
Submitted:
30 October 2023
Posted:
31 October 2023
You are already at the latest version
Abstract
Few clinical factors can help predict spontaneous culture conversion (SCC) in patients with Mycobacterium avium complex-pulmonary disease (MAC-PD). We retrospectively classified 373 MPD patients who had undergone watchful waiting without antibiotics according to the so-called ‘body mass index (BMI), age, cavity, erythrocyte sedimentation rate (ESR), and sex (BACES)’ severity. We evaluated whether lower severity is associated with a higher rate of SCC. Of 373 patients, 153 (41%) achieved SCC without antibiotics during a median follow-up of 48.1 months. There was a trend toward a higher SCC rate in patients with lower BACES severity: 48% (87/183), 37% (58/157), and 24% (8/33) in the mild, moderate, and severe BACES groups, respectively. In addition, a favorable outcome, defined as maintaining SCC or having two consecutive negative sputum cultures until the last follow-up date, was also more common in patients with lower BACES severity with 53% (97/183), 34% (54/157), and 18% (6/33) in the mild, moderate, and severe BACES groups, respectively. In multivariate analysis, moderate (hazard ratio [HR]=0.63; 95% confidence interval [CI] 0.44 – 0.91; p = 0.013) and severe BACES (HR 0.37; 95% CI 0.16 – 0.90; p = 0.028) had a significantly negative impact on favorable outcomes compared to mild BACES. Lower BACES severity may be associated with SCC in MAC-PD patients.
Keywords:
Mycobacterium avium complex
; outcome
; treatment
; severity
Introduction
Nontuberculous mycobacteria (NTM) are ubiquitous organisms that cause chronic pulmonary disease (PD) and the burden of this disease is increasing globally [1]. Of more than 200 NTM species, Mycobacterium avium complex (MAC), which includes mainly M. avium and M. intracellulare, is the most common pathogen [2,3]. Guidelines recommend long-term multi-drug antibiotic therapy, which includes a macrolide, ethambutol, and rifamycin, with or without an injectable aminoglycoside [3,4]. However, due to the high frequency of side effects associated with long-term antibiotics and unsatisfactory outcomes, antibiotic therapy imposes a significant burden on both clinicians and patients [5].
Notably, MAC-PD patients experience a heterogeneous clinical course. Approximately 30–40% of patients follow either a stable course or undergo spontaneous culture conversion (SCC) without requiring antibiotic treatment after diagnosis [6,7]. Therefore, given the challenges associated with antibiotic use and the relatively low success rate of antibiotic therapy, current clinical guidelines recommend watchful waiting rather than immediately starting antibiotics for less severe patients following a confirmed MAC-PD diagnosis.
In this context, knowing which clinical factors are associated with a higher likelihood of SCC could be important for guiding medical treatment decisions in clinical practice. However, it is still not clear which clinical characteristics lead to SCC or persistent cultivation of NTM. Although one study reported some clinical characteristics related to SCC [6], other studies have failed to identify any obvious clinical factors [7,8]. In addition, previous studies have not considered the severity of NTM-PD, and there are no tools for assessing the progression of MPD.
A recent study developed a severity scoring system, referred to as the ‘body mass index (BMI), age, cavity, erythrocyte sedimentation rate (ESR), and sex (BACES),’ to predict the prognosis of NTM-PD [9]. It may help predict the antibiotic treatment response [10,11]. Therefore, in this study, we retrospectively classified patients who underwent watchful waiting without antibiotics according to BACES severity and investigated whether the rate differs according to BACES severity.
