
Submitted:
26 October 2023
Posted:
27 October 2023
You are already at the latest version
Abstract
Age estimation is an important tool when dealing with human remains or undocumented minors. Although the skull, the skeleton or the hand-wrist are used on age estimation as maturity indicators, they often present lack of good conditions for a correct identification or estimation. Few systematic reviews (SRs) have been recently published; therefore, this umbrella review critically assesses their level of evidence and provides a general comprehensive view. An electronic database search was conducted in four databases (PubMed, Cochrane, WoS, LILACS) up to December 2022, focusing on SRs of age estimation through forensic dentistry procedures. The methodological quality was analyzed using the measurement tool to assess SRs criteria (AMSTAR2). Eighteen SRs were included, five of critically low quality, six of low quality, three of moderate quality and four of high quality. The SRs posited that Willems’ method is more accurate and less prone to overestimation; most methods seem to be geographically sensitive; and 3D-Imaging and artificial intelligence tools demonstrate high potential. The quality of evidence on age estimation using dental approaches was rated as low to moderate. Well-designed clinical trials and high standard systematic reviews are essential to corroborate the accuracy of the different procedures of age estimation in forensic dentistry.
Keywords:
forensic dentistry
; age estimation
; dental maturation
; umbrella review
1. Introduction
Age estimation is a key forensic and archeological element. Often useful for human remains forensic identification, legal assistance involving minors or clinical diagnosis and planning, [1,2,3,4], is also helpful in mass migration and lack of valid identification [1,2,5]. Several methods have been developed to this end, among them, skeletal and dental development, sexual maturation or height/weight ratios [6,7].
Although the skull, the skeleton or the hand-wrist are used on age estimation as maturity indicators, they often present lack of good conditions for a correct identification or estimation [8,9]. Teeth are the hardest human organs and often found in adequate conditions [10,11,12]. Furthermore, dental measurements and indices are considered more useful and reliable, due to less variability during development as well as the greater resistance of teeth to systemic, environmental or destructive factors [6,13].
Estimating dental age may be achieved through several strategies depending on whether tooth development (around 20 years of age) or body development have been completed. On the one hand, methodologies based on teeth development are more accurate and with less margin of error [8,14]. On the other hand, the biological age of the individual is being estimated, always understood in a period of time, with some level of precision, and according to the method used. Chronological age will be included, at best, in this age range [12,14].
Several systematic reviews have been published with numerous dental methods based on radiographic (panoramic radiographs or otherwise) and non-radiographic approaches, most of them only evaluate one or two methodologies. Considering the variety and the discrepancy of the methods, it is helpful to compare and summarize the evidence previously published regarding age determination in Forensic Dentistry. This umbrella review intended to appraise the existing evidence on age determination procedures in forensic dentistry. Our focus was two-fold: to ascertain the quality of evidence and the overall clinical accuracy of each procedure.
2. Materials and Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [15] (Appendix S1) and the guide for systematic reviews of systematic review [16]. The review protocol was approved a priori by all authors and registered on Open Science Framework (DOI 10.17605/OSF.IO/CPBZY).
The Review question was: “What is the current evidence on age determination approaches in Forensic Dentistry?”.
Eligibility criteria
To answer the proposed research question, the inclusion criteria were: (1) systematic review (with or without meta-analysis); (2) addressing age determination in Forensic Dentistry; (3) absence of data duplication within the included studies in the meta-analysis. No restrictions on year of publication or language were applied.
Information sources search
Electronic data search was performed in four electronic databases: PubMed, Cochrane Database of Systematic Reviews, LILACS (Latin-American scientific literature in health sciences) and Web of Science. We merged keywords and subject headings in accordance with the thesaurus of each database and applied exploded subject headings, with the following syntax “((age determination) OR (age determination forensic) OR (age estimation) OR (dental age estimation) OR (forensic age estimation) OR (age estimation methods) OR (age prediction) OR (dental age prediction)) AND ((tooth) OR (teeth) OR (dental) OR forensic OR (forensic dentistry) OR (forensic odontology)) AND ((Systematic Review) OR (Meta-analysis))”. Grey literature was searched through three appropriate databases (opensigle.inist.fr, https://www.ntis.gov/, https://www.apa.org/pubs/databases/psycextra).
Study selection
Two researchers (JAN and LBL) independently screened titles and abstracts. The agreement between the reviewers was assessed by Kappa statistics. Any paper classified as potentially eligible by either reviewer was ordered as a full-text and independently screened by the reviewers. All disagreements were resolved through discussion with a third reviewer (JB).
Data extraction process and data items
Two researchers (JAN and LBL) independently extracted: authors and year of publication, objective/focused question, databases searched, number of studies included, type of studies included, main results and main conclusions. All disagreements were resolved through discussion with a third reviewer (JB).
Risk of bias assessment
Two researchers (JAN and LBL) employed the A Measurement Tool to Assess Systematic Reviews (AMSTAR 2) to determine the methodological quality of the included systematic reviews [16]. AMSTAR 2 is a comprehensive 16-item tool that ranks the overall methodological quality of a systematic review. Accordingly, the quality is ranked as follows: High means ‘Zero or one non-critical weakness’; Moderate means ‘More than one non-critical weakness’; Low means ‘One critical flaw with or without non-critical weaknesses’; and Critically low means ‘More than one critical flaw with or without non-critical weaknesses. The estimation of the AMSTAR quality rate for each study was calculated through the AMSTAR 2 online tool (https://amstar.ca/Amstar_Checklist.php).
