
Submitted:
27 October 2023
Posted:
30 October 2023
You are already at the latest version
Abstract
Abstract
Objectives
To investigate histopathological changes and serous carcinoma precursors such as secretory cell outgrowths (SCOUTs) and p53 signature in bilateral tubal ligation (BTL) materials performed during cesarean section (S/C).
Materials and Methods
138 patients who underwent S/C and tubal sterilization (TS) between October 2020 and May 2021 at Konya City Hospital. Patients’ data were obtained from the haospital’s system. All data andd findings were investigated and statistically evaluated.
Results
The mean age was 34.62 years (22 - 44), the mean gravity was 4.89 (2-15) and the mean parity was 3.46 (1-10). 5.79% SCOUT, 7.24% atypia and 9.42% p53 signatures were observed. Significant correlations were shown between epithelial cell lineage and age and between KI-67, SCOUT, and gravity, between KI-67 results and gravity and parity, and between P53 score and age.
Conclusion
TS is a common, safe, and effective method worldwide. Today, BTL is increasing along with increasing S/C ratios. In addition to the reduced risk of ovarian cancers with ligation alone, precursor lesions such as hyperplasia, SCOUT, p53 signature, and STIL/ Serous tubal intraepithelial carcinoma (STIC) are encountered in the ampulla materials obtained. Considering the low rates of re-anastomosis, tubal excision may be recommended instead of ligation in women of relatively higher gravity and age.
Keywords:
ttubal ligation
; epithelial hyperplasia
; SCOUT
; p53 signature
1. Introduction
The uterine tubes are located bilaterally in the upper part of the uterine cavity and are on average 11-12 cm in length. Also known as the oviduct or Fallopian tube, it consists of the infundibulum (fimbria), ampulla, isthmus, and intramural segments. They are embryologically derived from the coelomic epithelium via the paramesonephric ducts. In its normal histology, there are three types of epithelial cells: ciliated, secretory, and intercalate (peg). The appearance of these cells may change due to cyclic hormonal changes and the use of oral contraceptives (1).
TS is a highly effective, widely used, safe, and permanent birth control method. It is usually preferred by women who do not have fertility aspirations or who have completed them. This method is applied around 700,000 times a year in the USA (2). The number and rate of preference are increasing, with more than 190 million TSs administered globally in 2017 and more than 220 million in 2022 (2, 3). While the preference rate of this method is 23.7% in the world, it reaches 4.3% in the USA (1,4)
Routine pathologic examinations of TS materials reveal different, normal histopathologic margins and preneoplastic/neoplastic changes. Hyperplasia that develops in normal mucosal cells is in the form of stratification and formation of small tufts and may show varying degrees of cytologic atypia( 5-6). Hyperplasia may be associated with conditions such as inflammation, excess estrogen, ectopic pregnancy, and neoplasia. It can be present in up to 83% of BTL and salpingectomies performed in benign and malignant conditions (5). Most cases show only mild atypia and in such settings, the presence of small papillary clusters and nuclear stratification should not be misinterpreted as a premalignant change. Mitotic figures are usually absent or few as in number. Cells preserve cilia and nuclear-cytoplasmic ratio (5).
The presence of at least 30 or more secretory cells is referred to as "SCOUT". ''p53 signatures'' are abnormal p53 immunostaining in at least 12 consecutive secretory nuclei that appear normal). STIL (serous tubal intraepithelial lesion) has been identified in the fallopian tube. STILs are lesions that fail to be classified as an STIC due to limited proliferation (p53 positive-KI-67 < 10% or p53 negative KI-67 > 10%). (7, 39) STICs are associated with nuclear enlargement, loss of polarity, increased nuclear atypia, abnormal p53 expression, and increased proliferative activity (KI-67) (8, 9).
Epithelial ovarian carcinoma is the second most common gynecologic malignancy in the United States and the most common cause of death in this group of tumors (10).
High-grade ovarian serous carcinoma (OSC) is responsible for approximately 70% of ovarian cancers. Most of them are bilateral. Low-grade OSC is uncommon (<5% of all ovarian cancers) (9, 11). High and low-grade OSCs are said to have different carcinogenesis origins (12). In many studies, it was reported that the risk of development of ovarian cancer decreased by 42-77% with salpingectomy (13).
2. Materials and methods
In our study, 138 patients who underwent BTL during S/C between October 2020 and May 2021 at Konya City Hospital were evaluated. For each patient, tubal ligation tissues were cut to 4-5 microns and prepared for hematoxylin-eosin and immunohistochemistry studies. An automated device (Leica Biosystems Melbourne Pty Ltd., Bond-max, M212536, 2014, Melbourne, Australia) was utilized for immunohistochemistry. Anti KI-67 antibody for immunohistochemistry (Mouse monoclonal, Biogenex, The Hague, The Netherlands), anti p53 (Mouse monoclonal, Zeta, Sierra Madre, CA, USA), and the Bond Polymer Refine Detection Kit (LeicaBiosystems, Newcastle Upon Tyne, UK) was used. The exhaustive protocol was attained from the anti-Ki-67 and anti-p53 product datasheets and in by the protocol. Diaminobenzidine (DAB) and hematoxylin counterstaining were performed for visualization. The stained preparations were then sealed with a coverslip using entellan)
Ethics committee approval of the study was obtained from Karatay University Faculty of Medicine, Pharmaceuticals and Medical Devices External Board on 24.01.2023 with the decision number 2023/036.
The number of cell layers observed most frequently and second frequently in the long-axis regions of the tubal epithelium were grouped separately as ≤ 2 and ≥3. Inflammation, intra-epithelial lymphocyte, papillary hyperplasia, tufting, atypia, SCOUT, p53 signature, and STIL conditions were evaluated as present/absent (8).
