
Submitted:
30 October 2023
Posted:
31 October 2023
You are already at the latest version
Abstract
Regional anesthesia in postoperative pain management have developed in recent years, especially with the advent of fascial plane blocks. This study aims to compare the ultrasound-guided bilateral erector spinae plane block (ESPB) versus bilateral transversus abdominis plane block (TAPB) on postoperative analgesia after laparoscopic or robotic urologic surgery. This was a retrospective observational study; 97 patients (ESPB-group) received bilateral ultrasound-guided ESPB with 20 mL of ropivacaine 0.375% plus 0.5 mcg/kg of dexmedetomidine in each side at the level of T7-T9, and 93 patients (TAPB-group) received bilateral ultrasound-guided TAPB with ropivacaine 0.375% or 0.25%. The primary outcome was post-operative numeric rating scale (NRS) pain score, which was significantly lower in the ESPB-group on postoperative days 0, 2, and 3 (p=0.012, p=0.016 and p=0.004). Concerning the secondary outcomes, consumption of ropivacaine was significantly lower in ESPB-group (p<0.001) and the total amount of analgesic rescue doses was significantly lower in the ESPB-group than TAPB-group in postoperative days from 2 to 4 (1 vs 3, p>0.001). Incidence of postoperative nausea and vomiting was higher in the TAPB-group and no block related complications were observed. We conclude that ESPB provide better postoperative pain control with less consumption of local anesthetic and less total rescue analgesic therapies.
Keywords:
postoperative analgesia
; plexus abdominal blocks
; abdominal surgery
; laparoscopic urologic surgery
; robotic urologic surgery
; post operative nausea and vomiting
; ERAS protocol
; postoperative pain
; opi
Introduction
Minimally invasive surgery associated with Enhanced Recovery After Surgery (ERAS) programs is nowadays a standard of care in many hospitals around the world, as it has demonstrated a reduction in post-operative recovery time and complications, without affecting the oncological outcomes [1,2,3,4].
However, even if pain is reduced by the surgical technique itself due to small keyhole incisions with limited tissue retraction and stretching of fascia and muscular fibres, a residual pain arises from abdominal distension and peritoneal irritation due to pneumoperitoneum, diaphragm stretching, trocar incision, abdominal wall extraction site and internal organs [5].
In accordance with ERAS protocols the anaesthetic and analgesic techniques have been changing over years and nowadays multi-modal strategies for post-operative pain management have been identified in order to spare partially or totally the use of opioids and non-steroid anti-inflammatory drugs (NSAIDs) [6]. Opioids are in fact responsible for nausea, vomiting or respiratory depression while NSAIDs increase the risk of post-operative acute kidney injury (PO-AKI), especially in urologic patients [6,7].
Among current analgesic strategies for laparoscopic or robotic-assisted urologic surgery there are neuraxial analgesia, (i.e. peridural or spinal analgesia), or inter-fascial blockade, such as transversus abdominis plane block (TAPB) or erector spinae plane block (ESPB) [5,6,8]. Several studies have compared efficacy of these techniques and superiority of one among others with controversial results [9,10]. Nevertheless, we still don’t have a current recommendation for use of one technique over the others, and the choice still relies to the on duty anaesthetist.
The aim of the present study was to describe the analgesic ERAS protocols in use at our institution and to compare the analgesic efficacy of intraoperative TAPB versus ESPB for postoperative pain control in minimally invasive urologic surgeries; pain control will be assessed with the numeric rating scale (NRS). Total local anesthetic requirement, reduction of opioids or NSAIDs consumption, and incidence of adverse effects or block related complications will also be evaluated as secondary outcomes.
Materials and methods
Study design and patients
This was a retrospective study conducted at the Galliera Hospital of Genova from January 2022 to July 2023. All patients signed informed consent on personal data storage and the local ethics committee approved the study (7/2019 id: 4378, amendment 2). The study involved 190 consecutive patients undergoing any type of major elective urologic surgery by laparoscopic or robotic-assisted techniques. All patients followed a consolidated perioperative ERAS program as previously described [7]. The only exclusion criteria was the inability to perform an inter-fascial blockage due to infection at the injection site, known allergy or hypersensitivity to local anaesthetics or serious heart arrhythmia. Ninety-three patients were submitted to TAPB analgesic protocol (TAPB-group) and 97 ESPB analgesic protocol (ESPB-group). The analgesic protocols for both groups have been previously defined in the ERAS protocol and patients were submitted to either one depending on the anaesthesiologist’s skill and personal clinical decision (Table 1).
