
Submitted:
31 October 2023
Posted:
01 November 2023
You are already at the latest version
Abstract
This is an opinion piece based on observations from more than two decades of biomedical data mining insights studying health and disease. It has led me to reevaluate modern life and how lived experiences in many parts of the world are being questioned and now answered through the various technological advances that have taken place in biomedical science. Our mitochondria are multi-faceted and the next generation will need to ensure that they develop a strong understanding from a scientific basis for how they are important to our health. The mind-body connection is also now being investigated through researching the networks of mitochondrial bioenergetics. This article provides a brief introduction to how we can reduce chronic disease burden globally, by introducing a simple first algorithm for healthy aging. This work is aimed to jump start the collection of Algorithms for Healthy Aging (AHA) in the context of global populations in their locally lived generational experiences, which may have underlying scientific bases that are yet to be discovered and validated.
Keywords:
Mitochondria
; Algorithms
; Healthy Aging
Introduction
Nikola Tesla pointed us in the right direction when he said ““If you want to find the secrets of the universe, think in terms of energy, frequency, and vibration.” I have spent more than two decades collaborating with biomedical scientists looking for biomarkers that underlie disease and health states. My laboratory for Pattern Recognition from Biomedical Evidence (PRoBE) in the Department of Biomedical Informatics at the University of Pittsburgh’s School of Medicine has analyzed biomedical datasets for early detection of diverse diseases including neurodegenerative Amyotrophic Lateral Sclerosis (ALS), cancers of the breast, lung, and esophagus, Ulcerative Colitis, microbiomes, heart disease and even spinal aging. Bioinformatics analyses include the mapping of markers from various omics such as proteomics, transcriptomics or metabolomics into known regulatory or metabolic pathways to help design and conduct validation studies that can lead to the translation of findings into useful tests for screening or therapy.
During the first decade of our analytical work studying various neurodegenerative diseases and heterogenous cancers, markers of inflammation, the now-well published immuno-metabolic concept of “inflammaging” was clearly a pathological driver. Additionally, it is already well-known that diseases such as type 2 diabetes are often driven by “overeating” (possibly caused by poor nutrients in the food) which causes chronic inflammation. While studying cardiovascular disease which is often a consequence of poor diet and exercise, and a known long-term complication of diabetes, it became clear to me that metabolism plays a very important role in chronic disease burden. As we researched further into the gut microbiome in infectious disease, the role of environmental toxins, and aging related data I became interested in following Tesla’s fundamental direction, namely energy.
Background and Discussion
Having a family history of diabetes and chronic fatigue, I was determined to understand more about what actions I could undertake to stave off chronic disease and its associated burden, while increasing or sustaining my energy levels as I aged. When working with federated electronic health data in a recent collaboration, I started researching more about the fundamental issues that lead to Type 2 Diabetes Mellitus, referred to as diabetes herein. Insulin resistance (IR) is a major factor it appears, along with dyslipidemia and hyperglycemia [1]. For cardiovascular disease (atherosclerosis), IR and mitochondrial dysfunction have been implicated as pathological processes in clinical investigations [2]. Furthermore, researchers have now linked metabolic health which refers to how our cells generate energy from the bioavailability of nutrients in our bloodstreams, to IR. Since IR seemed to be a common marker in this development of chronic disease, I looked at whether doctors are able to measure IR. The gold standard test for measuring insulin sensitivity is the hyperinsulinemic euglycemic clamp (HEC), which is time consuming and expensive. Therefore, other surrogate markers have been developed in the literature.
The Homeostasis model assessment of insulin resistance (Homa-IR) index, developed first in 1985 by Matthews et al. [3] indirectly quantifies IR and pancreatic β-cell function, but it has to be calibrated carefully as cut-offs vary among different populations. HOMA-IR is calculated using a timely assessment of fasting glucose and insulin concentration. This and other models for quantifying insulin sensitivity are discussed in [4]. These tests are not prescribed to many of us who are at risk for developing IR and diabetes. Those with a family history of diabetes are usually prescribed a Hemoglobin A1c (HbA1c) test which has established cutoff value ranges for prediabetes and diabetes. The problems with HbA1c tests are that many subpopulations including Asians have co-morbidities of thyroid dysfunction which require a non-standard interpretation of the HbA1c numbers [5,6]. Therefore, more precise non-invasive methods for measuring insulin sensitivity are needed.