Methods
Study design and population
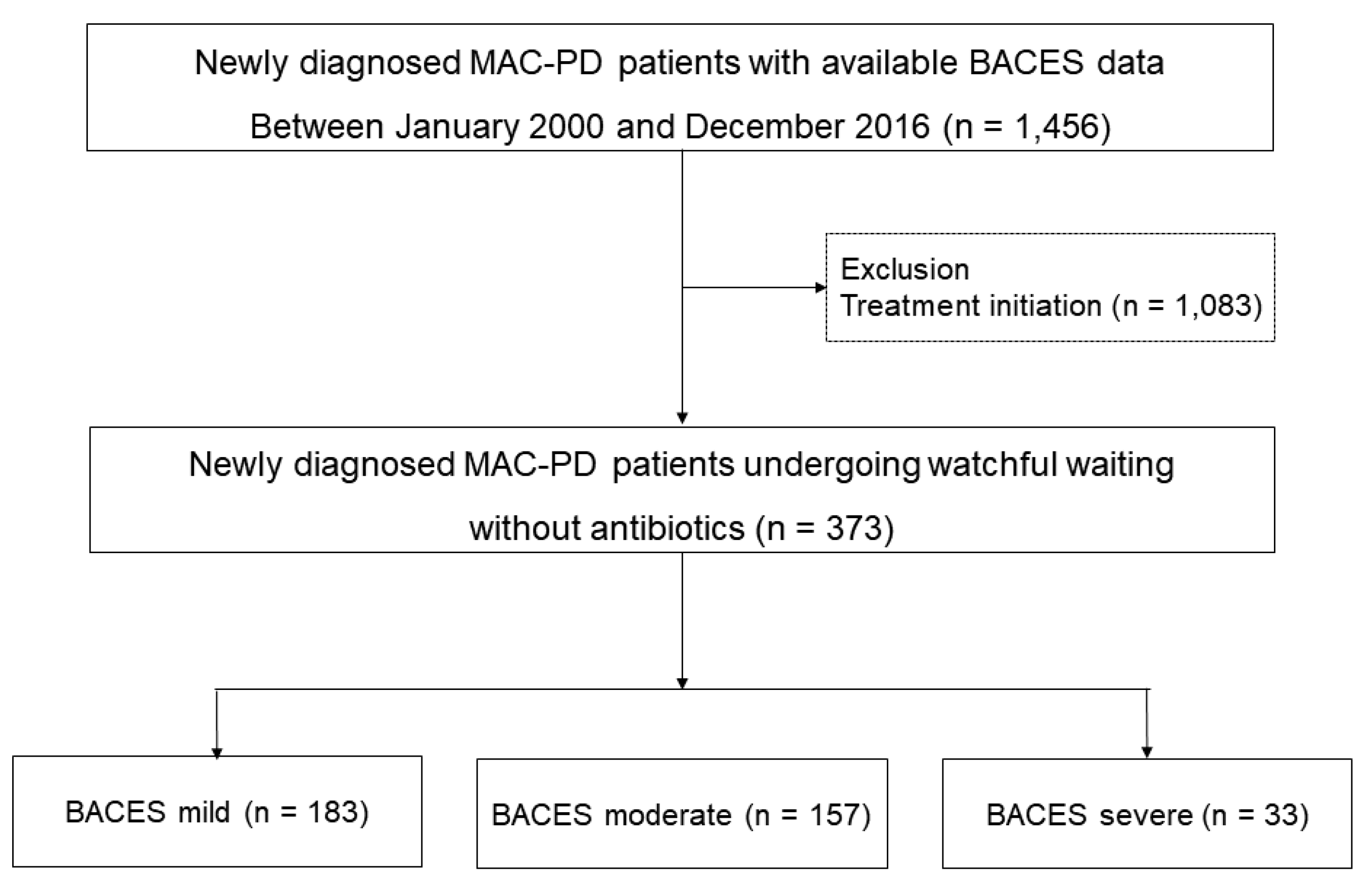
Patients who were newly diagnosed with MAC-PD between January 2002 and December 2016 were identified from the NTM Registry of Samsung Medical Center, a referral hospital in Seoul, South Korea. Data were obtained from a retrospective cohort from January 2002 to December 2007 and from an ongoing Institutional Review Board-approved prospective observational cohort beginning in January 2008 (ClinicalTrials.gov identifier: NCT00970801) [12]. During these periods, 1,456 MAC-PD patients with available BACES severity data were identified. From these, 1,083 patients who were started on antibiotic treatment were excluded. Ultimately, the analysis included 373 newly diagnosed MAC-PD patients who underwent watchful waiting without antibiotics (Figure 1). We investigated the SCC rate of MAC-PD based on the BACES severity. Data on clinical outcomes were last updated on June 2021.
Figure 1.
