
Submitted:
19 October 2023
Posted:
25 October 2023
You are already at the latest version
Abstract
Photon-counting Computed Tomography (PCCT) is a promising cardiovascular-imaging technique. Using detectors that count the number and energy of photons in multiple bins, PCCT offers several advantages over conventional CT, including a higher image quality, reduced contrast agent volume, radiation doses, and artifacts. Although PCCT is well established for cardiac imaging in assessing coronary artery disease, its application in vascular imaging remains limited. This review summarizes the available literature and provides an overview of the current use of PCCT for the diagnosis of vascular conditions. Of the 13 records selected in the initial search, 7 articles were included in the present review: 6 cohort studies and 1 case report. This review synthesized the available literature on PCCT in vascular imaging, focusing mainly on endoleaks detection and characterization after endovascular aneurysm repair (EVAR), contrast dose volume, and radiation exposure reduction, particularly in patients with chronic kidney disease and in those requiring follow-up CT.
Keywords:
Vascular
; Photon-counting
; CT Angiography
; Dose Exposure
; Contrast Agents
; EVAR
; Aorta
; Endoleaks
1. Introduction
Photon-counting CT (PCCT) is an innovative technology that delivers a high image quality and enhanced spatial resolution [1]. Using detectors that count the number and energy of photons in multiple bins, PCCT offers several advantages over conventional CT, including higher spatial and contrast resolutions, reduced artifacts, and lower radiation doses [2]. PCCT has been a well-established technique used in cardiac imaging [3] to assess coronary artery disease (CAD) since its introduction in 2021 [4]. Rajagopal et al. demonstrated that PCCT exhibited superior accuracy in detecting plaque composition in coronary phantoms, compared to standard CT [5]. Although high-resolution PCCT produces higher noise levels, it is less affected by artifacts and blooming caused by stents5. However, the application of PCCT to vascular imaging remains limited.
Recent studies have demonstrated the potential of PCCT for detecting and characterizing endoleaks (ELs) after EVAR. PCCT shows endoleak detection capabilities comparable to those of traditional CT, reducing radiation exposure [6,7]. Bicolor K-edge imaging and dual-contrast agent protocols in PCCT allowed accurate characterization of ELs within the thoracic aorta. Furthermore, PCCT low-volume contrast protocols have shown promising results in reducing contrast agent volume without compromising image quality [8]. This is particularly relevant for patients with chronic kidney disease or those requiring frequent follow-up imaging. Virtual monoenergetic images (VMI) reconstructed at optimal energy levels demonstrated improved contrast-to-noise ratios compared with energy-integrating detector (EID) CT, highlighting the potential of PCCT in achieving higher image quality while minimizing contrast-related risks[9]. This review aimed to synthesize the available literature and provide an overview of the current use of PCCT in diagnosing vascular conditions. (Table 1)
2. Photon-Counting Detector – Technical Considerations
Photon-counting Detector (PCD) directly measures the energy of each photon and converts it into an electrical signal. PCD quantifies the number of photons and divides the X-ray energy spectrum into multiple bins. This technology offers several advantages over conventional CT, including improved spatial and contrast resolution, reduced image noise and artifacts, lower radiation exposure, and the ability to perform multi-energy/multiparametric imaging based on the atomic properties of the tissues. This enables the use of different contrast agents and enhances quantitative imaging. [13]PCCT also provides the capability to differentiate between materials based on the energy of incoming photons. Conventional CT uses energy-integrating detectors (EID) with scintillator elements that convert X-rays into visible light, which are then detected by a photodiode[11]. The photodiode indirectly measured the energy of the X-ray photons. Instead, PCCT directly converts X-ray photons into an electrical signal by applying a high voltage to a semiconductor sensor between the cathode and pixelated anode[14]. Each X-ray photon is promptly converted into electron-hole pairs, which move toward the anode under an applied voltage [Figure 1]. The charge carriers collected by the pixels generate a second electrical signal proportional to the incoming X-ray photons. By setting energy thresholds, PCCT can separate photons that exceed a certain level, thereby reducing the electronic noise[15,16,17].
3. Photon-Counting CT - Endoleaks Detection
Abdominal aortic aneurysm (AAA) is a bulging of the abdominal aorta with a diameter ≥ 3 cm, affecting 1.6-7.2% of people and occurring in 0.4-0.7% per year in the Western population[18].
The current criteria for elective treatment of AAAs are based on aortic diameter. European Society for Vascular Surgery (ESVS) guidelines suggest elective repair for AAAs ≥ 5.5 cm in men (5 cm in women) or if they show rapid growth (greater than 1 cm/year). Elective repair is also recommended for asymptomatic fusiform AAAs of 5.5 cm in men and 5.0 cm in women.[19]
Endovascular aneurysm repair (EVAR) is a common treatment that involves insertion of a covered stent graft inside the aneurysm[20]. However, EVAR can lead to endoleaks (ELs), which are the persistence of blood flow outside the graft into the aneurysm sac[21], posing the risk of growth and rupture (Table 2). ELs were the most common complication (53% of all complications), with an incidence of 11.7%[22]. Detecting and managing ELs is challenging, and lifelong follow-up is essential, involving regular contrast-enhanced CT scans at specific intervals, including 1, 6, and 12 months after EVAR and yearly thereafter[23,24]. Traditional CT protocols include unenhanced, arterial-phase, and venous/delayed-phase scans to assess the blood vessels and stent grafts[25,26,27]. However, the drawback of repeated CT scans exposes patients to high radiation doses and kidney toxicity, necessitating the exploration of advanced imaging techniques to mitigate this concern[28].
Photon-counting CT (PCCT) has emerged as a promising advanced imaging modality aimed at reducing radiation exposure while improving endoleak detection accuracy. Gomollon et al. 6conducted a comparative study to evaluate the image quality and endoleak detection between traditional triphasic CT and virtual non-iodine (VNI) images on PCCT in 110 patients after EVAR. Their results demonstrated comparable endoleak detection between the two readout sets with high sensitivity and specificity. This study demonstrated the feasibility and potential of using virtual non-iodine image PCCT as a valuable tool to reduce radiation exposure during endoleak detection. Cosset et al. [8] has explored the potential of bicolor K-edge PCCT in endoleak analysis by employing a dynamic thoracic aorta phantom and creating three types of thoracic endoleaks using iodinated and gadolinium contrast agents. This imaging technique allowed the characterization of endoleaks within the thoracic aorta in a single acquisition combined with a biphasic contrast agent injection. The authors underscored the potential of SPCCT to accurately characterize endoleaks and offer valuable insights for improved diagnosis and management. Dangelmaier et al.7 explored the feasibility of PCCT with two contrast agents to detect endoleaks following EVAR. Using a specialized abdominal aortic aneurysm phantom filled with a mixture of iodine, gadolinium, and calcium chloride, they were able to differentiate the distribution of these agents, enabling reliable detection of endoleaks. The authors suggested that PCCT has the potential to replace multiphase CT scans, thereby reducing radiation exposure while maintaining the diagnostic accuracy. [ Figure 2 and Figure 3 ]
Overall, these studies highlight ongoing advancements in endoleak detection in patients with AAAs undergoing EVAR. photon counting CT hold promise in revolutionizing the management of ELs by reducing radiation exposure while enhancing accuracy.
