
Submitted:
30 October 2023
Posted:
31 October 2023
You are already at the latest version
Abstract
Aronia berries contain antioxidants that may have health promoting properties e.g., demonstrated positive effects on hypertension and dyslipidemia. There is a close link between cardiovascular diseases and hypertension and dyslipidemia, and cardiovascular events are the leading cause of death among subjects with T2D. Thus, we investigated the effect of 8 weeks supplementation with fermented aronia extract (FAE), non-fermented aronia extract (AE) and placebo on cardiovascular risk factors. The extracts were incorporated into snack bars containing 34 g (37%) aronia extract, or 17 g (21%) wheat bran for placebo, as well as raisins and coconut oil. The study was randomized and blinded with a triple-cross-over design. We examined the effects of aronia extracts on blood pressure, adiponectin and high-sensitive C-reactive protein and found no effects. After supplementation with placebo, there were significantly higher total-cholesterol, LDL-cholesterol, and HDL-cholesterol, with the placebo group showing significantly higher increases in total-cholesterol and LDL-cholesterol than the FAE group. Furthermore, we observed an increase in HDL-cholesterol in the AE group and an increase in triglyceride in the FAE group. Thus, we assume that raisins may have increased the participants’ cholesterol levels, however, with both AE and FAE having the potential to prevent this increase.
Keywords:
Aronia melanocarpa
; type 2 diabetes
; dietary supplement
; antioxidants
; polyphenols
; anthocyanins
; randomized controlled trial
1. Introduction
The aim of this study was to compare the effects of aronia extract, fermented aronia extract and placebo on cardiovascular risk parameters in subjects with type 2 diabetes (T2D). T2D represents a major health burden [1,2] in particular driven by the high occurrence of cardiovascular events associated with T2D [3]. Around 65% of those with T2D die from a cardiovascular event, which makes it obvious that there is a need for improved treatment [3]. It has been established that there is a close link between the occurrence of cardiovascular events and the presence of dyslipidemia and hypertension in T2D [3].
Aronia melanocarpa is a small shrub that produces small, nearly black berries [4]. The berry has a very high content of antioxidants, which has led to exploration of their clinical application possibilities [5,6,7]. The primary antioxidants in aronia are anthocyanins, proanthocyanidins and phenolic acids [4,5]. Despite conflicting evidence, several in vitro studies, in vivo animal studies and human studies have shown positive outcomes after supplementation with aronia on blood glucose and lipid levels [8]. Against dyslipidemia, which involves increased triglyceride and LDL-cholesterol and decreased HDL-cholesterol, statins effectively decrease LDL-cholesterol and improves triglyceride and HDL-cholesterol levels to some degree [9]. One of the most common side effects is myalgia, which is highly likely to be the main reason many individuals choose to discontinue statin treatment [10,11]. In contrast to statins, antihypertensive agents are better tolerated with higher compliance [12,13,14]. Nevertheless, a study by Naruszewicz et al. reported a reduction in systolic and diastolic blood pressure of 11 and 7 mmHg, respectively, in patients with previous myocardial infarction after supplementation with aronia for six weeks even though half of the patients were treated with ACE inhibitors [15]. Aronia supplementation may also have positive effects in subjects with previous myocardial infarction and have implications for blood pressure improvements. Aronia berries have a high content of polyphenols that may explain the anti-inflammatory and antioxidant properties [16,17]. Since hypertension is associated with by oxidative stress and low-grade inflammation, a supplementation with aronia may have a positive impact on blood pressure [17]. Thus, aronia supplementation may be a natural and well-tolerated, cost-effective alternative to statin treatment and adjunct to antihypertensive agents.
However, in comparison to many other polyphenols, those specific to aronia berries have low bioavailability and limited absorption from the gastrointestinal tract [18]. For some compounds, less than 1% is absorbed and detected in the blood after consumption [18,19,20]. The low bioavailability may reduce its usability as an antioxidant supplement. However, the bioavailability of aronia may be improved after fermentation, since the process reduces the compounds to simpler structures with higher bioavailability [21,22]. Most human studies that examine the effects of aronia on various diseases involve non-blinded investigations without a control group. In the present study, we looked at the effects on cardiovascular risk factors of eight weeks supplementation with aronia, both fermented and non-fermented, in individuals with T2D.
We hypothesized that fermented aronia extract (FAE) improves glycemia and lipidemia in T2D more efficiently than both non-fermented aronia extract (AE) and placebo. Our results on glycemia have been published previously, and this article reports impact on blood pressure, blood lipids, adiponectin and high-sensitive C-reactive protein (hs-CRP).
2. Materials and Methods
2.1. Test products
Study design and test product composition have been described in detail previously [23]. All test products were provided as snack bars twice daily and contained 55 g of raisins and 3 g of coconut oil per day. In addition, the test products contained 34 g of either fermented aronia extract or non-fermented aronia extract and the placebo contained 17 g of wheat bran together with 5 g water and colorants. Aronia extracts were made from berries that had been harvested in September 2020 and stored frozen. Snack bars were produced throughout the study to ensure durability and high quality. Each time a new batch of snack bars were produced, the aronia berries were slowly thawed and cold-pressed. Then, the pulp was used either unfermented directly in the snack bars or fermented before being used in the snack bars. The dry matter percentage in the pulp was around 40%. Lastly, the aronia extracts e.g., aronia pulp and fermented aronia pulp, were blended with the remaining ingredients. All snack bars including placebo was kindly provided by Elkaerholm (Egtved, Denmark).
The group receiving fermented aronia extract will be referred to as FAE and the group receiving non-fermented aronia extract as AE. The aronia extracts were based on aronia berry pulp. FAE and AE groups were supplemented with snack bars that administered approximately 893 mg or 533 mg anthocyanins, respectively, per day. Measurements on anthocyanin content were made by Elkaerholm (Egtved, Denmark) prior to the study, and since anthocyanins decay over time, the amount of provided anthocyanins might have decreased towards the end of the study. In order to minimize the decay, the supplements were stored in the dark at -18°C. The nutritional composition it outlined in Table 1.
2.2. Study design and participants
This study was carried out at Department of Endocrinology and Internal Medicine, Aarhus University Hospital, Denmark, spanning the period from December 2020 to April 2022. The study adhered to the principles outlined in the Declaration of Helsinki and received approval from The Central Denmark Region Committees on Health Research Ethics (Journal no. 1-10-72-102-19). Furthermore, the trial was registered on ClinicalTrials.gov (NCT04647175).