Study population.
Evaluation of BACES severity
MAC-PD severity was determined using the BACES, as follows: BMI <18.5 kg/m2, age ≥ 65 years, presence of a cavity, elevated ESR (men > 15 mm/h and women > 20 mm/h), and male sex. One point was given for each item, and the total score is considered an indicator of mild (0–1 point), moderate (2–3 points), or severe (4–5 points) disease [9].
Sputum and radiological examinations
Expectorated sputum was examined for patients who were not started on antibiotic therapy, usually after 3–6 months of follow-up. Acid-fast bacilli (AFB) smears and cultures were performed using standard methods. Specimens were cultured on 3% Ogawa solid medium (Shinyang, Seoul, Korea) and in a liquid broth medium in mycobacterial growth indicator tubes (Becton, Dickinson, and Co., Sparks, MD, USA). NTM species were identified using polymerase chain reaction (PCR)-restriction fragment length polymorphism analysis or reverse-blot hybridization of the rpoB gene. Species were identified via nested multiplex PCR and using a reverse-hybridization assay (AdvanSure™ Mycobacteria GenoBlot Assay; LG Life Sciences, Seoul, South Korea) of the internal transcribed spacer region beginning in June 2014 [13,14]. The radiological form of MAC-PD was classified as fibrocavitary or cavitary nodular bronchiectatic [12].
Evaluation of microbiological outcomes
We investigated the rate of SCC in MAC-PD patients undergoing observation without antibiotics during the study period. Culture conversion was defined as at least three consecutive negative sputum cultures, collected at least 4 weeks apart based on the modified NTM-NET consensus statement [15]. The time to culture conversion was defined as the time to the date of the first negative culture. For further analysis, ‘favorable outcome’ was defined to include maintaining culture conversion or having two consecutive negative sputum cultures until the last follow-up date. Time to favorable outcome was defined as the time to the date of the first negative culture in patients in whom a ‘favorable outcome’ was confirmed.
Statistical analysis
Data are presented as numbers (percentages) for categorical variables and medians (interquartile range [IQR]) for continuous variables. Continuous data were compared using the Mann–Whitney or Kruskal–Wallis test and categorical data were compared using the chi-square or Fisher’s exact test. Bonferroni’s method was used for post hoc analysis. The Kaplan–Meier method was used to estimate the cumulative conversion rates and the log-rank test was used to compare the curves. Cox proportional hazard regression analysis was used to identify factors associated with microbiological outcomes. All tests were two-sided, and a p-value < 0.05 was considered significant. All statistical analyses were performed using SPSS Statistics ver. 27 (IBM, Chicago, IL, USA).
Results
Baseline characteristics of study patients
Table 1 summarizes the baseline characteristics of the 373 MAC-PD patients who underwent watchful waiting without antibiotics at the time of diagnosis. Of these patients, 41% were ≥65 years old, 39% were male, 26% had a smoking history, and 20% had a low BMI. More than 60% had cough or sputum and 17% had hemoptysis. M. avium (61%) was the most common etiology and the nodular bronchiectatic form was present in 94% of the patients.

Table 1.
Baseline characteristics of the 373 MAC-PD patients who underwent watchful waiting without antibiotics
Table 1.
