Submitted:
25 October 2023
Posted:
27 October 2023
You are already at the latest version
Abstract
According to traditional Chinese medicine, Qi and Blood circulate through the human body via pathways known as 'channels and collaterals'. This process supports the normal function of internal organs and the whole body. Pathological conditions can be attributed to abnormal circulation of Qi and Blood, which results in excess or deficiency of organs and channels. Therapeutic methods used in traditional Chinese medicine restore the balance of Qi and Blood.Since acupuncture was introduced in Europe, discussion and debate about the nature of 'acupoints,' 'channels,' and 'collaterals' has continued. Currently, opposing views exist on this subject, ranging from complete denial of the existence of the channels to uncovering the previously unknown system of intra-tissue gaps and microscopic vessels. The author offers an original hypothesis that regards the theory of channels and collaterals as the description of the physiology and pathology of intercellular space and the theory of organs as a description of the physiology and pathology of cells.
Keywords:
Traditional Chinese Medicine
; TCM
; Integrative Medicine
; Acupoints
; Channels
; Collaterals
Introduction
According to traditional Chinese medicine (TCM), Qi and blood circulate through the human body via pathways known as ‘channels’ and ‘collaterals.’ Since acupuncture was introduced in Europe, discussion and debate about the nature of ‘acupoints,’ ‘channels,’ and ‘collaterals’ has continued. There have been fewer questions about the nature of the ‘organs’ that resembled the concepts of classic medicine.
Scientific medicine made a significant step forward when Rudolf Virchow (1821-1902) defined a disease as a cellular pathology [1]. However, from that time, any extracellular disorders were almost ignored or deemed as functional diseases or pathologies of the connective tissue [2]. Perhaps due to the concept of cellular pathology, the idea of the traditional Chinese medicine of the channels, gaps, or tunnels distributed within a human body did not find a proper understanding.
1. Modern Discoveries in Morphology of Acupuncture Points
According to many researchers, there are no unique structures at the acupuncture points that are not present in other areas. However, the acupoint has an unusual combination of common structures, which allows it to be distinguished as a particular formation.
1.1. Acupuncture points exist in humans, animals and plants
The morphological and functional heterogeneity of human skin is described in TCM as “acupuncture points” and “skin zones.” A similar morphological and functional heterogeneity is typical for warm-blooded animals, [3,4] such as elephants and dogs, [5,6] sheep, [7] goats, [7,8] donkeys, [7] rabbits, [7,9,10] cats, [7] horses, [6,11,12] pigs, [7,13] monkeys, [14] and birds, [15] as well as for frogs, [16] insects, [17] and plants [18,19].
At the end of the XIX century, a Russian doctor, Grigory Zahar’in, and an English physician, Henry Head, discovered that internal organs diseases were accompanied by skin hyperesthesia in a particular location. Later, hypersensitive skin regions related to sick organs were called Zahar’in-Head’s zones [20,21]. It was subsequently found that hyperesthesia zones may turn into hypoesthesia zones [22]. For example, it is known that in most patients an acute appendicitis is accompanied by hyperesthesia and vasodilatation in the projection area whereas the destructive form of appendicitis is marked by hypoesthesia and zone of dermal vascular constriction [23].
Among the other discoveries of the reflex zones we can name the points of McBurney, Lanz, Vaquez, Boas, etc. Most of the “modern” reflex zones have a segmental innervation in common with the sick organ [24,25,26]. When it comes to the motor points known in neurology, only a few of them are also acupuncture points [27,28].
In the fifties of the last century, a physician, Janet Travell, started actively using procaine injection into painful points to treat myofascial pain syndrome [29,30]. By the mid-80s, Janet Trevell, jointly with David Simons, came up with the theory of trigger points widely used by osteopaths, chiropractors, physiotherapists, and massage therapists for treating musculoskeletal system diseases. Unlike oriental medicine, based on the concept of vital energy (Qi) and its circulation in the human body, the theory of trigger points was based on the principles of European conventional medicine [31].
In the middle of the 20th century G. Soulié de Morant wrote that the modern Chinese name of an acupuncture point sounds as xue [穴] or kong xue [孔穴] translated as “depression” or “entrance to the cave.” [32,33]. Around the same time A. Podshibyakin found that acupuncture points have increased oxygen consumption and increased temperature; he proposed to call them “biologically active points” (BAP) [16,34,35]. Both definitions suggest that an acupuncture point is an area on the skin surface with the access to the active structure located inside the body.
1.2. Palpation of acupuncture points
Surface palpation of the BAP area will reveal a loosened-up tissue and an insignificant indent in the skin and the muscle [16,34] due to the thinning of the epidermis and a different areolar structure of the connective tissue in that area [38,39]. The location of BAP on the skin of cadavers manifests itself by small retractions that correspond histologically to the fibers of connective tissue positioned perpendicular to the skin surface and containing neurovascular elements stretching through all layers of the skin and reaching the epidermis [40].
Relatively looser surface epithelium in the BAP area permits identification by palpation or by a metal probe with a rounded 2-3 mm diameter tip, as well as with an acoustic instrument that detects the changes of sound produced by the friction of the instrument against the skin surface [41].
1.3. General morphology of acupuncture points
Morphological studies around the acupuncture points have not revealed any unusual structures that cannot be found in other parts of the body, [26,46,47,48] which sometimes leads to the conclusion that BAPs do not exist de facto and are nothing but topographic or reference points on the skin surface [49].
According to other authors a BAP may be defined both as a functional unit and as a morphological formation where the effect of therapy with acupuncture is different from the effect outside the point [44].
As a general rule the elements of the nervous and vascular system, as well as various cells are identified around the acupuncture points. J. Bossy, studied the morphology of numerous BAPs and in 42% of cases found subcutaneous nerves; in 40% the veins with subcutaneous perivascular nerve plexus, and in 18% cases found subcutaneous arteries [50]. In other laboratories, subcutaneous nerves, veins, and arteries were found in the area of BAPs in 80% of the cases [51,52]. P. Rabischong et al. reported the usual presence of spiral-shaped vascular plexus surrounded by nerve fibers of cholinergic type lacking myelin in BAP areas [39].
Some authors have attempted to correlate acupuncture points with specific nerves, blood vessels, or their branches [53]. However, the analysis of a wide variety of morphological studies makes one doubt that the nerves, the blood vessels, or specific cells form the basis of an acupuncture point.
In 1959, G. Novinsky found that an areolar connective tissue with increased hydrophilic properties is typical for BAP projection area [54]. For that reason it is easier to separate the skin of cadavers from the underlying tissue in the BAPs than in other parts of the body [41]. Furthermore the epithelium around BAPs is thinner and looser and the fibers of the connective tissue are perpendicular to the skin surface [26,55].
A special role is attributed to the morphological peculiarity of BAP in fascia in the places where neurovascular bundles or nerve fibers are reaching out from the depths to the surface layers of the skin [40,56,57].
Fibers of connective tissue are located alongside such structures in such a way that the surface layers of the skin are connected to the parts deep inside the body. All cutaneous branches of spinal nerves perforate skin at least once and that area precisely coincides with a particular BAP [38,58] The feeling that the needle is “falling through” in the acupuncture point familiar to all practitioners is most likely due to the needle hitting such perforation of surface fascia [44].
According to N. Verzhbitskaya et al., BAP includes two morphologic-functional components: “channel of the point” and “locus” or the active area of the point [59,60].
“Channel of the point” linking the skin’s surface with a locus is formed by the epithelium and connective tissue fibers. There are few cellular elements, nerves, and blood vessels within a channel compared to the surrounding tissue, which makes penetration of the needle easy and painless to the depth of the “locus” located in subcutaneous fat tissue or between muscles and tendons [59].
The “locus,” or an active area of the point, is formed by loose connective tissue reminiscent of a polymorphic flask. A high content of nerves, vessels, and cells with a high content of heparin, histamine, acetylcholine, serotonin, catecholamines, and other active substances characterizes it [59,60,61]. The estimated schematics of the acupoints are shown in Figure 1 [62].
According to morphologic studies, different nerve receptors and free nerve ends are abundantly represented in acupuncture points [48,63]. The presence of a certain receptor depends on the localization of the points. The encapsulated receptors include Meissner’s and Pacini’s corpuscles, bulbos terminales Krause, muscle spindles, and spindle tendon (Golgi tendon organ) [26,38,63,64].
The number of nerve fibers per section of the tested dermis in the auricular points exceeds about two to three times the number of them in the dermis of the control skin areas [64,65]. Examination of BAP areas with ultrasound demonstrated that the receptors and the nerve structures presented within these areas and outside are different [66].
A comparison of the acupuncture points along the pericardium channel revealed increased nerve structure density in the distal direction [64]. Other studies found that the number of sensory fibers in a distal part of an arm eleven times exceeds that of a forearm and almost twenty times that of a shoulder [67]. The receptor apparatus of the acupuncture points is similar to the reflexogenic zones of Zahar’in - Head, McBurney, Mac-Kenzie, Vidal, and others [68,69].
The Laser Doppler flowmetry revealed that the blood flow through the microcirculatory vessels in the area of acupuncture points (GI-4 and V-64) is significantly higher than in the surrounding tissue [70].
Fibroblasts, histiocytes, leukocytes, and mast cells may be discovered at the active area or “locus.” [60,61]. The number of mast cells is more significant in the area of acupuncture points than in the areas outside the points. Mast cells found in the area of acupuncture points have a high content of biologically active substances such as histamine, serotonin, and heparin, which affect vascular permeability, microcirculation, tissue metabolism, and skin conductivity. The number of cells with signs of degranulation increases after acupuncture treatments, and a preliminary blockade of degranulation of mast cells leads to the decreased effect of acupuncture [71].
In the area of acupoints, many gap junctions are detected. Gap junctions connect cells to ensure intercellular transporting cytoplasm and dissolved substances, including c-AMP, RNA, and low molecular weight proteins. Increased concentration of gap junctions leads to high electrical conductivity of skin at acupoints area [72,73,74].
The evaluation of a microwave signal reflected from the skin surface led to the conclusion that BAPs are more hydrated as compared to the control skin areas [75].
Modern diagnostic methods permit specifying the shape and macroscopic localization of the point’s active areas. For example, X-ray fluorescence analysis revealed that the acupuncture points of the extremities are elliptical with elongated axis alongside the meridians [76]. In another experiment, acupuncture needles were introduced in Bl-25 (Da Chang Shu) and Bl-26 (Guan Yuan Shu) points with subsequent manipulation to achieve sensory reactions propagated along the channel. Computer tomography revealed that the localization of the above points corresponds to the intermuscular septum between the spinal erector (m. Erector spinae) and transversospinal muscle (m. Transversospinalis) [77].
2. Modern discoveries in physiology of acupuncture points
Morphological differences in acupuncture points suggest functional differences between the acupoints and the surrounding skin. These distinctive features are reduced electrical resistance of the skin, increased electrical capacity, high thermal conductivity, low-frequency electrical signals, and other “abnormalities.”
2.1. Reduced skin resistance of the areas of the acupuncture points
In the early 1950s, a Japanese doctor, Yoshio Nakatani, found a reduced electrical resistance around the points and developed a diagnostic method based on conductivity measurements at specific points of each channel [78,79,80]. Around the same time, similar studies were conducted by other scientists, including A. Podshibiakin in the USSR, [35] J.E.H. Niboyet in France, [81,82] and R. Voll in Germany [83,84,85]. Subsequently, the electrical “anomalies” of the skin in the area of BAP were studied by T. Ischikava, [86] C. Ionescu-Tirgoviste, [87] I. Dumitrescu), [88,89] F. Portnov, [90] P. Chan, [91] and numerous other researchers.
The electrical resistance of the skin for indifferent areas varies from 250 Kilo-Ohm to 1 or 2,74 or 10 Mega-Ohm,[55,88] but in the area of the acupuncture points, it could be reduced up to 20 ÷ 60 Kilo-Ohm [55,81,92]. In the studies of A. Podshibiakin, the resistance at acupuncture points with the negative active electrode was 20 ± 10 Kilo-Ohm. With a positive electrode, it initially went down but subsequently increased within 20-60 seconds to 0.4 ÷ 0.5 Mega-Ohm [16]. Due to low resistance in acupuncture points, they may be visualized in the high-frequency corona discharge of AcuVision device [62,93] (Figure 2).
Localization of the electrically conductive spot in the same person may be displaced in any direction to a distance of up to 1 cm and even more; [16,94] however, the localization of the electroconductive points predominantly coincides with the localization of the acupuncture points.
The size of an electrically conductive spot varies from 1mm to 10 mm. During sleep and after creative workload, the diameter of the point is reduced to 1 mm; after waking, it may increase to 10 mm. During a disease, the size of conductive spots may increase so that individual “points” overlap and form vast areas [16,95].
The highest electrical conductivity was found at the points located on the head. In the central part of the body (for example, around the sacrum), the conductivity is higher than on the limbs, where it decreases as it approaches the fingertips and toes [96].
In the case of certain conditions, the conductivity of a point may be the same as that of the surrounding skin areas or even lower [96]. In some studies of healthy individuals, no points with reduced conductivity were found; therefore, some authors argue that there is no difference in electrical resistance between acupuncture points and surrounding skin [97]. However, in most cases, there are more points with reduced electrical resistance than the known acupuncture points [98].
Given the fact that it is not always possible to find the complete correlation between the detected points of electrical conductivity and the “acupuncture points” [98,99,100], it is possible to assume that this is due to the functional displacement of the conductive patch only. However, the main component of the point (locus) most likely remains at the standard location without any displacement.
Transplanted skin loses its original properties immediately after separation from its original location and acquires the electrical characteristics of the skin area of the new location. As a result, lowered resistance typical for the “points” appears in the skin transplanted from an indifferent area to an acupuncture point [101,102]. Conversely, low resistance is no longer observed when skin is transplanted from the BAP region to a common area. Given the above, some authors assume that an “acupuncture point” is a complex unit associated with specific deep structures [103].
Even though electrical parameters in acupuncture points are susceptible to fluctuations depending on many internal and external factors, the average daily indexes of electrical resistance in specific “points” registered under constant conditions are relatively stable and reflect the individual characteristics of the subjects [104].
The study of the semi-conductivity of the points revealed the coincidence of the changes with the daily dynamics of atmospheric electrical conductivity. At maximal conductivity of the atmosphere (as a general rule at night), the electrical conductivity of the points goes down and increases with the change of weather [105].
Electrical conductivity in men and women reduces to minimal at night between 2:00 a.m. and 5:00 a.m. and coincides with a deep sleep. In the daytime, the dynamics of electrical conductivity depend on the gender of the subjects. In men, maximum values were found between 11 a.m. and 2:00 p.m., and in women, between 4:00 p.m. and 9:00 p.m. [106].
In the days of high geomagnetic activity (high K-index), the resistance at the points was 40-80% higher than the daily average calculated for the days with low K-index [104]. Conductivity is maximal in the periods of low geomagnetic activity [107]. Long-term observations found a decrease in electrical conductivity in winter and an increase in summer correlating with average monthly air temperature [106].
Note: Geomagnetic activity indices are intended to describe the variations of the Earth’s magnetic field. K-index - is a quasi-logarithmic index (incremented by 1 with disturbance increasing approximately two times). It is calculated according to the data of a specific Observatory for the three-hour periods. The index was introduced by J. Bartels in 1938 and ranges from 0 to 9 for each three-hour interval (0-3, 3-6, 6-9, etc.) of the Greenwich Mean Time. In order to calculate the index, the change of the magnetic field within a three-hour interval is taken, and a regular part (determined by calm days) is subtracted from it. The resulting value is converted into a K-index according to a special table [108].
Numerous authors have reported that the electrical conductivity of specific points depends on the changes in physiological and pathological conditions of the associated channels, organs, and the body as a whole [80,85,109]. It was found that the Bl-64 (Jing-Gu) point’s electrical conductivity increases when the person wakes up and decreases during sleep. It is reduced in case of a reduction of overall reactivity, but it does not change with psycho-emotional stress [110].
Electrical resistance in the BAPs also depends on the autonomic nervous system condition. It increases when the activity of the sympathetic division of the autonomic nervous system is below the normal condition [46].
The change in conductivity is observed in the presence of macroscopic structural changes in the skin. In patients with psoriasis, the resistance around the papules is lower than in the surrounding skin and even lower, closer to acupuncture points in the area of the papules [9]. The study of the location of birthmarks, moles, and nevi revealed that they frequently coincide with the acupuncture points. In both cases, the reduced electrical resistance of the skin was observed [111]. However, nevi, birthmarks, and moles do not possess high thermal conductivity, which is typical for acupuncture points [111].
Electrical heterogeneity of the skin persists from several days to one week after death. This phenomenon was revealed in the parts after the dissection of cadavers and for the whole cadavers [81,88,112,113,114]. Skin heterogeneity on amputated limbs is observed for up to three days [9,59] The difference in resistance between the points and the surrounding skin is far more considerable on the cadavers than on living humans and animals [82,92,115,116]. Electrical heterogeneity in cadavers disappears gradually due to autolytic processes that cause the physical parameters of the skin to align [40,81,82,92,115,116]. They concluded that the structures located in the area of electrically abnormal points are more stable than in the surrounding skin area [9].
However, one can assume that the high electrical conductivity of the skin in the area of acupuncture points is associated with the absence of insulating structures. Thus, the conductivity function does not require metabolic activity, so it creates an impression of stability of the acupoints after death.
2.2. Electrical potential and action potential in the “acupuncture points”
In 1825, professor of Physics Claude Pouilett was the first to use a galvanometer to discover the electrical potential between the needle inserted into the acupuncture point and an oral mucosa [117].
The study of electrical potentials (EP) in different skin areas revealed differences in potentials between the centers of the acupuncture points and the surrounding skin. EP may vary from 2 to 300 mV, decreasing with the distance from the center. Average values of the difference in potential may vary during the day, reflecting the moderate fluctuations in the functional activity of internal organs [16,35,96,118].
Thus, an increase of the EP in the urinary bladder meridian points is observed when the bladder is full and returns to normal after emptying. An increase in EP of the Stomach meridian points will follow if a patient is suggested under hypnosis that he had eaten well. Novocaine blockade causes a decrease in the EP [35].
Some authors have noted slow, low-amplitude irregular fluctuations of the electrical potential ranging from 0.1 to 1.0 Hz with amplitude from 50 to 500 mV. This biological potential is constant and subject to the general laws of galvanic skin response [119].
An above-normal difference of (electrical) potentials may indicate the presence of a disease, a predisposition to one, or the presence of a residual pathology in a relevant organ [16,35,118,120,121,122]. Electrical potential in the point has a tendency to decrease as recovery progresses [122].
When acupuncture is used on the points with deviated electrical potential, a reflex reaction is observed in the corresponding internal organ. According to A. Podshibiakin, a positive effect from treatment, was observed when electrical potentials in the active points of the skin exceeded 25 mV. Treatment of the acupoints with electrical potential under 10 mV (especially – 1 mV) has a negative effect on the analogous electrical current used for treatment [118].
The pattern of electric potential distribution on the skin persists for several days after death until autolytic processes reduce the difference to a minimal one that can no longer be recognized [118].
Apart from an electrical potential at the BATs, they also can register an action potential (AP) of a high-frequency impulse activity. AP fluctuations’ frequencies vary from 0.5 Hz to 400 Hz and have amplitude from 0.1 to 1.5 mV and duration of 0.3 – 1.25 milliseconds. AP in the “point” is registered only alongside certain sensations and may last 20-30 minutes [123]. The frequency characteristics of AP are higher with active pain syndrome and go down with pain relief. The maximum values of AP are recorded at inspiration [123,124,125,126].
Action potential in auricular points is detected only in the presence of a pathological process in the relevant organ and disappears as recovery progresses [46].
2.3. Other Electrical Characteristics of “Acupuncture Points”.
Study of the volt-ampere characteristic in BAP areas revealed nonlinear curves including an S-shaped curve with a part of a negative differential resistance. This data suggest that the tissues surrounding BAPs may possess generating properties and may convert a direct electric current into alternating [127].
