
Submitted:
23 October 2023
Posted:
02 November 2023
You are already at the latest version
Abstract
Wildfires are a rising environmental threat which health impact remains poorly documented, in particular beyond the fire period. This ecological study investigates changes in health conditions before, during, and after two consecutive wildfires that occurred in France´s Gironde district in the summer 2022. Electronic records from the district´s emergency medical communication centre were used to identify calls with respiratory and cardiovascular diseases, and two specific subgroups of those, asthma (all ages and 0-5 years) and cardiac arrest, respectively. Compared to before the fires, respiratory disease cases were fewer during each fire (OR = 0.85, 95% CI: 0.79, 0.90 and OR = 0.62, 95% CI: 0.58, 0.67, respectively), cardiovascular disease cases, more common during the second fire, and asthma cases, higher following the fires (ORall ages= 1.85, 95% CI: 1.56, 2.21 and ORchildren= 3.52, 95% CI: 2.62, 4.80). Asthma cases also rose during the same calendar time in 2021, but to a lesser extent. In sum, except for asthma, emergency calls data in Gironde reveal few significant potentially smoke-related symptoms around fire periods, apart from post-fire asthma. Whether the effects are smoke- or season-related remains to be determined, preferably using additional data sources.
Keywords:
wildfires
; smoke
; air pollution
; climate change
; asthma
; respiratory diseases
; emergency medical services
1. Introduction
The World Health Organization (WHO) estimates that 99% of the global population is exposed to high levels of pollutants in the air, including nitrogen oxides, sulfur dioxide, and fine particles like dust and sand (1, 2). Long-term exposure to poor air quality is projected to reduce global life expectancy by an average of eight months, and in heavily polluted areas, by up to two years (3). Air pollution causes the deaths of seven million people annually, with half a million premature deaths occurring just in Europe (2), one of the regions currently most affected by climate change (4). The smoke of wildfire alone, releasing carbon dioxide, carbon monoxide, and particulate matter into the atmosphere, is one significant contributor to air pollution (1). Fine particulate matter (PM2.5) in particular poses the greatest public health risk due to its ability to enter deeply into the lungs (1, 5, 6). As witnessed in recent years, wildfire smoke can travel distances far beyond a wildfire itself and its impact on air quality persists long after it (7, 8).
Wildfires are a threat on the rise globally, not least in Europe. The year 2022 witnessed the second-worst wildfire season in Europe and marked the second-largest recorded burnt area in history for the region (4, 9). In the summer of that year, smoke emissions from wildfires were estimated at approximately 6.4 megatons of carbon, marking the highest levels in the past 15 years (10). The year 2023 started with yet new alarming signs whereby the continent witnessed numerous winter and spring fires, spanning from southern Ireland to the Balkan region (4, 9). In Europe, population exposure to wildfire smoke is projected to increase from 10 per 1,000 persons exposed, between 1981 and 2010, to a range of 12 to 20 per 1,000 persons during the years 2071-2100 (11). Globally, future projections indicate that the risk of wildfires will rise by 14% in 2030 and by 50% in 2050 as a result of climate change (12).
Between January and September 2022, wildfires in France consumed over 62,000 hectares of land, six times the average annual figure recorded between 2006 and 2021 (10). The Gironde district in southwestern France, which is the focus of this project, was particularly hard-hit, experiencing the most significant forest loss in the country since 1949, and the smoke emissions from these fires are estimated to have released close to one million metric tons of carbon (13, 14). The effect of those fires on the population has not yet been documented.
Several measures can be conceived to characterize wildfires when measuring their health impact, including data from satellite measurements, air pollution monitoring, and the number and duration of wildfires (15). However, few studies have distinguished pollutants from wildfires only from air pollutants that consist of the same components (15), and studies considering what happens beyond the fire period itself are uncommon (16-24) albeit well motivated as highlighted above. Over the years, focus has also been placed on fires that took place in North America (from the US (18-20, 22, 24-30) and Canada (31-33)) and Australia (23, 34-41), in particular ones that took place in California, US (in 2003, 2007, 2008), Victoria, Australia (in 2002-2003 and 2006-2007), and British Columbia, Canada (in 2003). The literature focuses on short-term effects with a few studies on long-term ones and there are limited studies that examine health outcomes from recent wildfire events (8, 11, 21, 26, 42, 43). The evidence accumulated thus far shows that wildfire smoke affects primarily the respiratory system. This is obvious from studies based on emergency visits and hospital admissions (16, 17, 22-25, 27, 44) as well as from those from outpatient data (28, 31). Emergency care is most often sought for conditions like asthma, bronchitis, dyspnea, and chronic obstructive pulmonary disease (8, 20, 24, 29, 30, 34, 45, 46). There is limited and mixed evidence regarding the effect of wildfire smoke on the cardiovascular system (8, 47), with some studies showing no increase in emergency department visits or hospital admissions (30, 31, 35-38), one reporting a protective effect on hospital care seeking for circulatory conditions, including coronary artery disease (19) and yet other ones an excess risk of out-of-hospital cardiac arrest and outpatient cardiovascular visits (20, 39, 40). Groups at risk have been defined as children (e.g., for asthma), the elderly (e.g., for higher rates of mortality and respiratory hospitalizations), and individuals with underlying respiratory and cardiovascular conditions (8, 25, 48).
The mortality of wildfire smoke is not easy to disentangle from that of air pollutants other than wildfire smoke (16). Yet, albeit some studies found increased particulate matter from wildfires to an increase in overall mortality (38, 41, 49, 50), and others on respiratory and cardiovascular mortality (7, 16), one study indicates that the observed mortality rate during wildfires aligns with the increase in mortality from increased air pollution, regardless of the source, making it challenging to ascertain if increased mortality is specifically attributable to wildfire smoke (51).
This study, focused on the wildfire in the Gironde district in 2022, investigates changes in smoke-related health conditions associated with the fires, when they occur, and shortly after. It considers respiratory and cardiovascular diseases, asthma, and cardiac arrest. It also compares the occurrence of those symptoms for similar calendar period the year prior to the fires.