Baseline characteristics of the 373 MAC-PD patients who underwent watchful waiting without antibiotics
| Variables | Total (n = 373) |
Spontaneous negative culture conversion (n = 153) |
No culture conversion (n = 220) |
p-value |
|---|---|---|---|---|
| BACES items | ||||
| BMI < 18.5kg/m2 | 73 (20) | 30 (20) | 43 (20) | 0.988 |
| Age ≥ 65 years | 153 (41) | 47 (31) | 106 (48) | 0.001 |
| Cavity | 36 (10) | 9 (6) | 27 (12) | 0.040 |
| Elevated ESR* | 234 (63) | 96 (63) | 138 (63) | 0.997 |
| Sex, male | 145 (39) | 56 (37) | 89 (41) | 0.453 |
| Ex- or current smoker | 98 (26) | 113 (74) | 161 (73) | 0.885 |
| Underlying condition | ||||
| Previous tuberculosis | 103 (28) | 43 (28) | 60 (27) | 0.860 |
| Chronic obstructive pulmonary disease | 24 (6) | 16 (11) | 8 (4) | 0.008 |
| Chronic pulmonary aspergillosis | 2 (1) | - | - | 0.515 |
| Lung cancer | 18 (5) | 6 (4) | 12 (6) | 0.497 |
| Symptoms† | ||||
| Cough | 230 (62) | 99 (65) | 131 (60) | 0.313 |
| Sputum | 227 (61) | 94 (61) | 133 (61) | 0.848 |
| Hemoptysis | 63 (17) | 28 (18) | 35 (16) | 0.544 |
| Weight loss | 17 (5) | 4 (3) | 13 (6) | |
| Positive sputum AFB smear | 122 (33) | 40 (26) | 82 (37) | 0.024 |
| Etiology | 0.081 | |||
| M. avium | 229 (61) | 102 (67) | 127 (58) | |
| M. intracellulare | 144 (39) | 51 (33) | 93 (42) | |
| Radiological phenotype | 0.096 | |||
| Nodular bronchiectatic form | 353 (94) | 147 (96) | 206 (94) | |
| Fibrocavitary form | 20 (5) | 6 (4) | 14 (6) |
Data are presented as number (%) or median (interquartile range). BACES, BMI, age, cavity, ESR, and sex; BMI, body mass index; ESR, erythrocyte sedimentation rate; AFB, acid-fast bacilli. *Elevated ESR: > 15 mm/h in men and > 20 mm/h in women.
The median follow-up period for all study patients was 48.1 (IQR 26.4–76.4) months. Of the 373 patients, SCC occurred in 153 (41%). Patients who achieved SCC tended to be ≤ 65 years old, to lack cavities, and to have a negative AFB smear compared to those with persistent NTM positivity
Microbiological outcomes in patients without antibiotic treatment
Table 2 shows the microbiological outcomes of patients who underwent watchful waiting without antibiotic treatment. SCC occurred in 153 (41%) of the 373 patients, with a median time to conversion of 6.2 (IQR 2.7–17.7) months. There was a trend toward higher conversion rates in patients with lower BACES severity. Among mild patients, 48% achieved conversion within a median observation period of 6.0 months while only 24% of severe patients achieved conversion within a median observation period of 22.1 months. The cumulative conversion rates (as determined using the Kaplan–Meier method) showed a similar trend among patient groups based on BACES severity (Supplementary Figure S1).
Table 2.
Microbiological outcomes in patients undergoing watchful waiting without antibiotics according to BACES severity.
Table 2.
Microbiological outcomes in patients undergoing watchful waiting without antibiotics according to BACES severity.
| Watchful waiting | Total (n = 373) |
Mild (n = 183) |
Moderate (n = 157) |
Severe (n = 33) |
p-value | p-trend† |
|---|---|---|---|---|---|---|
| Spontaneous negative culture conversion | 153 (41) | 87/183 (48) | 58/157 (37) | 8/33 (24) | 0.017ac | 0.005 |
| Time to culture conversion, months | 6.2 (2.7 – 17.7) | 6.0 (2.2 – 16.1) | 5.4 (2.8 – 17.2) | 22.1 (14.2 – 88.5) | 0.008bc | 0.037 |
| Favorable outcome* | 157 (42) | 97/183 (53) | 54/157 (34) | 6/33 (18) | <0.001ac | <0.001 |
| Time to favorable outcome, months | 6.2 (2.5 – 15.8) | 6.2 (2.3 – 14.3) | 5.4 (2.5 – 14.0) | 40.3 (11.8 – 98.2) | 0.022 bc | 0.346 |
Data are presented as number (%) or median (interquartile range). BACES, BMI, age, cavity, ESR, and sex; BMI, body mass index; ESR, erythrocyte sedimentation rate. *Maintaining culture conversion or having two consecutive negative sputum cultures until the last follow-up date. †p for trend was obtained using a linear-by-linear method and Jonckheere-Terpstra test. ap <0.05 with Bonferroni correction between mild and moderate groups. bp <0.05 with Bonferroni correction between moderate and severe groups. cp <0.05 with Bonferroni correction between mild and severe groups.
