
Submitted:
25 October 2023
Posted:
26 October 2023
You are already at the latest version
Abstract
The success rate of extracorporeal shock wave lithotripsy (ESWL) is influenced by various factors, including stone density, which is determined through computed tomography scans in Hounsfield Units (HU). Materials and method: This retrospective single-center study was conducted in King Fahad hospital. Sixty-seven adult patients with renal and ureteric stones were selected randomly and enrolled in the study. Their age ranged from 20 to 69 years. The patients were examined with non-contrast enhancement (NCCT) to assess the HU of stones, consequently, treated with ESWL. Results: of the 67 patients, 37.3% of the stones were completely fragmented, while 62.7% were partially fragmented. HU, location of the stone, a multiplicity of the stone, and patient age were significant factors contributing to stone fragility (p-values< 0.05). The HU has a positive significant linear correlation with serum calcium (r= .28, p-value=.036), while serum acid has a negative correlation (r=-.55, p-value= < .001). Thus, the probability of calcium-containing stones formation increased with increased HU. In contrast, uric acid stone formation is likely to develop with decreasing HU with serum uric acid. Renal stones in patients with diabetes mellitus and hypertension were not completely fragmented compared to those without clinical history. Conclusion: Mean HU, location of the stone, laterality, status of stone, and the number of ESWL sessions were the most significant factors affecting stone fragility. CT attenuation values can predict the composition of stones from serum calcium and uric acid examinations. Hypertension and Diabetes mellitus are risk factors for renal stone fragmentation.
Keywords:
fragmentation
; CT number
; renal stones
; ESWL
; serum calcium
; uric acid
1. Introduction
Extracorporeal shock wave lithotripsy (ESWL) is an effective procedure for treating renal and ureteral stones [1]. Most renal and upper ureteric stones still respond well to extracorporeal shock wave lithotripsy (ESWL), particularly those with a size range of 10–20 mm [2]. This therapeutic approach has a 60–90% success rate across several series [3,4,5]. However, a number of parameters, such as the size, location, composition, and existence of obstruction or infection, affect how well the ESWL treatment works [4,5]. Cysteine and calcium oxalate monohydrate stones are typically resistant to ESWL. Understanding stone composition is crucial for ESWL treatment, but doing so before treatment is complex. According to specific investigations, urinary stone HU levels may be able to predict the composition of the stones [6,7,8,9].
The use of spiral/helical non-contrast computed tomography (CT) in individuals with urinary system stones (CT) has grown recently. The density of the stone or structure of interest is connected to Hounsfield units (HU), a parameter produced from standard CT [10]. CT is considered the gold standard for evaluating stones before surgery and affects the decision of the surgical plan [11]. The density of renal calculi is determined by Hounsfield Units (HU), which also identify high-density stones that should not be subjected to shockwave lithotripsy (SWL). [12] Therefore, it’s crucial to identify the patients who would benefit from ESWL before starting treatment. Stone size, location, diversity, and Hounsfield Unit (HU) values evaluated by non-contrast computed tomography (NCCT) are just a few of the variables that have been reported to predict the success of ESWL [2,13].
This study aims to determine the outcome of ESWL of urolithiasis using CT attenuation (HU) for the prediction of stone fragmentation and to identify the associated risk factors such as stone size, location, and laboratory investigations (serum calcium and serum uric acid)..
2. Materials and Methods
This study is a retrospective type searched on a database of patients treated for renal and ureteral stones from March to December 2021 and evaluated 67 patients (56 males and 11 females) who were examined with no-contrast CT (NCCT) before ESWL at King Fahd Hospital. They had conducted more than one session of ESWL. The outcome of ESWL was determined in terms of complete or partial fragmentation of renal stones regardless of stone-free status. Inclusion criteria were adults ≥ 20 years with multiple or solitary renal or ureteral stones. Exclusion criteria were pregnancy, febrile urinary tract infections (UTIs), using anticoagulant treatment, and those who are lesser than 20 years old. Patients with thyroid diseases were excluded from the study
2.1. CT Renal Protocol
NCCT examination protocol of the renal system was applied using General Electric GE Pride Speed to assess the renal stones and estimate HU values. The following patients’ characteristics were considered: patient age, sex, stone laterality, stone length, stone side, mean and peak HU values, and stone position. The CT renal protocol was performed following the standard CT renal protocol. Scout was first taken in AP to map the CT volume’s precise distance. From the level of the diaphragm down to just below the symphysis pubis, a single volume of CT series is collected. The patient was prone with his feet first. The kV was 120, the mAs was 50, the scan time took 10 to 12 seconds, and the delay with one breath hold was 4 seconds. The slice thickness was 2 mm, and the gantry was not tilted. The chosen Kernel was standard for soft tissue. The CT images were delivered to a dedicated workstation, a photo archiving computer system (PACS). The images are observed using curved multiplanar and 3D volume rendering techniques and axial, coronal, sagittal, and oblique reconstruction. Techniques with maximum intensity and medium volume are frequently employed. Two radiologists reviewed the images, discussed the findings with the urologist, and agreed on the results.