2. Materials and Methods
2.1. Design
We implemented an ecological study design, utilizing a longitudinal approach to analyze medical records, and focusing on the periods before, during, and after the wildfires.
2.2. Setting
This study was conducted in Gironde, the largest district in the Nouvelle-Aquitaine region of southwestern France, with an area of 10,000 square kilometers and a population of 1,623,749 (52). Within the broader Nouvelle-Aquitaine region, which spans approximately one million hectares, forest areas account for 75% of the land, primarily consisting of maritime pine trees (53). Gironde is characterised by an oceanic climate and, in recent years, it has faced exceptionally warm summers with unprecedented high temperatures (54, 55). In 2022, the frequency of fires in the district was higher than during the past 10 years, leading to the highest recorded forest loss in the country since 1949 (14, 56). Two wildfires erupted on July 12th (in the La Teste-de-Buch) and August 10th (Landiras area) and destroyed a total of 27,000 hectares of forest (10, 57). The former fire occurred in a touristic and peri-urban zone, with large campsites, while the latter one primarily affected a rural area dominated by a forested landscape (53). In total, 46,000 individuals were evacuated, including thousands of tourists (58, 59).
The Gironde district has an Emergency Medical Call Centre (EMCC), called the SAMU33 (Service d’Aide Médicale Urgente de la Gironde), which answers medical emergency calls 24/7. Each days, medical assistants, emergency physicians, and general practitioners provides emergency pre-hospital response and care to local inhabitants and tourists (31, 36).
Air quality assessments made during the summer 2022 wildfires revealed alarming levels of suspended particulate matter that surpassed the region’s alert threshold (60). In response, local health authorities implemented a series of health recommendations (61), including the use of protective filtering masks, limiting traveling and time spent outdoors, and keeping doors and windows closed (61). At-risk individuals with pre-existing respiratory conditions like asthma, chronic respiratory insufficiency, or other respiratory diseases were recommended to seek medical care in the case of exacerbations of symptoms, and, in the case of severe symptoms, to call SAMU33 for immediate assistance (61).
2.3. Data Source and Outcome Definition
Data were retrieved from the EMCC information system. For all emergency calls received, a clinical report is made by a computerised free-text note and updated by medical staff throughout the telephone interactions concerning the case (62). The clinical report informs about the circumstances of the case and indicates the condition for which the call was made. The coding of conditions was based on a combination of the International Classification of Primary Care, version 2, and the International Classification of Diseases, version 10. The structure of the new dictionary also underwent changes during the period of interest. For these reasons, we utilized the plainly expressed call motifs in relation to each code to proceed with the creation of two groups of conditions of interest for our study: respiratory diseases on one hand, within which we isolated a subcategory for asthma, and cardiovascular diseases on the other hand, within which we isolated a subcategory for cardiac arrests. For each outcome, we considered all ages, and for asthma, also for children aged 0-5 years.
2.4. Data Treatment
In this study, two EMCC datasets were extracted corresponding to the years 2021 and 2022 for the period June 1st and October 31st. Extracted information from these datasets included reported smoke-related health complaints, age, and date (day, month, and year). We grouped the count of calls for each condition by date and then manually coded four time intervals : pre-fire, first wildfire, second wildfire, and post-fire. For asthma, age was dichotomized into two categories: children aged 0-5 years and individuals over the age of 5 years.
2.5. Statistical Analyses
We included in the analyses four main periods: pre-fire, first wildfire, second wildfire, and post-fire, using the pre-fire period as the reference one. The same time periods were used for 2022 (the year of the wildfires) and for 2021 (the previous year) to assess whether the patterns observed in 2022 were unique to this particular year. For each period, we compiled the total and daily average numbers of calls and the proportions of calls.
The strength of the association between time period and condition (all ages or age-specific) was measured using odds ratios (ORs) using the pre-fire period as a comparison and their corresponding 95% confidence intervals (CIs) computed with Fisher test. Data analysis was performed with Python version 3.9.7 using SciPy 1.10.
2.6. Ethical Approval
No personal data were needed for this study and all reporting is at the population level. All reports were de-identified which helped prevent breaches in confidentiality, and all data handling and analysis took place in one of the few physical environments authorised by the local authorities to use the data, in the vicinity of the Bordeaux Population Health Research Centre.
This work adheres to the guidelines outlined in Article 65-2 of the amended French Data Protection Act and the General Regulation on the protection of personal data, ensuring the safeguarding of personal health data and privacy. It was approved by the Bordeaux Teaching Hospital committee for ethics and data protection.
3. Results
A total of 353,576 call reports were included in the analysis. It corresponded to 184,020 and 169,556 call reports which were recorded during the selected time periods in 2021 and 2022, respectively. Table 1 presents the distribution of EMCC calls by health complaint for June to October 2022 and 2021. The table provides descriptive statistics for each health outcome of interest, including the total number of health complaint calls and the proportion of calls during each time period.
In 2022, 15,709 call reports were related to respiratory and cardiovascular diseases, asthma, and cardiac arrest (9.3%). Of the total call records, 48,245 (28.5%) calls occurred before the fires, 33,452 (19.7%) during the first fire, 38,142 (22.5%) in the second fire, and 49,717 (29.3%) following the fires. The proportion of calls related to respiratory and cardiovascular diseases, asthma, and cardiac arrest represented 9.6% of calls in the pre-fire period, 8.8% and 8.2% during each of the fires, respectively, and 10.1% in the post-fire period (Table 2). For pediatric asthma, a total of 331 call records were scrutinized, of which 58 (0.1%) calls occurred pre-fire, 26 (0.08%) during the first fire, 37 (0.1%) in the second fire, and 210 (0.4%) post-fire.