Advertisements in local newspapers, a dedicated recruitment website ("forsoegsperson.dk"), and various social media platforms were used to get in contact with possible study candidates. Hereafter, candidates were given all study information orally and written along with at least one week for consideration. Interested candidates were screened for eligibility, and if they fulfilled the study criteria, a written consent was obtained. This consent could be withdrawn throughout the entire study. Participants could be included if they had a diagnosis of T2D, an age of 30 to 80 years, fasting blood glucose ≤12 mmol/l, and HbA1c > 6.1% and <10% (>43 and < 86 mmol/mol, respectively) if participants were in medical diabetes treatment OR HbA1c > 6.5% and <10% (>48 and < 86 mmol/mol, respectively) if participants were treated with lifestyle only. Participants were excluded if they had changes in diabetes medication within the last 3 months, serious comorbidities, including cardiovascular-, neurological-, psychological- and/or renal diseases, alcohol- or substance abuse, and were pregnant or had planned pregnancy.
The study had a triple-blinded, triple-crossover design as illustrated in Figure 1. Each participant received all three interventions, e.g., FAE, AE and placebo twice daily for eight weeks each, with no less than 3 weeks washout in between. To further reduce carry over effects in our analysis we performed a random sequence generation in Excel and randomized the participants to the order of the interventions using blocks of the six possible orders. Consumption of aronia products aside from the supplements was prohibited from three weeks before the trial and during the trial.
Pre and post each supplementation period, we assessed 24-hour ambulatory blood pressure and took fasting blood samples to quantify lipids, adiponectin and hs-CRP levels.
2.3. 24-hour ambulatory blood pressure monitoring
24-hour ambulatory blood pressure monitoring was conducted using ambulatory blood pressure monitors (Spacelabs Medical). The monitors were calibrated to measure blood pressure at 30-minute intervals from 7:00 AM to 11:00 PM and at 60-minute intervals from 11:00 PM to 7:00 AM. Participants recorded wake-up and bed-times. Using this information, computer software (Sentinel) calculated systolic and diastolic blood pressure measurements for the entire monitoring period, as well as separately for the sleeping and waking periods. One participant that completed the trial did not complete the blood pressure monitoring due to experiencing pain during measurements.
2.4. Blood analyses
Blood samples were collected following an eight-hour fasting period and promptly underwent centrifugation at 4°C and 3989 RPM for 10 minutes. The resulting plasma samples were preserved at -80°C until the end of the study, where samples from all participants were analysed together.
2.4.1. Hs-CRP and adiponectin
Hs-CRP and adiponectin concentrations were measured using non-competitive, time-resolved immunoflouremetric assays. The method for determination of hs-CRP has been described previously by Reinhard et al. [24]. Measurement of adiponectin was performed like that of hs-CRP, but with different antibodies (#MAB10651 and #BAM1065, R&D Systems). In group F, one post-treatment value was found to be below the lower level of detection both in regard to hs-CRP and adiponectin. Only samples from participants completing the study were analysed.
2.4.2. Lipids
The Department of Clinical Biochemistry at Aarhus University Hospital, Denmark (DS/EN ISO 15189:2013 approved) measured HDL-cholesterol, total-cholesterol and triglyceride. They also provided LDL-cholesterol concentrations which were calculated using Friedewalds formula which is considered the gold standard for determining LDL-cholesterol levels [25]. In two samples, triglyceride concentrations were >4 mmol/l in which case the LDL-cholesterol concentration could not be calculated.
2.5. Power calculation
Based on a power calculation, which has been described previously [23], we calculated that statistical power could be obtained with 18 participants completing the trial. However, due to a rather large dropout rate early in the study, we chose to recruit 36 participants.
2.6. Statistics
Statistical analysis was performed in collaboration with a medical statistician that provided the code for fitting of a linear mixed effects model in Rstudio (Rstudio, Package lme4). As fixed effects, we included treatment order (six possible orders), period (first, middle, last), treatment (FAE, AE, placebo) and time (pre, post) along with the interaction between treatment and time. As random effects we included record id and record id within period. Standard normality tests of residuals were conducted, including quantile-quantile plots and histograms along with plots of residuals versus fitted values. We used the Rstudio package emmeans to compute estimated marginal means from the mixed model. The estimated marginal means, we will simply refer to as “means” throughout this article. We also compared mean differences (Δ-mean) between the three supplementations using the package emmeans. For normally distributed data, we present mean or Δ-mean ± standard error. The data on hs-CRP was not normally distributed; therefore, we compared ratios instead of Δ-means. To clarify, a ratio of 1.10 signifies a 10% increase from pre to post, whereas a value of 0.83 denotes a 17% decrease.
If values were below lower level of detection in the previously described essays, we imputed these values as half of the lower limit of detection for the respective essays. We assessed the baseline data for normality, and for normally distributed data, we will report the results as mean ± standard deviation (SD). Non-normally distributed data will be reported as the median along with the interquartile range (IQR).
3. Results
3.1. Baseline characteristics
As depicted in Figure 2, we assessed 44 participants for eligibility, and we included 36 participants of which 23 completed the study. We have previously reported the baseline values (see Table 2) [23]. For completers of the trial, 15 were men and 8 were women, mean body mass index was 82.0 ± 16.2 kg/m2 and mean age was 67.6 ± 5.5 years [23]. For non-completers, 21 were men and 15 were women, mean body mass index was 28.6 (24.3-32.0) kg/m2 and mean age was 66.9 ± 6.0 years. The participants continued with their regular medications during the course of the trial (see Table 3).
3.2. 24-hour ambulatory blood pressure monitoring
Results were obtained before and after each intervention period. We analysed 24-hour measurements as well as measurements from awake-and asleep-periods individually. However, no intra- or inter group differences were found regarding the 24-hour measurements (Table 4) or for awake- or asleep-periods analysed individually (data not shown).
3.3. Blood analyses
Overall, we observed no effects on hs-CRP or adiponectin. However, there was a trend towards improvements upon supplementation with AE with a 17% decrease in hs-CRP and -0.59 ± 0.26 mg/l decrease in adiponectin.
Regarding lipids, intra-group analysis revealed several increases dispersed across all groups after supplementation, an overview is provided in Figure 2. Firstly, HDL-cholesterol was increased from 1.14 ± 0.05 to 1.22 ± 0.05 mmol/l (p=0.03) after supplementation with AE. Secondly, triglyceride was increased from 1.58 ± 0.13 to 1.81 ± 0.13 mmol/l (p=0.03) after supplementation with FAE. Lastly, HDL-cholesterol was increased from 1.12 ± 0.05 to 1.20 ± 0.05 mmol/l (p=0.02), LDL-cholesterol was increased from 1.82 ± 0.11 to 2.02 ± 0.12 mmol/l (p=0.01) and total-cholesterol was increased from 3.67 ± 0.13 to 4.03 ± 0.14 mmol/l (p=0.0003) in the placebo group. Regarding inter-group differences, ΔLDL-cholesterol and Δtotal-cholesterol were significantly higher in the placebo group compared to in the AE group. Specifically, ΔLDL-cholesterol was -0.09 ± 0.07 mmol/l in the AE group and 0.20 ± 0.08 mmol/l in the placebo group (p=0.04) and Δtotal-cholesterol was 0.002 ± 0.08 mmol/l in the AE group versus 0.36 ± 0.09 mmol/l in the placebo group (p=0.01). However, it should be noted that differences within groups were small with changes of maximum 0.1 mmol/l after supplementation with AE and FEA, except for triglyceride, which increased 0.23 ± 0.08 mmol/l in the AE group. Increases were higher after supplementation with placebo with increases in triglyceride and LDL-cholesterol of 0.2 mmol/l and in total-cholesterol of 0.4 mmol/l.
