
Submitted:
01 November 2023
Posted:
03 November 2023
You are already at the latest version
Abstract
Although child-centred care is increasingly referred to within the nursing literature, a clear definition of child-centred care and clarity around the concept is yet to be achieved. The objectives of this review were to examine: 1) What constitutes the concept of child-centred care in healthcare? 2) How has the concept of child-centred care developed? 3) What is the applicability of child-centred care and what are its limitations? and 4) How does the concept of child-centred care benefit and inform children’s healthcare? In total, 2984 papers were imported for screening, following removal of duplicates and screening, 21 papers were included in the scoping review.The findings suggest that child-centred care is an emerging, ambiguous, poorly defined concept; no clear consensus exists about what constitutes child-centred care. Although it seems antithetical to argue against child-centred care, little robust evidence was identified that demonstrates the impact of, and benefit from, child-centred care. If child-centred care is to be a sustainable, convincing model to guide practice and compete with other models of care it needs to establish robust evidence of its effectiveness, impact on children and their families as well as the wider impacts on the healthcare system.
Keywords:
child-centred care
; agency
; participations
; decision making
; communication
; impact
1. Introduction
The position of children in healthcare reflects their changing and evolving positioning in society more broadly [1]. The concept of child-centred care orientates children to a more central position within children’s health care, where the child is at the centre of thinking and practice [1,2,3].
The concept of child-centred care adds to the different notions or concepts of centredness used to describe the focus of health care in general as well as health care for children and young people [4]. These include person- (and patient-) centred care, family-centred care (FCC) and various (and perhaps confounding) combinations of these. The precise meanings of each are subject to confusion and misunderstanding as well as uncertainties. Reactions or responses to societal shifts can be seen as the drivers for these different concepts. The different terms are considered in the following section.
The term ‘person-centred care’ (PCC) evolved from the term ‘patient-centred care’ and is defined as a holistic approach to care that is respectful and individualised, that includes negotiation of care, choice and where persons receiving care are empowered to be involved in health decisions at the level they choose [4]. PCC was described in the mid-20th century when there was the call to understand the patient as a whole person. It is informed by the work of Carl Rogers from the 1940s around client-centred psychotherapy and the physician Enid Balint in the 1960s who described the concept of patient-centred care in the context of the physician and patient relationship [5]. Also linked to the patient rights movement of the 1960s, PCC reflects a rejection of the paternalistic medical model of physician dominance (Nolte et al., 2020). Key attributes of PCC are that patients should be treated as individuals and with respect and dignity, and that their needs, wants, and preferences are included in care planning [5]. In PCC the focus is on the individual—an adult with autonomy [4] and PCC has been seen to typically, or traditionally, refer to adults rather than children with a strong representation within mental health care, older person and dementia care literature [4].
In the context of children’s health care, FCC recognises that children need to be cared for in the context of their family, that families are the constant in the child’s life and the family’s values and priorities should be central in the plan of care for the child [6]. The theoretical origins of FCC came from the understanding of child attachment theories emanating from the work of people such as David Winnicott, John Bowlby and James and Joyce Robertson on the effects of children’s separation from their mother and the effects of hospitalisation on children [2]. The Platt Report [7] investigated the care of children in hospital in Britain and recommendations from this report have also had a significant influence on changes to care practices. Where parents were largely excluded from children’s hospital wards in the 19th and first part of the 20th century, there have been incremental changes towards acceptance of parents, their presence and partnership [2].
The intent of FCC is a more equal partnership between health professionals and parents in the child’s health care. In FCC, the family is the unit of care [8] and FCC involves healthcare providers working in partnership with families and care of the child is in the context of their family [3].
Key attributes of FCC are collaboration, communication, negotiation and support [4]. Building trust, listening to parents’ concerns and valuing parents’ knowledge of their child are also recognised attributes of FCC. These factors, however, focus on adults—the parents and health professionals rather than the child. FCC is described as having been a preferred approach to children’s health care for some decades, however, complex issues have been identified that compromise the effectiveness and implementation of this model including relationship and attitudinal and resource factors [2,8].
Current constructions of childhood that lie within an emancipatory, rights-based and participatory paradigm have been major drivers in the development of the concept of child-centred care [9,10]. Child-centred care in health care reflects the broader societal view of children’s rights that is framed by the UN Convention on the Rights of the Child [11]. The approach recognises children as social actors both in their own right and as active participants in their care and the theoretical origins lie with the new sociology of childhood [12].
Rather than a model that provides a method or recipe for achieving child-centredness, child-centred care is seen as an approach or philosophy that underpins and informs children’s health care. The approach places children at the centre of health care practice and, where able, children and young people are included as active participants in their care and decision making [2,4]. Child-centred approaches recognise that children and young people experience illness and disability differently to adults and that their health care needs are different to those of adults [2]. The premise that the best interests of the child should be the paramount consideration underpins the approach [2]. In child-centred care the central role of parents and families in relationships and interactions continues to be acknowledged [2,4].
