
Submitted:
27 October 2023
Posted:
27 October 2023
You are already at the latest version
Abstract
This study aims to develop a novel retention method combining the retrievability of the screw retention method with the ideal occlusal table and the aesthetics capability of cement retention. Coping was developed to have lateral screw access allowing the screw to lock coping using lateral forces from screw tightening and friction between the tip of the screw and the sandblasted surface of an abutment. Sandblasting parameters varied based on particle size. Results show a positive correlation to surface roughness and indicate a positive correlation to retention force. The highest surface roughness and retention force result was shown by groups that were sandblasted using 686 μm of aluminum oxide. Experiment on the tightening strength of 48 subjects measured in simulated conditions similar to assembly conditions of lateral screw retention implant resulted in a mean of 69.75 Nmm with the highest and lowest values of 120.67 Nmm and 34.67 Nmm. This result became the basis of tightening torque variation. Each group's retention capability is measured and compared to cement-retained dental implants. Results show that tightening torque correlates positively with retention force, with the highest average retention score showed by lateral screw retained under tightening torque of 200 Nmm with 317.87 N higher than cement-retained.
Keywords:
lateral screw retained
; retrievability
; retention
; dental implants
m of aluminum oxide. Experiment on the tightening strength of 48 subjects measured in simulated conditions similar to assembly conditions of lateral screw retention implant resulted in a mean of 69.75 Nmm with the highest and lowest values of 120.67 Nmm and 34.67 Nmm. This result became the basis of tightening torque variation. Each group's retention capability is measured and compared to cement-retained dental implants. Results show that tightening torque correlates positively with retention force, with the highest average retention score showed by lateral screw retained under tightening torque of 200 Nmm with 317.87 N higher than cement-retained.
1. Introduction
Single implant restoration has become common in the dentistry field nowadays. The biological success rate of implant dentistry has the highest success rate (more than 90%) compared to other treatments to treat the loss of natural teeth [1,2]. However, as the most widely used type of retention in implant prostheses [3,4], cement-retained still faced mechanical complications that become a big issue, such as porcelain fractures, abutment fractures, and especially screw loosening [5,6]. A study by Dr. Elyce Link-Bindo states that about 9.3% screw loosening will occur in the 5 first years [7]. This technical issue was why the connection between the implant and abutment should be retrievable [8,9]. With a retrievable connection/retention method, the internal screw of a two-piece dental implant can be easily retightened if needed.
The retrievability of cement-retained dental implants is limited. Removing the crown requires significant force, which can permanently damage the crown, abutment, internal screw, or implant itself [10]. Although temporary cementation is relatively easy to remove because it was designed for temporary usage, most have low retention capability. A study by Veselinovic shows that the retention force of cement (both temporary and permanent) decreases after being subjected to mechanical cyclic loading, which is comparable up to 12 months of usage; this study demonstrates that temporary permanent cement retention force decreases up to 27.7% and 44.9% the initial values [10]. Several studies have been conducted to increase temporary cement's retention level. Studies use laser etching, acid etching, sandblasting, oxygen plasma, and other surface treatment method to modify the abutment's surface in order to increase retention forces shows a positive correlation with varied results ranging from 26.4 % to 90.7 % of the increase in retention forces [11,12,13]. Aside from surface treatment, several studies also analyzed the effects of geometry modification of an abutment through axial wall modification [14,15,16], screw access channel modifications [17], the addition of grooves [18], abutment height [19], and shape [20]. Even though several surface treatments and geometry modifications are proven to increase retention significantly, most studies show that cement failure mode leaves residue in both implant and coping. This residue can be categorized as a rough surface to which bacteria can adhere, resulting in higher possibilities of peri-implant diseases [21,22,23], making this method impractical.
Another way to develop a retrievable dental implant is by using a screw-retained dental implant, which holds a dental crown using a screw to retrieve it [24]. Another advantage of the screw-retained type is the minimum risk of inflammation in peri-implant tissue since no cement was used in this type of connection [1,25]. Although this type of crown retention is already available in the market, the price, aesthetic limitations, and clinical disadvantages compared to cement-retained implants are why clinicians prefer cement-retained implants [26,27]. Since the screw-retained has access placed vertically, it has the disadvantage of compromising aesthetics, and because the access screw occupies at least 50% of the occlusal table, it is difficult to establish ideal occlusal contacts (clinical disadvantages) [28,29].
Lateral screw retention has been developed to avoid occlusal access holes. The lateral screw method can help restore the excessive angulated implant while maintaining retrievability. The Cross-pinn retained implant-supported restoration requires modifying the abutments. This method is quite complex because the procedure starts with determining the milling direction of the abutment, followed by making access through the abutment from the lingual-labial direction and tapping the abutment. This method does not require special coping or screw angulation or mention the torque required when installing the crown [30,31,32]. Another way to use this type of connection is to use a prefabricated part, for example, in the Straumann implant system. In the Straumann system, specific components are required, such as abutment SynOcta TS, coping (gold or plastic coping for burnout technique), and the transversal screw. The lateral screw angle and position have been determined according to coping. However, this type of connection uses is limited in terms of availability because it requires a special abutment, laboratory procedures are very sensitive and expensive, and this type of connection can only be used exclusively by a specific dental implant brand. The similarity between the lateral screw in Straumann and the cross arch pin technique is it requires the lateral screw to go through the abutment. A study from Lasheras et al. shows that based on finite element analysis study shows that the lateral screw retained can be the choice with the lowest mechanical risk complication in abutment and abutment screw and the prosthetic screw when loads of 0° and 15° inclination forces are applied in the model [33].
This study offers a new approach to achieving lateral screw retention using additional coping with lateral screws, which retains the dental crown mainly using friction-based retention. The set of dental implants used in this study is widely used cement-retained dental implants subjected to surface treatment of sandblasting with a variation of particle size to increase the friction coefficient of the dental abutment. Aside from that, this study also experimented with the tightening torque needed for this novel friction-based lateral screw-retained dental implant. This study aims to develop a novel friction-based lateral screw retention method with a similar retention capability to cement-retained, which has better aesthetics and occlusal condition than vertical screw retention.
2. Materials and Methods
2.1. Prototype Design and Manufacturing
The main idea of friction-based lateral screw-retained dental crown is to use coping, which has lateral access for a general headless M2 screw that locks the coping into the abutment using lateral force generated by the tightening motion of the screw which combined with the friction coefficient of the abutment's flat surface. The combination of both factors resulted in the frictional force, which resists the motion of the entire crown structure. This coping then becomes the base structure for the crown structure, which aesthetic needs can be achieved from another process, such as porcelain fused to metal (PFM) (see Figure 1).
As mentioned, the friction coefficient is critical for this novel friction-based lateral screw-retained dental crown. Although there are many options for surface treatment, specifically to increase friction coefficient, this study uses sandblasting. Sandblasting can create irregularity in metal surfaces, increasing the object's surface roughness [34]. The sandblasting is done on the flat surface of the abutment, which becomes the contact surface between the lateral screw and the dental abutment. In cement-retained dental crowns, the flat surface of the abutment had the primary function of anti-rotation of the crown.
In this study, the coping design was developed by evaluating the Dentium dual abutment, which has a 4.5 mm diameter and 5.5 mm in height, using an optical Nikon SMZ 1270i Type 164 microscope and Indomicroview software. The measurement from the optical microscope became the basis of dental implant coping design, which was modeled using SolidWorks. As the retention test is performed by pulling the coping and dental implant set apart in a tensile test using a universal testing machine, aside from the original coping design, each coping was designed and manufactured with a cuboid part on top (Figure 2), designed to be gripped by a universal testing machine. This coping prototype was made using NiCr (4all, Ivoclar), a widely used material for coping, especially in developing countries [35]. Although using similar materials for cement-retained coping, this coping prototype was manufactured using CNC milling instead of casting.
2.2. Coping Retention Test for Varied Surface Roughness
As an effort to find the suitable parameters of sandblasting for this novel lateral screw retained coping method, an experiment was conducted to find the correlation between surface roughness and coping retention force. Several parameters in sandblasting can be varied, such as materials, particle size, pressure, distance from the nozzle to objects, duration, and even the angle [36]. Each parameter variation could give different results that directly affect the abutment's surface roughness, which could affect the retention capability of this novel friction-based lateral screw-retained dental crown.
Figure 3.
(a) Sandblasting of dental implant abutment using Al2O2 and (b) sandblasted flat surface of an abutment.
Figure 3.
(a) Sandblasting of dental implant abutment using Al2O2 and (b) sandblasted flat surface of an abutment.
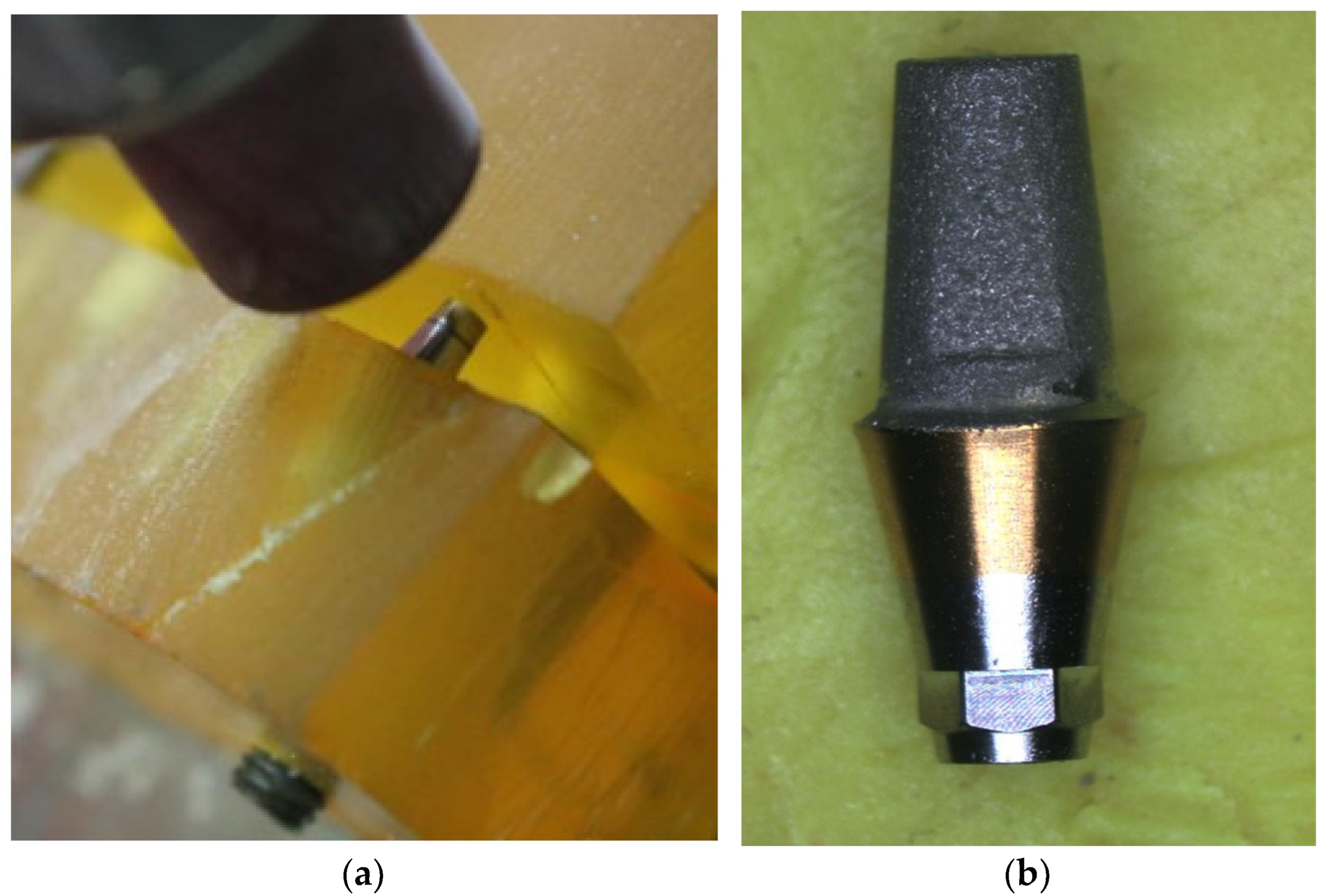
For this experiment, four groups of specimens sandblasted using various particle sizes of Aluminum Oxide (Al2O3) were compared to a group of untreated abutments. Those four groups have five specimens each, sandblasted using 63, 102, 254, and 686 m of Al2O3. The sandblasting uses a pressure of 0.3 MPa in a 10 mm distance between the nozzle and the abutment's flat surface for 10 seconds, based on previous studies [11,12]. In order to remove the remains of sandblasting materials in the abutment surface, the abutment is then cleaned using an ultrasonic cleaner with three steps using three different solutions: acetone, isopropyl alcohol (IPA), and distilled water. Each step was done in 5 minutes at 60 C [37]. Each specimen's surface roughness was then measured using Surfcom 2900SD3 with a probe placed in the abutment's flat surface so that the measurement conducted has the same direction as the coping retention test (vertical/parallel with the dental implant's axis). Since no information is available for screw tightening torque for lateral screw-retained or cross-pin retained as the closest approach to lateral screw-retained [30,31,32], the tightening torque of 200 Nmm was used since many commercially available dental implant sets use this value for their internal screw tightening torque [38,39,40]. In each specimen, the lateral screw is ensured to directly contact the sandblasted area without any angulation.
