
Submitted:
28 October 2023
Posted:
30 October 2023
You are already at the latest version
Abstract
Chronic rhinosinusitis (CRS) can have a significant impact on quality of life. With persistent symptoms and the failure of initial medical treatments, surgical management is indicated. Despite the excellent results of endoscopic sinus surgery for persistent CRS, it is quite a challenging procedure for frontal sinusitis given the complex anatomy and location of the frontal sinus. Frontal sinus cells significantly contribute to the complexity of the frontal sinus, and numerous studies have sought to establish their association with sinusitis. This review offers a comprehensive understanding of the frontal sinus cells, their different classifications, their prevalence among different populations, and their relationship to sinusitis. After an extensive review of the current literature, the International Frontal Sinus Anatomy Classification (IFAC) is the most recent classification method and a preferred practical preoperative assessment tool. Although the Agger Nasi Cell is the most prevalent cell among all reported populations, ethnic variations are still influencing the other cells' distribution. Studies are inconsistent in reporting a relationship between frontal sinus cells and sinusitis, and that is mainly because of the difference in the classification method used. More research using a standardized classification method is needed to understand the association between frontal sinus cells and sinusitis.
Keywords:
frontal sinus cell
; agger nasi
; sinusitis
; rhinosinusitis
; classification
1. Introduction
Chronic rhinosinusitis (CRS) poses a significant and pressing health issue, demanding our attention and understanding. It is a long-lasting condition that is characterized by inflammation of the nasal passages and the sinuses. This disease generally leads to a variety of symptoms like nasal congestion, headache, difficulty in breathing or nasal block, nasal discharge, decreased sense of smell (anosmia) and postnasal drip. Contrary to acute sinusitis which usually lasts for a short period, chronic rhinosinusitis persists for 12 weeks or more due to which patients suffer from reduced quality of life and financial and psychosocial burdens [1,2]. Despite the availability of medical management, surgical options might be indicated for persistent symptoms or failure of initial treatments. Endoscopic sinus surgery (ESS) has shown excellent results in persistent cases [3]. Nevertheless, it is still a challenging technique for frontal sinusitis. In fact, any surgical interventions involving the frontal sinus pose a real challenge because of its unique and complex anatomy [3]. Starting from the location, which is one factor of concern, to risk of injuring nearby structures like the olfactory apparatus, anterior skull base, anterior ethmoid artery, cribriform plate and medial orbital wall [4]. The anterior ethmoidal artery, for instance, is an essential anatomical landmark to know its location if it is below the skull base in mesentery during endoscopic sinus surgeries and access to the frontal sinus. It runs through the roof of the anterior ethmoidal sinus; hence it is prone to injuries in endoscopic sinus surgeries [5,6]. Another factor of concern is the narrow drainage tract between the orbital and the skull base, which carries the risk of serious complications [3]. The frontal sinus and the space where it drains, the frontal recess, are occupied with diverse cells [7]. Frontal sinus cells are groups of air-filled cells found at the anterior ethmoid in the frontal recess. This includes agger nasi, frontal, supraorbital, frontal bulbar, suprasellar, and interfrontal sinus septal cells. It can obstruct the frontal recess outflow, leading to sinusitis [8]. The agger nasi cells, for example, are part of the anterior ethmoidal air cells, and they are the most anterior. These cells are situated anterolaterally and inferiorly to the frontal recess and anteriorly and above the middle turbinate attachment. They are found in 90% of the population and are usually the most common among other frontal sinus cells as single cells but could be multiple smaller or larger [8]. These variations could be due to attachment of uncinet process and enlargement of the ethmoidal bulla as well as the present of large pneumatized frontal beak and crisa galli.
Generally, frontal sinus cells show anatomical variations, which can modify the sinus drainage pathway as discussed in the study done by Wormald et al., 2016 [7]. There is another study showing the arrangement of these cellular variations along the drainage tract which may increase the chance of obstruction and inflammation [4]. Thus, a comprehensive and clear understanding of this anatomy is required for a better management approach for safe surgery and an excellent outcome [4]. That is why multiple classifications have been proposed for better characterization since 1941 [9]. All these classifications are from a different perspective, which eventually led to a nomenclature discrepancy, and are discussed in detail further ahead in this paper. However, confusion has resulted, given the nature of the frontal cells, their complex anatomy, their variations between individuals and populations, and their different categorization methods, making it even more challenging to combine articles from different classifications or even to conclude their association with sinusitis. Therefore, this review attempts to answer whether frontal sinus cell variations are associated with frontal sinusitis. In addition, this paper provides an overview of frontal sinus anatomy, the prevalence of frontal sinus cells, the different classifications, and factors associated with sinusitis.
1.1. Frontal Sinus Anatomy
The frontal sinus is the most superior bilateral paranasal sinus, located just under the forehead, triangular and formed as a part of the frontal bone [10]. The posterior wall of the frontal sinus is formed by the ethmoid bulla and the base of the skull, while the anterior border is formed by the agger nasi cells and the frontal beak. The intersinus septum forms the medial side of each frontal sinus. The lacrimal bone forms the lateral border which is continuation of the frontal process of pre maxillary bone. The upper parts of each orbit make up the sinus floor [11]. The outflow pathway starts from the frontonasal duct located in the anterior part of the medial meatus, followed by a slight narrowing in the inferomedial angle of the sinus known as the frontal infundibulum that opens into the ostium, which can be recognized by a slight bone elevation at the anterior sinus wall continuing to the frontal recess. Moving on from there, two main variations are present for the rest of the drainage pathway: draining via the hiatus semilunaris, middle meatus and finally into the ethmoidal infundibulum, or draining directly to the middle meatus [12].
1.2. The history of frontal sinus cells classification
Before the second half of the 20th century, Van Alyea was the first to group frontal cells into “frontal recess cells” and “invading frontal cells.” [9]. In 1994, four different types of frontal cells (frontoethmoidal cells) were identified by Bent et al. [13]. Two years later, the Kuhn Classification was introduced [14]. Afterwards, this classification was slightly modified by Wormald and Chan for better clinical differentiation between type 3 (K3) and type 4 cells (K4). The Modified Kuhn Classification (MKC) was comprehensive and easy to use [15] which significantly facilitated the anatomical understanding of the frontal sinus and nearby structures (Figure 1) [16].
However, there were some limitations reported in terms of names and information redundancy [16,17]. Moreover, the European Position Paper (EPOS) suggested a general way to classify the cells [2,18]. Yet, it lacks cell relationship details which are required in surgery planning and guidance [7]. Recently, two more classifications were developed around the same time to overcome MKC’s limitations. One is the Agger-Bullar Classification (ABC) which is a compartment-based classification rather than depending on the cell’s morphology [16]. The other is the International Frontal Sinus Anatomy Classification (IFAC) [7]. IFAC provided comprehensiveness and more straightforward names using cells’ topographic positions [7,19]. It is the outcome of experts’ consensus internationally. Also, it is a reliable tool after assessing its inter- and intra-rater reliability [17].