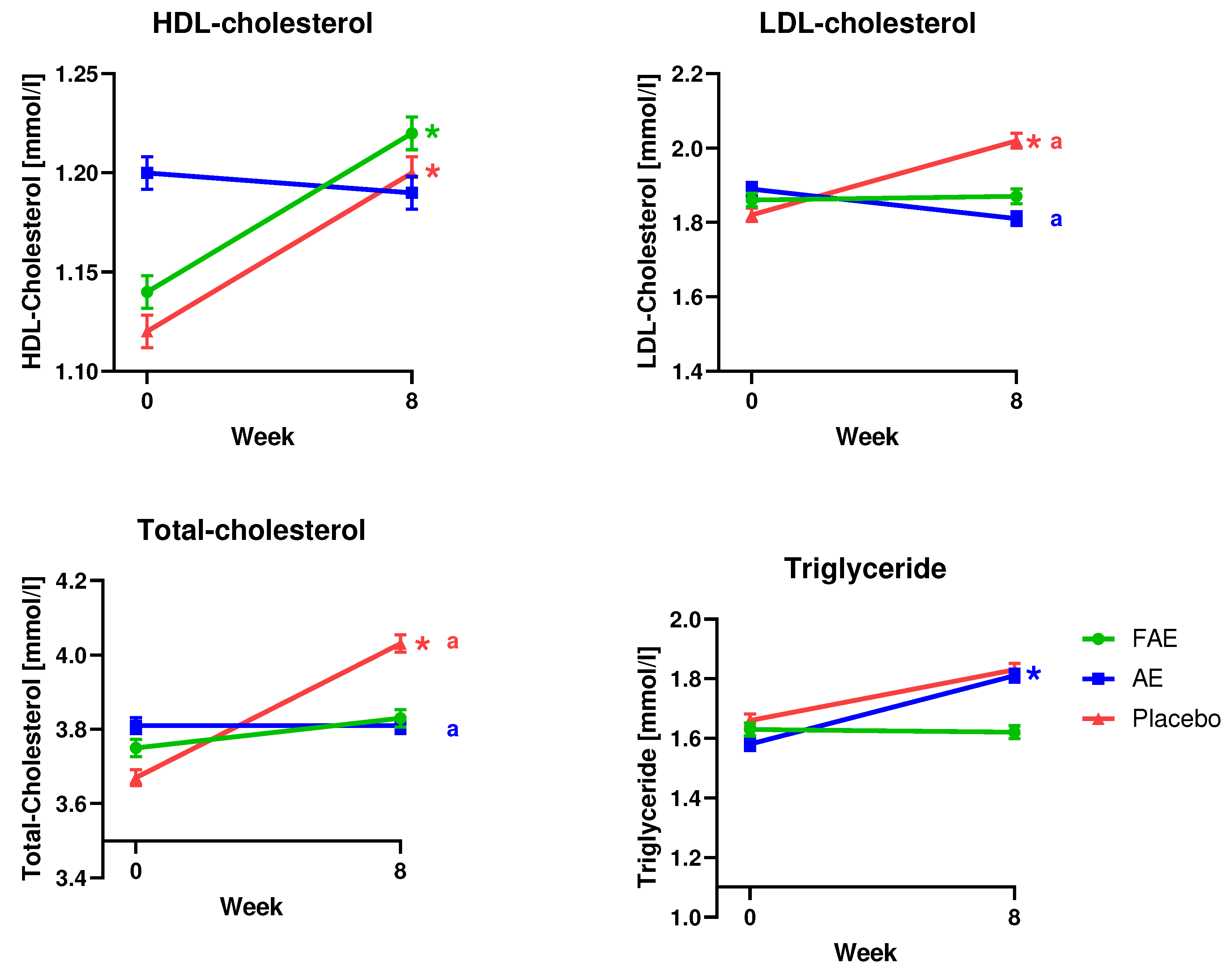
Figure 3.
Mean pre and post values for fasting levels of LDL-cholesterol, HDL-cholesterol, total-cholesterol and triglyceride. Data are presented mean ± standard error. * indicates a significant difference between pre and post values. a indicates significant differences between Δ-means. Abbreviations: FAE: Fermented aronia extract, AE: Aronia extract, HDL-cholesterol: High-density lipoprotein cholesterol, LDL-cholesterol: Low-density lipoprotein cholesterol.
Figure 3.
Mean pre and post values for fasting levels of LDL-cholesterol, HDL-cholesterol, total-cholesterol and triglyceride. Data are presented mean ± standard error. * indicates a significant difference between pre and post values. a indicates significant differences between Δ-means. Abbreviations: FAE: Fermented aronia extract, AE: Aronia extract, HDL-cholesterol: High-density lipoprotein cholesterol, LDL-cholesterol: Low-density lipoprotein cholesterol.
4. Discussion
In this study, we investigated the effects on cardiovascular risk factors of eight weeks supplementation with aronia extract, fermented aronia extract and placebo, respectively, in subjects with T2D. After 8 weeks supplementation with aronia, we did not observe any significant differences in blood pressure, adiponectin or hs-CRP.
Regarding blood pressure, our results are in line with findings from Simeonov et al. who did not find any significant effect on blood pressure in individuals with T2D after a 3-months non-blinded, non-controlled supplementation regimen [26]. Nevertheless, there was a non-significant reduction in systolic blood pressure from 144 to 134 mmHg and in diastolic blood pressure from 91 to 84 mmHg [26]. However, in line with our results, Milutinovic et al. also observed nearly unchanged blood pressure after three months supplementation with aronia juice [27]. It should be noted that their study was non-blinded and non-controlled, and they only provided 259 mg anthocyanins per day [27]. Furthermore, in a previous meta-analysis, we assessed the effect of aronia in individuals with increased cardiovascular risk, and we found no effect of aronia either [5].
No changes were observed for hs-CRP. However, baseline values were generally low with values below 1 mg/l, and a value below 10 mg/l indicates a low cardiovascular risk [28]. Thus, the baseline hs-CRP values may be too low for us to induce any improvements. In line with our results, Milutinovic et al. found no effect of aronia supplementation on hs-CRP in individuals with T2D either [27]. To our knowledge, no studies have investigated the impact of aronia on adiponectin in individuals with T2D. However, the effect has been studied in obese individuals, which had a mean baseline adiponectin level of 7.98 mg/l, which is comparable to our study participants’ values [29]. They observed a significant increase in adiponectin after two months supplementation with aronia, which is in in contrast to our results. However, the study was non-blinded, and the study population was small (n=10) [29]. Consequently, more studies are needed to verify the findings.