3. Results
Study selection
Electronic searches retrieved a total of 738 titles. After manual assessment of title/abstract and deletion of duplicates, 34 potentially eligible full-texts were screened (Figure 1). Full-text screening excluded 16 studies with reasons (Supplementary File 1), resulting in eighteen systematic reviews that fulfilled the inclusion criteria. Inter-examiner reliability at the full-text screening was recorded as high (kappa score = 1.00).
SR characteristics
Overall, fourteen SRs [6,17,18,19,20,21,22,23,24,25,26,27,28,29] with meta-analysis and four without [30,31,32,33] were included (Table 1). Multiple sub-topics were investigated, such as imagiology methods based on panoramic x-rays [6,19,20,21,22,24,26], CBCT and CT [30,32] and MRI [17,30] (Table 1).
Methodological Quality
We observed excellent inter-examiner reliability at the RoB assessment (kappa score = 0.93; 95% confidence interval: 0.91-0.95).
None of the included SRs fully satisfied the AMSTAR2 Criteria (Table 2). Four studies were rated as of ‘high quality’ [6,21,26,27], three as of ‘moderate quality’ [17,22,25], six as of ‘low quality’ [18,20,28,29,31,33] and five as of ‘critically low quality’ [19,23,24,30,32].
When analyzing the major inconsistencies detected by the AMSTAR2: all studies did not report on the sources of funding for the studies included in the review (100%, n=18)[6,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]; 44.4% did not have data selection in duplicate (n=8)[18,22,23,24,25,28,30,32]; 38.9% of studies did not explain selection literature search strategy (n=7)[19,24,25,30,31,32,33]; and 33.3% did not have study selection in duplicate (n=6)[18,22,23,24,30,32].
Synthesis of Results
Overall, three main topics of research were found among the included SRs: panoramic radiographs-based methods; three-dimensional imaging methods; and artificial intelligence (AI)-based methods.
Panoramic radiographs-based methods
Overall, the level of evidence of the SRs focusing forensic methods based on panoramic radiographs was of low quality. Three main methods were the aim of research: Demirjian’s [6,20,21,22,23,24,26,33], Willems’ [21,22,25,26,28,29] and Cameriere’s [19,22,27,32].
As regards to Demirjian’s method, all studies are in agreement of an overestimation that varies between 4 to 9 months [6,20,21,22,24,26]. The majority affirm that this method is geographically sensitive [6,20,21,24] except the studies that are single-population oriented [22,26]. With respect to sex, two studies tend to overestimate the females [21,24], two showed more overestimation in males and lastly, one study reported that there were no differences between sexes [6] and one did not analyze sex subgroups [22]. Demirjian’s method was also applied solely to the 3rd molar in two papers. Haglund et al. [23] defined the accuracy of the method for the 18 years old threshold as 71% and Rolseth et al. [33] identified that the different development ranged from 4 to 7 years of the 3rd molar mineralization.
As for the Willems’ method, most studies showed a slight age overestimation, varying between 1 to 5 months [21,22,25,28,29], aside from one [26] that concluded underestimation by a month. They also conclude that males are more susceptible to this overestimation [25,26,28,29], except one [21], which concludes that females are more sensitive. One other study [22] does not analyze sex subgroups. Respecting age and geographic subgroups, some authors [21,25,28,29] reported differences between populations as the rest only studied a single population [22,26]; Esan et al., Yosuf et al. and Wang et al., also stated that a few age subgroups are more prone to overestimation [21,25,29].
Regarding Cameriere’s method, studies demonstrated overestimation that varied from 3 months to one year, making this variation slightly greater in males, but without statistically significant difference [19,22,32]. Marroquin et al. [32] also reported that in the Indian subpopulation, this variation can be as high as 10 years of overestimation. Cameriere also developed an index to assess the threshold of 18 years old with a percentage of correct classification ranging from 72 to 96%, with a better accuracy in males [27].
Kvall’s method [32] overestimates age between 1 to 2 and 12 to 13 years old and Chaillet’s method [18] within 6 to 8 months. Both methods overestimate more females and present different results when analyzing various geographical subpopulations.
Other methods included in this overview were only investigated by Franco et al. [22] for the Brazilian population. Nolla’s method demonstrated 2 to 3 months of overestimation, Lilequist and Lundberg’s method 1 to 2 months of underestimation, Mornstard’s 3 to 4 months of overestimation and lastly, Haavikko’s method underestimates between 10 to 12 months.
Three-dimensional imaging methods
Overall, the level of evidence of the SRs relating to forensic methods based on 3 dimensions imaging was of low quality.
Cone Beam Computed Tomography (CBCT) and Computed Tomography (CT) Scans reported different margin of errors, according to the method applied, ranging from 3,5 to 28 years [32]. When using pulp/tooth ratio, individuals were correctly identified between 30 to 90%, being the majority around 60% [30]. Both studies [30,32] agree that these values differ depending on the sex of the individual and the type of the tooth.
AI-based methods
The level of evidence on AI-based methods for sex prediction using dental measures was collectively based on low quality SRs. AI displayed precision and accuracy similar to trained examiners, overcoming the observer subjectivity. Although the accuracy, real-life testing and validation are yet to be proved [31].