The number of cells presenting immunohistochemical staining with KI-67 was evaluated by modifying the methods described in the literature. Scores have been evaluated as, according to the number of cells with positive KI-67 staining; <10% = score 1, 10-25% = score 2, >25% = score 3, cells staining with p53; 0 =f score 0, <10% = score 1, 10-25% = score 2, 25%-50% = score 3, >50% = score 4 (14).
Descriptive statistics mean, standard deviation for quantitative variables and, frequency and percentage for categorical variables were given. For the analysis of categorical variables,Chi-square and Fisher tests were utilized, for the analysis of numerical variables T-test and analysis of variance were utilized. Analyses were performed with the R 4.2.2 program. p<0.05 was considered significant.
3. Results
138 women who underwent BTL during S/C have been included in the study. The mean age was 34.62 (22 - 44), the mean gravity was 4.89 (2-15) and the mean parity was 3.46 (1-10). In the extended period, which includes the study period, (between August 15, 2020, and December 31, 2021), there were 4568 S/C, 643 BTL, and 2 re-anastomoses in our institution.
Histologic findings related to epithelial cell sequence, inflammation, and other epithelial changes are shown in the tables (Table 1, Table 2, Figure 1).
Immunohistochemically obtained KI-67 and p53 scoring results, SCOUT, p53 signature, and STIL results are given in the tables (Table 3, Table 4). In the evaluations made in terms of epithelial hyperplasia, there were significant correlations between cell sequence and age (more in the higher aged, p=0.044) and cell sequence and Ki-67 score (p=0.044), while no correlation was found between cell line and gravity, parity p53 score, p53 signature and SCOUT (p>0.05).
There was a significant (p=0.011) association between SCOUT findings and low gravity, whereas no association was found between age and parity (p>0.05). Atypia was more common in those with higher cell sequences (p=0.002). No correlation was found between p53, p53 signature, and SCOUT (p>0.05) (Figure 2). P53 score increases with increased age (p=0.036). There was no correlation between gravity and parity and scores and p53 scoring (p>0.005).
Higher scoring with KI-67 in those with fewer gravities and parities, p=0.016 and p=0.049, respectively. There was no correlation with age (p>0.05) (Figure 3). No correlation was found between Tufting, SCOUT, p53 signature, atypia, intraepithelial lymphocyte and infiltration findings, and age, gravity, and parity (p>0.05) (Figure 3). Additional pathologic findings were paratubal cyst in 10 cases (7.24%), decidua in 4 cases (2.89%), Walthard nest in 5 cases (3.62%), paratubal cyst with Walthard nest in 2 cases (1.44%) and endometriosis and calcification in one case (0.72%) (Figure 4)
4. Discussion
In our study, we included 138 patients with BTL during S/C. Tubal excision is usually performed secondary to surgery, but it is also performed for primary sterilization. In a 7-year retrospective study published in 2001, TS was performed as an additional operation in 358 of 630 cases (56.82%) (15). Tubal ligation is a frequently used method, especially during cesarean section. Regarding the cesarean section delivery rate, Turkey ranks first with 54.9%, followed by Korea (45%) and Poland (38.9%) (16). In a 20-year study, tubal ligation during S/C increased from 5% to 24.7% (17). In a study conducted in the United States, it was reported that bilateral salpingectomy was performed in 397,260 (10.4%) and BTL in 203,400 (5.3%) of 3,813,823 female patients who delivered by cesarean section in approximately three years (18). While its efficacy and safety were recognized in most studies, side effects were reported at very low rates. In follow-up observations after cesarean section and tubal excisions performed in the postpartum period involving 435 cases, 26.2% of whom underwent tubal ligation, pregnancy developed at a rate of 0.7% (19).Pregnancy is most commonly ectopic. In a study conducted in 2000, it was revealed that 700 thousand TS were performed annually in the USA, ectopic pregnancy occurred most often in unsuccessful applications, and in addition, the risk of developing ovarian cancer decreased (7).
Moreover, tube ligation is suitable for patients who want to perform re-anastomosis for various reasons. In a study conducted with 80 patients, pregnancy occurred in 28 (47.4%) of the cases (2). Pregnancy occurred in 8 (28.6%) of 28 patients who underwent re-anastomosis in 2021 (20).
Pathologic examination of tubal tissues was limited in the early years and was mostly focused on whether the correct/adequate material was obtained. Over time, histologic changes especially the tubal lining of the ovaries are examined in detail for preneoplastic changes due to their association with ovarian cancers. In 2010, 548 (79%) tubal ligation materials were sent to pathology in a clinic and 3 of them were found to contain insufficient tissue (19).
Tubal ligation is increasing gradually in our country and reached a rate of 10% in 2018 (21). The rate of tube ligation during C/S is 14.07% in the institution we work in. The rate of re-anastomosis is quite low at 0.31%.
Comparative studies were conducted between bilateral total or partial / ligation of the tubes under different parameters. Even though the follow-up period was as brief as one year, there was no difference in both hormonal values (AMH, FSH, AFC, VI, FI, VFI ) and OvAge and ovarian volumes of patients who underwent 50 bilateral total salpingectomies and 52 BTL (22).
With the pathology data available, it has been demonstrated that up to 70% of ovarian cancers originate from the fallopian tubes. A study conducted in Sweden between 1973 and 2009 demonstrated that 251,465 women who underwent bilateral salpingoophorectomy for benign reasons during gynecological surgery had a lower risk of ovarian cancer than those who underwent BTL. (23) In the study, which lasted for about 14 years and had a considerably high number of cases (1,132,914 patients), TS was performed in 264,048 patients. As a result of this study, despite a 20% lower risk of developing high-grade OSC, there was no reduction in the risk of low-grade OSC (24).
