Submitted:
21 October 2023
Posted:
23 October 2023
You are already at the latest version
Abstract
Alzheimer's disease (AD) is a progressive and evolving neurodegenerative disease with an insidious onset that can lead to memory loss and cognitive impairment. There is no effective treatment for this disease. However, early diagnosis plays an important role in treatment planning to slow down its progression, as treatment has the greatest impact in the early stages of the disease. Neurological images obtained through different imaging techniques provide powerful information and help diagnose the disease. With the wide application of deep learning techniques in disease diagnosis, especially the prominence of Convolutional Neural Networks (CNNs) in computer vision and image processing, more and more studies are proposing the use of this algorithm for the diagnosis of AD. In this paper, we first systematically introduce the impact of AD on people, detailing the biomarkers, early clinical symptoms, and risk factors of this disease. Secondly, it goes on to detail the development of CNNs, their form, and methods to help diagnose AD. It is proposed that CNNs can help diagnose AD by analyzing medical imaging data, particularly structural brain scans such as magnetic resonance imaging (MRI) and functional scans such as positron emission tomography (PET). Finally, it is concluded that CNNs are of great importance for the diagnosis of AD and that they are likely to play an increasingly important role in the early detection of the disease, the understanding of disease mechanisms, and ultimately, in the development of effective AD therapies and interventions. CNNs are playing an increasingly important role in the Their potential impact on healthcare emphasizes the importance of continued research and innovation in neural networks and medical imaging.
Keywords:
Alzheimer's Disease (AD)
; Convolutional Neural Networks (CNNs)
; Biomarkers of AD
; Early clinical symptoms
; Risk factors
; Diagnosis of AD
; Medical Images
Introduction of Alzheimer’s Disease
Alzheimer’s disease is a progressive and devastating neurological disorder that primarily affects the cognitive functions of the brain, leading to memory loss, impaired thinking, and behavioral changes [1]. It is the most common cause of dementia, a condition characterized by a decline in cognitive abilities severe enough to interfere with daily life [2]. Alzheimer’s disease not only affects the individuals diagnosed but also places a significant emotional and economic burden on their families and society as a whole [3].
Alzheimer’s disease is a global health challenge, with millions of individuals affected worldwide. As populations age, the prevalence of Alzheimer’s is expected to rise significantly [4]. The disease has a profound impact not only on the quality of life of those diagnosed but also on their caregivers and healthcare systems.
Alzheimer’s disease poses a significant and growing public health challenge [5], and it underscores the importance of continued research, awareness, and support for both individuals living with the disease and their caregivers [6]. Efforts to find effective treatments and interventions to address this devastating condition are ongoing, with the hope of ultimately improving the lives of those affected by Alzheimer’s disease. Paper structure is shown in Figure 1:
Biomarkers of AD
Biomarkers of Alzheimer’s disease (AD) are measurable biological indicators that can provide valuable information about the presence, progression, and underlying pathology of the disease [7]. These biomarkers are essential for early diagnosis, tracking disease progression, and monitoring the effectiveness of potential treatments [8]. There are several types of biomarkers associated with Alzheimer’s disease, as shown in Figure 2:
Biomarkers in Cerebrospinal Fluid (CSF): Analysis of cerebrospinal fluid, which surrounds the brain and spinal cord, can reveal specific biomarkers associated with Alzheimer’s disease [9]. Two key biomarkers in CSF are elevated levels of tau protein and decreased levels of beta-amyloid [10]. Increased tau levels are indicative of neurodegeneration [11], while reduced beta-amyloid levels suggest amyloid plaque buildup in the brain, which is a hallmark of AD. These CSF biomarkers are considered strong indicators of AD pathology and are often used in research and clinical trials [12].
Neuroimaging Biomarkers: Advanced neuroimaging techniques, such as positron emission tomography (PET) and magnetic resonance imaging (MRI), can provide biomarkers related to structural and functional changes in the brain [13]. PET scans using radiotracers like Pittsburgh compound B (PiB) can detect amyloid plaques, while fluorodeoxyglucose (FDG) PET scans can assess brain metabolism [14]. Structural MRI can reveal changes in brain volume and atrophy associated with AD. Functional MRI (fMRI) can assess brain connectivity and network disruptions. These neuroimaging biomarkers aid in the early diagnosis and tracking of AD-related changes in the brain [15].
Blood-Based Biomarkers: Researchers are actively exploring blood-based biomarkers for Alzheimer’s disease. Recent advancements in blood tests have shown promise in detecting AD-related changes [16], such as elevated levels of specific proteins (e.g., tau, neurofilament light chain) and abnormal ratios of amyloid peptides. Blood-based biomarkers hold the potential for less invasive and more accessible screening and monitoring of Alzheimer’s disease [17].
Genetic Biomarkers: Genetic biomarkers, particularly specific gene variants, can increase the risk of developing Alzheimer’s disease [18]. The most well-known genetic risk factor is the apolipoprotein E (APOE) gene, with certain APOE variants associated with a higher risk of AD [19]. Other genes, such as those related to amyloid precursor protein (APP) and presenilin (PSEN1 and PSEN2), are linked to rare forms of early-onset Alzheimer’s disease [20]. Genetic testing and the identification of these biomarkers can help assess an individual’s susceptibility to AD. Biomarker types and tests for AD are shown in Table 1:
These biomarkers are crucial in advancing our understanding of Alzheimer’s disease, from its earliest stages through progression. They provide valuable tools for diagnosing AD, monitoring disease severity, and evaluating the effectiveness of potential treatments. The ongoing research into biomarkers continues to refine our ability to detect, track, and ultimately develop interventions for Alzheimer’s disease [21], offering hope for improved outcomes for individuals affected by this devastating condition.
Early Clinical Symptoms of AD
Clinical symptoms of Alzheimer’s disease (AD) manifest gradually and progress over time, ultimately leading to significant cognitive impairment and functional limitations [22]. The clinical presentation of AD varies among individuals [23], but there are common symptoms and stages associated with the disease, as shown in Table 2:
Mild Cognitive Impairment (MCI) and Early Stages: In the early stages of AD, individuals often experience subtle changes in cognitive function that may be attributed to normal aging [24]. Common early symptoms include:
Memory Loss: Difficulty remembering recent events, appointments, or conversations is a hallmark symptom. Individuals may forget important dates and details [25].
Difficulty with Complex Tasks: Completing complex tasks that involve multiple steps, such as managing finances or following a recipe, becomes challenging [26].
Language Problems: Word-finding difficulties, trouble following or participating in conversations, and repeating questions may occur [27].
Spatial and Navigation Challenges: Getting lost in familiar places or difficulty with spatial orientation may be noticed [28].