2.2. Statistical Analysis
The data were collected using a designed data collecting sheet and analyzed using IBM SPSS for Windows, version 23 (IBM Corp., Armonk, NY, USA). Due to missing data, several cases were omitted from the stud. Most of the missing data were related to the patient’s laboratory investigations. The study variables were categorical and quantitative. Descriptive statistics such as percentages and frequency distribution were used to describe the qualitative variables. Linear regression and Pearson correlation statistical tests were used to find the relationship between CT number with serum Calcium oxalate and uric acid. Binary logistic regression analyses were conducted to estimate the associated risk factors and to find factors related to the fragmentation of renal stones, such as HU, stone location, stone length, and the number of ESWL sessions. The result of the modeling process also incorporated all relevant components connected to the outcome variable, such as age, sex, and clinical history.
In contrast to the chosen referent, the crude and adjusted odds ratios (OR) and their respective 95% confidence intervals (CI) were provided to assess the contribution of each factor in the outcome of stone fragmentation.
3. Results
A total of 67 patients were retrospectively reviewed to assess the stone fragmentation. Patient characteristics are shown in Table 1. 68.7% of the participants had a history of diabetes mellitus, while 28.4% had primary hypertension (Table 1). The prevalence of renal stones was higher in males 56(83.6%) than in females 11(16.4%), and higher in the age groups of 41-50 years (38.8%) and 31-40 years (20.9%), respectively.
Table 2 summarizes the status of renal stones treated with ESWL with a degree of hydronephrosis. Most of the stones were single (67.2%), 44.8% of the stones were located in the calyces of the kidney, and 35.8% were in the upper ureter. The location in the lower and mid-ureter was less frequent. Most treated stones were found in the left and right kidneys (40.3%) (37.3%).
The outcome of stone ESWL treatment was 37.3% completely fragmented and 62.7 partially fragmented (Figure 1). The mean CT attenuation number was significantly higher in fragmented stones than in completely fragmented ones (978.79 vs. 841.95, p-value =.03), as shown in Figure 2. These findings indicate that CT attenuation numbers govern successful treatment by ESWL since attenuation values below 841.95 Hounsfield (HU) may predict success, and values ≥ 978.79 HU may lead to failure of the ESWL.
There was a significant linear relationship of CT number with serum calcium oxalate and uric acid values (P-values = .036, and < .001) (Table 3). The Correlation with serum calcium was positive (r=.28). At the same time, it was negative with serum uric acid (r= –.51). Since there was a positive correlation between the variables mentioned above, we derived a regression equation for predicting the type of the stone with CT attenuation values and serum calcium and uric acid, with minimal error (Figure 3 and Table 3). The linear regression equation revealed that an increase in the CT number of a stone was associated with an increased likelihood of exhibiting calcium stones. In contrast, a decreased CT number was associated with a reduced probability of predicting uric acid stones.
The outcome of ESWL treatment (stone fragmentation) was distributed according to stone location and kidney side regardless of stone clearance status. Twenty-two stones in the calyces and renal pelvis were partially fragmented, and only 8 were completely fragmented. Ten stones in the upper ureter were completely fragmented, and 14 were partially fragmented (Table 4). It was shown 19 cases of stones in the right kidney were partially fragmented, while 6 were completely fragmented. The left kidney shows 16 partially fragmented and 11 completely fragmented. The outcome in the right kidney is higher than in the left kidney.
The factors that predict stone fragmentation were summarized in Table 5 using binary logistic regression. Aging is a significant factor for stone fragmentation (AOR=1.29, 95% CI= 1.0–1.66). Males had 6.280 increased Odds compared to males to respond for stone fragmentation (OR= 6.280, 95% CI= .202–195.027). Stones in the right kidney had 3.619 increased Odds of being fragmented compared to stones located bilaterally (COR =3.619, 95% CI= .921–14.214), while stones in the left kidney had 1.662 increased Odds compared to those found in bilateral kidneys (COR -1.662, 95% CI =.466–5.932). The mean of stone length is a significant factor for stone fragmentation (AOR=1.037, 95% CI=.968–1.11). On the other hand, the site of the stone is also a significant factor contributing to fragmentation (AOR=.142, 95% CI = .032–.626).