Histopathological and preneoplastic transformations in the tubes were usually made in neoplastic patients compared to the control group and in operative materials covering the fimbrial end. There is a limited number of studies of tubal ampulla materials obtained as a result of TS, a widespread contraceptive method in the world, for the above purposes alone.
Within the framework of normal histology, mast cells, neutrophil polymorphs, plasmocytes, and lymphocytic inflammatory cells can be observed in the tuba (25). In a study with a large case series, Hunt et al. detected mast cells commonly in the material of 287 cases, however, the rate of lymphocytic inflammation was low. They reported the rate of lymphoid follicles as 2.1% (26). In our study, the rate of inflammatory cells was 33.34%, while the rate of intraepithelial lymphocytes was 14.492%. In the examination of the tubas of 201 patients, 60% of which had TAH+BSO, salpingitis was observed in 10.19%, hydrosalpinx in 7.86%, and pyosalpinx in 0.29% (27). In a study conducted in contrast, salpingitis was observed as low as 1.9% in 72 follow-up patients with hysterectomy (9). The salpingitis rate was found to be 7.24% in our study as opposed to two studies with such different rates.
Tubal epithelial hyperplasia in nonneoplastic and neoplastic cases has long been of interest. In 1989, Susan et al. found 68.7% epithelial hyperplasia in 99 cases with serous borderline (27). While the rate of epithelial hyperplasia was 3% in a study of 200 non-neoplastic cases (4), the rate of cases with epithelial cell line >3 was 1.4% in another overlap. (9). In our study, the rate of cases with epithelial cell sequence ≥3 was 13.05% and papillary hyperplasia was 5.07%.
Again, in the study conducted by Hunt et al., atypia was detected as 7.3% (26).
In a study by Fatemeh Sari Aslani, with 34 patients with ovarian neoplastic and 72 control patients, the rate of atypia in the control group was 0%. Significant differences were shown between the cases and the control group in terms of tubal, especially >3 cell layer thickness, atypia, mitosis, cribriform, and tufting (P < 0.05) (9). The rate of atypia in our study was (7.24%). Atypia was more common in patients with higher cell sequences (p=0.002). There was no correlation between p53 scoring values, p53 signature, and SCOUT (p>0.05).
In a study on KI-67 scoring by Khun et al. with 41 cases with STIC, 35 with HGSC, and 42 cases as the control group, KI-67 rates were significant between STIC and the control group, while no significant relationship was found between STIC and HGSC. There was no difference in KI-67 labeling rates for various regions of the tuba (28). Significant correlations between epithelial cell lineage and KI-67 and between KI-67 results and gravity and parity have been found in our study.
Studies on preneoplastic changes such as SCOUT, p53 signature, and STIL or preinvasive changes such as STIC have yielded different results in the ampulla and fimbria regions. In the study, the fimbriae are closer to the ovary than the ampulla and are more exposed to follicular fluid. Fimbriae were also shown to produce more CYYR1, SALL1, FOXP2, TAAR1, AKR1C2/C3/C4, NMBR, ME1, and GSTA2 genes that are effective in antioxidant and inflammation pathways compared to ampulla. (29). In a study conducted with 25 cases as the control group, 24 with OSC, and 75 with BRCA (+), the SCOUT rates were 12%, 83%, and 18%, respectively. SCOUT was more frequently observed at the fimbrial end than proximally. In parallel, the ratio of occurrence of SCOUT in the fimbriae and ampullae is 5:1 in cases with a higher p53 staining rate and 1.3:1 in cases with a lower p53 staining rate. (30). In a study of 34 cases of ovarian serous tumors and 72 as the control group, a significant difference in favor of tumor cases was observed in both bilateral fimbriae (P = 0.012) and (P = 0.004) and bilateral ampullae (P = 0.012) and (P = 0.000) (9). In our study, the SCOUT rate was found to be (5.79%).
Precursors of HGSC containing the p53 signature and STIC occur most frequently in the fimbriae of the tuba. As mentioned above, this region is directly exposed to ovulation, WNT, and Notch signaling. Therefore, the fimbria is considered a high and the ampulla a low-risk epithelial region prone to transformation (29). In a study, p53 mutation was detected by PCR and immunohistochemistry in 10 normal patients, 14 patients with carcinoma, and 1 patient with borderline, but only in 57% of patients with cancer. PCR was used to confirm 7 of these (31). The rate of patients with significant p53 score was (3.62%) in our study. The score increases with an increase in age (p0.036). We noted no correlation between gravity and parity counts and p53 scoring in our study (p>0.005). In a prospective study of 67 gynecologic and 46 obstetric patients, Tsutomu Ida et al. showed a lower incidence of p53 signatures in women who had given birth, were young, premenopausal, and had a history of pregnancy. p53 signatures were 21 (88%) in fimbriae and 3 (12%) in ampullae (11). In a study of 32 cases with OSC and 31 as the control group, p53 signatures, and STIC were most frequently seen in serous carcinomas. p53 signatures and STIC were always seen at the fimbrial end (32). In our study, the p53 signature rate was 9.42% and no correlation was found between age, gravity, and parity (p>0.05). In 495 cases, 110 of which were malignant SEE-FIM, STIC was diagnosed in 13 cases, including 12 in fimbrias. STIC was not observed in benign gynecologic cases(8). STIC was diagnosed in 2.4% of 85 elective hysterectomy patients over 40 years of age in Mexico after examination of their tubes (33). In salpingectomy materials of 400 patients carrying BRCA1/2 mutation, 1.5% for invasive serous carcinomas, 3.5% for STICs, and 1.3% for STILs were identified (36).