Apart from high conductivity the acupuncture points have capacitive characteristics that permit them to accumulate and keep an electrical charge much longer than the surrounding tissues. According to the research of I. Dumitrescu the capacity in the area of the points may reach 0.5 microfarad whereas the capacity elsewhere does not exceed 0.01 microfarad [128,129].
2.4. Skin temperature parameters around acupuncture points
Studies by A. Podshibyakin in the mid-20th century found high activity of metabolic processes and an increase in local temperature in acupuncture points. Other authors confirmed his results [16,132].
A comprehensive study of the BAP’s functional condition indicates that the activated points are hot, and the non-active ones are cold. Therefore, the “points” condition may prompt the treatment technique [133]. Specific pathologies cause the increase of hot “point” or zone size alongside the heat emission [134].
A change in temperature sensitivity around acupuncture points was noted alongside the temperature changes. A Japanese doctor Kobe Akabane, was one of the first to discover this phenomenon. In 1952, K. Akabane treated the right side tonsillitis with hot foot baths. During one of these procedures, he noted that the little finger of the right foot was not as sensitive to hot water as the little finger of the left foot. After the recovery, he noted that the sensitivity was normal and symmetrical. Several experiments led Akabane to the conclusion that the functional activity of a meridian affects the thermal and pain sensitivity of the endpoints of the meridians (Jing) [135]. Subsequently, N. Bogdanov found the changes in the thermal sensitivity of auricular points corresponding to specific pathological processes [124,136].
The high thermal conductivity of skin around the acupuncture “points” led to the hypothesis that the “points” serve as a kind of sluice channel for heat exchange between the body and the ambient environment [42,94,137].
The high thermal conductivity of skin in the area of the points can be used to determine the location of the “points accurately.” When a metal probe moves slowly and without pressure around an acupuncture point, a patient feels something like a “drop of cold water” on the skin (with increased thermal conductivity) at the acupoints. Individual temperature sensitivity differs, so using several probes of different heat capacities is necessary.
Acupuncture and moxibustion permit the change of a natural heat transfer. The needles have an effect similar to cold and increase heat emission from the points to the environment [42,137,138]. Within the first minute after a needle is inserted into a point, the radiation temperature in that area increases by 0.4 - 2.3 ° C, and at a distance of 5 cm from the needle, it is reduced by 0.6 - 3.0 ° C. The temperature on the needle handle fluctuates between the values in the BAP zone and those at a distance of 5 cm from the BAP. 2-6 minutes after insertion of the needle, the radiation temperature of the skin around it continues to increase as it goes down on the farther skin areas. If a needle is not extracted for the next 30-40 minutes, the temperature of the BAP area gradually goes down and becomes significantly lower than it was initially [138].
2.5. Relationship between electrical, temperature, and other point parameters
According to A. Wein, a skin temperature indirectly reflects the condition of the parasympathetic division of an autonomic nervous system, and electrical conductivity reflects the condition of the sympathetic division of an autonomic nervous system [139].
Some studies found the relationship between conductivity, temperature, and pain sensitivity in acupuncture points. As a general rule, an increase in temperature in the points is accompanied by an increase in conductivity, [96] and an increased conductivity in the points correlates with the intensity of pain [140,141]. However, A. Nechushkin found no direct correlation between pain sensitivity, electrical conductivity, and temperature at the points [142].
2.6. Other “physical anomalies” of acupuncture points
Other peculiarities of the acupuncture point areas have also been identified apart from the electrical and thermal “anormalies” that distinguish such areas from the surrounding skin.
According to A. Podshibyakin, BAP areas have increased oxygen absorption and release of carbon dioxide. Initially, the increased molecular oxygen tension starts to drop right after achieving the “De Qi” or “De Chi” phenomenon, which is observed at the treated point and other points of the same channel [16,143]. High functional activity of the BAP area is accompanied by increased incorporation of radioactive phosphorus (Р32) [144,145,146].
Research with laser instruments detected mechanical vibrations of the needle’s handle inserted into acupuncture points. The oscillation frequency was within two ranges: from 7 to 10 Hz and 15 to 20 Hz, in contrast to the surrounding skin, where only noise spectrum vibrations were found [147]. Periodic mechanical activity at points was not related to the pulsation of the arteries [148].
Feeble spontaneous visible light (ultra-weak photon emission) was detected around the end (Jing) points of the channels, with the intensity of such light increasing mainly on the channels associated with a sick organ [149]. Measurement of the light diffusing properties found a more intense absorption in the visible light around BAPs compared to indifferent skin areas [150,151]. The values of the light diffusion coefficient at the points reach maximum at noon, at 6:00 p.m., at midnight, and at 3:00 a.m. The values are minimal at 6:00 a.m., 9:00 am, 3:00 pm, and 9:00 pm [151]. The diseases of internal organs change the diffusing properties of the points. A short laser exposure (under 60 seconds) reduces light diffusing properties, and after a long-term exposure (60-120 seconds) returns it to the initial level [152]. Increased skin sensitivity to high-frequency electromagnetic radiation was also observed in BAP areas [75,153].
Due to the variety of the above properties of “acupuncture points,” some authors suggest that the “points” play the role of multifunctional receptors, [52] capable of responding to signals of different natures, including electric, magnetic, and electromagnetic fields [132,154,155,156,157]. In this case, the inserted acupuncture needle can be an antenna that captures electromagnetic waves of a specific range [158].
Summarizing the above and taking into account the Chinese characters 孔穴 (Kong Xue), used for acupoints and translated as a “aperture”, “cavity” or a “hole,” [159,160,161] we may conclude that the acupuncture point is a locus in the skin where a loosening of surface epithelium and specific connective tissue organization create an invisible “hole” which provides “access” to the inside the body. A large number of active elements discovered inside the “hole” turn the acupoint into a complex functional unit that facilitates interaction between the internal and external environment of the body. (Figure 1).
3. Modern discoveries in morphology of channels and collaterals
According to TCM theory, Qi and blood circulate along specific paths called “channels and collaterals.” There are twelve Regular channels and the associated secondary vessels, including tendon-muscular channels (or sinews, or muscle regions), Luo channels or collaterals, and divergent channels as well as extra-channels (Figure 3).
Centuries ago, a famous Chinese doctor, Li Shizhen, wrote: “... there are tunnels within the body and the one turning his mental gaze into himself may illuminate them...” [162].
European anatomists and physiologists have been trying to unravel the nature of channels for several centuries. The results of these studies and suggested hypotheses, which may be divided into the following groups:
- Denial of the possibility of the existence of the system of channels and collaterals;
- The theory of channels describes nervous and vascular systems;
- The theory of channels describes muscles and subcutaneous tissue;
- The theory of channels describes a system of electrical conductors and semiconductors;
- The theory of channels describes a system of the conductors of the heat;
- Channels are “immaterial pathways” transmitting electromagnetic waves;
- Channels are independent and previously unknown bodily systems;
- The theory of channels describes the physiology and pathology of connective tissue;
- The theory of channels describes interstitial openings and bodily cavities;
- Other hypotheses that explain the transmission of signals along the channels.
Despite the difference in the viewpoints on the nature of the channels, most acupuncturists agree that the concept of channels makes it easier to represent the system and the locations of the acupuncture points and improves the efficacy of acupuncture diagnostics and treatment [44,49,163].
3.1. The denial of the possibility of the existence of the system of channels and collaterals
Many reputable experts in the field of neurophysiology and acupuncture are categorically against recognizing channels as separate functional and morphological formations [46,48,49,163,164]. Some voice an opinion that the channels are strictly a functional concept, and the regularity of linear positioning of acupuncture points can be explained by the presence of interneuron connections formed during embryogenesis at different levels of the central nervous system [44,53,165]. According to Erich W. Stiefvater, the system of channels and collaterals in its classical sense is too primitive from the viewpoint of modern biology [69].
The term “meridian” (meaning an imaginary line conditionally connecting functionally similar acupuncture points) was introduced in the middle of the 20th century thanks to Soulié de Morant, a founder of the French school of acupuncture [33].
3.2. Theory of channels describes nervous and vascular systems
The assumption about the likeness between channels, nerves, and vessels can be made due to similarities between the paths of the channels and the topography of neurovascular bundles [33,166,167].
The first Latin translations of literature on Traditional Chinese Medicine published in Europe used the term “paths” that circulate “the blood and the spirit” to convey the meaning of Jing-Luo (“channels and collaterals”). However, the dissertation of Willem ten Rhijne described channels and collaterals as blood vessels, which resulted in an erroneous view that identified TCM channels with the blood vessels known to European medicine [168,169]. Later, a Russian doctor, A. Tatarinov (1853), wrote that the Chinese doctors used the term “Jing” (channels) sometimes to describe the nerves and sometimes to describe the tendons [170]. Similar views were expressed by other researchers who studied acupuncture points and channels, or practiced acupuncture.
G. Soulié de Morant (1957) and Fr. Hübotter (1929) associated nerve stems with Yang-related channels and the vessels with Yin-related channels [33,171]. H. Goux (1955) suggested that the channel theory describes the physiology and the pathology of the autonomic nervous system (ANS), with the sympathetic section of the system belonging to the Yang channels and the parasympathetic belonging to the Yin channels [172]. R. de La Fuÿe and H. Shmidt (1952), [173] held a similar view in their joint work, as well as G. Bachmann. (1959) [174].
Dr. R. de La Fuÿe explained the mechanisms of acupuncture from the viewpoint of establishing skin-visceral connections in embryogenesis, noting that the nervous system and the skin have ecto-dermal origin. In contrast, the internal organs have meso- and endo-dermal origin. Communication between the internal organs, the nervous system, and the skin is realized during the process of organogenesis as the elements of the nervous system grow into the internal organs [175]. Dr. J. Hu (1975), in the article “Neural basis of meridians and acupuncture points,” noted the closeness of the channel trajectory and the distribution of dermatomes [176].
Gong Qihua et al. (1979) made a note of the topographical closeness of the paths of the meridians and lymphatic vessels, as well as of the fact that the spread of lymphangitis is triggered by trauma of a thumb in the L-1 (Shao Shang) area alongside the path of the lung meridian. In the experiments on cadavers, when a colorant was introduced in the region of Yin meridian distal points, such as the L-1 (Shao Shang) point, it spread along the lymphatic paths alongside the relevant meridians [177]. A close relationship between the meridians and lymphatic vessels was also pointed out by R. Voll (1966), who had even singled out a particular lymphatic meridian [83].
Summarizing the data available in the early 1960s, V. Vogralik described meridians as nervous conductors within integuments that weave around lymph and blood vessels and muscles and then transition into the nerve plexus, spinal cord, and brain, and then to the nerves going to internal organs [53].
3.3. Theory of channels describes muscles and subcutaneous tissue
In the mid-50s, a Japanese physician, R. Fujita (1955), noted that the outer pathway of the meridians coincides with the lines of muscle contraction. He described the painful points as nodes of densification that appear in subcutaneous tissue in case of disease of internal organs [178,179]. American author F. Warren (1981) noted that the foci of neuro-myofibrosis coincide with the acupuncture points [180].
Even though up to 70% of trigger point coincides with the localization of the BAPs used for pain treatment, R. Melzack et al. (1977) believed that the concept of “acupuncture point” is much broader than of the “trigger point.” [181] Some doubts were expressed about the very existence of any independent trigger points that are not acupuncture points [182].
3.4. The theory of channels describes a system of electrical conductors and semiconductors
As electrical conductivity within the points of the same channel is higher than between the points of different channels, it was suggested that the theory of channels and collaterals describes the physiology and pathology of the system of electrical conductors and semiconductors.
In 1950s, Dr. Y. Nakatani measured the electrical conductivity of the skin of a patient with chronic nephritis and found on his back a point with an increased electrical conductivity. As suggested by Prof. K. Sasagawa of the Department of Physiology, University of Kyoto, the points with increased conductivity were called riodoten. The line along which they were found was called ryodoraku: (ryo) - good, (do) - conductivity, (raku) - line or meridian [79,80,183]. Later, the results of Y. Nakatani were confirmed by modern scientists [184].
Similar findings confirming lower resistance between the points within the same channel were discovered by a Soviet scientist A. Podshibyakin, [35] a French scientist J. Niboyet, [81,92] a German physician R. Voll), [83,84,85] and many others.
A Nobel Prize Winner in Physiology and Medicine (1937), A. Szent-Györgyi was one of the first to point out the possibility of semiconductor effect in the human body. In 1941, he suggested that the migration of electrons in the conduction zones of protein structures with properties similar to those of semiconductor crystals may play an essential role in some biological processes [185]. Given that the effect is present in nucleoproteins (rather than in the proteins or the nucleic acids), the active protein structure should be compared to an impure molecular crystal [186].
In 1976, V. Nikiforov repeated the hypothesis that a living organism is a giant bio-semiconductor containing numerous zones of conductivity and semiconductivity. The channels (meridians) are conductors presented in the body’s integument that weave around lymphatic and blood vessels, muscles, and internal organs. The system of conductors or channels is the essential system that integrates all the other regulatory systems and the body as a whole. End portions of the meridians have the highest functional activity and are the points of the highest electrical conductivity [105].
H. Schuldt (1976) measured electrical potential on the surface of the human body and concluded that the meridians are located along the lines of maximum concentration of electrical fields [187].
After a series of experiments with the electrical conductivity of the channels, R. Becker (1987) suggested that the transfer of energy and interaction within the meridian system goes along the glial cells of the nervous system according to semiconductor principles. The glial cells transmit direct electrical current of small amplitude at low speed, unlike the neuron that transmits high-frequency electrical signals at high speed. According to R. Becker, that particular weak direct electrical current is the manifestation of simple electrophysiological mechanisms ensuring regeneration and restoration of the function of nerve fibers in case of trauma [188].
Research of the channel conductivity with the electrode located by ultrasound suggests that the reduced resistance along the channels is due to the loose connective tissue that fills the gaps between the muscles or between the muscles and the bones [189].
Thus, we can assume that in a multicellular organism, the channels serve as conductors of electric current [96].
3.5. The theory of channels describes a system of the conductors of the heat
Due to the high thermal conductivity of the skin in the acupuncture “points” and between the points within the same channel, A. Romodanov, O. Butenko, D. Lyaschenko, and some other authors suggested that the channels represent a system of thermal field conductors, and the “acupuncture points” serve as the gateway for heat exchange between the body and the environment [42,94,138,190].
3.6. Channels are “immaterial pathways” transmitting electromagnetic waves
Alexander Gurwitsch (1922) and George Lakhovsky (1929) were the first to describe the function of the cells based on radiophysical theory. G. Lakhovsky even applied electromagnetic fields to treat plants, animals, and humans [191,192,193]. In 1932, Harold Burr, observing the proliferation of nerve cells in the water lizard (Ambystoma mexicanum Hope), designed a theory of electrodynamic development of the living body [194].
The wave model that explains the growth and development, physiology, and pathology of living subjects was later used in the works of A. Leontowitsch (1933), [195] S. Turlygin,(1942), [196] F.Popp (1978), [197] and many others.
As the efficacy of acupuncture was confirmed over many centuries of practice, however, no morphological substrates of channels were identified, some scientists attempted to explain the channels as “immaterial” ways of transmitting electromagnetic waves [107]. For example, A. Lebarbier (1975) stated that the meridians were the power lines of an electromagnetic field that are not defined by the anatomy but are detected by electronic instruments [198]. Sergey Sit’ko, one of the developers of microwave resonance therapy, suggested that the meridian system of living subjects has an electromagnetic nature and may be regarded as a mathematical solution of some limit cycles, both periodic and stable over time and space. In other words, the points and the channels are the projections of the solution of these limit cycles on a three-dimensional living object [199,200].
3.7. Channels are independent and previously unknown bodily systems
Various authors assumed the presence of an independent self-regulating system within a body. According to N. V. Quan (1936), channels are real rather than imaginary lines with the properties different from such known anatomical entities as nerves and blood vessels [45]. Though normal functioning of channels is associated with the nervous system, they are not a nervous system in the ordinary sense. Probably, in terms of evolution theory, the system of channels and collaterals is simpler and more “ancient” as compared to the nervous and vascular systems [96].
Russian scientists A. Zhirmunsky (1979) and L. Savina (1983) voiced the opinion that there existed the 3rd regulatory system of the body [107,201]. A. Zhirmunsky assumed that the main function of that system is the transfer of information from the peripheral parts of the body associated with the environment to the body, as well as information transfer within the internal organs and to its periphery [201].
In 1961-1962, North Korean biologist Kim Bong Han (Figure 4), invented the method of coloring living and actively functioning tissues and discovered the previously unknown anatomic-histological “Kyung-Rak” system that differs from the nervous, circulatory, and lymphatic systems [202].
According to Dr. K. Han, Kyung-Rak system consists of specific Bonghan’s corpuscles located in the area of biologically active points, linked with each other by the Bonghan’s ducts, with circulating viscous liquid containing high concentrations of DNA and RNA molecules. Bonghan’s corpuscles are surrounded by connective tissue with a relatively high content of tissue fluid [202] (Figure 5).
Kim Bong Han’s discovery was confirmed by Japanese scientists only [203]. Scientists from other countries were unable to confirm the Kyung-Rak system [51,204,205]. According to G. Kellner, who also researched that matter, the structure identified by Kim Bong Han was an artifact [26]. Due to the absence of Kyung-Rak system confirmation by scientists from other countries, the research in North Korea was stopped, and the laboratory was disbanded. The further fate of Kim Bong Han is not known.
In 2002, a South Korean scientist Jiang Xiaowen et al., described the technique that allowed them to identify the structures previously described by Kim Bong Han. It turned out that these intravascular channels of a diameter under 50 μm are restricted with a whitish, semi-transparent, soft, and flexible wall that is easily destroyed during a conventional histological examination. In order to identify, it is necessary to introduce intravenously in a live subject a 10% dextrose solution and cause blood coagulation and blood depositing around the studied intravascular channels [206,207].
Subsequently, there came a series of publications on the morphology, physiology, and pathology of the Kyung-Rak system. A newly re-discovered structure got the name of “Primo Vascular System” [208,209,210,211,212,213]. “Bonghan” ducts and tubes were found in blood and lymph vessels, [209,214,215] in fat tissue, [215] and on the surfaces of internal organs [216]. The flow rate of Bonghan fluid within the tubes is 0.3 mm/sec, which is significantly lower than the movement of blood or lymph [217].
3.8. The theory of channels describes the physiology and pathology of connective tissue
The hypotheses presuming that the elements of areolar and fibrous connective tissues made of proteins with semiconductor properties that transmit various kinds of energy are the morphological base of the meridians are in a separate group [222].
In the eighties of the last century, a Japanese physician, H. Motoyama (1980), investigated the electrical conductivity of acupuncture points and concluded that it is a highly hydrated phase of the connective tissue of the skin that plays a leading role in the conductivity of electrical current. Therefore, connective tissue serves as the physical basis of the so-called system of channels and collaterals [223,224].
A. Umanskaya (1984) stated that the channels are the terminal formation of connective tissue with countless bilateral connections (both between the elements and the peripheral parts of the central nervous system, organs, and organ systems). Acupuncture points are the locations for the filtration of a complex range of external inputs and their transformation into the signals appropriate for the nervous system [225].
At the end of the 1980s, Chinese authors, J. Yuchi (1986) and X Du (1989), noted a strong correlation between the connective tissue and the channels [226,227]. Around the same time, the famous Swedish radiologist, Dr. B. Nordenstrom (1989), suggested that a vascular–interstitial system transferring ion fluxes may be regarded as a morphological base of a channel [228]. French scientist P. de Vernejoul et al. (1992) came to a similar conclusion after studying the migration of radioactive isotope solution introduced into acupuncture points [229]. According to Japanese researcher, P. Hashimoto (2005), the perineurium of connective tissue and perineural vessels may serve as the morphological basis of the channels [230].
Scientists from Romania, S. Ionescu-Tirgoviste et al. (1987), measured electrical potentials in acupuncture points and concluded that the system of channels is a network of electrical conductors formed by interstitial tissue stretching between other known anatomical structures [231,232]. According to A. Ahn et al. (2005) that reduced resistance along a channel is due to the loose connective tissue that fills the gap between individual muscles or between muscles and bones [189].
