
Submitted:
24 October 2023
Posted:
24 October 2023
You are already at the latest version
Abstract
Granular cell tumors (GCTs), known also as Abrikossoff tumors, are rare tumors that originates from Schwann cells that primarily localize in the tongue, skin, and submucosal tissues and involve the gastrointestinal tract in 11% of cases. We present a case of a young woman who first presented to our centre in 2018, for an EGDS to assess a thickening of the esophageal wall, seen on a CT. In that occasion, a diagnosis of Abrikossoff tumor was made. She underwent endoscopic resection with subsequent yearly follow-up without evidence of recurrence. 5 Years later, on a routine colonoscopy, we found numerous white submucosal formations in all of the explored tracts, with a histological examination compatible with GCT. Her daughter presented with a white nodule on her tongue, also diagnosed as GCT. Her daughter was also diagnosed with GCT of the tongue a few months later.
Keywords:
granular cell tumor
; Abrikossoff tumor
; multifocal tumor
; gastrointestinal tract
; inherited tumor
1. Introduction
Granular cell tumor (GCT), also known as Abrikossoff tumor, is a rare tumor that originates from Schwann cells (1). It was first described in 1854 by Weber and Virchow (2)but in 1926 Russian pathologist Alexei Ivanovich Abrikosoff described it in a patient presenting with a tongue lesion (3), and was believed to stem from muscular cells and was, therefore, named “granular cell myoblastoma”.
It localizes, primarily, in the tongue, skin, and submucosal tissues; roughly 11% involve the gastrointestinal tract, especially the esophagus.
Gastrointestinal GCTs appear at endoscopy as isolated submucosal nodules covered by white-yellow mucosa. In immunohistochemistry, these lesions are, typically, positive for the S-100 protein (4,5). Most are benign, but cases of malignant GCTs have been reported (6). Fanburg-Smith istopathological criteria can help to predict this evolution. Preferred treatment for gastrointestinal GCTs is endoscopic removal (7,8), while surgical removal or instrumental follow-up may be considered in some cases.
2. Case Presentation
A 42-year-old patient was referred by her general practitioner, for a colonoscopy as diagnostic workup for chronic long-lasting constipation, presenting without alarm symptoms and responsive to laxatives. Her past medical history included a prolactin-secreting pituitary microadenoma for which she is being treated with Cabergoline and Drospirenone, migraine with aura treated with Triptans, and autoimmune chronic euthyroid-thyroiditis. She also had a pregnancy with spontaneous birth in 2011. The patient had never undergone surgery and she did not declare food or drug allergies. Her familial medical history was unremarkable for gastrointestinal tumors. Moreover in 2018, the patient underwent upper gastrointestinal endoscopy (EGDS) following the detection of esophageal wall thickening on a chest CT for a suspected pulmonary disease due to the presence of chronic cough. She denied having any upper GI symptoms. During the endoscopic examination, a white nodular formation, measuring approximately 10 mm, was found in the middle esophagus (Figure 1), along with subcentimetric submucosal lesions in the stomach and duodenal bulb; biopsies were taken. Histological examination of the esophageal lesion resulted in the following diagnosis: “submucosal lesion, composed of uniform epithelioid cells with abundant granular eosinophilic cytoplasm and small nuclei, S100+, with Ki67 index < 1-2%, devoid of mitoses (evaluated with PHH3), covered by hyperplastic esophageal epithelium, compatible with granular cell tumor (Abrikossoff tumor)”. Similar features were found in the biopsies of the gastric lesions. The patient was then referred to a tertiary center for endoscopic removal of the esophageal lesion, confirmed as a granular cell tumor, and underwent annual follow-up with endoscopic ultrasound (EUS) without evidence of recurrence. The gastric lesions remained stable in number and size during the subsequent follow-up.