In Khun's study, 11 (26.8%) of the STIC findings were composed of flat and highly atypical single-layered epithelium, 10 (24.4%) were composed of multi-layered epithelium, and 20 (48.8%) were tufted (29). STIC was not encountered in our study, whereas STIL was found in only 1 case (0.72%).
Meta-analyses of observational epidemiologic studies have repeatedly emphasized that tubal ligation is associated with an overall reduced risk of ovarian cancer (12). Even if it is only the ligation of the ampulla, it is the right approach to consider this advantage.
Bhattacharya et al. examined the tuba of 201 patients with 60% TAHB4SO and found that while only one case was neoplastic, paratubal cyst, ectopic tubal gestation, and Walthard Cell Nests were the most common (27). In a series of 287 cases, Hunt et al. reported stromal and structural changes as fibrosis in 35.5%, intramuscular edema in 12.5%, inclusion cysts in 7.7%, Walthard cell nests in 5.2%, tibial pigments 5.1%, Wolffian duct remnant 4.5%, decidualized stroma 3%, Decidualized stroma, Endosalpingiosis 2.4%, metastatic carcinoma infiltration 1.4% (26).
In the study of Fatemeh Sari Aslani, 2.8% endometriosis, 1.9% salpingitis, 0.9% hemangioma, and 0.9% calcification were found in 106 tubas in the control and study groups (9). In various studies, endometriosis rates have been reported between (1.4% to 43.3%) (35). In our study, aside from inflammation and epithelial changes, additional findings such as decidua, Walthard's nest, and calcification were detected in the same types and at similar rates on average. Further cross-sectioning and, if necessary, sampling of all material when examining tubal sterilization materials will make it easier to demonstrate the changes mentioned above.
5. Conclusion
TS with the possibility of re-anastomosis is a widely used, safe, and effective method. Tubal ligation is also increasing with the increasing S/C rates in the world. Numerous comparative studies (malignant versus benign groups) have been conducted, especially based on the relationship between HGSC development and the tuba. In these studies, fimbria and ampulla findings of the tuba were also evaluated. In addition to the reduced risk of ovarian cancers with ligation alone, a wide range of pathologic findings such as hyperplasia, SCOUT, p53 signature, and STIL/STIC are encountered in the ampulla materials collected. In our study, significant correlations were shown between age and epithelial cell lineage and p53, between KI-67 and epithelial cell lineage, gravity and parity, and between SOUT and gravity. Considering the low rates of re-anastomosis, tubal excision may be recommended instead of ligation in women of relatively higher gravity and age. With the evaluation of the above-mentioned findings, valuable data can be obtained both in the control and follow-up of patients and in prospective scientific studies.
References
- Sung, S. , & Abramovitz, A. (2019). Tubal ligation.
- Şentürk, M.B.; Budak, M.Ş.; Toğrul, C.; Tahaoğlu, A.E.; Balsak, D.; Akgöl, S. The Pregnancy Rates After Tubal Reanastomosis. Okmeydanı Tıp Dergisi 2016, 32(2), 79-82. [CrossRef]
- ÖZKAN, Hava, U. Z. U. N. Betül, and A. R. I. Özlem. A Current Overview of Cesarean Birth: The Modern Cesarean Theory. Arşiv Kaynak Tarama Dergisi 2021, 30, 226–235.
- Uaamnuichai, S.; Phutrakool, P.; Thammasitchai, N.; Sathitloetsakun, S.; Santibenchakul, S.; Jaisamrarn, U. Does socioeconomic factors and healthcare coverage affect postpartum sterilization uptake in an urban, tertiary hospital? Reproductive Health 2023, 20(1), 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yanai-Inbar, I.; Silverberg, S.G. Mucosal epithelial proliferation of the fallopian tube: prevalence, clinical associations, and optimal strategy for histopathologic assessment. International journal of gynecological pathology 2000, 19(2), 139–144. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Vang, R.; Junge, J.; Hannibal, C.G.; Kjaer, S.K.; Shih, I.M. Papillary tubal hyperplasia. The putative precursor of ovarian atypical proliferative (borderline) serous tumors, noninvasive implants and endosalpingiosis. The American journal of surgical pathology 2011, 35, 1605. [Google Scholar] [CrossRef] [PubMed]
- Lehn, Kristiana, et al. "Successful completion of total and partial salpingectomy at the time of cesarean delivery." Contraception 98.3 (2018): 232-236. [CrossRef]
- Koç, Nermin, Selçuk Ayas, and Lütfiye Uygur. "The association of serous tubal intraepithelial carcinoma with gynecologic pathologies and its role in pelvic serous cancer." Gynecologic oncology 134.3 (2014): 486-491. [CrossRef]
- Aslani, Fatemeh Sari, Mona Maleknasab, and Mojgan Akbarzadeh-Jahromi. "Fallopian tube epithelial changes in ovarian serous tumors compared with the control group: A single-center study." Nigerian Medical Journal: Journal of the Nigeria Medical Association 60.2 (2019): 47. [CrossRef]
- Luke, Shauntell, et al. "Benefits and Risks of Bilateral Salpingectomy Compared With Standard Tubal Ligation During Cesarean Delivery for Permanent Postpartum Contraception." Obstetrical & Gynecological Survey 77.3 (2022): 167-173. [CrossRef]
- Ida, Tsutomu, et al. "Relationship between the precursors of high grade serous ovarian cancer and patient characteristics: decreased incidence of the p53 signature in pregnant women." Journal of Gynecologic Oncology 30.6 (2019). [CrossRef]
- Gaitskell, Kezia, et al. "Tubal ligation and ovarian cancer risk in a large cohort: Substantial variation by histological type." International Journal of Cancer 138.5 (2016): 1076-1084. [CrossRef]
