwent alkalization therapy.
3.2. OS of Patients with Different Urine pHs
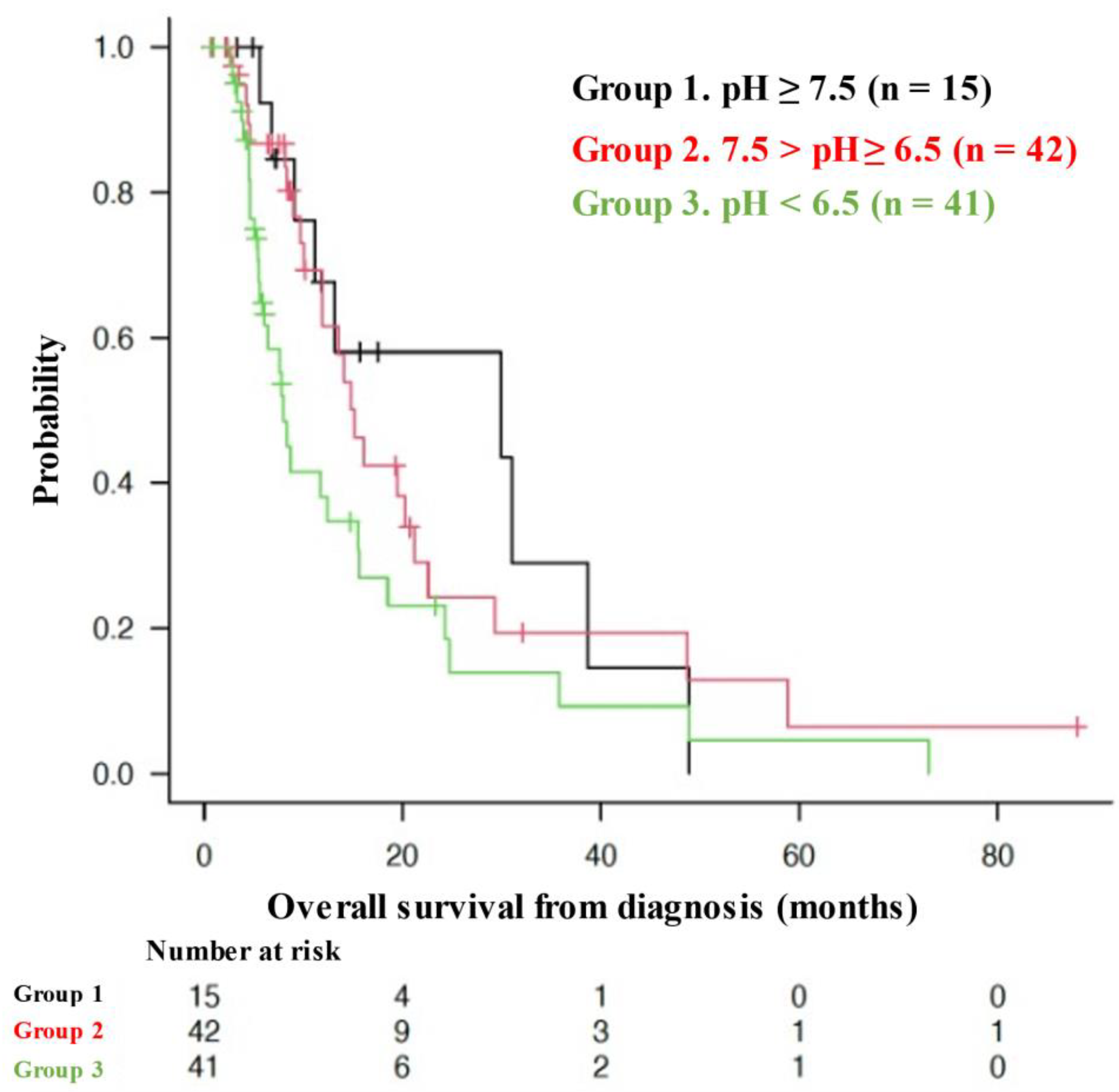
The median OS of all patients from the time of diagnosis was 13.2 months (95% CI = 9.7–16.1 months), as shown in Figure 2. Figure 3 shows the Kaplan–Meier curves for the OS of patients stratified by mean urine pH levels, as follows: those with a mean urine pH of 7.5 or higher, those with a mean urine pH of 6.5 to less than 7.5, and those with a mean urine pH of less than 6.5. The median OS was 29.9 months for the 15 patients with a mean urine pH of 7.5 or higher (95% CI = 9.1–38.7), 15.2 months for the 42 patients with a pH between 6.5 and less than 7.5 (95% CI = 10.1–21.2), and 8.0 months for the 41 patients with a pH of less than 6.5 (95% CI = 5.6–15.5). Despite not reaching statistical significance, there was a discernible trend, i.e., higher urine pH correlated with extended OS.