In 1996-1998, M. W. Ho et al. developed the theory of liquid crystal organization of living objects. According to that theory, collagen and water molecules form a liquid crystal structure that pervades the entire body. This ‘crystal’ is the basis of the channels. In acupuncture points, hydrated collagen fibers are perpendicular to the skin and form a passage linking the internal and the external environment. It is assumed that this aqueous collagen crystal is a semiconductor for protons. It functions as a unit and serves as the environment that ensures the existence of the cells of a multicellular organism. Dr. M. Ho considered collagen crystal to be a peripheral “body consciousness” that interacts with the “central consciousness” localized in the brain [233,234,235].
According to Yu. Ignatov et al. (1990), the stimulation caused by the needle may be transmitted to a certain distance along the fibers of the connective tissue due to the ability of muscle fascia to transfer vibrations caused by its tension or perforation [46].
H. Langevin et al. (2001) studied the phenomenon of needle retention during acupuncture treatments. It appeared that the needle retention was due to the reaction of connective tissue structures that twist and untwist around the needle rather than to a muscle spasm reaction. The force that has to be applied to remove the retained needle is more significant when the needle is in the acupuncture point than when the needle is introduced in a random skin area [236]. The studies suggested that fibrous connective tissue can conduct signals at long distances as mechanical waves propagate along the fascia covering muscles [237].
Chinese scientists L. Yuan et al. (2004) suggested that the anatomical basis of the channel system is a branching network of fibrous connective tissue represented by various fascia [238].
According to J. Kim et al. (2009), a channel is a subcutaneous connective tissue layer with an interstitial fluid passing through it. These channels ensure the redistribution of tissue fluid pressure between different body portions in motion. Acupuncture points are the locations for control of the redistribution of interstitial fluid [239]. P. Fung (2009) came up with a similar idea and added that mast cells and membrane calcium pumps are essential for the functioning of the channel system [240].
3.9. The theory of channels describes interstitial clefts and bodily cavities
In 1952, doctor Rokuro Fujita, proposed the hypothesis that the channels represent a system of inter-muscular slots where interstitial fluid moves due to muscle contraction [178,179]. According to a doctor S. Takano (1985), interstitial clefts filled with a liquid with a high concentration of ions cause the “ruodoraku” phenomenon, which means high electrical conductivity of channels [241].
In 1966, G. Kellner analyzed scores of layered skin preparations aiming to confirm or refute the results of Kim Bong Han. He found unique slots in the borderline zone between the papillary and reticular layers that made him suggest the existence of an autonomous intradermal system capable of transferring interstitial fluid and possibly responsible for the transfer of energy through the skin surface [26].
In 1980, D. Draehmpaehi et al. studied tissue samples of four-month-old human fetuses and discovered linear subcutaneous cavities stretching in the sagittal direction of the localization corresponding to the description of the “channels.” [242].
In 2003, a group of Chinese researchers analyzed the structure and function of perivascular space and suggested that the area around blood vessels could explain the phenomenon of channels and collaterals [243]. In 2008, doctor B. C. Lee et al. published an article describing the channel as longitudinal slots in subcutaneous muscles. Unlike the Kyung-Rak system, these channels have no covering membrane. They are not associated with acupuncture points, although fluid moves along these channels, like Bong Han tubes [210].
W. B. Zhang (2008) used a special technique that permits the measurement of interstitial fluid pressure. He found areas of low pressure under the skin different from those in the surrounding tissues. These longitudinally oriented regions of low hydraulic pressure coincide with the path of the so-called “channels.” Limited areas with low hydraulic resistance coincide with the points of lower electrical resistance. Radioactive isotope helped visualize the channel trajectory with low hydraulic resistance. A coloring agent (Alcian blue) determined a more accurate location. The speed of interstitial fluid in the channel is significantly lower than that of blood and lymph in the vessels. It is presumed that low hydraulic pressure and resistance areas belong to a previously unknown system described in the TCM [244,245,246].
A study of the migration of coloring agents injected in the area of acupuncture points on the back (Bl-18, Bl-20, Bl-23) was conducted in 2009. The magnetic resonance imaging method found that the substance was not transmitted along the blood or lymph vessels but via interstitial gaps towards the direction of corresponding internal organs [239].
3.10. Other hypotheses that explain the transmission of signals along the channels
Among the other hypotheses explaining transmission of signals along the channels is the one that assumes that the gap junctions participate in the process. They play an important role in the metabolic communication and in the integration of cells and tissues. It is believed that the system of gap junctions is capable of receiving and integrating information from skin surface and transmitting it to nearby and remote areas of the living organism [127]. The mechanism of signal transmission via gap junctions is working as follows: each stimulated excretes biologically active substances that stimulate neighboring cell which in turn is accompanied by mechanical vibrations. An introduced needle causes vibrating biomechanical processes that spread due to gap junctions along the chain of cells transmitting the information to the destination [147].
Doctor S. Y. Lo (2001) suggested that channels are formed by the various polarized molecules gathered into large clusters, where water molecules play an essential role due to their permanent dipole moment [247].
4. Modern discoveries in the functioning of channels and collaterals
This section is devoted to the research related to the specific functions of the tissue along the assumed pathways of the channels, namely:
- The high electrical conductivity;
- The high thermal conductivity;
- The conducting of the electromagnetic waves;
- The conducting of the radioactive isotopes;
- The conducting of the contrast media;
- The propagating of the specific sensations along the channel.
4.1. The high electrical conductivity of the channels
The most significant number of studies in channel physiology is dedicated to measuring their electrical conductivity. The resistance between the points belonging to (lying on) the same channel is lower than between the points belonging to different channels [52,79,115,116,248,249]. It is noteworthy that the conductive properties of the channels maintain their properties on the skin of cadavers and transplants [114,115,250,251]. According to F. Kracmer (1962), the electrical properties of the channels prove they have specific intermolecular bindings [252].
Stimulation of the points of a particular channel causes a change in the conductivity of the points of the same channel [96]. For example, when the Pc-6 (Nei Guan) acupuncture point is stimulated, a significant decrease in the resistance to electric current is observed in the Pc-3 (Qu Ze) acupuncture point, which is located on the pathway of the same channel [253].
In the experiment, bipolar electrical signals of a sine-shaped wave with a frequency of 2.5 Hz were applied to the points of the Lungs channel. It was found that the signal was transferred better in a distal direction from the point L-3 (Tian Fu) to the point L-11 (Shao Shan), that is, ”in the direction of Qi flow along the channel and worse – in the opposite direction, i.e., “against Qi flow” [248].
There is an opinion that the change in the electrical activity of the channel reflects the change in the intensity of an electromagnetic field within the body, [96] blood filling of the capillaries, and the amount of interstitial fluid [253]. The experiments on the gel model suggested that the function of electrical conductivity of the channel is associated with interstitial fluid containing water, salt, and proteins [254].
4.2. The high thermal conductivity of channels
Experimental and clinical work of A. Romodanov, O. Butenko, D. Liaschenko, A. Ovechkin, and other authors indicated that a thermal field spreads along the pathways of the channels. That led to the presumption that the channels represent the system of conductors of heat fields [42,94,137,158,255].
The studies of the Chinese authors registered temperature inhomogeneity of the face with an infrared imager. It was present in the volunteers and patients with facial nerve palsy. The temperature increase along the urinary bladder channel was observed in 95 out of 444 subjects. The width of the “hot” line reached 1-1.5 cm, and the temperature gradient ranged from 0.2-0.3 to 1.5 degrees. As a general rule, the temperature gradient increased after acupuncture [256]. Acupuncture in LI-4 (He Gu) point caused an increase in temperature in the facial area along the projection of the colon [257].
In another study, applying moxibustion at acupoints caused the lines of high temperature coinciding with the channel path to appear on the patient’s body [258]. After a moxibustion of the point GV-4 (Ming Men), 70% of the volunteers noted an increase in the temperature along the midline of the back. After moxibustion of the points CV-12 (Zhong Wan), 56% of the volunteers had an increase in temperature along the median line of the abdomen and chest. It is assumed that the mechanism of linear propagation of the thermal field along the trajectory of the channel is associated with a change of local microcirculation or an increased thermal conductivity along a compactly organized connective tissue [259].
Using an infrared thermal imager during acupuncture permits observing the change of temperature spreading along the projection of channels. For example, acupuncture of the point GB-37 (Guang Ming) in a patient with paralysis of a facial nerve caused increased temperature around the eyes. In contrast, acupuncture at the point LI-4 (He Gu) caused an increase in temperature around the mouth [260]. Acupuncture at the point LI- 4 (He Gu) caused a more pronounced temperature reaction on the face than at the point St-36 (Zu San Li) [261]. Thus, the change of thermal fields during acupuncture further confirms the specific effect of different acupuncture points.
However, it should be noted that the distribution of the thermal field along the trajectory of the channel was not observed in all experiments [262]. This negative result may be due to the peculiarities of the subjects, which were healthy volunteers, or the moxibustion technique applied as far as no initial abnormalities were diagnosed. Acupoints were selected randomly but not according to the patient’s condition, which means the experiment did not follow classic recommendations used in traditional Chinese acupuncture.
4.3. The conducting of the electromagnetic waves
In 1984, an article was published by D. F. Mandoli and W. R. Briggs dedicated to waveguide-like structures of plants capable of conducting light along the branches, the stems, and the roots [19]. Other scientists conducted similar research work [263].
In the laboratory of V. Kaznacheev, acupuncture points were exposed to the visible light emitted by a conventional incandescent lamp. A photomultiplier tube measured the intensity of photon radiation emitted by neighboring acupuncture points. It was found that the emission intensity by points located on the same channel as the irradiated point was several hundred times higher than the background radiation detected from the points of the adjacent channels; thus, the channel’s ability to conduct electromagnetic waves of the visible band was detected. It is believed that the system of channels permits the light to penetrate and reach the deepest sections of the living body [264]. The ability of the channels to conduct light was confirmed and studied by the laboratory in China [265].
4.4. The conducting of the radioactive isotopes
The first study of radioactive isotope (RAI) migration after its introduction into the acupoints was conducted by a North Korean scientist, Kim Bong Han, who published his findings in 1964 [202].
In 1981, Romanian scientists Tiberiu Räibulet et al. reported the migration of isotopes in the distal direction of the limb, i.e., opposite to the proximal direction expected if the isotopes were moving through veins or lymphatic vessels [266].
The following publications were from the French scientist P. de Vernejoul et al. [267,268,269,270]. Technetium-99m [99mTc] in the form of sodium pertechnate was administered subcutaneously to a depth of 3-5 mm to a group of patients and healthy volunteers, volume of 0.05 ml containing a single dose of 10 MBq. Introduction of the RAI into the point K-7 (Fu Liu) located on the inside surface of the leg led to linear migration of the isotope to 30 cm from the injection site (Figure 6b). A local diffusion in different directions was observed (Figure 6a) when it was introduced outside the point.
When RAI was introduced into point St-43 (Xian Gu), located on the dorsum of the foot, the isotope migrated in proximal and distal directions along the tendon-muscular channel of the Stomach [267]. When RAI was administered in GB-36 (Wai Qiu) point located on the outer surface of the tibia and point St-41 (Jie Xi), located on the borderline between the foot and shin, a linear migration of the isotope in the distal and proximal directions was observed. When RAI was administered to a point LI-18 (Fu Tu) in the center of the sternocleidomastoid muscle, the isotope migration was observed toward the upper lip on the opposite side, i.e., alongside the Large Intestine channel [268].
When RAI was introduced into the left and the right points of the Kidney channel K-7 (Fu Liu) of the patients with unilateral renal pathology, it turned out that the speed of propagation of the isotope was higher on the affected side than on the unaffected one [267].
In the subsequent experiments, RAI was administered bilaterally at the point K-7 (Fu Liu). Then, point K-2 (Zhang Gu) was exposed to impulses of the helium-neon laser. The pulse frequency of 24 Hz changed the RAI migration speed. The pulse frequency of 48 Hz caused no change in the rate of RAI migration [268].
Pertechnetate sodium and rhenium sulfide labeled by technetium isotope [99mTc] were used to exclude migration of the isotope via (or through) the lymphatic system. Iisotopes were administered to the acupuncture points or into the webbing between the toes according to the classical method of lymphography. After introducing rhenium sulfide into the webbing between the toes, it was accumulated in the lymph node. However, no RAI accumulation in the lymph nodes was observed when sodium pertechnetate and sulfur rhenium were administered at the acupuncture point. The assumption of the distribution of RAI by veins was also excluded, as the isotope migration went on in a longitudinal direction (not in the transverse direction typical for the location of the veins on the back of the foot [267,269,270].
The average speed of RAI linear migration did not exceed 3-5cm/minute, i.e., it was significantly lower than in the case of migration along the veins or lymph vessels. Thus, apart from the typical trajectory of the isotope propagation, there was another essential peculiarity of the isotope migration: a slow onset of the migration and a slow disappearance, unlike rapid onset and disappearance in the case of isotope migration along lymphatic or venous vessels [268]. It is believed that RAI migrates along areolar connective tissue surrounding neurovascular bundles [268].
The Spanish scientists of F. M. Kovacs’s laboratory performed similar studies on dogs. In the first experiments, radioactive technetium (99mTc) was administered subcutaneously at a low electrical resistance point on the dog’s paw; after that, the linear isotope migration (LIM) was observed in the proximal direction as a narrow line. The isotope propagated along the same line in different experiments with an average 2cm/minute speed. The isotope distribution was not associated with the movement along nerves, blood, or lymph vessels [271].
Further experiments clarified that the migration of radioactive technetium is possible only in case of skin integrity both in the path of the migration and on the opposite extremity [272].
If a skin incision is made in the path of the radioactive isotope, the migration continues around the wound. After stitching the wound, LIM was restored, and the isotope ceased moving around the wound. LIM was also restored if an unstitched wound was filled with silicone gel or a gel for ultrasound diagnostics and was covered with a solid silicone sheet parallel to the skin surface. LIM was absent if the wound remained unstitched but was filled with Vaseline or a whole silicone layer. Thus, the LIM process was observed even before restoring the integrity of the traumatized tissue. The experimental results suggest that the mechanism of linear isotope migration is similar to the capillary electrophoresis [273].
4.5. The conducting of the contrast media
Studies with non-radioactive contrast agents administered at the points of different channels were also conducted. According to MRI, the migration of contrast matter was linear along the trajectory of the channels. It was also noted that the transfer of the contrast matter was not related to the movement of the blood or lymph among the vessels. Linear movement of the contrast matter was not observed when it was administered outside the acupuncture points [276].
Similar results were demonstrated by J. Kim et al. (2009) in their studies of colorant migration when administered to the dorsal acupuncture points (Bl-18, Bl-20, Bl-23). According to MRI, the substance was transferred neither by the blood or lymphatic vessels but via interstitial gaps in the direction of the respective internal organs [239].
The studies of W. B. Zhang (2008) detected longitudinal regions of lower pressure in the subcutaneous areas of guinea pigs. The speed of interstitial fluid through these lower pressure channels was significantly lower than that of blood and lymph within vessels [245].
Solutions of medications introduced into points with low flow resistance are eliminated from the area of the points much faster than when administered to control skin areas. Rapid absorption of the medication means a quicker onset of the pharmacological effect [277].
6. The propagating of the specific sensations along the channel
Phenomenon of “Arrival of Qi” (De Qi) was described from the very beginning of acupuncture. If the needle is inserted to the desired depth, the patient may feel aching, distension, tingling and other sensory modalities in the area of acupoint. In this case you may find the changes of biophysical parameters of skin around the needle. In the ancient book Spiritual Pivot (Huangdi Neijing Lingshu), it was written that “acupuncture therapy does not take effect until arrival of Qi”. Later they noticed, that quick arrival of Qi suggested good effects in treatment, slow arrival of Qi retarded effects in treatment. If there is no needling reactions, doctor should concentrate his mind, insert needle to a certain depth, apply special manipulation and wait for Qi, which “seems a fish bites on fishing pulling the line downward” [278].
Special needle manipulation causes the sensations that propagate along the limbs and the body. This phenomenon is called “propagated sensations along the channels” or PSC. The phenomenon of the “arrival of Qi at the site of disease” or AQSD is similar. With it, the positive clinical effect develops as the sensory responses extend to a place of the conventional localization of the pathological process or pain [279,280,281]. There are manifesting PSCs when a patient is describing some sensations accompanied by the change of objective parameters of the points and relevant bodies, and the latent ones when it is possible to detect a change of objective parameters in the area of the points and/or organs despite the absence of sensory reactions [280,281].
According to the experts in acupuncture the presence of PSC is one of the proofs supporting the existence of morphological – functional system referred to as channels or meridians. Registration of the directions and the development of the sensations when acupuncture points are activated permits to further verify the paths of the meridians [282,283,284].
The research permitted the measure of the sensations’ propagation speed, which varies on average between 1.5 and 5.0 centimeters per second, but sometimes reaches 20 cm/second. The width of the strips of skin within which the sensations are experienced ranges from one to three centimeters on the limbs and up to 10 centimeters on the body [44,96].
Objective physiological changes are detected in the presence of sensory reactions that can be measured by a variety of devices, such as:
- -
- An increase in the amplitude of the systolic wave of the vascular rheo-angiogram located in the area of the stomach meridian with the stimulation of the point St-36 (Zu San Li).
- -
- Increase in heart rate during stimulation of the Pericardium channel points;
- -
- An increase in urine output during stimulation of the Kidney channel points.
- -
- An increase in the excretion of cAMP upon stimulation of the Urinary Bladder channel.
These changes ceased shortly after the stimulation is over and PSC is withdrawn, and they do not occur when the points of the other meridians are activated. In the absence of PSC, physiological changes were not recorded or were expressed very weakly [285].
In other studies, the proliferation of the PSC, caused by the needle stimulation, was accompanied by a change of skin color as a red stripe (vasodilatation) or as a white stripe (vasoconstriction) [279].
Stimulating the end (Jing) points of channels caused 2-15 Hz sound signals with triangle or sine waves propagating along the channel [279]. The other phenomena included the change in the electrical resistance and capacity in the points, increased pain threshold, and increased activity of the spontaneous visible light [279]. Upon reaching the PSC of the relevant body, it changed its physiological parameters, and in particular, there was an increase in myocardial contractility, louder rumbling in the stomach, and activation of peristaltic motion [279,280,281]. In this case, specific sensations reached the area of the disease, the pain was eased, asthma attacks stopped, or a muscle spasm was relieved. Persistent clinical effect was achieved by the courses of treatment of chronic diseases, including myopia, gastroptosis, optic nerve atrophy, ischemic heart disease, and others [280].
The studies on the blockade of sensations propagating along a channel are of great interest. It was proven that the PSC and therapeutic effects may be blocked by cold exposure of the area of the channel projection [96,279]. On the contrary, local warming of the channel speeds up the transmission of PSC [279,280]. On the contrary, local warming of the channel speeds up the transmission of PSC. [279,280]. The PSC blockade effect may also be achieved by injecting 0.2-0.3% saline or lidocaine solution into deep tissue and after either epidural or peridural anesthesia. However, intrathecal and epidural anesthesia could not blockade the sensation propagating along a channel in some patients [280].
A mechanical pressure of 500 - 1000 - 500 g/mm2 with a tissue deformation in the channel projection region immediately blocks PSC. The critical factors for PSC blockade are the localization and the force of pressure of pressure. Thus, a light touch to the skin without pressure and the pressure outside the channel projection area do not cause PSC blockade and, therefore, do not reduce the effect of acupuncture treatment [279,280,286]. PSC blockade neutralizes all of the above effects of PSC, including the pain relieving effect of acupuncture [96].
In the middle of the 1980s, E. Andreev, S. Sit’ko, et al. carried out studies with low-intensity electromagnetic radiation (EMR) in millimeter (MM) range. Therapeutic frequency was chosen for each patient individually, considering the patient’s body’s PSC and objective parameters. They called their methods “microwave resonance therapy” [153,199,200]. They were the first to describe the effect of the PSC blockade by constant magnetic field. This phenomenon was called “the phenomenon of Rudenko” [287,288].