Another important aspect that I believe is not properly managed by current medical education and practice is the proper administration of insulin. This is because we are not measuring insulin spikes which is not the same as blood glucose spikes. There is a possibility that IR is due to the fact that our body does not need to store any more energy. Diabetes can be reversed if caught early and metabolic functions can be restored if one understands what is happening from a mitochondrial and energy perspective. As beautifully described in the article [7], the mitochondria are especially susceptible to nutrient deficiencies, environmental toxins, and oxidative damage, and are implicated in many modern diseases including: Cardiovascular disease, Diabetes, and Parkinson’s disease to name a few. Other diseases listed in Table 1 in [7] include: Early aging, ALS, Alzheimer’s disease, Autism, Chronic fatigue syndrome, Dementia, Huntington’s disease, and Migraine headache. Alcohol, many prescription drugs, persistent organic pollutants and many other factors contribute to mitochondrial DNA (mtDNA) damage. Mitochondrial damage can also lead to the vicious cycle of oral and systemic disease [8].
The modern diet of refined and packaged baked goods can lead to a leaky gut, which can also lead to cardiovascular disease. Also, our microbiome can be washed out by a course of antibiotics and could lead to immune system response issues in cancer for example. In analyzing datasets containing metabolic markers of cardiovascular disease, it was clear that almost a third of patients who did not survive adverse cardiac events had toxicity build-up in the body [9]. Mitochondria are important organelles for opening up certain significant detoxification processes in our bodies which happens through signaling. Mitochondria are also involved in recycling of cells – called autophagy; as well as mitophagy, which ensures clearing away of cells and organelles that are damaged. To support health, therefore, it is important to have mitochondria that can perform their various physiological functions effectively [10].
It is important for us to note that mtDNA is passed on from the maternal side, and that our mitochondria likely formed in our grandmother or great-grandmother. Many cultures therefore historically protected women because of their importance to the future health of generations to follow. The mind-mitochondria connection has also been established [11], and Martin Picard’s Mitochondrial Psychobiology laboratory is moving this field forward. As discussed in interviews given by Picard, there are at least three ways to keep our mitochondria healthy: (1) Get physically active - moving your body improves circulation and more importantly, improves Mitochondrial biogenesis such as in muscle cells as moving stimulates the number and quality of mitochondria; (2) Not eating too much - excess nutrients can damage mitochondria, and it has been observed that Mitochondrial networks can disintegrate with nutrient overload. If we can give our digestive system a rest for cells to be at their best via some form of personalized intermittent fasting routines, it may optimize mitochondrial health, for example; (3) A positive attitude as psychological well-being – it has been shown that connectedness and positive feelings or experiences drive mitochondrial health. The Bioenergetic Health Index (BHI) gave a new concept in mitochondrial translational research in the emerging field of Bioenergetics [12]. More recently, the Mitochondrial Health Index (MHI) was developed and used to demonstrate the association between positive mood and mitochondrial functional health using human immune cells [13].