In accordance to European Society of Cardiology, it is recommended that individuals with T2D and high CVD risk are more closely monitored in regards to lipid levels than healthy people with LDL-cholesterol levels below 1.8 mmol/l [30]. We observed baseline values below or very close to the recommended in all intervention groups, which indicates that the participants were well regulated at baseline. However, there was significant increases of 0.20 ± 0.08 mmol/l in LDL-cholesterol from 1.82 ± 0.11 to 2.02 ± 0.12 mmol/l (p=0.01) after supplementation with placebo. This increase was accompanied by an increase in total-cholesterol from 3.67 ± 0.13 to 4.03 ± 0.14 mmol/l (p=0.0003). For both LDL- and total-cholesterol, the Δ-mean in the placebo group was significantly higher than in the AE group, where the levels were nearly unchanged.
In accordance with to European Society of Cardiology, it is recommended that fasting triglyceride levels are maintained below 2.3 mmol/l [30]. Thus, the participants had well-regulated levels at baseline. Unfortunately, we observed an unexpected increase in triglycerides of 0.23 ± 0.08 from 1.58 ± 0.13 to 1.81 ± 0.13 (p=0.03) after supplementation with FAE. Likewise, there was also a non-significant increase of 0.17 ± 0.09 mmol/l in triglyceride from 1.66 ± 0.13 to 1.83 ± 0.13 mmol/l after supplementation with placebo. Nevertheless, the levels remained within the recommended range and the increase regarded as not clinically relevant. Along with these increases, we also observed a 0.08 ± 0.03 mmol/l increase in HDL-cholesterol from 1.66 ± 0.13 to 1.83 ± 0.13 (p=0.03) after supplementation with AE and a 0.08 ± 0.03 mmol/l increase from 1.12 ± 0.05 to 1.2 ± 0.05 mmol/l after supplementation with placebo. Concerning HDL-cholesterol, American diabetes association recommends to maintain levels above 1.1 mmol/l for men and 1.2 mmol/l for women, and increasing the level is associated with decreased risk of cardiovascular events [31]. Thus, at baseline, the levels were already close to recommended levels, especially in the FAE intervention group, where mean baseline was 1.2 ± 0.05 mmol/l, which was non-significantly higher than baseline for AE and placebo. It is inexplicable why HDL-cholesterol levels increase after supplementation with FAE and placebo, but not after supplementation with AE. However, it might be because the AE group already had a mean HDL-cholesterol concentration of 1.2 mmol/l. Considering our findings on lipid concentrations, it is worth emphasizing that around 65% of the participants were receiving statin treatment during the study, which potentially mitigates the effects and reduce the effect of the supplements.
Since placebo, FAE and AE are similar in nutritional composition, but all contain rather large amounts of sugar, it is interesting that lipid levels change less than 0.1 mmol/l after supplementation with FAE and AE, with the exception of triglyceride, which was increased 0.23 ± 0.08 mmol/l after AE supplementation. This could suggest that FAE and AE might have protective effects by preventing rises in lipid levels after consumption of an unhealthy amount of sugars for eight weeks. On the other hand, it remains puzzling why triglyceride would increase after supplementation with FAE. However, an increased consumption of saturated fatty acids and a decreased consumption of polyunsaturated fatty acid and carbohydrates have been connected to lower triglyceride levels [32]. Thus, even though the nutritional composition is very similar in the test products, the slightly different composition of FAE in comparison to especially placebo might account for the increase. In summary, FAE provided a modestly higher amount of carbohydrates and saturated fatty acids as well as a lower amount of polyunsaturated fatty acids in comparison to placebo. Likewise, FAE also provides more carbohydrates than AE, however, they have the same concentration of polyunsaturated fatty acids. Furthermore, it has previously been reported that raisins have a low glycemic index, and that 50 g of raisins can be considered a healthy snack for individuals with T2D [33,34]. However, we do not know the glycemic index of our supplements, and an analysis of each test product’s glycemic index could give important information. It can’t be ruled out that the glycemic index of our test products is higher than expected, and diets containing food elements with a high glycemic index may have unfavourable effects on blood lipids with decreased HDL-cholesterol and increased triglyceride levels [35].
Even though the supplements have small variations in nutritional composition, it is unlikely that this alone could account for the observed differences. It is possible that the high content of anthocyanins, in AE and FAE, prevent increases in blood lipids as those observed after supplementation with placebo. In line with this postulation, a meta-analysis have reported that supplementation with anthocyanins have a positive effect in individuals with lipidemia [36,37]. If we assume that no change in blood lipids reflects a lipid lowering effect of aronia, our results are partly corroborated by Simeonov et al. and Milutinuvic et al. that found improvements in total-cholesterol and LDL-cholesterol, respectively, after aronia supplementation in subjects with T2D [26,27]. In opposition to our findings, Simeonov et al. found an improvement in triglyceride concentration [26] and Milutinovic et al. did not observe any effect on HDL-cholesterol, total-cholesterol or triglycerides [27]. Furthermore, our previously published meta-analysis on the effect of aronia in subjects at increased cardiometabolic risk did not report any effects of aronia on lipid levels [5]. In contrast, another meta-analysis examined the effect of aronia without any requirements regarding health status of the subjects and found increases in HDL-cholesterol and decreases in total-cholesterol and LDL-cholesterol after administration of aronia [7]. Thus, there are indications that aronia could have beneficial effects on lipid levels, but as evidence is conflicting, more studies are warranted to draw any conclusion.
In conclusion, aronia extracts, both fermented and non-fermented could contribute to improvements in lipid profiles in subjects with T2D, but more high-quality studies are needed to confirm our findings. Apparently, aronia does not affect blood pressure, adiponectin or hs-CRP.
Author Contributions
Conceptualization, C.C., P.B.J., K.H. and S.G.; validation, C.C., P.B.J., K.H. and S.G.; formal analysis, C.C.; investigation, C.C.; data curation, C.C.; writing—original draft preparation, C.C.; writing—review and editing, P.B.J., K.H. and S.G.; supervision, P.B.J., K.H. and S.G.; project administration, C.C., P.B.J., K.H. and S.G.; funding acquisition, C.C., P.B.J., K.H. and S.G.. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Innovation Fund Denmark, grant number 9065-00126B; Danish Diabetes Academy, grant number NNF17SA0031406; Ekhagastiftelsen, grant number 2019-04; Helsefonden, grant number 19-B-0179. Future Food Innovation; Aase og Ejner Danielsens Fond, grant number 18-10-0477; A.P. Møller Fonden, 19-L-0118; Frode V: Nyegaards Fond.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of The Central Denmark Region Committees on Health Research Ethics (Journal no. 1-10-72-102-19, 12/08/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results can obtained by contacting the corresponding author.