4. Photon Counting CT Aortic Imaging: Radiation Dose and Contrast Volume Reduction
PCCT has shown significant promise, particularly in patients with chronic kidney disease (CKD) or those requiring follow-up imaging. Several recent studies have demonstrated the potential benefits of PCCT, including excellent image quality, reduced contrast agent volume, and improved contrast-to-noise ratio (CNR). Higashigaito et al. [9] explored a low-volume contrast medium protocol for thoracoabdominal CT angiography using PCCT. This study compared PCCT with previous energy-integrating detector (EID) CT at equal radiation doses. Virtual monoenergetic images (VMI) at 50 keV exhibited the best trade-off between objective and subjective image quality, with a 25% higher CNR than that of EID CT. The low-volume contrast media protocol also reduced the volume of the contrast medium by 25%. These findings suggest that PCCT with a low-volume contrast media protocol achieves superior CNR while maintaining non-inferior image quality compared to EID CT. (Figure 4a-e)
Decker et al. [11]evaluated the potential of virtual non-contrast reconstructions using a calcium-preserving algorithm (VNCPC) compared with the standard algorithm (VNCConv) in patients after EVAR. This study demonstrated that VNCPC reconstructions exhibit excellent image quality with complete contrast removal and minimal erroneous subtractions, making them a potential alternative to true non-contrast acquisitions. Euler et al. [12] compared the image quality of high-pitch PCCT angiography with that of conventional CT at equal radiation doses. PCCT with virtual monoenergetic images (VMI) at 40 keV and 45 keV demonstrated a significantly increased CNR compared to traditional CT at matched radiation doses. Subjective image quality ratings revealed slightly higher subjective noise for VMI at 40 keV and 45 keV. However, this study suggests that VMI at 45–50 keV offers a favorable balance between the objective and subjective image quality.
Rau et al. [10]presented a case study of a patient with incipient chronic renal failure who required contrast-enhanced aortoiliac CT angiography for follow-up imaging of an asymptomatic abdominal aortic aneurysm (AAA) Utilizing a PCCT protocol with dual-source spectral image acquisition and dynamic monochromatic reconstruction near the K-edge of iodine, this study demonstrated a significantly reduced required contrast agent while preserving the diagnostic confidence. (Figure 5)
In conclusion, these studies demonstrated that PCCT offers advantages such as improved CNR, reduced contrast agent volume, and enhanced image quality, making it an attractive option for patients with CDK or those requiring follow-up imaging.
5. Conclusions and Future Directions
This review demonstrates the potential of PCCT in cardiovascular imaging. PCCT presents higher spatial and contrast resolutions than conventional CT, allowing endoleak detection with less radiation after EVAR. PCCT can also characterize endoleaks in the thoracic aorta with bicolor K-edge imaging and dual-contrast agents and reduce contrast agent volumes with low-volume protocols, benefiting patients with CKD or those needing frequent CT imaging. Furthermore, PCCT can improve CNR with VIM at optimal energy levels, thereby achieving a higher image quality and lower contrast-related risks. These advancements in imaging techniques hold promise for optimizing patient care and diagnosis for the management of aortic pathologies. Further research and extensive studies are needed to confirm these results and explore the full potential of PCCT in vascular imaging.
Key Points
- Compared with conventional CT, PCCT has potential advantages in cardiovascular imaging, including improved image quality, reduced artifacts, and lower radiation doses.
- PCCT can improve endoleak detection and characterization after EVAR with reduced radiation exposure using bicolor K-edge imaging and dual contrast agents.
- Low-volume protocols in PCCT can minimize the contrast agent volume, benefiting patients with CKD and those requiring frequent CT imaging.
- Virtual monoenergetic images at optimal energy levels improve contrast-to-noise ratios, resulting in higher image quality and reduced contrast-related risk.
Glossary
| AAA | abdominal aortic aneurysm |
| CAD | coronary artery disease |
| CNR | contrast-to-noise ratio |
| CTA | computed tomography angiography |
| EID | energy-integrating detector |
| ELs | Endoleaks |
| EVAR | Endovascular Aortic Repair |
| PCCT | Photon-Counting CT PCD = Photon-Counting Detector |
| TNC | True Non-Contrast; VMI =Virtual monoenergetic images |
| VNI | Virtual Non-Iodine image |
References
- Pepe, A.; Crimì, F.; Vernuccio, F.; Cabrelle, G.; Lupi, A.; Zanon, C.; Gambato, S.; Perazzolo, A.; Quaia, E. Medical Radiology: Current Progress. Diagnostics 2023, 13 (14), 2439. [CrossRef]
- Meloni, A.; Frijia, F.; Panetta, D.; Degiorgi, G.; De Gori, C.; Maffei, E.; Clemente, A.; Positano, V.; Cademartiri, F. Photon-Counting Computed Tomography (PCCT): Technical Background and Cardio-Vascular Applications. Diagnostics 2023, 13 (4), 645. [CrossRef]