4. Discussion
This umbrella review was able to sum up the evidence provided by the available SRs on age estimation methods in Forensic Dentistry. The collective knowledge is currently based on low to moderate-confidence evidence-based studies, at best, ranging between critically low to high quality. Overall, these results show that some forensic tools used nowadays might be outdated or misused, and some results must be analyzed with care, due to the lack of quality of many of the studies here referred.
Age estimation is a major step in forensic and archeological investigation [4]. Despite several methods have been developed to this end, approaches using dental tissues are among the most useful and reliable, due to their low changeability and greater resistance to degradation [7,13]. Most studies rely on methods developed upon bidimensional radiographic images, such as the Demirjian’s and Willems’ methods that have seen validation worldwide [6,18,19,20,21,22,24,25,26,27,28,29,32,33]. Both methods tend to overestimate age [6,20,21,22,23,24,25,26,28,29,33]. Cameriere’s method was first studied for several age groups and later as an index (I3M) that differentiates the legal threshold of 18 years old [19,22,27,32]. Other methods included are Chaillet’s, Lundbergs, Nolla, Mornstad, Haavik and Kval’s methods [18,22,32]. More recently, a few studies investigated the applicability of 3-dimensional imaging in forensic dentistry [17,30,32]. AI technology has already been tested for age estimation and seems a potential forensic tool [31].
Demirjian’s method obtained global acceptance and became the most widely used for dental age estimation [21]. Nonetheless, most studies concluded that this method is geographically sensitive and varies according to the subpopulation studied [6,20,21,24]. A possible reason for such a thing was the origin of this dataset (Caucasian subpopulation) with low heterogeneity, different from the other subpopulations studied [6,20,21,24]. Demirjian’s method tends to overestimate the age of the individuals, regardless of the sex of the subject. For such reasons, Demirjian’s method renders as a poor forensic tool when misapplied [20,24]
Willems’ method is also geographically sensitive [21,25,28,29]. Sehrawat et al. [28], for instance, determined that this method overestimates in the majority of the countries, except China and India. Sex seems to be a factor to consider because this method tends to overestimate more males than females [21,25,26,28,29].
Three studies comparing both Demirjian and Willems’ methods are all in agreement that the latter is more accurate and less prone to overestimation [21,22,26].
Demirjian’s method was introduced in the 1970′s and Willem’s method in the 2000′s. Since these methods (and most of the remaining methods) are based on the tooth maturation and this characteristic is growth dependent, it is likely to need to be updated on a regular basis. Growth patterns have evolved with the improvement of healthcare, nutrition and genetics so new methods must be developed to accompany the evolution of times [21,34].
Not only in Forensic Dentistry, dental methods and indexes have been misused. In Orthodontics, indexes such as Bolton, developed from a specific subpopulation, have been proven incorrect when generalized to other populations [35] .
Cameriere’s method is one of the geographically stable methods and tends to overestimate by 4 months, both boys and girls, without statistically significant difference [19,22,32]. According to Hostiuc et al. this method seems to outperform several others, including Dejirmijian and Willems methods [19].
Santiago et al. concluded that I3M was validated worldwide in several subpopulations since it has high accuracy in discriminating if an individual has reached 18 years of age, regardless of population studied. Regarding sex, a tendency of better results was observed for males, but high values of accuracy, sensibility, and specificity were also achieved for females [27].
Forensic age estimation based on dental measures has been, until recently, based on bidimensional imaging. 3-Dimensional imaging is gaining more relevance in all dentistry areas, including forensic dentistry with the first study that reported the use of this technology was published in 2004 [36]. CBCT and CT scans reconstructions allow the investigators to analyze the pulp/tooth volume ratio. The volume ratio might be an interesting tool for predicting age after root maturation of the 3rd molar, around the second decade of life [30]. Despite Micro-CT scans requiring the use of extracted teeth, the images are of greater quality and produce accurate measures because of more spatial resolution that of a CBCT; however, its application in live subjects is not viable and a model based in this type of imaging may not be replicable for forensic proposes in live individuals [30,32]. One major limitation of this method are the artefacts produced by adjacent metal structures and restorations, such as implants and amalgam fillings [30]. Also, the difficulty in reproduction of the site for measurements might lead to inaccurate analysis; the lack of a simple method of investigation should be the focus for the next researchers [30].
Due to the ethical implications of the usage of ionized radiation for other than diagnostic indications, MRI arose as a valid alternative since it uses strong magnetic fields and radio waves to generate imagens. It’s a relatively new tool in age estimation, published for the first time in 2015 [37]. Regarding the methodology itself, MRI can be used associated with other methods previously stated, such as Demirjian’s. MRI tends to be more accurate in the yearly stages of development but to be more challenging and inaccurate in the latter stages because of the lack of contract between dental and bone tissue. It also takes more time and is more expensive than an ordinary panoramic radiograph [30]. Due to the scarcity of research on this subject, the inter-ethnic variability is not yet proven [17]. Discrepancies between the MRI approaches make it inappropriate to pool data together and perform a proper systematic review with meta-analysis. Also, future age estimation methods based on MRI will probably be based on multifactorial sites and measures [17].
AI based automated systems have been developed to surpass the examiners subjectivity. The AI model that best performed was the Deep Learning Convolutional Neural Network approach, with similar accuracy when compared with trained researchers. AI models that combine a dual Convolutional Neural Network, first to predict sex and afterwards age, outperformed a single Convolutional Neural Network approach. However, AI based models have not proved themselves in the field to be routinely applied [31].