Risk Factors of AD
Alzheimer’s disease (AD) is a complex condition influenced by a combination of genetic, environmental, and lifestyle factors. While the exact cause of AD is not fully understood, there are several known risk factors that increase the likelihood of developing the disease. Eight risk factors for AD are listed below, as shown in Figure 3:
Age is the most significant risk factor for Alzheimer’s disease. The risk of developing AD increases significantly with advancing age. Most individuals with AD are diagnosed after the age of 65, and the prevalence of the disease doubles every five years in this age group [29].
Genetic factors play a role in the development of AD. The most well-known genetic risk factor is the apolipoprotein E (APOE) gene. Variants of the APOE gene, particularly the APOE ε4 allele, are associated with an increased risk of developing AD [30]. Individuals with one copy of the ε4 allele have an elevated risk, while those with two copies have an even higher risk.
A family history of Alzheimer’s disease can also increase an individual’s risk. Having a first-degree relative (such as a parent or sibling) with AD may raise the likelihood of developing the disease, suggesting a potential genetic component.
Women are more likely to develop Alzheimer’s disease than men [31]. Some of this gender difference may be attributed to differences in longevity, as women tend to live longer. However, research suggests that biological and hormonal factors may also play a role.
Cardiovascular risk factors, such as high blood pressure, high cholesterol, diabetes, and obesity, have been linked to an increased risk of AD [32]. The relevant descriptions of these four risk factors are shown in Table 3. These conditions can affect blood flow to the brain and contribute to vascular changes that may play a role in the development of AD.
Lower levels of education and limited cognitive engagement throughout life have been associated with a higher risk of AD. Engaging in lifelong learning, mentally stimulating activities, and maintaining cognitive health may help reduce the risk.
A history of head injuries, particularly those involving loss of consciousness or repeated concussions, may increase the risk of AD [33]. This is a concern, especially in contact sports and military settings.
Some environmental factors, such as air pollution, exposure to heavy metals (like lead and aluminum), and certain pesticides [34], have been studied for their potential links to Alzheimer’s disease. While the evidence is not definitive, ongoing research explores the impact of environmental factors on AD risk. The main risk factors for Alzheimer’s disease and its manifestations are shown in Table 4:
It’s important to note that having one or more of these risk factors does not guarantee the development of Alzheimer’s disease. Many individuals with one or more risk factors do not develop AD, and conversely, some individuals without known risk factors may develop the disease. Alzheimer’s disease is a multifactorial condition, and ongoing research aims to better understand the complex interplay of these factors in its development.
Convolutional Neural Networks
The history of Convolutional Neural Networks (CNNs) is closely tied to the evolution of artificial neural networks, image processing [35], and computer vision research. CNNs are a specialized type of deep neural network designed to excel in tasks involving visual data, such as image recognition and computer vision. The evolution of CNNs is shown in Figure 4. Here’s a brief history of CNNs:
Early Neural Network Research: The concept of artificial neural networks dates back to the 1940s and 1950s, with the development of perceptrons by Frank Rosenblatt [36]. However, perceptrons and early neural networks had limitations, and research in the field slowed down.
The resurgence of interest in neural networks, including CNNs, can be attributed to the work of Yann LeCun and his team in the late 1990s. LeCun’s LeNet-5 architecture, introduced in 1998, was a pioneering CNN designed for handwritten digit recognition. LeNet-5 incorporated convolutional layers, pooling layers, and fully connected layers [37]. It played a significant role in reviving the application of neural networks in computer vision.
The pivotal moment for CNNs came in 2012 when the AlexNet architecture, developed by Alex Krizhevsky, Ilya Sutskever, and Geoffrey Hinton, won the ImageNet Large Scale Visual Recognition Challenge. AlexNet demonstrated the power of deep CNNs for image classification tasks, achieving a significant reduction in error rates compared to traditional methods [38]. This victory marked the beginning of the deep learning revolution in computer vision.
Following AlexNet, there has been a surge in research and innovation in CNN architectures and applications. Researchers introduced various modifications , including GoogLeNet, VGGNet, and ResNet, with increasingly deep architectures, enabling CNNs to achieve remarkable accuracy in image recognition tasks [39]. CNNs have also been applied to a wide range of computer vision tasks beyond image classification, including object detection, segmentation, and generative tasks like style transfer.
CNNs have become a cornerstone of modern artificial intelligence [40], with applications extending beyond computer vision to fields like natural language processing and reinforcement learning. Their success has spurred the development of hardware accelerators [41], such as graphics processing units (GPUs) and dedicated AI chips, to support the training and deployment of deep CNN models [42]. Today, CNNs are widely used in industry and research, contributing to advancements in autonomous vehicles, medical image analysis, and many other domains [43].
Forms of CNN
Convolutional Neural Networks (CNNs) are structured to effectively process and analyze visual data, making them a foundational architecture in computer vision and image-related tasks [44]. The infrastructure of a CNNs is shown in Figure 5. The structure of CNNs is characterized by several key components, which work together to extract meaningful features from images:
Convolutional layers are the core building blocks of CNNs [45]. They consist of learnable filters (also called kernels) that slide across the input image, performing a mathematical operation known as convolution. Convolutional layers detect local patterns and features [46], such as edges, textures, and shapes. Multiple filters in each layer capture different features, allowing the network to learn hierarchical representations of the input data.
Pooling layers are used to reduce the spatial dimensions of the feature maps produced by convolutional layers [47]. Common pooling operations include max pooling and average pooling, which downsample the feature maps by selecting the maximum or average value within a small region (e.g., a 2x2 or 3x3 window). As shown in Figure 6, its stride is 2, ensuring that the two pooling zones do not overlap (otherwise it is overlapping pooling). Pooling helps decrease computational complexity, reduces overfitting, and retains important information.
Max-pooling (MP) is a mechanism to optimise the spatial size of the feature map while providing translation invariance to the network. Max-pooling is to take the maximum value of the pixel points in the pooled area, and the feature maps obtained in this way are more sensitive to texture feature information. The equation for max-pooling is
Average-pooling (AP) is averaging the images in the pooled region, the feature information obtained in this way is more sensitive to the background information. The expression for average-pooling can be written as
Activation functions, such as the Rectified Linear Unit (ReLU) [48], are applied after convolutional and pooling layers. The function image is shown in Figure 7. ReLU introduces non-linearity to the network, enabling it to learn complex relationships and representations. ReLU sets negative values to zero and allows positive values to pass unchanged, promoting sparsity and efficiency in feature maps [49].
In the usual sense, the ReLU refers to the algebraic slope function
Whereas in a neural network, the ReLU as the activation function of a neuron and defines the nonlinear output result of that neuron after a linear transformation
In other words, for the input vector x from the previous layer of the neural network that enters the neuron, the neuron using the ReLU outputs
to the next layer of neurons or as the output of the entire neural network.