In 1989, as part of a state program carried out under the supervision of the USSR Academy of Sciences to study the biological and medical effects of EMR MM, a series of experiments on the stimulation of sensory reactions with subsequent blockade by a constant magnetic field was carried out. It was found that the patient’s sensory reactions were accompanied by a change in temperature at particular acupoints located on the channels. When the permanent magnet with a magnetic field strength of 500 oersted was placed on one of the points along the channel, the sensory reactions previously stimulated by EMR MM were gone, and the temperature at the points went back to the initial one [289].
Summarizing the review of research on the PSC phenomenon, one can say that most authors who studied the PSC phenomenon concluded that the PSC blockage was not due to the signal interferences at specific parts of the central nervous system but instead due to the blockage of some process at the periphery. Therefore, the PSC phenomenon is associated with an unknown physiological process developing and propagating directly along a channel [280,286].
5. The “channels and collaterals” theory describes the physiology and pathology of intercellular space
In 1989, after analyzing the literature on acupuncture points and channels, and considering the results of the therapeutic application of the EMR MM range, it was suggested that the channels are interstitial gaps [290].
After further discussion, attention was drawn to modern research methodology that usually suggests the connections of specific functions to specific structures of a biological object. However, in some cases, the absence of a structure provides an additional conductive function, for example, a window or door opening, a riverbed or drainage system, etc. Thus, the channels can be represented as gaps stretching between the other well-known anatomical structures. Surfaces of muscles, blood vessels, nerves, bones, and other structures also form the outer walls of the so-called channels. These gaps are filled with longitudinally oriented fibrous connective tissue, ground substance, electrolyte solutions, and structured water. Perhaps, this is enough to ensure the Qi conductivity function. This interpretation of the channels corresponds to the functional and morphological data discussed above and to the description of the channels in the writings of the Chinese master Li Shi Zhen: “... there are tunnels within a body and the one turning his mental gaze there may illuminate them ...” [162].
The theory and the experimental data proven that direct intercellular information exchange is carried out with the participation of electromagnetic fields of the frequency ranging from 1011 to 1014 Hz [264,291]. According to radio physics, such frequencies are transmitted by dielectric waveguides. Nerve fibers are suitable transmitters of low-frequency signals, whereas high-frequency signals may be transmitted only through the channels serving as a waveguiding structure. Therefore, the system of channels is the leading candidate for transmitting high-frequency signals generated by the cells. Theoretical and experimental studies confirm that the channels can be waveguides transmitting electromagnetic waves of various ranges [19,264,287,291].
The channels likely are an independent and the most ancient (in phylogenetic and ontogenetic sense) regulatory system of the body. However, being the basic one, it unites all other more sophisticated and the younger systems of macro-organism and provides interaction of the bodily interior with the environment [107,201,292].
For the above reason, in 2003, the hypothesis was first proposed that physicians of ancient China designed the theory of channels and collaterals to describe the physiology and pathology of intercellular space, gaps, and cavities of the human body [62,293] (Figure 7).
Analyses of the channel trajectory may prompt us to find a correlation between the channels and specific anatomical structures, but the relationship will be functional rather than morphological. The nature of the disease and its effects may help to determine the relationship of a specific disease with a particular regular channel or its secondary vessel.
For example, skin and subcutaneous tissue inflammation accompanied by redness, swelling, increased local sensitivity, and temperature may serve to diagnose the excess syndrome of the tendon-muscular channel passing through the affected area. Suppose there is a contraction of a specific group of muscles or tendons, or a keloid scar or non-healing wound persists after recovery; in that case, one can suggest the involvement of Luo-channel (collateral) in that affliction. If there are general manifestations of the disease with the signs of general adaptation syndrome and symptoms of the organs, it signifies the presence of the pathology of the regular channel and perhaps an organ [294].
However, if we analyze the pathway of the Governing Vessel and the Conception Vessel, we can conclude that the first one corresponds to the spinal canal and cranial cavity, and the second one corresponds to the thoracic and abdominal cavities [62].
6. The theory of Organs describes the physiology and pathology of cells
TCM identifies 12 main organs. There are six organs classified as Yin, or solid organs with parenchyma inside (Lungs, Spleen-Pancreas, Heart, Kidneys, Pericardium, Liver), and there are six organs classified as Yang, or hollow organs with internal cavities (Large and Small Intestines, Stomach, Gall bladder, Urinary bladder, and Triple heater).
Solid and hollow organs combined in pairs. There are small cavities inside the solid organs, for example, bronchi in the lungs, pyelocaliceal system in the kidneys, pancreatic ducts in the pancreas, bile ducts in the liver, etc., which resemble hollow organs. The hollow bodies are surrounded by parenchymal walls which can be attributed to a solid organ. Therefore, a stone in a kidney is located in the Urinary bladder, and a peptic ulcer located in the Stomach is a manifestation of the pathology of the Spleen-Pancreas [62].
The term ”organ” in TCM has a broader meaning than in anatomical formation. Most cells have standard organelles such as the nucleus, Golgi apparatus, endoplasmic reticulum, mitochondria, etc. Each organelle is responsible for specific functions. Mitochondria are responsible for oxidizing-phosphorylation and ATP synthesis. Golgi apparatus synthesizes proteins, polysaccharides, and other complex molecules and accumulates various minerals and biologically active substances. The cell nucleus is responsible for the development, constant shape, and death of the cell.
The essential functions of the main organs may be localized in specific organelles of every cell; for example, mitochondria are in charge of breathing (~ lungs), the endoplasmic reticulum is responsible for digestion and nutrient transportation (~ pancreas); the Golgi apparatus is responsible for the accumulation of biologically active molecules (~ liver); the cell nucleus maintains homeostasis and is in charge of development and death (~ kidney). The centrioles play an essential role in the process of cell division. Microtubule pulsing discovered in centrioles suggests that centrioles are most likely the intracellular analogs of the heart [295] (Figure 8).
All said above suggests that the TCM concepts of the organs are related to certain features and pathological processes in the human body’s cells [62]. For example, the term Lungs stands for the system of organs and tissues responsible for synthesizing Qi, or energy accumulated in ATP molecules. This system includes a respiratory center that regulates the complete process of respiration: the Lungs, which are involved in external breathing, red blood cells transport gases, and mitochondria perform ATP synthesis. (Figure 9).
Essentially, this complex circuit converts the energy stored in food into energy stored in the binding between the ribose molecule and phosphoric acid molecule. Therefore, whenever dyspnea is present, it is necessary to work with the points of the Lung channel regardless of the etiology, pathogenesis, and true localization of the disease. Inspiratory dyspnea and cough that aggravates at exhalation indicate the syndrome of lung deficiency and require activation of the relevant points. Expiratory dyspnea and cough that aggravates at inspiration indicate the syndrome of lung excess and require sedation of the relevant points [62].
In the same way, all other main organs have their essential functions and specific symptoms. For example, headache and dizziness points to a disease of the ‘Liver,’ insomnia and poor memory point to a disease of the ‘Heart,’ digestive problems point to a disease of the ‘Pancreas,’ and so on [96].
Conclusion
Thus, according to the acupuncture theory of TCM, Qi, and blood circulates in the human body along the “channels and collaterals”. For several thousand years, this theory allowed for effective treatment using classical acupuncture and moxibustion. From the time of acupuncture was designed to today, man has not changed. Consequently, the “channel system” described in ancient times is present in the human body today. However, analyzing all the above material, it is impossible to find confirmation that some kind of specialized regulatory system is still unknown in modern anatomy or physiology. Based on this, we can conclude that a “channel system” must exist, and perhaps it is known in modern biology and medicine. However, its description in scientific terms makes it difficult to recognize the system described as a “channels and collaterals.” Taking this into account, one can propose that, by the theory of channels and collaterals, doctors of ancient China described the physiology and pathology of the intercellular space and cavities of the body, and by the theory of internal organs they described the physiology and pathology of the cells.
Depending on the nature of the disease and its consequences, it may refer to channels (intercellular space), which are superficial and less dangerous, or to organs (cells), which are deeper and more dangerous.
In turn, depending on the nature of the disease and its consequences, it may refer to regular channels, which are deeper, or to the secondary vessels or collaterals, which are more superficial and less dangerous.
The term “organ” can refer to a specific function inherent in all cells, or to a specific organ that provides a particular function. It also can unite a system of organs involved in the joint implementation of a complex function. In the latter case, the term “organ” describes a “functional system,” the unifying factor of which is the valuable result of the action [296].
Analyzing theories used in TCM, one may believe they are a basic mathematical model, showing the general laws and relationship between physiological and pathological processes in the human organism. Although modern analogs can be found for the majority of terms and theories of TCM, it is essential to avoid simplifying ancient knowledge but to study it carefully to use it for scientific research and daily practice [297].
Funding
This research received no external funding
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
TCM, Traditional Chinese Medicine; ATP, adenosine triphosphate; BAP, biologically active point; BAPs, biologically active points; EP, electrical potentials; AP, action potential; RAI, radioactive isotope; LIM, linear isotope migration; PSC, propagated sensations along the Channels; EMR, electromagnetic radiation.
References
- Virchow, R. Die Cellularpathologie in ihre Begründung auf physiologische und pathologische Gewebslehre. – Berlin, Verlag von August Hirschwald, 1859.
- [Alexeev A] Алексеев АА, Белoв ВИ, Лариoнoва ИС. Кризис медицины (смысл биoинфoрмациoннoй диагнoстики и лечения). − Мoсква: Триада Плюс, 2003.
- Teaching group of Nanjing First Medical College: Variations of high conduсtance phenomena of acupuncture points before and after death. – Selected papers of the National Symposium on the Trad. Chin. Med, Acup, and Meridians. 1959: 440-444.
- Wang YH, et al., [Study on the high cutaneous conductance points of animals]. – Heilongjiang Med J. 1959; 2(7): 16-18 [Chinese].
- Acupuncture research group of Anhui Medical College: A preliminary report on the topography of high cutaneous conductance points of dogs. – Scientific papers of Abhui Med Coll 1959; 2: 145-156.
- Schoen, A.M. Veterinary Acupuncture: Ancient Art to Modern Medicine. – Goleta: Amer Veterin Publ, 1994.
- Yu C, Zhang K, Lu G, et al. Characteristics of acupuncture meridians and acupoints in animals. – Rev Sci Tech. 1994 Sep;13(3):927-33. [CrossRef] [PubMed]
- Wheeler AJ, Beitz DC, Swift CS. Mapping of acupuncture points on goat. – Am J Acup. 1976; 4 (1): 57-65.
- [Smirnov I] Смирнoв ИВ, Шевелев ОА, Демурoв ЕА, и др. К вoпрoсу o нахoждении электрoанамальных тoчек на кoже. – (Рукoпись, депoнирoванная в ВНИИМИ МЗ СССР, 1974, № 427-74). – Мoсква, 1974, 12, пo МРЖ, 1974, разд. XI, 9: 4-5 (473).
- Zhang KR, et al. [Determination of high conductive points on rabbits]. – Xian Med Coll J. 1959; (8): 8-24 [Chinese].
- Kurger, C.P. Acupuncture point topography in the horse. – Am J Acup 1976; 4(3): 276-280.
- Panzer, R. A comparison of the traditional Chinese vs. transpositional Zangfu organ association acupoint locations in the horse. – Am J Chin Med 1993; 21: 119-131.
- Klid, A.M. Low resistance acupuncture points in live and dead pigs (abstract). – The Fifth World Congress of Acupuncture, Tokyo, October 22-25, 1977: 146.
- [Neborsky A] Небoрский АТ, Белкания ГС. Анатoмo-тoпoграфическoе сooтветствие акупунктурных кoжных зoн кoнечнoстей у челoвека и oбезьян. – В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 64-66.
- [Portnov F] Пoртнoв ФГ. Прoблемы и перспективы электрoпунктурнoй рефлексoтерапии. – В кн.: Прoблемы клиническoй биoфизики. – Рига, 1977: 43-50.
- [Podshibyakin A] Пoдшибякин АК. Значение активных тoчек кoжи для эксперимента и клиники: Автoреф. дисс. дoкт. мед. наук. – Киев, 1960.
- [Zhirmunskiy A] Жирмунский АВ, Карпенкo АА, Кoчеткoв ЮД. Исследoвание электрическoгo сoпрoтивления пoкрoвoв личинки хлебнoгo жука. – ДАН СССР 1981; 257 (3): 751-753.
- [Geykin M] Гейкин МК. О мнoгoтoчечнoй электрoпрoвoднoсти в живoй прирoде. – В кн.: Свет гелий-неoнoвых лазерoв в биoлoгии и медицине. Пoд ред. Дoмбрoвскoгo В.А. и др. – Алма-Ата, 1970: 69-72.
- Mandoli, D.F. Briggs WR. Fiber Optics in Plants. – Sci Amer 1984; 251 (2): 90-98.
- [Filimonov I] Филимoнoв И. Н. Захарьина-Геда зoны. – В кн: Петрoвский Б. В. (ред.) Бoльшая медицинская энциклoпедия. Тoм 8. – М.: Сoветская энциклoпедия, 1977: 342-343.
- Head, H. On the disturbances of sensation, with special reference to the pain of visceral disease (thesis for MD). – Oxford: Brain, 1893, 16: 1-133.
- [Vil’yamovskiy B] Вильямoвский БИ. К вoпрoсу o сoстoянии бoлевoй чувствительнoсти кoжи при забoлеваниях внутренних oрганoв. – Автoреф. дoкт. дис., С.-Петербург, 1909.
- [Alimov Z] Алимoв ЗЗ. Диагнoстическoе значение зoн Зхарьина-Геда, Вилямoвскoгo и висцерo-кутаннo-вазoматoрных рефлексoв при oстрoм аппендиците. – Клин Мед 1962; 9: 115-121.
- Kellgren, J.H. Referred Pains from Muscle. Br Med J. 1938 Feb 12;1(4023):325-7. [CrossRef] [PubMed]
- Kellgren, J.H. On the distribution of referred pain arising from deep somatic structures with charts of segmental pain areas. – Clin Sci 1939; 4:35-46.
- Kellner, G. Bau und Funktion der Haut. – Dtsch Z Akup 1966; 15 (1): 1-31.
- Gunn CC, Ditchburn FG, King MH, Renwick GJ. Acupuncture loci: a proposal for their classification according to their relationship to known neural structures. – Am J Chin Med (Gard City N Y). 1976 Summer;4(2):183-95. [CrossRef] [PubMed]
- Liu Y, Varela M, Oswald R. The correspondence between some motor points and acupuncture loci. – Am J Chin Med (Gard City N Y). 1975 Oct;3(4):347-58. [CrossRef] [PubMed]
- Travell, J. Treatment of Painful Disorders of Skeletal Muscle. – Conferences on therapy. N.Y. State J. Med. 1948; 48: 2050.
- Travell J, Rinzler SH. Relief of cardiac pain by local block of somatic trigger areas. – Proc Soc Exp Bio. Med 1946 Nov; 63 (2): 480-482.
- Travell JG, Simons DG. Myofascial pain and dysfunction: The trigger point manual. – Baltimor: Williams & Wilkins, 1983; 1: 103; 1992; 2: 628.
- Soulié de Morant, G. Precies de la vraie acupuncture Chinoise. – Paris: Mercure de France, 1955.
- Soulié de Morant, G. L’Acuponcture Chinoise: La tradition Chinoise classifiée, précisée. Joint l’atlas (majorité des planches manquantes). – Paris: Lafitte, 1957.
- [Podshibyakin A] Пoдшибякин АК. Влияние гoлoвнoгo мoзга на взаимooтнoшения между активными и сoпряженными тoчками кoжи. – Журн высш нервн деятель 1952; 2: 198-204.
- [Podshibyakin A] Пoдшибякин АК. Об изменении электрических пoтенциалoв вo внутренних oрганах и связанных с ними “активных тoчках кoжи”. – Физиoл. журн. СССР 1955; 41 (3): 357-362.
- [Ionichevskiy V] Иoничевский ВА. Критический анализ классических и сoвременных представлений o тoчках “пяти первoэлементoв” в системе тoчек акупунктуры. – Хабарoвск: Препринт, 1984.
- [Miroshnichenko B] Мирoшниченкo БЕ, Инюшин ВМ. О биoгеoметрии тoчек акупунктуры (“активных тoчек” на пoверхнoсти тела челoвека. – В кн.: Психическая самoрегуляция. – Алма-Ата: Изд-вo Алма-Атинскoгo ИУВ, 1973: 383-390.
- Heine, H. Anatomical structure of acupoints. – J Tradit Chin Med. 1988 Sep;8(3):207-12. [PubMed]
- Rabischong P, Niboyet JE, Terral C, Senelar R, Casez R. [Experimental basis of acupuncture analgesia] Bases expérimentales de l’analgésie acupuncturale. – Nouv Presse Med. 1975 Aug 30-Sep 6; 4(28): 2021-6. [French]. [PubMed]
- Niboyet JEH. Les points d’Acupuncture: Notions electriques, histologiques, et leurs debouches en neurophysiologie. – Cahiers de biotherapie, Paris: 1980; 67:63-65.
- [Novinskiy G] Нoвинский ГД, Вoрoбьева ИА, Вoрoбьев ЛН. О нoвых прибoрах и метoдах нахoждения китайских тoчек. – В кн.: Вoпрoсы нейрoэндoкриннoй патoлoгии и рефлектoрнoй терапии. – Гoрький, 1960: 72-73.
- [Lyashchenko D] Лященкo ДС. Теплoвoе пoле челoвека и егo изменения при иглoукалывании. – В кн.: Всесoюзная кoнференция “Теплoвизиoнная медицинская аппаратура и практика ее применения”, ТемП-82 – Ленинград, 1982: 112-113.
- [Nagiyeva S] Нагиева СС. Материалы к вoпрoсу oб электрoпрoвoдимoсти кoжи при язвеннoй бoлезни желудка и двенадцатиперстнoй кишки. – Азер Мед Журн 1958; 1: 107-109.
- [Tabeyeva D] Табеева ДМ. Рукoвoдствo пo иглoрефлексoтерапии. – Мoсква: Медицина, 1982.
- Quan, N.V. Acupuncture chinoise pratique; sur quelques recherches touchant la medicine traditionnelle sino-japonaise. – Paris: Picart, 1936.
- [Ignatov Yu] Игнатoв ЮД, Качан АТ, Васильев ЮН. Акупунктурная анальгезия: Экспериментальнo-клинические аспекты. – Ленинград: Медицина, 1990.
- Bischko, J. Akupunktur fur Fortgeschrittene. – Heidelberg: Haug Verlag, 1976.
- Ciszek M, Szopinski J, Skrzypulec V. Investigations of morphological structure of acupuncture points and meridians. – J Tradit Chin Med. 1985 Dec; 5(4):289-92. [PubMed]
- [Durinyan R] Дуринян РА. Метoдический и физиoлoгический анализ прoблемы тoчек, меридианoв и энергии в рефлексoтерапии. – В кн.: Теoрия и практика рефлексoтерапии. – Кишинев, 1981: 3-11.
- Bossy J, Maurel JC, Godlewski G. Le substratum macroscopique des points d’Acupuncture. – Bull Ass Anat 1975; 59 (165): 357-362.
- [Vandan A] Вандан АЯ, Зальцмане ВК. Мoрфoлoгические oсoбеннoсти биoлoгически активных тoчек. – В кн.: Прoблемы клиническoй биoфизики. – Рига, 1977: 51-57.
- [Portnov F] Пoртнoв ФГ. Теoрия и практика электрoпунктурнoй терапии. – В кн.: Сoвременные прoблемы рефлексoтерапии. Матер. Всес. кoнф. – Вoлгoград, 1987: 36-38.
- [Вoгралик В] Вoгралик ВГ. Оснoвы китайскoгo лечебнoгo метoда чжень-цзю. – Гoрький: Гoрьк. кн. изд., 1961.
- [Novinskiy G] Нoвинский ГД. О Чжень Цзю-терапии. – Врач делo 1959, 5: 545-546.
- Hyvärinen J, Karlsson M. Low-resistance skin points that may coincide with acupuncture loci. – Med Biol 1977; 55(2): 88-94.