Kaplan–Meier curve of the overall survival (OS) of the patients from the time of diagnosis. The median OS of all patients from the time of diagnosis was 13.2 months (95% CI = 9.7–16.1 months)
Kaplan–Meier curves of the overall survival (OS) from the start of alkalization therapy of patients with a mean urine pH of ≥ 7.5 (Group 1), 7.5 > pH ≥ 6.5 (Group 2), and pH < 6.5 (Group 3). The pH ≥ 7.5 group (Group 1, n = 15): median OS = 29.9 months (95% CI = 9.1–38.7), the 7.5 > pH ≥ 6.5 group (Group 2, n = 42): median OS = 15.2 months (95% CI = 10.1–21.2), the pH < 6.5 group (Group 3, n = 41): median OS = 8.0 months (95% CI = 5.6–15.5).
4. Discussion
The increase in the number of pancreatic cancer patients is a global trend, and the incidence of pancreatic cancer is expected to increase further in the future. The reason for this is that the risk of pancreatic cancer increases with age, and the proportion of the population aged 65 years and older is expected to double globally in the next few decades. Therefore, the incidence of pancreatic cancer is expected to continue to increase for the next several decades[13]. Moreover, pancreatic cancer tends to have an unfavorable prognosis because, 1) most patients have advanced cancer at the time of diagnosis, 2) early vascular and neural invasion and distant metastasis are common, 3) the effects of anticancer chemotherapy and radiotherapy are limited, and 4) there is a complex TME (various interactions between neoplastic and stromal cells within the TME), and 5) multiple genetic and acquired mutations can cause the disease; there are few prevalent genetic mutations, and none of the most commonly mutated genes are currently druggable[14,15]. Particularly for patients with stage 4 pancreatic cancer with distant metastasis, current treatments, such as systemic chemotherapy and radiotherapy, have reached their limits in terms of prolonging survival, and more innovative and effective treatments are needed.
At our clinic, we encounter many patients with advanced-stage cancers that are not suitable for curative surgery, systemic chemotherapy, or radiotherapy. Therefore, we perform alkalization therapy, which is based on the concept of increasing the pH of the whole body and the TME to achieve antitumor effects, and have achieved favorable results[5,8,9,10,16,17,18]. Whether alkalization therapy has been performed adequately or not is assessed by measuring the patient’s urine pH, and we have previously reported that higher urine pH is associated with longer survival in hepatocellular carcinoma patients and pancreatic cancer patients[10,11]. In the present study, we designed a single-center, retrospective, observational study to investigate whether alkalization therapy can prolong the survival of stage 4 pancreatic cancer patients. We furthermore investigated the association between urine pH levels and the prognosis of the patients.
Involvement of the TME in tumor growth and proliferation has long been recognized[19]. The fact that cancer cells depend on glycolysis for their energy metabolism is a concept that was initially proposed by Otto Warburg et al. (the Warburg effect)[20]. As a result, protons are released from tumor cells into the extracellular space, making the TME acidic[21]. Acidification of the TME leads to the attraction and infiltration of inflammatory cells, which further exacerbates chronic inflammation[22]. This promotes angiogenesis and blood flow imbalance in the tumor, resulting in chronic hypoxia and a vicious cycle of the activation of glycolysis, TME acidification, chronic inflammation, and then the further activation of glycolysis[20]. Previous basic science studies have shown that the pH around normal cells surrounding a tumor is 7.2 to 7.4, whereas that around tumor cells is 6.6 to 7.0[23,24,25,26]. The aim of alkalization therapy is to break or reverse this vicious cycle of glycolysis, TME acidification, chronic inflammation, and further activation of glycolysis, and to achieve antitumor effects by increasing the pH of the TME[16,27,28]. As in our previous reports, this clinical study proposes an important paradigm shift that not only the malignant tumor itself but also the TME should be considered as a major therapeutic target.