The HU is an essential factor associated with stone fragmentation. It had 1.003 increased Odds compared to stones with lesser values of HU (AOR= 1.003, 95% CI= 1.000–1.006). Regarding the number of ESWL treatment sessions, patients exposed to more than one session are more likely to respond to the fragmentation process than those with fewer sessions (AOR= .121, AOR = .023–.646).
Considering the clinical history of the patients, the results revealed that diabetic patients had 1.406 increased Odds compared to non-diabetic ones to respond for stone fragmentation (OR= 1.406, 95% CI= (.489–4.043), while hypertensive patients had 1.8 increased Odds compared to non-diabetic ones to respond for stone fragmentation (OR= 1.8, 95% CI= (.713–3.208). The stones in people with diabetes are 1.406 times more partially fragmented than in non-diabetic ones, in whom stones are easily fragmented.
4. Discussion
CT is the most sensitive and reliable imaging technique for detecting urinary calculi. It can assess small radiolucent stones and other illnesses affecting the urinary system or other organs. Numerous studies have attempted to use factors like HU, Skin-to-stone distance, SSD, and stone size to predict the composition and fragility of stones with CT [14,15]. The best parameter cutoff values that can forecast stone clearance are of clinical importance, particularly the cutoff values for the most potent predictive factors, since they may be helpful in selecting a treatment plan. We studied several factors that affected the fragility of renal stones. Laterality of the stone, status of the stone, stone location, and clinical history were the most significant factors predicting the fragmentation of renal stones. This study is different from others that we included the clinical history, such as diabetes and hypertension, as risk factors for stone fragmentation in addition to other factors such as stone location, stone length, stone status (single or multiple), HU, gender, and age.
The study showed that the laterality of the stone, status of the stone, and stone location were significant factors affecting the fragility of renal stones by ESWL. According to previous studies [16,17], the location of the stone is a reliable indicator of ESWL outcome. Our investigation examined the location of renal and ureter stones analysis on the calyces or renal pelvis, or the proximal, middle, and lower ureters., whereas many studies focused on the location of the kidney only. It was found that laterality is a significant factor in stone fragility. Thus, it was found that stones on the right or left kidney were more likely to respond to fragmentation than those located on both kidneys. To our knowledge, this finding has yet to be reported in a study.
The study found stone status, multiple or single, was a significant predictor for ESWL outcome. In our analysis, we found numerous stones more difficult to fragment than a single stone. In agreement with this finding, Ozgor et al. reported that after a single session of laser lithotripsy, patients with solitary kidney stones had a considerably higher stone-free status. [18].
The study showed that the stone length was not a significant predicting factor for stone fragmentation, although the stone volume was considered an essential factor in the literature. In a study of individuals with solitary upper urinary tract calculi, Bandi et al. reported that stone volume was the best predictor of ESWL outcome. However, they also detected significant variations in axial diameters. [19]. According to Nakasato et al., large stones frequently stay removed. [20] Large stones ordinary have longer diameters than small ones. Thus, they remained unchanged. Therefore, there are better ways to determine the ESWL outcome than classifying stones by length or size.
Regarding the CT number of the renal stone, the study found a significant association with the fragmentation process, either partially or entirely. Stones with higher CT numbers are partially fragmented than those with low CT numbers, which are completely fragmented. Our study found that complete fragmentation occurs in stones with HU of 841.95 and 978.79 HU for the partial, fragmented ones. Several studies have reported the impact of HU on stone fragmentation. Wang et al. provided cutoff values of stone density > 900 HU [21], Park et al. reported that an 863 HU threshold was the most significant predictor of ESWL outcome among the factors examined [22], and Ouzaid et al. reported a 970 HU threshold [12]. Therefore, CT attenuation values can help distinguish between stones that are expected to fragment quickly on ESWL and stones that would need more shock waves to disintegrate or not fragment on ESWL.
Regarding the prediction of stone composition, the present study revealed a significant linear relationship between CT number with serum Calcium and uric acid examinations. A significant linear correlation was existed between CT number, serum calcium, and uric acid. It is important to note that calcium nephrolithiasis can occur in people with hypercalcemia/hypercalciuria and those with normocalcemia/normocalciuria, even though calcium makes up the majority of crystalline components of kidney stones in 80% of instances. [23]. The study found that serum calcium values in patients with renal stones increased the CT number, yielding a statistically positive linear correlation. In literature, it was reported that hypercalcemia and hypercalciuria produce calcium nephrolithiasis [24,25]. Therefore, increasing CT attenuation values are associated with serum calcium, thus predicting calcium stones.
On the other hand, we found that serum uric acid decreases the CT attenuation values. In agreement with this finding, a study reported that uric acid stones exhibit no change in CT number [26]. Therefore, decreasing attenuation values predict uric acid stones as they have lower attenuation values compared to stones made of calcium salts. The relationship of serum calcium and uric acid with the HU of the stones needs a comprehensive investigation to predict the type of renal stones.