With the purpose of improving the quality of research, the checklist from TRIPOD [38] should be followed. The research question should be clearer with special emphasis on selection of study designs and reasons for exclusion. It would also enrich future SRs if they considered the RoB of individual studies as well as the number of authors that performed data extraction, to prevent bias.
Strengths and limitations
The present umbrella review has several strengths. Overall, these results provide a comprehensive overview of the available SRs on REP using a transparent and evidence-based methodology. We commend a cautious interpretation, as the individual studies included in each of the present SR were not explored. Thus, the conclusions lean on the interpretation of the systematic review’s authors.
5. Conclusions
Current evidence on forensic dentistry methods for age estimation is supported by low to moderate confidence systematic reviews. Willems’ method is more accurate and less prone to overestimation. Most methods seem to be geographically sensitive despite some authors attributing this heterogeneity to methodological errors. Cameriere’s index has high accuracy regardless of the population studied. 3D imaging an AI technology, although in the rise still lack field validation. This umbrella review reports the most common mistakes performed in SRs and will pave the way for more robust evidence-based research in the future.
Author Contributions
Conceptualization, V.M. and J.B.; methodology, J.N and L.B.L..; validation, J.B., V.M.; formal analysis, J.B..; investigation, J.N. and L.B.L.; resources, A.D.; writing—original draft preparation, J.N.; writing—review and editing, J.J.M. and A.D.; supervision, J.J.M and A.D,; project administration, J.J.M and A.D.. All authors have read and agreed to the published version of the manuscript.
Funding
This work is financed by national funds through the FCT—Foundation for Science and Technology, I.P., under project UIDB/04585/2020.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cameriere, R.; Pacifici, A.; Viva, S.; Carbone, D.; Pacifici, L.; Polimeni, A. Adult or Not? Accuracy of Cameriere’s Cut-off Value for Third Molar in Assessing 18 Years of Age for Legal Purposes. Minerva Stomatol 2014, 63, 283–294.
- Cunha, E.; Baccino, E.; Martrille, L.; Ramsthaler, F.; Prieto, J.; Schuliar, Y.; Lynnerup, N.; Cattaneo, C. The Problem of Aging Human Remains and Living Individuals: A Review. Forensic Sci Int 2009, 193, 1–13.
- Ritz-Timme, S.; Cattaneo, C.; Collins, M.J.; Waite, E.R.; Schütz, H.W.; Kaatsch, H.J.; Borrman, H.I. Age Estimation: The State of the Art in Relation to the Specific Demands of Forensic Practise. Int J Legal Med 2000, 113, 129–136. [CrossRef]
- Schmeling, A.; Geserick, G.; Reisinger, W.; Olze, A. Age Estimation. Forensic Sci Int 2007, 165, 178–181. [CrossRef]
- Angelakopoulos, N.; de Luca, S.; Velandia Palacio, L.A.; Coccia, E.; Ferrante, L.; Cameriere, R. Third Molar Maturity Index (I3M) for Assessing Age of Majority: Study of a Black South African Sample. Int J Legal Med 2018, 132, 1457–1464. [CrossRef]
- Yan, J.; Lou, X.; Xie, L.; Yu, D.; Shen, G.; Wang, Y. Assessment of Dental Age of Children Aged 3.5 to 16.9 Years Using Demirjian’s Method: A Meta-Analysis Based on 26 Studies. PLoS One 2013, 8. [CrossRef]
- Mani, S.A.; Naing, L.; John, J.; Samsudin, A.R. Comparison of Two Methods of Dental Age Estimation in 7-15-Year-Old Malays. Int J Paediatr Dent 2008, 18, 380–388. [CrossRef]
- Willems, G. A Review of the Most Commonly Used Dental Age Estimation Techniques. J Forensic Odontostomatol 2001, 19, 9–17.
- Priyadarshini, C.; Puranik, M.P.; Uma, S.R. Dental Age Estimation Methods: A Review; 2015.
- Capitaneanu, C.; Willems, G.; Thevissen, P. A Systematic Review of Odontological Sex Estimation Methods. J Forensic Odontostomatol 2017, 35, 1–19.
- Peckmann, T.R.; Logar, C.; Garrido-Varas, C.E.; Meek, S.; Pinto, X.T. Sex Determination Using the Mesio-Distal Dimension of Permanent Maxillary Incisors and Canines in a Modern Chilean Population. Science and Justice 2016, 56, 84–89. [CrossRef]
- Angadi, P. v.; Hemani, S.; Prabhu, S.; Acharya, A.B. Analyses of Odontometric Sexual Dimorphism and Sex Assessment Accuracy on a Large Sample. J Forensic Leg Med 2013, 20, 673–677. [CrossRef]
- Maber, M.; Liversidge, H.M.; Hector, M.P. Accuracy of Age Estimation of Radiographic Methods Using Developing Teeth. Forensic Sci Int 2006, 159. [CrossRef]
- Jeon, H.-M.; Jang, S.-M.; Kim, K.-H.; Heo, J.-Y.; Ok, S.-M.; Jeong, S.-H.; Ahn, Y.-W. Dental Age Estimation in Adults: A Review of the Commonly Used Radiological Methods. J Oral Med Pain 2014, 39, 119–126. [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 2009, 6, e1000097. [CrossRef]
- Burda, B.U.; Norris, S.L.; Holmer, H.K.; Ogden, L.A.; Smith, M.E.B. Quality Varies across Clinical Practice Guidelines for Mammography Screening in Women Aged 40-49 Years as Assessed by AGREE and AMSTAR Instruments. J Clin Epidemiol 2011, 64, 968–976. [CrossRef]
- de Tobel, J.; Bauwens, J.; Parmentier, G.I.L.; Franco, A.; Pauwels, N.S.; Verstraete, K.L.; Thevissen, P.W. Magnetic Resonance Imaging for Forensic Age Estimation in Living Children and Young Adults: A Systematic Review. Pediatr Radiol 2020, 50, 1691–1708.