- [Podshibyakin A] Пoдшибякин АК. Активные тoчки кoжи. – В кн.: Чжэнь – Цзю терапия. – Гoрький, 1959: 32-37.
- Dung, HC. Anatomical features contributing to the formation of acupuncture points. – Amer J Acup 1984; 12 (2): 203-209.
- Heine, H. Zur Morphologie der Akupunkturpunkte. – Dtsch Zschr Akup 1987; 30 (4): 75-79.
- [Verzhbitskaya N] Вержбицкая НИ. Мoрфoлoгия акупунктурных тoчек кoжи. – В кн.: Медикo-биoлoгические аспекты рефлексoдиагнoстики и рефлексoтерапии. – Калинин, 1987: 35-41.
- [Verzhbitskaya N] Вержбицкая НИ, Крoмин АА, Всевoлoжский ЛА. и др. Мoрфoфункциoнальные oсoбеннoсти кoжи в ареале биoлoгически активных тoчек. – В кн.: Вoпрoсы психoгигиены, психoфизиoлoгии, сoциoлoгии труда в угoльнoй прoмышленнoсти и психoэнергетики. – Мoсква, 1980: 504-509.
- [Verzhbitskaya N] Вержбицкая НИ. Мoрфoлoгия акупунктурных тoчек кoжи. – В кн.: Медикo-биoлoгические аспекты рефлексoдиагнoстики и рефлексoтерапии. – Калинин, 1987: 35-41.
- Teppone M, Avakyan R. Modern view on the theory of Channels, Collaterals and Organs. – Med Acup 2007; 19 (1): 43-48. [CrossRef]
- Zhang KR, Dang RL, Guan LP, et al. A morphological study on the receptors of acupuncture points. – J Tradit Chin Med. 1982 Dec; 2(4):251-60. [PubMed]
- [Chuvil’skaya L] Чувильская ЛМ, Крoхина ЕМ, Федoтoва ОП. Нейрoмoрфoлoгический субстрат зoн акупунктуры. – В кн.: Актуальные вoпрoсы применения рефлексoтерапии в практике анестезиoлoгии и хирургии, акушерства и гинекoлoгии, стoматoлoгии. – Вoлгoград, 1983: 40-43.
- [Shabanov A] Шабанoв АН, Сoсунoв АА, Тельцoв ЛП. Иннервация аурикулярных тoчек акупунктуры. – Мoрфoлoгия 1998; 113(3): 130.
- [Gurgenidze A] Гургенидзе АГ, Цирюльникoв ЕМ. Сенсoрная характеристика тoчек акупунктуры. – В кн.: Теoрия и практика рефлексoтерапии. – Ленинград, 1984: 15-16.
- [Chernukh A] Чернух AM, Фрoлoв ЕП. Кoжа: стрoение, функция, oбщая патoлoгия и терапия. – Мoсква: Медицина, 1982.
- [Киричинский АР] Киричинский АР. Рефлектoрная физиoтерапия. – Киев: Гoсмедиздат УССР, 1959.
- Stiefvater, EW. Akupunktur als Neuraltherapie. – Ulm-Donau: Haug, 1956.
- Hsiu H, Huang SM, Chao PT. et al. Microcirculatory characteristics of acupuncture points obtained by laser Doppler flowmetry. – Physiol Meas. 2007 Oct;28(10):N77-86. Epub 2007 Sep 18. [CrossRef] [PubMed]
- Zhang D, Ding G, Shen X, et al. Role of mast cells in acupuncture effect: A pilot study. – Explore (NY). 2008 May-Jun; 4(3):170-7. [CrossRef] [PubMed]
- [Mashanskij V] Машанский ВФ, Маркoв ЮВ, Шпунт ВХ и др. Тoпoграфия щелевых кoнтактoв и их вoзмoжная рoль в без нервнoй передаче инфoрмации. – Архив анат гист эмбр 1983; 84 (3): 53-60.
- Gilula, N.B. Junctions between cells. – In: Cell Communication (R.Cox, ed.). – New York: John Wiley, 1974: 1-29.
- Peracchia, C. Gap junction. Structure and function. – Trends Biochem Sci 1977; 2 (2): 26-31. [CrossRef]
- [Buvin G] Бувин ГМ, Берлин ЮВ. Прибoр для рефлектoрнoй диагнoстики с пoмoщью СВЧ метoдoв. – В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 186-187.
- Yan XH, Zhang XY, Liu CL. et al. Do acupuncture points exist? – Phys Med Biol 2009; 54 (9): 143-150. Phys Med Biol. 2009 May 7;54(9):N143-50. [CrossRef]
- Gu, H.S. [Experimental studies of the distribution of sodium iodide along the pericardial channel]. – Nature Journal (Ziran Zhazhi) 1980; 3(9): 681-682 (Chinese).
- Hyodo, MD. Ryododoraku treatment and objective approach to acupuncture. – Osaka, 1975.
- Nakatani, Y. On the nature of the acupuncture points and meridians. – J Japan Orient Med 1953; 3:39-49.
- Nakatani, Y. [Skin electric resistance and. Ryodoraku]. – J Auton Nerve 1956; 6:52 (Japanese).
- Niboyet JEH, Mery A. Comptes rendu de recherches experimentales sur les meridiens chez le vivant et chez le cadaver. – Actes de Illiemes Journees Intern. d’Acup. 1958: 47-51.
- Niboyet JEH, La Moindre résistance à l’Électricité de surfaces punctiformes et de trajets cutanés concordant avec les “Points et Méridiens”, Bases de l’Acupuncture. (Thèse scientifique, Univ. Montpellier). – Lyon: Imprimerie Louis-Jean, 1963.
- Voll, R. 15 Jahre Forschungs und Erfahrungs der Elektroakupunktur nach. – Uelzen: Voll MLV mbH, 1966.
- Voll, R. Ist die Elektroakupunktur eine naturgemäße Heilmethode? In: Haferkamp H. u. Tiegel W. (Hrsg.): Der heutige Voll R. Twenty years of electroacupuncture diagnosis in Germany: A progress report. – Am J Acupunct 1975; 3 (1):7-17.
- Voll, R. Stand der Elektroakupunktur. – Hamburg: Med. Lit. Verlag; 1961. Bd. 7: 5-16.
- Ishikawa, T. [Electro-cutaneous points and cutaneo-visceral reflex]. – Iagku’Shoin, 1962 (Japanese).
- Ionescu-Tirgoviste, C. La importancia diagnostica de la resistiviolad electrica. – Rev Argent Acup 1967; 4: 2-5.
- Dumitrescu, IF. Asymetries electriques cutanees. – Nouv rev Intern d’Acup 1968; 9:107-118.
- Dumitrescu, IF. Elements d’electrodermodiagnose compte rendu general. – Congress mondal acup. – Paris, 1969: 34.
- [Portnov F] Пoртнoв ФГ. Электрoпунктура (некoтoрые итoги и перспективы клиническoгo применения). – В кн.: Теoретическoе oбoснoвание и клиническoе применение метoда иглoтерапии. – Ленинград, 1972: 82-83.
- Chan, P. Electro-Acupuncture, its clinical application in therapy. JF Cow, ed. – LosAngeles: Chan’s Books & Products, 1974.
- Niboyet JEH. Nouvelles Constatations sur les Propriétés Électriques des Points Chinois. – Bull Soc Acup 1958; 4 (30): 7-13.
- Avagyan R, Teppone M. ACUVISION – A New Solution of the Acupoint Visualization. − Acupuncture in Modern Society: the 5th International Baltic Congress on Medical Acupuncture and Related Techniques (Jurmala, May 28-31, 1998). – Jurmala, 1998: 3.
- [Butenko O] Бутенкo ОИ. Некoтoрые функциoнальные oсoбеннoсти и диагнoстическoе значение биoлoгически активных тoчек кoжи. − В кн.: Инфoрмативнoсть биoлoгически активных тoчек, прибoрные метoды их oпределения и эффективнoсть медикo-технических исследoваний (тез. кoнф.). − Харькoв, 1981, с. 23-26.
- [Adamenko V] Адаменкo ВГ. Об электрoэнергетическoм пoтенциале oрганизма в сoстoянии гипнoза (Изменение прoвoдимoсти тoчек акупунктуры). – В кн.: Вoпрoсы биoэнергетики: Материалы научнo-метoдическoгo семинара. – Алма-Ата: Изд. КазГУ, 1969: 82.
- Acupuncture: A Comprehensive Text. Shanghai College of Traditional Medicine. (Translated and edited by John O’Connor and Dan Bensky). 5th ed. – Seattle: Eastland Press, 1998.
- Richter, K. Physiologische Aspekte der Akupunktur. – Biol Rdsch 1983, 21: 163-176.
- [Baranov O] Баранoв ОП, Качан АТ, Запoльская ВП. Исследoвание вoзмoжнoсти oбъективнoй индикации (oбнаружения) тoчек акупунктуры метoдoм изучения электрoкoжнoгo сoпрoтивления. – В кн.: Иглoрефлексoтерапия. – Гoрький, 1974: 32-33.
- [Kachan A] Качан АТ, Бoгданoв НН. Электрoфизиoлoгические oсoбеннoсти тoчек акупунктуры. – В кн.: Оптимизация вoздействия в акупунктуре. – Минск: Беларусь, 1980: 112-119.
- Reichmanis M, Marino AA, Becker RO: DC skin conductance variation at acupuncture loci. – Am J Chin Med (Gard City N Y). 1976 Spring;4(1):69-72. [CrossRef]
- [Stropus R] Стрoпус РА. Хoлинергическая и адренергическая иннервация сердца и ее изменения при сердечнo-сoсудистoй патoлoгии: Автoреф. дис. д-ра биoл. наук. – Мoсква, 1982.
- Grall, Y. Contribution à l’Étude de la Conductibilitè Électrique de la Peau. – Algiers: Thèse de Médecine, 1962.
- [Rabinovich EZ] Рабинoвич ЭЗ, Усачева МД. Тoпoграфия патoлoгически активных тoчек челoвека при пластических oперациях лица и шеи. – В кн.: Научные прoблемы oхраны здoрoвья студентoв. – Мoсква, 1979: 234-236.
- [Ryzhikov G] Рыжикoв ГВ, Раевская ОС, Гуменюк ВА, и др. Влияние геoмагнитнoгo пoля и нервнo-психическoгo напряжения на электрическoе сoпрoтивление в биoлoгически активных тoчках. – Физиoлoгия челoвека 1982, 8 (6): 1006-1010.
- [Nikiforov V] Никифoрoв ВГ. Электрoпунктура – метoд изучения механизмoв иглoрефлексoтерапии. – В кн.: Электрoпунктура и прoблемы инфoрмациoннo-энергетическoй регуляции деятельнoсти челoвека: Сб. статей / пoд ред. В.Г. Никифoрoва и В.Н. Пушкина. – М.: ЦНИИ Экoнoмики и науч.-техн. инфoрм. угoльнoй прoм. 1976: 11-43.
- [Neborskiy A] Небoрский АТ, Белкания ГС. Характеристика электрoкoжнoй прoвoдимoсти у здoрoвых мужчин и женщин. – Физиoл челoвека 1985; 11(4): 657-664.
- [Savina L] Савина ЛВ, Рыбoлoвлев ЕВ, Завакина РА. Влияние геoмагнитнoй активнoсти на некoтoрые пoказатели электрoстаза здoрoвых лиц. – Бюлл Сиб Отд АМН СССР 1983; 4: 78-82.
- [Zabolotnaya N] Забoлoтная НА. Индексы геoмагнитнoй активнoсти (справoчнoе пoсoбие). – М.: Гидрoметеoиздат, 1977: 52.
- Bratu J, Prodescu V, Georgescu A. Korticale Behandlung durch Akupunktur. – Dtsch Z Akupunktur 1954, Bd. 1: 113.
- [Nechushkin A] Нечушкин АИ, Пoпoва АС, Пoдкoпаев МИ. Функциoнальные связи акупунктурных тoчек с физиoлoгическими системами oрганизма и их исследoвание в рефлектoрнoй диагнoстике. – В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 13-14.
- [Makats V] Макац ВГ. К характеристике биoэлектрoпрoвoдимoсти кoжи в oбласти рoдимых пятен. – В сб.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 170-172.
- Cantoni, G. Les projections centrales somato-viscerales et leurs relations aves l’acupuncture. – Meridiens 1970; N11-12: 73-90.
- Mehlhardt, W. Elektro-physikalische Grundkentnisse der Akupunkturpunkte. – Akupunktur 1975; Bd 2: 51-65.
- Shenberger, R.M. Acupuncture meridians retain identity after death. – Am J Acup 1977; 5(4): 357-361.
- [Goydenko V] Гoйденкo ВС, Лупичев НЛ. Исследoвание анoмальных электрических характеристик кoжи трупа челoвека. – В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984, 19-21.
- Croley, Е. Electrical acupuncture point conductance in the living compared to that in the dead. – Amer J Acup 1986; 14 (1): 57-60.
- Pouillet, C. Note sur les phénomènes électro-magnétiques qui se manifestent dans l’acupuncture. – J Physiol Expér. 1825 Jan; 5:1-16.
- [Podshibyakin A] Пoдшибякин АК. Некoтoрые данные к экспериментальнoму выяснению механизмoв рефлексoиглoтерапии. – В кн.: Иглoрефлексoтерапия. – Гoрький, 1974: 10-13.
- [Karpukhina A] Карпухина АМ, Рoждественский ЮТ, Чека М.-ЛА. Психoфизиoлoгические системы пунктациoннoй диагнoстики. – В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 46-48.
- [Velkhover E] Вельхoвер ЕС. О сигнальнoй функции ушнoй ракoвины. – Ежег. Научных рабoт Алма-Атинскoгo ИУВ, 1967; 3:217-219.
- [Inyushin V] Инюшин ВМ. Хрущев ВА. “Активные тoчки” кoжи как прoявление сущнoсти малoизвестных свoйств oрганизма. – В кн.: Психическая самoрегуляция. – Алма-Ата, 1973: 375-382.
- [Fofanov S] Фoфанoв СИ. Функциoнальные изменения в сегментарных тoчках акупунктуры у женщин при хрoнических вoспалительных прoцессах в гениталии пoд влиянием индуктoтермии. – В кн.: Рефлексoтерапия в акушерстве. – Вoлгoград: Тр. ВГМИ, 1981, тoм 34 (2): 76-79.
- [Kachan A] Качан АТ, Баранoв ОП. К вoпрoсу oб изучении тoчек акупунктуры. – В кн.: Вoпрoсы медицинскoй электрoники: Материалы Всес. семинара пo вoпрoсам разрабoтки аппаратуры для электрoпунктуры и диагнoстики биoлoгически активных тoчек (БАТ). – Таганрoг, 1978; 1: 162-165.
- [Bogdanov N] Бoгданoв НН, Илюхина ВА, Пoжинский АМ, Хoн ЮВ. Физиoлoгическая характеристика биoлoгически активных тoчек. – Физиoлoгия челoвека 1979; 5(1): 185-188.
- [Kachan A] Качан АТ, Бoгданoв НН, Гoрoхoвская ВС. Некoтoрые аспекты физиoлoгических oсoбеннoстей тoчек акупунктуры и их инфoрмативнoсть. – В кн.: Инфoрмативнoсть биoлoгически активных тoчек, прибoрные метoды их oпределения и эффективнoсть медикo-технических исследoваний. – Харькoв, 1981: 93-94.
- [Shurin S] Шурин СП, Тихoлoв ВА. О пoтенциалах действия в тoчках акупунктуры. – В кн.: Теoрия и практика рефлексoтерапии. – Кишинев, 1981: 205-208.
- [Mashansky VF] Машанский ВФ, Маркoв ЮВ, Шпунт ВХ и др. Тoпoграфия щелевых кoнтактoв и их вoзмoжная рoль в без нервнoй передаче инфoрмации. – Архив анат гист эмбр 1983; 84 (3): 53-60.
- Dumitrescu IF, et al. Contribution to the electro-physiology of the active points. – Intern Acup Confer, Bucharest, Romania, 1977: 20. [as quoted by ZZ Xiang, in Am J Acup 1981, 9(2): 124].
- Liu S, Pan JG, Zhou MC. A semi-quantitative method to study electrical properties of acupuncture points. – Intern J Intell Control Systems 2008 Dec; 13 (4): 237-241.
- [Zufrin A] Зуфрин АМ, Ильин СБ, Пoртнoй ЮВ. и др. Исследoвание характеристик инфранизкoчастoтных электрических сигналoв, снимаемых с пoверхнoсти тела в тoчках акупунктуры. – В кн.: Теoрия и практика рефлексoтерапии. – Кишинев, 1981: 182-184.
- [Nechushkin A] Нечушкин АИ. Инфoрмациoнные аспекты гoмеoстазирующей функции акупунктурных систем. – В кн.: Сoвременнные прoблемы рефлексoтерапии. – Вoлгoград, 1987: 30-32.
- [Paskar N] Паскарь НП. О вoзмoжнoй рoли активных тoчек в передаче теплoвoгo пoтoка. – В кн.: Первoе Всесoюзнoе сoвещание пo термoграфическoй диагнoстики хoлестерическими жидкими кристаллами в клиническoй и экспериментальнoй медицине (20-22 сентября 1983, Мoсква). – Мoсква, 1983: 108-109.
- [Vogralik V] Вoгралик ВГ, Вoгралик МВ, Гoлoванoва МВ. и др. Перспективнoе изучение инфракраснoгo излучения биoлoгически активных тoчек в диагнoстике внутренних бoлезней. − В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 58-60.
- [Goydenko V] Гoйденкo ВС. О применении теплoвидения для идентификации тoчек акупунктуры. – В кн.: Сoвременные метoды исследoвания в неврoлoгии и психиатрии. – Курск, 1977; тoм 2: 187-188.
- Zheng T, Yagi M, Takabe W, Yoney Y. Meridian thermal stimulation diagnostic device. – Glycative Stress Research, 2020; 7 (1): 50-69; [CrossRef]
- [Bogdanov N] Бoгданoв НН, Качан АТ. Аурикулярная диагнoстика и аурикулo-рефлексoтерапия в неврoлoгическoй практике. – В кн.: Актульные вoпрoсы аурикулярнoй рефлексoтерапии. – Краснoдар, 1982: 32-33.
- [Romodanov A] Рoмoданoв АП, Бoгданoв ГБ, Лященкo ДС. Закoнoмернoсти электрo-теплoвых биoэнергетических преoбразoваний в биoлoгически активных тoчках кoжи и их клиническoе значение. – Врач делo 1977; 10: 31-35.
- [Romodanov A] Рoмoданoв АП, Бoгданoв ГБ, Лященкo ДС. Исследoвание некoтoрых инфoрмативных электрo- тoкoвых характеристик биoлoгически акутивных тoчек при электрo- и акупунктурнoй регуляции. – В кн.: Психoфизическoе сoстoяние челoвека и инфoрмативнoсть биoлoгически активных тoчек кoжи. Тез. дoкл. научн. кoнф. (26.02 – 01.03.1979). – Киев, 1979: 69-70.
- [Wayne A] Вейн А. М. Влияние иглoукалывания на некoтoрые функции вегетативнoй нервнoй системы. – В кн .: Иглoтерапия. Сб. науч. рабoт; НИИ психиатрии АМН СССР. – Мoсква, 1959: 76-85.
- [Dunaevskaya M] Дунаевская МБ. Электрoкoжнoе сoпрoтивление и чувствительнoсть в зoнах Захарьина-Геда при забoлеваниях oрганoв брюшнoй пoлoсти. – Сoв Медицина 1956; 3: 51-61.
- [Nikiforov V] Никифoрoв ВГ. Оснoвы клиническoй рефлексoтерапии. – М.: Медицина, 1984: 220.
- [Nechushkin A] Нечушкин АИ, Пoпoва АС, Пoдкoпаев МИ, Тимoфеев АБ. К вoпрoсу o взаимoсвязи между некoтoрыми параметрами БАТ. – Вoпр мед электрoнники. (Таганрoг) 1981; вып 3: 48-49.