- Kim, Miseon, et al. "Bilateral salpingectomy to reduce the risk of ovarian/fallopian/peritoneal cancer in women at average risk: a position statement of the Korean Society of Obstetrics and Gynecology (KSOG)." Obstetrics & gynecology science 61.5 (2018): 542-552. [CrossRef]
- Sungu, Nuran, et al. "Evaluation of p53 and Ki67 expression profiles in basal cell carcinomas in a usual and an unusual location." Turk Patoloji Dergisi 34.2 (2018). [CrossRef]
- Gül, A.; Şimşek, Y.; Şahin, G. The Review of the Cases of Tubal Sterilization Which Were Performed in the Department of Obstetrics and Gynecology. Van Tıp Dergisi 2000, 7, 57–59. [Google Scholar]
- Christopher, G. L. (2021). Lalana Newborn Resuscitation. Jour Clin Med Res, 2(3), 1-55. [CrossRef]
- Moreno, J. M., Bartual, E., Carmona, M., Araico, F., Miranda, J. A., & Herruzo, A. J. (2001). Changes in the rate of tubal ligation done after cesarean section. European Journal of Obstetrics & Gynecology and Reproductive Biology, 97(2), 147-151. [CrossRef]
- Mandelbaum, R. S., Matsuzaki, S., Sangara, R. N., Klar, M., Matsushima, K., Roman, L. D., ... & Matsuo, K. (2021). Paradigm shift from tubal ligation to opportunistic salpingectomy at cesarean delivery in the United States. American Journal of Obstetrics and Gynecology, 225(4), 399-e1. [CrossRef]
- Werawatakul, Y.; Prasit, M.; Leelapongwattana, K.; Kleebkaow, P. Evaluation of female sterilization and tubal tissue confirmation at Srinagarind Hospital. Journal of the Medical Association of Thailand 2012, 95, 1252. [Google Scholar] [PubMed]
- Yener, A.; Giray, B. Pregnancy Outcomes After Tubal Reanastomosis: A Novel Technique. Dicle Tıp Dergisi 2021, 48, 839–843. [Google Scholar] [CrossRef]
- Akalın, A.; Bostancı, Ş. Sexual functions and sexual quality of life in the reproductive age women using method of family planningi. Androloji Bülteni (Andrology Bullettin) 2022, 24, 110–117. [Google Scholar]
- Elnory, M. A., & Elmantwe, A. (2019). Impact of bilateral total salpingectomy versus standard tubal ligation at time of cesarean section on ovarian reserve: A randomized controlled trial. Evidence Based Women's Health Journal, 9(2), 458-467. [CrossRef]
- Piek, J. M. (2004). Hereditary serous ovarian carcinogenesis, a hypothesis. Doctoral Theses—Medicine. Amsterdam: Vrije Universiteit.
- Powell, C. B., Alabaster, A., Simmons, S., Garcia, C., Martin, M., McBride-Allen, S., & Littell, R. D. (2017). Salpingectomy for sterilization: change in practice in a large integrated health care system, 2011–2016. Obstetrics & Gynecology, 130(5), 961-967. [CrossRef]
- Rigby, C. H., Aljassim, F., Powell, S. G., Wyatt, J. N., Hill, C. J., & Hapangama, D. K. (2022). The immune cell profile of human fallopian tubes in health and benign pathology: a systematic review. Journal of Reproductive Immunology, 152, 103646. [CrossRef]
- Hunt, J. L., & Lynn, A. A. (2002). Histologic features of surgically removed fallopian tubes. Archives of pathology & laboratory medicine, 126(8), 951-955. [CrossRef]
- Bhattacharya, N., Perween, S., & Gupta, K. Histopathological study of surgically resected specimens of fallopian tube. [CrossRef]
- Kuhn, E., Kurman, R. J., Sehdev, A. S., & Shih, I. M. (2012). Ki-67 labeling index as an adjunct in the diagnosis of serous tubal intraepithelial carcinoma. International journal of gynecological pathology: official journal of the International Society of Gynecological Pathologists 31(5), 416. [CrossRef]
- Sowamber, R. , Nelson, O., Dodds, L., DeCastro, V., Paudel, I., Milea, A.,... & George, S. H. (2020). Integrative transcriptome analyses of the human fallopian tube: Fimbria and ampulla—site of origin of serous carcinoma of the ovary. Cancers, 12(5), 1090. [CrossRef]
- Chen, E. Y., Mehra, K., Mehrad, M., Ning, G., Miron, A., Mutter, G. L., ... & Crum, C. P. (2010). Secretory cell outgrowth, PAX2 and serous carcinogenesis in the Fallopian tube. The Journal of pathology, 222(1), 110-116. [CrossRef]
- Zheng, W., Sung, C. J., Cao, P., Zhang, Z. F., Cai, R., Godwin, T. A., ... & Lauchlan, S. C. (1997). Early occurrence and prognostic significance of p53 alteration in primary carcinoma of the fallopian tube. Gynecologic oncology, 64(1), 38-48. [CrossRef]
- Mittal, N., Srinivasan, R., Gupta, N., Rajwanshi, A., Nijhawan, R., Gautam, U., ... & Dhaliwal, L. (2016). Secretory cell outgrowths, p53 signatures, and serous tubal intraepithelial carcinoma in the fallopian tubes of patients with sporadic pelvic serous carcinoma. Indian Journal of Pathology and Microbiology, 59(4), 481. [CrossRef]
- Briseño Campos, A. G., Cruz Rodríguez, A., García Perales, M. O., Serna Vela, F. J., Camarillo Elizalde, D. G., & Robles Martínez, M. D. C. (2019). Incidence of intraepithelial fallopian tube neoplasias in mexican women over 40 years of age that underwent elective hysterectomy. Journal of Ovarian Research, 12(1), 1-6. [CrossRef]
- Visvanathan, K. , Shaw, P., May, B. J., Bahadirli-Talbott, A., Kaushiva, A., Risch, H., & Shih, I. M. (2018). Fallopian tube lesions in women at high risk for ovarian cancer: a multicenter study. Cancer prevention research, 11(11), 697-706. [CrossRef]
- Tissot, M. , Lecointre, L., Faller, E., Afors, K., Akladios, C., & Audebert, A. (2017). Clinical presentation of endometriosis identified at interval laparoscopic tubal sterilization: Prospective series of 465 cases. Journal of gynecology obstetrics and human reproduction, 46(8), 647-650. [CrossRef]
Figure 1.