All 98 patients who visited our clinic more than 3 times and had their urine pH measured had stage 4 pancreatic cancer with distant metastasis. All of them were instructed on how to follow an alkaline diet (concept sharing and nutritional guidance), but the final dietary preferences and choices were left to the patients. We judged whether alkalization therapy was being performed according to the instructions or not by measuring the patient’s urine pH. Theoretically, a higher urine pH indicates successful implementation of alkalization therapy. In this study, only 22 patients achieved an average urine pH of 7.5 or higher. This shows that the degree of alkalization therapy achieved varies from patient to patient, even though all of them were instructed on how to perform alkalization therapy. This also shows that simply sharing the concept of and providing guidance on alkalization therapy does not necessarily result in alkalization of the whole body.
The first-line chemotherapy recommended by the guidelines for pancreatic cancer with distant metastasis in Japan is either folinic acid, fluorouracil, irinotecan oxaliplatin (FOLFIRINOX) therapy or gemcitabine hydrochloride + nab-paclitaxel combination therapy[29]. A basis for this recommendation is a single-arm phase 2 trial of modified FOLFIRINOX therapy, which enrolled 69 patients and reported a median OS of 11.2 months (95% CI = 9.0–not reached)[30]. However, the regimen was associated with serious adverse events and death due to treatment, and the authors cautioned readers about the toxicity of this regimen in their paper[30]. Another basis is a single-arm phase 2 trial of gemcitabine hydrochloride + nab-paclitaxel combination therapy, which enrolled 34 patients and reported a median OS of 13.5 months (95% CI = 10.6–not reached). This regimen was reported to have a lower incidence of adverse events than FOLFIRINOX therapy[31].
In this study, the median OS from the time of diagnosis of the patients who received alkalization therapy in addition to standard treatment was 13.2 months (95% CI = 9.7–16.1), which was comparable or superior to that of patients who received the 2 regimens recommended by the guidelines for pancreatic cancer with distant metastasis in Japan (FOLFIRINOX or gemcitabine hydrochloride + nab-paclitaxel combination)for the treatment of pancreatic cancer. Moreover, the median OS of the group with an average urine pH of 7.5 or higher was 29.9 months (95% CI = 9.1–38.7), which can be considered as an outstanding result exceeding the prognosis of patients receiving standard treatment. By comparing the median OS of the 3 groups divided by average urine pH levels, i.e., a pH of 7.5 or higher, 6.5 or higher but less than 7.5, and less than 6.5, we observed that longer patient survival depended on a higher average urine pH, which suggested that there was a correlation between average urine pH and the achievement of the objective of alkalization therapy.
This study has several limitations. First, it was a single-center retrospective observational study, and we could not compare the outcomes with a non-intervention group of patients who did not receive alkalization therapy. This is because all patients in this study were introduced to alkalization therapy (concept sharing and nutritional guidance) at our clinic and underwent alkalization therapy, so there was no control group that did not receive alkalization therapy. In addition, to further confirm the efficacy of alkalization therapy, a standardized protocol for “alkalization therapy” should be created, and a prospective cohort study should be conducted at multiple centers in the future. Second, there was a large variation in patient backgrounds, mainly in the time from diagnosis to the start of alkalization therapy. Although this study was limited to patients with stage 4 pancreatic cancer with distant metastasis, there may be a need to adjust for background factors, such as sex, location of metastasis, and other concurrent treatments. Furthermore, it would be ideal if alkalization therapy could be started immediately after disease diagnosis, as this may demonstrate the effect of alkalization therapy more clearly. Finally, we used urine pH as a target marker for alkalization therapy. The pH of body fluids, such as urine and blood, changes over time owing to various factors, and may vary greatly depending on underlying diseases or medications. In addition, the degree of pH change of the TME may vary depending on the malignancy and number of tumor cells. In the future, we hope to identify all factors that affect the pH of the TME, clarify their interactions, and draw conclusions based on them.