Acknowledgments
We thank Elkaerholm (Egtved, Denmark) for supporting us with aronia extracts and placebo.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Federation, I.D. IDF Diabetes Atlas, 10th edn. Available online: https://www.diabetesatlas.org (accessed on April).
- (WHO), W.h.o. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on.
- Wang, C.C.L.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Clinical Update: Cardiovascular Disease in Diabetes Mellitus. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef]
- Kulling, S.E.; Rawel, H.M. Chokeberry (Aronia melanocarpa) - A review on the characteristic components and potential health effects. Planta medica 2008, 74, 1625–1634. [Google Scholar] [CrossRef]
- Christiansen, C.B.; Mellbye, F.B.; Hermansen, K.; Jeppesen, P.B.; Gregersen, S. Effects of Aronia melanocarpa on Cardiometabolic Diseases: A Systematic Review of Quasi-Design Studies and Randomized Controlled Trials. Rev Diabet Stud 2022, 18, 76–92. [Google Scholar] [CrossRef]
- Hawkins, J.; Hires, C.; Baker, C.; Keenan, L.; Bush, M. Daily supplementation with aronia melanocarpa (chokeberry) reduces blood pressure and cholesterol: a meta analysis of controlled clinical trials. Journal of Dietary Supplements 2021, 18, 517–530. [Google Scholar] [CrossRef]
- Rahmani, J.; Clark, C.; Kord Varkaneh, H.; Lakiang, T.; Vasanthan, L.T.; Onyeche, V.; Mousavi, S.M.; Zhang, Y. The effect of Aronia consumption on lipid profile, blood pressure, and biomarkers of inflammation: A systematic review and meta-analysis of randomized controlled trials. Phytotherapy research: PTR 2019, 33, 1981–1990. [Google Scholar] [CrossRef]
- Banjari, I.; Misir, A.; Šavikin, K.; Jokić, S.; Molnar, M.; De Zoysa, H.K.S.; Waisundara, V.Y. Antidiabetic Effects of Aronia melanocarpa and Its Other Therapeutic Properties. Frontiers in nutrition 2017, 4, 53–53. [Google Scholar] [CrossRef] [PubMed]
- Barter, P.J.; Brandrup-Wognsen, G.; Palmer, M.K.; Nicholls, S.J. Effect of statins on HDL-C: a complex process unrelated to changes in LDL-C: analysis of the VOYAGER Database. Journal of Lipid Research 2010, 51, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.K.; Wang, T.Y.; Li, S.; Robinson, J.G.; Roger, V.L.; Goldberg, A.C.; Virani, S.S.; Louie, M.J.; Lee, L.V.; Peterson, E.D. Patient-reported reasons for declining or discontinuing statin therapy: insights from the PALM registry. Journal of the American Heart Association 2019, 8, e011765. [Google Scholar] [CrossRef] [PubMed]
- Ramkumar, S.; Raghunath, A.; Raghunath, S. Statin Therapy: Review of Safety and Potential Side Effects. Acta Cardiol Sin 2016, 32, 631–639. [Google Scholar] [CrossRef]
- Zanchetti, A.; Grassi, G.; Mancia, G. When should antihypertensive drug treatment be initiated and to what levels should systolic blood pressure be lowered? A critical reappraisal. Journal of hypertension 2009, 27, 923–934. [Google Scholar] [CrossRef] [PubMed]
- ANDERSSON, O.K.; NELDAM, S. The antihypertensive effect and tolerability of candesartan cilexetil, a new generation angiotensin II antagonist, in comparison with losartan. Blood Pressure 1998, 7, 53–59. [Google Scholar]
- Barrios, V.; Escobar, C.; Navarro, A.; Barrios, L.; Navarro-Cid, J.; Calderón, A.; INVESTIGATORS, L. Lercanidipine is an effective and well tolerated antihypertensive drug regardless the cardiovascular risk profile: The LAURA study. International journal of clinical practice 2006, 60, 1364–1370. [Google Scholar] [CrossRef]
- Naruszewicz, M.; Laniewska, I.; Millo, B.; Dłuzniewski, M. Combination therapy of statin with flavonoids rich extract from chokeberry fruits enhanced reduction in cardiovascular risk markers in patients after myocardial infraction (MI). Atherosclerosis 2007, 194, e179–184. [Google Scholar] [CrossRef]
- Banach, M.; Wiloch, M.; Zawada, K.; Cyplik, W.; Kujawski, W. Evaluation of Antioxidant and Anti-Inflammatory Activity of Anthocyanin-Rich Water-Soluble Aronia Dry Extracts. Molecules 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Valentina, B.; Minodora, A.; Antal, D.; Florina, A.; Ioana Zinuca, P.; Cristina, D.; Codruta, S.; Roxana, F.; Felicia, A.; Corina, D. Cardioprotective Effects of Cultivated Black Chokeberries (Aronia spp.): Traditional Uses, Phytochemistry and Therapeutic Effects. In Bioactive Compounds in Nutraceutical and Functional Food for Good Human Health; Kavita, S., Kanchan, M., Kula Kamal, S., Corina, D., Eds.; IntechOpen: Rijeka, 2020; p. Ch. 9. [Google Scholar]
- Denev, P.N.; Kratchanov, C.G.; Ciz, M.; Lojek, A.; Kratchanova, M.G. Bioavailability and Antioxidant Activity of Black Chokeberry (Aronia melanocarpa) Polyphenols: in vitro and in vivo Evidences and Possible Mechanisms of Action: A Review. Comprehensive Reviews in Food Science and Food Safety 2012, 11, 471–489. [Google Scholar] [CrossRef]
- Kamiloglu, S.; Capanoglu, E.; Grootaert, C.; Van Camp, J. Anthocyanin Absorption and Metabolism by Human Intestinal Caco-2 Cells--A Review. Int J Mol Sci 2015, 16, 21555–21574. [Google Scholar] [CrossRef] [PubMed]