Tensile test to determine the retention force comparison between cement-retained and friction-based lateral screw-retained crown performed using Universal Testing Machine AND RTF 2350 with tensile speed of 1 mm/min [41,42,43]. For friction-based lateral screw retained specimens, cuboid space in coping is clamped using a jig, as shown in Figure 4 below. The highest retention force was recorded in Newtons (N), which was then compared between each group to understand the retention capability of each assembly.
2.3. Maximum Tightening Torque for Lateral Screw Retained
Aside from the effect of surface roughness of abutment on the retention capability of a dental crown, in this study, we also try to understand whether this friction-based lateral screw-retained dental crown will need additional tools to be assembled easily into a patient's mouth. An experiment was conducted using a digital torque meter placed lateral to the dental implant's axis between the phantom to simulate lateral screw tightening conditions with an existing Dentium screwdriver (Hex Driver L/T). The phantom from M.tech (South Korea) placed with a mouth opening of 40.5 mm [44] combined with the position of tightening in the second molar chosen to purposefully restrict the subjects hand movement, which simulates the most challenging position for lateral screw tightening condition in patient's mouth. The jig is designed to simulate the restriction of the mouth opening and fixate the digital torque meter. The assembly clamped on the table, and the subjects were instructed to sit beside the assembly. This experiment setup mimics the patient's actual condition in the orthodontic dental chair. This jig was 3D Printed using PLA+ (eSun) as the material. The tip of the digital torque meter was connected to Dentium's screwdriver, and then 48 subjects (27 male and 21 female) were instructed to turn the screwdriver as hard as possible, simulating the assembly condition of the lateral screw-retained dental implant. Each subject was asked to repeat the tightening process three times, and the average recorded torque was then used in this study.
Figure 5.
(a) The device assembly to record the maximum tightening torque of the lateral screw; (b) The actual implementation of the device.
Figure 5.
(a) The device assembly to record the maximum tightening torque of the lateral screw; (b) The actual implementation of the device.

2.4. Coping Retention Test for Varied Tightening Torque
After finding the effect of surface roughness in coping retention force and human tightening torque capability, this experiment divided each group based on variations of tightening torque used. Tightening torque of a lateral screw results in the development of lateral force, one of to main parameters in friction-based lateral screw retain methods. Tightening torque of 69.75 Nmm (SB686 T69.75) and 120 Nmm (SB686 T120) were used, and since the tightening torque of 200 Nmm (SB686 T200) was used in the previous experiment (see 2.3), this result will also be included in the analysis for this experiment. Each of these specimens was subjected to sandblasting conditions, which shows the highest retention score based on the previous experiment. In this experiment, each friction-based lateral screw-retained group variation was then compared to the cement-retained group (CR), which was treated as a benchmark in this study. Five specimens in the cement-retained group use specially made casted coping made from the same material as the friction-based lateral screw retained coping and designed to have a loop to place the hook during the tensile test. Before coping was placed, all the abutment screw access holes were filled with gutta-percha to avoid potential chemical bonds between materials. The coping was placed into the abutment using screw-retained glass ionomer cement type 1 (Fuji). Immediately after placement, the coping was then subjected to a 50 N load for 10 minutes [41,45,46]. All samples prepared for this experiment were stored in distilled water at 37 C for 24 hours before testing [47]. This condition helps ensure the cement is fully cured under similar conditions with placement in the patient. These specimens were then tested in similar settings and conditions for the coping retention test for surface roughness variations.
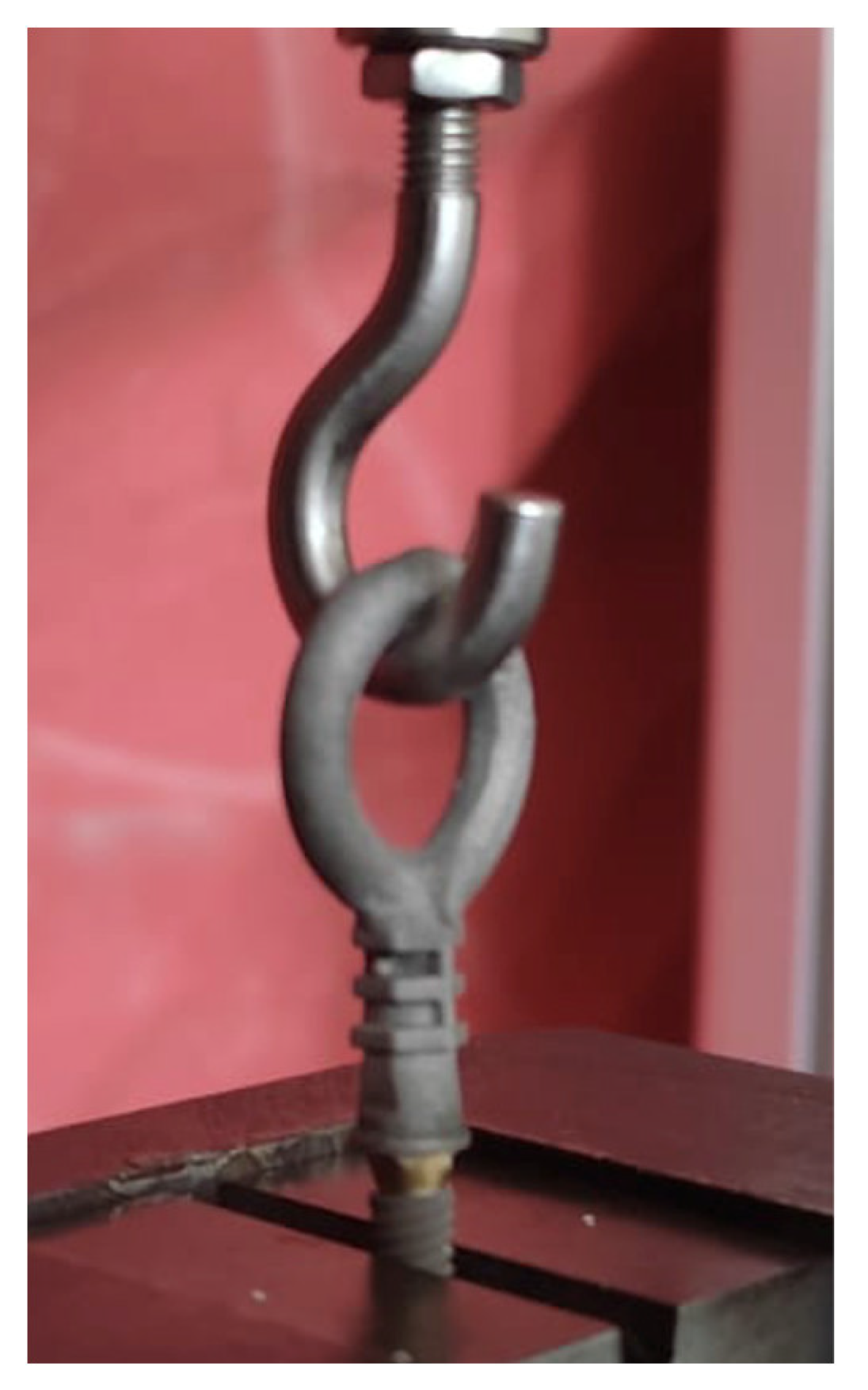
Figure 6.
Tensile test for cement-retained dental implant with custom coping.
2.4. Statistical Analysis
Each gender category in maximum tightening torque for lateral screw retained was analyzed using Shapiro-Wilk, and the differences were then analyzed using T-Test. For the coping retention test in surface roughness and tightening torque variations, each group was analyzed by one-way analysis of variance (ANOVA). Statistical analysis was performed using SPSS (SPSS Inc, Chicago, IL, USA). A p-value 0.05 was considered statistically significant.
3. Results
3.1. Coping Retention Based on Varied Surface Roughness
Variation of sandblasting particle resulted in variation of retention capability shown in Table 1 below. Each variation was divided into groups with specimens sandblasted by 63 m Al2O3 particle as SB63 T200, 102 m particle size as SB102 T200, 254 m particle size as SB254 T200, 686 m particle size as SB686 T200, and untreated (not sandblasted) specimens as NS.
Figure 7 shows the comparison of Ra between groups based on particle size used in sandblasting. It shows that the average Ra from highest to lowest showed by SB686 T200 with 0.67 0.04 m, SB254 T200 with 0.58 0.04 m, SB102 T200 with 0.56 0.03 m, SB63 T200 with 0.44 0.05 m, and NS with 0.04 0.002 m.
The retention force of each group is shown in Figure 8, with the highest retention force being SB686 T200 with 317.87 21.08N, followed by SB254 T200 with 304.38 34.30N, SB102 T200 with 249.78 8.06N, NS with 163.420 23.76 N, and the weakest retention force on average being SB63 T200 with 159.106 41.47N.