The difference between child-centred care and FCC is one of emphasis based upon the extent to which children’s interests are highlighted or prioritised in the planning and delivery of care [13]. In child-centred care the focus is on the child in the context of their family. FCC views the family as a unit [4] and the focus tends to be primarily on the parents, with the child’s perspectives secondary [2,14]. In FCC parents and health professionals are the recognised active members and children and young people are allocated a more passive and less prominent role [1,15]. Child-centred care acknowledges the need to specifically focus on children and young people. It also recognises that their views and concerns are not necessarily the same as those of parents/carers or health care providers [2,15,16].
PCC and child-centred care have more similar attributes than child-centred care and FCC. [4]. These commonalities include competence, values, own needs and participation as active participants [4].
Although the concept of child-centred care is increasingly referred to in health care literature, particularly within the nursing literature, a clear definition of child-centred care and clarity around the concept is yet to be achieved and further work is needed in developing the definition [15,17].
Aims and objectives
The aim of this scoping review is to identify the concept of child-centred care in healthcare, to provide clarity on the concept of child-centred care, and to evaluate its application/appropriateness.
The objectives of this review are to examine:
- What constitutes the concept of child-centred care in healthcare?
- How has the concept of child-centred care developed?
- What is the applicability of child-centred care and what are its limitations?
- How does the concept of child-centred care benefit and inform children’s healthcare?
2. Methods
The scoping review protocol was published [17]. This scoping review was designed with the intention of evaluating the concept of child-centered care in healthcare in order to achieve clarity on the concept and its applicability, benefits, and potential to inform the evidence base of children’s healthcare, policy and practice. To achieve this aim, a literature review method was adopted, using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) approach [18,19,20].