1.3. International Frontal Sinus Anatomy Classification (IFAC)
The IFAC addresses the number and position of the cells and their effect on drainage pathways as shown in Figure 2. Anterior cells shift drainage posteriorly, medially, or posteromedially, these include agger nasi cells (ANC), supra agger cells (SAC), and supra agger frontal cells (SAFC). ANC are directly first cell behind the frontal process of the maxilla, near the middle turbinate, whereas SAC lie behind the insertion of the middle turbinate (second part of middle turbinate) to the skull base and are just superior to the ANC. SAFC found on the floor of the frontal sinus can be either small or large, depending on the pneumatization into the frontal sinus and the corresponding surgical approach which can cause obstruction or re direction of the drainage pathway [19,20]. Supra bulla cell (SBC), supra bulla frontal cell (SBFC), and the supraorbital ethmoid cells (SOEC) are all posterior frontoethmoidal cells that push the drainage pathway anteriorly. The SBC lies above the bulla ethmoidalis but does not pneumatize through the frontal ostium, whereas the SBFC is like the SBC with pneumatization through the frontal ostium. Lastly, SOEC is identical to SBFC apart from the pneumatization of the orbit. The final type of cells is the interfrontal septal cells, they are located medially in the interfrontal sinus septum, thus pushing the drainage pathway laterally or posteriorly [19]. Figure 3 shows the IFAC cell types in sagittal, coronal, and axial CT scans.
2. Frontal sinus cells prevalence in different populations
Multiple studies investigated frontal cells prevalence based on IFAC within different populations [8,19,21,22,23,24,25,26,27] (Table 1). Similarly, other studies investigated their prevalence based on Kuhn classification [28,29,30,31,32,33] (Table 2). When comparing prevalence results between these populations, ANC is found to be the highest in all of them. However, the remaining frontal cells distribution showed variability [24]. Even when comparing them based on anterior, posterior, and medial groups, there was still no agreement [24]. SBCs prevalence was similarly high among Malaysians, Germans, and North Americans, unlike among the Indians and Vietnamese. Almost half or more of the White, Malaysian, German and Egyptian populations had SAC, while it was lower with the rest. In contrast, SOECs were much lower among Malaysians and Caucasians. Interestingly, Turkish pediatrics showed the highest prevalence in SAFC and SBFC, while they were the only group not reporting any Frontal Septal Cell (FSC). This diversity between different populations might reflect the heterogeneity in different frontal cells [24]. Nevertheless, Fawzi et al. reported that when excluding ANC, posterior-based groups (SBCs and SBFCs) had a higher prevalence than anterior-based cells (SACs and SAFCs) in previous studies [24]. Which seems also to be the case with the following studies except with the white population (Table 1). This supports Fawzi’s argument to classify the cells according to their topographical arrangement rather than individually.
A study [33] compared the frequency of frontal sinus cells in Caucasian and Korean subjects using the classification mentioned by Lee et al. [34]. Interestingly, they found the differences between both populations are compatible with their distinctive external facial features which means, having a more protuberant nasion, glabella, and superior orbital rim was associated with an increased incidence of certain groups of frontal cells which was the case with Caucasians [33]. They also concluded that these differences in some cells were more likely attributed to racial reasons. These were less likely to be related to the difference in antero-posterior length of the skull base. Howser et al. also supported the link between craniofacial development and the frontal sinus which might explain the differences between ethnic groups [21]. Furthermore, Johari et al. also compared Malaysian subjects with more than one population using the same classification and they also reported some differences between South-East Asian and other East Asian populations in some cells [29]. These discrepancies were similarly attributed to their ethnic background. Previous studies show no correlation between the different anatomical variations and the increased incidence of signs of opacification. These variations only alter the surgical approach based on radiological signs and patient symptoms [19].
3. Frontal sinus cells and their association with sinusitis
The association between frontal sinus cell variations and sinusitis has been studied in various studies. Brunner et al. was one of the early studies to examine if agger nasi cells contribute to sinusitis [35]. Although they had a relatively small sample size, they found a significant link between a narrowed nasofrontal duct due to agger nasi cell pneumatization and chronic frontal sinusitis. In addition, Meyer et al. reported that some pneumatization variants significantly affect the presence of frontal cells. In hyperpneumatization, for example, there was a positive association with the appearance of frontal cells and vice versa [36]. It is essential to address the classifications used when discussing what was reported in previous articles. That is because cell identification or labelling might vary according to each model. Thus, to ensure accuracy, we grouped them accordingly. For instance, in 2003, Meyer et al. [36] indicated that individuals with type III and type IV had a significant relationship with frontal mucosal thickening using the Bent et al. classification [13]. Nevertheless, their presence does not always lead to sinusitis [36]. In contrast, three more recent articles following the same classification have yet to find significance [37,38,39]. Several authors have attributed these insignificant findings to sinusitis as a mucosal inflammation rather than anatomical obstruction [30,31,39].
The following articles used the Kuhn classification [14]. It was challenging to differentiate whether they used the original Kuhn classification [14] or the modified Kuhn classification [15], as the authors did not clarify in most articles. Lien et al. reported that SBCs, FBCs, and SOECs were significantly related to frontal sinusitis, probably due to a narrowed drainage pathway as shortening happens on the anteroposterior parameters of the frontal recess or frontal ostium [31]. They have also reported a significant association with recessus terminalis (RT) due to the absence of a physical barrier along the drainage tract against allergens, irritants, or ascending infections [40]. In the study of Langille et al. although type VI frontal cells were not identified in any subjects, a significance was found with Type I, II, and III [41]. It has also been noted that ethnic diversity, seasonality, and the classical presentation of sinusitis are all factors that might explain the variability between different authors [41]. Both Kubota et al. [30] and Johari et al. [29] reported a p-value less than 0.05 for only Frontal Bulla Cells (FBC) with sinusitis. Type III and IV frontal cells were significant in both studies by House et al. and Meyer et al. [36,42]. Interestingly, they also reported a significant p-value on the interfrontal sinus septal cell with an Odds ratio of 0.51 (0.26, 0.99). This suggests a lesser chance of developing a sinus disease if this cell is present. Lai and Hashimoto’s findings indicate no significance when it comes to the presence of these cells [43,44]. On the other hand, they reported a significant association between some opacified areas or opacified frontal cells and sinusitis, respectively. These were the frontal recess and sinus lateralis for the former, agger nasi, type I Frontal Cell (FC1), and SBC for the latter.