3.1. Hand Tightening Torque
The summary of the data for hand tightening torque shown in Table 2 with the detailed data can be seen in Appendix A. The histogram of the tightening torque capability of the overall data is shown in Figure 9.
The Shapiro-Wilk test shows that each group of male, female, and overall data has a normal data distribution with a p-value > 0.05. As such, a comparison between male and female data for tightening torque in this experiment was done using the T-Test, resulting in significant differences between groups with male data showing higher tightening torque (p < 0.05).
3.2. Coping Retention Based on Tightening Torque
Dental implant retention of each group Cement Retained (CR) as standard/benchmark and three groups of lateral screw with tightening torque of 69.75 Nmm (SB686 T69.75) and 120 Nmm (SB686 T120) shown in Table 3 below.
Figure 10 shows the comparison between groups, including SB686 T200, in which specimens were tightened with 200 Nmm tightening torque. It shows that the average coping retention of lateral screw retention with 200 Nmm tightening torque (SB686 T200) has the highest retention by 317.87 21.08 N, followed by 120 Nmm (SB686 T120) with 158.48 23.37 N, cement retention (CR) with 155.83 19.85 N, and lateral screw retention with 69.75 Nmm tightening torque (SB686 T69.75) as the weakest with 96.67 16.66N.
Compared to the cement-retained group, the SB686 T69.75 is significantly lower (p < 0.01), SB686 T120 has a higher average but statistically insignificant, and SB686 T200 is significantly higher (p < 0.01). Among screw retained groups, compared to SB686 T200, both SB686 T69.75 and SB686 T120 are significantly lower (p < 0.01).
Figure 11.
(a) Cement retained and (b) lateral screw retained failure mode.
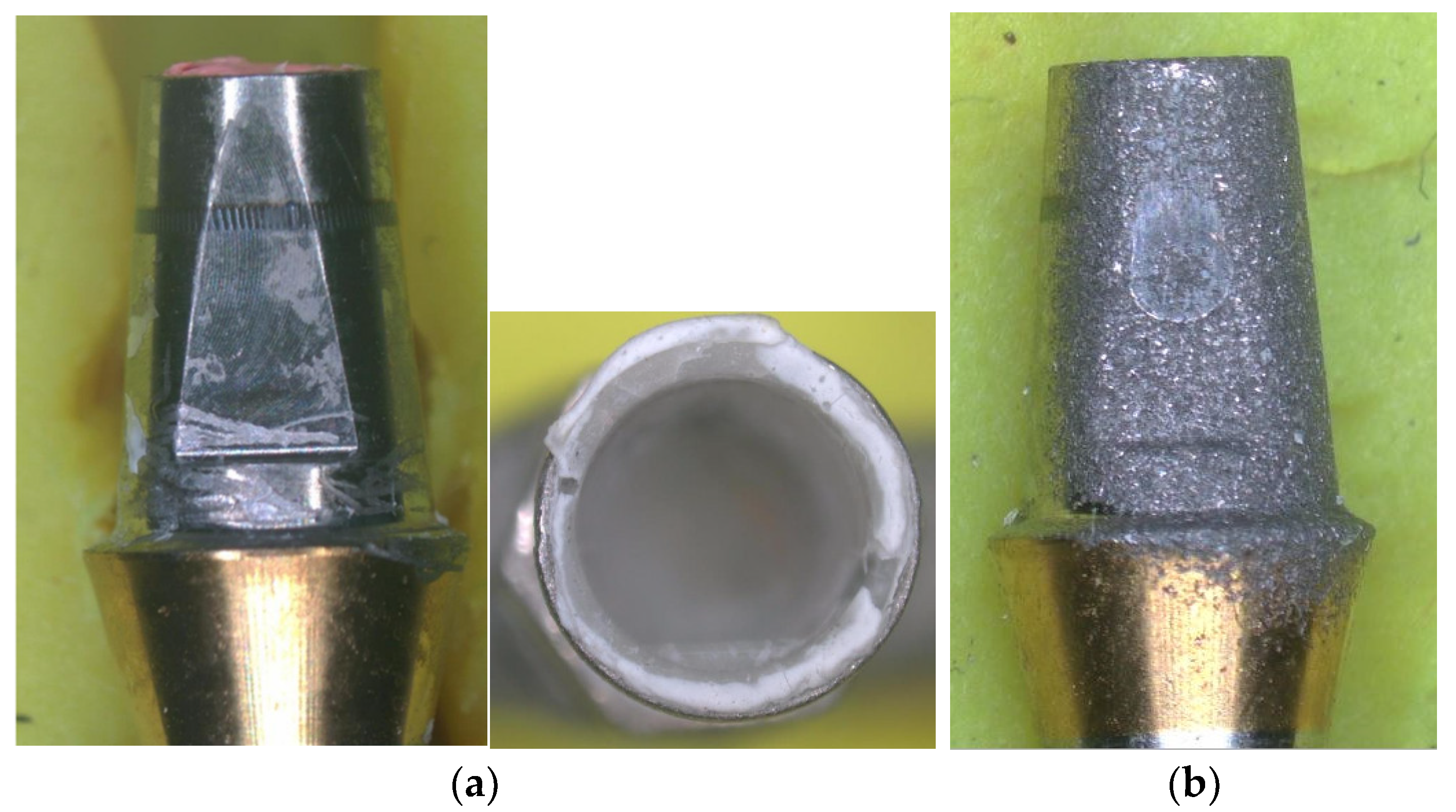
The failure mode of the cement-retained group under tensile test shows residue of cement in the abutment and coping, and the lateral screw-retained (SB686 T69.75, SB686 T120, and SB686 T200) shows a mark that resulted from friction between the screw and sandblasted surface of the abutment.
4. Discussion
This study developed a novel friction-based lateral screw-retained method approach by designing a universal coping and surface treatment of an existing abutment. This approach to the novel retention method can be used on most single implant restoration with a flat surface (in this case is an anti-rotation feature for Dentium), with a simple manufacturing procedure done to the coping to give access to the lateral screw and surface treatment done to the flat surface of the abutment to increase the surface roughness. With this coping, the retrievability of screw-retained implants can be achieved at the same time. Although currently, this coping design is limited, this design structure can be further developed to provide better support. A study by Wang et al. shows that the maximum fracture resistance strength of porcelain in porcelain-fused-to-metal (PFM) crowns highly depends on its metal structure substructure design [48].
Sandblasting is done in order to increase static friction, which can lead to stronger retention achieved. Sandblasting is done to create irregularity in the titanium surface of the abutment, which increases the surface roughness [49]. Surface roughness is related to the friction coefficient, and a higher friction coefficient could increase the retention capability of this retention method. Sandblasting was chosen because it is one of the easiest and most inexpensive methods of surface treatment [50], which increases the possibility of this method being replicated and used around the world since it does not need any specific abutment or implant manufactured. The result of this study also demonstrates that it can be done by modifying the existing abutment's surface.
The sandblasting using variations of particle size experiment results shows a positive correlation between particle size and surface roughness. Larger particle size results in higher surface roughness of the object's surface. This correlation is similar to a study by Hasan & Abood, which also uses variations of Al2O3 particle sizes [34]. In this study, the highest surface roughness was shown by SB686 T200 (0.67 0.04 m) which was also significantly higher compared to other groups (p < 0.01), and the untreated surface of abutment (0.04 0.002 m) as the lowest surface roughness (Ra), which also significantly lower compared to other groups (p < 0.01). However, the result also shows that groups SB102 T200 and SB254 T200 are insignificantly different compared to each other but the SB254 T200, which has a larger particle size, shows a higher average of surface roughness. The result of this experiment also shows that surface roughness mainly has a positive correlation with retention force, which confirms the positive correlation between surface roughness and static friction coefficient. Though NS groups show higher retention force compared to SB63 T200 it is insignificant, and it shows that within that surface roughness conditions, the retention is mainly affected by the tightening torque instead of friction between the lateral screw and abutment. In this study, the highest retention force was also shown by groups with the highest surface roughness (SB686 T200), and the lowest retention force was shown by both SB63 T200 and NS groups, which also have low surface roughness. A positive correlation between surface roughness and static friction open the possibility of using other surface treatment option to increase surface roughness in the abutment's flat surface, increasing the versatility of this method. Other surface treatments that can be used as a strategy to increase surface roughness are laser etching, acid etching, ion implantation, sputtering, and other combinations of several surface treatment methods, such as SLA, which combines sandblasting using large grit and acid etching [51]. Aside from that, geometry alteration, like making a groove in an abutment, is worth trying since the study by de Campos et al. found that the surface roughness (Ra) of a grooved abutment can reach up to 8.38 m [52]. As the SB686 T200 group shows the highest surface roughness and retention score, Al2O3 with a particle size of 686 m was then used as a parameter for sandblasting for retention force based on the tightening torque experiment. The result of this group was also then compared to other variations in the tightening torque experiment since the parameters are already similar.
For coping retention under different tightening torque experiments, the lowest retention was shown by the SB686 T69.75 group with 96.67 16.66 N and the highest was shown by the SB686 T200 group with force retention of 317.87 ± 21.08 N, which was significantly different (p < 0.01). This shows that tightening torque is one of the crucial aspects to consider in which the value groups subjected to lower tightening torque show significantly lower strength than higher torque. Considering the wide range of tightening capabilities shown in the hand tightening torque experiment (lowest value in 34.67 Nmm and highest value in 120.67 Nmm), the importance of standardization for tightening torque is imminent, which could be achieved by developing tools. Study shows that current torque wrenches readily available in the market has excellent accuracy [53,54,55] One of the factors is the angle at which the examiner read the torque value, with 90 being the best [56]. One of the approaches for lateral screw-retained implant assembly in a study by Lee et al. [57], uses lateral screwdriver with contra-angle attachment, which is easily managed within the oral cavity with 500-1000 Nmm torque, which is a lot higher compared to the highest tightening torque for this study. For this friction-based lateral screw-retained crown, using a similar lateral screwdriver with a contra-angle attachment can easily surpass this study's highest tightening torque value. It might give a more accurate value considering that different tightening torque resulted in significantly different retention forces.
Cement retained has become the benchmark/standard in this study because it has already been proven that cement retained can perform adequate retention during daily usage of dental implants. Studies show that most mechanical complications are the result of dynamic compression forces to dental implants, such as screw loosening, porcelain fractures, and abutment fractures [5,6,7]. The tensile test was conducted using five samples to obtain the coping retention force from each group; the result from the cement-retained group shows an average of 155.83 19.85 N. Studies with a similar condition to calculate retention force show the difference between one and another varied by types cement, abutment used, even thickness of the cement used. A study by El-Helbawy shows the average retention force of 138.8 10.2 N for the assembly of cast coping with titanium abutment (dentist) using Temp-Bond Non-Eugenol (Kerr) as the cement [11], another study by Reddy et al. involving three brands of cement widely available in the market shows various average retention force ranging from 138.41 N to 258.28 N [58]. The thickness of the cement has also been shown to influence the retention of dental implant coping. A study by Abou-Obaid and Al-Khudairy comparing different cement thicknesses shows that the optimum thickness recorded in this study is 20m, which has the highest retention force compared to groups with 35 and 50 m cement thickness, it is also demonstrated that in cement-retained dental implant, abutment height also affects retention strength, which related to the different surface area [59].