As this was a scoping review no ethics approval was required.
Inclusion criteria
In a scoping review, it is important to establish inclusion criteria to determine which studies are eligible for inclusion in the review [19]. In this case, the context of included studies was those related to any setting where healthcare may be provided (e.g., in-patient and out-patient settings; tertiary, secondary and primary care setting; respite and hospice settings; medical home, home-based care and school settings) [17]. The types of studies included in this review include peer reviewed papers and opinion papers. In light of the complex nature of this scoping review that addresses the development of the concept of child-centred care, the decision was made not to include documents related to policy documents from governments, healthcare organisations, professional bodies, and consumer advocacy groups.
Search strategy
Several databases (CINAHL, MEDLINE, Web of Science) were searched using a combination of terms. Studies were restricted to English language with a date range of 1990-2021. The year 1990 was chosen as the cut-off date as this is the point at which the concept of CCC in healthcare appears in the literature. Peer-reviewed literature, as well as some grey literature and dissertations, were eligible for inclusion in the study. Search terms included: (child+ OR adolescence+) OR (child OR children OR adolescent); adolescent health services OR child health services+ or family centered care+ OR patient centered care+; (child* centered OR child* centered OR child* rights OR child* perspective OR child* voice OR child* view OR child* participation OR child* involvement) OR patient autonomy OR decision making, patient+ OR decision making, family OR patient rights+; and combinations of these searches.
Screening and eligibility
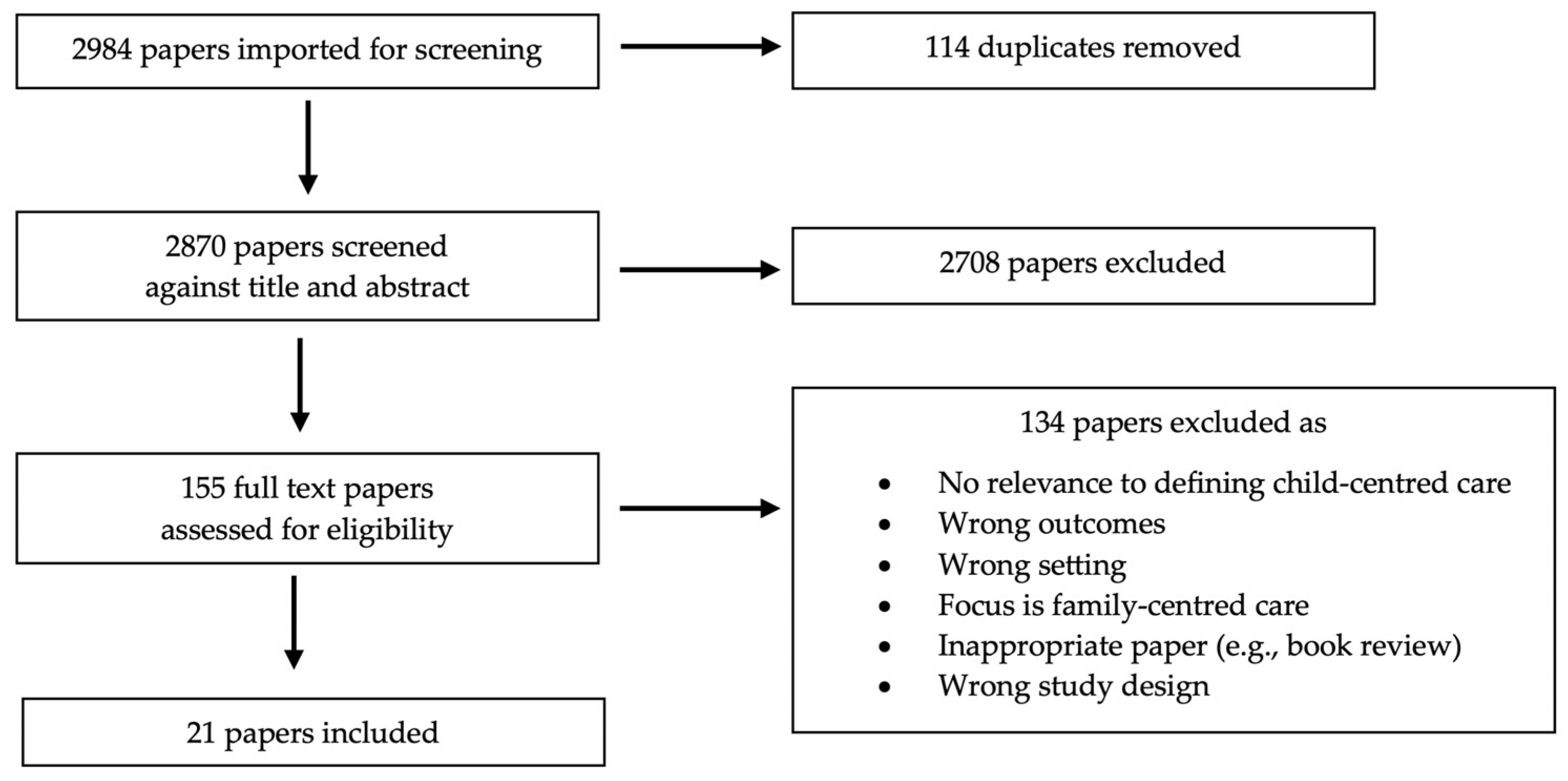
From the three databases, 2984 results were retrieved and exported to Covidence®, and after automatic removal of 114 duplicates, 2870 records remained. The titles and abstracts of these records were assessed against the inclusion criteria listed above. All abstracts and metadata were imported into Covidence® to facilitate the implementation of the PRISMA-ScR screening approach (see Figure 