Technique
ESPB
Patients were taken to a preanesthetic room 1 hour before surgery. After placement of a 18-16 G peripheral intravenous cannula, patients were pre-medicated with midazolam 1-3 mg i.v. and monitored by pulse oximetry, electrocardiography, and non-invasive arterial pressure measurement. Patients were first positioned in a sitting position, and an ultrasound evaluation was performed to identify the transverse process of the vertebra corresponding to the desired level and the erector spinae muscle. ESPB was performed between T7-T9 transverse process, preferring T7-T8 for kidney surgery and T9 for pelvic surgery. A linear probe 10 MHz was used for ultrasound evaluation and a convex probe with a musculoskeletal setting (Mindray TE7 ultrasound device, Shenzhen Mindray Bio-Medical Electronics Co.) was used only if a deeper view was required by high BMI or particular physical conformation. Once identified the transverse process between T7-T9, a 22G x 88 mm needle (SonoTAP, PAJUNK GmbH, Medizin technologie, Germany) was inserted after disinfection of the puncture site, using an in-plane technique with 30° angle in a cranio-caudal direction; the needle was advanced through the muscle to hit the transverse process. After negative aspiration test, ropivacaine 0.375% or 0.5% mixed with normal saline for 20 mL plus dexmedetomidine 0.5 mcg/kg was administered. During injection, the spread of the local anaesthetic mixture was monitored in real-time, and the correct execution of the block was evidenced by the separation of the erector spinae muscle from the transverse process. The same procedure was repeated on the contralateral side. (Figure 1 panel A)
TAPB
TAPB was performed after induction of anaesthesia. For pelvic surgery, TAPB was performed through four injection sites (two inferolateral and two subcostal sites bilaterally). For kidney surgery, due to the monolateral position of the trocar incisions, TAPB was performed through three injection sites (one inferolateral and two bilateral subcostal sites). Ropivacaine total dose was calculated depending on the number of injection sites and patient’s weight (total amount of ropivacaine 3 mg/kg divided into 3 or 4 injection sites). In supine position, a linear 10-mHz transducer (Mindray TE7 ultrasound device, Shenzhen Mindray Bio-Medical Electronics Co.) was placed laterally on the abdominal wall between the lower costal edge and the iliac crest to identify the three abdominal wall muscles (external oblique, internal oblique and transverse abdominis). After disinfection of the puncture site, a 22G x 88 mm needle (SonoTAP, PAJUNK GmbH, Medizin technologie, Germany) was inserted latero-medially with an in-plane technique until it reached the fascia delimited by the internal oblique and the abdominal transverse muscle. (Figure 1 panel B) After negative aspiration test, ropivacaine 0.375% or 0.25% mixed with normal saline for 20 ml was injected. During injection, the spread of the local anaesthetic mixture was monitored in real-time, and the correct execution of the block was evidenced by the separation of the muscles.
Anaesthesia management
General anaesthesia was induced with propofol (1.5-2 mg/kg), remifentanil at 0.15 mcg/kg/min and rocuronium (1 mg/kg). Anaesthesia was maintained with sevoflurane (MAC 0.5-0.8) and remifentanil infusion (0.005-0.2 mcg/kg/min) keeping the bispectral index value (BIS) between 50-60. Deep neuromuscular blockage was maintained throughout the surgery with a train-of-four (TOF)=0 and a post-tetanic count (PTC)<4. All patients were managed with an individualised goal-directed fluid therapy. Pressure-controlled ventilation with volume guaranteed was used for intra-operative mechanical ventilation. Tidal volume was set at 7-8 mL/kg and the respiratory rate adjusted to maintain 30-35 mmHg end-tidal CO2. All patients had a pneumoperitoneum pressure of 10 mmHg, using AirSeal Intelligent Flow System® (ConMed, Utica, NY, USA) or Lexion System® (Lexion Medical, St Paul, Minnesota, USA) throughout the surgery procedure, either laparoscopic or robotic assisted. Patients undergoing radical prostatectomy were positioned at 20° Trendelenburg for laparoscopic or 24° for robotic-assisted technique. Patients undergoing nephrectomy were placed in lumbotomy position. Before awakening from anaesthesia, all patients received intra-venous paracetamol 1 gr. NSAIDs, namely, ketoprofen 30 mg or ibuprofen 600 mg, were administered only to patients with an estimated glomerular filtration rate (eGFR) >60 ml/min/1.73m2 otherwise no NSAIDs were administered. TAPB-group also received morphine 5 mg while ESPB-group did not receive any opioid. At the end of the procedure, patients were extubated by reversing rocuronium with 2-4 mg/kg sugammadex. Patients were monitored for 60 min in the recovery room and discharged when modified Aldrete score system was> 8.
Analgesia protocol and rescue analgesia
For post-operative analgesia (Table 1), patients received paracetamol 1 g every 8 hours in post-operative Day (POD)-0 and 1. From POD-2 no fixed analgesic therapy was foreseen, but it was set up only as needed, with a first rescue therapy based on paracetamol and a second rescue therapy based on NSAID (Ketorolac 30 mg). The second rescue therapy with NSAID was excluded for patients at high risk of PO-AKI or with eGFR<60 ml/min/1.73m2, and in these cases the second rescue dose was Morphine 3 mg s.c. Pain was evaluated by an 11-points numerical rating scale (NRS), with 0 indicating “no pain” and 10 “the worst pain ever possible”; nurses asked patients to score pain three times a day, every 8 hours. First rescue analgesia was administered when NRS was >4. If a first rescue dose was not sufficient and NRS was still >4, a second rescue analgesia was administered at doctor’s discretion. Post-operative nausea and vomiting were evaluated by a verbal descriptive scale.
Outcomes
The primary outcome was to compare post-operative NRS between groups from POD0 to POD4. Secondary outcomes included postoperative consumption of rescue therapies, nausea and vomiting events, incidence of block-related complications (bleeding, infection, pneumothorax, perforation) or other side effects (nausea, vomiting, bradycardia, hypotension) and total local anaesthetic consumption.