Epidemiologically, previous studies reported that diabetes and hypertension are risk factors for the formation of stones, although they did not affect the number of stones. [27, 28]. The present study found a relationship between stone fragility, diabetes, and hypertension. It was found that stones in diabetic and hypertensive are not easily fragmented compared to those of non-diabetics and non-hypertensive whose stones are entirely fragmented. No studies in the literature verified the impact of diabetes mellitus and hypertension on the fragmentation of renal stones. This finding needs comprehensive investigation.
The study found significant and minor limitations, as the sample size is not large enough, which may yield some statistical errors and bias. Secondly, no other technique was utilized to determine the composition of the stone, although chemical analysis is performed in the laboratory evaluation of extracted stones. Further studies with larger sample are recommended to confirm these findings.
5. Conclusions
Many factors influence the outcome of ESWL for renal stone fragmentation. Mean HU, location of the stone, laterality, status of stone, and the number of ESWL sessions were the most significant factors affecting stone fragility. CT attenuation values can predict the composition of stones from serum calcium and uric acid examinations. Diabetes mellitus and hypertension are risk factors for renal stone fragmentation.
Author Contributions
Conceptualization, A.S. A and M.G.; methodology, A.G.; software, M.A.S; validation, X.X., Y.Y. and Z.Z.; formal analysis, X.X.; investigation, X.X.; resources, X.X.; data curation, H.I.A and A.Q; writing—original draft preparation, M.G.; writing—review and editing, A.Q.; visualization, K.M.A; supervision, M.G.; project administration, A.S.A; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the general directorate of health affairs in Madinah approved the study and provided the ethically approved number (IRB 19-2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting the reported results are available upon request from the corresponding author of the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lee, H.; Yang, Y.-H.; Lee, Y.-L.; Shen, J.-T.; Jang, M.-Y.; Shih, P.M.-C.; Wu, W.-J.; Chou, Y.; Juan, Y.-S. Noncontrast Computed Tomography Factors That Predict the Renal Stone Outcome after Shock Wave Lithotripsy. Clinical Imaging 2015, 39, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Joseph, P.; Mandal, A.K.; Singh, S.K.; Mandal, P.; Sankhwar, S.N.; Sharma, S.K. Computerized Tomography Attenuation Value of Renal Calculus: Can It Predict Successful Fragmentation of the Calculus by Extracorporeal Shock Wave Lithotripsy? A Preliminary Study. Journal of Urology 2002, 167, 1968–1971. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.Y.; Kang, D.H.; Cho, K.S.; Jeong, W.S.; Jung, H.D.; Kwon, J.K.; Lee, S.H.; Lee, J.Y. Comparison of Stone-Free Rates Following Shock Wave Lithotripsy, Percutaneous Nephrolithotomy, and Retrograde Intrarenal Surgery for Treatment of Renal Stones: A Systematic Review and Network Meta-Analysis. PLoS ONE 2019, 14, e0211316. [Google Scholar] [CrossRef] [PubMed]
- Srisubat, A.; Potisat, S.; Lojanapiwat, B.; Setthawong, V.; Laopaiboon, M. Extracorporeal Shock Wave Lithotripsy (ESWL) for Kidney Stones. In Cochrane Database of Systematic Reviews; The Cochrane Collaboration, Ed.; John Wiley & Sons, Ltd: Chichester, UK, 2008; p. CD007044. [Google Scholar]
- D’Addessi, A.; Vittori, M.; Racioppi, M.; Pinto, F.; Sacco, E.; Bassi, P. Complications of Extracorporeal Shock Wave Lithotripsy for Urinary Stones: To Know and to Manage Them—A Review. The Scientific World Journal 2012, 2012, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.-F.; Siu, D.Y.-W.; Wong, A.; Goggins, W.; Chan, E.S.; Wong, K.-T. Development of a Scoring System From Noncontrast Computerized Tomography Measurements to Improve the Selection of Upper Ureteral Stone for Extracorporeal Shock Wave Lithotripsy. Journal of Urology 2009, 181, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; Haleblian, G.; Zabbo, A.; Pareek, G. Hounsfield Units on Computed Tomography Predict Calcium Stone Subtype Composition. Urol Int 2009, 83, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Deveci, S.; CoŞkun, M.; Tekin, M.İ.; PeŞkircioglu, L.; Tarhan, N.Ç.; ÖzkardeŞ, H. Spiral Computed Tomography: Role in Determination of Chemical Compositions of Pure and Mixed Urinary Stones—an in Vitro Study. Urology 2004, 64, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Mostafavi, M.R.; Ernst, R.D.; Saltzman, B. Accurate Determination of Chemical Composition of Urinary Calculi by Spiral Computerized Tomography. J Urol 1998, 159, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, A.; Silbergleit, A.; Olson, R.; Cotant, M. Urolithiasis: The Influence of Stone Size on Management. Nat Rev Urol 2007, 4, 570–573. [Google Scholar] [CrossRef]