There was a tendency toward a higher rate of favorable outcomes with a decrease in BACES severity. In the mild group, 53% had a favorable outcome with a median observation period of 6.2 months, while in the severe group only 18% had a favorable outcome with a median observation period of 40.3 months.
Factors associated with the microbiological outcome
We conducted multivariate analysis using Cox proportional hazard regression models to assess factors associated with microbiological outcomes in patients undergoing watchful waiting without antibiotic treatment (Table 3). We constructed models based on SCC and favorable outcomes as individual outcome criteria. Compared to mild BACES, there was a tendency for moderate and severe BACES to have a negative impact on SCC, although it was not significant. However, regarding favorable outcomes, moderate (hazard ratio 0.63; 95% confidence interval 0.44 – 0.91; p = 0.013) and severe (hazard ratio 0.37; 95% confidence interval 0.16 – 0.90; p = 0.028) BACES had a significantly negative impact on favorable outcomes compared to mild BACES.
Table 3.
Factors associated with microbiological outcome in patients undergoing watchful waiting without antibiotics (n = 373).
Table 3.
Factors associated with microbiological outcome in patients undergoing watchful waiting without antibiotics (n = 373).
| Variables | Univariable analysis | Multivariable analysis | ||
|---|---|---|---|---|
| Unadjusted HR (95% CI) |
p-value | Adjusted HR (95% CI) |
p-value | |
| Spontaneous negative culture conversion | ||||
| Ex- or current smoker | 0.85 (0.59 – 1.22) | 0.388 | 0.99 (0.66 – 1.49) | 0.971 |
| Underlying condition | ||||
| Previous pulmonary tuberculosis | 1.02 (0.72 – 1.46) | 0.901 | 1.12 (0.77 – 1.62) | 0.556 |
| Chronic obstructive pulmonary disease | 1.54 (0.91 – 2.58) | 0.106 | 1.76 (1.02 – 3.05) | 0.043 |
| Lung cancer | 0.92 (0.40 – 2.07) | 0.915 | 0.89 (0.38 – 2.08) | 0.792 |
| Etiology | ||||
| M. avium | Reference | Reference | ||
| M. intracellulare | 0.83 (0.60 – 1.17) | 0.287 | 0.83 (0.59 – 1.17) | 0.295 |
| BACES severity | ||||
| Mild | Reference | Reference | ||
| Moderate | 0.75 (0.54 – 1.05) | 0.093 | 0.74 (0.52 – 1.07) | 0.106 |
| Severe | 0.53 (0.26 – 1.10) | 0.089 | 0.49 (0.22 – 1.08) | 0.076 |
| Positive sputum AFB smear at diagnosis | 0.68 (0.47 – 0.97) | 0.034 | 0.70 (0.48 – 1.01) | 0.057 |
| Favorable outcome* | ||||
| Ex- or current smoker | 0.77 (0.53 – 1.12) | 0.167 | 1.04 (0.69 – 1.57) | 0.861 |
| Underlying condition | ||||
| Previous pulmonary tuberculosis | 0.83 (0.58 – 1.19) | 0.313 | 0.95 (0.65 – 1.38) | 0.767 |
| Chronic obstructive pulmonary disease | 1.11 (0.63 – 1.95) | 0.728 | 1.35 (0.75 – 2.44) | 0.317 |
| Lung cancer | 0.89 (0.40 – 2.02) | 0.785 | 1.01 (0.44 – 2.33) | 0.982 |
| Etiology | ||||
| M. avium | Reference | Reference | ||
| M. intracellulare | 0.67 (0.48-0.94) | 0.021 | 0.67 (0.47-0.94) | 0.020 |
| BACES severity | ||||
| Mild | Reference | Reference | ||
| Moderate | 0.63 (0.45 – 0.88) | 0.007 | 0.63 (0.44 – 0.91) | 0.013 |
| Severe | 0.37 (0.16 – 0.84) | 0.017 | 0.37 (0.16 – 0.90) | 0.028 |
| Positive sputum AFB smear | 0.79 (0.55 – 1.12) | 0.787 | 0.84 (0.59 – 1.20) | 0.333 |
MAC-PD, Mycobacterium avium complex pulmonary disease; HR, hazard ratio; CI, confidence interval; BACES, BMI, age, cavity, ESR, and sex; BMI, body mass index; ESR, erythrocyte sedimentation rate; AFB, acid-fast bacilli. *Maintaining culture conversion or having two consecutive negative sputum cultures until the last follow-up date.