Since IFAC is a relatively new classification, a few studies only used it to look for its association with sinusitis. In 2019, Sommer et al., using IFAC, attempted to investigate any relationship between the cells and radiological signs of opacification but the study ended up with no significant findings [19]. However, it is important to keep in mind the way in which frontal cell incidence was reported in this study. It did not differentiate whether a patient had it unilaterally or bilaterally, unlike most previous studies, which reported each side separately. One patient can have two cells (one on each side) which might affect the total incidence and the explanation of the results. One year later, Seth et al. failed to draw a significant association. Furthermore, the inconsistency between various studies can be attributed to different ethnicities, classifications, or even a small sample size [25]. Among the IFAC-based articles, only Fawzi et al. found a significant association between developing sinusitis and two types of frontal cells: SOEC and FSC [24]. It is worth mentioning that both were the minor prevalent group of cells in their sample. However, given the position of the FSC, for example, the possibility of frontal sinus blockage can be explained. Thus, its role in sinusitis should be considered especially during endoscopic sinus surgery. As part of post-surgical management, recurrence is sometimes attributed to incomplete resection of cells situated within the sinus drainage pathway or cause or blockage of the drainage pathway [24]. There is an attempt to correlate the IFAC and Kuhn classifications for comparison purposes. Types I and II were assumed to be SAC, and Types III and IV were assumed to be SAFC [26]. Such an assumption must be examined in further studies to reach a clearer conclusion regarding sinusitis and frontal sinus cells.
Given all the discrepancies between different classifications and, therefore, different findings, it has been found that having sinusitis can make it even more challenging to identify the cells [45]. On the other hand, IFAC classification made it easier to assess frontal cells in healthy individuals or those who have a less severe degree of sinusitis [45]. Therefore, concluding an association between frontal cells and sinusitis is limited when severe sinusitis cases are usually excluded due to visualization difficulty [21]. Similarly, Sommer reported the simplicity of using such classification, especially with those with prior anatomical backgrounds [19]. The discrepancies with regard to association between frontal sinus variations and sinusitis from various studies are presented in Table 3.
3.1. Other factors associated with sinusitis
A number of authors have looked into sinusitis in children [46,47,48,49]. Among this age group, the maxillary sinus was the most involved in sinusitis [49,50,51]. And that could be due to a smaller middle meatus compared to adults [49]. On the other hand, the anterior ethmoid was the most common in adults [49]. April et al. have also compared adults and children [46]. They found sinusitis was significantly more frequent in the maxillary, anterior ethmoid, posterior ethmoid, and frontal sinuses with children [46]. However, again among the children’s group, one of the studies reported no association between their age and the severity of sinusitis [51]. Also, two studies found no relationship between anatomic variations and sinusitis in the paediatric population [47,49]. This might be due to the size of these variations, which do not extend enough to block the sinuses [47]. Others report this anatomical variation can cause more complications with sinus or brain/meningeal or orbit due to simple acute sinusitis [4,52].
In terms of the effect of gender on sinusitis, a study done by Lien et al. found no significant relationship [31]. However, more recent evidence revealed a significantly higher sinusitis rate among males in frontal cell type VI [42]. Knowing such differences with gender or ethnicity might decrease the threshold to order dispensable scans [42]. Given all that has been mentioned so far, several authors could not reach a clear conclusion regarding the effect of frontal cells or anatomic variations. Thus, some studies suggested that other causes might be more important than anatomical factors [47,53]. However, overall, there is a consensus that sinusitis is a multifactorial disease. Adding to the anatomical aspect, other factors include mucosal inflammation, sinonasal polyposis, upper respiratory tract infection, allergic rhinitis, adenoid hypertrophy, impaired immunity, gastroesophageal reflux disease and environmental factors [31,54].
4. Surgical approaches with anatomical variations of frontal sinus anatomy
Considering the complexity of the frontal sinus and the overall knowledge of the direct pathway, multiple explanations have been added to address this point. For example, in the presence of a supra agger cell (SAC) with a small bulla cell, the technique is to divert the drainage through the agger nasi window to drain the frontal sinus, while in comparison to the supra-aggar nasi cell without a small bulla cell, the technique is to go with an intact bulla to drain the frontal sinus through an intact bulla with the use of an angled scope and instrument. In contrast, if a large supra agger frontal cell (SAFC) is present, the removal of the bulla and any cells above it is required in order to expose the frontal recess and sinus drainage safely without damaging the orbits, skull base, or anterior ethmoid artery. However, if the nasion is short and low, with a small agger nasi cells, and the drainage is blocked, then entry to the frontal sinus is achieved laterally by drilling the frontal beak in order to face the frontal sinus posterior table using straight degree scope and equipment without the need of curved degreed scope [55]. Further drilling of the frontal beak to the orbital superior medial wall and the medial part of the crisa galli or middle turbinate attachment may be necessary for large supra agger frontal cells and medially supra orbital ethmoid cells, making the procedure Draf 2a/2b or Draf III [7].
5. Conclusion
Interventions for frontal sinusitis are considered a surgical challenge given the unique anatomy of this structure. In an attempt to ease this process, different classifications have been developed. Yet, multiple studies reported variations in the frontal cells’ prevalence. Others suggested their association with sinusitis. This paper aimed to see if there was any association between frontal sinus cells and frontal sinusitis. After carefully reviewing the available literature, there is still inconsistency between the published results. One explanation might be that severe sinusitis cases were excluded due to distorted imaging. Although some significant associations were found with specific groups of cells, the sample size is still insufficient for generalization. Adding to that, some of these associations were related to other anatomical characteristics. Moreover, the ethnic factor plays a crucial role, whether for the prevalence of frontal cells or their association with sinusitis.
Although it is still safe to say that sinusitis is a multifactorial disease, this work enhances our understanding of the frontal sinus cells and the factors contributing to sinusitis. Grouping studies according to the classification model used was a beneficial step in analysing the results. We noticed that IFAC is a preferred practical classification and preoperative assessment tool. Although it is still a relatively new model compared to Khun, for example, most recent studies rely on it. This is a promising step, as this consensus will standardize the published data. Subsequently, it will help establish a more accurate analysis of future research. Further studies can also investigate the associations of the frontal cells to sinusitis as groups (anterior, posterior, and medial) rather than individually. This approach is more surgically relatable. A natural progression of this work is to assess the association of frontal sinusitis with other anatomical landmarks apart from frontal cells.