1). Of the 155 papers remaining after title/abstract screening, 134 were excluded after full-text review, leaving 21 papers for inclusion. Three authors (SY, KF, BC) participated in the abstract/title screening process, and three authors (SC, KF, BC) participated in the full-text review process. The validity of the papers included in the full-text review was assessed against the following three eligibility criteria:
- The focus of the paper was adequately on child-centred care and not FCC;
- There was sufficient content relevant to defining child-centred care on a practical or conceptual level, including papers who may not have used the term child-centered care but whose content was relevant to the germinal concept of child-centred care; and
- The outcomes and setting were relevant to this scoping review.
If the three above criteria were met, the paper was retained. Figure 1 shows the flow of papers through the review process.
Data extraction and charting
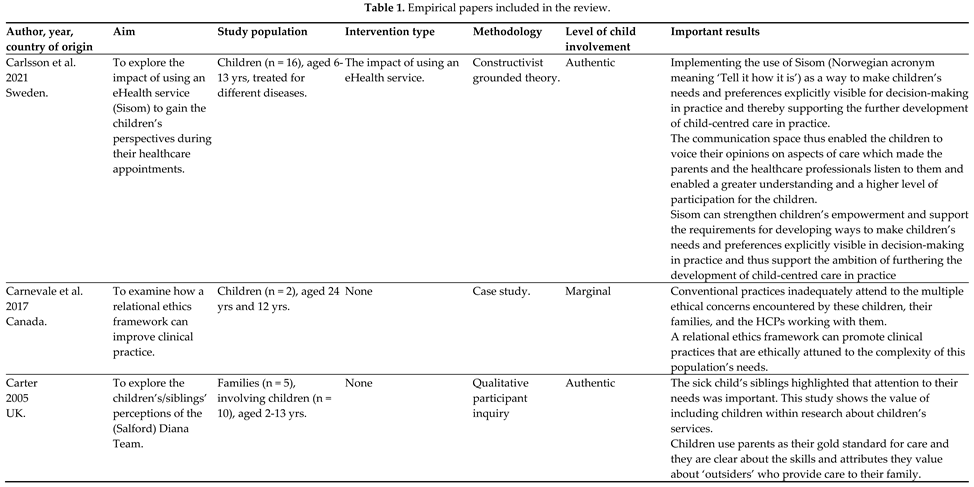
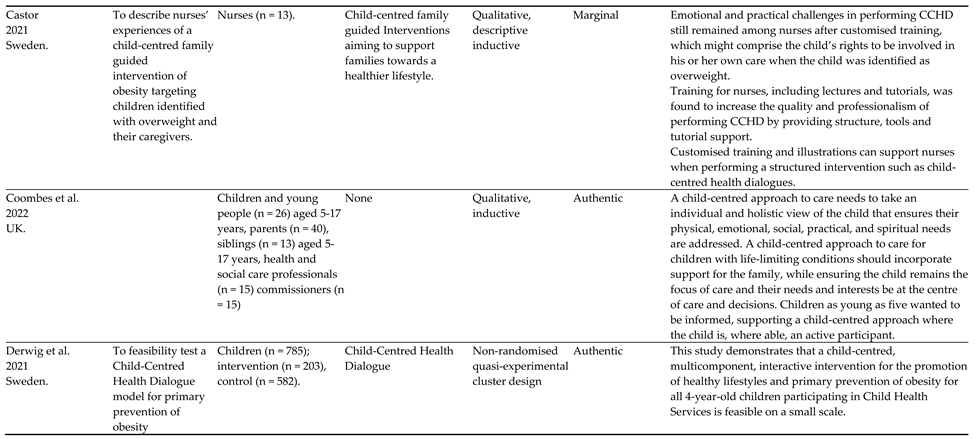
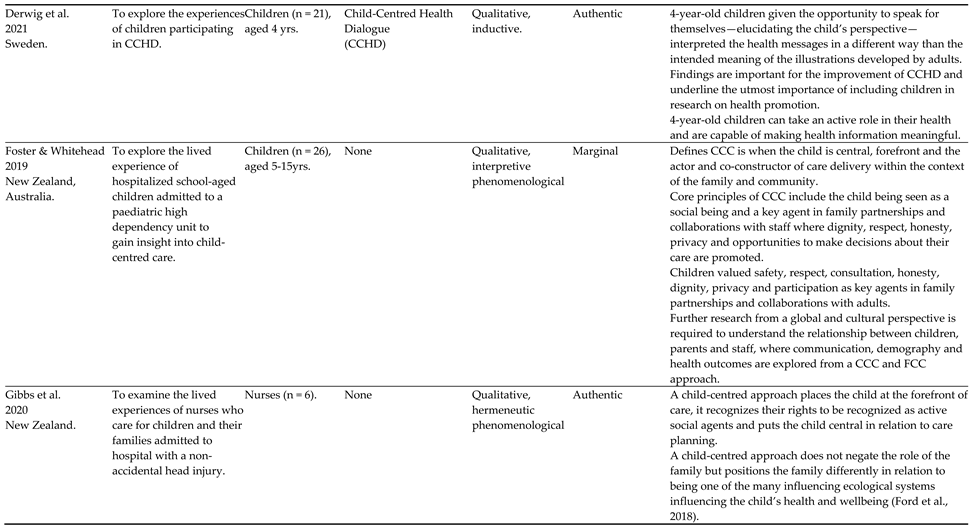
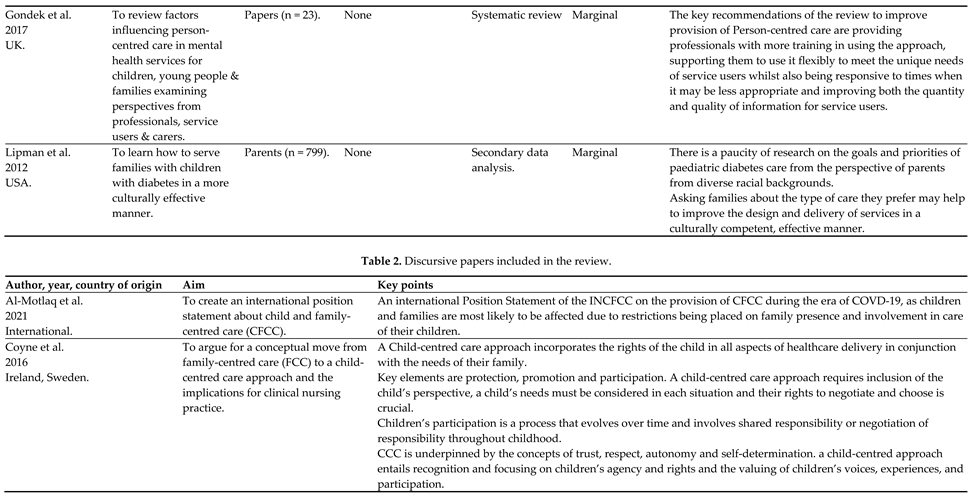
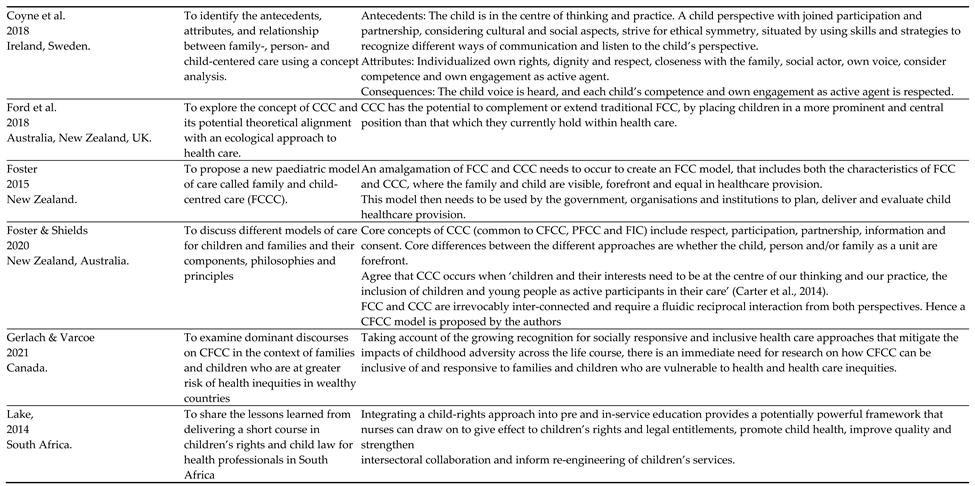
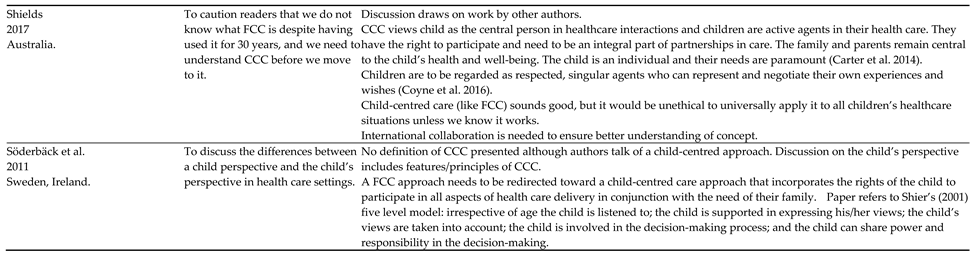
For each paper, the author, year, study population, country of origin, intervention type, study aims, methodology, outcome measure(s), and important results were abstracted from the article, as per guidance for scoping review procedures [19,21]. A summary of these findings is shown in the data extraction table (Table 1 and Table 2) which presents a summary of key data from the review.
3. Results
The results are presented in narrative format.
Demographics of included papers
Overview of discursive papers
Dates of publication
Authorship
Discursive focus
Most papers (n = 4) were focused on a conceptual consideration of CCC in relation to other models and focused on types of ‘centredness’ such as FCC and PCC [3,4,15,24]. Two papers were proposing or considering a merger of child-centred care with FCC with one paper proposing that the merger should be ‘family and child-centred care’ (FCCC) [23] and the other proposing a different ordering of the concepts with the child as the lead concept with the term being ‘child and family-centred care’ (CFCC) [25]. Individual papers addressed child-centred care in relation to other theories (Ford et al., 2018b), or