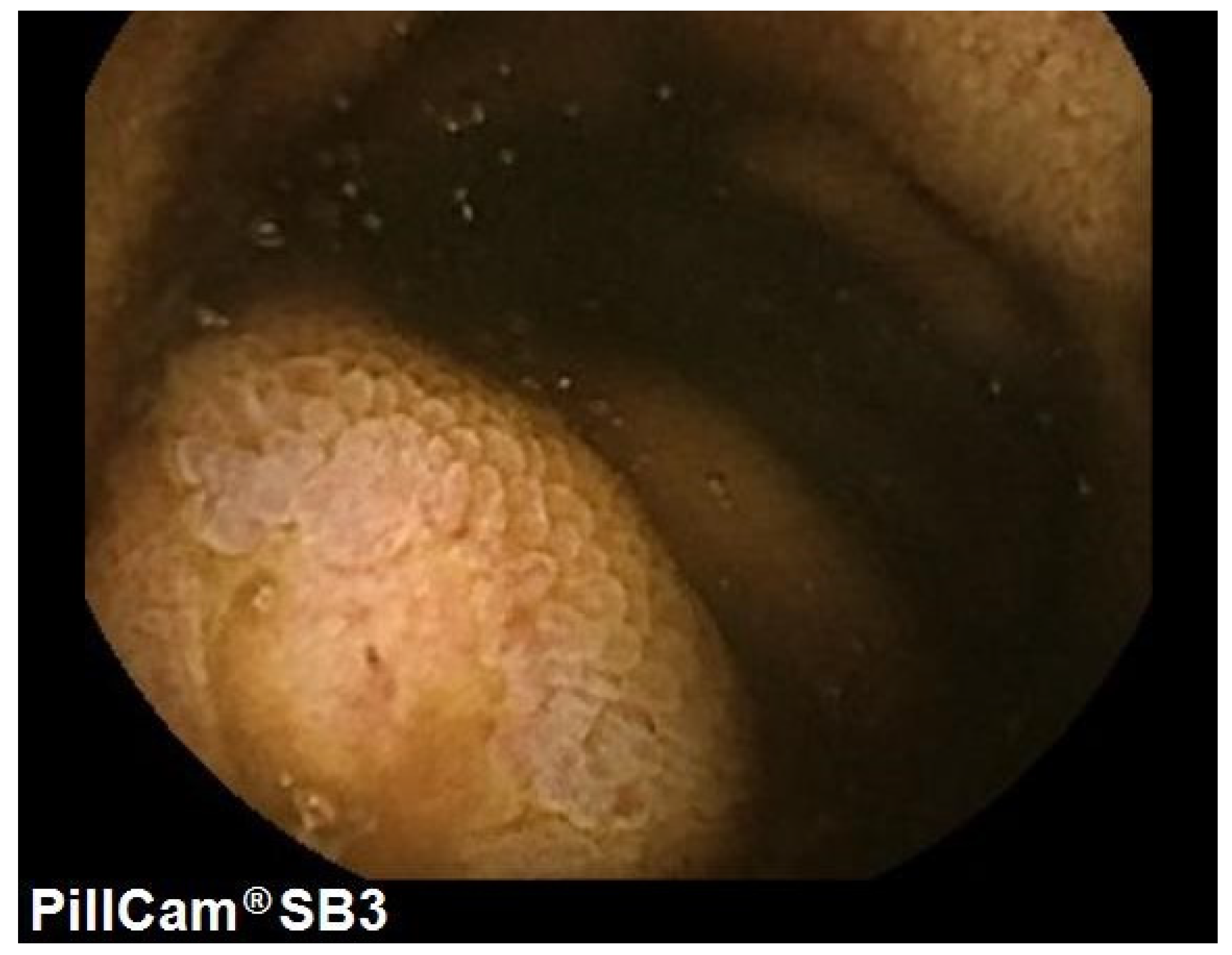
Colonoscopy was performed in April 2023 and showed numerous whitish and slightly elevated, submucosal lesions throughout the entire colon and terminal ileum. The size of the lesions varied from 5 to 20 mm (Figure 2), with a rigid consistency on biopsy and a negative “pillow sign”; Histological examination resulted in a diagnosis of multifocal granular cell tumors based on morphological, immunohistochemical, and immunophenotypic characteristics which were close to those observed five years earlier. Slides from these lesions were comparable to those from the biopsies taken in 2018 of the esophageal lesion. To complete the GI tract study, Video Capsule Endoscopy (VCE) was performed, revealing the presence of more than 20 lesions throughout the whole small intestine, ranging in size from 2 to 10 mm and macroscopically compatible with granular cell tumors (Figure 3).