Discussion
We evaluated whether the severity of BACES at the time of MAC-PD diagnosis affected the rate of SCC in MAC-PD patients who underwent watchful waiting without antibiotics. There was a tendency toward a higher SCC rate with a decrease in the severity of BACES, and multivariate analysis showed that greater BACES severity had a negative impact on favorable outcomes. Thus, our data suggest that the rate of SCC depends on the severity of MAC-PD as evaluated by BACES at the time of diagnosis. Therefore, we believe that considering BACES severity during the watchful waiting period may help when planning MAC-PD treatment strategies.
A major concern of clinicians treating MAC-PD patients is predicting the likelihood of SCC after confirming the MAC-PD diagnosis. In clinical practice, patients are eager to understand the course of their disease, yet there is no suitable predictive tool capable of assessing this accurately on an individual basis. Research has identified several factors related to SCC, such as younger age, higher BMI, and low bacterial burden (negative AFB smear) [6]. However, no single factor alone can predict it accurately. Furthermore, despite some previous attempts to analyze factors associated with SCC in a large number of patients, even multivariate analysis has failed to identify significant factors [7,8]. Here, we demonstrated that the BACES severity tool, which integrates various relevant factors, can help predict the likelihood of SCC in individual patients. Therefore, we believe that our research has clinical significance.
Because MAC-PD is a multifactorial disease, there have been numerous attempts to identify immunological, environmental, and microbiological factors associated with disease progression or spontaneous improvement [16,17,18,19]. However, there is still no validated parameter that can be used in clinical practice. In this context, a strategy based on BACES severity for classifying MAC-PD patients should help predict SCC and formulate post-diagnosis treatment strategies. In other words, patients with mild severity may expect culture conversion with long-term observation, provided there is no rapid clinical or radiological deterioration. In comparison, patients with moderate to severe severity may need more frequent follow-up to monitor clinical and radiological changes due to their lower likelihood of SCC.
BACES was originally an indicator of severity based on 5-year mortality [9]. However, according to recent data, it is also being considered a predictor of the response to antibiotic treatment [10,11]. This implies that patients with mild disease may respond well to antibiotic treatment, while increasing severity suggests a less favorable treatment response. Therefore, considering our results, we believe that the utility of BACES will increase. However, we do not consider BACES to be a perfect tool and it has its limitations. In particular, its usefulness may change as patients age. However, just as scoring systems have been developed for bronchiectasis, followed by modified scoring systems that work well in clinical practice [20,21,22], we believe that for MAC-PD, there is a need to develop and modify such practical clinical tools to serve the field better.
Our study had several limitations. First, it was retrospective and performed at a single referral center with specialized NTM-PD clinics in South Korea, so our results may not be generalizable. Second, patients who belonged to our cohort during the study but did not have information on any BACES factors were excluded. Third, we used the provisional concept of a ‘favorable outcome’ because applying concepts such as ‘microbiological cure’ or ‘clinical cure’ as presented in the NTM-NET consensus statement is challenging, because our study patients were not receiving antibiotic treatment [15]. Moreover, when patients have mild symptoms, collecting consecutive sputum samples regularly may be impractical.
In conclusion, our data suggest that the rate of SCC depends on the severity of MAC-PD as evaluated by BACES at the time of diagnosis. Lower BACES severity may be associated with SCC in MAC-PD patients. Therefore, we believe that considering BACES severity during the watchful waiting period may help to plan MAC-PD treatment strategies.
Author Contributions
B. Kim, Jin Young Yu, and B.W. Jhun conceived of and designed the study; acquired, analyzed, and interpreted the data; and wrote the manuscript. B. Kim, Jin Young Yu, and B.W. Jhun provided critical revision and approved the final version.
Funding
No funding.