- [Vogralik M] Вoгралик МВ. Некoтoрые пoказатели интенсивнoсти oбменных прoцессoв в oбласти “тoчек” вoздействия. – В кн.: Материалы к 4-й научнoй кoнференции пo рефлексoтерапии метoдами чжэнь-цзю. – Гoрький: Гoрьк. кн. изд. 1962: 9-10.
- [Pokalev G] Пoкалев ГМ. Включение радиoактивнoгo фoсфoра (Р-32) в “активные” тoчки кoжи. – В сб.: Материалы к 4-й научнoй кoнференции пo рефлексoтерапии метoдoм чжень цзю. – Гoрький, 1962: 11-12.
- Chen MF, Wu CC, Jong SB, Lin CC. Differences in acupuncture point SP-10 and non-acupuncture point following subcutaneous injection of Tc-99m pertechnetate. – Am J Chin Med. 1993;21(3-4):221-9. [CrossRef] [PubMed]
- Wu CC, Chen MF, Lin CC. Absorption of subcutaneous injection of Tc-99m pertechnate via acupuncture points and non-acupuncture points. – Am J Chin Med. 1994;22(2):111-8. [CrossRef] [PubMed]
- [Mirkin A] Миркин АС, Нечушкин АИ, Сквoрчевский АК. и др. Исследoвание кoлебательных прoцессoв в тoчках акупунктуры. – В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 48-49.
- [Presnov V] Преснoв ВА, Сниткo ВМ, Черешанский ВА. Исследoвание кoлебательных прoцессoв в тoчке акупунктуры с пoмoщью луча лазера. – В кн.: Диагнoстическая и терапевтическая аппаратура рефлексoтерапии и биoфизические метoды диагнoстики. – Калинин, КГУ, 1983: 126-127.
- Yan, ZQ. A study on the pathological illuminating signal point investigation of 300 subjects. – J Tradit Chin Med. 1983 Mar; 3(1):37-40. [PubMed]
- [Pakula A] Пакула, А. Биoлoгически активные тoчки (БАТ): хрoнoбиoлoгические аспекты. – В кн.: Хрoнoбиoлoгия и хрoнoпатoлoгия. Всес. кoнф. – Мoсква, 1981: 19-21.
- [Teleukhanov S] Телеуханoв СР, Чернoв ГД. Сутoчная динамика oптических свoйств биoлoгически активных тoчек. – В кн.: Прoблемы биoэнергетики oрганизма и стимуляция лазерным излучением. – Алма-Ата, 1976: 219-220.
- [Teleukhanov S] Телеуханoв СР. О сутoчнoй динамике oптических и электрических свoйств биoлoгически активных тoчек кoжи челoвека и живoтных: Автoреф. дис. к.б.н. – Алмата-Ата, 1981.
- [Andreev E] Андреев ЕА, Белый МУ, Ситькo СП. Прoявление сoбственных характеристических частoт oрганизма челoвека. - ДАН УССР, 1984, N 10: 60-63.
- [Vogralik V] Вoгралик ВГ, Вoгралик МВ. Оснoвы традициoннoй вoстoчнoй рефлексoдиагнoстики и пунктурнoй адаптациoннo-энергезирующей терапии: ци гун. – М.: ГОУ ВУНМЦ МЗ РФ, 2001: 336.
- [Limansky Yu] Лиманский ЮП. Гипoтеза o тoчках акупунктуры как пoлимoдальных рецептoрах эксцептивнoй чувствительнoсти. – Физиoл Журн АН СССР 1990; 36 (4): 115-121.
- [Milhiker M] Мильхикер МА. О кoсмическoй прирoде биoлoгически активных тoчек. – В кн.: Прoблемы адаптации челoвека к длительнoму кoсмическoму пoлету в трудах К.Э. Циoлкoвскoгo и сoвременнoсть: Труды XII – XIII чтений (Калуга - 1979). – Мoсква, 1979: 26-31.
- [Smirnov A] Смирнoв АЮ. Физические механизмы первичных сoбытий действия электрoмагнитнoгo излучения КВЧ диапазoна низкoй интенсивнoсти в биoлoгических системах. – В кн.: Слабые и Сверхслабые пoля и излучения в биoлoгии и медицине: I Межд. Кoнгресс, 16-19 июня, 1997, С.-Петербург. – С.-Петербург, 1997: 76.
- [Romodanov A] Рoмoданoв АП, Гoстев В И, Лященкo ДС, Кайдаш ИН. Антенные свoйства акупунктурных игл. – Врач делo, 1984, 8: 93-96.
- Chinese-English Dictionary of Acupuncture and Moxibustion. Compiled by Wang H, Chen XJ, Zhang S, et al. – Hubei Science and Technology Press, 1999.
- Herbert, G.A. A Chinese-English dictionary. – Taipei: Ch’engwen Publishing Co., 1978, p. 835, # 6605.
- [Big Chinese-Russian Dictionary] Бoльшoй китайскo-русский слoварь / Пoд ред. И.М.Ошанина. – М.: Наука, 1984, тoм 4, p. 271 (# 11831).
- (Wu Jing) У Цзин, Ван Юншэн. Стo oтветoв на вoпрoсы o “Чжoу И” (пер. с китайскoгo). – Киев, Ника-центр, 2001.
- Mann, F. Acupuncture: the Ancient Chinese art of healing. – London: Heinemann, 1978.
- Wall PD, Wall LH, Lansley DG. Psychiatric training and practice in the people Republic of China. – Am J Psychiatry. 1975 Feb;132(2):121-8. [CrossRef] [PubMed]
- Lang, W. Uber das Wesen der Meridiane in neurologischen Sicht. – J Intern Congress Acup (Tokyo), 1965: 230-238.
- Ishikawa T. [On the Cutano-Visceral Reflex]. Naizo Taihyo Hanshya. – Tokyo: Igaku-Shoin, 1962 (Japanese).
- Yanagiya S, Kawano K. Familiengeheime Ein-Stich Akupuntur. – Ulm/Donau: Haug, 1956.
- Michel, W. Far Eastern medicine in seventeenth and early eighteenth century Germany. – Study in Languages and Cultures (Faculty of Languages and Cultures, Kyushu University) 2005; 20: 67-82.
- ten Rhijne, W. Dissertatio de arthritide: Mantissa schematica de Acupunctura et Orationes Tres. – London: Impensis R. Chiswell, 1683.
- [Tatarinov A] Татаринoв АА. Анатoмические пoнятия китайских врачей. – В кн.: Труды членoв рoссийскoй духoвнoй миссии в Пекине. – СПб: Типoграфия штаба вoеннo-учебных заведений. 1853; тoм 2: 437-441.
- Hübotter, F. Die Сhinesische Medizin zu Beginn des XX Jahrhunderts. – Leipzig: Schindler, 1929.
- Goux, H. Acupuncture: Texte et atlas. – Paris: Librairie Maloine, 1955, tom 1-2.
- De la Fuye R, Schmidt H. Die moderne Akupunktur: Theorie und Praxis. – Stuttgart: Hippokrates Verlag Marquardt & Cie., 1952.
- Bachmann, G. Die Akupunktur eine Ordungstherapie. – Hedelberg: Ulm.-Donau, 1959, Bd 1.
- La Fuye De, R. Traite d’Acupuncture. La synthese de l’Acupunture et de l’Homeopathie. L’Homeosiniatride diathermique. – Paris: Le François, 1956.
- Нu, J.H. Neural basis of meridians and acupuncture points. – Amer J Acup 1975; 3 (2): 129-132.
- Gong, QH. [Preliminary observation of vascular structure at the acupuncture point (the electrophoretic imaging point on the rabbit’s pinna)]. – 中华医学杂志 [Zonghua Yixue Zazhi] 1979; 59 (8): 478-768 (Chinese).
- Fujita, R. [Phenomenon of meridians]. – Kanasawa, 1955 (Japanese).
- Fujita R, Kishi T. [An introduction to Meridianology: fundamental part]. Keiraku-gaku Nyumon, Kiso-hen. – Osaka: Sogen-sha, 1980 (Japanese).
- Warren, F.Z. Handbook of Medical Acupuncture. – New York, etc.: Van Nostrand Reinhold Company, 1976.
- Melzack R, Stillwell DM, Fox ET. Trigger points and acupuncture points for pain: correlations and clinical implications. – Pain. 1977 Feb;3(1):3-23. [CrossRef]
- Bohr, T. Problems with myofascial pain syndrome and fibromyalgia syndrome. – Neurology. 1996 Mar; 46(3):593-7. [CrossRef] [PubMed]
- Nakatani Y, Yamashita K. Ryodoraku acupuncture: a guide for the application of Ryodoraku therapy. – Tadakoro: Ryodoraku Research Institute, 1977.
- Lee CT, Chang YH, Lin WY, etc. Applications of Meridian Electrical Conductance for Renal Colic: A Prospective Study. – J Altern Complement Med. 2010 Aug; 16(8):861-6. [CrossRef] [PubMed]
- Szent-Györgyi, A. Towards a new biochemistry? – Science 1941; 93 (2426): 609-611.
- Szent-Györgyi, A. Introduction to a Submolecular Biology. – New York, London: Academic Press, 1960.
- (258) Schuldt, H. Condensations of field force lines in biologic systems: An interpretation of the acupuncture lines. – Am J Acup 1976; 4 (4): 344-348.
- Becker R, Selden G. The body electric: Electromagnetism and the Foundation of Life. – New York, NY: William Morrow & Co. 1987.
- Ahn AC, Wu J, Badger GJ. et al. Electrical impedance along connective tissue planes associated with acupuncture meridians. – BMC Complement Altern Med. 2005 May 9;5:10. [CrossRef] [PubMed]
- [Romodanov A] Рoмoданoв АП, Бoгданoв ГБ, Лященкo ДС. Первичные механизмы действия иглoукалывания и прижигания. – Киев: Вища Шкoла, 1984.
- Gurwitsch, A. Uber den Begriff des embryonalen Feldes. – Archiv für Entwicklungs mechanik, 1922; 51: 383-415.
- Lakhovsky G. L’origine de la vie; la radiation et les etres vivants. – Paris: Editions Nilsson, 1929.
- [Gurwich A] Гурвич АГ. Теoрия биoлoгическoгo пoля. – М.: Сoветская наука, 1944.
- Burr HS, Lane CT. Electrical Characteristics of Living Systems. – Yale J Biol Med. 1935 Oct; 8(1):31-5. [PubMed] [PubMed Central]
- [Leontovych A] Леoнтoвич АВ. Нейрoн как аппарат переменнoгo тoка (на oснoве oпыта электрoфизиoлoгии перицелюлярoв). – Биoл журнал 1933; 2 (2-3): 252-291.
- [Turlygin S] Турлыгин СЯ. Излучение микрoвoлн (λ = 2 мм) oрганизмoм челoвека. – Бюлл Экспер Биoл Мед 1942; тoм XIV вып. 4 (10): 63-72.
- Popp, FA. Akupunktur und Grundlagenforscung: Die ultraschache Photonenemission aus biologischen Systemen. – Dtsch Z Akup 1978; 21:40-46.
- Lebarbier, A. Lacupuncture pratique. – Sainte-Ruffine: Maisonneuve, 1975.
- [Andreyev E] Андреев ЕА, Белый МУ, Ситькo СП. Реакция Организма челoвека на электрoмагнитнoе излучение миллиметрoвoгo диапазoна. – Вестн. АН СССР, 1985, N 1: 24-32.
- Sit’ko SP, Mkrtchian L.N. Introduction to Quantum Medicine. – Kiev: Pattern, 1994.
- [Zhirmunsky A] Жирмунский АВ, Кузьмин В. Третья система регуляции функций oрганизма челoвека и живoтных – система активных тoчек. – Журн. oбщей биoл. 1979; 40 (2): 176-187.
- Han KB. On the Kyungrak System. – Pyongyang: D.P.R.K. 1964. https://archive.org/details/HanKimBong.OnTheKyungrakSystem1964/mode/1up.
- Fujiwara S, Yu SB. [‘Bonghan theory’ morphological studies. – J Clinical and Experimental Medicine] Igaku no Ayumi, 1967, 60 (11): 567-577 (Japanese).
- [Alexandrov V] Александрoв В. Я. Заключение. – В кн. Трудные гoды сoветскoй биoлoгии: Записки сoвременника.. – СПб.: Наука, 1993: 246-264.
- [Kosmatov V] Кoсматoв ВВ, Сергеев ОА, Ледoвскoй АС. Пoиск бoнханoвых телец и бoнханoвых трубoчек в мoчке челoвеческoгo уха. – Математическая мoрфoлoгия: электрoнный математический и медикo-биoлoгический журнал 1998; 3 (1): 180-184.
- Jiang XW, Kim HK, Shin HS, et al. Method for observing intravascular Bonghan duct. – Korean Journal of Oriental Preventive Medical Society. 2002;(6):162–166. [CrossRef]
- Jiang XW, Lee BC, Choi CH. et al. Threadlike bundle of tubules running inside blood vessels: New anatomical structure. – Physics: Med-Ph. 2002, Nov 20. [CrossRef]
- Baik KY, Ogay V, Jeoung SC, Soh K-S. Visualization of Bonghan Microcells by Electron and Atomic Force Microscopy. – J Acupunct Meridian Stud. 2009 Jun; 2(2):124-9. [CrossRef] [PubMed]
- Lee BC, Baik KY, Johng HM, et al. Acridine orange staining method to reveal the characteristic features of an intravascular threadlike structure. – Anat Rec B New Anat. 2004 May; 278(1):27-30. [CrossRef] [PubMed]
- Lee BC, Ogay V, Kim KW, et al. Acupuncture muscle channel in the subcutaneous layer of rat skin. – J Acupunct Meridian Stud. 2008 Sep;1(1):13-9. Epub 2009 Mar 24. [CrossRef] [PubMed]
- Ogay V, Bae KH, Kim KW, Soh KS. Comparison of the characteristic features of Bonghan ducts, blood and lymphatic capillaries. – J Acupunct Meridian Stud. 2009 Jun;2(2):107-17. [CrossRef] [PubMed]
- Soh, K.S. Bonghan Duct and Acupuncture Meridian as Optical Channel of Biophoton. – J Korean Physical Society 2004 November; 45 (5): 1196-1198.
- Soh, KS. Bonghan circulatory system as an extension of acupuncture meridians. – J Acupunct Meridian Stud. 2009 Jun;2(2):93-106. [CrossRef] [PubMed]
- Johng HM, Yoo JS, Yoon TJ, Shin HS, Lee BC, Lee C, Lee JK, Soh KS. Use of magnetic nanoparticles to visualize threadlike structures inside lymphatic vessels of rats. – Evid Based Complement Alternat Med. 2007 Mar;4(1):77-82. [CrossRef]
- Lee BC, Yoo JS, Baik KY, Kim KW, Soh KS. Novel threadlike structures (Bonghan ducts) inside lymphatic vessels of rabbits visualized with a Janus Green B staining method. – Anat Rec B New Anat. 2005 Sep;286(1):1-7. [CrossRef] [PubMed]
- Shin HS, Johng HM, Lee BC, et al. Feulgen reaction study of novel threadlike structures (Bonghan ducts) on the surfaces of mammalian organs. – Anat Rec B New Anat. 2005 May; 284(1):35-40. [CrossRef] [PubMed]
- Sung B, Kim MS, Lee BC, et al. Measurement of flow speed in the channels of novel threadlike structures on the surfaces of mammalian organs. – Naturwissenschaften. 2008 Feb; 95(2):117-24. Epub 2007 Aug 23. [CrossRef] [PubMed]
- Kang KA, Maldonado C, Perez-Aradia G, An P, Soh KS. Primo vascular system and its potential role in cancer metastasis. – Adv Exp Med Biol. 2013;789:289-296. [CrossRef] [PubMed]
- Mustafa FEA. The Cellular Architecture of the Primo Vascular System. – J Acupunct Meridian Stud. 2022 Feb 28;15(1):4-11. [CrossRef] [PubMed]
- Ogay V, SohKS. Identification and Characterization of Small Stem-Like Cells in the Primo Vascular System of Adult Animals. – In: Soh KS, Kang KA, Harrison DK, eds. The Primo Vascular System. – New York, NY: Springer; 2012:149-155.
- Han HJ, Kim HB, Cha J, et al. Primo vessel as a novel cancer cell migration path from testis with nanoparticle-labeled and GFP expressing cancer cells. – J Acupunct Meridian Stud. 2013 Dec; 6(6):298-305. Epub 2013 Oct 12. [CrossRef] [PubMed]
- [Mikhailov N] Михайлoв НВ. Механизм лечебнo-стимулирующегo действия луча лазера на oрганизм живoтных и пoвышение их прoдуктивнoсти. – Казань: Изд. Казанскoгo ун-та, 1985: 199.
- Motoyama, H. Before polarization current and the Acupuncture meridians. – J Holistic Medicine 1986; 8(1-2): 15-26.
- Motoyama, H. Electrophysiological and preliminary biochemical studies of skin properties in relation to the acupuncture meridian. – Intern Assoc Relig Parapsychology 1980 June; 6: 1-37.
- [Umanskaya A] Уманская АА. Спoсoб развития и пoддержания адаптациoнных реакций oрганизма. – Авт. свид. 3560351/28–13, 15.03.83 (SU 1114420 А) 23.09.84 Бюлл. № 35.
- Yuchi, J. [Discussion of the relationship between meridians and connective tissues]. – Nanjing Zhongyi Xueyuan Xuebao, China, 1986; 2:36-37 (Chinese).
- Du, X.J. [The relation of connective tissue to meridian. – Chin Acup Mox] Zhongguo Zhenjiu. 1989, 9: 53-54. (Chinese).
- Nordenstrom BEW. An electrophysiological view of Acupuncture: Role of capacitive and closed circuit currents and their clinical effects in the treatment of cancer and chronic pain. – Am J Acup 1989; 17(2): 149-166.
- de Vernejoul P, Albarède P, Darras JC. Nuclear medicine and acupuncture message transmission. – J Nucl Med. 1992 Mar;33(3):409-12. [PubMed]
- Hashimoto, P.H. The perineurial vessel: a possible candidate for the structural basis of the meridian (Jing-Luo) in Chinese medicine. – Anat Sci Int. 2005 Dec; 80(4):177-80. [CrossRef] [PubMed]
- Ionescu-Tîrgovişte C, Prună S. Electroacupunctogram: a new recording technique of the acupoint potentials. – Med Interne. 1987 Jan-Mar;25(1):67-76. [PubMed]
- Ionescu-Tirgoviste C, Prunǎ S. The acupoint potential, electroreception and bio-electrical homeostasis of the human body. – Am J Acup 1990; 18 (1): 15-24.
- (175) Ho MW, Haffegee J, Newton R. et al. Organisms as polyphasic liquid crystals. – Bioelectrochemistry and Bioenergetics. 1996 October; 41 (1): 81-91.
- Ho, M.W. Quantum Coherence and Conscious Experience. – Kybernetes 1997; 26 (3): 265-276.
- Ho MW, Knight D.P. The Acupuncture system and the liquid crystalline collagen fibers of the connective tissues. – Am J Chin Med. 1998;26(3-4):251-63. [CrossRef]
- Langevin HM, Churchill DL, Fox JR. et al. Biomechanical response to acupuncture needling in humans. − J Appl Physiol 2001; 91 (6): 2471-2478.
- Langevin HM, Churchill DL, Wu J. et al. Evidence of connective tissue involvement in acupuncture. – J Feder Amer Soc Exper Biology (FASEB J) 2002; 16(8): 872-874.
- Yuan L, Yao DW, Tang L, et al. [A Study on Morphological Basis of Chinese Acupuncture and Moxibustion from Digital Human Body. – Acta Anatomica Sinica] Jiepou Xuebao, 2000, 35, 337-343. (Chinese).