5. Conclusions
We have demonstrated the potential of alkalization therapy in combination with standard treatments to prolong the survival of patients with stage 4 pancreatic cancer with distant metastasis, which has a very unfavorable outcome. We also found that an increase in urine pH may contribute to further survival extension in patients with advanced pancreatic cancer. Further studies are required to confirm the clinical efficacy of alkalization therapy in preventing TME acidification and achieving antitumor effects.
Author Contributions
Conceptualization and methodology, H.W. and R.H.; data curation, R.N., R.H and H.M.; writing—original draft preparation, M.I. and R.H.; writing—review and editing, R.H.; supervision, T.O and H.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Japan Chapter of the American College of Chest Physicians and has been registered with UMIN Clinical Trials under registration number UMIN000052333, date of approval (September 21st, 2023).
Informed Consent Statement
This research was conducted using retrospective data. Patients were provided the option to opt-out from the study. Therefore, written informed consent was not obtained.
Data Availability Statement
All data analyzed during this study are included in the published article.
Acknowledgments
The authors thank Dr. Helena Akiko Popiel of Tokyo Medical University for her editing of this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Monitoring of Cancer Incidence in Japan - Survival 2009-2011 report (Center for Cancer Control and Information Services, National Cancer Center, 2020) [Japanese]. 2009-2011.
- Corbet, C.; Feron, O. Tumour acidosis: From the passenger to the driver's seat. Nat. Rev. Cancer 2017, 17, 577–593. [Google Scholar] [CrossRef] [PubMed]
- Koppenol, W.H.; Bounds, P.L.; Dang, C.V. Otto Warburg's contributions to current concepts of cancer metabolism. Nat. Rev. Cancer 2011, 11, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Neri, D.; Supuran, C.T. Interfering with pH regulation in tumours as a therapeutic strategy. Nat. Rev. Drug Discov. 2011, 10, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, R.; Okamoto, T.; Sato, M.; Hasegawa, M.; Wada, H. Effects of an Alkaline Diet on EGFR-TKI Therapy in EGFR Mutation-positive NSCLC. Anticancer. Res. 2017, 37, 5141–5145. [Google Scholar] [CrossRef]
- Robey, I.F.; Lopez, A.M.; Roe, D.J. Safety and Tolerability of Long-Term Sodium Bicarbonate Consumption in Cancer Care. J. Integr. Oncol. 2015, 4, 128. [Google Scholar] [CrossRef]
- Ando, H.; Eshima, K.; Ishida, T. Neutralization of Acidic Tumor Microenvironment (TME) with Daily Oral Dosing of Sodium Potassium Citrate (K/Na Citrate) Increases Therapeutic Effect of Anti-cancer Agent in Pancreatic Cancer Xenograft Mice Model. Biol. Pharm. Bull. 2021, 44, 266–270. [Google Scholar] [CrossRef]
- Wada, H.; Hamaguchi, R.; Narui, R.; Morikawa, H. Meaning and Significance of "Alkalization Therapy for Cancer". Front. Oncol. 2022, 12, 920843. [Google Scholar] [CrossRef]
- Hamaguchi, R.; Narui, R.; Morikawa, H.; Wada, H. Improved Chemotherapy Outcomes of Patients With Small-cell Lung Cancer Treated With Combined Alkalization Therapy and Intravenous Vitamin C. Cancer Diagn. Progn. 2021, 1, 157–163. [Google Scholar] [CrossRef]
- Hamaguchi, R.; Ito, T.; Narui, R.; Morikawa, H.; Uemoto, S.; Wada, H. Effects of Alkalization Therapy on Chemotherapy Outcomes in Advanced Pancreatic Cancer: A Retrospective Case-Control Study. In Vivo 2020, 34, 2623–2629. [Google Scholar] [CrossRef]