The patient’s 12 year-old daughter, during a routine dental checkup, was found to have a white and painless nodule on the tongue, at high clinical suspicion for a granular cell tumor. She was asymptomatic and denied any symptom of dysphagia, food impaction or weight loss, her past medical history was unremarkable and her physical and psychological development were within the norm, she regularly attends school.
The nodule was subsequently biopsied, resulting in an histological confirmation of GCT. The girl has not yet undergone endoscopy due to the parents’ wishes.
3. Discussion
Granular cell tumor (GCT), known as Abrikossoff tumor, is a rare tumor that originates from
Schwann cells (1).
This type of tumor can potentially affect soft tissues of any organ, but it most frequently involves the head and neck region, the oral cavity, the skin, or subcutaneous tissues. The tongue is the most frequently affected site (9).
Individuals of any age can present with this tumor, most commonly during the fourth, fifth, and sixth decades of life, with an incidence peaking between the fourth and the sixth decade (9). Females are more frequently affected than males, with an M/F ratio = ½.
Pediatric cases are rare, but some reports are available, including a case series of neonatal or congenital oral GCTs (10).
Histologically, they are composed of nests or sheets of plump epithelioid or spindle cells (or both) with a small, round nucleus and abundant granular eosinophilic cytoplasm. These histological characteristics are highly suggestive of GCT, making it possible to diagnose with scarce samples of just a few cells. From an immunohistochemistry point of view, gastrointestinal GCTs are characterized by positivity for S-100 protein (100%), CD56 (95%), CD68 (95%), SOX-10 (93%), and inhibin alpha (52%) (7). Cases of S-100 negative GCTs have also been reported in the literature (11). While most of these tumors are benign, cases of malignant GCTs have been reported.
Malignancy is defined using the Fanburg-Smith histopathological criteria (12): necrosis, spindling, vesicular nuclei with large nucleoli, mitotic activity (>2/10 HPF), increased nucleus/cytoplasm ratio, and pleomorphism. Lesions exhibiting none of the aforementioned features or with isolated focal pleomorphism are classified as benign, those presenting with one or two are classified as atypical, and those with 3 or more characteristics are categorized as malignant (12).
Cases of metastatic GCTs have been reported, both in cases of metastatic benign GCTs and in cases of metastatic malignant GCTs. The most common site for metastasis are regional lymph nodes, lungs, liver and bones (13).
The gastrointestinal tract is involved in up to 11% of cases, with the esophagus, especially the distal esophagus, being the most frequently affected site, followed by the colon and the stomach (14). There have also been reports of GCTs detected in the pancreas (15), biliary tree(16) or the appendix (17), but these locations are less common.
Typically, these lesions present as solitary nodules covered by white or yellow mucosa. GCTs of the colon and stomach tend to be larger in size than those found in the esophagus, with an average dimension of 0.75 cm, 0.6 cm, and 0.27 cm, respectively (14). Gastrointestinal GCTs are histologically similar to GCTs found in other locations, even though those located in the colon tend to exhibit more nuclear atypia, a feature that has not been correlated with malignancy (4). Most gastrointestinal granular cell tumors are incidentally detected during endoscopic examinations performed for other reasons, with the majority of patients being asymptomatic. Rarely, esophageal GCTs present in patients reporting voice changes such as hoarseness or dysphagia.
Endoscopic removal with EMR or ESD is the safest and most effective treatment when feasible (18), especially for single lesions. The benefits of endoscopic treatment versus surgical removal are: a less invasive procedure that can prevent skin scars caused by incisions, reduces the perceived pain associated with surgical trauma, and lowers the risk of postoperative infections. No specific guidelines are available to aid in the decision of the best removal technique, but some involved factors, such as the size and dimension or location of the nodule, could be applied to guidelines used for the endoscopic removal of different subepithelial lesions (19). EMR is the easier and less
time-consuming technique, however, it can be applied only in smaller lesions, usually up to 10 mm in diameter, in order to maximize the probability of “en-bloc” curative resection. Seldomly, this technique can lead to serious complications, such as perforation (20–22). Cap-assisted EMR has also been employed for small esophageal GCTs (23). An attempt to remove a 13-mm esophageal GCT by EMR was unsuccessful, in a report from the Mayo Clinic (24).