Among the lateral screw-retained group, SB686 T200 has the highest coping retention force, followed by SB686 T120, and SB686 T69.75 as the lowest. This demonstrates that tightening torque affects coping's retention capability (positive correlation), with higher tightening torque resulting in higher coping retention force. Compared to cement-retained, the SB686 T69.75 is significantly lower (p < 0.01). Compared to study by Nagasawa et al., the average coping retention force of SB686 T69.75, which is 96.67 16.66 N, is higher compared to 5 of 6 commercially available temporary cement tested after 7 days of seating and higher than all of them when compared to 28 days old specimens [43]. The coping retention force of cement-retained compared to SB686 T120 is insignificantly different, which shows that with the right tightening torque, the retention performance of friction-based lateral screw retained is comparable to various cement-retained groups. Compared to SB686 T200, the coping retention force of cement-retained is significantly lower (p < 0.01).
There are no known standards regarding the retention force of dental implant coping. However, there are studies regarding the pull-out strength of dental implants. One of them is a study by Seong et al. investigating the pull-out strength of a dental implant implanted in a rabbit tibia for 1 to 12 weeks of healing time shows that healing time affects pull-out strength, which is similar to human bone [60], it shows that after one week the pull-out force is 187.9 69.2 N. After twelve weeks, the pull-out force shows 351.8 69.2 N, and this value is also shown in a study by Oliscovicz et al. for pull-out force on Synbone, which simulates the artificial bone of the human femur [61]. The pull-out force shown in both studies shows a value close to SB686 T200, demonstrating that based on pull-out force setup conditions (sandblasting and tightening torque) for SB686T200 groups shows promising results since it is expected that dental crown has lower pull-out force compared to dental implant in a failure condition.
The lateral screw retained failure mode shows tracks from friction between the lateral screw and the abutment's surface, but the overall abutment did not show any damage. As shown in previous studies, the assembly and failure mode of cement-retained leaves residue in abutment and coping, which could result in peri-implantitis diseases [21,22,23]. he failure mode in lateral screw needs further investigations to understand whether its condition after failure affects the retention capability, as the surface roughness may decrease due to friction between the screw and the abutment's surface. If this type of failure affects retention performance, then the abutment needs to be replaced or re-sandblasted, and since there is no damage done to the overall abutment, it can just be removed without any further disturbance to the implant and surrounding bones. This phenomenon also needs to be one of the considerations of using a one-piece implant for friction-based later screw-retained dental crowns since any damage done to the abutment area may need further invasive surgery.
This study has its limitations regarding sample size, available abutment type, and surface treatment procedure performed. But it shows the prospect of friction-based lateral screw retention being one of the methods to gain the advantage of cement and screw retention, which is easy to replicate and use with limited resources.
5. Conclusions
Within the limitation of this study, conducted tests show the potential of a novel friction-based lateral screw retention method. The coping design in this study combined the advantage of the cement-retained and vertical screw retention method. This design gives an ideal occlusal advantage, better aesthetics, and is retrievable. This study shows that particle size positively correlates with surface roughness in the sandblasting process of titanium dental abutments. Aside from that, surface roughness was also found to be a critical factor that positively correlates with retention force. Sandblasting on titanium dental abutments using Al2O3 with 686m particle size (highest particle size used in this study) under 0.3 MPa pressure from a 10 mm distance in 10 seconds resulted in the highest surface roughness (Ra) with 0.67 0.04 m and retention force with 317.87 ± 21.08 N, in which this sandblasting condition then used in the following experiment as the standard sandblasting condition.
In order to understand the human capability to produce tightening torque for this novel friction-based lateral screw retention, an experiment was conducted under simulated conditions. The jig with a 40.5 mm mouth opening and condition similar to lateral skew tightening in the second molar shows an average of 69.75 Nmm with a standard deviation of 22.91 Nmm.
Using sandblasting parameters and considering variations of tightening torque from the previous experiment, the novel friction-based lateral screw retention was tested under variations of tightening torque, namely 69.75, 120, and 200 Nmm. The result of this experiment is promising for the possibility of this novel crown retention method. The retention force of SB686 T69.75 gives the lowest value of 96.67 16.66 N which significantly lower compared to CR groups (p < 0.01). SB686 T120 average in 158.48 23.37 N, which is insignificantly different compared to CR with 155.83 19.85 N. Lastly, SB686 T200 shows a significantly higher result in 317.87 ± 21.08 N compared to CR (p < 0.01). This phenomenon, combined with the tightening capability of this study's subject, proved that tightening torque can have a significant impact on coping retention in this method.
Even though the result of this study shows it can be one of the solutions in today's crown retention method, there is still much room for improvement and study that needs to be conducted to explore the full potential of this novel retention method.
6. Patents
This work's prototype design and results are intended to be filed as a patent.
Author Contributions
Conceptualization, S.S., Y.W., T.M., R.S.D., and L.S.K.; methodology, T.M., P.R.M., and R.A.U.; formal analysis, S.S., T.M., P.R.M., and R.A.U; data curation, T.M., P.R.M., and R.A.U.; writing—original draft preparation, T.M., and R.A.U.; writing—review and editing, S.S., T.M., and R.A.U.; visualization, R.A.U.; supervision, S.S., Y.W., T.M., R.S.D., and L.S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research is funded by Directorate of Research and Development, Universitas Indonesia under Hibah PUTI 2023, grant number NKB-837/UN2.RST/HKP.05.00/2023.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article and available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
| Gender | Age | Height (cm) | Weight (kg) | Average Tightening Torque (Nmm) |
| Male | 25 | 169 | 55 | 109.33 |
| Male | 25 | 185 | 81 | 34.67 |
| Male | 26 | 180 | 82 | 75.00 |
| Male | 26 | 183 | 68 | 92.33 |
| Male | 26 | 170 | 100 | 71.00 |
| Male | 26 | 165 | 65 | 86.67 |
| Male | 26 | 171 | 64 | 50.00 |
| Male | 27 | 177 | 78 | 56.00 |
| Male | 28 | 173 | 66 | 53.00 |
| Male | 28 | 165 | 77 | 46.00 |
| Male | 29 | 178 | 85 | 101.67 |
| Male | 29 | 173 | 85 | 58.67 |
| Male | 30 | 180 | 92 | 61.00 |
| Male | 30 | 168 | 76 | 70.67 |
| Male | 30 | 168 | 70 | 67.33 |
| Male | 30 | 175 | 95 | 69.00 |
| Male | 31 | 168 | 72 | 88.67 |
| Male | 31 | 168 | 63 | 49.67 |
| Male | 31 | 167 | 82 | 118.00 |
| Male | 32 | 158 | 61 | 112.67 |
| Male | 32 | 168 | 84 | 55.00 |
| Male | 35 | 170 | 90 | 105.00 |
| Male | 35 | 186 | 100 | 90.67 |
| Male | 35 | 180 | 75 | 120.67 |
| Male | 36 | 198 | 112 | 70.33 |
| Male | 36 | 169 | 70 | 44.33 |
| Female | 26 | 148 | 45 | 55.67 |
| Female | 27 | 165 | 53 | 37.67 |
| Female | 27 | 163 | 49 | 71.00 |
| Female | 28 | 164 | 66 | 35.67 |
| Female | 29 | 164 | 48 | 52.00 |
| Female | 29 | 159 | 60 | 63.00 |
| Female | 30 | 162 | 58 | 87.33 |
| Female | 30 | 155 | 54 | 81.00 |
| Female | 30 | 155 | 50 | 73.67 |
| Female | 30 | 167 | 75 | 77.00 |
| Female | 30 | 167 | 78 | 36.67 |
| Female | 31 | 155 | 52 | 39.00 |
| Female | 34 | 158 | 70 | 50.00 |
| Female | 36 | 165 | 48 | 59.67 |
| Female | 36 | 165 | 58 | 50.67 |
| Female | 36 | 158 | 52 | 76.67 |
| Female | 36 | 173 | 90 | 100.33 |
| Female | 37 | 170 | 56 | 89.33 |
| Female | 38 | 153 | 60 | 66.33 |
| Female | 40 | 156 | 67 | 54.00 |
| Female | 42 | 158 | 62 | 64.67 |
References
- B. Pjetursson, A. Asgeirsson, M. Zwahlen, and I. Sailer, “Improvements in Implant Dentistry over the Last Decade: Comparison of Survival and Complication Rates in Older and Newer Publications,” Int. J. Oral Maxillofac. Implants, vol. 29, no. Supplement, 2014. [CrossRef]
- R. Resnik, Misch’s Contemporary Implant Dentistry, 4th ed. El Sevier, 2019.
- R. Reda et al., “A Systematic Review of Cementation Techniques to Minimize Cement Excess in Cement-Retained Implant Restorations,” Methods Protoc., vol. 5, no. 1, 2022. [CrossRef]
- Makke, A. Homsi, M. Guzaiz, and A. Almalki, “Survey of Screw-Retained versus Cement-Retained Implant Restorations in Saudi Arabia,” Int. J. Dent., vol. 2017, 2017. [CrossRef]
- R. Caricasulo, L. Malchiodi, P. Ghensi, G. Fantozzi, and A. Cucchi, “The influence of implant-abutment connection to peri-implant bone loss: A systematic review and meta-analysis,” Clinical Implant Dentistry and Related Research, vol. 20, no. 4. 2018. [CrossRef]
- J. C. Kim, J. Lee, S. Kim, K. T. Koo, H. Y. Kim, and I. S. L. Yeo, “Influence of implant-abutment connection structure on peri-implant bone level in a second molar: A 1-year randomized controlled trial,” J. Adv. Prosthodont., vol. 11, no. 3, 2019. [CrossRef]
- E. E. Link-Bindo, J. Soltys, D. Donatelli, and R. Cavanaugh, “Common Prosthetic Implant Complications in Fixed Restorations,” Compend. Contin. Educ. Dent., vol. 37, no. 7, 2016.