Fully connected (FC) layers are traditionally found at the end of CNN architectures. They connect all neurons from the previous layer to each neuron in the current layer [50]. FC layers are responsible for making final predictions or decisions based on the extracted features. In image classification tasks, FC layers are followed by a softmax activation function to produce class probabilities. The features and functionalities of the convolutional, pooling and fully connected layers are shown in Table 5:
The overall structure of a CNN typically follows a pattern of stacking multiple convolutional and pooling layers to progressively learn features at different levels of abstraction [51,52]. This hierarchy of features allows CNNs to recognize simple patterns in the early layers and gradually build up to more complex and abstract representations in the deeper layers. The final FC layers are responsible for making high-level predictions based on the learned features.
In addition to these core components, modern CNN architectures often incorporate techniques such as batch normalization, dropout, and skip connections to enhance training stability, prevent overfitting, and improve model performance [53]. Architectures like VGGNet, GoogLeNet, and ResNet have demonstrated the effectiveness of deep CNNs in various computer vision tasks and have inspired further advancements in the field.
CNN Helps Diagnose AD
Convolutional Neural Networks (CNNs) have shown promise in aiding the diagnosis of Alzheimer’s disease (AD) by analyzing medical imaging data, particularly structural brain scans like magnetic resonance imaging (MRI) and functional scans such as positron emission tomography (PET) [54]. Here’s how CNNs contribute to the diagnosis of AD:
CNNs excel at automatically extracting relevant features from medical images, even subtle patterns that may not be apparent to the human eye. In the context of AD diagnosis, CNNs can identify structural and functional abnormalities in the brain, including changes in brain volume, the presence of beta-amyloid plaques, and altered patterns of glucose metabolism [55]. These extracted features serve as important diagnostic markers.
After extracting relevant features, CNNs can be trained to classify medical images into different categories, such as AD, mild cognitive impairment (MCI), or normal controls. This classification task can be performed based on patterns and abnormalities identified in the images. For example, a CNN can distinguish between brain scans with characteristic AD-related changes and those without, helping radiologists and clinicians make more accurate diagnoses [56]. The diagnostic process is shown in Figure 8:
CNNs are particularly valuable for the early detection of AD. Subtle brain changes associated with the disease may occur years before clinical symptoms become apparent [57]. By analyzing images from asymptomatic individuals, CNNs can identify early signs of AD, potentially allowing for timely intervention and treatment to slow the progression of the disease.
CNN-based AD diagnosis offers the advantage of objectivity and reproducibility. Unlike manual interpretation, which may vary among radiologists and clinicians, CNNs consistently apply predefined criteria and algorithms to evaluate medical images [58]. This can lead to more consistent and reliable diagnoses, reducing the risk of misdiagnosis.
Conclusions
In conclusion, Convolutional Neural Networks (CNNs) have emerged as a powerful and promising tool in the field of Alzheimer’s disease (AD) diagnosis and research. Their ability to automatically extract, analyze, and classify complex patterns from medical imaging data [59], particularly structural and functional brain scans, has the potential to revolutionize the early detection and understanding of AD. Here are the key takeaways from the role of CNNs in AD:
CNN-based AD diagnosis offers objectivity and reproducibility, reducing the risk of misdiagnosis and ensuring consistent evaluation of medical images. These networks serve as valuable aids to healthcare professionals, enhancing the accuracy of diagnoses.
CNNs are instrumental in advancing our understanding of AD by providing quantitative data and insights into the disease’s progression. Researchers can use CNNs to analyze large datasets and identify potential biomarkers or imaging markers associated with AD.
While CNNs hold great promise, challenges such as interpretability, data privacy, and the need for large, well-curated datasets continue to be important considerations in their application to AD diagnosis.
In the quest to combat Alzheimer’s disease, CNNs represent a significant technological advancement that complements the expertise of radiologists, neurologists, and researchers. As research and technology continue to evolve, CNNs are likely to play an increasingly vital role in early detection, understanding the disease’s mechanisms, and ultimately contributing to the development of effective treatments and interventions for AD. Their potential impact on the healthcare landscape underscores the importance of continued research and innovation in the field of neural networks and medical imaging.
Funding
This research did not receive any grants.
Acknowledgment
We thank all the anonymous reviewers for their hard reviewing work.
References
- Lu, Y.; Li, J.; Hu, T. Analysis of correlation between serum inflammatory factors and cognitive function, language, and memory in alzheimer’s disease and its clinical significance. Computational and Mathematical Methods in Medicine 2022, 2022. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.-R.; Huang, J.-B.; Yang, S.-L.; Hong, F.-F. Role of cholinergic signaling in Alzheimer’s disease. Molecules 2022, 27, 1816. [Google Scholar] [CrossRef]
- Zhang, Y. Prediction of MCI to Alzheimer’s conversion based on tensor-based morphometry and kernel support vector machine. Alzheimer’s & Dementia 2015, 11, 702. [Google Scholar]
- Li, X.; Feng, X.; Sun, X.; Hou, N.; Han, F.; Liu, Y. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2019. Frontiers in Aging Neuroscience 2022, 14, 937486. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, M. Temporal patterns of the burden of Alzheimer’s disease and their association with Sociodemographic Index in countries with varying rates of aging 1990–2019. Aging Medicine 2023, 6, 281–289. [Google Scholar] [CrossRef]