- Zsarnóczay, E.; Varga-Szemes, A.; Emrich, T.; Szilveszter, B.; van der Werf, N. R.; Mastrodicasa, D.; Maurovich-Horvat, P.; Willemink, M. J. Characterizing the Heart and the Myocardium With Photon-Counting CT. Invest Radiol 2023, 58 (7), 505–514. [CrossRef]
- Mastrodicasa, D.; Aquino, G. J.; Ordovas, K. G.; Vargas, D.; Fleischmann, D.; Abbara, S.; Hanneman, K. Radiology: Cardiothoracic Imaging Highlights 2022. Radiol Cardiothorac Imaging 2023, 5 (3). [CrossRef]
- Rajagopal, J. R.; Farhadi, F.; Richards, T.; Nikpanah, M.; Sahbaee, P.; Shanbhag, S. M.; Bandettini, W. P.; Saboury, B.; Malayeri, A. A.; Pritchard, W. F.; Jones, E. C.; Samei, E.; Chen, M. Y. Evaluation of Coronary Plaques and Stents with Conventional and Photon-Counting CT: Benefits of High-Resolution Photon-Counting CT. Radiol Cardiothorac Imaging 2021, 3 (5). [CrossRef]
- Turrion Gomollon, A. M.; Mergen, V.; Sartoretti, T.; Polacin, M.; Nakhostin, D.; Puippe, G.; Alkadhi, H.; Euler, A. Photon-Counting Detector CT Angiography for Endoleak Detection After Endovascular Aortic Repair. Invest Radiol 2023. [CrossRef]
- Dangelmaier, J.; Bar-Ness, D.; Daerr, H.; Muenzel, D.; Si-Mohamed, S.; Ehn, S.; Fingerle, A. A.; Kimm, M. A.; Kopp, F. K.; Boussel, L.; Roessl, E.; Pfeiffer, F.; Rummeny, E. J.; Proksa, R.; Douek, P.; Noël, P. B. Experimental Feasibility of Spectral Photon-Counting Computed Tomography with Two Contrast Agents for the Detection of Endoleaks Following Endovascular Aortic Repair. Eur Radiol 2018, 28 (8), 3318–3325. [CrossRef]
- Cosset, B.; Sigovan, M.; Boccalini, S.; Farhat, F.; Douek, P.; Boussel, L.; Si-Mohamed, S. A. Bicolor K-Edge Spectral Photon-Counting CT Imaging for the Diagnosis of Thoracic Endoleaks: A Dynamic Phantom Study. Diagn Interv Imaging 2023, 104 (5), 235–242. [CrossRef]
- Higashigaito, K.; Euler, A.; Eberhard, M.; Flohr, T. G.; Schmidt, B.; Alkadhi, H. Contrast-Enhanced Abdominal CT with Clinical Photon-Counting Detector CT: Assessment of Image Quality and Comparison with Energy-Integrating Detector CT. Acad Radiol 2022, 29 (5), 689–697. [CrossRef]
- Rau, S.; Soschynski, M.; Schlett, C. L.; Hagar, M. T. Spectral Aortoiliac Photon-Counting CT Angiography with Minimal Quantity of Contrast Agent. Radiol Case Rep 2023, 18 (6), 2180–2182. [CrossRef]
- Decker, J. A.; Bette, S.; Scheurig-Muenkler, C.; Jehs, B.; Risch, F.; Woźnicki, P.; Braun, F. M.; Haerting, M.; Wollny, C.; Kroencke, T. J.; Schwarz, F. Virtual Non-Contrast Reconstructions of Photon-Counting Detector CT Angiography Datasets as Substitutes for True Non-Contrast Acquisitions in Patients after EVAR—Performance of a Novel Calcium-Preserving Reconstruction Algorithm. Diagnostics 2022, 12 (3), 558. [CrossRef]
- Euler, A.; Higashigaito, K.; Mergen, V.; Sartoretti, T.; Zanini, B.; Schmidt, B.; Flohr, T. G.; Ulzheimer, S.; Eberhard, M.; Alkadhi, H. High-Pitch Photon-Counting Detector Computed Tomography Angiography of the Aorta. Invest Radiol 2022, 57 (2), 115–121. [CrossRef]
- Stein, T.; Rau, A.; Russe, M. F.; Arnold, P.; Faby, S.; Ulzheimer, S.; Weis, M.; Froelich, M. F.; Overhoff, D.; Horger, M.; Hagen, F.; Bongers, M.; Nikolaou, K.; Schönberg, S. O.; Bamberg, F.; Weiß, J. Photon-Counting Computed Tomography – Basic Principles, Potenzial Benefits, and Initial Clinical Experience. RöFo - Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgebenden Verfahren 2023. [CrossRef]
- Tortora, M.; Gemini, L.; D’Iglio, I.; Ugga, L.; Spadarella, G.; Cuocolo, R. Spectral Photon-Counting Computed Tomography: A Review on Technical Principles and Clinical Applications. J Imaging 2022, 8 (4), 112. [CrossRef]
- Leng, S.; Bruesewitz, M.; Tao, S.; Rajendran, K.; Halaweish, A. F.; Campeau, N. G.; Fletcher, J. G.; McCollough, C. H. Photon-Counting Detector CT: System Design and Clinical Applications of an Emerging Technology. RadioGraphics 2019, 39 (3), 729–743. [CrossRef]
- Willemink, M. J.; Persson, M.; Pourmorteza, A.; Pelc, N. J.; Fleischmann, D. Photon-Counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289 (2), 293–312. [CrossRef]
- Rajendran, K.; Petersilka, M.; Henning, A.; Shanblatt, E. R.; Schmidt, B.; Flohr, T. G.; Ferrero, A.; Baffour, F.; Diehn, F. E.; Yu, L.; Rajiah, P.; Fletcher, J. G.; Leng, S.; McCollough, C. H. First Clinical Photon-Counting Detector CT System: Technical Evaluation. Radiology 2022, 303 (1), 130–138. [CrossRef]
- Aggarwal, S.; Qamar, A.; Sharma, V.; Sharma, A. Abdominal Aortic Aneurysm: A Comprehensive Review. Exp Clin Cardiol 2011, 16 (1), 11–15.
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; Kölbel, T.; Loftus, I.; Mani, K.; Melissano, G.; Powell, J.; Szeberin, Z.; ESVS Guidelines Committee; de Borst, G. J.; Chakfe, N.; Debus, S.; Hinchliffe, R.; Kakkos, S.; Koncar, I.; Kolh, P.; Lindholt, J. S.; de Vega, M.; Vermassen, F.; Document reviewers; Björck, M.; Cheng, S.; Dalman, R.; Davidovic, L.; Donas, K.; Earnshaw, J.; Eckstein, H.-H.; Golledge, J.; Haulon, S.; Mastracci, T.; Naylor, R.; Ricco, J.-B.; Verhagen, H. Editor’s Choice – European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. European Journal of Vascular and Endovascular Surgery 2019, 57 (1), 8–93. [CrossRef]
- Keisler, B.; Carter, C. Abdominal Aortic Aneurysm. Am Fam Physician 2015, 91 (8), 538–543.