Statistical analyses
Assuming a difference in the proportion of postoperative complications between the two groups = 0.15 (effect size for proportions = 0.502), a minimum sample size of 63 patients for each group was required to obtain a statistical power = 0.8 (alpha = 0.05 with two-sided alternative hypothesis). Categorical data are presented as numbers and percentages, and continuous data are presented as mean and standard deviation (SD). Categorical data were compared by Pearson’s 𝜒2 test with Yates correction or Fisher’s exact test, when appropriate. Continuous variables were compared by Student’s 𝑡-test for unpaired data. P<0.05 was considered to indicate statistical significance. Statistical analyses were performed using the SPSS software packages, version 27.0 (SPSS, Chicago, IL, USA).
Results
The two groups were comparable regarding age, sex, BMI, ASA physical status, type and duration of surgery, and duration of anaesthesia (Table 2). Mean NRS in POD0, POD2 and POD3 were significantly lower in the ESPB group than in the TAPB group (p=0.012, p=0.016 and p=0.004, respectively, Figure 2). A significantly lower amount of ropivacaine was administered to patients of ESBP than TAPB group (170+25 vs 305+25, p<0.001). The number of analgesic rescue doses was insignificantly different between groups in POD0 and POD1 but significantly lower in ESPB than TAPB group in POD2 and POD4 (1 vs 3, p<0.001). Comparing type of rescue drugs, the ESPB group required significantly less Paracetamol (p=0.005), NSAID (p<0.001), and morphine (p=0.033). Significantly lower occurrence of post-operative nausea and vomiting (PONV) was reported by ESPB than TAPB patients (18 vs 4, p<0.001). No block-related complications were observed in any patient in the two groups. Only 3 vasovagal events were reported in the ESPB group during plexus procedure, but none of them was so relevant to prevent the block from being completed.
This retrospective observational study evaluated the efficacy of intraoperative TAPB versus ESPB for post operative pain control, in addition to the development of complications due to the blocks, opioids or NSAIDs consumption, and need of rescue analgesic doses. The main findings were that an analgesic strategy with ESPB 1) effectively controlled post-operative pain better than with TAPB, 2) was obtained in a totally opioid-free mode and with lower ropivacaine doses, and 3) required less post-operative analgesic rescue therapies (paracetamol, NSAIDS and morphine), thus reducing post-operative nausea and vomiting.
Several studies have demonstrated the effectiveness of ESPB in providing analgesia for thoracic, abdominal and lumbar surgeries, depending on where it is performed[11]. Indeed, ESPB at low thoracic levels (T8-T12) effectively affects the abdominal dermatomes involved in major urological surgery[12]. Post-mortem studies have shown that 15-20 mL of local anaesthetics are able to produce a craniocaudal spread from the injection point to 4-5 transverse processes above and below[13]. Moreover, a simultaneous spread of local anaesthetic to craniocaudal and paravertebral areas affects dorsoventral branches of spinal nerves and sympathetic ganglia, thus achieving either somatic and visceral sensory blockade. This allows reducing substantially the use of opioids both intra- and post-operatively, thus limiting adverse effects[14]. Our results confirm those of previous studies demonstrating a high efficacy of ESPB in an opioid-free strategy and extends ESPB efficacy to minimally invasive urologic surgeries. In fact, up to date, only few experiences on ESPB in urologic surgery have been reported for percutaneous nephrolithotomy [15,16], radical prostatectomy either laparoscopic or open [12,17], and laparoscopic nephrectomies, [18,19] mostly comparing ESPB to epidural or completely intravenous analgesia.
TAPB provides blockade of the cutaneous nerves of anterior and lateral abdominal wall from T6 to T12 [8], affecting somatic but not visceral components of pain. For this reason, low opioid doses are required upon awakening from surgery to cover the immediate postoperative period. However, even if in our study we demonstrated TAPB to be inferior to ESPB, an analgesic strategy with TAPB achieves great benefits compared to standard analgesic treatments in the first 24-48 hours after surgery in terms of pain scores and overall opioid consumption. In fact, TAPB has been described to be effective in analgesic pain control with a reduction in opioid consumption even in urologic surgery with good results in either radical robotic-assisted prostatectomies [20], laparoscopic nephrectomies [21] and percutaneous nephrolithotomy [22].
From a technical point of view, in our study we chose a multiple-site TAPB technique, using both subcostal and lateral approaches, with different numbers of injection sites, depending on the positioning of trocar edges for the different types of surgery. Four injection sites were chosen for all pelvic procedures, while for nephrectomies, we opted for three injection sites, two subcostal and one lateral on the intervention side[8]. The latter enabled us to inject concentrations of ropivacaine in the organ extraction area requiring a surgical enlargement of trocar edge [21] higher than in the two subcostal bilateral sites, aimed at attenuating pain from pneumoperitoneum overdistension. The total volume for each site was always 20 mL as in numerous previous studies and the ropivacaine total dose was determined as the maximal safe dose. On the contrary, the two injection sites required for ESPB have demonstrated a significant reduction in the total dose of local anesthetics, with a consequent significative reduction of risk of systemic toxicity [23].