- Türk, C.; Petřík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU Guidelines on Diagnosis and Conservative Management of Urolithiasis. European Urology 2016, 69, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Ouzaid, I.; Al-qahtani, S.; Dominique, S.; Hupertan, V.; Fernandez, P.; Hermieu, J.-F.; Delmas, V.; Ravery, V. A 970 Hounsfield Units (HU) Threshold of Kidney Stone Density on Non-Contrast Computed Tomography (NCCT) Improves Patients’ Selection for Extracorporeal Shockwave Lithotripsy (ESWL): Evidence from a Prospective Study: NCCT ATTENUATION VALUES OF URINARY CALCULI HELP TO PREDICT ESWL TREATMENT OUTCOME. BJU International 2012, 110, E438–E442. [Google Scholar] [CrossRef] [PubMed]
- Weld, K.J.; Montiglio, C.; Morris, M.S.; Bush, A.C.; Cespedes, R.D. Shock Wave Lithotripsy Success for Renal Stones Based on Patient and Stone Computed Tomography Characteristics. Urology 2007, 70, 1043–1046. [Google Scholar] [CrossRef] [PubMed]
- Miah, T.; Kamat, D. Pediatric Nephrolithiasis: A Review. Pediatr Ann 2017, 46. [Google Scholar] [CrossRef] [PubMed]
- Roberson, N.P.; Dillman, J.R.; Reddy, P.O.; DeFoor, W.; Trout, A.T. Ultrasound versus Computed Tomography for the Detection of Ureteral Calculi in the Pediatric Population: A Clinical Effectiveness Study. Abdom Radiol 2019, 44, 1858–1866. [Google Scholar] [CrossRef] [PubMed]
- Pearle, M.S.; Lingeman, J.E.; Leveillee, R.; Kuo, R.; Preminger, G.M.; Nadler, R.B.; Macaluso, J.; Monga, M.; Kumar, U.; Dushinski, J.; et al. PROSPECTIVE, RANDOMIZED TRIAL COMPARING SHOCK WAVE LITHOTRIPSY AND URETEROSCOPY FOR LOWER POLE CALICEAL CALCULI 1 CM OR LESS. Journal of Urology 2005, 173, 2005–2009. [Google Scholar] [CrossRef] [PubMed]
- Psihramis, K.E.; Jewett, M.A.S.; Bombardier, C.; Caron, D.; Ryan, M. The Toronto Lithotripsy Associates Lithostar Extracorporeal Shock Wave Lithotripsy: The First 1,000 Patients. Journal of Urology 1992, 147, 1006–1009. [Google Scholar] [CrossRef] [PubMed]
- Ozgor, F.; Kucuktopcu, O.; Ucpinar, B.; Gurbuz, Z.G.; Sarilar, O.; Berberoglu, A.Y.; Baykal, M.; Binbay, M. Is There a Difference between Presence of Single Stone and Multiple Stones in Flexible Ureterorenoscopy and Laser Lithotripsy for Renal Stone Burden <300mm2? Int. braz j urol. 2016, 42, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Bandi, G.; Meiners, R.J.; Pickhardt, P.J.; Nakada, S.Y. Stone Measurement by Volumetric Three-dimensional Computed Tomography for Predicting the Outcome after Extracorporeal Shock Wave Lithotripsy. BJU International 2009, 103, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Nakasato, T.; Morita, J.; Ogawa, Y. Evaluation of Hounsfield Units as a Predictive Factor for the Outcome of Extracorporeal Shock Wave Lithotripsy and Stone Composition. Urolithiasis 2015, 43, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-J.; Wong, Y.-C.; Chuang, C.-K.; Chu, S.-H.; Chen, C.-S.; See, L.-C.; Chiang, Y.-J. Predictions of Outcomes of Renal Stones after Extracorporeal Shock Wave Lithotripsy from Stone Characteristics Determined by Unenhanced Helical Computed Tomography: A Multivariate Analysis. Eur Radiol 2005, 15, 2238–2243. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.I.; Yu, J.H.; Sung, L.H.; Noh, C.H.; Chung, J.Y. Evaluation of Possible Predictive Variables for the Outcome of Shock Wave Lithotripsy of Renal Stones. Korean J Urol 2010, 51, 713. [Google Scholar] [CrossRef] [PubMed]
- Devuyst, O.; Pirson, Y. Genetics of Hypercalciuric Stone Forming Diseases. Kidney International 2007, 72, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Craven, B.L.; Passman, C.; Assimos, D.G. Hypercalcemic States Associated with Nephrolithiasis. Rev Urol 2008, 10, 218–226. [Google Scholar] [PubMed]
- Stechman, M.J.; Loh, N.Y.; Thakker, R.V. Genetics of Hypercalciuric Nephrolithiasis: Renal Stone Disease. Annals of the New York Academy of Sciences 2007, 1116, 461–484. [Google Scholar] [CrossRef]
- Wisenbaugh, E.S.; Paden, R.G.; Silva, A.C.; Humphreys, M.R. Dual-Energy vs Conventional Computed Tomography in Determining Stone Composition. Urology 2014, 83, 1243–1247. [Google Scholar] [CrossRef]
- Sancak, E.B.; Resorlu, M.; Akbas, A.; Gulpinar, M.T.; Arslan, M.; Resorlu, B. Do Hypertension, Diabetes Mellitus and Obesity Increase the Risk of Severity of Nephrolithiasis? Pak J Med Sci 1969, 31. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Huang, R.; Lin, B.; Hong, Y.; Lin, M.; He, X. Associations between Nephrolithiasis and Diabetes Mellitus, Hypertension and Gallstones: A Meta-analysis of Cohort Studies. Nephrology 2020, 25, 691–699. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Outcome of ESWL for renal stone fragmentation in the study population.