Ethics Approval
Data were obtained from an ongoing prospective observational cohort (ClinicalTrials.gov identifier: NCT00970801), and the Institutional Review Board of the Samsung Medical Center approved this study (IRB no. 2008-09-016, Initial Approval Number). Written informed consent was obtained from all research participants.
Data Availability Statement
All relevant data are within the paper.
Acknowledgment
We would like to express our heartfelt gratitude and respect to Dr. Won-Jung Koh, for giving us invaluable guidance and unfailing support for NTM-PD research. Dr. Won-Jung Koh passed away in August 2019. We dedicate this work to his memory.
Competing Interests
No authors have competing interests.
Patient Consent For Publication
Not required.
References
- Lee, H.; Myung, W.; Koh, W.J.; Moon, S.M.; Jhun, B.W. Epidemiology of nontuberculous mycobacterial infection, South Korea, 2007-2016. Emerg Infect Dis 2019, 25, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007, 175, 367–416. [Google Scholar] [CrossRef]
- Daley, C.L.; Iaccarino, J.M.; Lange, C.; Cambau, E.; Wallace, R.J., Jr.; Andrejak, C.; Böttger, E.C.; Brozek, J.; Griffith, D.E.; Guglielmetti, L.; et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J 2020, 56, 2000535. [Google Scholar] [CrossRef] [PubMed]
- Haworth, C.S.; Banks, J.; Capstick, T.; Fisher, A.J.; Gorsuch, T.; Laurenson, I.F.; Leitch, A.; Loebinger, M.R.; Milburn, H.J.; Nightingale, M.; et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax 2017, 72, ii1–ii64. [Google Scholar] [CrossRef] [PubMed]
- Pasipanodya, J.G.; Ogbonna, D.; Deshpande, D.; Srivastava, S.; Gumbo, T. Meta-analyses and the evidence base for microbial outcomes in the treatment of pulmonary Mycobacterium avium-intracellulare complex disease. J Antimicrob Chemother 2017, 72, i3–i19. [Google Scholar] [CrossRef]
- Hwang, J.A.; Kim, S.; Jo, K.W.; Shim, T.S. Natural history of Mycobacterium avium complex lung disease in untreated patients with stable course. Eur Respir J 2017, 49, 1600537. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.M.; Jhun, B.W.; Baek, S.Y.; Kim, S.; Jeon, K.; Ko, R.E.; Shin, S.H.; Lee, H.; Kwon, O.J.; Huh, H.J.; et al. Long-term natural history of non-cavitary nodular bronchiectatic nontuberculous mycobacterial pulmonary disease. Respir Med 2019, 151, 1–7. [Google Scholar] [CrossRef]
- Kwon, B.S.; Lee, J.H.; Koh, Y.; Kim, W.S.; Song, J.W.; Oh, Y.M.; Lee, S.D.; Lee, S.W.; Lee, J.S.; Lim, C.M.; et al. The natural history of non-cavitary nodular bronchiectatic Mycobacterium avium complex lung disease. Respir Med 2019, 150, 45–50. [Google Scholar] [CrossRef]
- Kim, H.J.; Kwak, N.; Hong, H.; Kang, N.; Im, Y.; Jhun, B.W.; Yim, J.J. BACES score for predicting mortality in nontuberculous mycobacterial pulmonary disease. Am J Respir Crit Care Med 2021, 203, 230–236. [Google Scholar] [CrossRef]
- Kim, H.J.; Song, M.J.; Kwon, B.S.; Kim, Y.W.; Lim, S.Y.; Lee, Y.J.; Park, J.S.; Cho, Y.J.; Lee, C.T.; Lee, J.H. Usefulness of the BACES score in nontuberculous mycobacterial pulmonary disease for various clinical outcomes. Sci Rep 2023, 13, 7495. [Google Scholar] [CrossRef]
- Kim, B.G.; Jhun, B.W.; Kim, H.; Kwon, O.J. Treatment outcomes of Mycobacterium avium complex pulmonary disease according to disease severity. Sci Rep 2022, 12, 1970. [Google Scholar] [CrossRef] [PubMed]