Another technical aspect to be underlined is that TAPB was performed during general anesthesia before starting surgical procedures, to avoid patient’s discomfort or interference. On the contrary, ESPB required collaboration by the patient being in a sitting position. This was likely the reason for three vasovagal episodes in our ESPB group, which were quickly resolved by placing the patient in a supine position and administering a bolus of epinephrine. Neither group had side effects during intraoperative or postoperative periods.
We decided to use dexmedetomidine in ESPB as an adjuvant to prolong our plexus block due to reduction of neuronal activity, reduction of acute local anaesthetic-induced perineurial inflammation and local vasoconstriction able to delay local anaesthetic absorption[24,25,26]. Moreover adding dexmedetomidine we took advantage also of some systemic effects such as mild sedative, anti-anxiety, and hypnotic[27,28]. The optimal dose has not yet been determined. In our ERAS protocol we added dexmedetomidine to ESPB at a total dose of 1 μg/kg according to previous studies[27,29], which provided mild sedative and relaxing effects, facilitating patients’ management both on entering the operating room and awakening from anesthesia,[29] and a long lasting block up to 48-60 hours.[27] This enabled us to avoid opioids administration, as rescue doses on POD1 and POD2, with a significant reduction in post-operative PONV. Furthermore, we were able to substantially reduce the use of NSAIDs, especially in POD2, with a lower risk of post-operative acute kidney injury and gastric ulcers. Finally, at the dosage used in this study no serious side effects occurred in terms of hemodynamic instability or bradycardia.
This study has several limitations. First, because of its retrospective observational nature, the results need to be confirmed in further randomized controlled studies. Second, NRS pain scores were collected by nurses during nursing times and the mean of 3 NRS per day taken for analysis. No different assessments were taken at rest and physical activity, although per our ERAS protocol all patients in POD1 are already out of bed and walking. Third, we did not assess block success and lasting by evaluation of dermatomal sensory loss using pinprick test or cold alcohol swab, which might have contributed to better define efficacy of our sensory blockades. Fourth, the two analgesic strategies were identical regarding post-operative i.v. analgesic administrations but different intraoperative strategies were adopted, mainly as no adjuvants of local anesthetic were used in the TAPB.
Conclusions
An opioid-free analgesic strategy with ESPB plus dexmedetomidine can reduce the need of rescue analgesic drugs and effectively controls post-operative pain in minimally invasive major urologic surgery. Moreover, ESPB requires lower dosage of local anesthetic than TAPB, thus reducing the risk of systemic toxicity. Therefore, ESPB may be a good analgesic strategy in the context of ERAS programs to avoid side effects of opioids and NSAIDs that may slow down post-operative recovery.
Author Contributions
Dr Micali and Brusasco contributed to the study design, data collection and analysis, data interpretation, the writing of the manuscript and are the guarantor of the paper, Dr Cucciolini and Bertoni contributed to the study design, data analysis, writing of the manuscript, creating graphical abstract and figures, Dr Gandini and Lattuada contributed to data collection, data analysis and checking of the manuscript; Prof Santori contributed to data analysis, data results interpretation and checking of the manuscript; Prof Corradi and Dr Introini contributed to the study design, data analysis, data results interpretation and writing of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Regione Liguria (7/2019 id: 4378, amendment 2).
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Data availability statement
Data was not inserted in publicly archived datasets but is available anonymized for research purposes if asked to corresponding author.
References
- Ashrafi, A.N.; Yip, W.; Graham, J.N.; Yu, V.; Titus, M.; Widjaja, W.; Dickerson, S.; Berger, A.K.; Desai, M.M.; Gill, I.S.; et al. Implementation of a Multimodal Opioid-Sparing Enhanced Recovery Pathway for Robotic-Assisted Radical Prostatectomy. J Robot Surg 2022, 16, 715–721. [Google Scholar] [CrossRef]