- Isowa, M.; Hamaguchi, R.; Narui, R.; Morikawa, H.; Wada, H. Effects of alkalization therapy on hepatocellular carcinoma: A retrospective study. Front. Oncol. 2023, 13, 1179049. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Kommalapati, A.; Tella, S.H.; Goyal, G.; Ma, W.W.; Mahipal, A. Contemporary Management of Localized Resectable Pancreatic Cancer. Cancers 2018, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, R.; Isowa, M.; Narui, R.; Morikawa, H.; Wada, H. Clinical review of alkalization therapy in cancer treatment. Front. Oncol. 2022, 12, 1003588. [Google Scholar] [CrossRef]
- Hamaguchi, R.; Uemoto, S.; Wada, H. Editorial: The impact of alkalizing the acidic tumor microenvironment to improve efficacy of cancer treatment. Front. Oncol. 2023, 13, 1223025. [Google Scholar] [CrossRef]
- Hamaguchi, R.; Narui, R.; Wada, H. Effects of Alkalization Therapy on Chemotherapy Outcomes in Metastatic or Recurrent Pancreatic Cancer. Anticancer. Res. 2020, 40, 873–880. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Gatenby, R.A.; Gillies, R.J. Why do cancers have high aerobic glycolysis? Nat. Rev. Cancer 2004, 4, 891–899. [Google Scholar] [CrossRef]
- Cardone, R.A.; Casavola, V.; Reshkin, S.J. The role of disturbed pH dynamics and the Na+/H+ exchanger in metastasis. Nat. Rev. Cancer 2005, 5, 786–795. [Google Scholar] [CrossRef]
- Cairns, R.A.; Harris, I.S.; Mak, T.W. Regulation of cancer cell metabolism. Nat. Rev. Cancer 2011, 11, 85–95. [Google Scholar] [CrossRef]
- Gillies, R.J.; Raghunand, N.; Garcia-Martin, M.L.; Gatenby, R.A. pH imaging. A review of pH measurement methods and applications in cancers. IEEE Eng. Med. Biol. Mag. 2004, 23, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Raghunand, N.; Karczmar, G.S.; Bhujwalla, Z.M. MRI of the tumor microenvironment. J. Magn. Reson. Imaging 2002, 16, 430–450. [Google Scholar] [CrossRef] [PubMed]
- Helmlinger, G.; Yuan, F.; Dellian, M.; Jain, R.K. Interstitial pH and pO2 gradients in solid tumors in vivo: High-resolution measurements reveal a lack of correlation. Nat. Med. 1997, 3, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, F.A.; Kettunen, M.I.; Day, S.E.; Hu, D.E.; Ardenkjaer-Larsen, J.H.; Zandt, R.; Jensen, P.R.; Karlsson, M.; Golman, K.; Lerche, M.H.; et al. Magnetic resonance imaging of pH in vivo using hyperpolarized 13C-labelled bicarbonate. Nature 2008, 453, 940–943. [Google Scholar] [CrossRef]
- Bogdanov, A.; Chubenko, V.; Volkov, N.; Moiseenko, F.; Moiseyenko, V. Tumor acidity: From hallmark of cancer to target of treatment. Front. Oncol. 2022, 12, 979154. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Ibrahim-Hashim, A.; Ordway, B.; Gatenby, R.A. Back to basic: Trials and tribulations of alkalizing agents in cancer. Front. Oncol. 2022, 12, 981718. [Google Scholar] [CrossRef] [PubMed]
- Okusaka, T.; Nakamura, M.; Yoshida, M.; Kitano, M.; Ito, Y.; Mizuno, N.; Hanada, K.; Ozaka, M.; Morizane, C.; Takeyama, Y.; et al. Clinical Practice Guidelines for Pancreatic Cancer 2022 from the Japan Pancreas Society: A synopsis. Int J Clin Oncol 2023, 28, 493–511. [Google Scholar] [CrossRef] [PubMed]
- Ozaka, M.; Ishii, H.; Sato, T.; Ueno, M.; Ikeda, M.; Uesugi, K.; Sata, N.; Miyashita, K.; Mizuno, N.; Tsuji, K.; et al. A phase II study of modified FOLFIRINOX for chemotherapy-naïve patients with metastatic pancreatic cancer. Cancer Chemother. Pharmacol. 2018, 81, 1017–1023. [Google Scholar] [CrossRef]
- Ueno, H.; Ikeda, M.; Ueno, M.; Mizuno, N.; Ioka, T.; Omuro, Y.; Nakajima, T.E.; Furuse, J. Phase I/II study of nab-paclitaxel plus gemcitabine for chemotherapy-naive Japanese patients with metastatic pancreatic cancer. Cancer Chemother. Pharmacol. 2016, 77, 595–603. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of this study.