Overview of empirical papers
Dates of publication
Countries data generated from
Study design
Most papers (n = 8) used a qualitative design [27,28,29,30,31,33,34,35]. Of these, two used a phenomenological approach [34,35], one used grounded theory [27], one used participant inquiry [29], and one used case study [28] with the remaining three papers not stating a specific design [30,31,33].
Two papers reported using a quantitative approach [32,37]; of these, one was a feasibility study using a non-randomised quasi experimental cluster design [32] and one used secondary data analysis [37].
One paper was a systematic review [36].
Level of child involvement
Since the focus of the review was on child-centered care it seemed appropriate to try and appraise the level to which work underpinning the papers involved children. To this end we created three, arguably crude, categories that could be utilised to report the level of child involvement. The categories were ‘no involvement’ (papers in which there was no evidence of child involvement or engagement, e.g., in academic opinion pieces where the only voice is that of academic/researchers); ‘marginal involvement’ (evidence of some indirect involvement of children), and ‘authentic involvement’ (evidence of direct involvement of children, such as in research studies where children’s voices were either evident or children acted as advisors). Five papers were categorised as indicating ‘authentic involvement’ [27,29,31,32,33], four papers were categorised as ‘marginal involvement’ [28,30,34,35], and two categorised as ‘no involvement’ [36,37].
Sample size and characteristics
Sample size of children ranged from two [28] to 785 [32], with most falling in the range from 10 [29] to 26 [31,34] children.
Themes
Five themes were identified: agency, participation, impact, decision-making, and communication.
Agency
Of the 21 papers ten made direct reference to children being agentic, social agents or agentic beings [1,3,4,25,28,31,32,33,34,35]. Of these, six were empirical papers [28,31,32,33,34,35] and four were discursive [1,3,4,25]. Although one of the empirical papers mentioned agency frequently it was not directly related to CCC but to a relational ethics framework [28].