We recorded fewer calls related to respiratory diseases during the fires than before, while the number of calls for asthma remained comparable. Following the fires, the proportion of calls for respiratory diseases continued to be lower, while that of calls for asthma slightly rose (0.4%). For cardiovascular diseases, including cardiac arrest, the proportion of calls remained consistent during the first fire and was slightly higher in the second fire and after the fires, compared to the pre-fire period. In 2021, the number of calls related to respiratory diseases was consistently higher throughout similar calendar periods when compared to the pre-fire period in 2022. For asthma and cardiovascular diseases, including cardiac arrest, a similar pattern to the year of the fires persisted.
3.1. Outcome-Specific Associations between Time Periods in 2022 and 2021
Figure 1 presents the outcome-specific associations between the number of calls and fire-related periods in 2022 and 2021, respectively, measured using ORs with their corresponding 95% CIs.
During the year of the fires, there were a 15% and 38% lower number of cases of respiratory diseases during the first fire period (OR = 0.85, 95% CI: 0.79-0.90) and the second one (OR = 0.62, 95% CI: 0.58, 0.67) when compared to the period before the fires, an 11% higher number of cardiovascular cases during the second fire (OR = 1.11, 95% CI: 1.04, 1.20), and an 85% higher number of asthma cases post-fire, all ages aggregated (OR = 1.85, 95% CI: 1.56, 2.21) (Figure 1). For pediatric asthma, children faced significantly higher odds of asthma compared to all ages aggregated after the fires, with more than triple the odds (OR = 3.52, 95% CI: 2.62, 4.80) compared to the pre-fire period.
In 2021, the main difference compared to the year of the fires was the significantly higher number of respiratory disease cases observed across the time periods. Specifically, compared to the reference period, there were 43% and 30% higher numbers of respiratory disease cases during what corresponds to the first fire period in 2022 (OR = 1.43, 95% CI: 1.33, 1.53) and the second one (OR = 1.30, 95% CI: 1.21, 1.40), as well as a 31% higher number of cases in the fall (OR 1.31, 95% CI: 1.22, 1.40). For pediatric asthma, children faced a 57% higher number of cases in the fall (OR = 1.57, 95% CI: 1.21, 2.04), and there was a significantly lower number of asthma cases during the summer of 2021, which was not observed during the year of the fires.
4. Discussion
4.1. Main Findings
In this study, we paid attention to two smoke-related sets of symptoms, pertaining in turn to respiratory conditions, far more reported in the literature at hand, and cardiovascular conditions. We found that, when comparing fire and post-fire periods with the pre-fire one, the number of EMCC calls does not change remarkedly as regards respiratory and cardiovascular diseases in general and asthma and cardiac arrest in particular. There are however a few exceptions, including lower numbers of calls for respiratory symptoms during each active fire period (15% and 38% respectively), an 11% higher number of calls for cardiovascular symptoms during the second fire, and an 85% higher number of asthma cases in the post-fire period all ages aggregated (85% increase) and for children (an odds that tripled). Compared to the previous year, the single most noteworthy difference was the excess number of asthma-related cases post-fires.
As opposed to our study, significant excess risks of respiratory diseases were observed during at least three previous wildfires that took place about 15-20 years ago, including two in California, in 2003 (20, 24) and in 2007 (22, 30), and one in Victoria (Australia) in 2002-2003 (23). In addition, asthma cases stood out as the most prevalent respiratory condition in excess during the fires in California (20, 22, 24, 30) and in another one in North Carolina in 2008 (29), let alone in the pediatric populations (25, 63). In fact, considering a time window of a five-day exposure period pertaining to the fires in California in 2007, emergency department visits for asthma increased by 112% all ages aggregated but as much as by 243% among children aged 0-1 years and by 136% among those aged 0-4 years (25). Similar to our study, consideration of the post-fire period in California (in 2003) revealed that the increase in respiratory outcomes, not least asthma, was greater post than during the fire (20).
When it comes to cardiovascular diseases, the literature at hand remains scarce and also relatively dated. Similar to our study, the 2003 California fire revealed a slight rise in admission rates for overall cardiovascular outcomes during and after the fires (4.4% and 6.1%, respectively) (20). For cardiac arrest in particular, two Australian studies from fires in Victoria in 2006-2007 found elevated numbers of out-of-hospital cardiac arrests during both a 12-day exposure period (23.9%), a rise that was attributed to increased PM2.5 emissions (39), and a 2-day exposure period (7.0%) (40). For their part, investigations of other fires did not reveal any increase in hospital admissions or emergency department visits for cardiovascular outcomes in Australia during fire seasons in Darwin (in 1996-2005, 2000, 2004, and 2005), Sydney (in 1994-2007 and 2001), Newcastle and Wollongong (in 1994-2007) (35-38), British Columbia (Canada) in 2003 (31), and California (the US) in 2007 (30).
4.2. Strengths and Limitations
This study is the first one investigating the health effects of the 2022 Gironde fires. Based on data from the EMCC, which ensures full population coverage and is an integral part of the healthcare system while operating on well-established routines and protocols for coordinating emergency medical services, the study provides a comprehensive picture of reported health complaints at the population level. The inclusion of a post-fire period in the design enhanced our ability to detect health effects that may arise in the aftermath of wildfires or over a longer term, which has received less attention in current studies.
Compared to on-site clinical diagnoses, the use of emergency call data most likely decreases the level of certainty and imprecise categorisation and classification of health symptoms may occur as information about each case is collected over the phone. Further, observed associations may be underestimated as individuals with smoke-sensitivity symptoms may seek care from a general practitioner, potentially resulting in missing cases of interest. Additional methodological limitations pertain to the absence of robust methods to quantify smoke exposure during and after the fires, and the use of smoke exposure measures could potentially have provided more precise health effects of exposure to poor air quality caused by wildfires. As our focus was on over-the-phone emergency assistance data, our results do not lend themselves well to total morbidity and mortality assessments. Earlier studies show an association between wildfires and increased risk of mortality (7), attributable supposedly to air pollution during a fire. We also present the effect of the fire on the population that resides in the Gironde district itself, not in neighbouring municipalities, which may also underestimate some of the potential effects of the fires, during and after. Further, given that many factors come into play to determine the magnitude and nature of the impact of a fire on health (15), the results of this study may also be specific to the situation that prevailed in place and time, i.e., the Gironde district in 2022. Indeed attributes of the fire itself (e.g., size, intensity, and duration), and those of the environment may, in combination play a role in the level of exposure.