- J. G. Wittneben, T. Joda, H. P. Weber, and U. Brägger, “Screw retained vs. cement retained implant-supported fixed dental prosthesis,” Periodontol. 2000, vol. 73, no. 1, pp. 141–151, 2017. [CrossRef]
- S. Ma and A. Fenton, “Screw- Versus Cement-Retained Implant Prostheses: A Systematic Review of Prosthodontic Maintenance and Complications,” Int. J. Prosthodont., vol. 28, no. 2, pp. 127–145, 2015. [CrossRef]
- V. Veselinović et al., “Application of Semipermanent Cements and Conventional Cement with Modified Cementing Technique in Dental Implantology,” Acta Stomatol. Croat., vol. 55, no. 4, pp. 367–379, 2021. [CrossRef]
- N. El-Helbawy, A. El-Hatery, and M. Ahmed, “Comparison of Oxygen Plasma Treatment and Sandblasting of Titanium Implant-Abutment Surface on Bond Strength and Surface Topography,” Int. J. Oral Maxillofac. Implants, pp. 555–562, 2016. [CrossRef]
- M. Kurt, T. Külünk, Ç. Ural, Ş. Külünk, Ş. Danişman, and S. Savaş, “The effect of different surface treatments on cement-retained implant-supported restorations,” J. Oral Implantol., vol. 39, no. 1, pp. 44–51, 2013. [CrossRef]
- L. G. R. Drummond, R. M. H. Segundo, H. M. S. Oshima, and R. S. A. Shinkai, “The effect of surface texture on the retention of single implant-supported crowns cemented on wide-platform abutments,” Rev. Odonto Cienc., vol. 32, no. 4, pp. 169–173, 2017. [CrossRef]
- K. M. Tan, R. Masri, C. F. Driscoll, P. Limkangwalmongkol, and E. Romberg, “Effect of axial wall modification on the retention of cement-retained, implant-supported crowns,” J. Prosthet. Dent., vol. 107, no. 2, pp. 80–85, 2012. [CrossRef]
- R. Derafshi, A. H. Ahangari, K. Torabi, and M. Farzin, “Evaluation of the Effect of Axial Wall Modification and Coping Design on the Retention of Cement-retained Implant-supported Crowns.,” J. Dent. Res. Dent. Clin. Dent. Prospects, vol. 9, no. 1, pp. 35–9, 2015, [Online]. Available: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4417491&tool=pmcentrez&rendertype=abstract.
- M. Farzin, K. Torabi, A. H. Ahangari, and R. Derafshi, “Effect of abutment modification and cement type on retention of cement-retained implant supported crowns.,” J. Dent. (Tehran)., vol. 11, no. 3, 2014.
- C. Wadhwani, T. Hess, A. Piñeyro, and K.-H. Chung, “Effects of Abutment and Screw Access Channel Modification on Dislodgement of Cement-Retained Implant-Supported Restorations,” Int. J. Prosthodont., vol. 26, no. 1, pp. 54–56, 2013. [CrossRef]
- Lewinstein, L. Block, Z. Lehr, Z. Ormianer, and S. Matalon, “An in vitro assessment of circumferential grooves on the retention of cement-retained implant-supported crowns,” J. Prosthet. Dent., vol. 106, no. 6, pp. 367–372, 2011. [CrossRef]
- R. Biyani, M. Ali, D. Belles, and J. M. Powers, “Effect of metal extension of crown in the screw access channel of a posterior implant abutment on the retention of cement retained prosthesis,” J. Oral Implantol., vol. 41, no. 5, pp. 537–541, 2015. [CrossRef]
- M. Bresciano, G. Schierano, C. Manzella, A. Screti, C. Bignardi, and G. Preti, “Retention of luting agents on implant abutments of different height and taper,” Clin. Oral Implants Res., vol. 16, no. 5, pp. 594–598, 2005. [CrossRef]
- F. Nematollahi, E. Beyabanaki, and M. Alikhasi, “Cement Selection for Cement-Retained Implant-Supported Prostheses: A Literature Review,” J. Prosthodont., vol. 25, no. 7, pp. 599–606, 2016. [CrossRef]
- T. Linkevicius, A. Puisys, E. Vindasiute, L. Linkeviciene, and P. Apse, “Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis,” Clin. Oral Implants Res., vol. 24, no. 11, pp. 1179–1184, 2013. [CrossRef]
- Scarano, F. Inchingolo, S. Scogna, L. Leo, A. Greco Lucchina, and L. Mavriqi, “Peri-implant disease caused by residual cement around implant-supported restorations: a clinical report,” J. Biol. Regul. Homeost. Agents, vol. 35, no. 2, pp. 211–216, 2021. [CrossRef]
- P. V. B. Da Rocha, M. A. Freitas, and T. De Morais Alves Da Cunha, “Influence of screw access on the retention of cement-retained implant prostheses,” J. Prosthet. Dent., vol. 109, no. 4, pp. 264–268, 2013. [CrossRef]
- Sailer, D. Karasan, A. Todorovic, M. Ligoutsikou, and B. E. Pjetursson, “Prosthetic failures in dental implant therapy,” Periodontol. 2000, vol. 88, no. 1, pp. 130–144, 2022. [CrossRef]
- M. T. Hamed, H. A. Mously, S. K. Alamoudi, A. B. H. Hashem, and G. H. Naguib, “A systematic review of screw versus cement-retained fixed implant supported reconstructions,” Clin. Cosmet. Investig. Dent., vol. 12, pp. 9–16, 2020. [CrossRef]
- R. Shadid and N. Sadaqa, “A comparison between screw-and cement-retained implant prostheses. A literature review,” J. Oral Implantol., vol. 38, no. 3, pp. 298–307, 2012. [CrossRef]
- H. Kenneth and G. C. Reena, “Cement-retained versus screw-retained implant restorations: Achieving optimal occlusion and esthetics in implant dentistry,” J. Prosthet. Dent., vol. 77, no. 1, pp. 28–35, 1997.
- B. Andersson, P. Odman, A. M. Lindvall, and P. I. Brånemark, “Cemented single crowns on osseointegrated implants after 5 years: results from a prospective study on CeraOne.,” Int. J. Prosthodont., vol. 11, no. 3, pp. 212–8, 1998, [Online]. Available: http://www.ncbi.nlm.nih.gov/pubmed/9728114.
- M. J. Gervais, P. Hatzipanagiotis, and P. R. Wilson, “Cross-pinning: The philosophy of retrievability applied practically to fixed, implant-supported prostheses,” Aust. Dent. J., vol. 53, no. 1, pp. 74–82, 2008. [CrossRef]
- R. J. Sambrook, R. B. Judge, and M. A. Abuzaar, “Strategies for restoration of single implants and use of cross-pin retained restorations by Australian prosthodontists,” Aust. Dent. J., vol. 57, no. 4, pp. 409–414, 2012. [CrossRef]
- S. RJ and J. RB, “The cross-pin retained implant supported restoration: a study of gasket placement and leakage.,” Aust. Dent. J., vol. 57, no. 4, pp. 415–420, 2012, [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/23186564/.
- F. Sánchez Lasheras et al., “Does the transversal screw design increase the risk of mechanical complications in dental implants? A finite elements analysis,” Int. j. numer. method. biomed. eng., vol. 35, no. 6, 2019. [CrossRef]
- S. F. Hasan and A. Z. Abood, “Effect of Various Particle Size of Sand-blast on Roughness and Shear Bond Strength of Ips E.max Press With Ceramic Veneer Materials (An in Vitro Study),” Malaysian J. Med. Heal. Sci., vol. 18, pp. 45–52, 2022.
- Haider, S. H. I. Jaffery, A. N. Khan, N. Qadir, and X. Jing, “Effect of Cerium on Mechanical, Metallurgical and Biomedical Properties of NiCrMoB Dental Alloy,” SSRN Electron. J., 2023. [CrossRef]
- Finger, M. Stiesch, M. Eisenburger, B. Breidenstein, S. Busemann, and A. Greuling, “Effect of sandblasting on the surface roughness and residual stress of 3Y-TZP (zirconia),” SN Appl. Sci., vol. 2, no. 10, 2020. [CrossRef]
- W. Yuda, S. Supriadi, and A. S. Saragih, “Surface modification of Ti-alloy based bone implant by sandblasting,” AIP Conf. Proc., vol. 2193, 2019. [CrossRef]
- Y. Sameera and R. Rai, “Tightening torque of implant abutment using hand drivers against torque wrench and its effect on the internal surface of implant,” J. Indian Prosthodont. Soc., vol. 20, no. 2, pp. 180–185, 2020. [CrossRef]
- E. Haack, R. L. Sakaguchi, T. Sun, and J. P. Coffey, “Elongation and preload stress in dental implant abutment screws.,” Int. J. Oral Maxillofac. Implants, vol. 10, no. 5, pp. 529–36, 1995, [Online]. Available: http://www.ncbi.nlm.nih.gov/pubmed/7590997.
- H. H. Mohammed, J. H. Lee, J. M. Bae, and H. W. Cho, “Effect of abutment screw length and cyclic loading on removal torque in external and internal hex implants,” J. Adv. Prosthodont., vol. 8, no. 1, pp. 62–69, 2016. [CrossRef]
- S. Bishti, J. Siouri, S. Wolfart, and T. Tuna, “Retention Forces of Implant-Supported Single Crowns and Fixed Dental Prostheses after Cementation: An In-Vitro Study,” Oral, vol. 2, no. 1, pp. 29–40, 2022. [CrossRef]
- H. Sarfaraz, A. Hassan, K. Kamalakanth Shenoy, and M. Shetty, “An in vitro study to compare the influence of newer luting cements on retention of cement-retained implant-supported prosthesis,” J. Indian Prosthodont. Soc., vol. 19, no. 2, pp. 166–172, 2019. [CrossRef]
- Y. Nagasawa, Y. Hibino, and H. Nakajima, “Retention of crowns cemented on implant abutments with temporary cements,” Dent. Mater. J., vol. 33, no. 6, pp. 835–844, 2014. [CrossRef]
- Rahmania, I. Tanti, and F. Gita, “The association of normal mouth opening with gender and height,” J. Int. Dent. Med. Res., vol. 10, no. Specialissue, 2017.
- P. Anilkumar, D. S. Chokhani, S. K. Mangrulkar, I. Gupta, R. Singh, and S. Kumar, “A comparative study of retention of cement retained implant prosthesis cemented with different luting cements,” Int. J. Health Sci. (Qassim)., pp. 9136–9144, 2022. [CrossRef]
- E. C. Keum and S. Y. Shin, “A comparison of retentive strength of implant cement depending on various methods of removing provisional cement from implant abutment,” J. Adv. Prosthodont., vol. 5, no. 3, pp. 234–240, 2013. [CrossRef]
- F. Dähne, H. Meißner, K. Böning, C. Arnold, R. Gutwald, and E. Prause, “Retention of different temporary cements tested on zirconia crowns and titanium abutments in vitro,” Int. J. Implant Dent., vol. 7, no. 1, 2021. [CrossRef]
- H. Wang, J. H. Wu, H. Y. Li, P. P. Wang, H. E. Lee, and J. K. Du, “Fracture resistance of different metal substructure designs for implant-supported porcelain-fused-to-metal (PFM) crowns,” J. Dent. Sci., vol. 8, no. 3, pp. 314–320, 2013. [CrossRef]
- P. Osak, J. Maszybrocka, M. Zubko, J. Rak, S. Bogunia, and B. Łosiewicz, “Influence of sandblasting process on tribological properties of titanium grade 4 in artificial saliva for dentistry applications,” Materials (Basel)., vol. 14, no. 24, 2021. [CrossRef]
- G. E. Kunt, G. Ceylan, and N. Yilmaz, “Effect of surface treatments on implant crown retention,” J. Dent. Sci., vol. 5, no. 3, pp. 131–135, 2010. [CrossRef]
- Jemat, M. J. Ghazali, M. Razali, and Y. Otsuka, “Surface modifications and their effects on titanium dental implants,” Biomed Res. Int., vol. 2015, 2015. [CrossRef]
- T. N. de Campos et al., “Effect of surface topography of implant abutments on retention of cemented single-tooth crowns.,” Int. J. Periodontics Restorative Dent., vol. 30, no. 4, pp. 409–13, 2010, [Online]. Available: http://www.ncbi.nlm.nih.gov/pubmed/20664843.