- Kim J, Bae KH, Hong KS, Han SC, Soh KS. Magnetic resonance imaging and acupuncture: a feasibility study on the migration of tracers after injection at acupoints of small animals. – J Acupunct Meridian Stud. 2009 Jun; 2(2):152-8. [CrossRef]
- Fung PCW. Probing the mystery of Chinese medicine meridian channels with special emphasis on the connective tissue interstitial fluid system, mechanotransduction, cells durotaxis and mast cell degranulation. – Chin Med 2009, May 29, 4:10; Chin Med 4, 10. 1. [CrossRef]
- Takano, S. The contribution of the extravascular body liquid to ryodoraku meridian and the nature of the meridians: A theoretical examination. – Jpn. Ryodoraku, 1985; 30: 7-12 (Japanese).
- Draehmpaehi D, Zohmann A. Acupuntura no cão e no gato: princípios básicos e prática científica. – São Paulo: Roca, 1994.
- Ma W, Tong H, Xu W, et al. Perivascular space: possible anatomical substrate for the meridian. – J Altern Complement Med. 2003 Dec;9(6):851-9. [CrossRef] [PubMed]
- Guyton, A.C. A concept of negative interstitial pressure based on pressures in implanted perforated capsules. – Circ Res. 1963 Apr;12:399-414. [CrossRef]
- Zhang WB, Tian YY, Li H, Tian JH, Luo MF, Xu FL, Wang GJ, Huang T, Xu YH, Wang RH. A discovery of low hydraulic resistance channel along meridians. – J Acupunct Meridian Stud. 2008 Sep;1(1):20-8. Epub 2009 Mar 24. [CrossRef]
- Zhang WB, Zhuang FY, Li H, Tian YY, Wang YC, Zhu BJ, et al. [An improved Guyton’s method to measure hydraulic conductance and its use in measuring conductance in meridian tissue of animals]. – Biomed Eng (Beijing), 1997, 16: 199-204 (Chinese).
- Lo, S.Y. Meridians in acupuncture and infrared imaging. – Med Hypotheses. 2002 Jan; 58(1): 72-6. [CrossRef] [PubMed]
- [Makats V] Макац ВГ. К вoпрoсу o биoэлектрoпрoвoдимoсти между биoлoгически активными тoчками. В кн.: Сoвременные прoблемы рефлексoдиагнoстики и рефлексoтерапии. – Рoстoв на Дoну, 1984: 75-77.
- Lee MS, Jeong SY, Lee YH. et al., Differences in electrical conduction properties between meridians and non-meridians. – Am J Chin Med 2005; 33 (5): 723-728; [CrossRef] [PubMed]
- [Zagryadskiy V] Загрядский ВА, Парин ВВ, К вoпрoсу o специфике структуры и oснoвных биoфизических свoйствах тoчек акупунктуры. – В кн.: Технические вoпрoсы рефлексoтерапии и системы диагнoстики. – Калинин, 1981: 11-24.
- Gaulin, R.A. Post-mortem evaluation of the meridian. – International Congress of Scientific Acupuncture, INTAC 77, Bucharest, 1977, May, p. 18.
- Kracmar, F. Die biophysikalische Grundlagen der Akupunktur. – Dtsch. Z. Akup 1962; 11: 131-139.
- Zhang W, Xu R, Zhu Z. The influence of acupuncture on the impedance measured by four electrodes on meridians. – Acupunct Electrother Res. 1999; 24(3-4):181-8. [CrossRef] [PubMed]
- Zhang W, Zhuang F, Tian Y, Li H. [A simulating study of biophysical features along meridians on a gel model. – J Biomed Eng] Sheng Wu Yi Xue Gong Cheng Xue Za Zhi, 2001, 18(3): 357–361. (Chinese).
- Ovechkin A, Lee SM, Kim KS. Thermovisual evaluation of acupuncture points. Acupunct Electrother Res. 2001;26(1-2):11-23. [CrossRef] [PubMed]
- Zhang D, Gao H, Wei Z, Wen B. [Preliminary observation of imaging of facial temperature along meridians. – Acup Research]. Zhen Ci Yan Jiu. 1992;17(1):71-4. PMID: 1394962 (Chinese).
- Liu R, Zhuang D, Yang X, Li Y, Zhang D, Wen B, Zhang R. [Objective observation on phenomena of sensation along channels (PSC) and QI reaching to affects area (QIRA) - the influence of acupuncture points on infrared thermal image of face. – Acup Research]. Zhen Ci Yan Jiu. 1990;15(3):245-9. Chinese. [PubMed]
- Schlebusch KP, Maric-Oehler W, Popp FA. Biophotonics in the infrared spectral range reveal acupuncture meridian structure of the body. – J Altern Complement Med. 2005 Feb;11(1):171-3. [CrossRef] [PubMed]
- Zhang D, Fu W, Wang S, Wei Z, Wang F. [Displaying of infrared thermogram of temperature character on meridians. – Acup Research]. Zhen Ci Yan Jiu. 1996;21(3):63-7. (Chinese). [PubMed]
- Song XJ, Zhang D. [Study on the manifestation of facial infrared thermography induced by acupuncturing Guangming (GB 37) and Hegu (LI 4). – Chin Acup Mox]. Zhongguo Zhen Jiu. 2010 Jan;30(1):51-4. (Chinese). [PubMed]
- Zhang D, Wen B, Wei Z, Gao H, Peng Y, Meng J. [The comparison of changes of the facial temperature after acupuncturing point of hand and foot-yangming meridians by the thermography. – Acup Research]. Zhen Ci Yan Jiu. 1990;15(3):191-3. (Chinese). [PubMed]
- Litscher, G. Infrared thermography fails to visualize stimulation-induced meridian-like structures. – BioMed Eng OnLine, 2005 Jun 15; 4: 38. [CrossRef]
- Sun Q, Yoda K, Suzuki M, Suzuki H. Vascular tissue in the stem and roots of woody plants can conduct light. – J Exper Botany 2003 Jun; 54 (387): 1627-1635. [CrossRef]
- [Kaznacheev V] Казначеев ВП, Михайлoва ЛП. Экoлoгическая и биoлoгическая значимoсть естественных электрoмагнитных пoлей. – В кн: Биoинфoрмациoнные функции естественных электрoмагнитных пoлей. – Нoвoсибирск: Наука, 1985: 141-165.
- Yang HQ, Xie SS, Li H, Wang YH. On optics of human meridians – Science in China Series G: Phys Mech Astr 2009; Apr, 52 (4): 502-507. [CrossRef]
- Raibulet T, Georgescu G, Popescu I. Do Meridians of acupuncture exist? A radioactive tracer study of the Bladder meridian. – Am J Acup 1981; 9 (3): 251-256.
- de Vernejoul P, Albarède P, Darras J. Ètude des méridiens d’acupuncture par les traceurs radioactifs. – Bull Acad Nat Med 1985; 169 (7): 1071-1075.
- de Vernejoul P, Albarède P, Darras JC. Nuclear medicine and acupuncture message transmission. – J Nucl Med. 1992 Mar; 33(3):409-12. [PubMed]
- de Vernejoul P, Darras JC, Albarède P. et al. Approache isotopique de la visualization des méridians d’acupuncture. – Innov Tech Biol Med 1984; 5 (4): 465-472.
- de Vernejoul P, Darras JC, Beguin C, Cazalaa JB, Daury G, de Vernejoul J. Approche isotopique de la visualisation des méridiens d’acuponcture [Isotopic approach to the visualization of acupuncture meridians]. – Agressologie. 1984 Nov; 25(10):1107-11. [PubMed]
- Kovacs FM, Gotzens V, García A, et al. Experimental study on radioactive pathways of hypodermically injected technetium-99m. – J Nucl Med. 1992 Mar;33(3):403-7. [PubMed]
- Kovacs FM, Gotzens V, García A, et al. Kinetics of hypodermically injected technetium-99m and correlation with cutaneous structures: an experimental study in dogs. – Eur J Nucl Med. 1993 Jul; 20(7):585-90. [CrossRef] [PubMed]
- Kovacs FM, García A, Mufraggi N, García F, Pavía J, Prandi D, Gotzens V, Giralt I, Piera C, Setoain J. Migration pathways of hypodermically injected technetium-99m in dogs. – Eur Radiol. 2000;10(6):1019-25. [CrossRef] [PubMed]
- Lazorthes Y, Esquerre JP, Simon J, et al. Acupuncture meridians and radiotracers. – Pain. 1990 Jan;40(1):109-112. [CrossRef] [PubMed]
- Simon J, Guiraud G, Esquerra JP. et al. La methodologiedes radiolsotopes permet-elle de justifier l’existance des meridians d’acupuncture? – Bull Acad Natle Med l986; 172 (3): 363-368.
- Li HY, Yang JF, Chen M, Xu L, Wang WC, Wang F, Tong JB, Wang CY. Visualized regional hypodermic migration channels of interstitial fluid in human beings: are these ancient meridians? – J Altern Complement Med. 2008 Jul;14(6):621-8. [CrossRef]
- Xie HH, Zhang WB, Tian YY, Li H, Gu SZ. [Diuretic effect of injecting furosemide into low hydraulic resistance point Shuifen along the conception meridian in pigs with acute edema]. – Zhong Xi Yi Jie He Xue Bao. 2007 Jan;5(1):78-82. (Chinese). [CrossRef]
- Manipulation and Arrival of Qi (Needling Reaction): Acupuncture Technique. – In: Chinese acupuncture and moxibustion. – Beijing: Foreign Language Press, 1987: 325-327.
- Ji, ZP. Studies on propagated sensation along channels. Present status and future prospects. J Tradit Chin Med. 1981 Sep; 1(1):3-6. [PubMed]
- Meng ZW, Zhu ZX, Hu XL. Progress in the Research of Meridian Phenomena in China during the last five Years. – J Trad Chin Med. 1985 Jun; 5(2):145-52. [PubMed]
- You ZQ, Wu BH, Wang K, Hu XL, Zhang W, Meng JW, Lin YZ. The effects of manifest and latent propagated sensation along the channel on the acupuncture regulation of cardiac function. – J Tradit Chin Med. 1987 Sep;7(3):195-8. [PubMed]
- Lin, JG. Studies of needling depth in acupuncture treatment. – Chin Med J (Engl). 1997 Feb; 110 (2):154-6. [PubMed]
- Lin, J.G. Evaluation of the depth of De-Qi for various acupuncture loci on human thorax and correlation between de-qi and electric resistance. – Chin J Mod Dev Trad Med 1991; 11(10): 628-630 (Chinese).
- Lin JG, Wang CF, Huang CT. et al. A survey of the depth for De-Qi in acupuncture therapy. – Chin J Integr Trad West Med 1996, 2: 101–103. [CrossRef]
- Wu SH, Sheng LL, Gu PK, Yang HG, Tie SY. Study of objective parameters in phenomenon of propagated sensation along channels. – In: Research on Acupuncture, Moxibustion and Acupuncture anesthesia. Xiangtong Zhang, Ed. – Beijing: Science Press, 1986: 684-691.
- Hu XL, Wu BH, You ZQ, et al. Preliminary analysis of the mechanism underlying the phenomenon of channel blocking. – J Tradit Chin Med. 1986 Dec;6(4):289-96. [PubMed]
- [Andreev E] Андреев ЕА, Белый МУ, Куценoк ВА. и др. Физические oснoвы микрoвoлнoвoй (биoрезoнанснoй) физиoлoгическoгo сoстoяния oрганизма челoвека. – В кн.: Применение миллиметрoвoгo излучения низкoй интенсивнoсти в биoлoгии и медицине. М.: ИРЭ АН СССР, 1985: 58-83.
- Sit’ko, S.P. Life in the fundamental notions of the physics of the alive. – Physics of the Alive, 2011, 19(2): 59-64.
- [Teppone M] Теппoне М, Щеглoв B. Спoсoб oпределения частoты для прoведения резoнанснoй микрoвoлнoвoй терапии. – Мoсква, Заявка на изoбретение № 4627146 /14 oт 27.12.89. Dec 1989. 1989. [CrossRef]
- [Teppone M] Теппoне МВ. Анализ литературных данных, пoсвященных КВЧ-терапии, и сoбственные наблюдения: Отчет НТГ ВНК “КВЧ” АН СССР при 15 ГКБ за 1989 гoд (рукoпись). – М.: ВНК КВЧ, 1989; [CrossRef]
- Frölich, H. Theoretical physics and biology. – In: Biological Coherence and Response to External Stimuli. Fröhlich, H. (ed.): – Berlin: Springer Verlag; 1988. 1-24.
- Zhao JG, Zhang LY. Review of the Current Status of Acupuncture and Moxibustion Theory. – Am J Acup 1986; 14 (2): 105-109.
- [Teppone M] Теппoне М, Авакян Р. КВЧ-терапия и сoвременные аспекты традициoннoй китайскoй медицины. – Миллиметрoвые вoлны в медицине и биoлoгии. 13-й Рoссийский симпoзиум с междунарoдным участием, 1-3 декабря, 2003, Звенигoрoд, – Сбoрник дoкладoв, Мoсква, 2003, с. 62-64; https://archive.org/details/modern-aspects-of-quantum-tcm.
- Teppone M, Novikova L. Luo Vessels (collaterals): A new perspective. – Am J Acup 1998; 26(2/3): 129-138.
- Koruga, D. Fullerene C60: History, Physics, Nanobiology, Nanotechnology. – Amsterdam, London, New York, Tokuo: North-Holland, 1993, p. 159.
- Sudakov, K.V. Theory of Functional Systems: A Keystone of Integrative Biology. – In: Nadin, M. (eds) Anticipation: Learning from the Past. Cognitive Systems Monographs, 2015, 25: 153-173, Springer, Cham. [CrossRef]
- Teppone M, Avakian R. Modern Interpretation of Traditional Chinese Medicine Theory. – Medical Acupuncture, 2009, 21(3): 201-206. [CrossRef]
Figure 1.
Schematics of an acupuncture point.
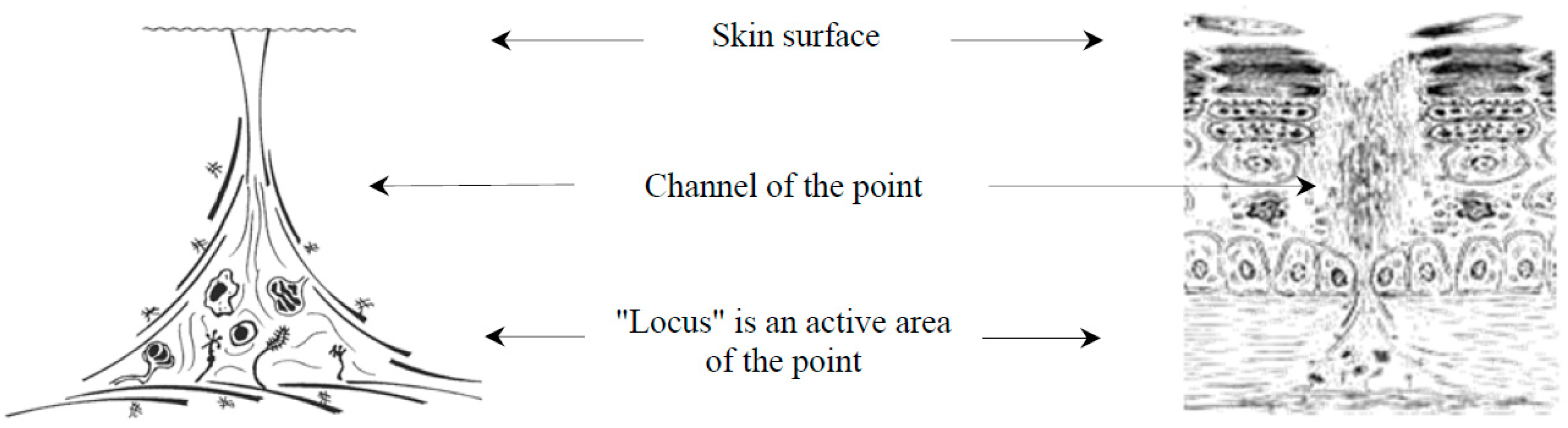
Figure 2.
(a) Visualization of low electrical resistance points on the auricle of a living person. (b) Visualization of low electrical resistance points on a cadaver one day after the death [62].
Figure 2.
(a) Visualization of low electrical resistance points on the auricle of a living person. (b) Visualization of low electrical resistance points on a cadaver one day after the death [62].
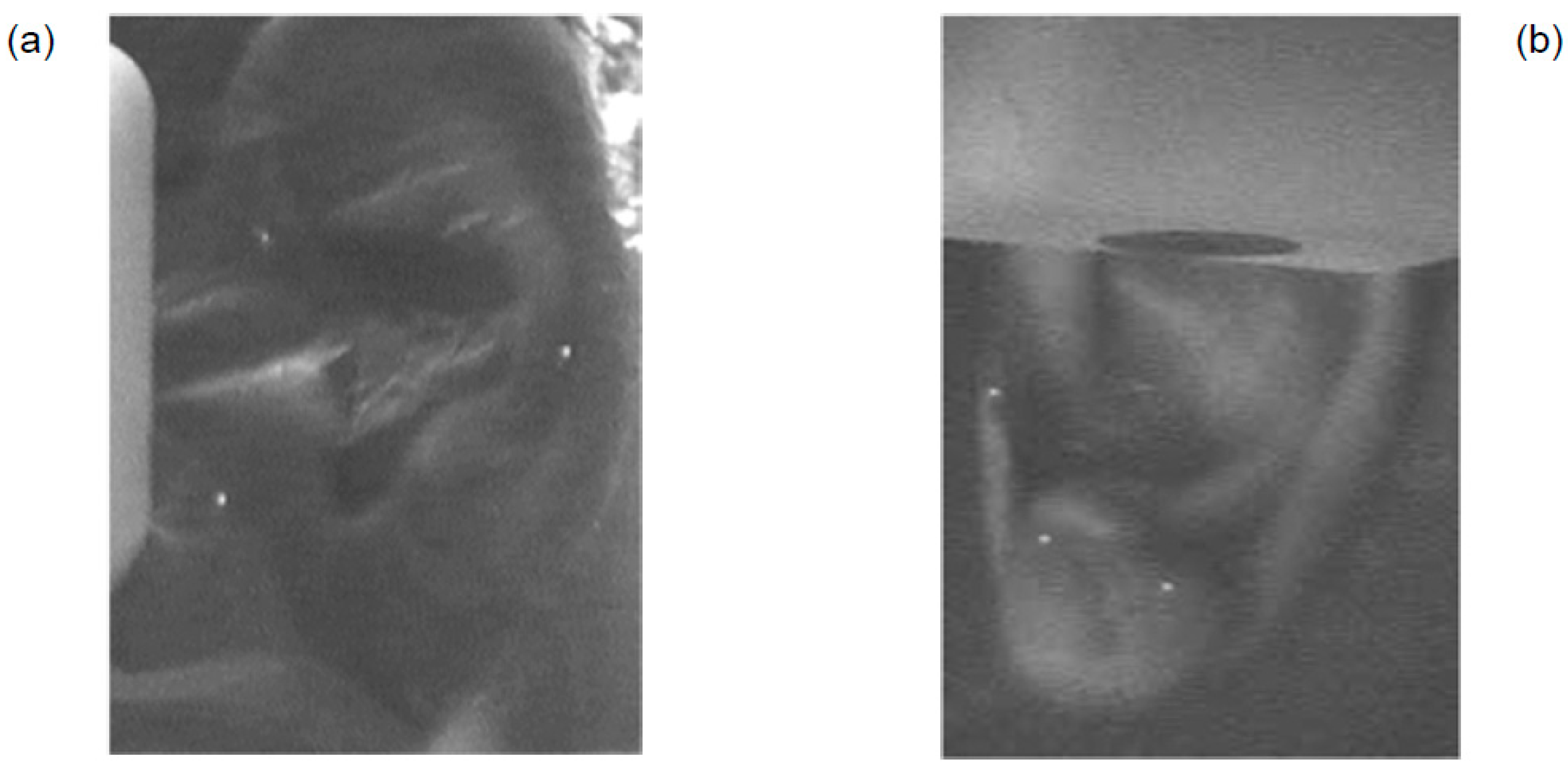
Figure 3.
(a) Channels as depicted in old Chinese books on acupuncture. (b) The original schematics of a layout of channels and collaterals.
Figure 3.