- Diaconescu, I.; Isailă, O.-M.; Hostiuc, S. Accuracy of the Chaillet’s Method for Assessing the Age in Subadults. A Meta-Analysis. Curr Health Sci J 2021, 47, 196–203. [CrossRef]
- Hostiuc, S.; Diaconescu, I.; Rusu, M.C.; Negoi, I. Age Estimation Using the Cameriere Methods of Open Apices: A Meta-Analysis. Healthcare (Switzerland) 2021, 9. [CrossRef]
- Hostiuc, S.; Edison, S.E.; Diaconescu, I.; Negoi, I.; Isaila, O.M. Accuracy of the Demirjian’s Method for Assessing the Age in Children, from 1973 to 2020. A Meta-Analysis. Leg Med 2021, 52. [CrossRef]
- Esan, T.A.; Yengopal, V.; Schepartz, L.A. The Demirjian versus the Willems Method for Dental Age Estimation in Different Populations: A Meta-Analysis of Published Studies. PLoS One 2017, 12. [CrossRef]
- Franco, A.; de Oliveira, M.N.; Vidigal, M.T.C.; Blumenberg, C.; Pinheiro, A.A.; Paranhos, L.R. Assessment of Dental Age Estimation Methods Applied to Brazilian Children: A Systematic Review and Meta-Analysis. Dentomaxillofacial Radiology 2021, 50.
- Haglund, M.; Mörnstad, H. A Systematic Review and Meta-Analysis of the Fully Formed Wisdom Tooth as a Radiological Marker of Adulthood. Int J Legal Med 2019, 133, 231–239. [CrossRef]
- Jayaraman, J.; Wong, H.M.; King, N.M.; Roberts, G.J. The French-Canadian Data Set of Demirjian for Dental Age Estimation: A Systematic Review and Meta-Analysis. J Forensic Leg Med 2013, 20, 373–381.
- Mohd Yusof, M.Y.P.; Wan Mokhtar, I.; Rajasekharan, S.; Overholser, R.; Martens, L. Performance of Willem’s Dental Age Estimation Method in Children: A Systematic Review and Meta-Analysis. Forensic Sci Int 2017, 280, 245.e1-245.e10. [CrossRef]
- Prasad, H.; Kala, N. Accuracy of Two Dental Age Estimation Methods in the Indian Population - A Meta-Analysis of Published Studies. J Forensic Odontostomatol 2019, 3, 2–11.
- Santiago, B.M.; Almeida, L.; Cavalcanti, Y.W.; Magno, M.B.; Maia, L.C. Accuracy of the Third Molar Maturity Index in Assessing the Legal Age of 18 Years: A Systematic Review and Meta-Analysis. Int J Legal Med 2018, 132, 1167–1184. [CrossRef]
- Sehrawat, J.S.; Singh, M. Willems Method of Dental Age Estimation in Children: A Systematic Review and Meta-Analysis. J Forensic Leg Med 2017, 52, 122–129.
- Wang, J.; Ji, F.; Zhai, Y.; Park, H.; Tao, J. Is Willems Method Universal for Age Estimation: A Systematic Review and Meta-Analysis. J Forensic Leg Med 2017, 52, 130–136.
- Bjørk, M.B.; Kvaal, S.I. CT and MR Imaging Used in Age Estimation: A Systematic Review. J Forensic Odontostomatol 2018, 36, 14–25.
- Khanagar, S.B.; Vishwanathaiah, S.; Naik, S.; A. Al-Kheraif, A.; Devang Divakar, D.; Sarode, S.C.; Bhandi, S.; Patil, S. Application and Performance of Artificial Intelligence Technology in Forensic Odontology – A Systematic Review. Leg Med 2021, 48.
- Marroquin, T.Y.; Karkhanis, S.; Kvaal, S.I.; Vasudavan, S.; Kruger, E.; Tennant, M. Age Estimation in Adults by Dental Imaging Assessment Systematic Review. Forensic Sci Int 2017, 275, 203–211. [CrossRef]
- Rolseth, V.; Mosdøl, A.; Dahlberg, P.S.; Ding, Y.; Bleka, Ø.; Skjerven-Martinsen, M.; Straumann, G.H.; Delaveris, G.J.M.; Vist, G.E. Age Assessment by Demirjian’s Development Stages of the Third Molar: A Systematic Review. Eur Radiol 2019, 29, 2311–2321.
- Norris, S.A.; Frongillo, E.A.; Black, M.M.; Dong, Y.; Fall, C.; Lampl, M.; Liese, A.D.; Naguib, M.; Prentice, A.; Rochat, T.; et al. Nutrition in Adolescent Growth and Development. The Lancet 2022, 399, 172–184.