Author Contributions
Conceptualization, S.R.S., E.A.A., and T.A.H.; methodology, T.A.H., and M.A.W.; software, T.A.H., M.A.L., and S.A.M.; validation, E.A.A., A.M., M.A.W., and S.R.S.; data curation, T.A.H., M.A.L., M.A.W., and S.A.M.; writing—original draft preparation, E.A.A., S.R.S., T.A.H., M.A.L., and S.A.M.; writing—review and editing, S.R.S., E.A.A., and A.M.; supervision, S.R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Erskine, S.E.; Verkerk, M.M.; Notley, C.; Williamson, I.G.; Philpott, C.M. Chronic Rhinosinusitis: Patient Experiences of Primary and Secondary Care–a Qualitative Study. Clinical Otolaryngology 2016, 41, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Dieudonné Nyenbue Tshipukane 2020, 103. [Google Scholar] [CrossRef]
- DeConde, A.S.; Smith, T.L. Outcomes after Frontal Sinus Surgery: An Evidence-Based Review. Otolaryngol Clin North Am 2016, 49, 1019–1033. [Google Scholar] [CrossRef]
- Korban, Z.R.; Casiano, R.R. Standard Endoscopic Approaches in Frontal Sinus Surgery: Technical Pearls and Approach Selection. Otolaryngol Clin North Am 2016, 49, 989–1006. [Google Scholar] [CrossRef] [PubMed]
- El-Anwar, M.W.; Khazbak, A.O.; Eldib, D.B.; Algazzar, H.Y. Anterior Ethmoidal Artery: A Computed Tomography Analysis and New Classifications. J Neurol Surg B Skull Base 2020, 82, e259–e267. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.B.; Kim, M.G.; Jung, Y.G. The Anatomical Relationship between the Anterior Ethmoid Artery, Frontal Sinus, and Intervening Air Cells; Can the Artery Be Useful Landmark. Korean J Otorhinolaryngol-Head Neck Surg 2014, 57, 687–691. [Google Scholar] [CrossRef]
- Wormald, P.; Hoseman, W.; Callejas, C.; Weber, R.K.; Kennedy, D.W.; Citardi, M.J.; Senior, B.A.; Smith, T.L.; Hwang, P.H.; Orlandi, R.R. The International Frontal Sinus Anatomy Classification (IFAC) and Classification of the Extent of Endoscopic Frontal Sinus Surgery (EFSS). In Proceedings of the International forum of allergy & rhinology; Wiley Online Library, 2016; Vol. 6, pp. 677–696.
- Gotlib, T.; Kołodziejczyk, P.; Kuźmińska, M.; Bobecka-Wesołowska, K.; Niemczyk, K. Three-dimensional Computed Tomography Analysis of Frontoethmoidal Cells: A Critical Evaluation of the International Frontal Sinus Anatomy Classification (IFAC). Clinical Otolaryngology 2019, 44, 954–960. [Google Scholar] [CrossRef]
- Van Alyea, O.E. Frontal Cells: An Anatomic Study of These Cells with Consideration of Their Clinical Significance. Arch Otolaryngol 1941, 34, 11–23. [Google Scholar] [CrossRef]
- Shokri, A.; Faradmal, M.J.; Hekmat, B. Correlations between Anatomical Variations of the Nasal Cavity and Ethmoidal Sinuses on Cone-Beam Computed Tomography Scans. Imaging Sci Dent 2019, 49, 103. [Google Scholar] [CrossRef]
- Dassi, C.S.; Demarco, F.R.; Mangussi-Gomes, J.; Weber, R.; Balsalobre, L.; Stamm, A.C. The Frontal Sinus and Frontal Recess: Anatomical, Radiological and Surgical Concepts. Int Arch Otorhinolaryngol 2020, 24, 364–375. [Google Scholar] [CrossRef]
- L. Drake, R.; Vogl, A.W.; Mitchell, A.W.M. Grays Anatomy For Students, 3rd Edition; 2014; ISBN 978-0-7020-5131-9.
- Bent, J.P.; Guilty-Siller, G.; Kuhn, F.A. The Frontal Cell As a Cause of Frontal Sinus Obstruction; 1994; Vol. 156;
- Kuhn, F.A. CHRONIC FRONTAL SINUSITIS: THE ENDOSCOPIC FRONTAL RECESS APPROACH; 1996;
- Wormald, P.-J. Three-Dimensional Building Block Approach to Understanding the Anatomy of the Frontal Recess and Frontal Sinus. Oper Tech Otolayngol Head Neck Surg 2006, 17, 2–5. [Google Scholar] [CrossRef]
- Pianta, L.; Ferrari, M.; Schreiber, A.; Mattavelli, D.; Lancini, D.; Bottazzoli, M.; Maroldi, R.; Rodella, L.F.; Ravanelli, M.; Nicolai, P. Agger-Bullar Classification (ABC) of the Frontal Sinus Drainage Pathway: Validation in a Preclinical Setting. Int Forum Allergy Rhinol 2016, 6, 981–989. [Google Scholar] [CrossRef]
- Villarreal, R.; Wrobel, B.B.; Macias-Valle, L.F.; Davis, G.E.; Prihoda, T.J.; Luong, A.U.; McMains, K.C.; Weitzel, E.K.; Yao, W.C.; Brunworth, J. International Assessment of Inter-and Intrarater Reliability of the International Frontal Sinus Anatomy Classification System. In Proceedings of the International Forum of Allergy & Rhinology; Wiley Online Library, 2019; Vol. 9, pp. 39–45.
- Lund, V.J.; Stammberger, H.; Fokkens, W.J.; Bernal-Sprekelsen, M. European Position Paper on the Anatomical Terminology of the Internal Nose and Paranasal Sinuses. Rhinology Supplement 24 2014, 50, 1–34. [Google Scholar]
- Sommer, F.; Hoffmann, T.K.; Harter, L.; Döscher, J.; Kleiner, S.; Lindemann, J.; Leunig, A. Incidence of Anatomical Variations According to the International Frontal Sinus Anatomy Classification (IFAC) and Their Coincidence with Radiological Sings of Opacification. European Archives of Oto-Rhino-Laryngology 2019, 276, 3139–3146. [Google Scholar] [CrossRef] [PubMed]
- Dassi, C.S.; Demarco, F.R.; Mangussi-Gomes, J.; Weber, R.; Balsalobre, L.; Stamm, A.C. The Frontal Sinus and Frontal Recess: Anatomical, Radiological and Surgical Concepts. Int Arch Otorhinolaryngol 2020, 24, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Howser, L.A.; Jones, A.J.; Sreenath, S.B.; Ting, J.Y.; Illing, E.A. Frontal Sinus Anatomy Variations in Race and Sex Using the International Frontal Sinus Anatomy Classification. Ear Nose Throat J 2023, 01455613231185701. [Google Scholar] [CrossRef] [PubMed]
- Köksal, A.; Tuğtağ Demir, B.; Çankal, F. Change of Frontal Sinus in Age of According to the International Frontal Sinus Anatomy Classification. Acta radiol 2023, 02841851231172775. [Google Scholar] [CrossRef]
- Nofal, A.A.B.; El-Anwar, M.W. Frontal Recess Cells in International Frontal Sinus Anatomy Classification (IFAC); Prevalence, Infection Incidence, and Relation to Frontal Sinus Infection in Chronic Sinusitis Patients. Indian Journal of Otolaryngology and Head & Neck Surgery 2022, 1–8.