- White, G. H.; Yu, W.; May, J.; Chaufour, X.; Stephen, M. S. Endoleak as a Complication of Endoluminal Grafting of Abdominal Aortic Aneurysms: Classification, Incidence, Diagnosis, and Management. Journal of Endovascular Therapy 1997, 4 (2), 152–168. [CrossRef]
- Schlösser, F. J. V.; Muhs, B. E. Endoleaks after Endovascular Abdominal Aortic Aneurysm Repair. Curr Opin Cardiol 2012, 27 (6), 598–603. [CrossRef]
- Gozzo, C.; Caruana, G.; Cannella, R.; Farina, A.; Giambelluca, D.; Dinoto, E.; Vernuccio, F.; Basile, A.; Midiri, M. CT Angiography for the Assessment of EVAR Complications: A Pictorial Review. Insights Imaging 2022, 13 (1), 5. [CrossRef]
- Isselbacher, E. M.; Preventza, O.; Hamilton Black, J.; Augoustides, J. G.; Beck, A. W.; Bolen, M. A.; Braverman, A. C.; Bray, B. E.; Brown-Zimmerman, M. M.; Chen, E. P.; Collins, T. J.; DeAnda, A.; Fanola, C. L.; Girardi, L. N.; Hicks, C. W.; Hui, D. S.; Schuyler Jones, W.; Kalahasti, V.; Kim, K. M.; Milewicz, D. M.; Oderich, G. S.; Ogbechie, L.; Promes, S. B.; Gyang Ross, E.; Schermerhorn, M. L.; Singleton Times, S.; Tseng, E. E.; Wang, G. J.; Woo, Y. J. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022, 146 (24). [CrossRef]
- Hong, C.; Heiken, J. P.; Sicard, G. A.; Pilgram, T. K.; Bae, K. T. Clinical Significance of Endoleak Detected on Follow-Up CT After Endovascular Repair of Abdominal Aortic Aneurysm. American Journal of Roentgenology 2008, 191 (3), 808–813. [CrossRef]
- Reginelli, A.; Capasso, R.; Ciccone, V.; Croce, M. R.; Di Grezia, G.; Carbone, M.; Maggialetti, N.; Barile, A.; Fonio, P.; Scialpi, M.; Brunese, L. Usefulness of Triphasic CT Aortic Angiography in Acute and Surveillance: Our Experience in the Assessment of Acute Aortic Dissection and Endoleak. International Journal of Surgery 2016, 33, S76–S84. [CrossRef]
- Lehmkuhl, L.; Andres, C.; Lücke, C.; Hoffmann, J.; Foldyna, B.; Grothoff, M.; Nitzsche, S.; Schmidt, A.; Ulrich, M.; Scheinert, D.; Gutberlet, M. Dynamic CT Angiography after Abdominal Aortic Endovascular Aneurysm Repair: Influence of Enhancement Patterns and Optimal Bolus Timing on Endoleak Detection. Radiology 2013, 268 (3), 890–899. [CrossRef]
- Partovi, S.; Trischman, T.; Rafailidis, V.; Ganguli, S.; Rengier, F.; Goerne, H.; Rajiah, P.; Staub, D.; Patel, I. J.; Oliveira, G.; Ghoshhajra, B. Multimodality Imaging Assessment of Endoleaks Post-Endovascular Aortic Repair. Br J Radiol 2018, 20180013. [CrossRef]
- Stavropoulos, S. W.; Clark, T. W. I.; Carpenter, J. P.; Fairman, R. M.; Litt, H.; Velazquez, O. C.; Insko, E.; Farner, M.; Baum, R. A. Use of CT Angiography to Classify Endoleaks after Endovascular Repair of Abdominal Aortic Aneurysms. Journal of Vascular and Interventional Radiology 2005, 16 (5), 663–667. [CrossRef]
- D’Oria, M.; Mastrorilli, D.; Ziani, B. Natural History, Diagnosis, and Management of Type II Endoleaks after Endovascular Aortic Repair: Review and Update. Ann Vasc Surg 2020, 62, 420–431. [CrossRef]
- Maleux, G.; Poorteman, L.; Laenen, A.; Saint-Lèbes, B.; Houthoofd, S.; Fourneau, I.; Rousseau, H. Incidence, Etiology, and Management of Type III Endoleak after Endovascular Aortic Repair. J Vasc Surg 2017, 66 (4), 1056–1064. [CrossRef]
- Pandey, N.; Litt, H. Surveillance Imaging Following Endovascular Aneurysm Repair. Semin Intervent Radiol 2015, 32 (03), 239–248. [CrossRef]
- Trocciola, S. M.; Dayal, R.; Chaer, R. A.; Lin, S. C.; DeRubertis, B.; Ryer, E. J.; Hynececk, R. L.; Pierce, M. J.; Prince, M.; Badimon, J.; Marin, M. L.; Fuster, V.; Kent, K. C.; Faries, P. L. The Development of Endotension Is Associated with Increased Transmission of Pressure and Serous Components in Porous Expanded Polytetrafluoroethylene Stent-Grafts: Characterization Using a Canine Model. J Vasc Surg 2006, 43 (1), 109–116. [CrossRef]
Figure 1.
Physical principle of the Photon-counting Detector CT.
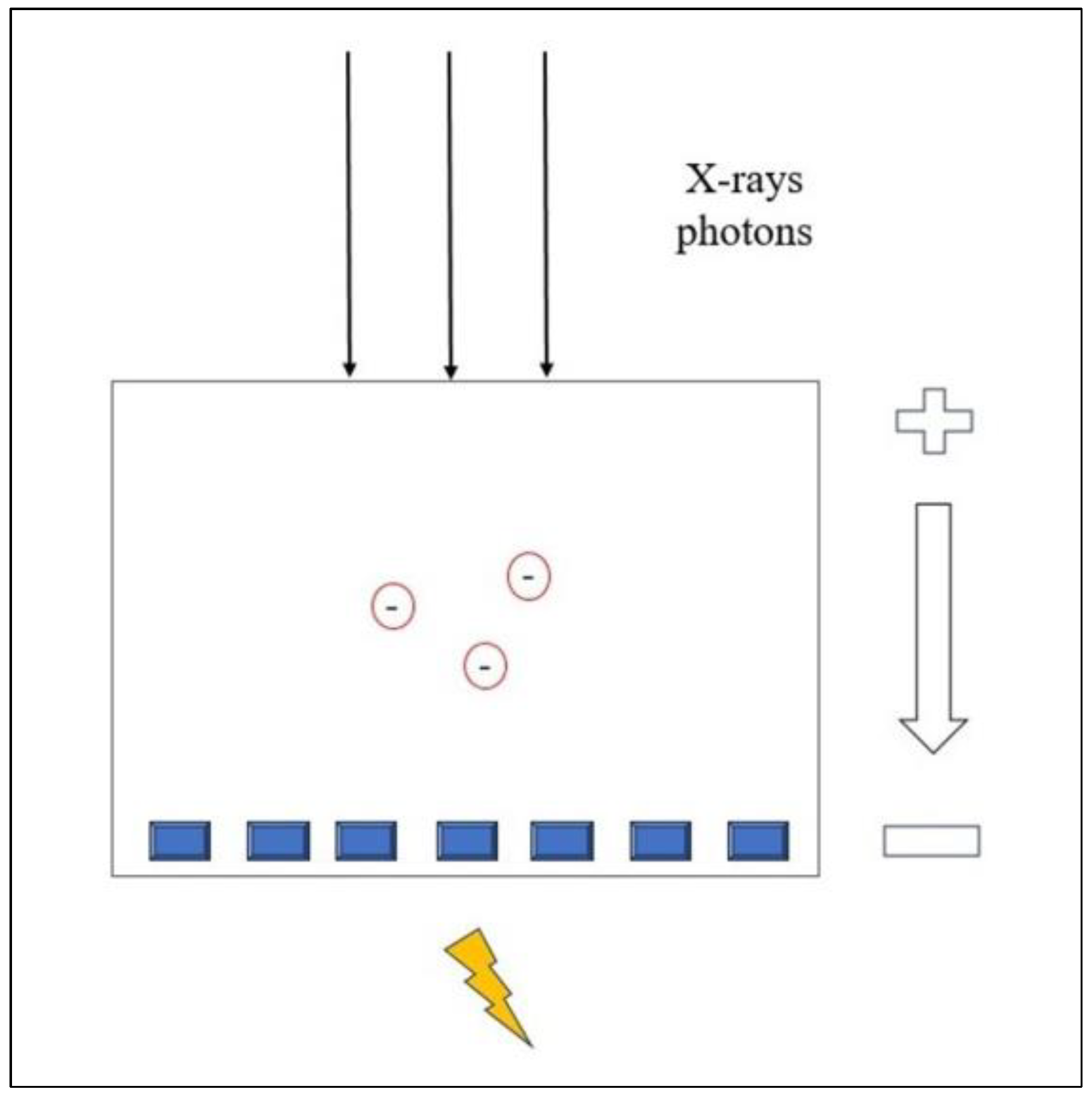
Figure 2.