4.3. Implications for Research and Practice
The few significant differences in the outcome-specific number of calls observed during the fires in this study may be explained by implemented wildfire prevention and management strategies, such as the evacuation of populations in affected areas, staying indoors, keeping doors and windows closed, and wearing protective face masks. These practices are particularly important from a public health perspective and highlight the need for continued efforts to develop and implement effective interventions to mitigate potential health effects during wildfires. Further, combining multiple data sources, such as emergency call data, hospital visits, and admissions, could provide a more complete understanding of the impact of wildfire smoke exposure on health.
It is also of note to investigate the impact of elevated particulate matter resulting from wildfires on mortality, something that could not be investigated using the emergency data at hand. Several studies on mortality have found different associations with fires from different parts of the world. In Sydney, Australia, smoke events between the years 1994-2007 were associated with a 5% increase in non-accidental mortality and a 10% increase in cardiovascular mortality (41). Further, during two major fire events in 1994 and 2001, also in Sydney, wildfire air pollution was associated with a small increase in all-cause mortality but no associations were found with cardiovascular or respiratory mortality (38). A study on different European regions in 2005 and 2008 revealed that exposure to PM2.5 from wildfires caused tens of hundred of premature deaths with the highest impacts in southern and eastern Europe (49). In Southeast Asia, increases in particulate matter from fires in 1997 were associated with a relative risk of 1.07 in total mortality (50). In contrast to these findings, a study investigating population exposure to smoke from East European fires in Finland in 2002 found no significant associations in daily all cause-mortality (51).
Wildfire smoke exposures are becoming increasingly acknowledged as a significant public health concern and have been a long-standing issue in public policy (16). Numerous challenges need to be addressed to fully comprehend the impact of wildfire smoke on human health, including comprehensive exposure assessments to assess potential increases in morbidity and mortality during wildfire smoke exposure (16). Enhancing health outcomes at the population level during and after wildfire events is a crucial priority and could identify valuable implemented prevention practices that effectively address health concerns, while also shedding light on critical areas for improvement (16, 21). The level of exposure, depending on the unique characteristics of each fire, should be taken into consideration both in surrounding areas and at a regional scale (64).
The findings of this study make a useful contribution to understanding the variation in emergency call volume and characteristics before, during, and shortly after wildfires and the use of emergency call data could serve as a sensitive outcome indicator to reflect certain acute health effects.
5. Conclusions
This study highlights that the number of emergency calls for smoke-related symptoms appears to vary by time period, with different symptoms exhibiting varying risks during and following the two executive fires in 2022. Noteworthy, a higher number of asthma cases was found after the fires, with the highest increase observed in pediatric cases, compared to the period before the fires. Comparable associations in the number of emergency calls for the same smoke-related symptoms were identified across the calendar periods in 2022 and 2021. Whether the effects are smoke- or seasonal-related remains to be determined. Thus, further research is warranted to better understand these findings.
References
- Organization, WH. Wildfires [Internet]: World Health Organization; [date unknown]. Available online: https://www.who.int/health-topics/wildfires#tab=tab_1.
- Forecasts ECfM-RW. Air quality, climate change and public health [Internet]: European Centre for Medium-Range Weather Forecasts; [date unknown]. Available online: https://stories.ecmwf.int/air-quality-climate-change-and-public-health/index.html.
- Copernicus. Air quality [Internet]: Copernicus; [date unknown]. Available online: https://atmosphere.copernicus.eu/air-quality.
- ESOTC 2022 Europe Wildfires [Internet] [date unknown]. Available online: https://climate.copernicus.eu/esotc/2022/wildfires.
- Agency USEP. Why Wildfire Smoke is a Health Concern [Internet]: United States Environmental Protection Agency; 2022. Available online: https://www.epa.gov/wildfire-smoke-course/why-wildfire-smoke-health-concern.
- Agency USEP. Health and Environmental Effects of Particulate Matter (PM) [Internet]: United States Environmental Protection Agency; 2022. Available online: https://www.epa.gov/pm-pollution/health-and-environmental-effects-particulate-matter-pm.
- Chen, G.; Guo, Y.; Yue, X.; Tong, S.; Gasparrini, A.; Bell, M.L.; et al. Mortality risk attributable to wildfire-related PM2·5 pollution: a global time series study in 749 locations. Lancet Planet. Health 2021, 5, e579–e87. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Yu, P.; Abramson, M.J.; Johnston, F.H.; Samet, J.M.; Bell, M.L.; et al. Wildfires, Global Climate Change, and Human Health. N. Engl. J. Med. 2020, 383, 2173–2181. [Google Scholar] [CrossRef] [PubMed]
- How the EU is preparing for the 2023 wildfire season [Internet]: European Civil Protection and Humanitarian Aid Operations; 2023. Available online: https://civil-protection-humanitarian-aid.ec.europa.eu/news-stories/stories/how-eu-preparing-2023-wildfire-season_en.
- Service CAM. Euorpe´s summer wildfire emissions highest in 15 years [Internet]: Euorpe´s summer wildfire emissions highest in 15 years [Internet]; 2022. Available online: https://atmosphere.copernicus.eu/europes-summer-wildfire-emissions-highest-15-years.
- Grant, E.; Runkle, J.D. Long-term health effects of wildfire exposure: A scoping review. J. Clim. Chang. Health 2022, 6, 100110. [Google Scholar] [CrossRef]
- Programme UNE. Number of wildfires to rise by 50% by 2100 and governments are not prepared, experts warn [Internet]: United Nations Environment Programme; 2022. Available online: https://www.unep.org/news-and-stories/press-release/number-wildfires-rise-50-2100-and-governments-are-not-prepared.
- EGUsphere. Impact of Landes forest fires on air quality in France during the summer 2022 [Internet]: EGUsphere; 2023. Available online: https://egusphere.copernicus.org/preprints/2023/egusphere-2023-421/egusphere-2023-421.pdf.