Agency and its synonyms were linked to children’s rights [1,3,4,31]. Agency and being agentic were linked to participation in general [3,25] and more specifically participation in the construction of their own lives [4], in healthcare [31], health dialogues [32], and care planning [35].
Children’s agency reflected adults respecting children’s independence [1,3], competence [1], their ability to construct understanding of issues related to them [33] and acknowledgment of their experiences [3]. Agency or being agentic were linked to partnerships and/or collaborations and interconnectedness [4,34], and respect [3].
Participation
Of the 21 studies, 18 referred to children’s participation. Of those 18 studies, eight were empirical papers [27,29,30,31,32,33,34,37] and 10 were discursive [1,3,4,15,16,22,24,25,26,28]. One empirical paper identified participation solely in terms of [29] research.
The synonyms ‘involvement’ and ‘inclusion’ were also used to indicate participation. Participation as a concept is not well defined [27] but includes participation in decision making and care and eliciting children’s opinions, perspectives and preferences [3,22,27,30,31,32].
Participation was identified as essential in accordance with children’s rights with 14 papers referring to the UN Convention on the Rights of the Child and/or national guidance [1,3,4,15,16,22,24,25,26,28,30,31,32,33].
Although a prerequisite for rights based child-centred care, the level of participation can vary from exclusion, limited opportunities [27,28] or minor degrees of participation in more trivial matters [27] to involvement in serious subjects such as complex care [28] and end of life [30,31].
Decision making
Of the 21 papers included in this review, 12 mentioned decision making in some way [1,3,4,15,16,22,27,28,31,33,34,36]. Of the empirically based papers, six referred to decision making [27,28,31,33,34,36]. And for the discursive papers, six also referred to decision making [1,3,4,15,16,22].
In terms of defining decision making, this was loosely presented, and has clear links with another theme in this review, agency. For the discursive papers, there were positive statements about children being involved in decision making [27,33], clear statement of them not being involved in decision making [28,36] and calls for children to be involved in decision making [31,34]. Calls were made for children to be involved in their own decision making [27] and it was noted that children liked to participate and that they could influence their choice. However, others made claims about the exclusion of children’s voices [28] and that they are rarely involved in decision making. For the assertions these included the child’s needs and interests always being at the centre of care and decisions [31] (Coombes et al., 2022) and for children needing to be “creators of their own healthcare experience” [34]. For the discursive papers, the divisions were not quite so clear, there were the assertions for positive involvement in decision making [22,36] and participate in all aspects of healthcare delivery (including decision making) [3]. Clearer was the discussion about whether the views of parents should supersede the views of children in decision making [1,16] which was not overt in the empirical papers. Notions of dignity impinge on this, including whether dignity can be maintained if the child is not involved in the decision making [4].
Communication
Of the 21 papers included in this review, 14 mentioned communication in some manner [1,3,4,15,16,24,27,28,29,32,33,34,36,37]. Of the empirically based papers, seven [27,28,32,33,34,36,37] referred to communication in some form. And for the discursive papers, six papers [1,3,15,16,24,29] discussed some aspects of communication.
Various terms are incorporated in this interpretation of communication [37]. For the empirical papers, these included, creating a communication space [27], children’s voices [28], dialogue [33], expression of views [32,33], co-creation [34], information sharing [36] and ‘sitting with’ [37]. For the discursive papers, a similar and complementary set of terms were discussed. These included encouraging dialogue [29], children representing their own experiences and wishes [3], Ubuntu-type interdependence [1], conversations about support [24]. Having a right to participate [15] was also mentioned, including the need to consider the children’s perspective to improve the way they are encountered [16].
As shown above the terms for communication often fence around the actual term communication. Few directly discussed communication [15,32,33,37]. However, the other aspects cannot occur without communication with the children. It is also clear that communication is not a clearly defined aspect of child-centred care, including its key role in achieving child-centred care.
Impact
There is limited discussion of the impacts of child-centred care on any level amongst the papers included in this review. Ten of the 21 papers included mentioned the impact of CCC on some level, be it on practice, outcomes, or experience [1,15,25,27,29,30,31,33,35,36]. Of these papers, three were discursive [1,15,25] and seven were empirical [27,29,30,31,33,35,36]. Of the seven empirical papers, none were quantitative studies, six were qualitative studies [27,29,30,31,33,35], and one systematic review was included [36]. There is limited evidence of broad outcome or impact assessment, as evidenced by the lack of quantitative, empirical papers included in this section.
Of the ten papers that discuss the impact of child-centred care, six (five empirical [27,30,33,35,36], one discursive [1]), included direct reference to the impact of child-centred care, but often these impacts were context specific and not generalisable [27,30,33,35]. For example, one paper [35] showed that a child-centred care model is the approach preferred by healthcare providers in an acute situation where the child has been potentially endangered by their family (in this case, non-accidental head injury of infants). Other papers made more generalisable, less context-specific conclusions [1,36]. One paper stated that child-centred care is becoming more significant in terms of shaping children’s healthcare [1], and another that child-centred care has positive impacts on children in terms of self-esteem, patient empowerment, and numerous treatment outcomes [36].