- Zhang, Y. Three-Dimensional Eigenbrain for the Detection of Subjects and Brain Regions Related with Alzheimer’s Disease. Journal of Alzheimer’s Disease 2016, 50, 1163–1179. [Google Scholar] [CrossRef]
- Hampel, H.; Broich, K.; Hoessler, Y.; Pantel, J. Biological markers for early detection and pharmacological treatment of Alzheimer’s disease. Dialogues in clinical neuroscience 2022. [CrossRef] [PubMed]
- Klyucherev, T.O.; Olszewski, P.; Shalimova, A.A.; Chubarev, V.N.; Tarasov, V.V.; Attwood, M.M.; et al. Advances in the development of new biomarkers for Alzheimer’s disease. Translational Neurodegeneration 2022, 11, 1–24. [Google Scholar] [CrossRef]
- Wang, B.; Zhong, X.; Fields, L.; Lu, H.; Zhu, Z.; Li, L. Structural proteomic profiling of cerebrospinal fluids to reveal novel conformational biomarkers for Alzheimer’s disease. Journal of the American Society for Mass Spectrometry 2023, 34, 459–471. [Google Scholar] [CrossRef]
- Virgilio, E.; Vecchio, D.; Crespi, I.; Puricelli, C.; Barbero, P.; Galli, G.; et al. Cerebrospinal fluid biomarkers and cognitive functions at multiple sclerosis diagnosis. Journal of Neurology 2022, 269, 3249–3257. [Google Scholar] [CrossRef]
- Wang, S.-H. Alzheimer’s Disease Detection by Pseudo Zernike Moment and Linear Regression Classification. CNS & Neurological Disorders - Drug Targets 2017, 16, 11–15. [Google Scholar]
- Zhou, J.; Benoit, M.; Sharoar, M.G. Recent advances in pre-clinical diagnosis of Alzheimer’s disease. Metabolic Brain Disease 2022, 37, 1703–1725. [Google Scholar] [CrossRef] [PubMed]
- McKay, N.S.; Gordon, B.A.; Hornbeck, R.C.; Dincer, A.; Flores, S.; Keefe, S.J.; et al. Positron emission tomography and magnetic resonance imaging methods and datasets within the Dominantly Inherited Alzheimer Network (DIAN). Nature Neuroscience 2023, 26, 1449–1460. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jin, C.; Zhou, J.; Zhou, R.; Tian, M.; Lee, H.J.; et al. PET molecular imaging for pathophysiological visualization in Alzheimer’s disease. European Journal of Nuclear Medicine and Molecular Imaging 2023, 50, 765–783. [Google Scholar] [CrossRef] [PubMed]
- Brickman, A.M.; Manly, J.J.; Honig, L.S.; Sanchez, D.; Reyes-Dumeyer, D.; Lantigua, R.A.; et al. Correlation of plasma and neuroimaging biomarkers in Alzheimer’s disease. Annals of clinical and translational neurology 2022, 9, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, C.E.; Verberk, I.M.; Thijssen, E.H.; Vermunt, L.; Hansson, O.; Zetterberg, H.; et al. Blood-based biomarkers for Alzheimer’s disease: towards clinical implementation. The Lancet Neurology 2022, 21, 66–77. [Google Scholar] [CrossRef]
- Varesi, A.; Carrara, A.; Pires, V.G.; Floris, V.; Pierella, E.; Savioli, G.; et al. Blood-based biomarkers for alzheimer’s disease diagnosis and progression: An overview. Cells 2022, 11, 1367. [Google Scholar] [CrossRef]
- Li, R.-X.; Ma, Y.-H.; Tan, L.; Yu, J.-T. Prospective biomarkers of Alzheimer’s disease: A systematic review and meta-analysis. Ageing Research Reviews 2022, 101699. [Google Scholar] [CrossRef]
- Fernández-Calle, R.; Konings, S.C.; Frontiñán-Rubio, J.; García-Revilla, J.; Camprubí-Ferrer, L.; Svensson, M.; et al. APOE in the bullseye of neurodegenerative diseases: Impact of the APOE genotype in Alzheimer’s disease pathology and brain diseases. Molecular Neurodegeneration 2022, 17, 62. [Google Scholar] [CrossRef]
- Maurya, R.; Bhattacharjee, G.; Khambhati, K.; Gohil, N.; Singh, P.; Mani, I.; et al. Amyloid precursor protein in Alzheimer’s disease. Progress in Molecular Biology and Translational Science 2023, 196, 261–270. [Google Scholar]
- Hansson, O.; Edelmayer, R.M.; Boxer, A.L.; Carrillo, M.C.; Mielke, M.M.; Rabinovici, G.D.; et al. The Alzheimer’s Association appropriate use recommendations for blood biomarkers in Alzheimer’s disease. Alzheimer’s & Dementia 2022, 18, 2669–2686. [Google Scholar]
- Zhu, Z.; Ma, X.; Wu, J.; Xiao, Z.; Wu, W.; Ding, S.; et al. Altered gut microbiota and its clinical relevance in mild cognitive impairment and Alzheimer’s disease: Shanghai Aging Study and Shanghai Memory Study. Nutrients 2022, 14, 3959. [Google Scholar] [CrossRef]
- Wang, S. Detection of Alzheimer’s Disease by Three-Dimensional Displacement Field Estimation in Structural Magnetic Resonance Imaging. Journal of Alzheimer’s Disease 2016, 50, 233–248. [Google Scholar] [CrossRef] [PubMed]
- Mirakhori, F.; Moafi, M.; Milanifard, M.; Tahernia, H. Diagnosis and Treatment Methods in Alzheimer’s Patients Based on Modern Techniques: The Orginal Article. Journal of Pharmaceutical Negative Results, 1907. [Google Scholar]
- Jahn, H. Memory loss in Alzheimer’s disease. Dialogues in clinical neuroscience 2022. [Google Scholar] [CrossRef] [PubMed]
- Corriveau-Lecavalier, N.; Machulda, M.M.; Botha, H.; Graff-Radford, J.; Knopman, D.S.; Lowe, V.J.; et al. Phenotypic subtypes of progressive dysexecutive syndrome due to Alzheimer’s disease: A series of clinical cases. Journal of Neurology 2022, 269, 4110–4128. [Google Scholar] [CrossRef] [PubMed]
- Polsinelli, A.J.; Apostolova, L.G. Atypical Alzheimer disease variants. CONTINUUM: Lifelong Learning in Neurology 2022, 28, 676–701. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Martínez, M.C. Spatial memory deficits in Alzheimer’s disease and their connection to cognitive maps’ formation by place cells and grid cells. Frontiers in Behavioral Neuroscience 2023, 16, 1082158. [Google Scholar] [CrossRef]
- Gillis, C.; Montenigro, P.; Nejati, M.; Maserejian, N. Estimating prevalence of early Alzheimer’s disease in the United States, accounting for racial and ethnic diversity. Alzheimer’s & Dementia 2023, 19, 1841–1848. [Google Scholar]
- Jabeen, K.; Rehman, K.; Akash, M.S.H. Genetic mutations of APOEε4 carriers in cardiovascular patients lead to the development of insulin resistance and risk of Alzheimer’s disease. Journal of biochemical and molecular toxicology 2022, 36, e22953. [Google Scholar] [CrossRef]