- Monde, L. France's unprecedented summer of wildfires, in maps and graphs [Internet]: Le Monde; 2022. Available online: https://www.lemonde.fr/en/les-decodeurs/article/2022/08/25/fires-in-france-maps-and-graphs-to-visualize-an-unprecedented-summer_5994672_8.html.
- Youssouf, H.; Liousse, C.; Roblou, L.; Assamoi, E.M.; Salonen, R.O.; Maesano, C.; et al. Quantifying wildfires exposure for investigating health-related effects. Atmos. Environ. 1994 2014, 97, 239–251. [Google Scholar] [CrossRef]
- Black, C.; Tesfaigzi, Y.; Bassein, J.A.; Miller, L.A. Wildfire smoke exposure and human health: Significant gaps in research for a growing public health issue. Environ. Toxicol. Pharmacol. 2017, 55, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Borchers Arriagada, N.; Horsley, J.A.; Palmer, A.J.; Morgan, G.G.; Tham, R.; Johnston, F.H. Association between fire smoke fine particulate matter and asthma-related outcomes: Systematic review and meta-analysis. Environ. Res. 2019, 179 Pt A, 108777. [Google Scholar] [CrossRef]
- Navarro, K.M.; Kleinman, M.T.; Mackay, C.E.; Reinhardt, T.E.; Balmes, J.R.; Broyles, G.A.; et al. Wildland firefighter smoke exposure and risk of lung cancer and cardiovascular disease mortality. Environ. Res. 2019, 173, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-S.; Falter, K.; Meyer, P.; Mott, J.; Gwynn, C. Risk factors associated with clinic visits during the 1999 forest fires near the Hoopa Valley Indian Reservation, California, USA. Int. J. Environ. Health Res. 2009, 19, 315–327. [Google Scholar] [CrossRef]
- Delfino, R.J.; Brummel, S.; Wu, J.; Stern, H.; Ostro, B.; Lipsett, M.; et al. The relationship of respiratory and cardiovascular hospital admissions to the southern California wildfires of 2003. Occup. Environ. Med. 2009, 66, 189–197. [Google Scholar] [CrossRef]
- Finlay, S.E.; Moffat, A.; Gazzard, R.; Baker, D.; Murray, V. Health impacts of wildfires. PLoS Curr. 2012, 4, e4f959951cce2c. [Google Scholar] [CrossRef]
- Dohrenwend, P.B.; Le, M.V.; Bush, J.A.; Thomas, C.F. The impact on emergency department visits for respiratory illness during the southern california wildfires. West. J. Emerg. Med. 2013, 14, 79–84. [Google Scholar] [CrossRef]
- Tham, R.; Erbas, B.; Akram, M.; Dennekamp, M.; Abramson, M.J. The impact of smoke on respiratory hospital outcomes during the 2002-2003 bushfire season, Victoria, Australia. Respirology 2009, 14, 69–75. [Google Scholar] [CrossRef]
- Viswanathan, S.; Eria, L.; Diunugala, N.; Johnson, J.; McClean, C. An Analysis of Effects of San Diego Wildfire on Ambient Air Quality. J. Air Waste Manag. Assoc. 1995 2006, 56, 56–67. [Google Scholar] [CrossRef]
- Hutchinson, J.A.; Vargo, J.; Milet, M.; French, N.H.F.; Billmire, M.; Johnson, J.; et al. The San Diego 2007 wildfires and Medi-Cal emergency department presentations, inpatient hospitalizations, and outpatient visits: An observational study of smoke exposure periods and a bidirectional case-crossover analysis. PLoS Med. 2018, 15, e1002601. [Google Scholar] [CrossRef]
- Reid, C.E.; Maestas, M.M. Wildfire smoke exposure under climate change: impact on respiratory health of affected communities. Curr. Opin. Pulm. Med. 2019, 25, 179–187. [Google Scholar] [CrossRef]
- Liu, J.C.; Wilson, A.; Mickley, L.J.; Dominici, F.; Ebisu, K.; Wang, Y.; et al. Wildfire-specific Fine Particulate Matter and Risk of Hospital Admissions in Urban and Rural Counties. Epidemiology 2017, 28, 77–85. [Google Scholar] [CrossRef]
- Kunzli, N.; Avol, E.; Wu, J.; Gauderman, W.J.; Rappaport, E.; Millstein, J.; et al. Health Effects of the 2003 Southern California Wildfires on Children. Am. J. Respir. Crit. Care Med. 2006, 174, 1221–1228. [Google Scholar] [CrossRef]
- Rappold, A.G.; Cascio, W.E.; Kilaru, V.J.; Stone, S.L.; Neas, L.M.; Devlin, R.B.; et al. Cardio-respiratory outcomes associated with exposure to wildfire smoke are modified by measures of community health. Environ. Health 2012, 11, 71. [Google Scholar] [CrossRef] [PubMed]
- Schranz, C.I.; Castillo, E.M.; Vilke, G.M. The 2007 San Diego Wildfire Impact on the Emergency Department of the University of California, San Diego Hospital System. Prehospital Disaster Med. 2010, 25, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.B.; Brauer, M.; MacNab, Y.C.; Kennedy, S.M. Three Measures of Forest Fire Smoke Exposure and Their Associations with Respiratory and Cardiovascular Health Outcomes in a Population-Based Cohort. Environ. Health Perspect. 2011, 119, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Copes, R.; Fisk, R.; Joy, R.; Chan, K.; Brauer, M. Population Health Effects of Air Quality Changes Due to Forest Fires in British Columbia in 2003: Estimates from Physician-visit Billing Data. Can. J. Public Health 2006, 97, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Elliott, C.T.; Henderson, S.B.; Wan, V. Time series analysis of fine particulate matter and asthma reliever dispensations in populations affected by forest fires. Environ. Health 2013, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H.; Kavanagh, A.M.; Bowman, D.M.J.S.; Scott, R.K. Exposure to bushfire smoke and asthma: an ecological study. Med. J. Aust. 2002, 176, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Hanigan, I.C.; Johnston, F.H.; Morgan, G.G. Vegetation fire smoke, indigenous status and cardio-respiratory hospital admissions in Darwin, Australia, 1996-2005: a time-series study. Environ. Health 2008, 7, 42. [Google Scholar]