Figure 2.
Relationship between CT attenuation values and outcome of ESWL for renal stone fragmentation.
Figure 2.
Relationship between CT attenuation values and outcome of ESWL for renal stone fragmentation.
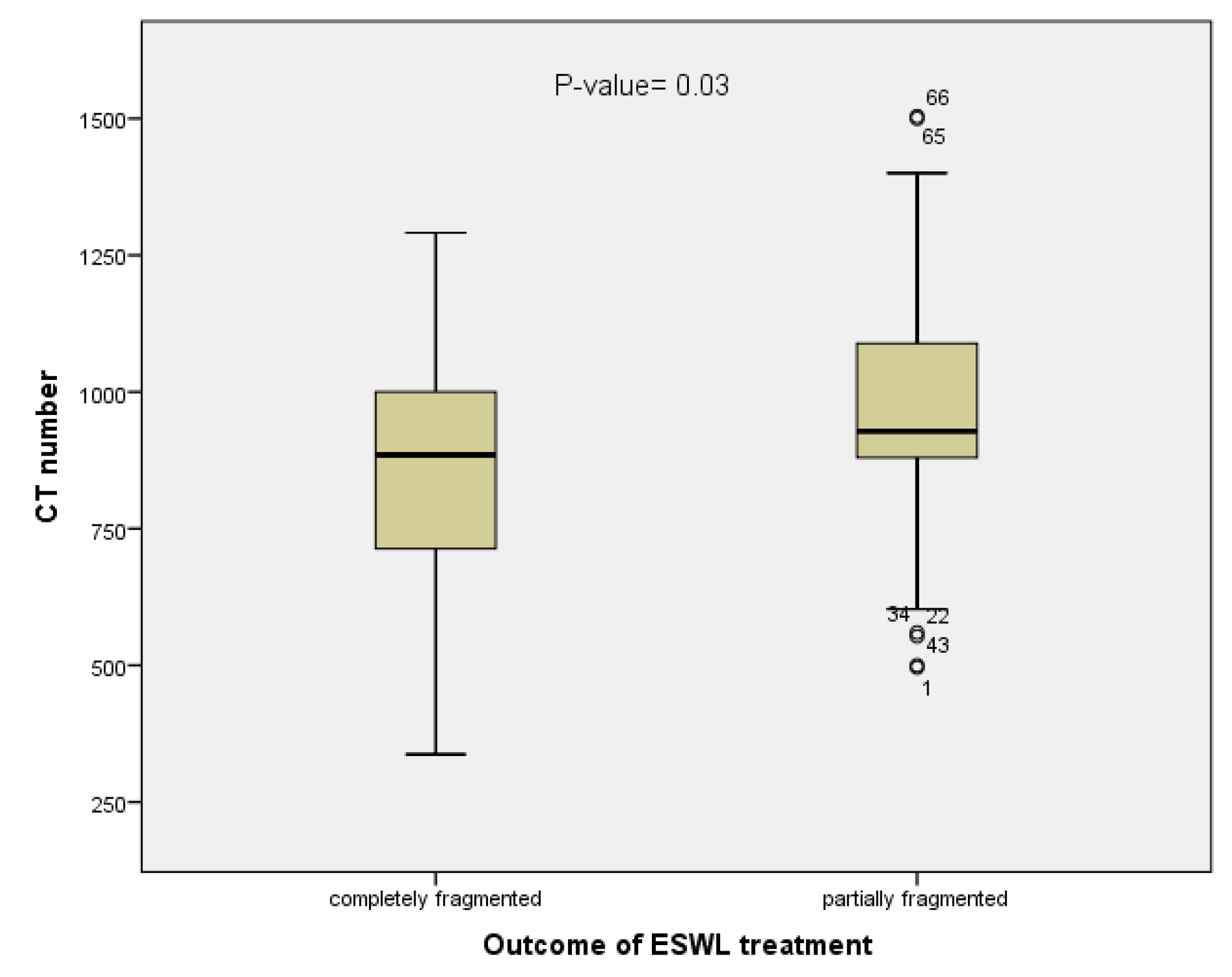
Figure 3.