- Cao, J.; Gu, J.; Wang, Y.; Guo, X.; Gao, X.; Lu, X. Clinical Efficacy of an Enhanced Recovery after Surgery Protocol in Patients Undergoing Robotic-Assisted Laparoscopic Prostatectomy. J Int Med Res 2021, 49, 3000605211033173. [Google Scholar] [CrossRef]
- Schiavina, R.; Droghetti, M.; Bianchi, L.; Ercolino, A.; Chessa, F.; Casablanca, C.; Piazza, P.; Mottaran, A.; Recenti, D.; Salvador, M.; et al. The Robotic Approach Improves the Outcomes of ERAS Protocol after Radical Cystectomy: A Prospective Case-Control Analysis. Urol Oncol 2021, 39, 833.e1–833.e8. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, S.; Liu, B.; Li, J.; Hong, H. Clinical Efficacy of Enhanced Recovery after Surgery (ERAS) Program in Patients Undergoing Radical Prostatectomy: A Systematic Review and Meta-Analysis. World J Surg Oncol 2020, 18, 131. [Google Scholar] [CrossRef] [PubMed]
- Batley, S.E.; Prasad, V.; Vasdev, N.; Mohan-S, G. Post-Operative Pain Management in Patients Undergoing Robotic Urological Surgery. Curr Urol 2016, 9, 5–11. [Google Scholar] [CrossRef]
- Khater, N.; Comardelle, N.J.; Domingue, N.M.; Borroto, W.J.; Cornett, E.M.; Imani, F.; Rajabi, M.; Kaye, A.D. Current Strategies in Pain Regimens for Robotic Urologic Surgery: A Comprehensive Review. Anesth Pain Med 2022, 12, e127911. [Google Scholar] [CrossRef]
- Brusasco, C.; Germinale, F.; Dotta, F.; Benelli, A.; Guano, G.; Campodonico, F.; Ennas, M.; Di Domenico, A.; Santori, G.; Introini, C.; et al. Low Intra-Abdominal Pressure with Complete Neuromuscular Blockage Reduces Post-Operative Complications in Major Laparoscopic Urologic Surgery: A before-after Study. J Clin Med 2022, 11, 7201. [Google Scholar] [CrossRef] [PubMed]
- Mallan, D.; Sharan, S.; Saxena, S.; Singh, T.K. ; Faisal, null Anesthetic Techniques: Focus on Transversus Abdominis Plane (TAP) Blocks. Local Reg Anesth 2019, 12, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhang, Y.; Chen, Y.; Xu, M.; Lei, X.; Fu, Q. Analgesic Effect of Erector Spinae Plane Block in Adults Undergoing Laparoscopic Cholecystectomy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. BMC Anesthesiol 2023, 23, 7. [Google Scholar] [CrossRef]
- Peltrini, R.; Cantoni, V.; Green, R.; Greco, P.A.; Calabria, M.; Bucci, L.; Corcione, F. Efficacy of Transversus Abdominis Plane (TAP) Block in Colorectal Surgery: A Systematic Review and Meta-Analysis. Tech Coloproctol 2020, 24, 787–802. [Google Scholar] [CrossRef]
- Saadawi, M.; Layera, S.; Aliste, J.; Bravo, D.; Leurcharusmee, P.; Tran, D.Q. Erector Spinae Plane Block: A Narrative Review with Systematic Analysis of the Evidence Pertaining to Clinical Indications and Alternative Truncal Blocks. J Clin Anesth 2021, 68, 110063. [Google Scholar] [CrossRef] [PubMed]
- Dost, B.; Kaya, C.; Ozdemir, E.; Ustun, Y.B.; Koksal, E.; Bilgin, S.; Bostancı, Y. Ultrasound-Guided Erector Spinae Plane Block for Postoperative Analgesia in Patients Undergoing Open Radical Prostatectomy: A Randomized, Placebo-Controlled Trial. J Clin Anesth 2021, 72, 110277. [Google Scholar] [CrossRef] [PubMed]
- Bonvicini, D.; Boscolo-Berto, R.; De Cassai, A.; Negrello, M.; Macchi, V.; Tiberio, I.; Boscolo, A.; De Caro, R.; Porzionato, A. Anatomical Basis of Erector Spinae Plane Block: A Dissection and Histotopographic Pilot Study. J Anesth 2021, 35, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Kamel, A.A.F.; Amin, O.A.I.; Ibrahem, M.A.M. Bilateral Ultrasound-Guided Erector Spinae Plane Block Versus Transversus Abdominis Plane Block on Postoperative Analgesia after Total Abdominal Hysterectomy. Pain Physician 2020, 23, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.P.; Yadav, U.; Khan, M.M.A.; Singh, A.K.; Verma, S.; Nigam, S. Efficacy of Ultrasound-Guided Erector Spinae Plane Block in Percutaneous Nephrolithotomy. Cureus 2023, 15, e40186. [Google Scholar] [CrossRef] [PubMed]
- Unal, S.; Baskan, S.; Guven Aytac, B.; Aytac, I.; Balci, M. Should the Erector Spinae Plane Block Be Applied in the Pain Management of Percutaneous Nephrolithotomy? Cureus 2022, 14, e22554. [Google Scholar] [CrossRef] [PubMed]
- Buonanno, P.; Logrieco, N.; Marra, A.; Spirito, L.; Califano, G.; Blasio, F.; Falco, N.D.; Aveta, A.; Spena, G.; Servillo, G. Robot-Assisted Radical Prostatectomy: Comparison of Subarachnoid Analgesia, Erector Spine Plane Block, and Intravenous Analgesia for Postoperative Pain Management. Korean J Anesthesiol 2023. [Google Scholar] [CrossRef] [PubMed]