- Johnston, F.H.; Bailie, R.S.; Pilotto, L.S.; Hanigan, I.C. Ambient biomass smoke and cardio-respiratory hospital admissions in Darwin, Australia. BMC Public Health 2007, 7, 240. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.L.; Hanigan, I.C.; Morgan, G.G.; Henderson, S.B.; Johnston, F.H. Air pollution from bushfires and their association with hospital admissions in Sydney, Newcastle and Wollongong, Australia 1994–2007. Aust. N. Zealand J. Public Health 2013, 37, 238–243. [Google Scholar] [CrossRef]
- Morgan, G.; Sheppeard, V.; Khalaj, B.; Ayyar, A.; Lincoln, D.; Jalaludin, B.; et al. Effects of Bushfire Smoke on Daily Mortality and Hospital Admissions in Sydney, Australia. Epidemiology 2010, 21, 47–55. [Google Scholar] [CrossRef]
- Dennekamp, M.; Straney, L.D.; Erbas, B.; Abramson, M.J.; Keywood, M.; Smith, K.; et al. Forest Fire Smoke Exposures and Out-of-Hospital Cardiac Arrests in Melbourne, Australia: A Case-Crossover Study. Environ. Health Perspect. 2015, 123, 959. [Google Scholar] [CrossRef]
- Haikerwal, A.; Akram, M.; Del Monaco, A.; Smith, K.; Sim, M.R.; Meyer, M.; et al. Impact of Fine Particulate Matter (PM2.5) Exposure During Wildfires on Cardiovascular Health Outcomes. J. Am. Heart Assoc. 2015, 4. [Google Scholar] [CrossRef]
- Johnston, F.; Hanigan, I.; Henderson, S.; Morgan, G.; Bowman, D. Extreme air pollution events from bushfires and dust storms and their association with mortality in Sydney, Australia 1994–2007. Environ. Res. 2011, 111, 811–816. [Google Scholar] [CrossRef]
- Cohen, O.; Shapira, S.; Furman, E. Long-Term Health Impacts of Wildfire Exposure: A Retrospective Study Exploring Hospitalization Dynamics Following the 2016 Wave of Fires in Israel. Int. J. Environ. Res. Public Health 2022, 19, 5012. [Google Scholar] [CrossRef]
- Gao, Y.; Huang, W.; Yu, P.; Xu, R.; Yang, Z.; Gasevic, D.; et al. Long-term impacts of non-occupational wildfire exposure on human health: A systematic review. Environ. Pollut. 2023, 320, 121041. [Google Scholar] [CrossRef] [PubMed]
- Romanello, M.; Di Napoli, C.; Drummond, P.; Green, C.; Kennard, H.; Lampard, P.; et al. The 2022 report of the Lancet Countdown on health and climate change: health at the mercy of fossil fuels. Lancet 2022, 400, 1619–1654. [Google Scholar] [PubMed]
- Chew, F.T.; Ooi, B.C.; Hui, J.K.S.; Saharom, R.; Goh, D.Y.T.; Lee, B.W. Singapore's haze and acute asthma in children. Lancet 1995, 346, 1427. [Google Scholar] [CrossRef]
- Dennekamp, M.; Abramson, M.J. The effects of bushfire smoke on respiratory health. Respirology 2011, 16, 198–209. [Google Scholar] [CrossRef]
- Chen, H.; Samet, J.M.; Bromberg, P.A.; Tong, H. Cardiovascular health impacts of wildfire smoke exposure. Part. Fibre Toxicol. 2021, 18, 2–22. [Google Scholar] [CrossRef] [PubMed]
- Reid, C.E.; Brauer, M.; Johnston, F.H.; Jerrett, M.; Balmes, J.R.; Elliott, C.T. Critical Review of Health Impacts of Wildfire Smoke Exposure. Environ. Health Perspect. 2016, 124, 1334–1343. [Google Scholar] [CrossRef] [PubMed]
- Kollanus, V.; Prank, M.; Gens, A.; Soares, J.; Vira, J.; Kukkonen, J.; et al. Mortality due to Vegetation Fire-Originated PM2.5 Exposure in Europe-Assessment for the Years 2005 and 2008. Environ. Health Perspect. 2017, 125, 30–37. [Google Scholar] [CrossRef]
- Sastry, N. Forest Fires, Air Pollution, and Mortality in Southeast Asia. Demography 2002, 39, 1–23. [Google Scholar] [CrossRef]
- Hänninen, O.O.; Salonen, R.O.; Koistinen, K.; Lanki, T.; Barregard, L.; Jantunen, M. Population exposure to fine particles and estimated excess mortality in Finland from an East European wildfire episode. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 414–422. [Google Scholar] [CrossRef]
- Wikipedia. Gironde [Internet]: Wikipedia. Available online: https://en.wikipedia.org/wiki/Gironde.
- FIRE-RES. 2022 Summer fires in the Living Lab in Nouvelle Aquitaine, France 2022: FIRE-RES; 2022. Available online: https://fire-res.eu/2022-summer-fires-in-the-living-lab-in-nouvelle-aquitaine-france/.
- Gironde, France Climate [Internet]: Weather and Climate; [date unknown]. Available online: https://tcktcktck.org/france/gironde.
- Méheut, C. Scenes of Devastation Emerge From a Fire-Ravaged Southwestern France [Internet] 2022. Available online: https://www.nytimes.com/2022/07/19/world/europe/france-wildfires-europe-heat-wave.html.