It must be noted that the majority of esophageal GCTs are not confined to the mucosa, but rather, involve the submucosa, which results in frequent involvement of the resection margins. ESD removal consists of the dissection of submucosal tissues beneath the lesion; its use is described for GCTs only in the right colon (25). Despite a higher probability of obtaining an “en-bloc” curative resection, this technique is not yet widespread. New strategies to facilitate the procedure, especially applying counter-traction strategies (i.e. the clip and rubber band approaches) and new knives have been proposed (26) but the procedure remains quite challenging and of limited experience in the context of GCTs, and should be applied only in tertiary referral centers. However, when conducted by expert endoscopists, this technique lasts between 25 to 60 minutes and guarantees complete resection rates of more than 90%. Further benefits include lower complications and recurrence-free periods of up to 18 months after resection (27). Surgical removal can be considered for lesions larger than 3 cm, those invading the muscularis propria, or those with suspicious malignancy features. Cases of endoscopic surveillance for small, stable-sized lesions with follow-up endoscopies are reported (24).
The etiology and pathophysiology of GCTs is yet poorly understood as well as their specific association with genetic syndromes. A possible role of GCTs pathogenesis could be played by trauma; there have been several reports of GCTs occurring at trauma sites, such as surgical scars, vaccination sites or within a tattoo.
An interesting association between Eosinophilic Esophagitis (EoE) and esophageal granular cell tumors has been reported by different authors, both in children and in adults (28–30). A possible cause of this association is believed to be chronic esophageal inflammation found in patients affected by EOE even though further data and research is needed to understand the immunological pathway linking EoE and esophageal GCTs.
No specific genetic mutation has been linked to the development of GCTs.
Somatic mutations of ATP6AP1 and ATP6AP2 genes in Schwann cells, which results in an accumulation of intracytoplasmic granules typical of GCTs, have been proposed as lonely drivers of GCTs, and appear to be pathognomonic for these tumors (31).
The presence of multiple granular cell tumors has been associated with syndromes, such as Noonan syndrome (32), neurofibromatosis type I (33), and LEOPARD syndrome (34). A possible feature present in all of the three syndromes is an abnormal RAS/MAPK pathway but mutations of PTPN11 (34)gene link LEOPARD and Noonan syndrome.
To our knowledge, there are no reported cases in the literature of multifocal GCTs involving the entire gastrointestinal tract.
Currently, there are no guidelines for the treatment and follow-up of gastrointestinal GCTs.
The role of conventional chemotherapy and/or radiation is still debated and should be considered in patients with recurrent malignant or metastatic GCTs. For these reasons, given the impossibility of an operative approach through endoscopic and/or surgical removal due to the presence of too many lesions, we proposed that the best management in our case could include annual endoscopic monitoring with EGDS, VCE, and colonoscopy, annual mammography and Pap tests, and monitoring for any newly appearing formations on the skin and oral cavity with regular dermatological and odontostomatological check-ups. Furthermore, considering the possible familial component to this tumor in our case, we believe it could be beneficial to conduct genetic counseling as part of research protocols to understand the potential presence of a predisposing genetic mutation
5. Conclusions
Granular Cell Tumors are rare tumors that may affect the gastrointestinal tract with bening or potentially malignant behaviour in both pediatric or adult life. Their appearance is typically described as submucosal isolated lesions of the esofagus or the stomach, making them potentially amenable of endoscopic or surgical resection. Our research presents one of the first documented cases of a patient with panenteric gastrointestinal GCTs while also suggesting a potential hereditary component, due to the concomitant diagnosis of a tongue GCT affecting the patient’s daughter. We believe that reporting such cases is of utmost importance for such conditions as no clinical or endoscopic guidelines exist to manage these rare tumors. Genetic counseling will be essential to identify possible genetic mutations.