Comparison of image quality of an abdominal aortic aneurysm evaluated with photon-counting CT and standard contrast media (axial images). A thickened aortic wall related to aortitis (between solid and empty arrowhead) and intraluminal thrombotic stratification are visible at the level of the abdominal aortic aneurysm. High Resolution evaluation (Matrix 1024 x 1024) (a); Virtual Non-Contrast VCN (b); Iodine Map (c); 55keV reconstruction (d); Pure Lumen reconstruction (e); Spectral Dual Energy Reconstruction (f).
Figure 2.
Comparison of image quality of an abdominal aortic aneurysm evaluated with photon-counting CT and standard contrast media (axial images). A thickened aortic wall related to aortitis (between solid and empty arrowhead) and intraluminal thrombotic stratification are visible at the level of the abdominal aortic aneurysm. High Resolution evaluation (Matrix 1024 x 1024) (a); Virtual Non-Contrast VCN (b); Iodine Map (c); 55keV reconstruction (d); Pure Lumen reconstruction (e); Spectral Dual Energy Reconstruction (f).
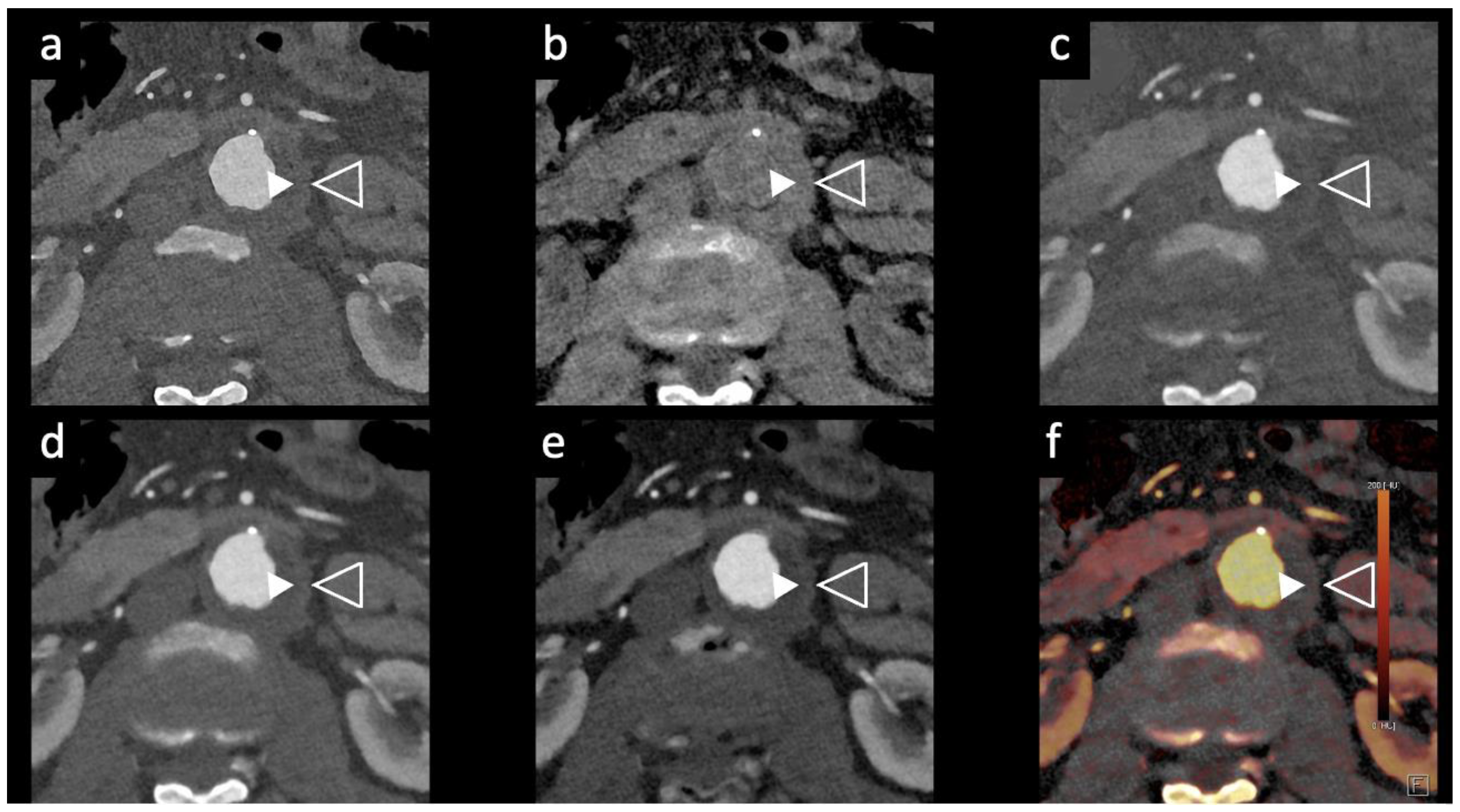
Figure 3.
Comparison of image quality with photon-counting CT and standard contrast media. Abdominal aortic lumen with wall calcification axial images. High Resolution images (Matrix 1024 x 1024) with different reconstruction kernels (window level W2000, C700): 40keV Kernel Bv48, Q4 (a); 55keV Kernel Bv48, Q4 (b); 55keV Kernel Bv68, Q4 (c); 70keV Kernel Bv48, Q4 (d); Iodine map reconstruction, kernel Bv40, Q4 (e); Virtual Non-Contrast VCN reconstruction (f); 3D-Cinematic Rendering of the abdominal aorta (g).