One paper ([31] empirical) included more indirect reference to the impacts of child-centred care, including discussion of potential rather than assessed impacts and that development of a child-centred outcome measure was needed but not yet developed. One paper ([29], empirical) cited both direct and indirect impacts of child-centred care on practice. This paper included empirical findings from a child-centred intervention, but also concluded, more indirectly, that children’s perspectives should have a greater influence on future practice.
4. Discussion
In this scoping review 21 papers were reviewed, and five themes (agency, participation, impact, decision making, and communication) were identified as being perceived and reported to be core to the concept of child-centred care in healthcare. In the Discussion these themes are considered in the context of the wider literature on children’s agency, participation, decision-making, and communication. The Discussion also contextualises child-centred care in the wider discussions of centredness and person-centred care in healthcare. The Discussion also considers the development and adoption and application (or lack thereof) of child-centred care, its limitations, and benefits.
What constitutes the concept of child-centred care in healthcare?
What is clear from the review is that there is no clear consensus across the papers about what constitutes child-centred care suggesting that it is an emerging, ambiguous and poorly defined concept. However, four interconnected concepts—agency, participation, decision-making and communication—were identified or discussed to some degree in many but not all papers. These concepts are ones which typically appear in contemporary literature about children’s positioning with society, healthcare and children’s health literacy and it would be hard to argue that any of these are unimportant. However, even when these concepts were present in the reviewed papers they were often simply referred to rather than clearly defined, perhaps reflecting the complexity of such concepts and the fact that definitions are contested. For the most part the papers neither state the depth or degree to which agency, participation, decision-making and communication should be present or how they can be enacted authentically to ensure that child-centred care ensues. The belief that child-centred care is important is evident in the reviewed papers and this aligns to other work that proposes the importance of child-centred approaches to care are key to good quality care (see for example [31].
In the review, agency was mostly discussed in terms of children’s rights [1,3,31] and their positioning in society, and closely linked with participation [3,4,25]. Agency is argued to result from relationships between human beings and their environment [38] and that it is a continuum characterised by interdependence [39]. Agency is clearly important as it requires adults to acknowledge the inherent wisdom and skills of children and young people [40] perceiving them as citizens [41]. Healthcare professionals who wish to work in a child-centred care way need to accept that children are already beings with agency who can reflect on and co-construct their worlds [42].This means that child-centred care requires healthcare professionals and organisations to ensure that they reduce barriers to children acting agentically, and create opportunities for children to actively participate and enact their agency, for example, through shared decision-making [43] and participation in clinical encounters [44] and during periods of hospitalisation [45] as well as interventions focusing on health and well-being [46]. However, as seen in the review [e.g.,3, 27, 28, 30] research that specifically focuses on children’s participation in medical encounters reveals that their participation is typically marginal [47,48].
Agency and participation require acknowledgement that children and health professionals are actors within what has been described as a networked system [49]. In a networked system everything affects everything else, meaning that factors (in the case of our review, participation, agency, decision-making and communications) are contingent on each other, competing agendas and ultimately interdependent [39]. Child health literacy is a field with growing momentum, and closely mirrors the core concepts of participation, agency, decision-making and communication identified in our review. The current global attention being given to health literacy in general, as well as to child health literacy, may well be a driver towards achieving child-centred care.
The review found that communication was perceived to be a core element of child-centredness and that this involved creating a space for communication [27] and supporting children to be able to express their views and engage in dialogue and conversation [24,29,32,33]. Recent work addressing child-centred communication strategies aligns with findings from the review and proposes core steps (greet, engage, involve and share) upon which good communication, even in time limited encounters, can be built [50]. Other work, albeit not expressed as overtly child-centred, supports the need to actively promote communication with all children [51,52], respect children’s expertise [53], and address health literacy issues [54]. The shift toward more child-centred communication practices can be seen in the endorsement of using resources co-developed with children and young people to support communication [55].
Decision-making was another aspect of child-centredness that was identified in the review (see for example, [27,31,33]. However, there is robust evidence that shared decision making is not consistently implemented, often resulting from barriers such as healthcare professionals having insufficient time, the presence of power imbalances and healthcare professionals not having the requisite skills for shared decision making [56]. To overcome such issues, strategies to promote shared decision-making include the use of decision support tools to facilitate the participation of children. However, the review also noted the tension between whether the views of parents should supersede the views of children in decision making [1,16]. The ethics of whose voice (child or parent) should hold sway and in what circumstances is complex and contextual. Yet until children can be active participants in communication that concerns them, engagement in decision making is not possible. Research shows that children are often marginalised in triadic (child-parent-healthcare professional) clinical encounters [48] and that dialogue is often dyadic (parents-professionals) [47] resulting in exclusion of children’s perspectives.