Author Contributions
Conceptualization, M.C; writing- original draft preparation, R.S. and, L.F.; writing- reviewing and editing, F.M.; supervision, M.C. and, F.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Clinical and endoscopic data of the patient are available in our Hospital server.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Stefansson, K.; Wollmann, R.L. S-100 protein in granular cell tumors (granular cell myoblastomas). Cancer 1982, 49, 1834–1838. [Google Scholar] [CrossRef]
- Weber, C.O.; Virchow, R. Anatomische Untersuchung einer hypertrophischen Zunge nebst Bemerkungen über die Neubildung quergestreifter Muskelfasern. Archiv für Pathologische Anatomie und Physiologie und für Klinische Medicin 1854, 7, 115–125. [Google Scholar] [CrossRef]
- Abrikossoff, A. Über Myome. Virchows Arch Pathol Anat Physiol Klin Med 1926, 260, 215–233. [Google Scholar] [CrossRef]
- Na, J.I.; Kim, H.J.; Jung, J.J.; Kim, Y.; Kim, S.S.; Lee, J.H.; et al. Granular cell tumours of the colorectum: histopathological and immunohistochemical evaluation of 30 cases. Histopathology 2014, 65, 764–774. [Google Scholar] [CrossRef]
- Fahim, S.; Aryanian, Z.; Ebrahimi, Z.; Kamyab-Hesari, K.; Mahmoudi, H.; Alizadeh, N.; et al. Cutaneous granular cell tumor: A case series, review, and update. J Family Med Prim Care 2022, 11, 6955–6958. [Google Scholar]
- Salaouatchi, M.T.; De Breucker, S.; Rouvière, H.; Lesage, V.; Rocq LJA, Vandergheynst, F. ; et al. A Rare Case of a Metastatic Malignant Abrikossoff Tumor. Case Rep Oncol. 2021, 14, 1868–1875. [Google Scholar] [CrossRef]
- Canavesi, A.; Berrueta, J.; Pillajo, S.; Gaggero, P.; Olano, C. Endoscopic resection of a granular cell tumor (Abrikossoff’s tumor) in the esophagus using cap-assisted band ligation. Endoscopy. 2023, 55 (Suppl. 1), E796–E797. [Google Scholar] [CrossRef]
- De Vincentis, F.; Manzi, I.; Di Giorgio, V.; Mussetto, A. Endoscopic full-thickness resection of a residual scar in ascending colon to assess post-EMR complete removal of an Abrikossoff tumor. Dig Liver Dis 2023, 55, 985–986. [Google Scholar] [CrossRef]
- van de Loo, S.; Thunnissen, E.; Postmus, P.; van der Waal, I. Granular cell tumor of the oral cavity; a case series including a case of metachronous occurrence in the tongue and the lung. Med Oral Patol Oral Cir Bucal 2015, 20, e30–e33. [Google Scholar] [CrossRef]
- Zheng, C.; Su, J.; Liang, X.; Wu, J.; Gu, W.; Zhao, X. Clinical and pathological analysis of congenital granular cell tumor. Hua Xi Kou Qiang Yi Xue Za Zhi 2022, 40, 710–715. [Google Scholar]
- Parfitt, J.R.; McLean, C.A.; Joseph, M.G.; Streutker, C.J.; Al-Haddad, S.; Driman, D.K. Granular cell tumours of the gastrointestinal tract: expression of nestin and clinicopathological evaluation of 11 patients. Histopathology 2006, 48, 424–430. [Google Scholar] [CrossRef]
- Fanburg-Smith, J.C.; Meis-Kindblom, J.M.; Fante, R.; Kindblom, L.G. Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol 1998, 22, 779–794. [Google Scholar] [CrossRef]
- Menaker, G.M.; Sanger, J.R. Granular Cell Tumor of Uncertain Malignant Potential. Ann Plast Surg 1997, 38, 658–660. [Google Scholar] [CrossRef]
- An, S.; Jang, J.; Min, K.; Kim, M.S.; Park, H.; Park, Y.S.; et al. Granular cell tumor of the gastrointestinal tract: histologic and immunohistochemical analysis of 98 cases. Hum Pathol 2015, 46, 813–819. [Google Scholar] [CrossRef]
- Kanno, A.; Satoh, K.; Hirota, M.; Hamada, S.; Umino, J.; Itoh, H.; et al. Granular cell tumor of the pancreas: A case report and review of literature. World J Gastrointest Oncol 2010, 2, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, D.J.; Klapper, E.; Gordon, L.A.; Silberman, A.W. Granular cell tumor of the biliary system. Med Pediatr Oncol. 1994, 23, 50–56. [Google Scholar] [CrossRef]
- Lv, X.; Sun, X.; Zhou, J.; Zhang, Y.; Lv, G. Granular cell tumor of the appendix: a case report and literature review. Journal of International Medical Research 2022, 50, 030006052211093. [Google Scholar] [CrossRef]