- Fawzi, N.E.A.; Lazim, N.M.; Aziz, M.E.; Mohammad, Z.W.; Abdullah, B. The Prevalence of Frontal Cell Variants According to the International Frontal Sinus Anatomy Classification and Their Associations with Frontal Sinusitis. European Archives of Oto-Rhino-Laryngology 2022, 279, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Seth, N.; Kumar, J.; Garg, A.; Singh, I.; Meher, R. Computed Tomographic Analysis of the Prevalence of International Frontal Sinus Anatomy Classification Cells and Their Association with Frontal Sinusitis. J Laryngol Otol 2020, 134, 887–894. [Google Scholar] [CrossRef]
- Tran, L. V; Ngo, N.H.; Psaltis, A.J. A Radiological Study Assessing the Prevalence of Frontal Recess Cells and the Most Common Frontal Sinus Drainage Pathways. Am J Rhinol Allergy 2019, 33, 323–330. [Google Scholar] [CrossRef]
- Choby, G.; Thamboo, A.; Won, T.; Kim, J.; Shih, L.C.; Hwang, P.H. Computed Tomography Analysis of Frontal Cell Prevalence According to the International Frontal Sinus Anatomy Classification. In Proceedings of the International forum of allergy & rhinology; Wiley Online Library, 2018; Vol. 8, pp. 825–830.
- Abraham, Z.S.; Kahinga, A.A. Prevalence of Frontal Cells and Their Relation to Frontal Sinusitis among Patients Who Underwent Functional Endoscopic Sinus Surgery: A Prospective Cross-Sectional Study in Tanzania. Annals of Medicine and Surgery 2022, 84, 104907. [Google Scholar] [CrossRef] [PubMed]
- Johari, H.H.; Mohamad, I.; Sachlin, I.S.; Aziz, M.E.; Mey, T.Y.; Ramli, R.R. A Computed Tomographic Analysis of Frontal Recess Cells in Association with the Development of Frontal Sinusitis. Auris Nasus Larynx 2018, 45, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Takeno, S.; Hirakawa, K. Frontal Recess Anatomy in Japanese Subjects and Its Effect on the Development of Frontal Sinusitis: Computed Tomography Analysis. Journal of Otolaryngology-Head & Neck Surgery 2015, 44, 1–6. [Google Scholar]
- Lien, C.; Weng, H.; Chang, Y.; Lin, Y.; Wang, W. Computed Tomographic Analysis of Frontal Recess Anatomy and Its Effect on the Development of Frontal Sinusitis. Laryngoscope 2010, 120, 2521–2527. [Google Scholar] [CrossRef] [PubMed]
- Han, J.K.; Ghanem, T.; Lee, B.; Gross, C.W. Various Causes for Frontal Sinus Obstruction. Am J Otolaryngol 2009, 30, 80–82. [Google Scholar] [CrossRef]
- Cho, J.H.; Citardi, M.J.; Lee, W.T.; Sautter, N.B.; Lee, H.-M.; Yoon, J.-H.; Hong, S.-C.; Kim, J.K. Comparison of Frontal Pneumatization Patterns between Koreans and Caucasians. Otolaryngology—Head and Neck Surgery 2006, 135, 780–786. [Google Scholar] [CrossRef]
- Lee, W.T.; Kuhn, F.A.; Citardi, M.J. 3D Computed Tomographic Analysis of Frontal Recess Anatomy in Patients without Frontal Sinusitis. Otolaryngology—Head and Neck Surgery 2004, 131, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Brunner, E.; Jacobs, J.B.; Shpizner, B.A.; Lebowitz, R.A.; Holliday, R.A. ROLE OF THE AGGER NASI CELL IN CHRONIC FRONTAL SINUSITIS; 1996;
- Meyer, T.K.; Kocak, M.; Smith, M.M.; Smith, T.L. Coronal Computed Tomography Analysis of Frontal Cells. Am J Rhinol 2003, 17, 163–168. [Google Scholar] [CrossRef]
- Abraham, Z.S.; Kahinga, A.A. Prevalence of Frontal Cells and Their Relation to Frontal Sinusitis among Patients Who Underwent Functional Endoscopic Sinus Surgery: A Prospective Cross-Sectional Study in Tanzania. Annals of Medicine and Surgery 2022, 84. [Google Scholar] [CrossRef] [PubMed]
- Eweiss, A.Z.; Khalil, H.S. The Prevalence of Frontal Cells and Their Relation to Frontal Sinusitis: A Radiological Study of the Frontal Recess Area. Int Sch Res Notices 2013, 2013. [Google Scholar] [CrossRef]
- DelGaudio, J.M.; Hudgins, P.A.; Venkatraman, G.; Beningfield, A. Multiplanar Computed Tomographic Analysis of Frontal Recess Cells: Effect on Frontal Isthmus Size and Frontal Sinusitis. Arch Otolaryngol Head Neck Surg 2005, 131, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Turgut, S.; Ercan, I.; Sayın, I.; Bas¸ak, B. The Relationship Between Frontal Sinusitis and Localization of the Frontal Sinus Outflow Tract A Computer-Assisted Anatomical and Clinical Study; 2005;
- Langille, M.; Walters, E.; Dziegielewski, P.T.; Kotylak, T.; Wright, E.D. Frontal Sinus Cells: Identification, Prevalence, and Association with Frontal Sinus Mucosal Thickening. Am J Rhinol Allergy 2012, 26, e107–e110. [Google Scholar] [CrossRef] [PubMed]
- House, L.K.; Stringer, S.P.; Seals, S. Correlation of Frontal Sinus Recess Anatomy with Ethnicity, Gender, and Pathology. Am J Otolaryngol 2017, 38, 452–455. [Google Scholar] [CrossRef]
- Hashimoto, K.; Tsuzuki, K.; Okazaki, K.; Sakagami, M. Influence of Opacification in the Frontal Recess on Frontal Sinusitis. J Laryngol Otol 2017, 131, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Lai, W. Sen; Yang, P.L.; Lee, C.H.; Lin, Y.Y.; Chu, Y.H.; Wang, C.H.; Wang, H.W.; Shih, C.P. The Association of Frontal Recess Anatomy and Mucosal Disease on the Presence of Chronic Frontal Sinusitis: A Computed Tomographic Analysis. Rhinology 2014, 52, 208–214. [Google Scholar] [CrossRef]
- Jaremek-Ochniak, W.; Sierdziński, J.; Popko-Zagor, M. Three-Dimensional Computed Tomography Analysis of Frontal Recess Cells According to the International Frontal Sinus Anatomy Classification (IFAC) – Difficulties in Identification of Frontal Recess Cells in Patients with Diffuse Primary Chronic Rhinosinusitis? Otolaryngologia Polska 2022, 76, 7–14. [Google Scholar] [CrossRef] [PubMed]
- April, M.M.; Zinreich, S.J.; Baroody, F.M.; Naclerio, R.M. Coronal CT Scan Abnormalities in Children with Chronic Sinusitis. Laryngoscope 1993, 103, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Jun Kim, H.; Jung Cho, M.; Lee, J.-W.; Tae Kim, Y.; Kahng, H.; Sung Kim, H.; Hahm, K.-H. The Relationship between Anatomic Variations of Paranasal Sinuses and Chronic Sinusitis in Children. Acta Otolaryngol 2006, 126, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Lusk, R.P.; McAlister, B.; el Fouley, A. Anatomic Variation in Pediatric Chronic Sinusitis: A CT Study. Otolaryngol Clin North Am 1996, 29, 75–91. [Google Scholar] [CrossRef]
- Al-Qudah, M. The Relationship between Anatomical Variations of the Sino-Nasal Region and Chronic Sinusitis Extension in Children. Int J Pediatr Otorhinolaryngol 2008, 72, 817–821. [Google Scholar] [CrossRef]
- April, M.M.; Zinreich, S.J.; Baroody, F.M.; Naclerio, R.M. Coronal CT Scan Abnormalities in Children with Chronic Sinusitis. Laryngoscope 1993, 103, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Cho, M.J.; Lee, J.W.; Kim, Y.T.; Kahng, H.; Kim, H.S.; Hahm, K.H. The Relationship between Anatomic Variations of Paranasal Sinuses and Chronic Sinusitis in Children. Acta Otolaryngol 2006, 126, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Kendall, K.A.; Senders, C.W. Orbital and Intracranial Complications of Sinusitis in Children and Adults. In Diseases of the sinuses: a comprehensive textbook of diagnosis and treatment; Springer, 1996; pp. 247–271.