- Jhun, B.W.; Moon, S.M.; Jeon, K.; Kwon, O.J.; Yoo, H.; Carriere, K.C.; Huh, H.J.; Lee, N.Y.; Shin, S.J.; Daley, C.L.; et al. Prognostic factors associated with long-term mortality in 1445 patients with nontuberculous mycobacterial pulmonary disease: a 15-year follow-up study. Eur Respir J 2020, 55, 1900798. [Google Scholar] [CrossRef]
- Jhun, B.W.; Kim, S.Y.; Moon, S.M.; Jeon, K.; Kwon, O.J.; Huh, H.J.; Ki, C.S.; Lee, N.Y.; Shin, S.J.; Daley, C.L.; et al. Development of macrolide resistance and reinfection in refractory Mycobacterium avium complex lung disease. Am J Respir Crit Care Med 2018, 198, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Jhun, B.W.; Kim, J.; Huh, H.J.; Lee, N.Y. Clinical characteristics and outcomes of surgically resected solitary pulmonary nodules due to nontuberculous mycobacterial Infections. J Clin Med 2019, 8, 1898. [Google Scholar] [CrossRef]
- van Ingen, J.; Aksamit, T.; Andrejak, C.; Böttger, E.C.; Cambau, E.; Daley, C.L.; Griffith, D.E.; Guglielmetti, L.; Holland, S.M.; Huitt, G.A.; et al. Treatment outcome definitions in nontuberculous mycobacterial pulmonary disease: an NTM-NET consensus statement. Eur Respir J 2018, 51, 1800170. [Google Scholar] [CrossRef]
- Pan, S.W.; Shu, C.C.; Feng, J.Y.; Wang, J.Y.; Chan, Y.J.; Yu, C.J.; Su, W.J. Microbiological persistence in patients with Mycobacterium avium complex lung disease: The predictors and the impact on radiographic progression. Clin Infect Dis 2017, 65, 927–934. [Google Scholar] [CrossRef]
- Prieto, M.D.; Jang, J.; Franciosi, A.N.; Av-Gay, Y.; Bach, H.; Tebbutt, S.J.; Quon, B.S. Whole blood RNA-seq demonstrates an increased host immune response in individuals with cystic fibrosis who develop nontuberculous mycobacterial pulmonary disease. PLoS One 2022, 17, e0278296. [Google Scholar] [CrossRef]
- Hull, R.C.; Huang, J.T.J.; Barton, A.K.; Keir, H.R.; Ellis, H.; Cookson, W.O.C.; Moffatt, M.F.; Loebinger, M.R.; Chalmers, J.D. Sputum proteomics in nontuberculous mycobacterial lung disease. Chest 2022, 161, 1180–1191. [Google Scholar] [CrossRef]
- Pan, S.W.; Su, W.J.; Chan, Y.J.; Ho, M.L.; Feng, J.Y.; Shu, C.C.; Wang, J.Y.; Wang, H.C.; Yu, C.J.; Chen, Y.M. Disease progression in patients with nontuberculous mycobacterial lung disease of nodular bronchiectatic (NB) pattern: The roles of cavitary NB and soluble programmed death protein-1. Clin Infect Dis 2022, 75, 239–247. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Goeminne, P.; Aliberti, S.; McDonnell, M.J.; Lonni, S.; Davidson, J.; Poppelwell, L.; Salih, W.; Pesci, A.; Dupont, L.J.; et al. The bronchiectasis severity index. An international derivation and validation study. Am J Respir Crit Care Med 2014, 189, 576–585. [Google Scholar] [CrossRef]
- Martínez-García, M.; de Gracia, J.; Vendrell Relat, M.; Girón, R.M.; Máiz Carro, L.; de la Rosa Carrillo, D.; Olveira, C. Multidimensional approach to non-cystic fibrosis bronchiectasis: the FACED score. Eur Respir J 2014, 43, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Garcia, M.A.; Athanazio, R.A.; Girón, R.; Máiz-Carro, L.; de la Rosa, D.; Olveira, C.; de Gracia, J.; Vendrell, M.; Prados-Sánchez, C.; Gramblicka, G.; et al. Predicting high risk of exacerbations in bronchiectasis: the E-FACED score. Int J Chron Obstruct Pulmon Dis 2017, 12, 275–284. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