- Wiczkowski, W.; Romaszko, E.; Piskula, M.K. Bioavailability of cyanidin glycosides from natural chokeberry (Aronia melanocarpa) juice with dietary-relevant dose of anthocyanins in humans. Journal of agricultural and food chemistry 2010, 58, 12130–12136. [Google Scholar] [CrossRef] [PubMed]
- Semaming, Y.; Pannengpetch, P.; Chattipakorn, S.C.; Chattipakorn, N. Pharmacological properties of protocatechuic Acid and its potential roles as complementary medicine. Evid Based Complement Alternat Med 2015, 2015, 593902. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; He, Y.; Luo, C.; Feng, B.; Ran, F.; Xu, H.; Ci, Z.; Xu, R.; Han, L.; Zhang, D. New progress in the pharmacology of protocatechuic acid: A compound ingested in daily foods and herbs frequently and heavily. Pharmacological Research 2020, 161, 105109. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, C.B.; Jeppesen, P.B.; Hermansen, K.; Gregersen, S. Aronia in the Type 2 Diabetes Treatment Regimen. Nutrients 2023, 15, 4188. [Google Scholar] [CrossRef]
- Reinhard, M.; Frystyk, J.; Jespersen, B.; Bjerre, M.; Christiansen, J.S.; Flyvbjerg, A.; Ivarsen, P. Effect of hyperinsulinemia during hemodialysis on the insulin-like growth factor system and inflammatory biomarkers: a randomized open-label crossover study. BMC Nephrology 2013, 14, 80. [Google Scholar] [CrossRef] [PubMed]
- Knopfholz, J.; Disserol, C.C.; Pierin, A.J.; Schirr, F.L.; Streisky, L.; Takito, L.L.; Massucheto Ledesma, P.; Faria-Neto, J.R.; Olandoski, M.; da Cunha, C.L.; et al. Validation of the friedewald formula in patients with metabolic syndrome. Cholesterol 2014, 2014, 261878. [Google Scholar] [CrossRef] [PubMed]
- Simeonov, S.B.; Botushanov, N.P.; Karahanian, E.B.; Pavlova, M.B.; Husianitis, H.K.; Troev, D.M. Effects of Aronia melanocarpa juice as part of the dietary regimen in patients with diabetes mellitus. Folia medica 2002, 44, 20–23. [Google Scholar]
- Milutinović, M.; Radovanović, R.V.; Šavikin, K.; Radenković, S.; Arvandi, M.; Pešić, M.; Kostić, M.; Miladinović, B.; Branković, S.; Kitić, D. Chokeberry juice supplementation in type 2 diabetic patients-impact on health status. 2019. [CrossRef]
- Cozlea, D.L.; Farcas, D.M.; Nagy, A.; Keresztesi, A.A.; Tifrea, R.; Cozlea, L.; Carașca, E. The impact of C reactive protein on global cardiovascular risk on patients with coronary artery disease. Curr Health Sci J 2013, 39, 225–231. [Google Scholar]
- Boncheva, M.; Turnovska, T. Administration of bioflavonoides improves plasma levels of adipocyte hormones. Acta Medica Bulgarica 2014, 41, 5–11. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Association, A.D. Standards of Medical Care in Diabetes. Diabetes Care 2005, 28, s4–s36. [Google Scholar] [CrossRef]
- Lopez-Alvarenga, J.C.; Ebbesson, S.O.; Ebbesson, L.O.; Tejero, M.E.; Voruganti, V.S.; Comuzzie, A.G. Polyunsaturated fatty acids effect on serum triglycerides concentration in the presence of metabolic syndrome components. The Alaska-Siberia Project. Metabolism 2010, 59, 86–92. [Google Scholar] [CrossRef]
- Esfahani, A.; Lam, J.; Kendall, C.W. Acute effects of raisin consumption on glucose and insulin reponses in healthy individuals. J Nutr Sci 2014, 3, e1. [Google Scholar] [CrossRef]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International Tables of Glycemic Index and Glycemic Load Values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef]
- Denova-Gutiérrez, E.; Huitrón-Bravo, G.; Talavera, J.O.; Castañón, S.; Gallegos-Carrillo, K.; Flores, Y.; Salmerón, J. Dietary glycemic index, dietary glycemic load, blood lipids, and coronary heart disease. J Nutr Metab 2010, 2010. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.-H.; Hwang, I.-G.; Lee, Y.-M. Effects of anthocyanin supplementation on blood lipid levels: a systematic review and meta-analysis. Frontiers in Nutrition 2023, 10. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Sun, J.; Lu, Y.; Bo, Y. Effects of Anthocyanin on Serum Lipids in Dyslipidemia Patients: A Systematic Review and Meta-Analysis. PLOS ONE 2016, 11, e0162089. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study design. The order of the interventions was random with six possible orders. Each intervention had a duration of eight weeks. Intervention periods were separated by washout periods with a duration of three weeks, resulting in a total study duration of 30 weeks. 24-hour blood pressure and fasting blood samples were taken before and after each intervention period, which is marked with orange dots.
Figure 1.
Study design. The order of the interventions was random with six possible orders. Each intervention had a duration of eight weeks. Intervention periods were separated by washout periods with a duration of three weeks, resulting in a total study duration of 30 weeks. 24-hour blood pressure and fasting blood samples were taken before and after each intervention period, which is marked with orange dots.
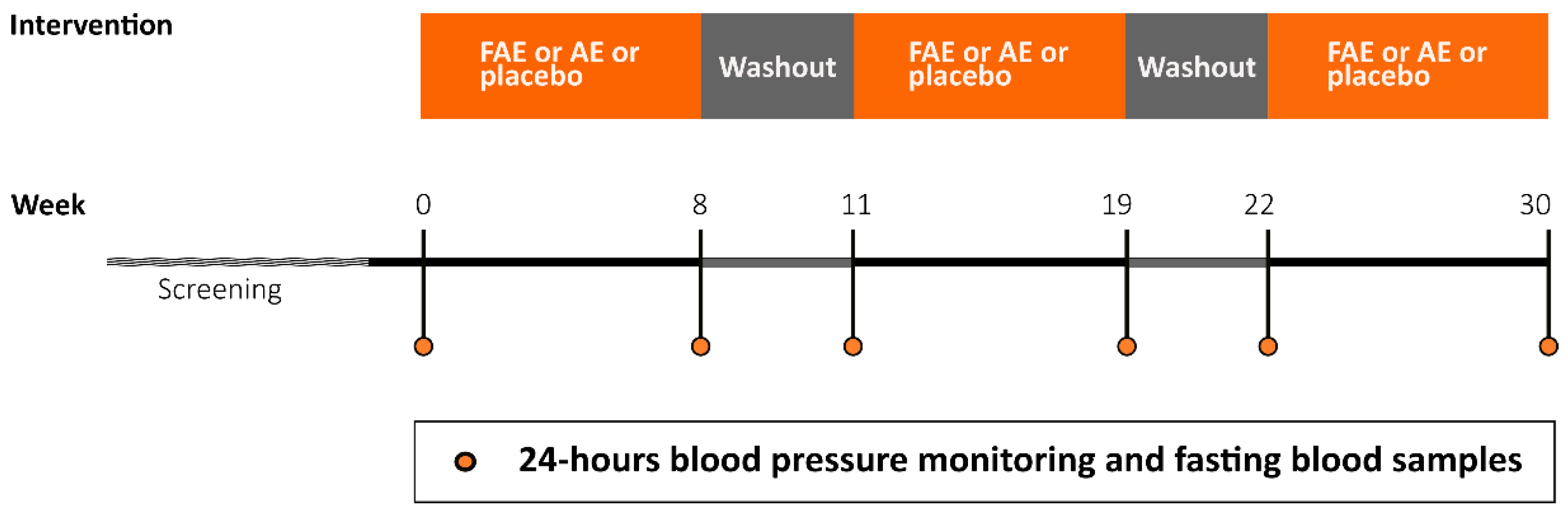
Figure 2.