- Mielke, M.M.; Aggarwal, N.T.; Vila-Castelar, C.; Agarwal, P.; Arenaza-Urquijo, E.M.; Brett, B.; et al. Consideration of sex and gender in Alzheimer’s disease and related disorders from a global perspective. Alzheimer’s & dementia 2022, 18, 2707–2724. [Google Scholar]
- Pasqualetti, G.; Thayanandan, T.; Edison, P. Influence of genetic and cardiometabolic risk factors in Alzheimer’s disease. Ageing Research Reviews 2022, 101723. [Google Scholar] [CrossRef]
- Mielke, M.M.; Ransom, J.E.; Mandrekar, J.; Turcano, P.; Savica, R.; Brown, A.W. Traumatic brain injury and risk of Alzheimer’s disease and related dementias in the population. Journal of Alzheimer’s disease 2022, 88, 1049–1059. [Google Scholar] [CrossRef]
- Rezende-Teixeira, P.; Dusi, R.G.; Jimenez, P.C.; Espindola, L.S.; Costa-Lotufo, L.V. What can we learn from commercial insecticides? Efficacy, toxicity, environmental impacts, and future developments. Environmental Pollution 2022, 300, 118983. [Google Scholar] [CrossRef]
- Zhang, Y. Image processing methods to elucidate spatial characteristics of retinal microglia after optic nerve transection. Scientific Reports 2016, 6, 21816. [Google Scholar] [CrossRef]
- Taki, O.; Rhazi, K.S.; Mejdoub, Y. Stirling engine optimization using artificial neural networks algorithm. in ITM Web of Conferences 2023, 02010. [Google Scholar] [CrossRef]
- Turhan, G.; Küçük, H.; Isik, E.O. Spatio-temporal convolution for classification of alzheimer disease and mild cognitive impairment. Computer Methods and Programs in Biomedicine 2022, 221, 106825. [Google Scholar] [CrossRef]
- Zhou, W.; Wang, H.; Wan, Z. Ore image classification based on improved CNN. Computers and Electrical Engineering 2022, 99, 107819. [Google Scholar] [CrossRef]
- Nugraha, G.S.; Darmawan, M.I.; Dwiyansaputra, R. Comparison of CNN’s Architecture GoogleNet, AlexNet, VGG-16, Lenet-5, Resnet-50 in Arabic Handwriting Pattern Recognition. Kinetik: Game Technology, Information System, Computer Network, Computing, Electronics, and Control 2023. [Google Scholar] [CrossRef]
- Zhang, Y.D.; Satapathy, S. A seven-layer convolutional neural network for chest CT-based COVID-19 diagnosis using stochastic pooling. IEEE Sensors Journal 2022, 22, 17573–17582. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-D. Improving ductal carcinoma in situ classification by convolutional neural network with exponential linear unit and rank-based weighted pooling. Complex & Intelligent Systems 2021, 7, 1295–1310. [Google Scholar]
- Chen, H. Hardware Implementation for Convolutional Neural Networks in Artificial Intelligence. Highlights in Science, Engineering and Technology 2023, 62, 73–77. [Google Scholar] [CrossRef]
- Nazir, S.; Dickson, D.M.; Akram, M.U. Survey of explainable artificial intelligence techniques for biomedical imaging with deep neural networks. Computers in Biology and Medicine 2023, 106668. [Google Scholar] [CrossRef]
- Torres, M.; Cantú, F. Learning to see: Convolutional neural networks for the analysis of social science data. Political Analysis 2022, 30, 113–131. [Google Scholar] [CrossRef]
- Cao, J.; Li, Y.; Sun, M.; Chen, Y.; Lischinski, D.; Cohen-Or, D.; et al. Do-conv: Depthwise over-parameterized convolutional layer. IEEE Transactions on Image Processing 2022, 31, 3726–3736. [Google Scholar] [CrossRef]
- Wang, S. Cerebral micro-bleeding identification based on a nine-layer convolutional neural network with stochastic pooling. Concurrency and Computation: Practice and Experience 2020, 31, e5130. [Google Scholar] [CrossRef]
- Zafar, A.; Aamir, M.; Nawi, N.M.; Arshad, A.; Riaz, S.; Alruban, A.; et al. A comparison of pooling methods for convolutional neural networks. Applied Sciences 2022, 12, 8643. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhu, H.; Meng, Z.; Koniusz, P.; King, I. Graph-adaptive rectified linear unit for graph neural networks. in Proceedings of the ACM Web Conference 2022, 2022, 1331–1339. [Google Scholar]
- Sharma, A.; Singh, S.; Ratna, S. Graph Neural Network Operators: a Review. Multimedia Tools and Applications 2023, 1–24. [Google Scholar] [CrossRef]
- Zheng, T.; Wang, Q.; Shen, Y.; Lin, X. Gradient rectified parameter unit of the fully connected layer in convolutional neural networks. Knowledge-Based Systems 2022, 248, 108797. [Google Scholar] [CrossRef]
- Fan, X.; Feng, X.; Dong, Y.; Hou, H. COVID-19 CT image recognition algorithm based on transformer and CNN. Displays 2022, 72, 102150. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Shi, Y.; Lin, R.; Qiao, W.; Ba, W. A novel oil pipeline leakage detection method based on the sparrow search algorithm and CNN. Measurement 2022, 204, 112122. [Google Scholar] [CrossRef]
- Tufail, A.B.; Ullah, I.; Rehman, A.U.; Khan, R.A.; Khan, M.A.; Ma, Y.-K.; et al. On disharmony in batch normalization and dropout methods for early categorization of Alzheimer’s disease. Sustainability 2022, 14, 14695. [Google Scholar] [CrossRef]
- Bonakdarpour, B.; Takarabe, C. Brain Networks, Clinical Manifestations, and Neuroimaging of Cognitive Disorders: The Role of Computed Tomography (CT), Magnetic Resonance Imaging (MRI), Positron Emission Tomography (PET), and Other Advanced Neuroimaging Tests. Clinics in Geriatric Medicine 2023, 39, 45–65. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Guo, Q.; Zhang, Y.; Zheng, J.; Yang, Y.; Du, X.; et al. Application of Deep Learning for Prediction of Alzheimer’s Disease in PET/MR Imaging. Bioengineering 2023, 10, 1120. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-T.T.; Rosa-Neto, P.; Gauthier, S. Advanced brain imaging for the diagnosis of Alzheimer disease. Current Opinion in Neurology 2023, 36, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Fathi, S.; Ahmadi, M.; Dehnad, A. Early diagnosis of Alzheimer’s disease based on deep learning: A systematic review. Computers in biology and medicine 2022, 146, 105634. [Google Scholar] [CrossRef]
- Aytaç, U.C.; Güneş, A.; Ajlouni, N. A novel adaptive momentum method for medical image classification using convolutional neural network. BMC Medical Imaging 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Wang, S. Pathological Brain Detection by a Novel Image Feature—Fractional Fourier Entropy. Entropy 2015, 17, 8278–8296. [Google Scholar] [CrossRef]
Figure 1.
Paper structure.