- Piliego, C.; Longo, F.; Agrò, F.E. Erector Spinae Plane Block Growing Potential: Pain Management in Laparoscopy Nephrectomy. Saudi J Anaesth 2020, 14, 275–276. [Google Scholar] [CrossRef] [PubMed]
- Şahin, A.; Baran, O. Effect of Ultrasound-Guided Erector Spinae Plane Block on Post-Surgical Pain in Patients Undergoing Nephrectomy: A Single-Center, Randomized, Double-Blind, Controlled Trial. J Int Med Res 2022, 50, 3000605221086737. [Google Scholar] [CrossRef]
- Taninishi, H.; Matsusaki, T.; Morimatsu, H. Transversus Abdominis Plane Block Reduced Early Postoperative Pain after Robot-Assisted Prostatectomy: A Randomized Controlled Trial. Sci Rep 2020, 10, 3761. [Google Scholar] [CrossRef]
- Park, J.-M.; Lee, J. Effect of Transversus Abdominis Plane Block on the Quality of Recovery in Laparoscopic Nephrectomy: A Prospective Double-Blinded Randomized Controlled Clinical Trial. Medicine (Baltimore) 2022, 101, e31168. [Google Scholar] [CrossRef] [PubMed]
- Özdilek, A.; Beyoğlu, Ç.A.; Demirdağ, Ç.; Şen, Ö.; Erbabacan, Ş.E.; Ekici, B.; Altindaş, F.; Köksal, G.M. Perioperative Analgesic Effects of Preemptive Ultrasound-Guided Subcostal Transversus Abdominis Plane Block for Percutaneous Nephrolithotomy: A Prospective, Randomized Trial. J Endourol 2020, 34, 434–440. [Google Scholar] [CrossRef]
- Macfarlane, A.J.R.; Gitman, M.; Bornstein, K.J.; El-Boghdadly, K.; Weinberg, G. Updates in Our Understanding of Local Anaesthetic Systemic Toxicity: A Narrative Review. Anaesthesia 2021, 76 Suppl 1, 27–39. [Google Scholar] [CrossRef]
- Brummett, C.M.; Hong, E.K.; Janda, A.M.; Amodeo, F.S.; Lydic, R. Perineural Dexmedetomidine Added to Ropivacaine for Sciatic Nerve Block in Rats Prolongs the Duration of Analgesia by Blocking the Hyperpolarization-Activated Cation Current. Anesthesiology 2011, 115, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.-S.; Peng, H.; Wu, S.-N. Dexmedetomidine, an Alpha2-Adrenergic Agonist, Inhibits Neuronal Delayed-Rectifier Potassium Current and Sodium Current. Br J Anaesth 2009, 103, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Yoshitomi, T.; Kohjitani, A.; Maeda, S.; Higuchi, H.; Shimada, M.; Miyawaki, T. Dexmedetomidine Enhances the Local Anesthetic Action of Lidocaine via an Alpha-2A Adrenoceptor. Anesth Analg 2008, 107, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Yi-Han, W.; Rong, T.; Jun, L.; Min, W.; Yan, Z.; Yi, L.; Jie-Ting, L.; Sheng-Hui, H. Dexmedetomidine Combined with Ropivacaine for Erector Spinae Plane Block after Posterior Lumbar Spine Surgery: A Randomized Controlled Trial. BMC Musculoskelet Disord 2022, 23, 235. [Google Scholar] [CrossRef] [PubMed]
- Carollo, D.S.; Nossaman, B.D.; Ramadhyani, U. Dexmedetomidine: A Review of Clinical Applications. Curr Opin Anaesthesiol 2008, 21, 457–461. [Google Scholar] [CrossRef]
- Urits, I.; Virgen, C.G.; Alattar, H.; Jung, J.W.; Berger, A.A.; Kassem, H.; Shehata, I.M.; Elhassan, A.; Kaye, A.D.; Viswanath, O. A Comprehensive Review and Update of the Use of Dexmedetomidine for Regional Blocks. Psychopharmacol Bull 2020, 50, 121–141. [Google Scholar]
Figure 1.
Panel A: Erector Spinae Plane Block (ESPB); from left: level of puncture, in plane technique, ultrasound visualization of transverse process, and ultrasound image of anaesthetic spread. Panel B: Transversus Abdominis Plane Block (TAPB); from left: position of the probe for four or three puncture sites (box with star, subcostal approach; simple box, lateral approach) with in plane technique, ultrasound image of needle puncture and anaesthetic spread through the fascia delimited by the internal oblique and the abdominal transverse muscle.
Figure 1.
Panel A: Erector Spinae Plane Block (ESPB); from left: level of puncture, in plane technique, ultrasound visualization of transverse process, and ultrasound image of anaesthetic spread. Panel B: Transversus Abdominis Plane Block (TAPB); from left: position of the probe for four or three puncture sites (box with star, subcostal approach; simple box, lateral approach) with in plane technique, ultrasound image of needle puncture and anaesthetic spread through the fascia delimited by the internal oblique and the abdominal transverse muscle.