CONSORT flow diagram outlining inclusions, exclusions and reasons for discontinuation. Reprinted with permission from [23] under the Creative Commons Attribution (CC BY) license.
Figure 2.
CONSORT flow diagram outlining inclusions, exclusions and reasons for discontinuation. Reprinted with permission from [23] under the Creative Commons Attribution (CC BY) license.
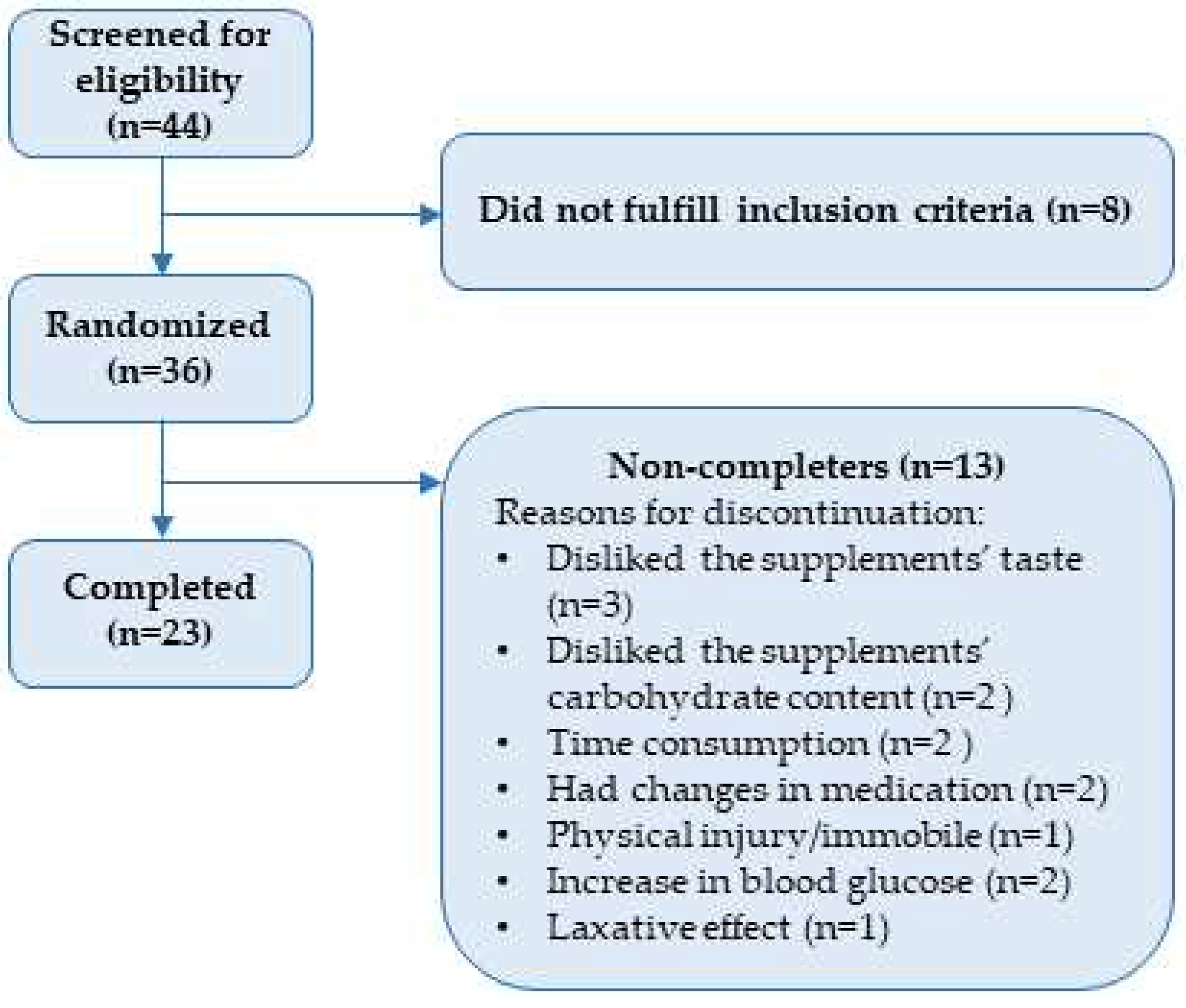

Table 1.
Nutritional composition of FAE, AE and placebo. Values are for one daily dose (2 bars). For macronutrients, we also provide energy in percentage in square brackets, which are calculated by assigning 4 kcal/g of carbohydrate or protein and 9 kcal/g of fat and dividing that value with the energy content. Reprinted with permission from [23] under the Creative Commons Attribution (CC BY) license.
Table 1.
Nutritional composition of FAE, AE and placebo. Values are for one daily dose (2 bars). For macronutrients, we also provide energy in percentage in square brackets, which are calculated by assigning 4 kcal/g of carbohydrate or protein and 9 kcal/g of fat and dividing that value with the energy content. Reprinted with permission from [23] under the Creative Commons Attribution (CC BY) license.
| Nutritional content per daily dose | FAE | AE | Placebo |
| Energy (kcal) | 234.6 | 240.1 | 227.3 |
| Total fats (g) [%] | 3.7 [14.2] | 4.0 [15.0] | 3.5 [13.9] |
| - Saturated (g) | 2.9 | 3.0 | 2.4 |
| - Unsaturated (g) | 0.4 | 0.6 | 0.5 |
| - Polyunsaturated | 0.2 | 0.2 | 0.5 |
| Total carbohydrates (g) [%] | 43.2 [73.7] | 45.1 [75.1] | 41.1 [72.3] |
| - Free sugars (g) | 38.6 | 38.6 | 34.7 |
| Dietary fibers (g) | 9.2 | 6.6 | 8.1 |
| Protein (g) [%] | 2.5 [4.3] |
2.5 [4.2] |
3.7 [6.5] |
Abbreviations: FAE: fermented aronia extract, AE: aronia extract.
Table 2.
Baseline values for participants that have completed the trial. Reprinted with modifications from [23] under the Creative Commons Attribution (CC BY) license.
Table 2.
Baseline values for participants that have completed the trial. Reprinted with modifications from [23] under the Creative Commons Attribution (CC BY) license.
| Variable (unit) | Completers (n=23). Value in mean ± SD or median (IQR) | Randomized (n=36). Value in mean ± SD or median (IQR) |
| Gender | 15 (M) 8 (W) |
21 (M) 15 (W) |
| Age (years) | 67.6±5.5 | 66.9±6.0 |
| Bodyweight (kg) | 82.0±16.2 | 85.9 (72.6-95.5) |
| Body mass index (kg/m2) | 26.7 (23.2-29.8) | 28.6 (24.3-32.0) |
| Hemoglobin A1c (mmol/mol) | 50.0 (47.5-54) | 50.5 (47.0-55.0) |
Abbreviations: SD: standard deviation, IQR: interquartile range, W: women, M: men.