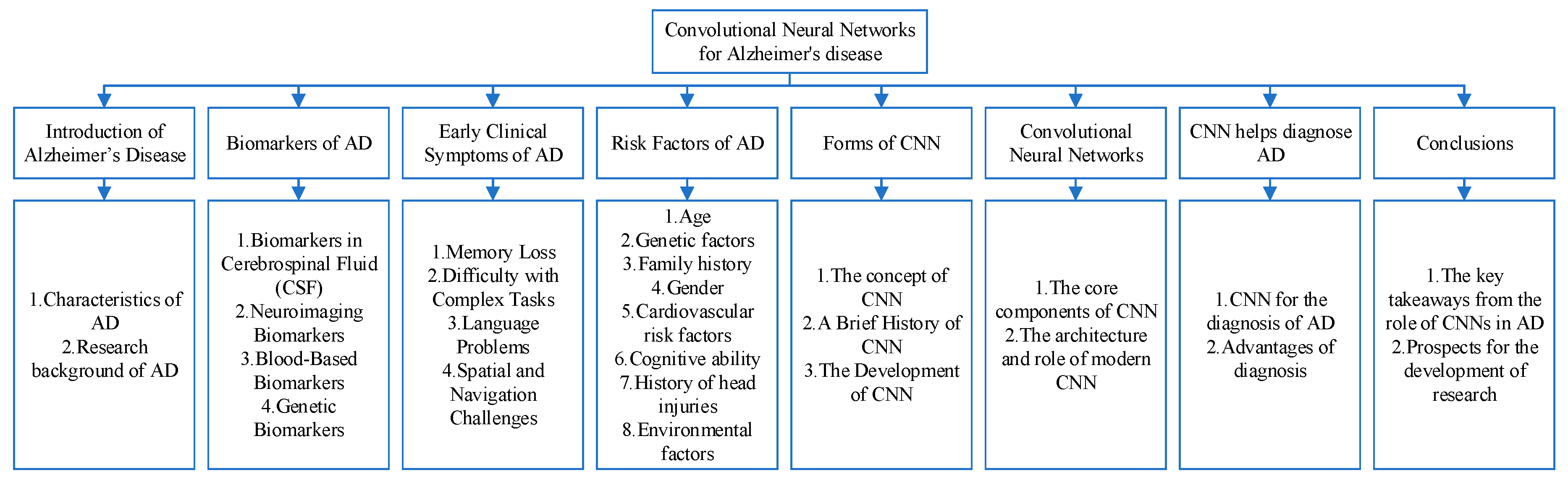
Figure 2.
Biomarkers of Alzheimer’s disease (AD).

Figure 3.
Risk factors of Alzheimer’s disease (AD).

Figure 4.
The evolution of CNNs.
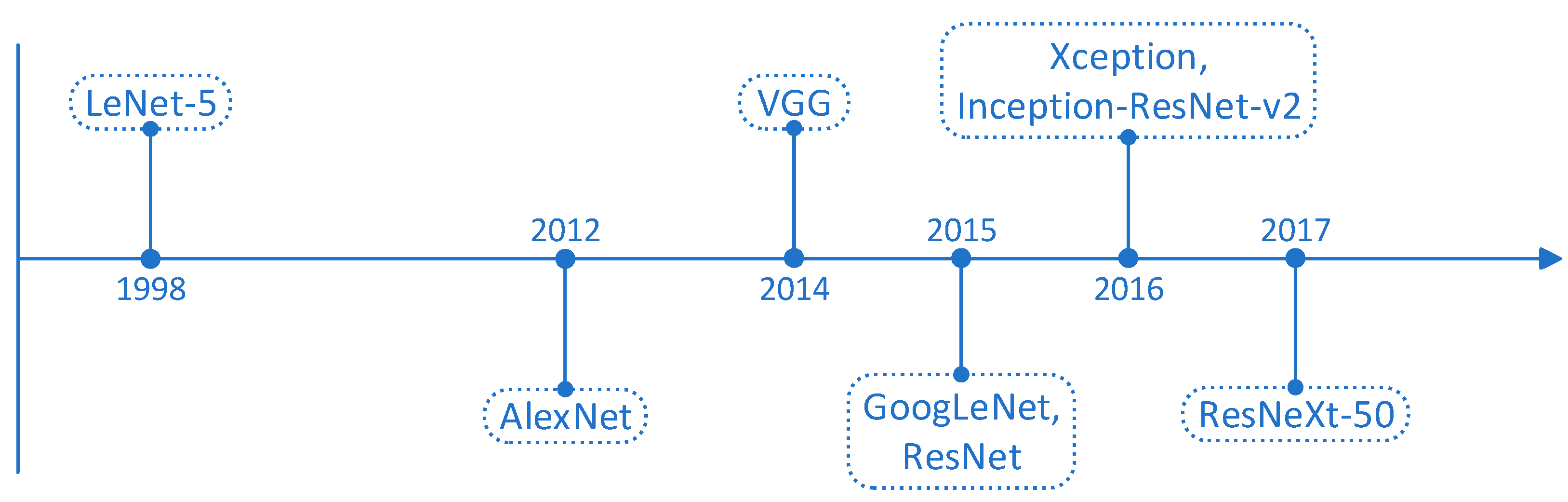
Figure 5.
The infrastructure of a CNNs.

Figure 6.
Max-pooling and Average-pooling.