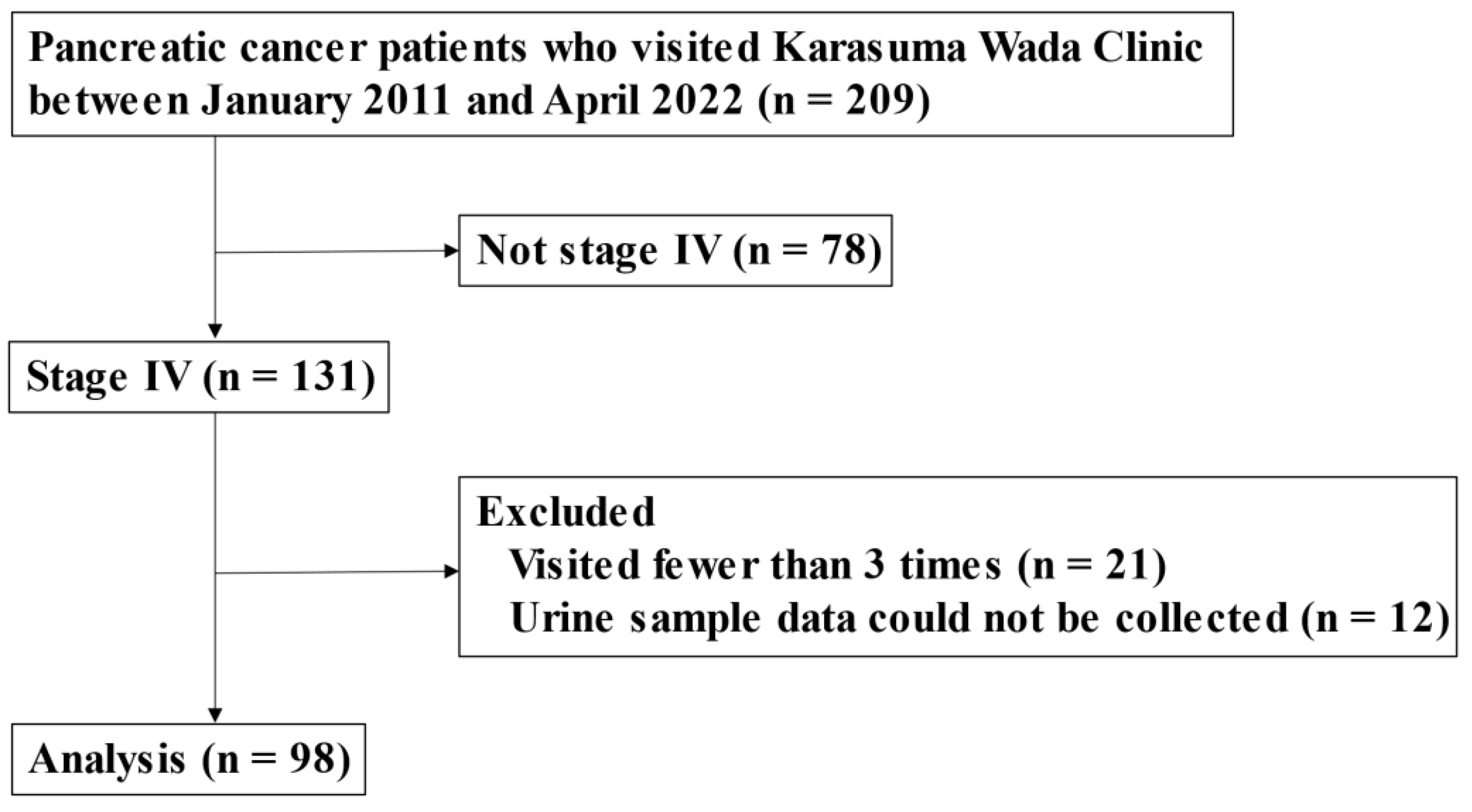
Figure 2.