Regression estimation curve shows positive relationship of CT number with serum calcium (a) and negative linear relation with serum uric acid (b).
Figure 3.
Regression estimation curve shows positive relationship of CT number with serum calcium (a) and negative linear relation with serum uric acid (b).
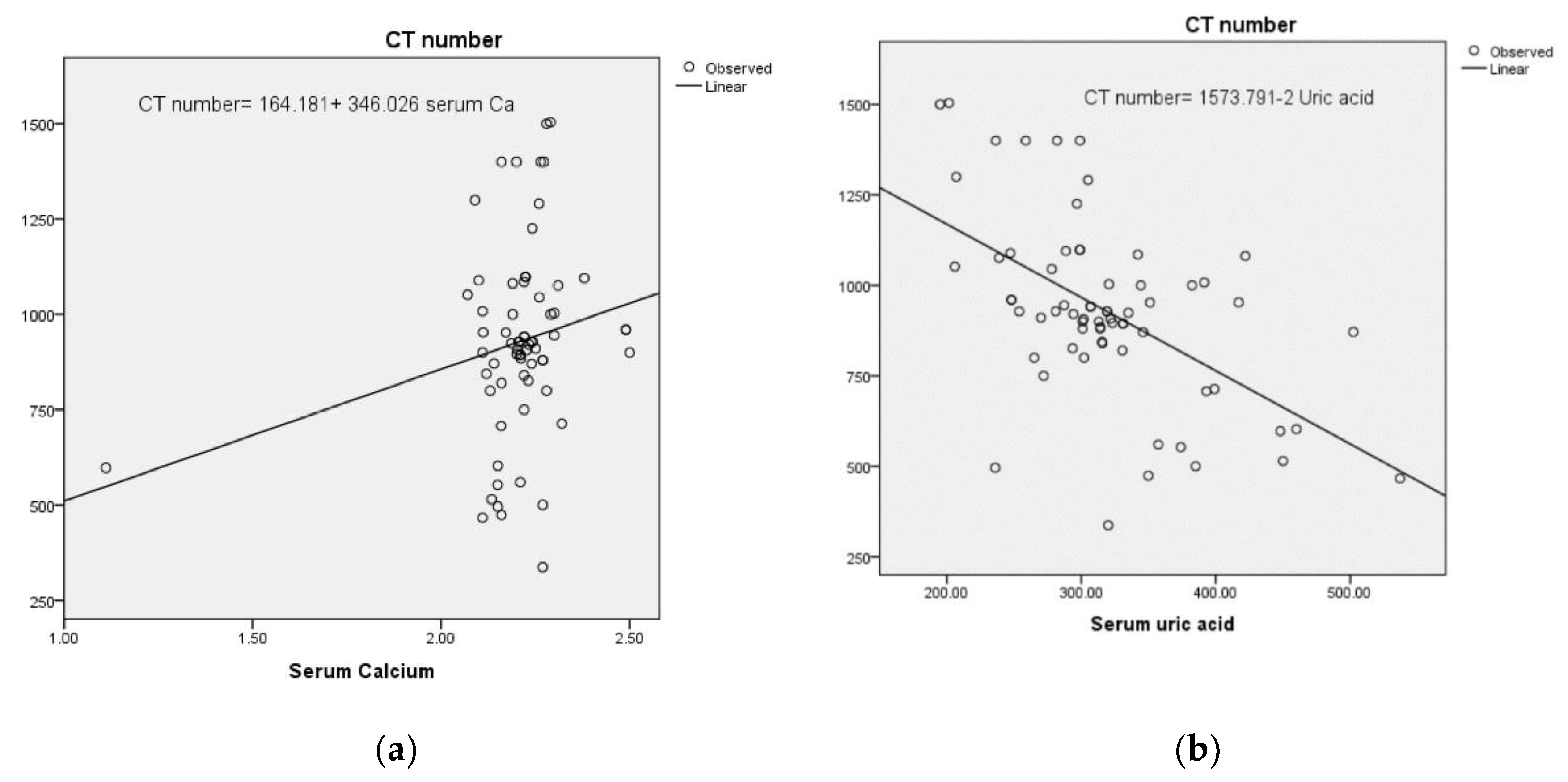

Table 1.