Figure 3.
Comparison of image quality with photon-counting CT and standard contrast media. Abdominal aortic lumen with wall calcification axial images. High Resolution images (Matrix 1024 x 1024) with different reconstruction kernels (window level W2000, C700): 40keV Kernel Bv48, Q4 (a); 55keV Kernel Bv48, Q4 (b); 55keV Kernel Bv68, Q4 (c); 70keV Kernel Bv48, Q4 (d); Iodine map reconstruction, kernel Bv40, Q4 (e); Virtual Non-Contrast VCN reconstruction (f); 3D-Cinematic Rendering of the abdominal aorta (g).
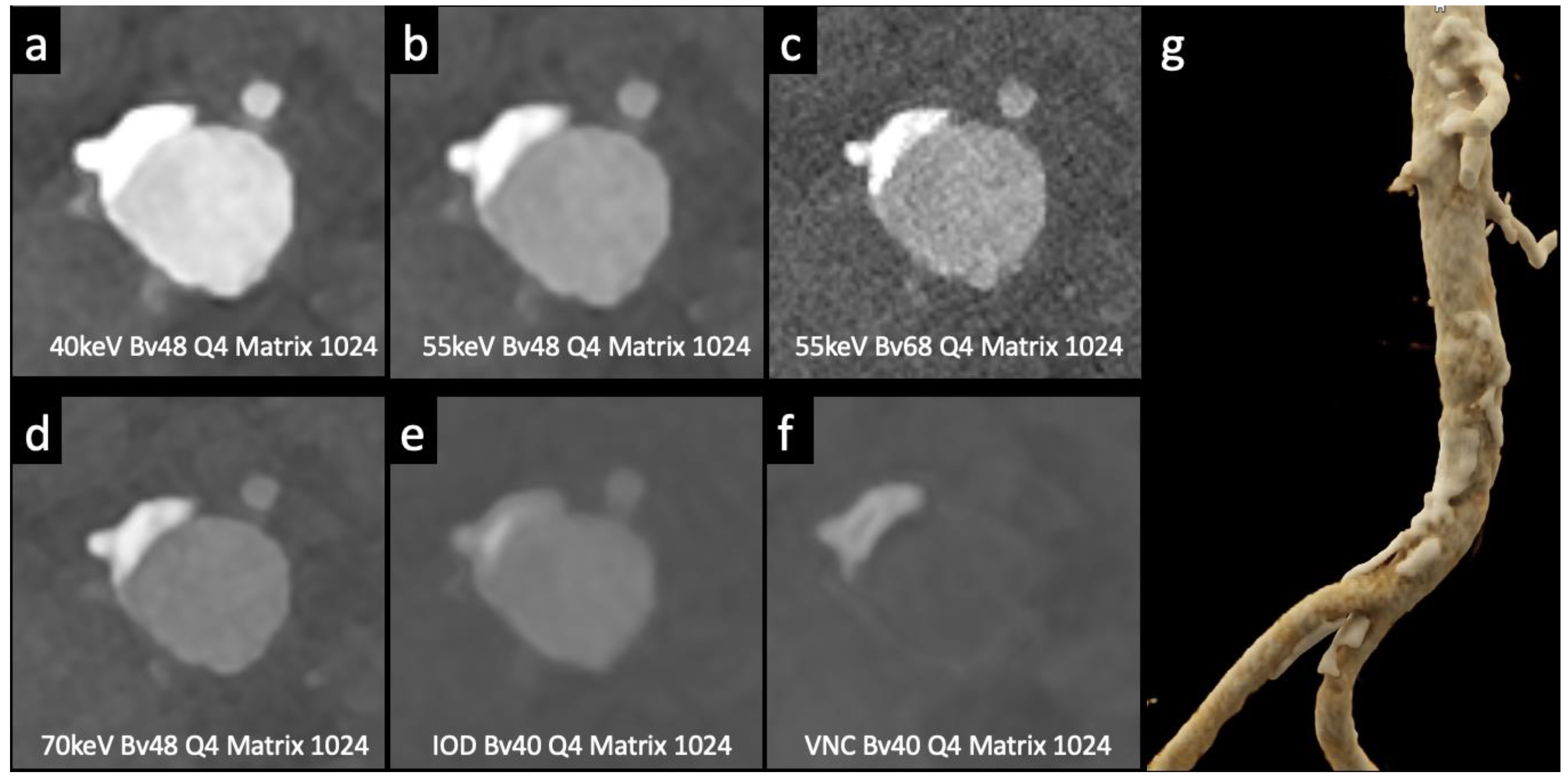
Figure 4.
Comparison of image quality with photon-counting CT and standard contrast media. Abdominal aortic lumen with wall calcification coronal images. High Resolution images (Matrix 1024 x 1024) with different reconstruction kernels (window level W2000, C700): 40keV Kernel Bv48, Q4 (a); 55keV Kernel Bv48, Q4 (b); 55keV Kernel Bv68, Q4 (c). 70keV Kernel Bv48, Q4 (d); Iodine map reconstruction, kernel Bv40, Q4 (e); Virtual Non Contrast VCN reconstruction (f).
Figure 4.
Comparison of image quality with photon-counting CT and standard contrast media. Abdominal aortic lumen with wall calcification coronal images. High Resolution images (Matrix 1024 x 1024) with different reconstruction kernels (window level W2000, C700): 40keV Kernel Bv48, Q4 (a); 55keV Kernel Bv48, Q4 (b); 55keV Kernel Bv68, Q4 (c). 70keV Kernel Bv48, Q4 (d); Iodine map reconstruction, kernel Bv40, Q4 (e); Virtual Non Contrast VCN reconstruction (f).