- M. A. Erdem et al., “The accuracy of new and aged mechanical torque devices employed in five dental implant systems,” Biomed Res. Int., vol. 2017, 2017. [CrossRef]
- S. Pincha, S. Shetty, and A. Mithra, “Accuracy of Implant Torque Wrenches after Clinical Service,” J. Interdiscip. Dent., vol. 8, no. 1, p. 13, 2018. [CrossRef]
- Y. Sameera and R. Rai, “Tightening torque of implant abutment using hand drivers against torque wrench and its effect on the internal surface of implant,” J. Indian Prosthodont. Soc., vol. 20, no. 2, p. 180, 2020. [CrossRef]
- H. Shiba et al., “Experimental study on the factors affecting torque of beam-type implant torque wrenches,” BMC Oral Health, vol. 21, no. 1, 2021. [CrossRef]
- H. Lee, J. Bin Lee, M. Y. Kim, J. H. Yoon, S. H. Choi, and Y. T. Kim, “Mechanical and biological complication rates of the modified lateral-screw-retained implant prosthesis in the posterior region: An alternative to the conventional Implant prosthetic system,” J. Adv. Prosthodont., vol. 8, no. 2, pp. 150–157, 2016. [CrossRef]
- S. Varalakshmi Reddy, M. Sushender Reddy, C. Rajaneesh Reddy, P. Pithani, R. Santosh Kumar, and G. Kulkarni, “The infuence of implant abutment surface roughness and the type of cement on retention of implant supported crowns,” J. Clin. Diagnostic Res., vol. 9, no. 3, pp. ZC05–ZC07, 2015. [CrossRef]
- Abou Obaid, “Effect of Abutment Height and Cement Thickness on the Retention of Cement-Retained Implant-Supported Restorations,” Adv. Dent. Oral Heal., vol. 9, no. 4, 2018. [CrossRef]
- W. J. Seong, S. Grami, S. C. Jeong, H. J. Conrad, and J. S. Hodges, “Comparison of Push-In versus Pull-Out Tests on Bone-Implant Interfaces of Rabbit Tibia Dental Implant Healing Model,” Clin. Implant Dent. Relat. Res., vol. 15, no. 3, pp. 460–469, 2013. [CrossRef]
- N. F. Oliscovicz, A. C. Shimano, É. Marcantonio Junior, C. P. Lepri, and A. C. Dos Reis, “Analysis of primary stability of dental implants inserted in different substrates using the pullout test and insertion torque,” Int. J. Dent., vol. 2013, 2013. [CrossRef]
Figure 1.
Usage of coping in friction based lateral screw retained dental implant set.
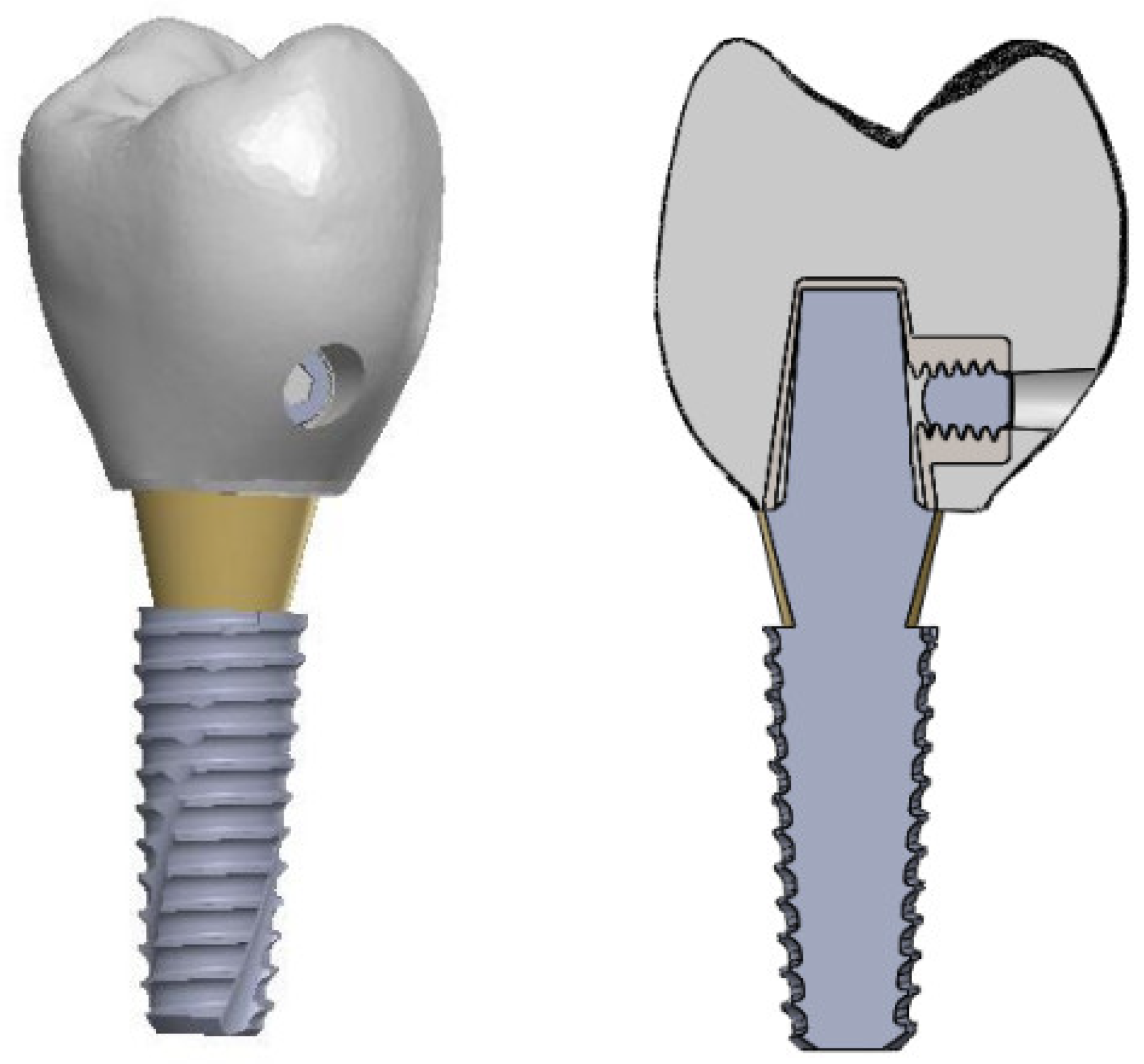
Figure 2.
Manufactured coping prototype for coping retention test.
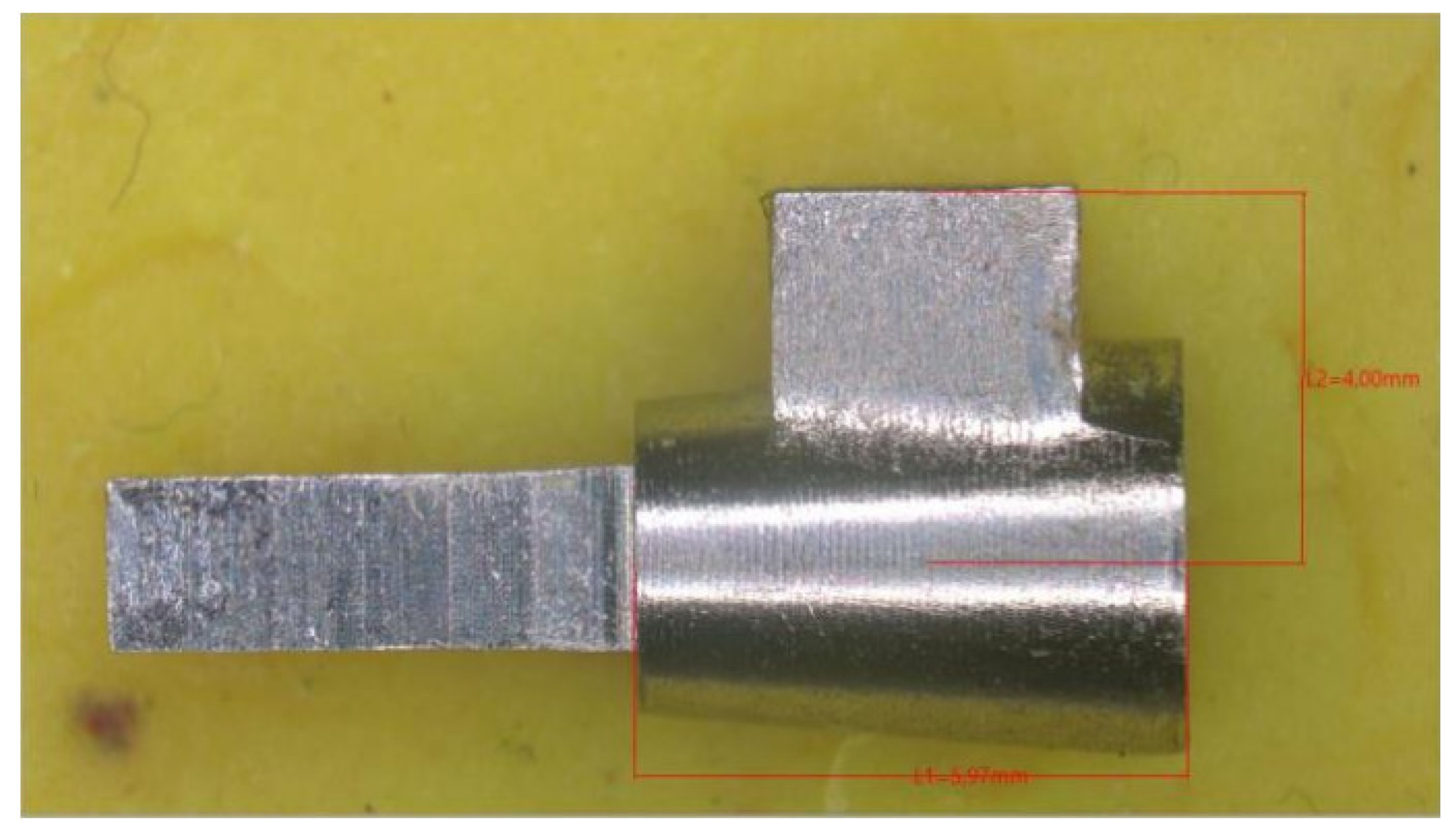
Figure 4.
Tensile test setup for lateral screw-retained dental implant.