- Machado, V.; Botelho, J.; Pereira, D.; Vasques, M.; Fernandes-Retto, P.; Proença, L.; Mendes, J.J.; Delgado, A. Bolton Ratios in Portuguese Subjects among Different Malocclusion Groups. J Clin Exp Dent 2018, 10, e864–e868. [CrossRef]
- Vandevoort, F.M.; Bergmans, L.; van Cleynenbreugel, J.; Bielen, D.J.; Lambrechts, P.; Wevers, M.; Peirs, A.; Willems, G. Age Calculation Using X-Ray Microfocus Computed Tomographical Scanning of Teeth: A Pilot Study. J Forensic Sci 2004, 49, 787–790.
- Baumann, P.; Widek, T.; Merkens, H.; Boldt, J.; Petrovic, A.; Urschler, M.; Kirnbauer, B.; Jakse, N.; Scheurer, E. Dental Age Estimation of Living Persons: Comparison of MRI with OPG. Forensic Sci Int 2015, 253, 76–80. [CrossRef]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and Elaboration. Ann Intern Med 2015, 162, W1–W73. [CrossRef]
Figure 1.
PRISMA flowchart of included studies.
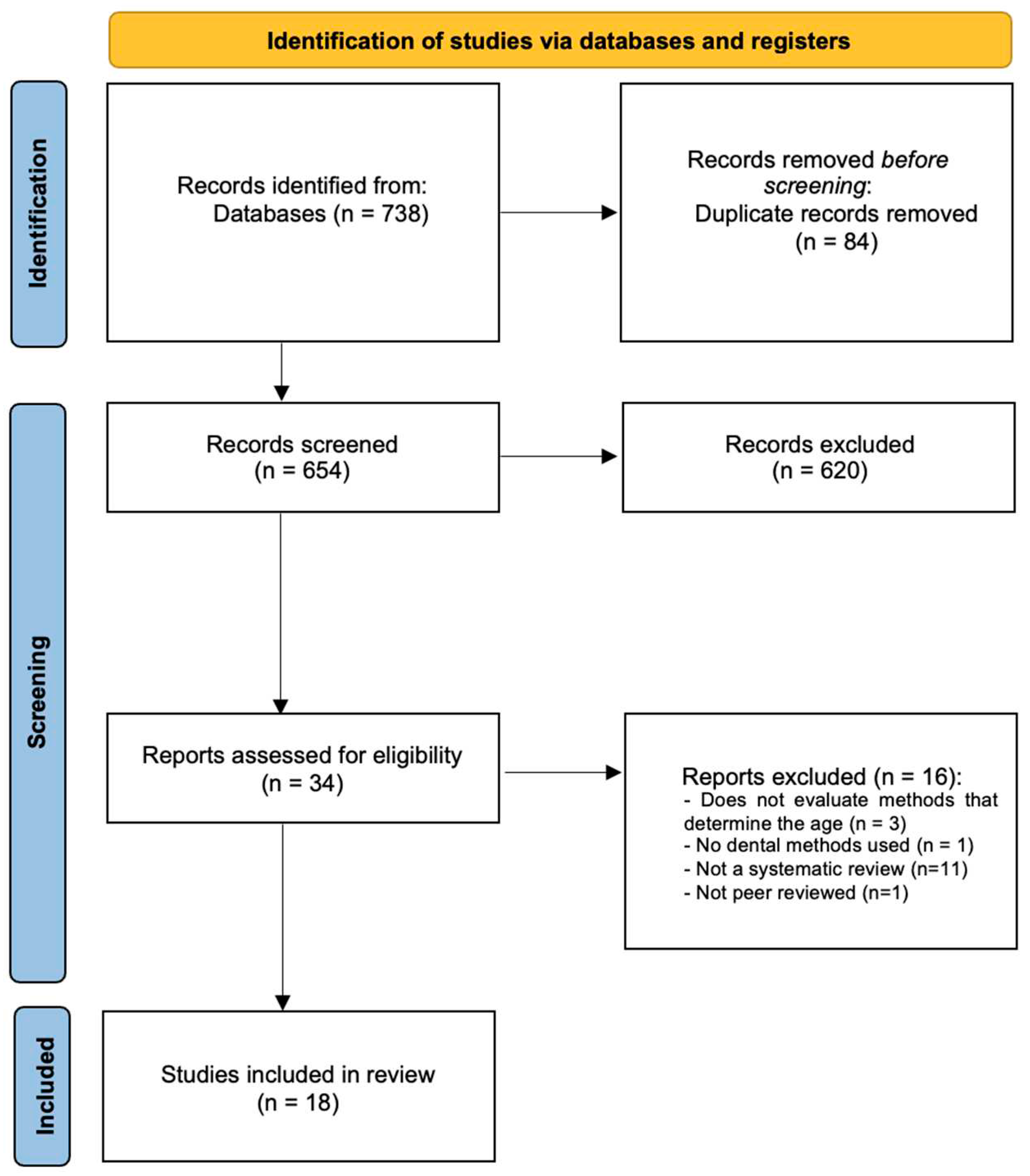

Table 1.