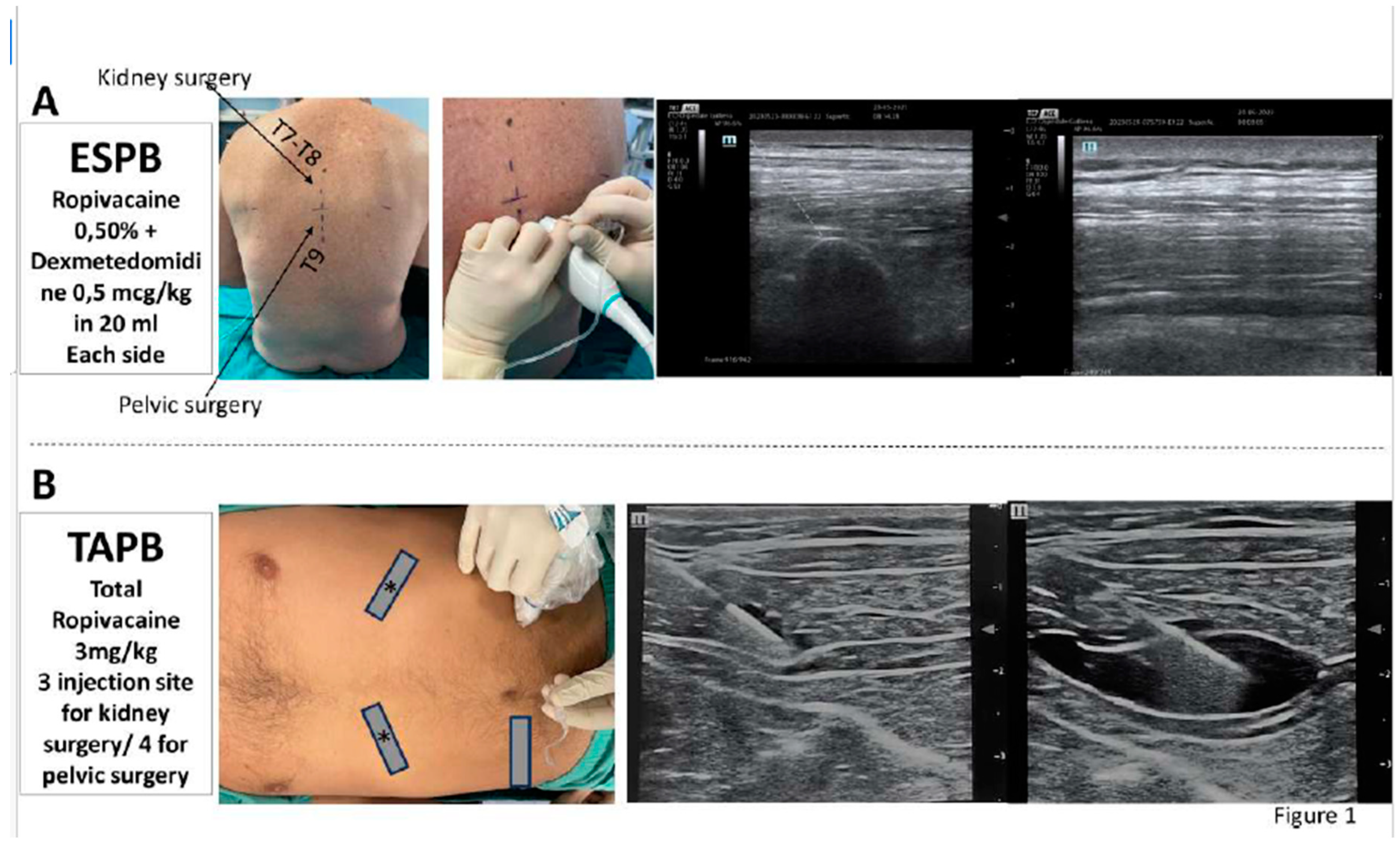
Figure 2.
Trend of changes of postoperative numeric rating scale (NRS) in both groups from postoperative day 0 to 4. ESPB: erector spinae plane block. TAPB: transversus abdominis plane block.SE: standard error of the mean.
Figure 2.
Trend of changes of postoperative numeric rating scale (NRS) in both groups from postoperative day 0 to 4. ESPB: erector spinae plane block. TAPB: transversus abdominis plane block.SE: standard error of the mean.
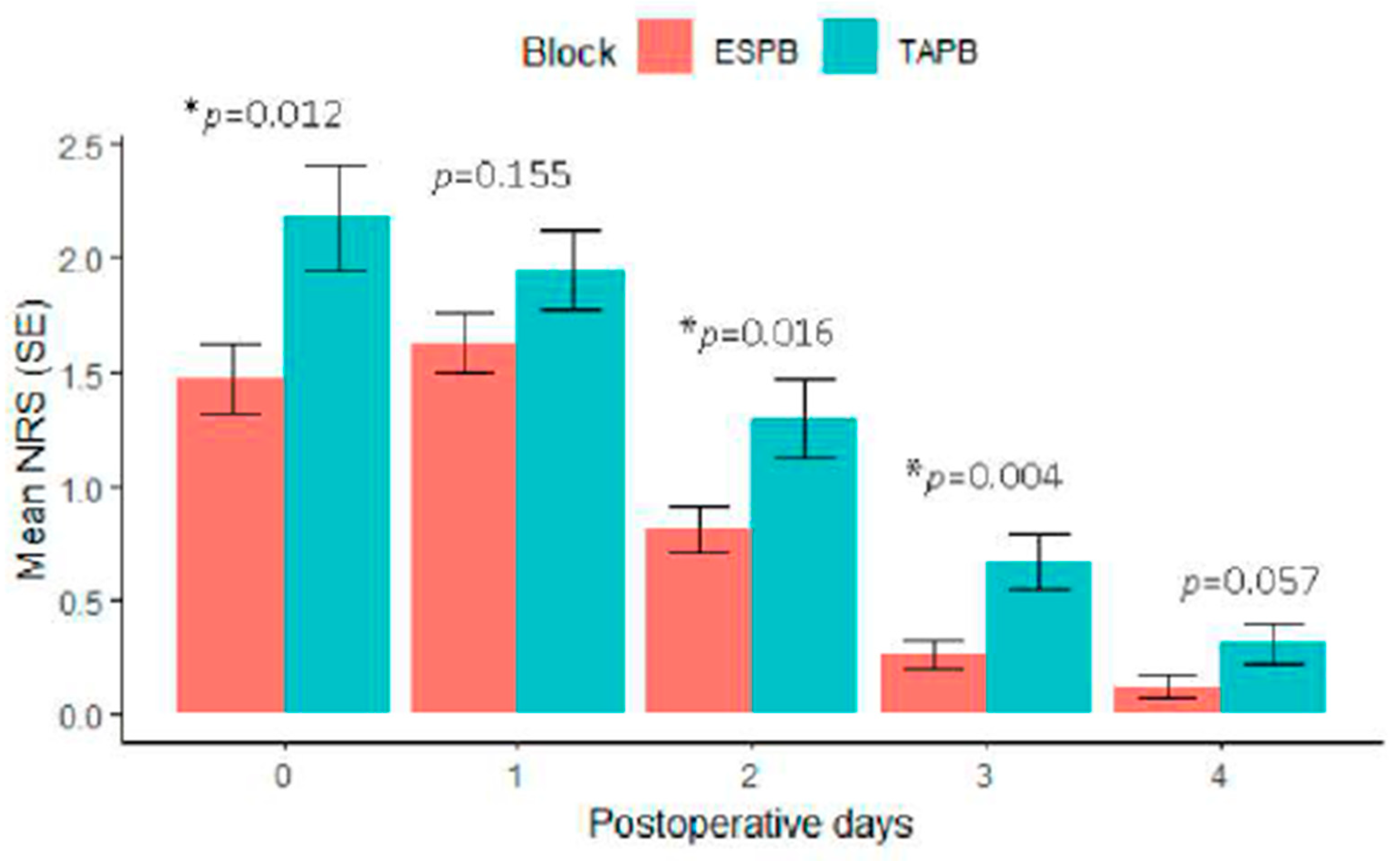

Table 1.
ERAS analgesic protocols.
| Intra-operative analgesia strategies | TAPB + Morphine 5 mg + Paracetamol 1 gr + Ketorolac 30 mg/Ibuprofen 600 mg | |
| ESPB + Paracetamol 1 gr + Ketorolac 30 mg/Ibuprofen 600 mg | ||
| Post-operative analgesia strategy | POD 0-1 | Paracetamol 1 gr x 3/die Ketorolac 30 mg if NRS>4 (If NSAIDs forbidden, Morphine 3 mg s.c.) |
| POD 2 until discharge | Paracetamol 1 gr if NRS>4 Ketorolac 30 mg if paracetamol not effective (If NSAIDs forbidden, Morphine 3 mg s.c.) |
|
ERAS Enhanced recovery after surgery, TAPB Transverse Abdominis Plane Block, ESPB Erector Spinae Plane Block, POD post-operative day, NRS numerical rating scale; s.c. Sub-cutaneous, NSAIDs non-steroid anti-inflammatory drugs.
Table 2.
Demographic data and baseline characteristics.
| TAPB-group (n. 93) | ESPB-group (n. 97) | p value | |
|---|---|---|---|
| Age, yr | 64 + 13 | 66 + 12 | 0.174 |
| Sex, m/f n | 77/16 | 87/10 | 0.207 |
| BMI, Kg/m2 | 26 + 4 | 25 + 4 | 0.646 |
| ASA class I II III |
14 68 11 |
5 81 11 |
|