Sociodemographic characteristics of the study sample.
| Character | Frequency | Percent |
|---|---|---|
| Male | 56 | 83.6 |
| Female | 11 | 16.4 |
| Age groups (years) | ||
| 20-30 | 9 | 13.4 |
| 31-40 | 14 | 20.9 |
| 41-50 | 26 | 38.8 |
| 51-60 | 6 | 9.0 |
| > 60 | 12 | 17.9 |
| Mean age= 45.57±13.8 | ||
| Occupation | ||
| employer | 47 | 70.1 |
| non-employer | 20 | 29.9 |
| Diabetes mellitus | ||
| yes | 21 | 31.3 |
| no | 46 | 68.7 |
| Hypertension | ||
| yes | 19 | 28.4 |
| no | 48 | 71.6 |
Table 2.
Status of renal stones treated by ESWL.
| Status of renal stones | frequency | Percent % |
|---|---|---|
| single | 45 | 67.2 |
| multiple | 22 | 32.8 |
| Site of stone in the kidney | ||
| calyces of the kidney | 30 | 44.8 |
| upper ureter | 24 | 35.8 |
| lower ureter | 7 | 10.4 |
| mid-ureter | 6 | 9.0 |
| Hydronephrosis | ||
| No hydronephrosis | 16 | 23.9 |
| mild | 35 | 52.2 |
| moderate | 14 | 20.9 |
| Severe | 2 | 3.0 |
| Laterality | ||
| Right kidney | 25 | 37.3 |
| Left kidney | 27 | 40.3 |
| Bilateral | 15 | 22.4 |
| Right kidney | 25 | 37.3 |
Table 3.
Relationship of CT number with serum Calcium and uric acid examinations using Pearson correlation and linear regression tests.
Table 3.
Relationship of CT number with serum Calcium and uric acid examinations using Pearson correlation and linear regression tests.
| characteristic | Statistical Correlation | Serum Calcium (mmol/L) | Serum uric acid(µmol/L) | Regression equation |
|---|---|---|---|---|
| CT number | Pearson correlation | .28* | -.55** | acid |
| Significant 2-tailed | .036 | < .001 | ||
| Significant 2-tailed | .036 | < .001 | ||
* Correlation is significant at the 0.05 level (2-tailed). ** Correlation is significant at the 0.01 level (2-tailed).
Table 4.
Outcome of ESWL treatment according to stone status.
| Stone location | Stone (n) | Completely fragmented | Partially fragmented |
|---|---|---|---|
| calyces and renal pelvis | 30 | 8 | 22 |
| Upper ureter | 24 | 10 | 14 |
| Mid-ureter | 6 | 4 | 2 |
| Lower ureter | 7 | 3 | 4 |
| laterality | |||
| Right kidney | 25 | 6 | 19 |
| Left kidney | 27 | 11 | 16 |
| Bilateral | 15 | 8 | 7 |
| Status of stone | |||
| single | 45 | 18 | 27 |
| multiple | 22 | 7 | 22 |
Table 5.
Binary Logistic regression analysis for factors that predict stone fragmentation by ESWL.
| Variables | COR (95% CI) | AOR (95% CI) |
|---|---|---|
| Mean age(SD) | .993 (.958–1.029 | *1.29 (1.0–1.66) |
| Gender (n) | ||
| Males | 2.34 (.631–8.656) | 6.280 (.202–195.027) |
| Females | Ref | Ref |
| Clinical history | ||
| Diabetes mellitus | 1.406 (.489–4.043) | 3.981 (.343–46.240) |
| Hypertension | 1.8 (.713–3.208) | 4.354 (.436–1.488) |
| Laterality | ||
| Right kidney | 3.619 (.921–14.214) | 8.261 (.396–172.531) |
| Left kidney | 1.662 (.466–5.932) | *22.338 (1.003–497.552) |
| Bilateral | Ref | Ref |
| site of the stone within the kidney | .599 (.349–1.029) | *.24 (.079–.731) |
| Mean of HU (SD) | *1.002(1–1.005) | *1.003 (1.000–1.006) |
| Status of stone | ||
| multiple | 1.120 (.803–1.562) | *3.516 (.398–31.036) |
| single | Ref | - |
| Mean of stone length (SD) | 1.035 (.980–1.093) | 1.078 (.973–1.193) |
| Frequency of ESWL treatment sessions | .592 (.293–1.195) | *.121(.023–.646) |
*Significance > 0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