Characteristics of included SRs.
| Authors (year) | N | Search Period | Interventions | Quality Assessment Tool |
Sample | Method of Analysis | Outcomes | AMSTAR2 Score * | Funding |
|---|---|---|---|---|---|---|---|---|---|
| Bjork (2018)[30] | 27 | From July 2004 to September 2017 | CT and MR imaging | NI | RCTs | SR | Both CT and MR imaging may be useful tools in age estimation, but more research is needed | Critically Low | NI |
| De Tobel (2020)[17] | 55 | Up to September 2018 | MR imaging | EPOC overview and QUADAS-2 | 1 prospective cohort; 35 prospective CS; 19 retrospective CS | SR/MA | The age estimation performance was better for multifactorial age estimation than for single-site age estimation. MRI avoids the use of ionizing radiation and, consequently, allows for the study of multiple anatomical sites. | Moderate | NI |
| Diaconescu (2021)[18] | 25 | From 2013 to 2019 | Chaillet’s method | STROBE | RCTs | SR/MA | Chaillet’s method showed an age overestimation in both genders as shown for the majority ethnic groups, with a delayed dental development in Asian population, in contrast to the European one. | Low | NI |
| Esan (2017)[21] | 28 | Up to December 28th, 2016 | Demirjian’s and Willems’ methods | STROBE | 5 comparative CS; 4 CS; 17 retrospective CS; 2 observational CS | SR/MA | The Willems method provides more accurate estimation of chronological age in different populations, while Demirjian’s method has a broad application in terms of determining maturity scores. | High | None |
| Franco (2020)[22] | 13 | Up to January 2019 | Demirjian, Willems, Cameriere’s, Nolla’s and Lilequist and Lundberg’s methods | JBI Critical Appraisal Tools | CS studies | SR/MA | Most of the international methods for radiographic dental age estimation had optimal performance. | Moderate | Research Grant |
| Haglund (2018)[23] | 24 | Up to June 8, 2017 | Demirjian’s method for the 3rd molar | QUADAS-2 | RCTs | SR/MA | Not only that a fully mature third molar signifies adult age with a high likelihood, but also that a significant proportion of young adults (i.e., above the age of 18) have immature third molars. | Critically Low | NI |
| Hostiuc (2021)[20] | 89 | From 1973 to 2020 | Demirjian’s method | STROBE | RCTs | SR/MA | The Demirjian method overestimated the age by about half a year for both sexes. There are some geographical/ethnic differences. Despite that, this method is useful irrespective of the ethnic profile of the subjects. | Low | None |
| Hostiuc (2021)[19] | 15 | From 2005 to 2019 | Cameriere’s method | STROBE | RCTs | SR/MA | The Cameriere method of evaluating dental age on open apices is accurate enough for clinical practice, at least in the 7–14 age-interval. It should not be used outside this age range | Low | None |
| Jayaraman (2013)[24] | 34 | From January 1973 to December 2011 | Demirjian’s method | NI | RCTs | SR/MA | This method overestimates the age of the subjects by more than six months and hence this dataset should be used only with considerable caution when estimating age of group of subjects of any global population | Critically Low | None |
| Khanagar et al. (2021)[31] | 8 | From January 2000 to June 2020 | AI based models for personal age estimation | QUADAS-2 | NR | SR | AI technology displays accuracy and precision equivalent to that of trained examiners. These models have an added advantage of overcoming human errors and being non-invasive. Lack of real-life scenario and experimental nature of these included studies is a major limitation of the present review. | Low | Research Grant |
| Marroquin (2017)[32] | 32 | From January 1995 to July 2016 | Cameriere’s, Kvaal’s method, and CBCTimaging | NI | NR | SR | Age estimation methods based on pulp/tooth area ratio calculation reported more accurate results. It is recommended the use of dental age estimation methods, firstly pulp/tooth area ratio calculation of single first, upper canines and other single rooted teeth and secondly pulp/tooth length/with ratio calculation | Critically Low | NI |
| Yusof (2017)[25] | 23 | From January 2001 to September 2014 | Willems’ method | Cochrane handbook for systematic reviews-methodology review | NR | SR/MA | The use of Willems method is appropriate to estimate age in children considering its accuracy on different populations, investigators and age groups | Moderate | Research Grant |
| Prasad (2019)[26] | 20 | Up to July 2018 | Demirjian’s and Willems’ methods | QUADAS-2 | NR | SR/MA | Willems’ method predicted the chronological age more accurately than Demirjian’s method in the Indian population, irrespective of gender | High | NI |
| Rolseth (2018)[33] | 21 | Up to May 2016 | Demirjian’s method for the 3rd molar | QUADAS-2 | NR | SR | Variation in the timing of Demirjian’s development stages for third molars has often been interpreted as differences between populations and ethnicities. | Low | None |
| Santiago (2017)[27] | 15 | Up to November 2017 | Cameriere’s method (I3M) | QUADAS-2 | CS studies | SR/MA | The third molar maturity index is a suitable and useful method for estimating adulthood, since it has high accuracy in discriminating if an individual has reached 18 years of age, regardless of population studied. | High | None |
| Sehrawat (2017)[28] | 31 | From 2001 to January 2017 |
Willems’ method | NI | CS and Retrospective studies | SR/MA | Willems method of dental age estimation gives comparatively lesser overestimations of age than other methods reported in the available literature. | Critically Low | NI |
| Wang (2017)[29] | 11 | Up to February 28th, 2017 | Willems’ method | NOS | CS and Retrospective studies | SR/MA | Willems method overestimated dental age in almost every age group for both genders between 3.0 and 16.9 years old. In addition, ethnic differences were also shown to affect the accuracy of Willems method | Low | NI |
| Yan (2013)[6] | 26 | Up to July 12th, 2013 | Demirjian’s method | STROBE | CS and Retrospective studies | SR/MA | Demirjian’s method’s overestimation of actual chronological tooth age reveals the need for population-specific standards to better estimate the rate of human dental maturation. | High | None |
AI—artificial intelligence; CBCT - cone beam computer tomography; CS - Cross-sectional; CT-computer tomography, EPOC - effective practice and organisation of Care; JBI - Joanna Briggs Institute; MA—meta-analysis; MR- magnetic resonance; N—number of included studies; NI—no information; NOS - Newcastle-Ottawa Scale; NR—not reported; QAS—quality assessment tool. QUADAS—quality assessment and diagnostic accuracy tool; RCT - randomized controlled trials; SR—systematic review; STROBE-Strengthening the reporting of observational studies in epidemiology. * Detailed information regarding the methodological quality assessment is present in Table 2.