- Watch, G.F. France, Nouvelle-Aquitaine, Gironde [Internet]: Global Forest Watch; [date unknown]. Available online: https://www.globalforestwatch.org/dashboards/country/FRA/10/7/?category=fires&dashboardPrompts=eyJzaG93UHJvbXB0cyI6dHJ1ZSwicHJvbXB0c1ZpZXdlZCI6WyJkb3dubG9hZERhc2hib2FyZFN0YXRzIiwid2lkZ2V0U2V0dGluZ3MiXSwic2V0dGluZ3MiOnsic2hvd1Byb21wdHMiOnRydWUsInByb21wdHNWaWV3ZWQiOlsiZG93bmxvYWREYXNoYm9hcmRTdGF0cyJdLCJzZXR0aW5ncyI6eyJzaG93UHJvbXB0cyI6dHJ1ZSwicHJvbXB0c1ZpZXdlZCI6W10sInNldHRpbmdzIjp7Im9wZW4iOmZhbHNlLCJzdGVwSW5kZXgiOjAsInN0ZXBzS2V5IjoiIn0sIm9wZW4iOnRydWUsInN0ZXBJbmRleCI6MCwic3RlcHNLZXkiOiJkb3dubG9hZERhc2hib2FyZFN0YXRzIn0sIm9wZW4iOnRydWUsInN0ZXBJbmRleCI6MCwic3RlcHNLZXkiOiJ3aWRnZXRTZXR0aW5ncyJ9LCJzdGVwc0tleSI6IndpZGdldFNldHRpbmdzIiwiZm9yY2UiOnRydWV9&location=WyJjb3VudHJ5IiwiRlJBIiwiMTAiLCI3Il0%3D&map=eyJjZW50ZXIiOnsibGF0Ijo0NC44ODc0NTc1MDQzMjE4MywibG5nIjotMC40NzMwOTc2MTk5OTc5OTQ4fSwiem9vbSI6Ni45NDUwNzk5ODE0OTgzMzcsImNhbkJvdW5kIjpmYWxzZSwiZGF0YXNldHMiOlt7ImRhdGFzZXQiOiJwb2xpdGljYWwtYm91bmRhcmllcyIsImxheWVycyI6WyJkaXNwdXRlZC1wb2xpdGljYWwtYm91bmRhcmllcyIsInBvbGl0aWNhbC1ib3VuZGFyaWVzIl0sImJvdW5kYXJ5Ijp0cnVlLCJvcGFjaXR5IjoxLCJ2aXNpYmlsaXR5Ijp0cnVlfSx7ImRhdGFzZXQiOiJmaXJlLWFsZXJ0cy12aWlycyIsImxheWVycyI6WyJmaXJlLWFsZXJ0cy12aWlycyJdLCJvcGFjaXR5IjoxLCJ2aXNpYmlsaXR5Ijp0cnVlLCJwYXJhbXMiOnsidmlzaWJpbGl0eSI6dHJ1ZSwiYWRtX2xldmVsIjoiYWRtMiJ9LCJ0aW1lbGluZVBhcmFtcyI6eyJzdGFydERhdGVBYnNvbHV0ZSI6IjIwMjMtMDItMjUiLCJlbmREYXRlQWJzb2x1dGUiOiIyMDIzLTA1LTI1Iiwic3RhcnREYXRlIjoiMjAyMy0wMi0yNSIsImVuZERhdGUiOiIyMDIzLTA1LTI1IiwidHJpbUVuZERhdGUiOiIyMDIzLTA1LTI1In19XX0%3D&showMap=true.
- A-M S, S S, Wagemann, F F. Summer 2022: exceptional wildfire season in Europe [Internet]: European Organisation for the Exploitation of Meteorological Satellites; 2022. Available online: https://www.eumetsat.int/summer-2022-exceptional-wildfire-season-europe.
- 2022 European and Mediterranean wildfires [Internet]: Wikipedia; 2022. Available online: https://en.wikipedia.org/wiki/2022_European_and_Mediterranean_wildfires#cite_note-13.
- France: Emergency crews responding to wildfires in Gironde Department as of [Internet]: Crisis24; 2022. 13 July. Available online: https://crisis24.garda.com/alerts/2022/07/france-emergency-crews-responding-to-wildfires-in-gironde-department-as-of-july-13.
- Nouvelle-Aquitaine, A. Communiqué de presse - Feux de forêt en Gironde : recommandations sanitaires aux populations du 22 juillet 2022 2022. Available online: https://www.nouvelle-aquitaine.ars.sante.fr/communique-de-presse-feux-de-foret-en-gironde-recommandations-sanitaires-aux-populations-du-22.
- Nouvelle-Aquitaine, A. Feux de forêts - Impact sanitaire et recommandations 2023. Available online: https://www.nouvelle-aquitaine.ars.sante.fr/feux-de-forets-impact-sanitaire-et-recommandations.
- Gil-Jardine, C.; Chenais, G.; Pradeau, C.; Tentillier, E.; Revel, P.; Combes, X.; et al. Trends in reasons for emergency calls during the COVID-19 crisis in the department of Gironde, France using artificial neural network for natural language classification. Scandinavian journal of trauma, resuscitation and emergency medicine. 2021, 29, 55. [Google Scholar] [CrossRef] [PubMed]
- Holm, S.M.; Miller, M.D.; Balmes, J.R. Health effects of wildfire smoke in children and public health tools: a narrative review. J. Expo. Sci. Environ. Epidemiol. 2021, 31, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Wildland Fire Research: Health Effects Research [Internet]: United States Environmental Protection Agency; 2023. Available online: https://www.epa.gov/air-research/wildland-fire-research-health-effects-research.
Figure 1.
Outcome-specific associations between periods during and after the wildfires with the pre-fire period as the reference, in 2022 and 2021.
Figure 1.
Outcome-specific associations between periods during and after the wildfires with the pre-fire period as the reference, in 2022 and 2021.