Method and Conclusion
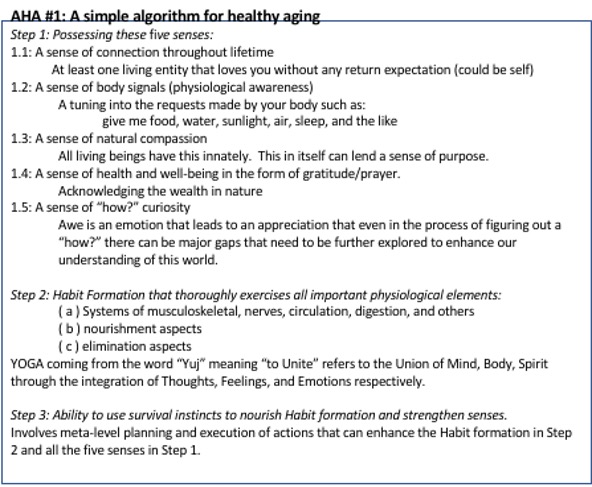
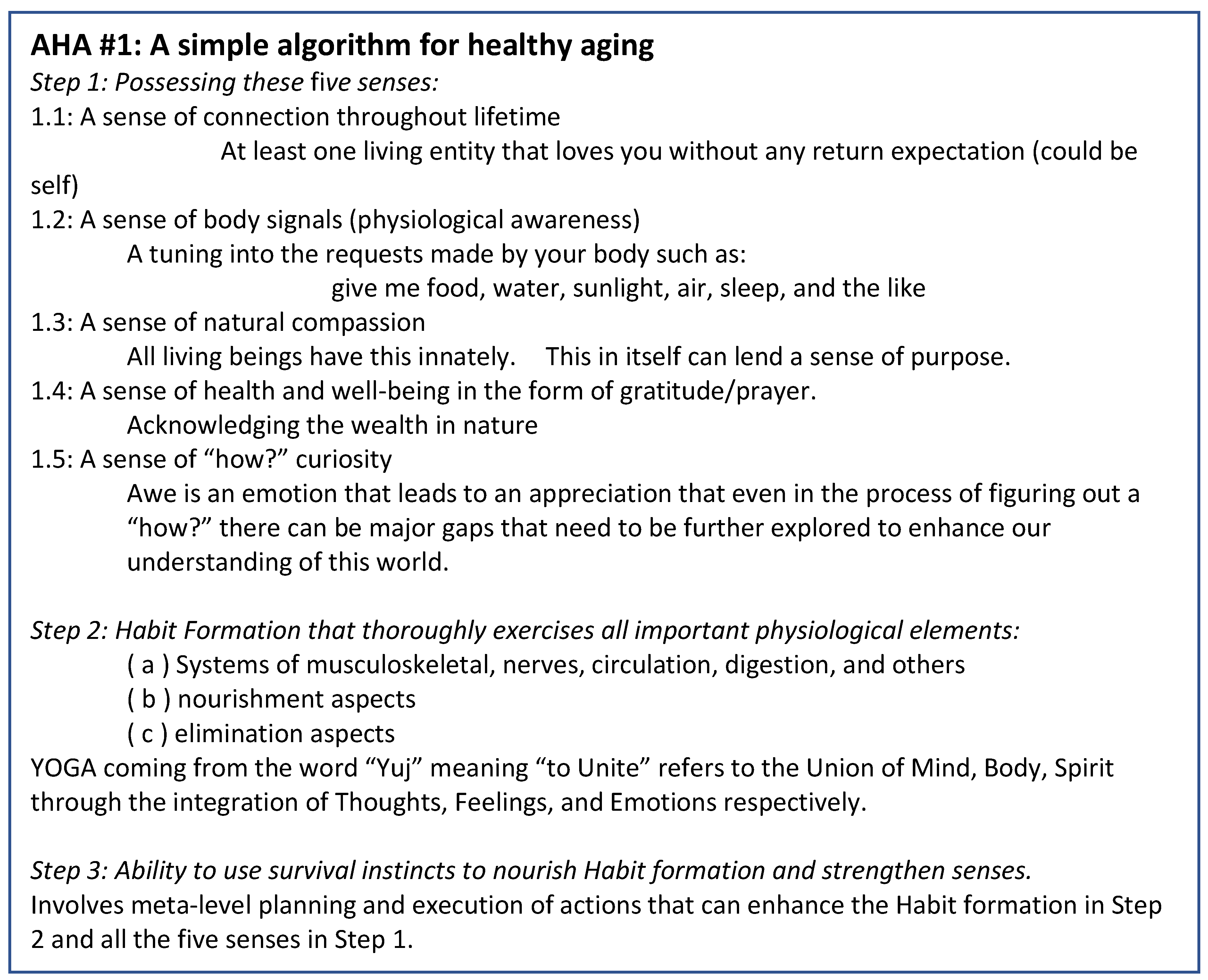
Based on my experience and research into health and disease and how we may age in a healthy manner, I present in Figure 1, a first algorithm for healthy aging. As we create more algorithms for healthy aging that can include different social contexts, we can create a compendium of Algorithms for Healthy Aging (AHA). Many biomarker studies have yielded interesting clues to exceptional longevity, a most recent one being a report from a 35-year follow-up of the Swedish cohort of centenarians and non-centenarians [14]. Their findings reported a few common trends among people over 65 who went on to become centenarians (n= 1224, out of total=44,636 participants) in their blood biomarker profiles. These observations were that higher levels of total cholesterol and iron, and lower levels of glucose, creatinine, uric acid, aspartate aminotransferase, gamma-glutamyl transferase, alkaline phosphatase, total iron-binding capacity, and lactate dehydrogenase were associated with a greater likelihood of becoming a centenarian. Genetics and lifestyle factors are known to play a role in exceptional longevity and therefore, such studies are likely to yield variable insights depending on the study characteristics and population. Nevertheless, the significant role that mitochondria play in the intracellular signaling reveals their vital importance in the maintenance of our health through energy production (metabolism), maintaining redox balance (homeostasis), and eliminating damaged cells and organelles (apoptosis and mitophagy) through cell-fate determination [15].
It is also well-known that nuclear DNA mutates less often than mitochondrial DNA because of energy optimization strategies. As research progresses in our understanding of mitochondrial structure and function relevant to human health and disease, I believe that we will get closer to the secrets of the dynamic cycles of creation, preservation, and destruction at the cellular level. The overwhelming evidence in recent literature [16] combined with my own observations seem to align very well with the theory of an underlying mitochondrial basis for most chronic diseases of body and mind. Therefore, to reduce the global burden of chronic disease, we must take care of our mitochondria through physical activity for mitochondrial biogenesis, eating smaller portion sizes of nutrient-dense and plant-based fiber food that satiates the body for longer periods of time along with some form of intermittent fasting as we age, and maintaining a positive attitude, as starting points to transforming our human experience. The future of work should include these vital aspects of health and well-being into our workplaces to allow a collective unfolding of healthful practices that humanity embraces as a whole.