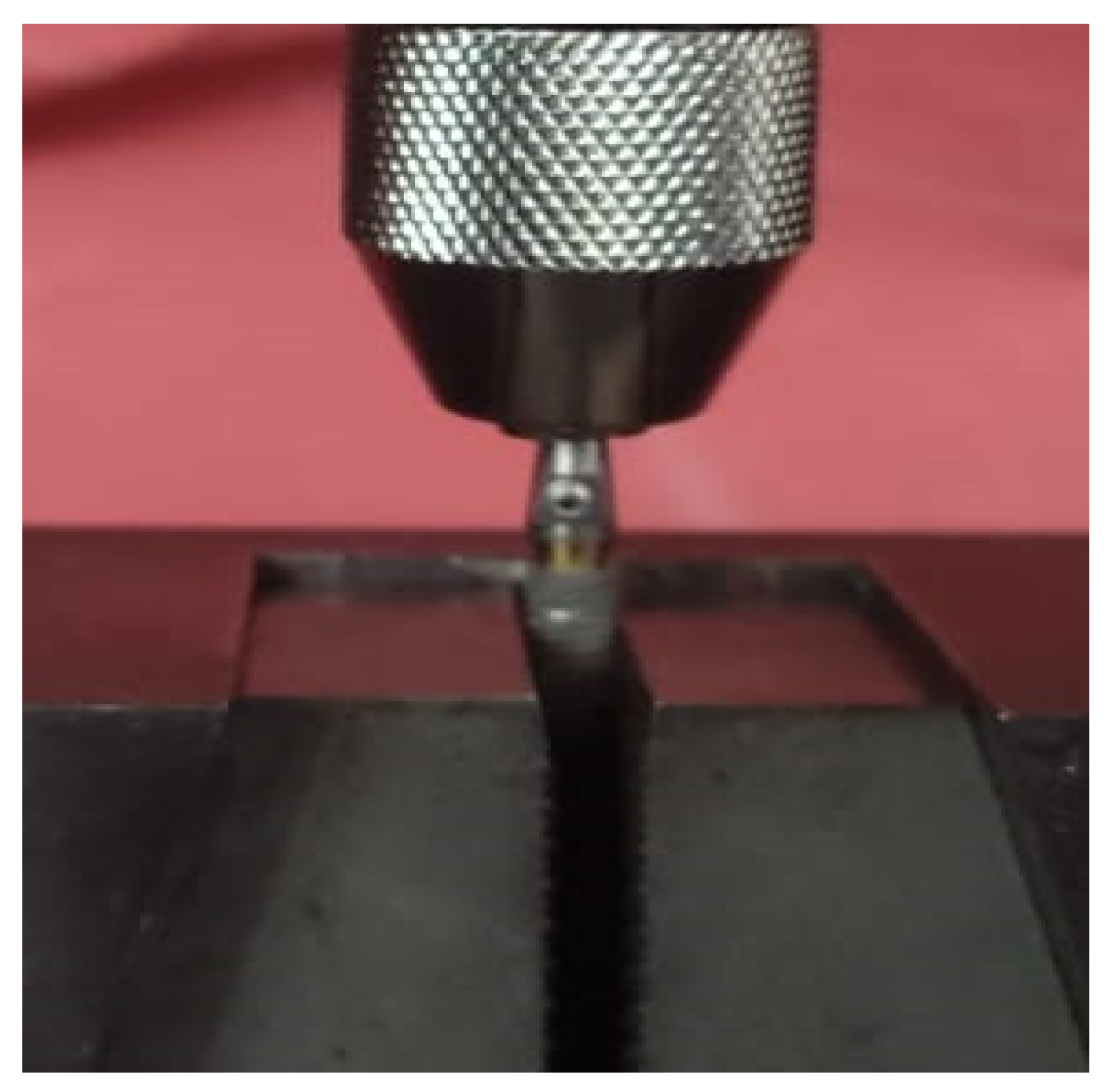
Figure 7.
Surface roughness comparison among sandblasting particle size variations.
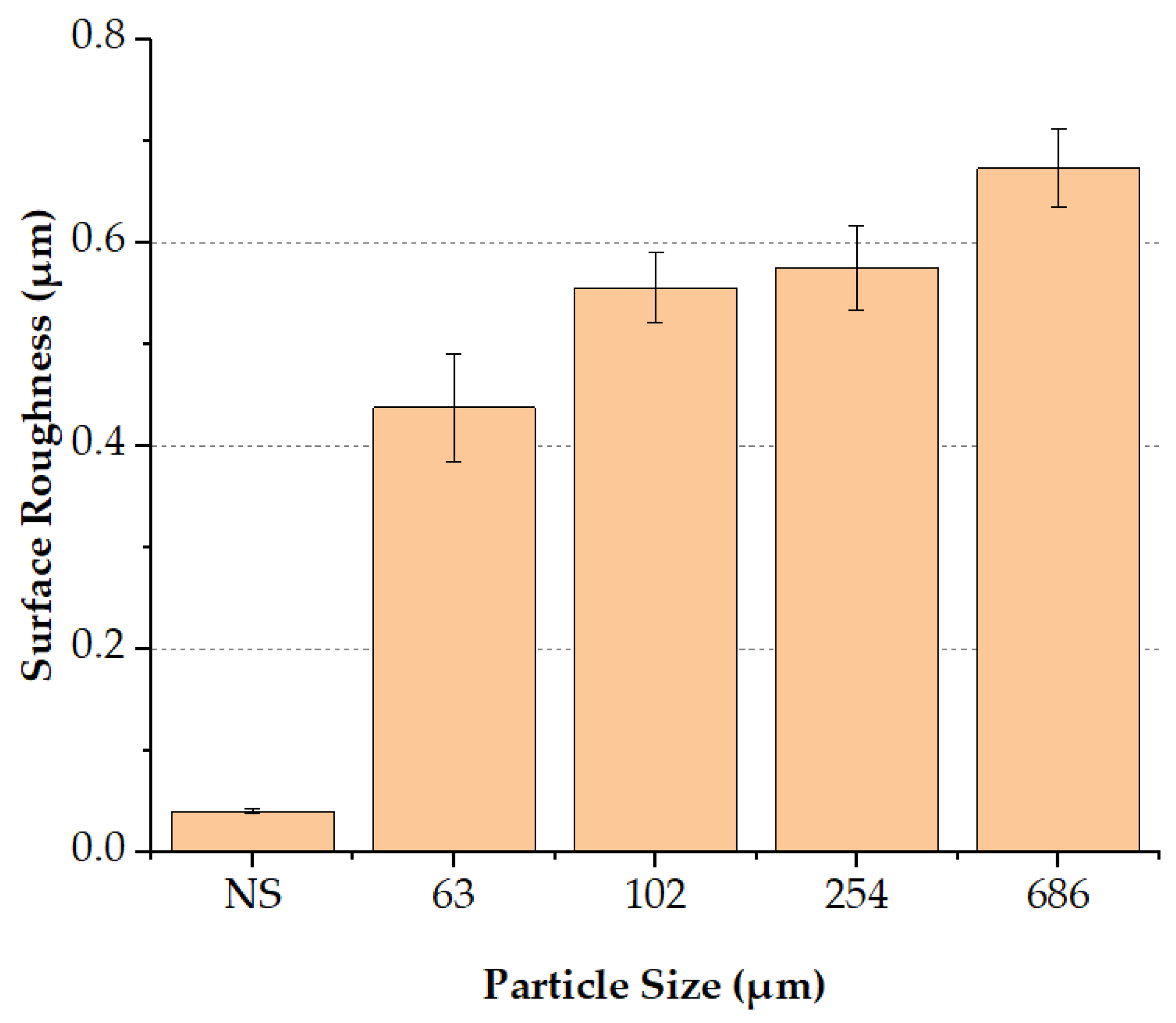
Figure 8.
Coping retention force comparison among sandblasting particle size variations.
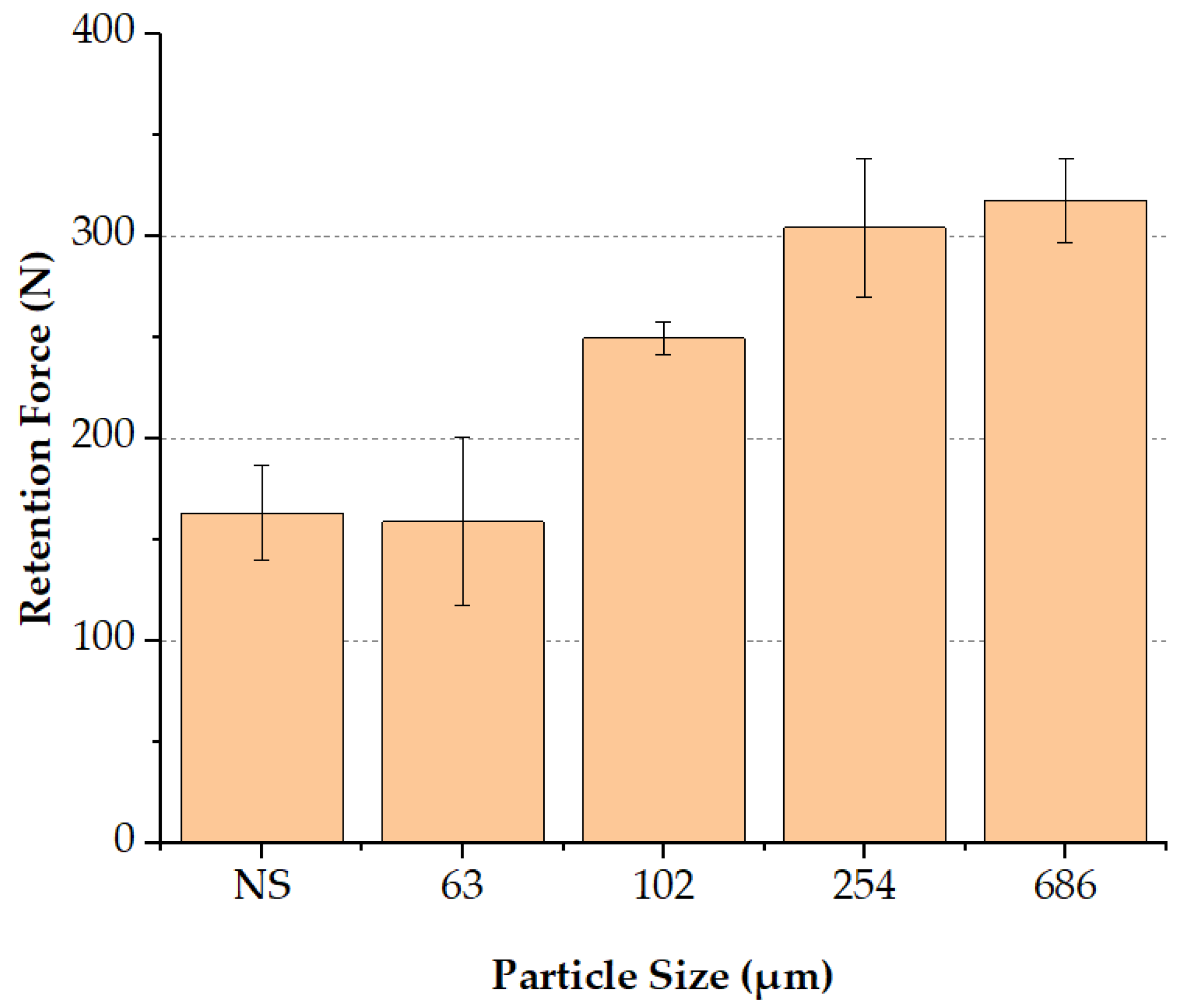
Figure 9.