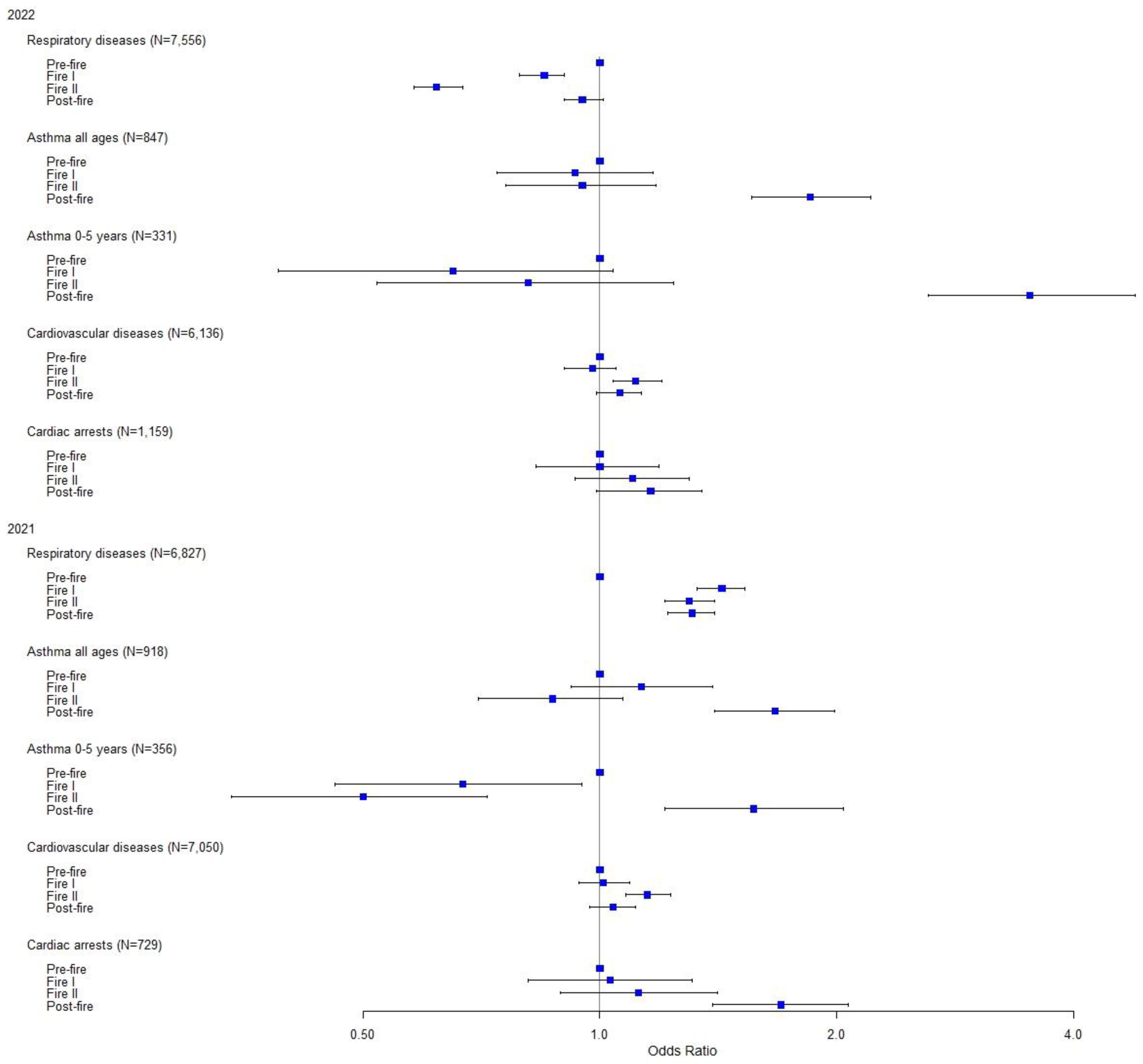

Table 1.
Distribution of the EMCC calls by health complaint and periods before, during, and after the wildfires in 2022 and during these time periods in 2021.
Table 1.
Distribution of the EMCC calls by health complaint and periods before, during, and after the wildfires in 2022 and during these time periods in 2021.
| EMCC Calls | Pre-Fire Period 1/6 - 11/7 |
Fire Period I 12/7 - 9/8 |
Fire Period II 10/8 - 15/9 |
Post-fire Period 16/9 - 31/10 |
||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| 2022 | ||||||||
| Respiratory diseases | 2,457 | 5.1 | 1,453 | 4.3 | 1,233 | 3.2 | 2,413 | 4.9 |
| Asthma all ages (0-5 yrs) | 197 (58) | 0.4 (0.1) | 127 (26) | 0.4 (0.08) | 148 (37) | 0.4 (0.1) | 375 (210) | 0.8 (0.4) |
| Cardiovascular diseases | 1,684 | 3.5 | 1,141 | 3.4 | 1,478 | 3.9 | 1,833 | 3.7 |
| Cardiac arrests | 309 | 0.6 | 214 | 0.6 | 268 | 0.7 | 368 | 0.7 |
| Other | 43,598 | 90.4 | 30,517 | 91.2 | 35,015 | 91.8 | 44,728 | 89.9 |
| Total | 48,245 | 100.0 | 33,452 | 100.0 | 38,142 | 100.0 | 49,717 | 100.0 |
| 2021 | ||||||||
| Respiratory diseases | 1,484 | 3.0 | 1,599 | 4.2 | 1,675 | 3.8 | 2,069 | 3.9 |
| Asthma all ages (0-5 yrs) | 208 (98) | 0.4 (0.2) | 180 (50) | 0.5 (0.1) | 158 (43) | 0.4 (0.1) | 372 (165) | 0.7 (0.3) |
| Cardiovascular diseases | 1,814 | 3.7 | 1,401 | 3.7 | 1,820 | 4.2 | 2,015 | 3.8 |
| Cardiac arrests | 159 | 0.3 | 125 | 0.3 | 156 | 0.4 | 289 | 0.5 |
| Other | 45,860 | 92.6 | 34,562 | 91.3 | 39,619 | 91.2 | 48,455 | 91.1 |
| Total | 49,525 | 100.0 | 37,867 | 100.0 | 43,428 | 100.0 | 53,200 | 100.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