- Al-Qudah, M. The Relationship between Anatomical Variations of the Sino-Nasal Region and Chronic Sinusitis Extension in Children. Int J Pediatr Otorhinolaryngol 2008, 72, 817–821. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, A.J.; Rosenfeld, R.M. Treatment of Pediatric Sinusitis. Pediatric Clinics 2003, 50, 413–426. [Google Scholar] [CrossRef]
- Seresirikachorn, K.; Sit, A.; Png, L.H.; Kalish, L.; Campbell, R.G.; Alvarado, R.; Harvey, R.J. Carolyn’s Window Approach to Unilateral Frontal Sinus Surgery. Laryngoscope 2023. [Google Scholar] [CrossRef]
Figure 1.
Modified Kuhn Classification of frontal sinus cells [15].
Figure 1.
Modified Kuhn Classification of frontal sinus cells [15].
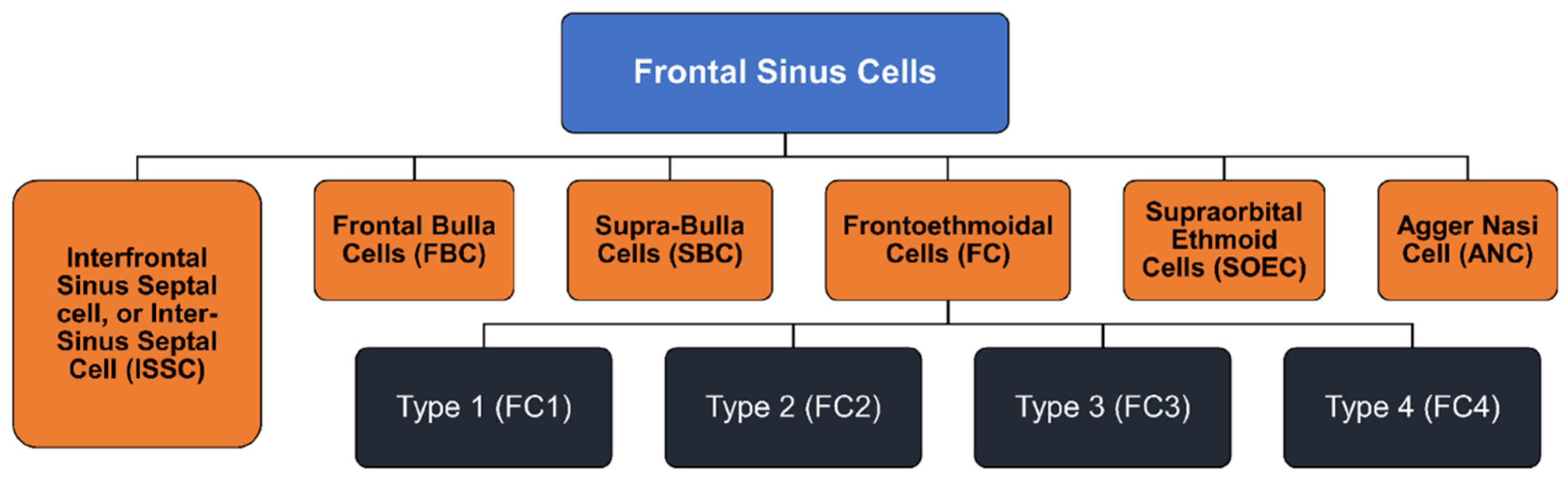
Figure 2.
International Frontal Sinus Anatomy Classification (IFAC) [7].
Figure 2.
International Frontal Sinus Anatomy Classification (IFAC) [7].