- Chen W shu, Zheng X ling, Jin, L. ; Pan X jie, Ye M fan. Novel diagnosis and treatment of esophageal granular cell tumor: report of 14 cases and review of the literature. Ann Thorac Surg 2014, 97, 296–302. [Google Scholar] [CrossRef]
- Deprez, P.H.; Moons LMG, OʼToole, D. ; Gincul, R.; Seicean, A.; Pimentel-Nunes, P.; et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022, 54, 412–429. [Google Scholar]
- Battaglia, G.; Rampado, S.; Bocus, P.; Guido, E.; Portale, G.; Ancona, E. Single-band mucosectomy for granular cell tumor of the esophagus: safe and easy technique. Surg Endosc 2006, 20, 1296–1298. [Google Scholar] [CrossRef]
- Wehrmann, T.; Martchenko, K.; Nakamura, M.; Riphaus, A.; Stergiou, N. Endoscopic Resection of Submucosal Esophageal Tumors: A Prospective Case Series. Endoscopy 2004, 36, 802–807. [Google Scholar] [CrossRef]
- Sakamoto, H.; Suga, M.; Ozeki, I.; Kobayashi, T.; Sugaya, T.; Sasaki, Y.; et al. Subcapsular hematoma of the liver and pylethrombosis in the setting of cholestatic liver injury. J Gastroenterol [Internet] 1996, 31, 880–884. [Google Scholar] [CrossRef]
- Canavesi, A.; Berrueta, J.; Pillajo, S.; Gaggero, P.; Olano, C. Endoscopic resection of a granular cell tumor (Abrikossoff’s tumor) in the esophagus using cap-assisted band ligation. Endoscopy. 2023, 55 (Suppl. 1), E796–E797. [Google Scholar] [CrossRef]
- Zhong, N.; Katzka, D.A.; Smyrk, T.C.; Wang, K.K.; Topazian, M. Endoscopic diagnosis and resection of esophageal granular cell tumors. Diseases of the Esophagus 2011, 24, 538–543. [Google Scholar] [CrossRef]
- Biscay, M.; Chabrun, E.; Menguy, S.; Cesbron-Métivier, E.; Barthet, M.; Marty, M.; et al. Colonic Abrikossoff tumor: fortuitous discovery at colonoscopy for serrated adenomas polyposis, and resection by endoscopic submucosal dissection. Endoscopy 2019, 51, E176–E178. [Google Scholar] [CrossRef]
- Utzeri, E.; Jacques, J.; Charissoux, A.; Rivory, J.; Legros, R.; Ponchon, T.; et al. Traction strategy with clips and rubber band allows complete en bloc endoscopic submucosal dissection of laterally spreading tumors invading the appendix. Endoscopy 2017, 49, 820–822. [Google Scholar] [CrossRef]
- Lu, W.; Xu, M.D.; Zhou, P.H.; Zhang, Y.Q.; Chen, W.F.; Zhong, Y.S.; et al. Endoscopic submucosal dissection of esophageal granular cell tumor. World J Surg Oncol. 2014, 12, 221. [Google Scholar] [CrossRef]
- Malik, F.; Bernieh, A.; Saad, A.G. Esophageal Granular Cell Tumor in Children: A Clinicopathologic Study of 11 Cases and Review of the Literature. Am J Clin Pathol 2023, 160, 106–112. [Google Scholar] [CrossRef]
- Riffle, M.E.; Polydorides, A.D.; Niakan, J.; Chehade, M. Eosinophilic Esophagitis and Esophageal Granular Cell Tumor. American Journal of Surgical Pathology 2017, 41, 616–621. [Google Scholar] [CrossRef]
- Reddi, D.; Chandler, C.; Cardona, D.; Schild, M.; Westerhoff, M.; McMullen, E.; et al. Esophageal granular cell tumor and eosinophils: a multicenter experience. Diagn Pathol 2021, 16, 49. [Google Scholar] [CrossRef]
- Pareja, F.; Brandes, A.H.; Basili, T.; Selenica, P.; Geyer, F.C.; Fan, D.; et al. Loss-of-function mutations in ATP6AP1 and ATP6AP2 in granular cell tumors. Nat Commun 2018, 9, 3533. [Google Scholar] [CrossRef] [PubMed]
- Castagna, J.; Clerc, J.; Dupond, A.S.; Laresche, C. Tumeurs à cellules granuleuses multiples chez un enfant atteint d’un syndrome de Noonan compliqué de leucémie myélomonocytaire juvénile. Ann Dermatol Venereol 2017, 144, 705–711. [Google Scholar] [CrossRef]
- Weinreb, I.; Bray, P.; Ghazarian, D. Plexiform intraneural granular cell tumour of a digital cutaneous sensory nerve. J Clin Pathol 2007, 60, 725–726. [Google Scholar] [CrossRef] [PubMed]
- Schrader, K.; Nelson, T.; De Luca, A.; Huntsman, D.; McGillivray, B. Multiple granular cell tumors are an associated feature of LEOPARD syndrome caused by mutation in PTPN11. Clin Genet 2009, 75, 185–189. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
EGDS 2018: white nodule, granular cell tumor on histology.