Intra-epithelial lymphocytes (arrows) (A), Epithelial hyperplasia (arrows) (B).
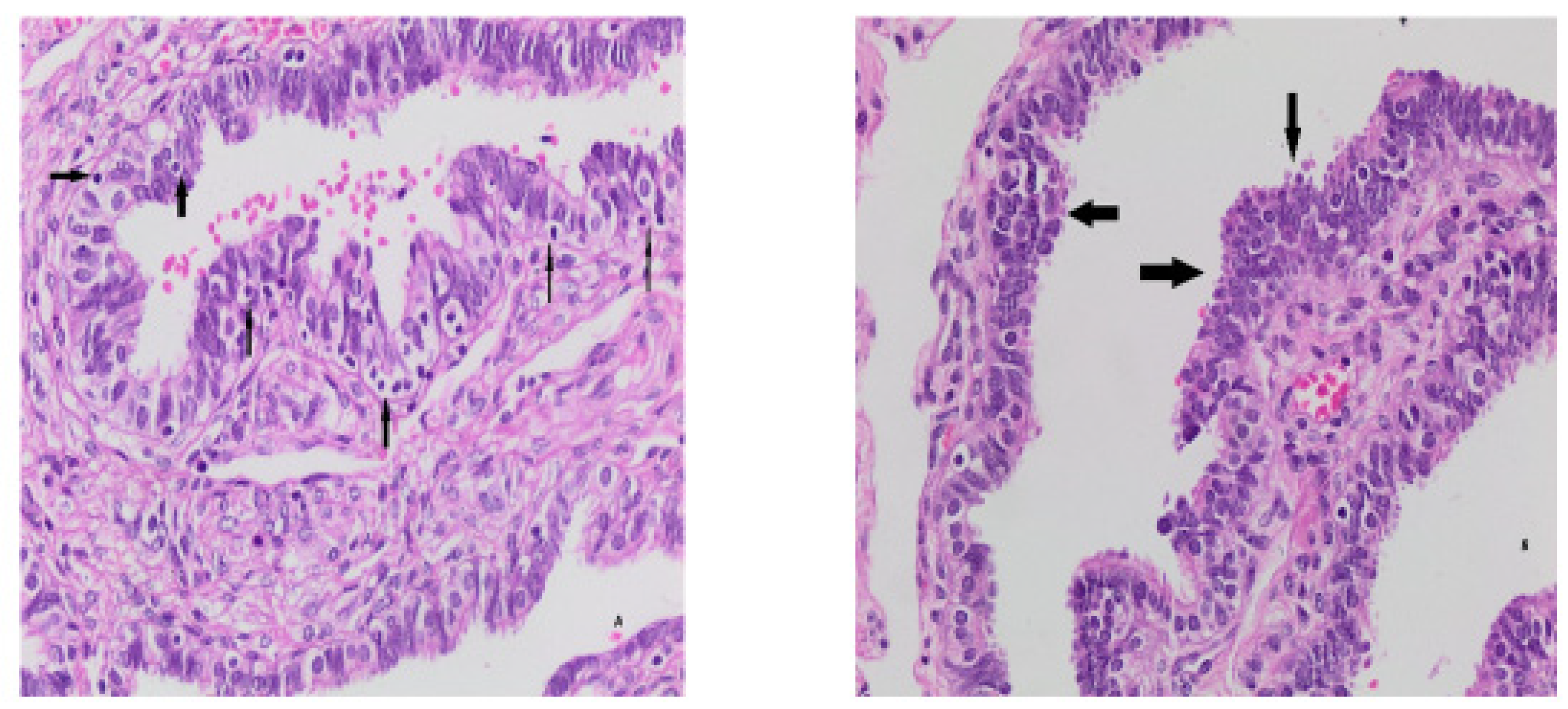
Figure 2.
Atypical changes (arrows) (A), very low p53 (B) and KI-67 (C) values.