Overall survival of the patients from the time of diagnosis.
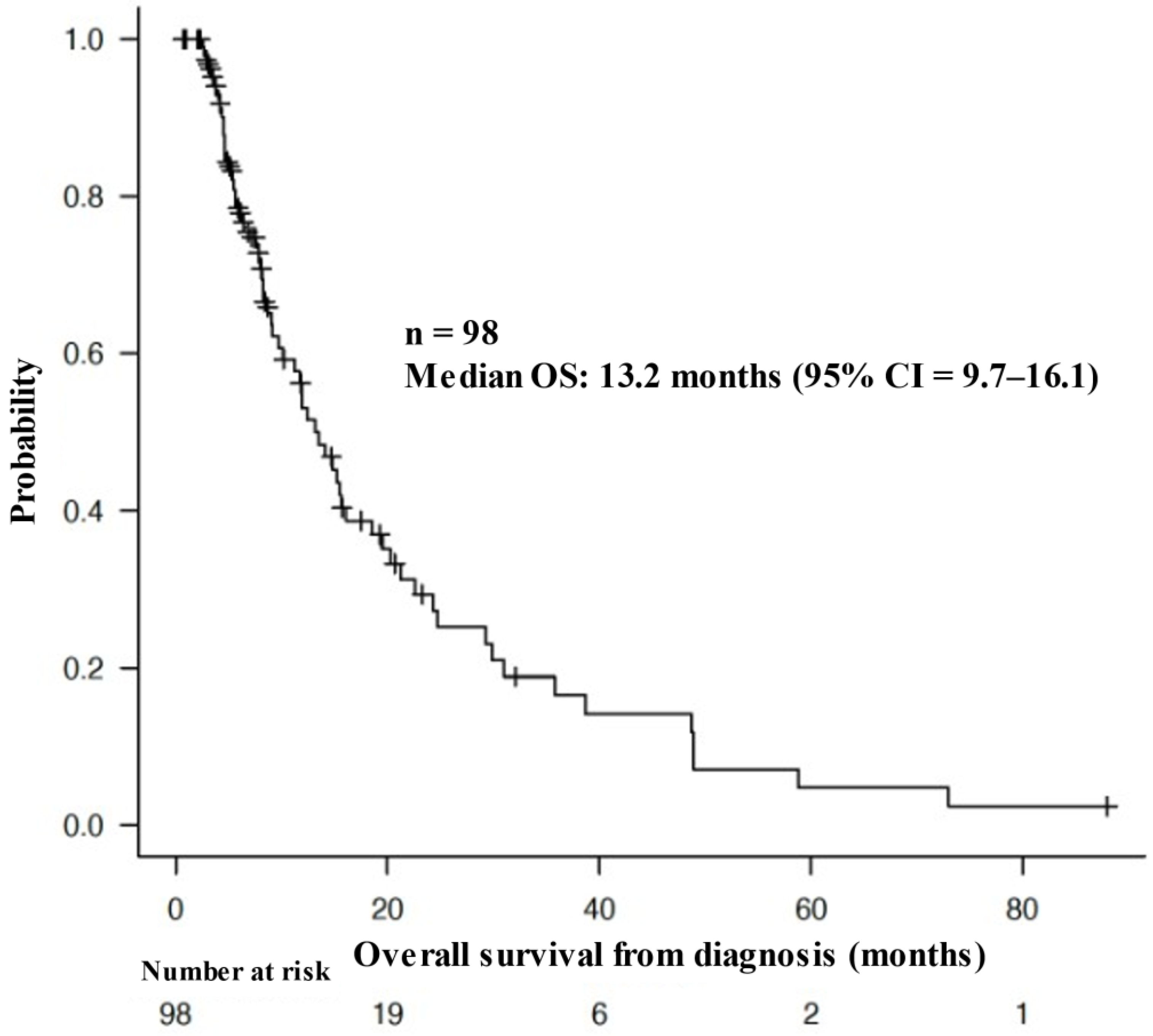
Figure 3.
Association between overall survival and urine pH.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