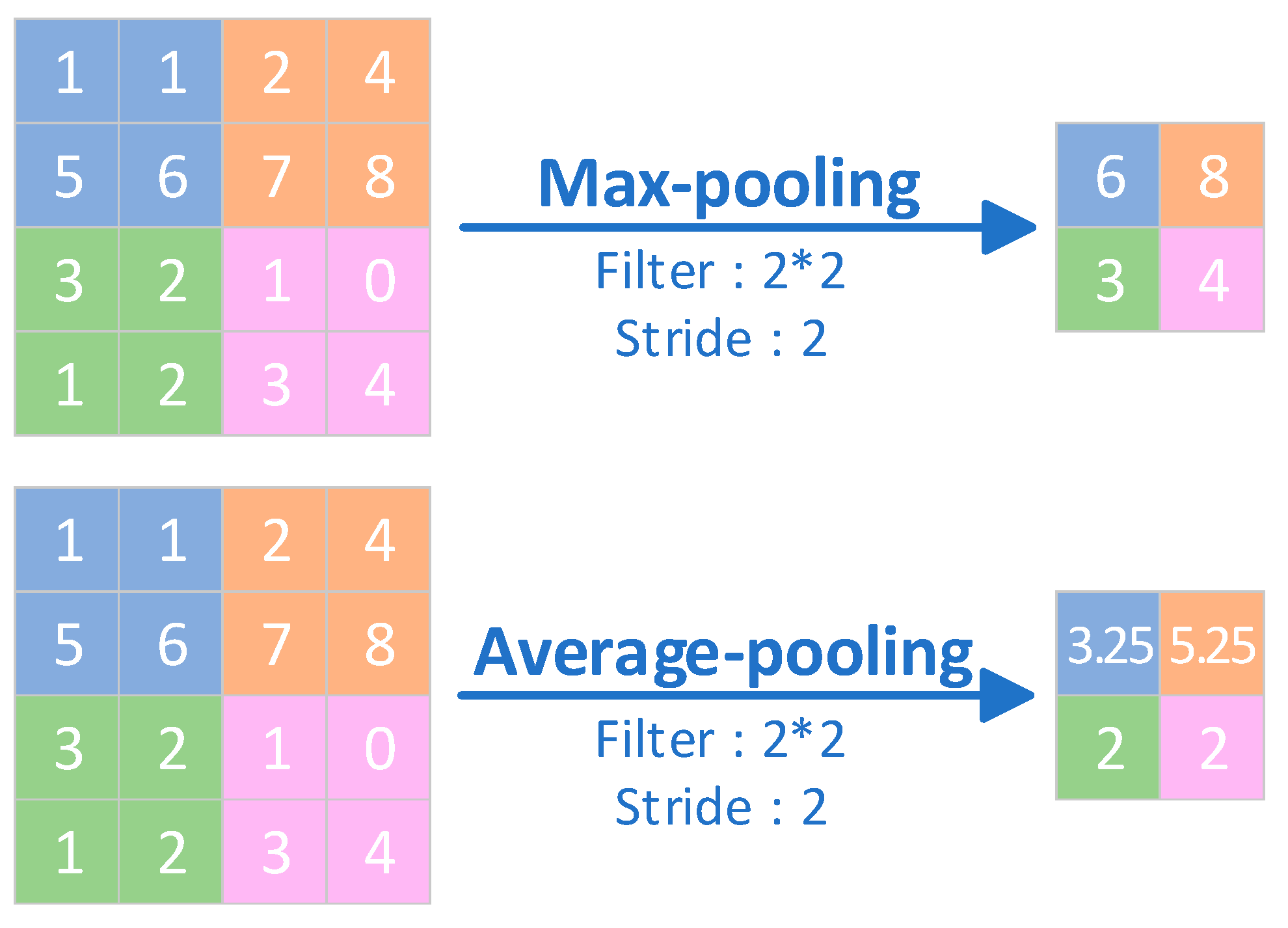
Figure 7.
ReLU image.
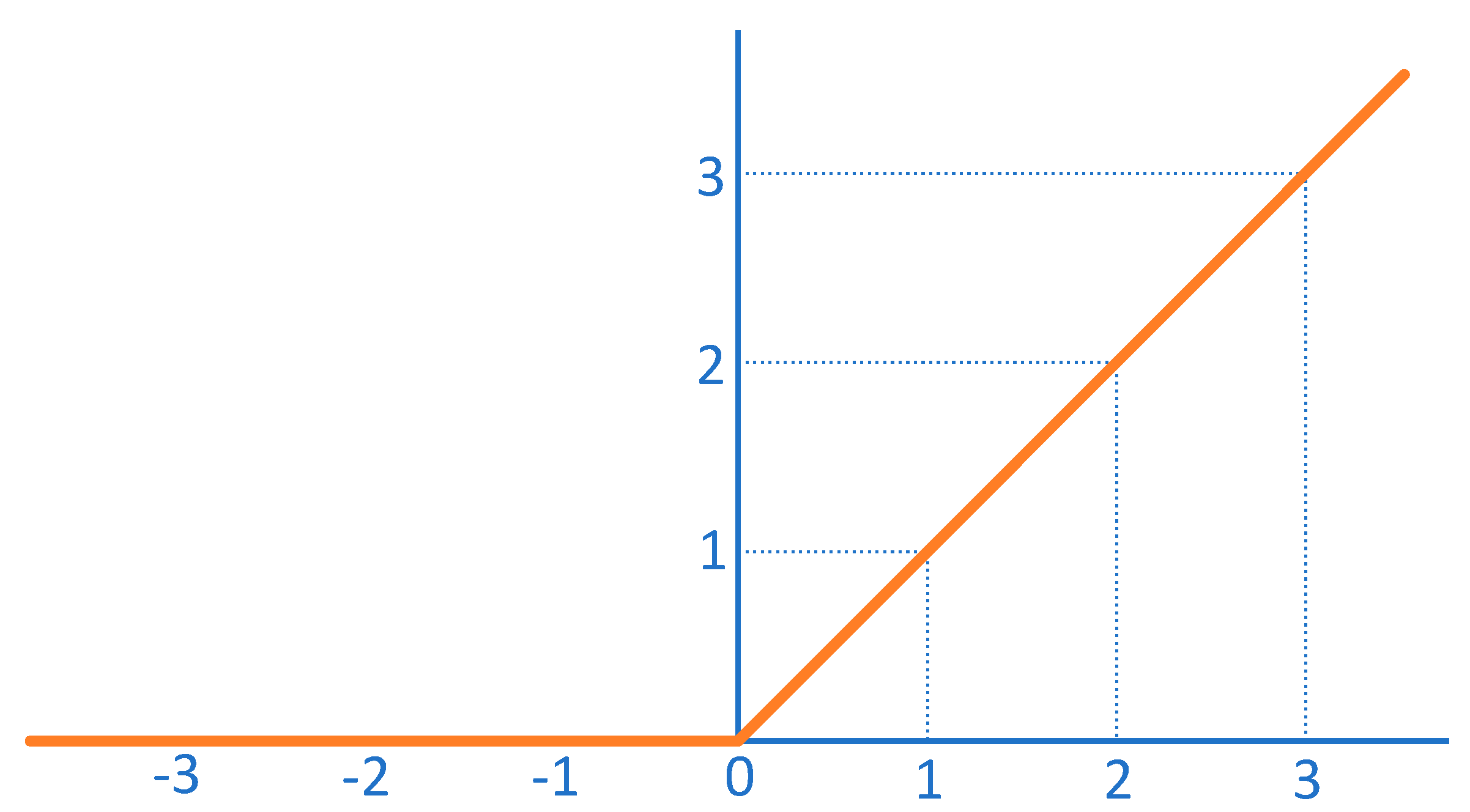
Figure 8.
Diagnostic process for AD.