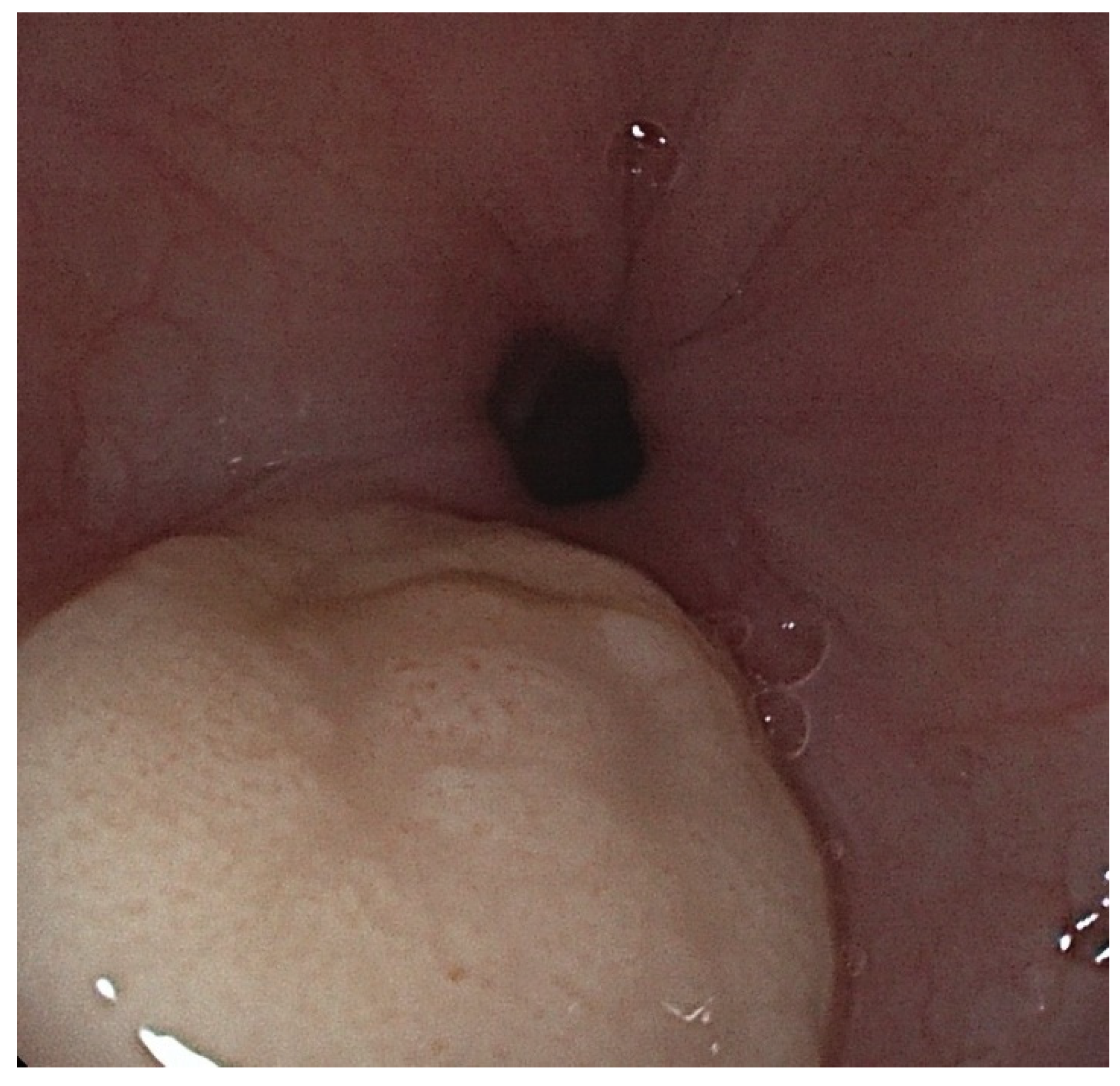
Figure 2.