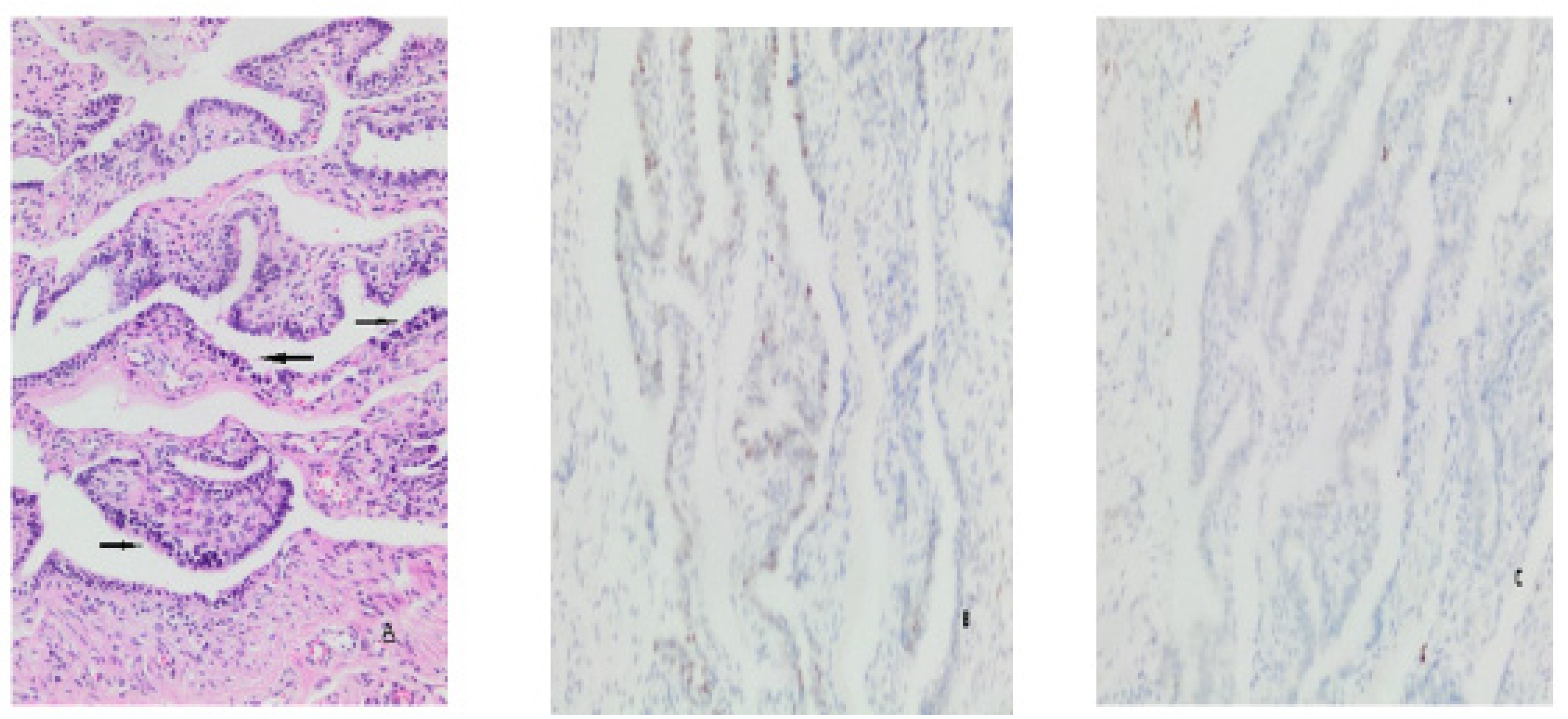
Figure 3.
Secretory cell outgrowths (SCOUTs) (arrows) (A), p53 signature (arrows) (B), Low KI-67 index Score 1 (C).
Figure 3.
Secretory cell outgrowths (SCOUTs) (arrows) (A), p53 signature (arrows) (B), Low KI-67 index Score 1 (C).
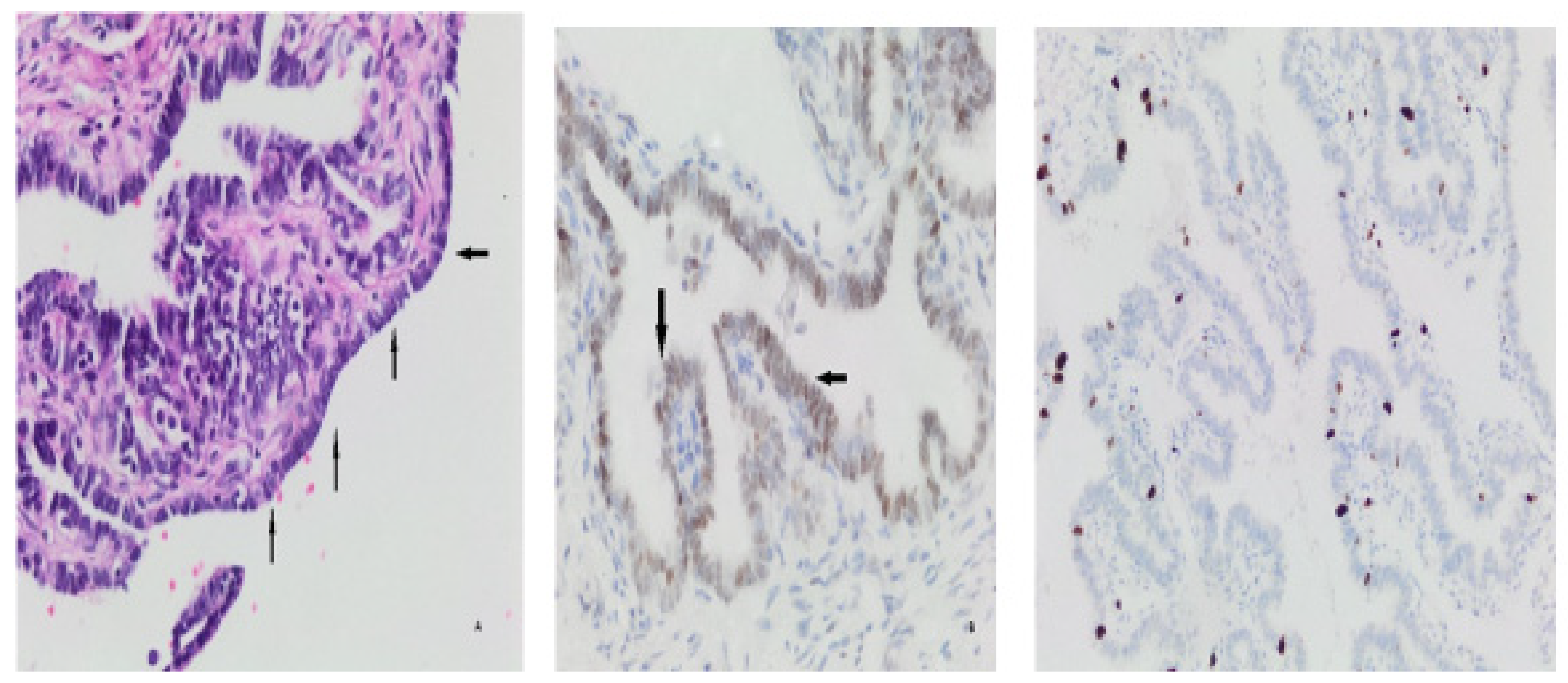
Figure 4.