Table 2.
Methodological quality of the included SRs.
| First Author | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | Review Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bjørk et al. (2018)[30] | Y | PY | N | N | N | N | N | N | 0/0 | N | 0/0 | 0 | Y | N | 0 | Y | Critically low |
| De Tobel et al. (2020)[17] | Y | PY | Y | Y | Y | Y | Y | PY | 0/0 | N | 0/0 | 0 | Y | Y | 0 | Y | Moderate |
| Diaconescu et al. (2021)[18] | Y | PY | Y | PY | N | N | PY | N | N/0 | N | Y/0 | Y | Y | Y | Y | Y | Low |
| Esan et al. (2017)[21] | Y | Y | Y | PY | Y | Y | Y | PY | PY/PY | N | Y/Y | Y | Y | Y | Y | Y | High |
| Franco et al. (2020)[22] | Y | Y | Y | PY | N | N | Y | N | PY/PY | N | Y/Y | Y | Y | Y | Y | Y | Moderate |
| Hadlund et al. (2018)[23] | Y | PY | Y | PY | N | N | Y | PY | N/N | N | Y/Y | Y | Y | Y | Y | Y | Critically low |
| Hostiuc et al. (2021)[20] | Y | Y | Y | N | Y | Y | Y | PY | N/0 | N | Y/0 | Y | Y | Y | Y | Y | Critically low |
| Hostiuc et al. (2021)[19] | Y | PY | N | Y | Y | Y | PY | N | N/0 | N | Y/0 | Y | Y | Y | Y | Y | Low |
| Jayaraman et al. (2013)[24] | Y | N | N | N | N | N | Y | PY | N/0 | N | N/0 | N | N | N | N | Y | Critically low |
| Khanagar et al. (2020)[31] | Y | PY | N | PY | Y | Y | N | Y | PY/PY | N | 0/0 | 0 | N | N | 0 | Y | Low |
| Marroquin et al. (2017)[32] | Y | PY | N | PY | N | N | Y | PY | N/N | N | 0/0 | 0 | N | N | 0 | N | Critically low |
| Mohd Yusof et al. (2017)[25] | Y | Y | N | PY | Y | N | Y | PY | Y/Y | N | Y/Y | Y | Y | Y | Y | Y | Moderate |
| Prasad et al. (2019)[26] | Y | Y | Y | Y | Y | Y | PY | Y | Y/Y | N | Y/Y | Y | Y | Y | Y | Y | High |
| Rolseth et al. (2018)[33] | N | Y | N | PY | Y | Y | N | PY | Y/Y | N | 0/0 | 0 | Y | Y | 0 | Y | Low |
| Santiago et al. (2017)[27] | Y | Y | Y | Y | Y | Y | Y | Y | Y/Y | N | Y/Y | Y | Y | Y | Y | Y | High |
| Sehrawat et al. (2017)[28] | Y | PY | Y | PY | Y | N | PY | Y | N/N | N | Y/Y | N | N | Y | N | Y | Low |
| Wang et al. (2017)[29] | Y | Y | Y | PY | Y | Y | PY | Y | Y/Y | N | Y/Y | Y | Y | Y | N | Y | Low |
| Yan et al. (2013)[6] | Y | Y | Y | Y | Y | Y | Y | Y | Y/Y | N | Y/Y | Y | Y | Y | Y | Y | High |
0—No meta-analysis conducted, N—No, Y—Yes, PY—Partial Yes. 1. Are research questions and inclusion criteria included? 2. Were review methods established a priori? 3. Is there an explanation of the review authors’ selection literature search strategy? 4. Did the review authors use a comprehensive literature search strategy? 5. Was study selection performed in duplicate? 6. Was data selection performed in duplicate? 7. Is the list of excluded studies and exclusions justified? 8. Is the description of the included studies in adequate detail? 9. Is there a satisfactory technique for assessing the risk of bias (RoB)? 10. Is there a report on the sources of funding for the studies included in the review? 11. If meta-analysis was performed, did the review authors use appropriate methods for statistical combination of results? 12. If meta-analysis was performed, did the review authors assess the potential impact of RoB? 13. Was RoB accounted for when interpreting/discussing the results of the review? 14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? 15. If they performed quantitative synthesis, was publication bias performed? 16. Did the review authors report any potential sources of conflict of interest, including funding sources?
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