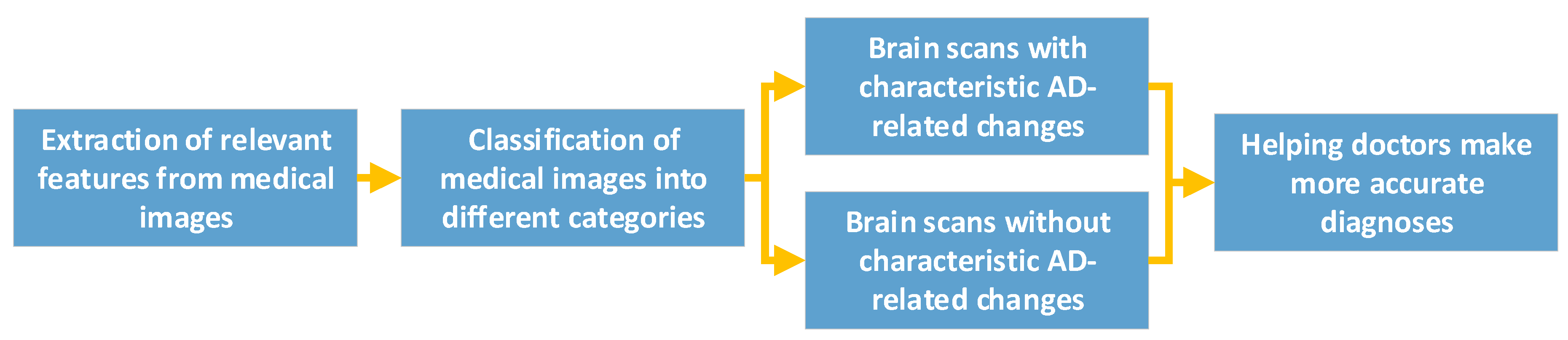

Table 1.
Biomarker types and tests for AD.
| Type of biomarkers for AD | Biomarker testing |
|---|---|
| Biomarkers in Cerebrospinal Fluid (CSF) | Two key biomarkers in CSF are elevated levels of tau protein and decreased levels of beta-amyloid. Increased tau levels are indicative of neurodegeneration, while reduced beta-amyloid levels suggest amyloid plaque buildup in the brain, which is a hallmark of AD. |
| Neuroimaging Biomarkers | PET scans using radiotracers like PiB can detect amyloid plaques, while FDG PET scans can assess brain metabolism. Structural MRI can reveal changes in brain volume and atrophy associated with AD. Functional MRI can assess brain connectivity and network disruptions. |
| Blood-Based Biomarkers | Plasma Aβ42 reflects changes in brain amyloid, and the Aβ42/Aβ40 ratio is thought to predict Aβ protein pathology deposition in people at risk for AD, and can be used as a prescreening method for AD in people with subjective cognitive decline and mild cognitive impairment. Elevated plasma Tau concentrations in patients with AD can help in the diagnosis of AD. |
| Genetic Biomarkers | The genetic risk of Alzheimer’s disease can be assessed by testing the APOE and MTHFR genes. Mutations in pathogenic AD genes (APP, PSEN1 or PSEN2) can increase the certainty of clinical diagnosis of AD dementia. |
Table 2.
Stage and common symptoms of Alzheimer’s disease (AD).
| Stage of AD | Common symptom |
|---|---|
| Asymptomatic stage | Amyloidosis occurs only in brain cells, without significant cognitive decline or mental behavioural abnormalities, and the process often lasts from ten to twenty years. |
| Mild cognitive impairment | Subjective cognition continues to decline from the previous level, and objective testing confirms the presence of cognitive impairment or psycho-behavioural changes. However, the patient can carry out activities of daily living independently. The patient’s main manifestation is memory loss, and there may also be emotional apathy. |
| Mild dementia | The patient is unable to perform labour and work independently, and the main symptoms are severe memory loss and loss of time orientation. |
| Moderate dementia | Extensive impact on daily life, basic functions partially impaired, patients unable to live independently, often needing assistance, disorientation of the location. |
| Severe dementia | It has a serious impact on daily life, and the patient is completely dependent on others for basic activities, including self-care. The main symptoms are aphasia, dysfunction, incontinence, and so on. |
Table 3.
Introduction to the four risk factors of hypertension, high cholesterol, diabetes and obesity.
Table 3.
Introduction to the four risk factors of hypertension, high cholesterol, diabetes and obesity.
| Risk factor | Introduction |
|---|---|
| Hypertension | Hypertension is one of the most common chronic diseases in modern times and is an important risk factor for cardiovascular disease, and current research suggests that high blood pressure (either elevated systolic or diastolic) in midlife (between the ages of 40 and 60) increases the risk of developing Alzheimer’s disease. |
| High cholesterol | Cholesterol cannot penetrate the blood-brain barrier, but hypercholesterolaemia is associated with an increased risk of Alzheimer’s disease and vascular cognitive impairment. |
| Diabetes | The age of onset of diabetes is significantly associated with the risk of developing dementia later in life, with the earlier the age of onset the higher the risk of dementia. |
| Obesity | When a person gains weight, activity and blood flow to all areas of the brain decrease. Being overweight or obese severely affects brain activity and can increase the risk of Alzheimer’s disease as well as many other mental and cognitive disorders. |
Table 4.
Risk factors for Alzheimer’s disease and its manifestations.
| Risk factor | Manifestation |
|---|---|
| Age | Age is the biggest risk factor for Alzheimer’s disease. Studies have shown that the incidence of Alzheimer’s disease increases by a factor of one for every 5 to 10 years of age over the age of 65, on average. And if you carry Alzheimer’s disease risk genes such as APOEε4, the likelihood of developing the disease is even greater with age. |
| Family history | Familial Alzheimer’s disease is autosomal dominant, which means that if a parent has familial Alzheimer’s disease, the causative agent must be passed on to the offspring, and the incidence of the disease in the offspring carrying the causative gene is almost 100 per cent, whereas in those not carrying the causative gene, the offspring will not have the disease. |
| Gene | Studies have shown that APOE genes play an important role in the development of late-onset Alzheimer’s disease and sporadic Alzheimer’s disease, with the APOε4 allele being the best-known for people over the age of 65. |
| Traumatic brain injury | Traumatic Brain Injury (TBI) often leads to changes in brain structure and function, as well as cognitive problems such as memory deficits, impaired social functioning, and decision-making difficulties. Mild TBI (also known as concussion) is a known risk factor for Alzheimer’s disease. |
Table 5.
The features and functionalities of the convolutional, pooling and fully connected layers.
| The key component of CNNs | Features | Functionalities |
|---|---|---|
| Convolutional layers | A convolutional layer is a layer in which the output is obtained by performing a convolutional operation on the input by means of a convolutional kernel (also known as a filter). | Convolutional layers can efficiently extract local features from the input and are therefore widely used in fields such as image recognition and computer vision. |
| Pooling layers | The pooling layer is the layer where the output is obtained by performing a downsampling operation on the input. | The pooling layer reduces the size of the inputs and reduces computational complexity, while providing a degree of translation invariance that helps to improve the generalisation of the model. |
| Fully-connected layers | The fully connected layer is the layer that connects all neurons of the input to all neurons of the output. | Fully-connected layers can make full use of all the information in the input, but they are also prone to overfitting, and therefore require attention to techniques such as regularisation during training. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