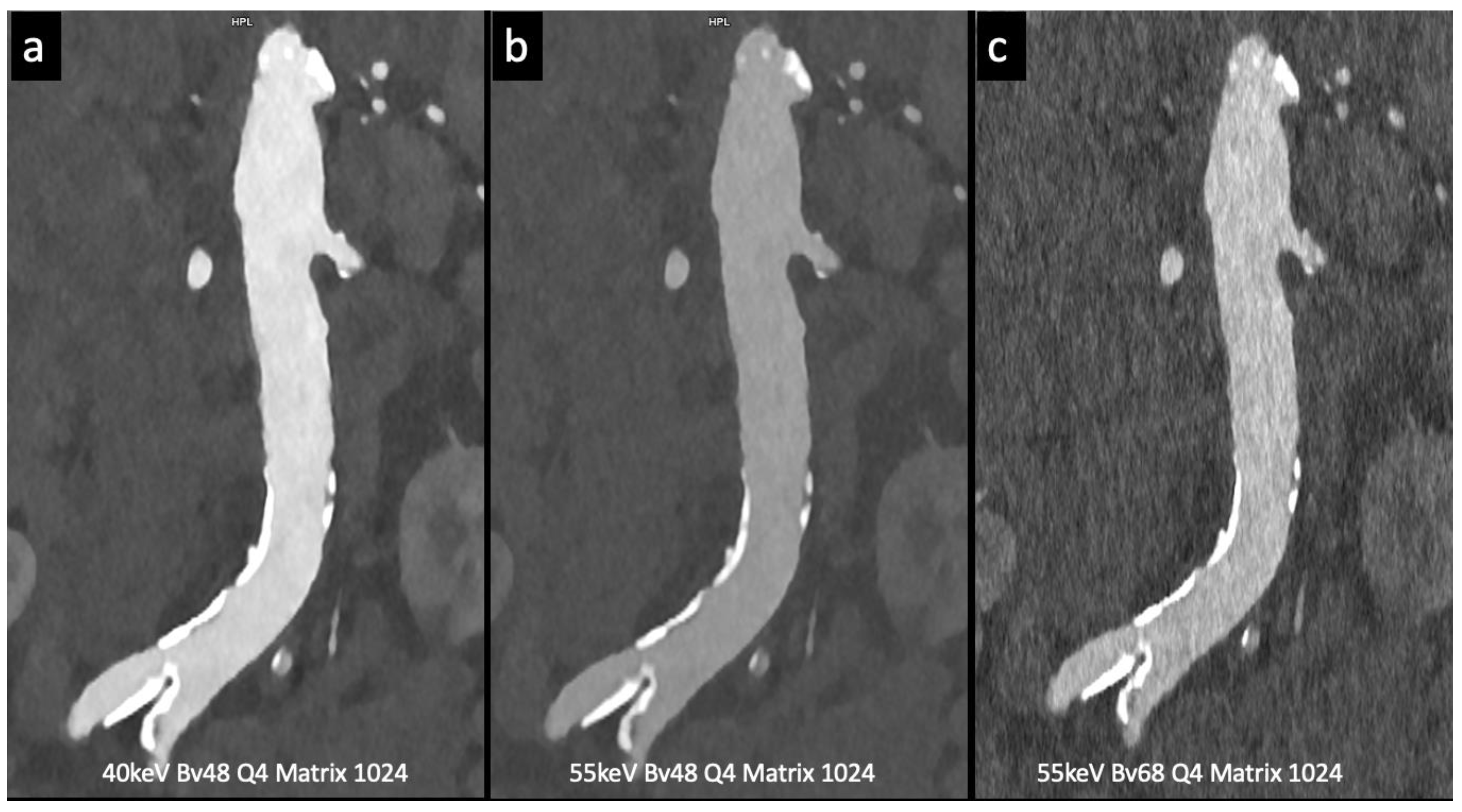
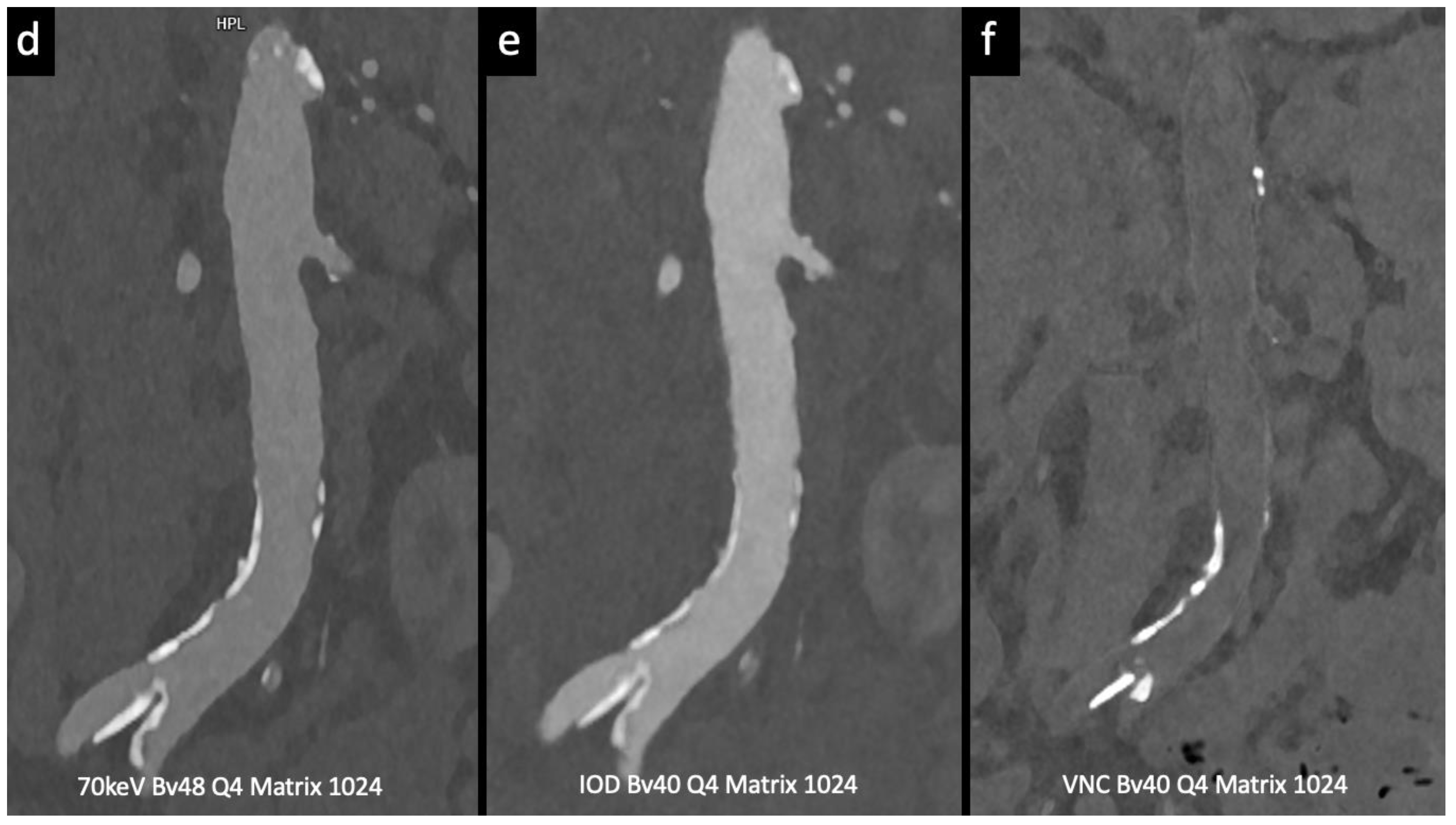
Figure 5.
aortic angiographic evaluation of the abdominal aortic aneurysm evaluated with photon-counting CT and standard contrast media (the same example of Figure 1, coronal view). 3D-Volume Rendering representation (a); High Resolution coronal evaluation, 55keV, Kernel Bv68 Q4 Matrix 1024 (b); Spectral Dual Energy coronal Reconstruction (c).