Histogram of tightening torque capability of all subjects.
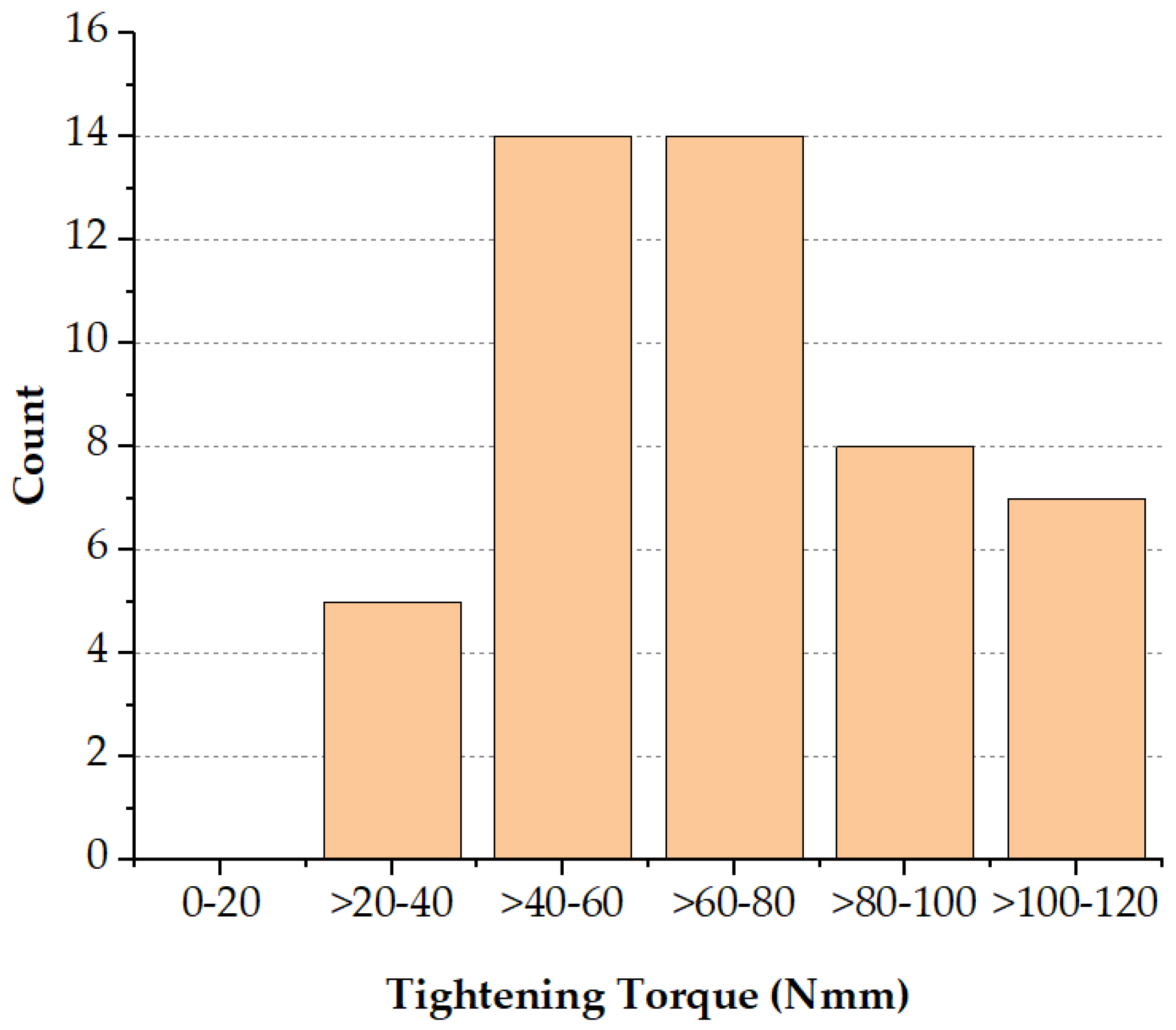
Figure 10.
Coping retention force comparison among variations of tightening torque groups.
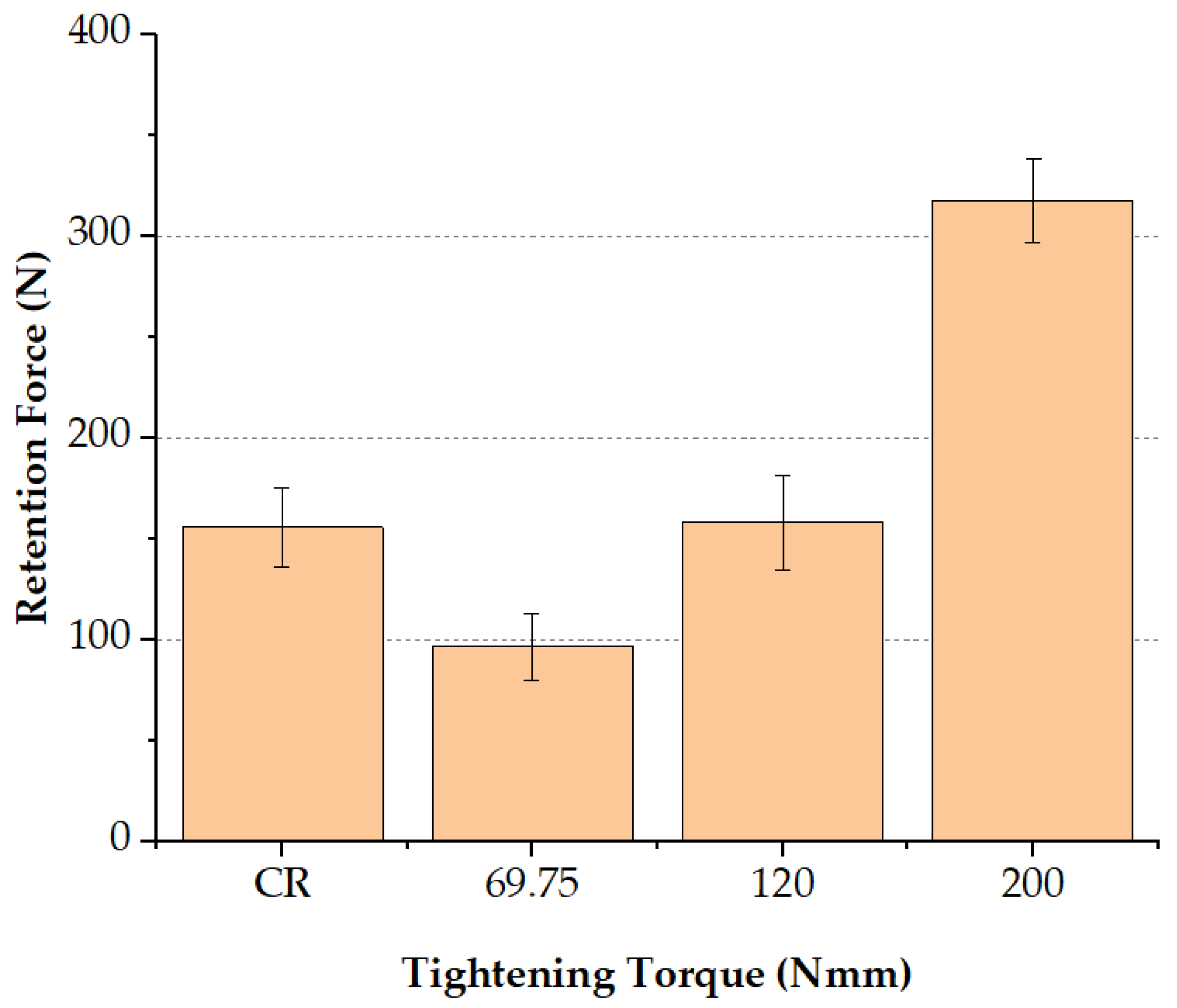

Table 1.
Retention force from each group in sandblasting using particle size variations experiment.
| Group | Sample | m) | Retention (N) |
|---|---|---|---|
| Not Sandblasted (NS) |
Sample 1 | 0.04 | 153.82 |
| Sample 2 | 0.04 | 129.28 | |
| Sample 3 | 0.04 | 191.93 | |
| Sample 4 | 0.04 | 177.05 | |
| Sample 5 | 0.04 | 165.02 | |
| Sandblasted 63 m (SB63 T200) |
Sample 1 | 0.35 | 135.36 |
| Sample 2 | 0.44 | 102.20 | |
| Sample 3 | 0.49 | 209.68 | |
| Sample 4 | 0.47 | 179.87 | |
| Sample 5 | 0.44 | 168.42 | |
| Sandblasted 102 m (SB102 T200) | Sample 1 | 0.55 | 251.86 |
| Sample 2 | 0.59 | 259.77 | |
| Sample 3 | 0.51 | 237.29 | |
| Sample 4 | 0.59 | 249.85 | |
| Sample 5 | 0,54 | 250.13 | |
| Sandblasted 254 m (SB254 T200) | Sample 1 | 0.51 | 305.06 |
| Sample 2 | 0.62 | 307.08 | |
| Sample 3 | 0.58 | 350.70 | |
| Sample 4 | 0.60 | 253.86 | |
| Sample 5 | 0.57 | 305,18 | |
| Sandblasted 686 m (SB686 T200) | Sample 1 | 0.73 | 320.07 |
| Sample 2 | 0.68 | 327.69 | |
| Sample 3 | 0.67 | 287.07 | |
| Sample 4 | 0.62 | 343.86 | |
| Sample 5 | 0.67 | 310.67 |
Table 2.
Summary of hand tightening torque data based on gender and overall data.
| Gender | Mean | Standard Deviation | Minimum | Maximum |
| Male | 75.28 | 24.94 | 34.67 | 120.67 |
| Female | 62.92 | 18.47 | 35.67 | 100.33 |
| Overall | 69.75 | 22.91 | 34.67 | 120.67 |
Table 3.
Retention force of each group.
| Group | Sample | Retention (N) |
| Cement Retained (CR) | Sample 1 | 153.33 |
| Sample 2 | 145.181 | |
| Sample 3 | 186.66 | |
| Sample 4 | 160.19 | |
| Sample 5 | 133.78 | |
| Lateral Screw (Tightening Torque 69.75 Nmm) (SB686 T69.75) |
Sample 1 | 100.33 |
| Sample 2 | 108.14 | |
| Sample 3 | 110.66 | |
| Sample 4 | 95.23 | |
| Sample 5 | 68.97 | |
| Lateral Screw (Tightening Torque 120 Nmm) (SB686 T120) |
Sample 1 | 161.828 |
| Sample 2 | 187.31 | |
| Sample 3 | 149.676 | |
| Sample 4 | 124.51 | |
| Sample 5 | 169.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