This article provided a brief introduction to how we can reduce chronic disease burden globally, by introducing a simple first algorithm for healthy aging. This work is aimed to jump start the collection of Algorithms for Healthy Aging (AHA) in the context of global populations in their locally lived generational experiences, which may have underlying scientific bases that are yet to be discovered and validated. Our mitochondria are indeed multi-faceted, playing an important role in our physical and mental health, and taking care of them while enhancing our scientific understanding of their underlying biochemistry will be crucial for the human species.
References
- Poznyak A, Grechko AV, Poggio P, Myasoedova VA, Alfieri V, Orekhov AN. The Diabetes Mellitus-Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int J Mol Sci. 2020 Mar 6;21(5):1835. PMID: 32155866; PMCID: PMC7084712. [CrossRef]
- Semenkovich CF. Insulin resistance and atherosclerosis. J Clin Invest. 2006 Jul;116(7):1813-22. PMID: 16823479; PMCID: PMC1483180. [CrossRef]
- Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9. [CrossRef]
- Gutch M, Kumar S, Razi SM, Gupta KK, Gupta A. Assessment of insulin sensitivity/resistance. Indian J Endocrinol Metab. 2015 Jan-Feb;19(1):160-4. PMID: 25593845; PMCID: PMC4287763. [CrossRef]
- Huang X, Zhang X, Zhou X, Han X, Fu Z, Li Y, Ji L. Prevalence of Thyroid Dysfunction in a Chinese Population with Different Glucose Intolerance Status: A Community-Based Cross-Sectional Study. Diabetes Metab Syndr Obes. 2020 Nov 16;13:4361-4368. PMID: 33235476; PMCID: PMC7678694. [CrossRef]
- Nair A, Jayakumari C, Jabbar PK, Jayakumar RV, Raizada N, Gopi A, George GS, Seena TP. Prevalence and Associations of Hypothyroidism in Indian Patients with Type 2 Diabetes Mellitus. J Thyroid Res. 2018 Aug 9;2018:5386129. PMID: 30174822; PMCID: PMC6106958. [CrossRef]
- Pizzorno J. Mitochondria-Fundamental to Life and Health. Integr Med (Encinitas). 2014 Apr;13(2):8-15. PMID: 26770084; PMCID: PMC4684129.
- Kudva PB. “The era of prevention:” Prevention is better than cure. J Indian Soc Periodontol. 2016 Jan-Feb;20(1):2–3. PMCID: PMC4795127. [CrossRef]
- Gopalakrishnan V, Balasubramanian J, Kip K, Reis S. Towards learning clinically relevant explainable models via Bayesian Rule Learning with utilities. [Print]. Porto, Portugal: Proceedings of the 12th International Workshop on Knowledge Representation for Health Care (KR4HC 2021); 2021 June. 14 pages (41-54).
- Brand MD, Orr AL, Perevoshchikova IV, Quinlan CL. The role of mitochondrial function and cellular bioenergetics in ageing and disease. Br J Dermatol. 2013 Jul;169 Suppl 2(0 2):1-8. PMID: 23786614; PMCID: PMC4321783. [CrossRef]
- Picard, M. (2022). Energy transduction and the mind–mitochondria connection. The Biochemist. [CrossRef]
- Balu K. Chacko, Philip A. Kramer, Saranya Ravi, Gloria A. Benavides, Tanecia Mitchell, Brian P. Dranka, David Ferrick, Ashwani K. Singal, Scott W. Ballinger, Shannon M. Bailey, Robert W. Hardy, Jianhua Zhang, Degui Zhi, Victor M. Darley-Usmar; The Bioenergetic Health Index: a new concept in mitochondrial translational research. Clin Sci (Lond) 1 September 2014; 127 (6): 367–373. [CrossRef]
- Picard M, Prather AA, Puterman E, Cuillerier A, Coccia M, Aschbacher K, Burelle Y, Epel ES. A Mitochondrial Health Index Sensitive to Mood and Caregiving Stress. Biol Psychiatry. 2018 Jul 1;84(1):9-17. Epub 2018 Feb 3. PMID: 29525040; PMCID: PMC6014908. [CrossRef]
- Murata, S., Ebeling, M., Meyer, A.C. et al. Blood biomarker profiles and exceptional longevity: comparison of centenarians and non-centenarians in a 35-year follow-up of the Swedish AMORIS cohort. GeroScience (2023). [CrossRef]
- Jay X. Tan, Toren Finkel; Mitochondria as intracellular signaling platforms in health and disease. J Cell Biol 4 May 2020; 219 (5): e202002179. [CrossRef]
- Amorim, J.A., Coppotelli, G., Rolo, A.P. et al. Mitochondrial and metabolic dysfunction in ageing and age-related diseases. Nat Rev Endocrinol 18, 243–258 (2022). [CrossRef]
Figure 1.
A simple AHA: Algorithm for Healthy Aging.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