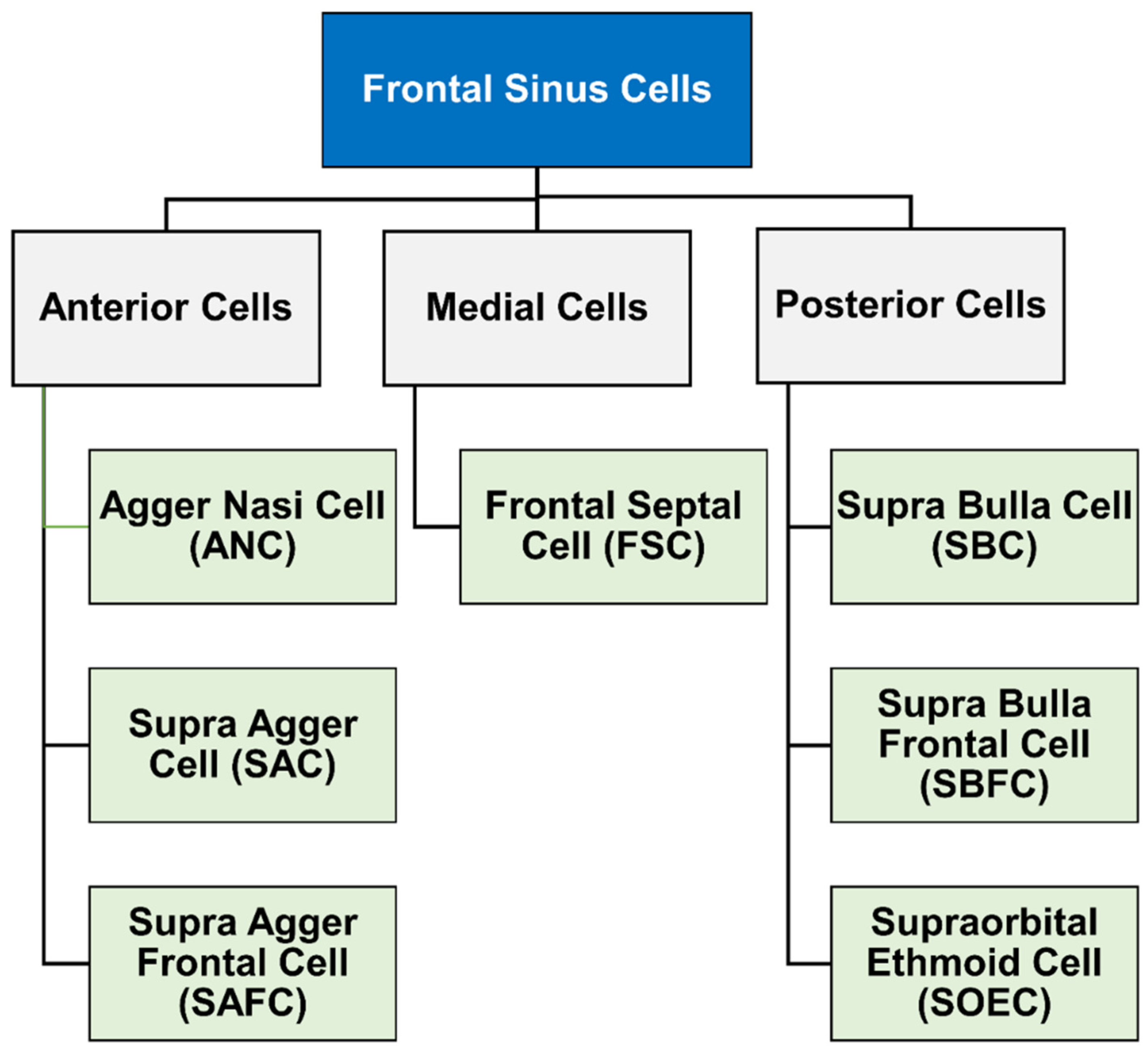
Figure 3.
IFAC cell types using computed tomography. Different cell types according to IFAC on CT using sagittal, axial and coronal planes for each cell type: (A–C) aggar nasi cell, (D–F) supra aggar cell, (G–I) supra aggar frontal cell, (J–L) supra bulla cell, (M–O) supra bulla frontal cell, (P–R) supraorbital ethmoid cell, and (S–U) frontal septal cell.
Figure 3.
IFAC cell types using computed tomography. Different cell types according to IFAC on CT using sagittal, axial and coronal planes for each cell type: (A–C) aggar nasi cell, (D–F) supra aggar cell, (G–I) supra aggar frontal cell, (J–L) supra bulla cell, (M–O) supra bulla frontal cell, (P–R) supraorbital ethmoid cell, and (S–U) frontal septal cell.
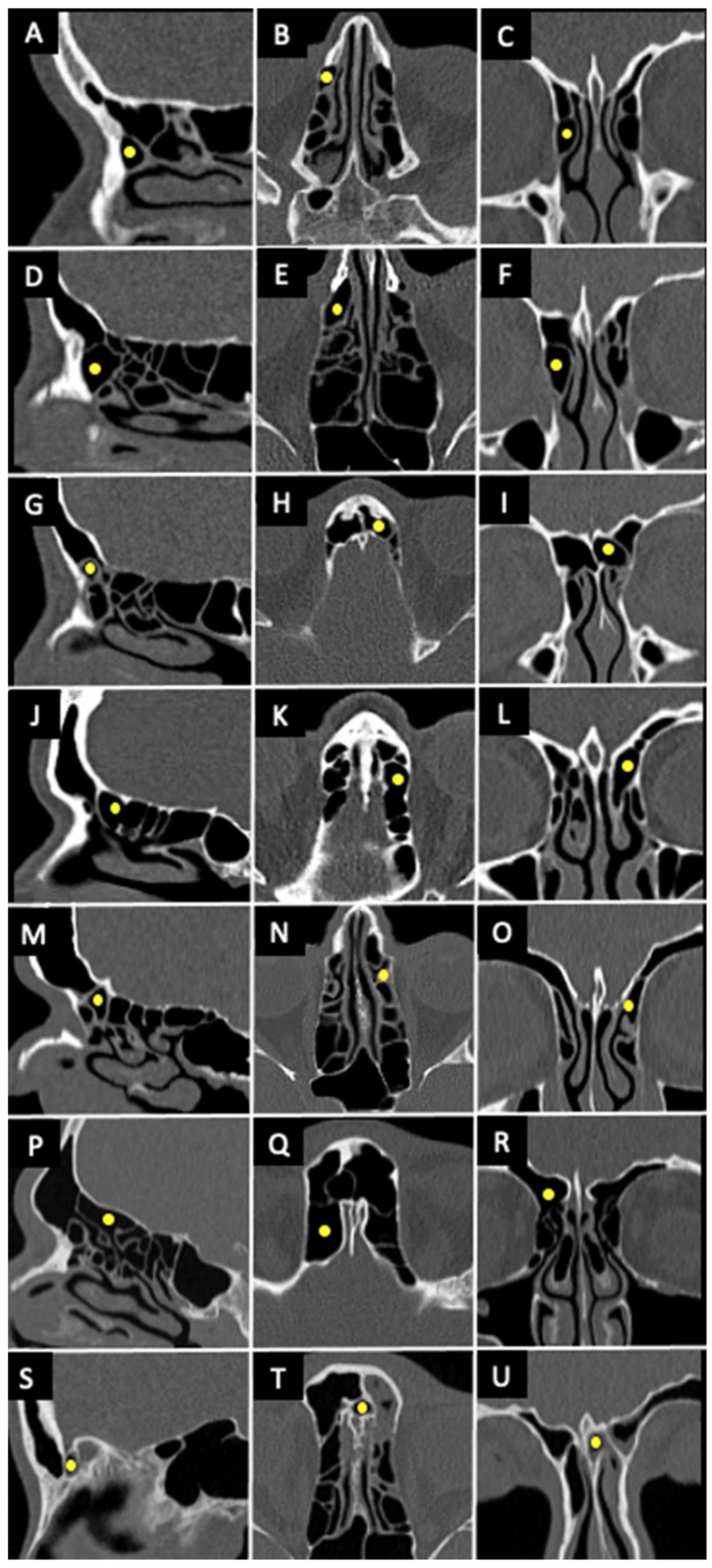

Table 1.