Table 3.
Overview over participants’ medications. Reprinted with modifications from Reprinted with permission from [23] under the Creative Commons Attribution (CC BY) license.
Table 3.
Overview over participants’ medications. Reprinted with modifications from Reprinted with permission from [23] under the Creative Commons Attribution (CC BY) license.
| Medication/compound | Completers (n=23). Received by [number participants (%)] | Randomized (n=36). Received by [number participants (%)] |
| Metformin | 21 (91.3) | 33 (91.7) |
| Insulin | 1 (4.3) | 3 (8.3) |
| GLP-1 receptor agonist | 4 (17.4) | 6 (16.7) |
| Dipeptidyl peptidase-4 inhibitor | 2 (8.7) | 2 (5.6) |
| Sodium-glucose Cotransporter-2 inhibitor | 8 (34.8) | 9 (25.0) |
| Sulfonylurea | 2 (8.7) | 3 (8.3) |
| Statins | 15 (65.2) | 25 (69.4) |
| ACE inhibitor | 10 (43.5) | 15 (41.7) |
| Angiotensin II receptor blocker | 4 (17.4) | 9 (25.0) |
| Beta blocker | 8 (34.8) | 11 (30.6) |
| Antiplatelet/anticoagulant treatment | 6 (26.1) | 9 (25.0) |
| Calcium channel blocker | 6 (26.1) | 10 (27.8) |
| Cardiac glycosides | 0 (0.0) | 1 (2.8) |
| Diuretics | 5 (21.7) | 8 (22.2) |
| Levothyroxine treatment | 2 (8.7) | 2 (5.6) |
| Dietary supplement | 12 (52.2) | 20 (55.6) |
Table 4.
Mean pre and post values as well as mean difference (Δ-mean) for 24-hour ambulatory blood pressure monitoring and blood analyses. Normally distributed data are presented as the difference between pre and post values ± standard error (Δ-mean). Not normally distributed data are presented as ratio (confidence levels) and written in italics. The data on hs-CRP was not normally distributed; therefore, we compared ratios instead of Δ-means. To clarify, a ratio of 1.10 signifies a 10% increase from pre to post, whereas a value of 0.83 denotes a 17% decrease. Means for pre and post values are all presented on original scale ± standard error. Significant differences are bold and marked by *. If more significant values are present in one line, differences are marked by superscript letters.
Table 4.
Mean pre and post values as well as mean difference (Δ-mean) for 24-hour ambulatory blood pressure monitoring and blood analyses. Normally distributed data are presented as the difference between pre and post values ± standard error (Δ-mean). Not normally distributed data are presented as ratio (confidence levels) and written in italics. The data on hs-CRP was not normally distributed; therefore, we compared ratios instead of Δ-means. To clarify, a ratio of 1.10 signifies a 10% increase from pre to post, whereas a value of 0.83 denotes a 17% decrease. Means for pre and post values are all presented on original scale ± standard error. Significant differences are bold and marked by *. If more significant values are present in one line, differences are marked by superscript letters.
| Variable (unit) | Δ-mean for FAE | Δ-mean for AE | Δ-mean for placebo | p value | ||||
| Pre | Post | Pre | Post | Pre | Post | |||
| 24-hours systolic BP (mmHg) n=35 |
-0.71 ± 1.18 | 0.03 ± 1.07 | -0.30 ± 1.17 | |||||
| 125 ± 2.14 | 125 ± 2.19 | 124 ± 2.14 | 124 ± 2.14 | 124 ± 2.12 | 124 ± 2.14 | |||
| 24-hours diastolic BP (mmHg) n=35 |
0.16 ± 0.77 | 0.03 ± 0.70 | -1.40 ± 0.77 | |||||
| 71 ± 1.47 | 71 ± 1.49 | 71 ± 1.43 | 71 ± 1.46 | 71 ± 1.46 | 71 ± 1.49 | |||
| Hs-CRP n=23 | (ratio) | 1.10 (0.69-1.76) | 0.83 (0.52-1.34) | 1.05 (0.66-1.68) | ||||
| (mg/l) | 0.56 ± 0.11 | 0.62 ± 0.12 | 0.69 ± 0.14 | 0.58 ± 0.12 | 0.53 ± 0.10 | 0.55 ± 0.11 | ||
| Adiponectin (mg/l) n=23 |
0.14 ± 0.26 | -0.59 ± 0.26 | 0.06 ± 0.26 | |||||
| 8.44 ± 0.87 | 8.58 ± 0.87 | 9.14 ± 0.87 | 8.55 ± 0.87 | 8.38 ± 0.87 | 8.43 ± 0.87 | |||
| HDL-cholesterol (mmol/l) n=36 |
0.08 ± 0.03 | -0.01 ± 0.03 | 0.08 ± 0.03 | |||||
| 1.14 ± 0.05a | 1.22 ± 0.05a | 1.2 ± 0.05 | 1.19 ± 0.05 | 1.12 ± 0.05b | 1.2 ± 0.05b |
a0.03 b0.02 |
||
| LDL-cholesterol (mmol/l) n=36 |
0.01 ± 0.08 | -0.09 ± 0.07* | 0.20 ± 0.08* | 0.04 | ||||
| 1.86 ± 0.11 | 1.87 ± 0.12 | 1.89 ± 0.11 | 1.81 ± 0.11 | 1.82 ± 0.11* | 2.02 ± 0.12* | 0.01 | ||
| Total-cholesterol (mmol/l) n=36 |
0.08 ± 0.09 | 0.002 ± 0.08* | 0.36 ± 0.09* | 0.01 | ||||
| 3.75 ± 0.14 | 3.83 ± 0.14 | 3.81 ± 0.13 | 3.81 ± 0.13 | 3.67 ± 0.13* | 4.03 ± 0.14* | 0.0003 | ||
| Triglyceride (mmol/l) n=36 |
-0.01 ± 0.09 | 0.23 ± 0.08 | 0.17 ± 0.09 | |||||
| 1.63 ± 0.13 | 1.62 ± 0.13 | 1.58 ± 0.13* | 1.81 ± 0.13* | 1.66 ± 0.13 | 1.83 ± 0.13 | 0.03 | ||
Abbreviations: FAE: Fermented aronia extract, AE: Aronia extract, BP: Blood pressure, Hs-CRP: High-sensitive C-reactive protein, HDL-cholesterol: High-density lipoprotein cholesterol, LDL-cholesterol: Low-density lipoprotein cholesterol.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