| Type of surgery, n (%) Partial nephrectomy Radical nephrectomy Radical prostatectomy Adrenalectomy other |
17 (18) 13 (14) 57 (62) 2 (2) 4 (4) |
18 (19) 13 (13) 58 (60) 1 (1) 7 (7) |
|
| VLS/robotic surgery, n | 53/41 | 61/36 | 0.104 |
| Duration of surgery, min | 132 + 55 | 150 + 51 | 0.121 |
| Duration of anaesthesia, min | 173 + 53 | 177 + 50 | 0.592 |
BMI Body Mass Index; VLS video-laparoscopic surgery; ASA American Society of Anesthesiology.
Table 3.
Comparison of quality of analgesia between groups and outcomes.
| TAPB-group (n. 93) | ESPB-group (n. 97) | p value | |
|---|---|---|---|
| Total ropivacaine consumption, mg | 305 + 60 | 170 + 25 | <0.001 |
| Total patients requiring a rescue dose, n | 43 | 33 | 0.104 |
| Total rescue dose requested, n | 3 (2-5) | 1 (0-2) | <0.001 |
| Total NSAIDs consumption as rescue in POD1, n | 40 | 26 | 0.092 |
| Total morphine consumption as rescue in POD1, n | 2 | 0 | 0.502 |
| Total Paracetamol consumption as rescue in POD2 and over, n | 12 | 5 | 0.005 |
| Total NSAIDs consumption as rescue in POD2 and over, n | 29 | 6 | <0.001 |
| Total morphine consumption as rescue in POD2 and over, n | 6 | 0 | 0.033 |
| Time to first rescue analgesia, day | 1 (0-1) | 1 (0-1) | 0.195 |
| Intraoperative complications, n -bradycardia -hypotension |
0 0 |
0 0 |
0.999 0.999 |
| Postoperative complications, n -PONV -block related complications |
18 0 |
4 0 |
0.001 0.999 |
| Length of stay, n | 4 (3-6) | 4 (3-5) | 0.401 |
NSAIDs non steroid anti-inflammatory drugs; PONV post-operative nausea and vomiting. Media + standard deviation; POD post-operative day.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