Extra findings. Decidua (arrows) in tubal tissue (A), Walthard remnants (arrows) (B), paratubal cyst (arrows) (C).
Figure 4.
Extra findings. Decidua (arrows) in tubal tissue (A), Walthard remnants (arrows) (B), paratubal cyst (arrows) (C).
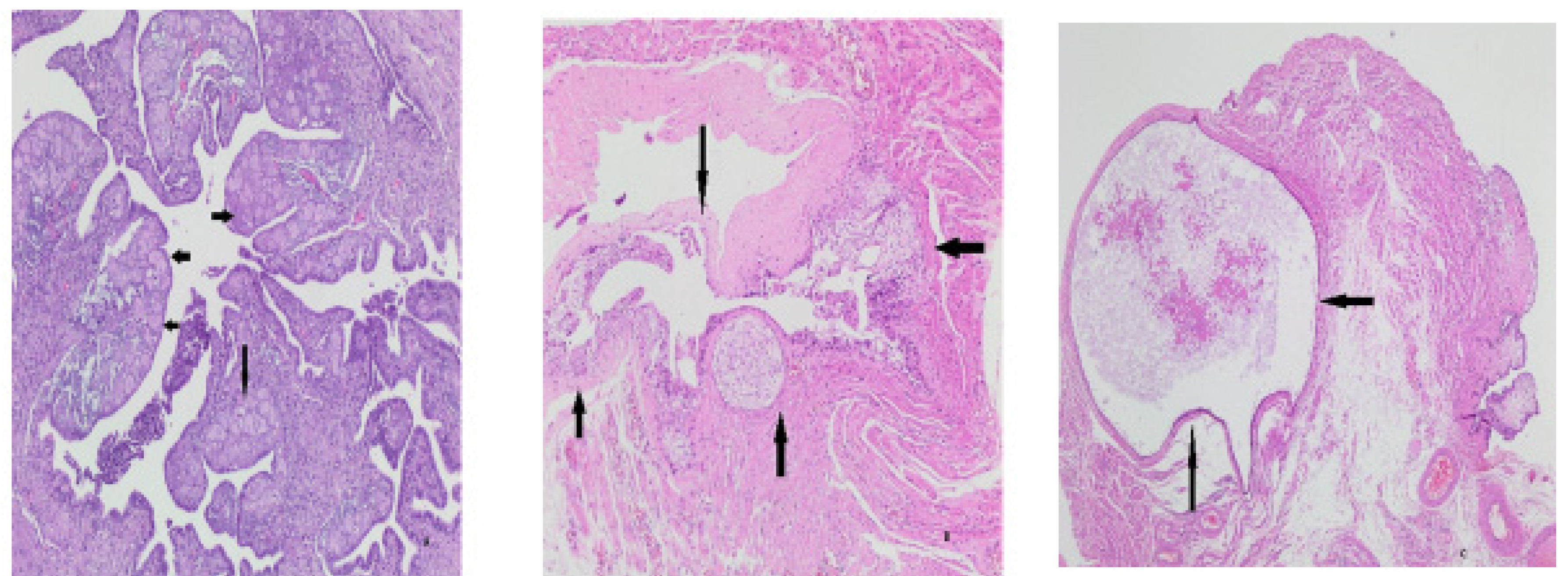

Table 1.
Results related to epithelial cell sequence numbers.
| ≤ 2 | ≥3 | |
|---|---|---|
| Maximum cell layer sequence | 120 (86.95 %) | 18 (13.05 %) |
| Cell layer sequence at the second frequency | 98 (71.01 %) | 40 (28.99%) |
Table 2.
Findings related to inflammation and histologic parameters.
| Present | Absent | |
|---|---|---|
| Inflammatory cells | 46 (33.34%) | 92 (66.66%) |
| IEL | 20 (14.49%) | 118 (85.51%) |
| Salpingitis | 10 (7.24%) | 128 (92.76%) |
| Papillary Hyperplasia | 7 (5.07%) | 110 (94.93%) |
| Tufting | 24 (17.39%) | 114 (82.61 %) |
| Atypia | 10 (7.24%) | 128 (92.76% ) |
IEL(Intraepithelial lymphocyte).
Table 3.
KI-67 p53 scoring results.
| KI-67 SCORE | 1 | 2 | 3 | ||||
| Count | 127 (92.02 %) | 8 (5.79 %) | 3 (2.17 %) | ||||
| p53 score | 0 | 1 | 2 | 3 | 4 | ||
| Count | 50 (36.23 %) | 38 (27.53 %) | 27(19.56% ) | 18 (13.04% ) | 5 (3.62% ) | ||
Table 4.
SCOUT, p53 Signature and STIL results.
| Present | Absent | |
|---|---|---|
| SCOUT | 8 ( 5.79%) | 130 ( 94.21% ) |
| p53 signature | 13 ( 9.42%) | 125 ( 90.58% ) |
| STIL | 1 (0.72% ) | 137 ( 99.28% ) |
SCOUT (secretory cell outgrowths), STIL (serous tubal intraepithelial lesion).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