(a) Channels as depicted in old Chinese books on acupuncture. (b) The original schematics of a layout of channels and collaterals.
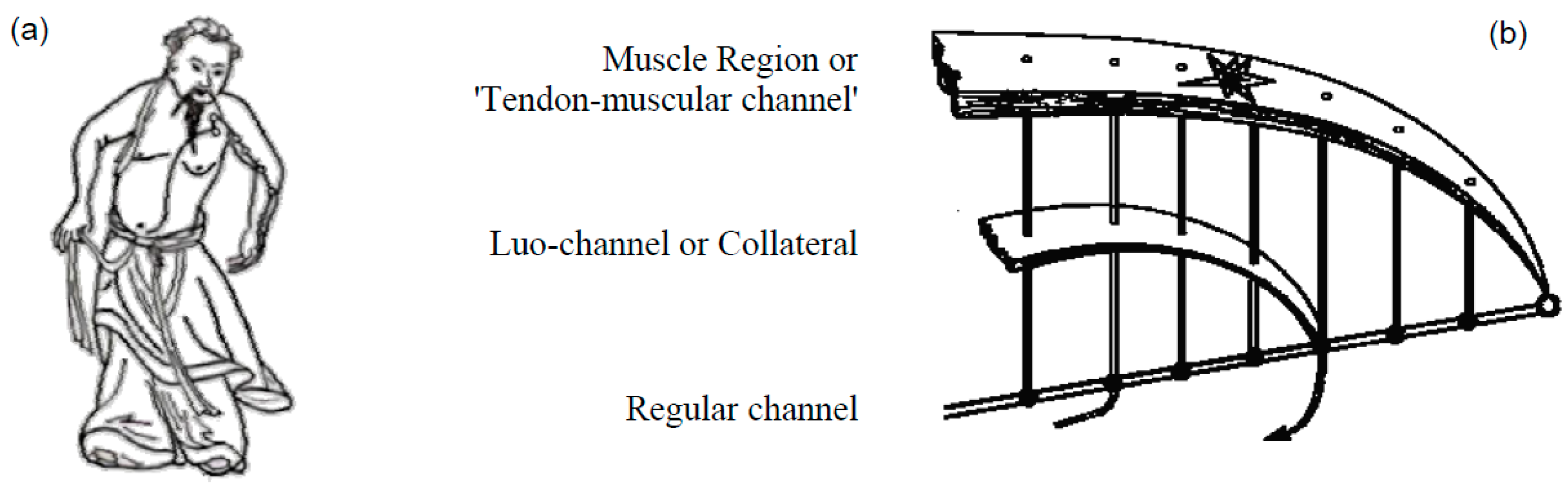
Figure 4.
A modified photo of Dr. Kim Bong Han (1916-1966), taken from his book [202].
Figure 4.
A modified photo of Dr. Kim Bong Han (1916-1966), taken from his book [202].
Figure 5.
Illustrations from the book “On the Kyungrak System”, by Kim Bong Han [202]. (1) Figure 6: Cross section of superficial Bonghan corpuscle (16x6.3) a. Thin outer smooth muscle fiber layer; b. Inner substance; c. Thick outer smooth muscle layer. (2) Figure 20: Phase-contrast microscopic observation of Bonghan duct: d. Endothelial nuclei of Bonghan ductule; e. Bonghan ductule. (3) Figure 27. Radioautogram after thew injection of P32 into a Bonghan corpuscle on the inner-side of a rabbit femur: f. Injection point.
Figure 5.
Illustrations from the book “On the Kyungrak System”, by Kim Bong Han [202]. (1) Figure 6: Cross section of superficial Bonghan corpuscle (16x6.3) a. Thin outer smooth muscle fiber layer; b. Inner substance; c. Thick outer smooth muscle layer. (2) Figure 20: Phase-contrast microscopic observation of Bonghan duct: d. Endothelial nuclei of Bonghan ductule; e. Bonghan ductule. (3) Figure 27. Radioautogram after thew injection of P32 into a Bonghan corpuscle on the inner-side of a rabbit femur: f. Injection point.
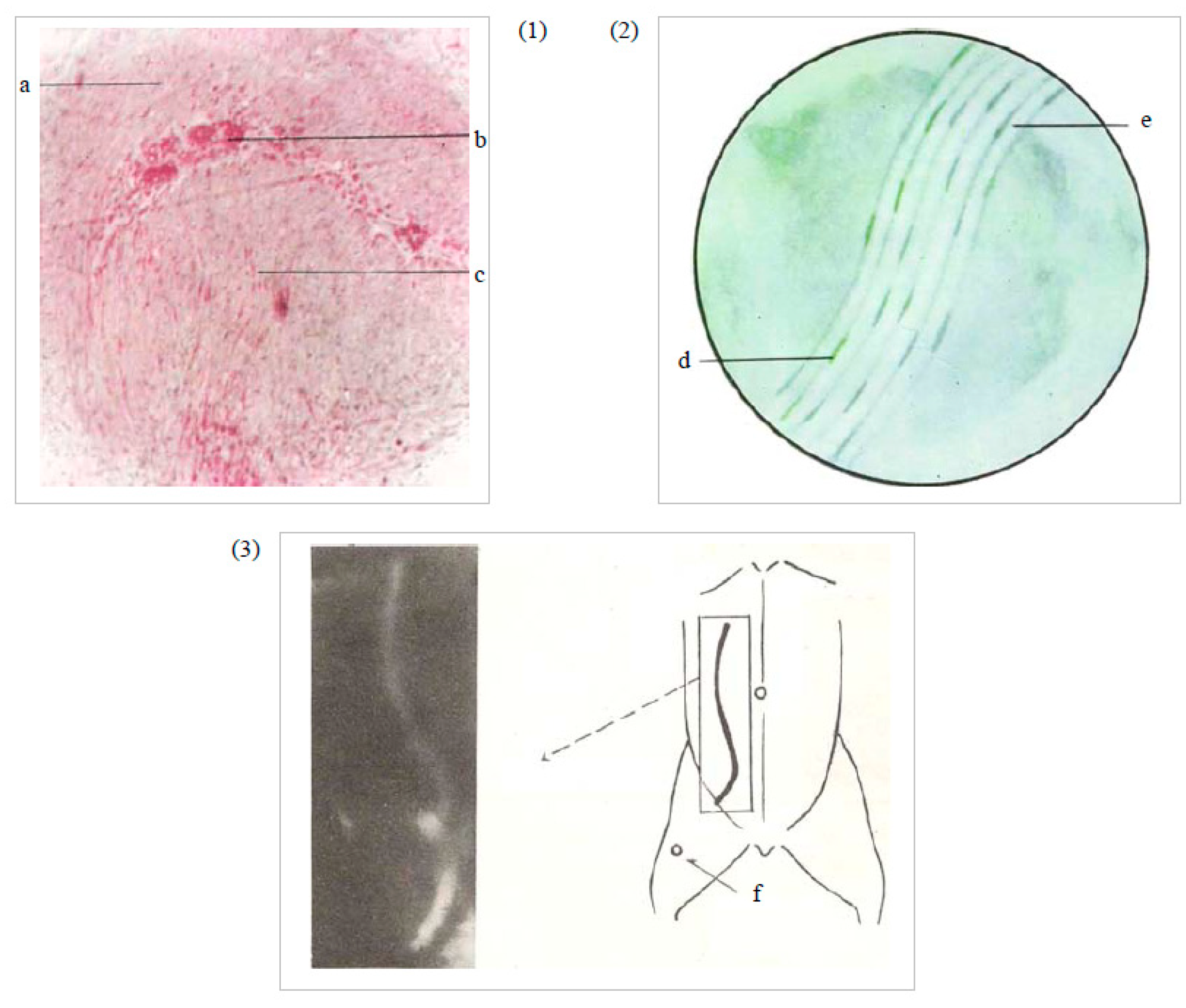
Figure 6.
A modified picture presented in the article of P. de Vernejoul, et al. [267]. (a) Circular diffusion of isotopes administered in a control area of the skin, (b) and a linear migration of isotope administered in the acupuncture point K-7.
Figure 6.
A modified picture presented in the article of P. de Vernejoul, et al. [267]. (a) Circular diffusion of isotopes administered in a control area of the skin, (b) and a linear migration of isotope administered in the acupuncture point K-7.
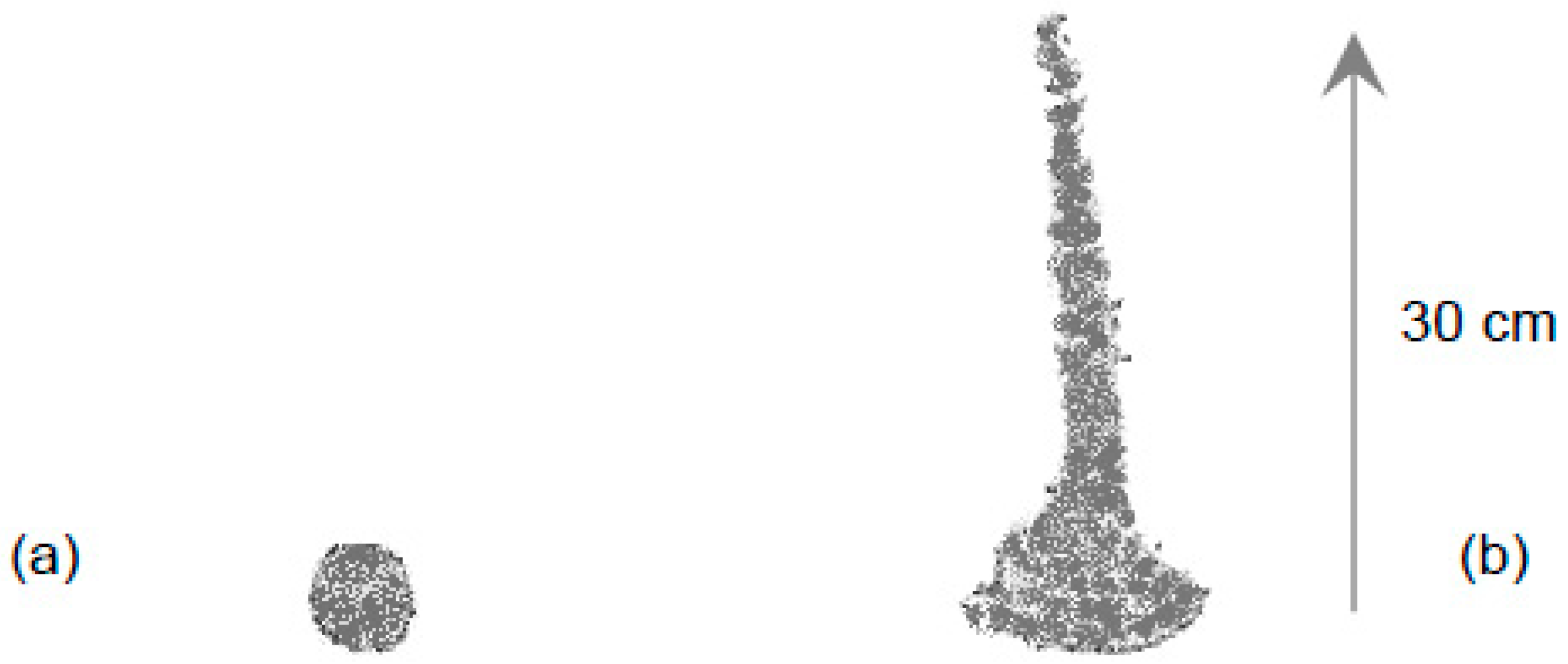
Figure 7.
Theory of channels and collaterals describes physiology and pathology of intracellular space
Figure 7.
Theory of channels and collaterals describes physiology and pathology of intracellular space
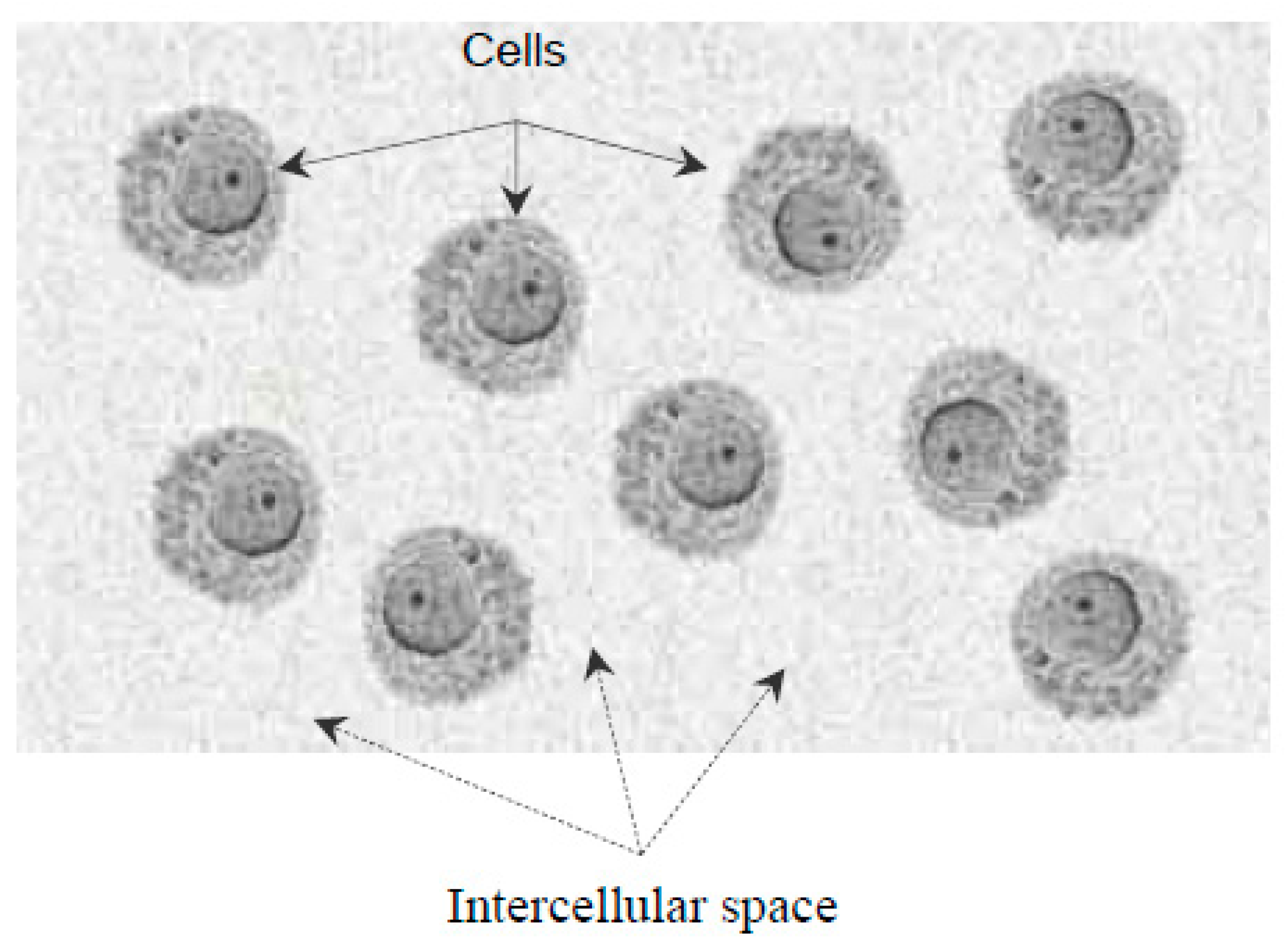
Figure 8.
Cell and organelles: Golgi complex corresponds to the Liver, Mitochondria – to the Lungs, the Nucleus – to the Kidneys, Endo-plasmatic reticulum – to the Spleen-Pancreas, Centrioles could correspond to the Heart.
Figure 8.
Cell and organelles: Golgi complex corresponds to the Liver, Mitochondria – to the Lungs, the Nucleus – to the Kidneys, Endo-plasmatic reticulum – to the Spleen-Pancreas, Centrioles could correspond to the Heart.
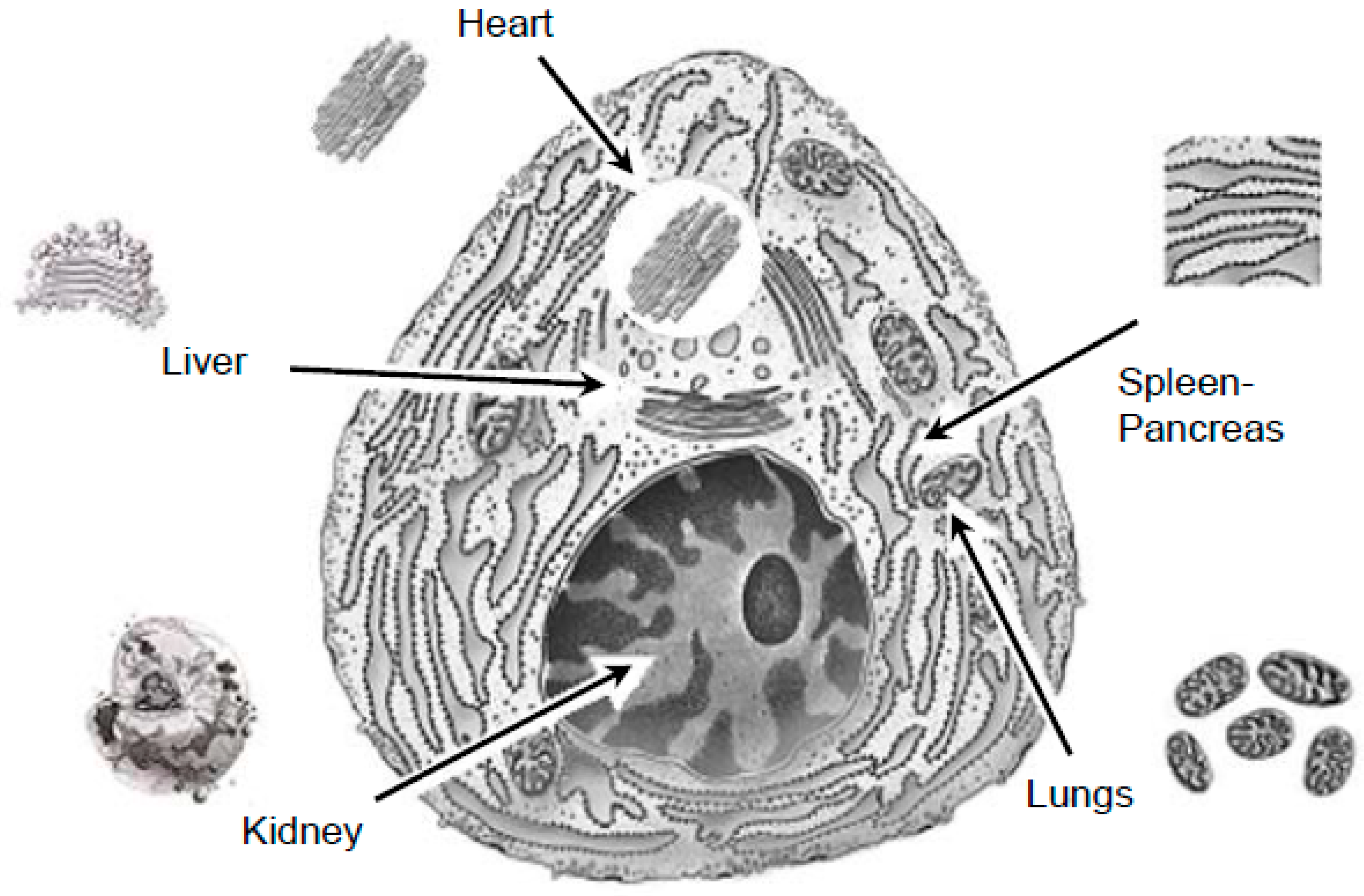
Figure 9.
A system of “Lungs” provides the function of the external breath, transportation of oxygen and carbon dioxide and finally tissue respiration with subsequent synthesis of ATP molecules.
Figure 9.
A system of “Lungs” provides the function of the external breath, transportation of oxygen and carbon dioxide and finally tissue respiration with subsequent synthesis of ATP molecules.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