Figure 5.
aortic angiographic evaluation of the abdominal aortic aneurysm evaluated with photon-counting CT and standard contrast media (the same example of Figure 1, coronal view). 3D-Volume Rendering representation (a); High Resolution coronal evaluation, 55keV, Kernel Bv68 Q4 Matrix 1024 (b); Spectral Dual Energy coronal Reconstruction (c).
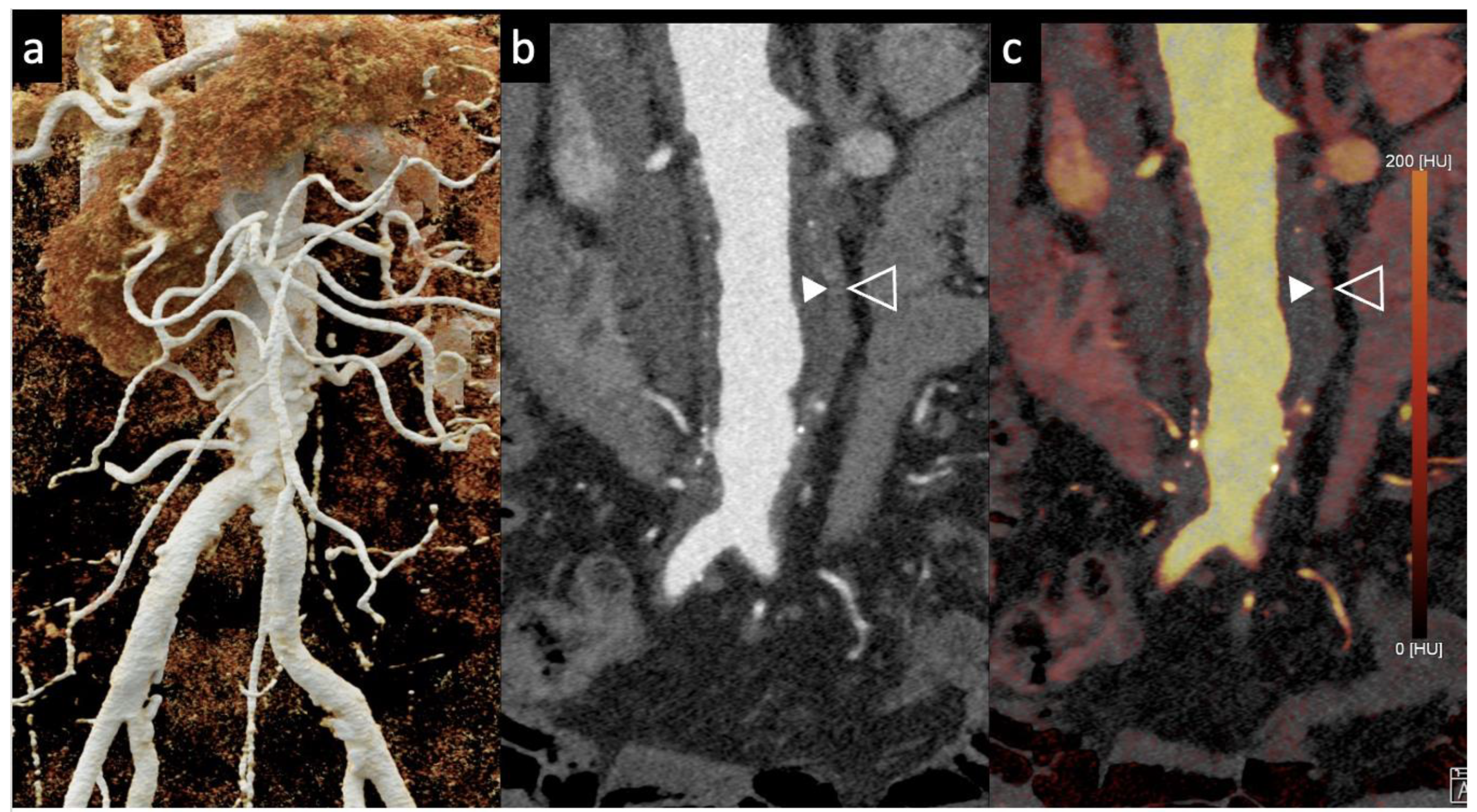

Table 1.
Study selected from our research. Abbreviations: PCCT, PCCT; VNI = Virtual Non-iodine; TNC =True Non-contrast; CTA, computed tomography angiography; AAA, abdominal aortic aneurysm ; EID = Energy-Integrating Detector; CNR = Contrast to Noise Ratio ; ATVS = Automatic Tube Voltage Selection.
Table 1.
Study selected from our research. Abbreviations: PCCT, PCCT; VNI = Virtual Non-iodine; TNC =True Non-contrast; CTA, computed tomography angiography; AAA, abdominal aortic aneurysm ; EID = Energy-Integrating Detector; CNR = Contrast to Noise Ratio ; ATVS = Automatic Tube Voltage Selection.
| Endoleaks detection |
Gomollon et al. Investigative Radiology 2023 [6] |
Retrospective study (110 patients) |
|
|
Cosset et al. Diagnostic and Interventional Imaging 2023 [8] |
Phantom experimental study |
|
|
|
Dangelmaier et al. European Radiology 2018 [8] |
Phantom experimental study |
|
|
| Contrast Volume Reduction |
Higashigaito et al. Radiology Cardiothoracic Imaging 2023[9] |
Prospective study (100 patients) |
|
|
Rau et al. Radiology Case Reports 2023[10] |
Case report (follow-up imaging of AAA) |
|
|
| Radiation Dose Reduction |
Decker et al. Diagnostics 2022[11] |
Retrospective study (20 patients) after EVAR |
|
|
Euler et al. Investigative Radiology 2022[12] |
Prospective study (40 patients) |
|
Table 2.
Endoleak classification.
| Type 1 Endoleak (EL1) | 5-10% | EL1a: leakage from proximal attachment site of the graft[29] |
| EL1b: leakage from distal attachment site of the graft | ||
| EL1c: leakage from back filling due to an incomplete common iliac arterial occlusion | ||
| Type 2 Endoleak (EL2) | 10-40% | Backflow of collateral arteries into the aneurysm sac [30] |
| Type 3 Endoleak (EL3) | 2-4% | Stent graft component separation or EL due to a fabric tear [31] |
| Type 4 Endoleak (EL4) | Almost never seen with new generation grafts | Leakage due to porosity of the graft[32] |
| Type 5 Endoleak (EL5),also known as “endotension” | Diagnosis of exclusion | Expansion of the sac without an apparent EL on imaging33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