Frontal sinus cells prevalence among different populations using IFAC method. (ANC: agger nasi cells, SAC: supra agger cells, SAFC: supra agger frontal cells, FSC: frontal septal cell, SBC: supra bulla cell, SBFC: supra bulla frontal cell, SOEC: supraorbital ethmoid cells; CT: computed tomography).
Table 1.
Frontal sinus cells prevalence among different populations using IFAC method. (ANC: agger nasi cells, SAC: supra agger cells, SAFC: supra agger frontal cells, FSC: frontal septal cell, SBC: supra bulla cell, SBFC: supra bulla frontal cell, SOEC: supraorbital ethmoid cells; CT: computed tomography).
| First author | Year | Population | Screening method | Number of sides | Cells prevalence (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ANC | SAC | SAFC | SBC | SBFC | SOEC | FSC | |||||
| Howser et al. [21] | 2023 | White | maxillofacial or sinus CT | 100 | 96.0 | 57.0 | 26.0 | 64.0 | 17.0 | 12.0 | 20.0 |
| Black | 100 | 95.0 | 40.0 | 31.0 | 56.0 | 17.0 | 8.0 | 18.0 | |||
| Asian | 78 | 94.9 | 37.2 | 23.1 | 55.1 | 11.5 | 21.8 | 24.4 | |||
| Latino | 90 | 97.8 | 35.6 | 25.6 | 54.4 | 7.8 | 7.8 | 16.7 | |||
| Koksal et al. [22] | 2023 | Turkish | paranasal sinus CT | 160 (Adults) | 86.3 | 35.0 | 44.4 | 54.4 | 46.9 | 19.4 | 3.4 |
| 160 (Pediatrics) | 93.1 | 41.9 | 60.0 | 76.3 | 58.5 | 18.8 | 0 | ||||
| Nofal & El-Anwar [23] | 2022 | Egyptian | maxillofacial CT | 200 | 97.0 | 48.0 | 11.0 | 72.0 | 23.0 | 42.0 | 21.0 |
| Fawzi et al. [24] | 2022 | Malaysian | paranasal sinus CT | 400 | 95.5 | 50.0 | 36.0 | 60.8 | 53.0 | 5.5 | 8.3 |
| Seth et al. [25] | 2020 | Indian | maxillofacial or sinus CT | 180 | 95.5 | 33.3 | 22.2 | 36.1 | 21.1 | 39.4 | 21.1 |
| Gotlib et al. [8] | 2019 | Caucasian | paranasal sinus CT | 206 | 86.9 | 34.0 | 17.5 | 77.2 | 22.8 | 5.8 | 27.2 |
| Tran et al. [26] | 2019 | Vietnamese | sinus CT | 208 | 95.7 | 16.3 | 13 | 46.2 | 4.3 | 17.3 | 10.6 |
| Sommer et al. [19] | 2019 | German | sinus CT | 498 | 95.2 | 49 | 24.9 | 88.8 | 26.5 | 9.2 | 27.7 |
| Choby et al. [27] | 2018 | North American | sinus CT | 200 | 96.5 | 30 | 20 | 72 | 5.5 | 28.5 | 30 |
Table 2.
Frontal sinus cells prevalence among different populations using Kuhn method. (ANC: agger nasi cells, FC: frontal cell, FBC: frontal bulla cell, SBC: supra bulla cell, SBFC: supra bulla frontal cell, SOEC: supraorbital ethmoid cells; CT: computed tomography).
Table 2.
Frontal sinus cells prevalence among different populations using Kuhn method. (ANC: agger nasi cells, FC: frontal cell, FBC: frontal bulla cell, SBC: supra bulla cell, SBFC: supra bulla frontal cell, SOEC: supraorbital ethmoid cells; CT: computed tomography).
| First author | Year | Population | Screening method | Number of sides | Cells prevalence (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ANC | FC1 | FC2 | FC3 | FC4 | SBC | SOEC | FBC | IFSSC | |||||
| Abraham & Kahinga [28] | 2022 | Tanzanian | paranasal sinus CT | 90 | 83.3 | 22.2 | 35.6 | 11.1 | 3.3 | N/A | N/A | N/A | N/A |
| Johari et al. [29] | 2018 | Malaysian | paranasal sinus CT | 312 | 98.1 | 28.8 | 31.1 | 14.4 | 0 | 40.3 | 16.7 | 33.0 | 10.8 |
| Kubota et al. [30] | 2015 | Japanese | Spiral CT scans | 300 | 88.0 | 37.0 | 6.3 | 4.3 | 1.3 | 37.0 | 6.0 | 7.0 | 8.6 |
| Lien et al. [31] | 2010 | Taiwanese | Spiral CT scans | 363 | 89.0 | 21.5 | 10.5 | 7.7 | 0 | 39.1 | 7.7 | 6.3 | 9.6 |
| Han et al. [32] | 2008 | Chinese | Spiral CT scans | 404 | 94.1 | 24.4 | 7.0 | 8.2 | 0 | 36.6 | 5.4 | 9.0 | 12.4 |
| Cho et al. [33] | 2006 | Korean | sinus CT | 114 | 94.0 | 22.8 | 14.0 | 7.9 | 0 | 39.5 | 2.6 | 14.0 | 8.8 |
| Caucasian | 82 | 86.6 | 35.4 | 20.7 | 8.5 | 0 | 11.0 | 64.6 | 6.1 | 7.3 | |||
Table 3.
The association between frontal sinus cells and sinusitis from different studies.
| Study | Year | Method of classification used | Association | If yes, which cells? |
|---|---|---|---|---|
| Meyer et al. [36] | 2003 | Bent | Yes | type III and IV |
| Delgaudio et al. [39] | 2005 | Bent | No | N/A |
| Eweiss & Khalil [38] | 2013 | Bent | No | N/A |
| Abraham & Kahinga [28] | 2022 | Bent | No | N/A |
| Lien et al. [31] | 2010 | Kuhn | Yes | SBC, FBC, and SOEC |
| Langille et al. [41] | 2012 | Kuhn | Yes | type I, II, and III |
| Lai et al. [44] | 2014 | Kuhn | No | N/A |
| Kubota et al. [30] | 2015 | Kuhn | Yes | FBC |
| Hashimoto et al. [43] | 2017 | Kuhn | No | N/A |
| House et al. [42] | 2017 | Kuhn | Yes | type III and IV |
| Johari et al. [29] | 2018 | Kuhn | Yes | FBC |
| Sommer et al. [19] | 2019 | IFAC | No | N/A |
| Seth et al. [25] | 2020 | IFAC | No | N/A |
| Fawzi et al. [24] | 2022 | IFAC | Yes | SOEC and FSC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