Colonoscopy 2023: numerous submucosal formations present in the whole colon.
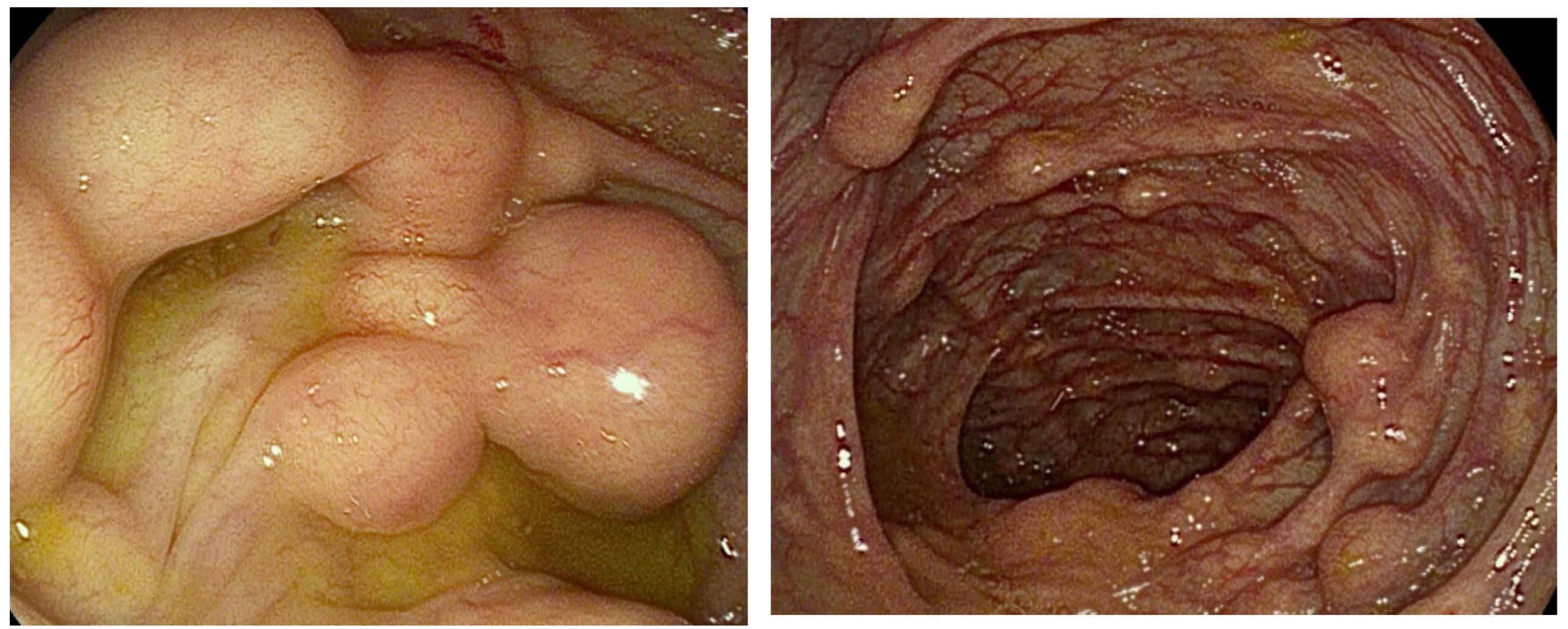
Figure 3.
VCE 2023: multiple white submucosal nodules seen in the small intestine.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