The review revealed a lack of evidence for the impact of child-centred care and how children benefit from child-centred care. This is perhaps unsurprising considering the more firmly embedded concept of FCC in children’s healthcare is still reported to lack robust impact evidence [15,25,57,58]. No clearly defined consensus measures to determine impact of child-centred care were evident within the review, reflecting the lack of attention to developing measures and/or measuring the impact of child-centred care in the literature. This is somewhat at odds with what is seen in the much larger field of (primarily adult) patient-centred care which is now widely recognised internationally as a means of delivering high quality healthcare. A meta narrative review of patient-centred care [59] identified 50 measurement instruments being used, albeit only 10 of these were directly measuring patient-centred care. If child-centred care is to be a sustainable and convincing model to guide practice and able to compete with other models or frameworks of care, it needs to establish robust evidence of its effectiveness. Other facets of child health practice that are child-centred if not completely embodying child-centred care are child-centred outcome measures and child-centred experience measures. Scott et al. [60] argue that using person-centred outcome measures in “routine paediatric care is key to child- centred quality care” (p42) but they note that implementation of and adherence to such measures is not simple and barriers exist.
Evidence from different countries with different health systems shows that the lack of a systematic approach, at all levels in an organisation, can impede the well-integrated adoption of person-centred care [61]. Successful adoption requires the use of evidence-based knowledge, guidelines and national regulations [61]. The lack of a clear evidence base for impact and benefit as well as a lack of guidelines and regulation perhaps provides a rationale for why child-centred care has not, so far, been effectively adopted across health care systems.
How has the concept of child-centred care developed?
It is difficult to identify whether or if child-centred care has developed over the period covered in this review as the term has been used loosely; lack of definitional sources lies at the root of this challenge. What is clearer is the tension between child-centred care and FCC [25]. Previously there was no seeming questioning of the relationship between the two forms of care [25]. Now there is greater evidence of a realisation that while the two forms of care can be mutually supportive, they can also be at odds with each other, and the rights of children (for instance a child’s rights to be involved in decision making) might be “trumped” by parental rights [16]. There is an overlap between child-centred care and person-centred care. However, work relating to person-centred care typically focuses on adults [62] and there is the potential that person-centred approaches miss the particularities, uniqueness and the changing dynamic of providing care for children. A future development proposed is melding the concept of child-centred care with FCC to become child and family-centred care (CFCC) [25], although this is likely to just blur the distinction between the two concepts and may not necessarily advance the position of children’s agency, participation, and decision-making.
What is the applicability of child-centred care and what are its limitations?
The applicability of child-centred care lies in its potential to create a better balance in terms of power, agency, participation and respect for the child [3]. In many circumstances, the evidence shows that family-centred care has essentially became parent-oriented and often primarily oriented to maternal involvement [3]. The focus on child-centred care means the needs and voice of the child being heard first, so that the care genuinely become child-centred. Its limitations are twofold, firstly that the legal rights are with the parents about decision making and secondly the capacity and norm forming of the child being involved in decisions about her or his care, rather than passive receiver of care.
How does the concept of child-centred care benefit and inform children’s healthcare?
A child-centred care approach has the potential, if implemented effectively, to acknowledge and reaffirm the rights of the child outlined in the United Nations Convention on the Rights of the Child (UNCRC) [11]. The approach recognises children’s rights to participation in healthcare matters and decisions about their care. The concept of child-centred care positions children to a more central orientation within health care, so that the focus is on the child in the context of the family rather than the other way around (where the child’s perspectives are secondary).
Considering the evidence from the person-centred care literature where benefits are considered in the wider context such as impacts on patient safety [63], rationales proposed for child-centred care need to extend to debates about wider contextual issues rather than being inwardly focused.
Strengths and limitations of the review
The strength of the review is that it focused on literature that specifically included the term child-centred care. However, the requirement for this specific term to be used resulted in the exclusion of many papers that were inherently child-centred in spirit, but which did not refer to the term. This resulted in the inclusion of only 21 papers and of these ten were discursive and most empirical papers reported using qualitative approaches. More detailed and extensive research needs to be undertaken to create a more robust knowledge base from which to argue the merits or otherwise of child-centred care.
5. Conclusions
The findings from the review suggest that child-centred care is an emerging, ambiguous and poorly defined concept with no clear consensus about what constitutes child-centred care. Although it seems antithetical to argue against child-centred care, little robust evidence was identified that demonstrates the impact of and benefit from child-centred care. If child-centred care is to be a sustainable and convincing model to guide practice and able to compete with other models or frameworks of care such as person-centred care, it needs to establish robust evidence of its effectiveness, impact on children and their families as well as the wider impacts (such as patient safety and cost effectiveness) on the healthcare system.
It is difficult to identify whether or if child-centred care has developed over the period covered in this review as the term has been used loosely; lack of definitional sources are at the root of this challenge.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, BC, KF, SC.; methodology, BC, KF, SC.; validation, BC, SY, KF, SC.; formal analysis, BC, SY, KF, SC.; investigation, BC, SY, KF, SC.; writing—BC, SY, KF, SC, X.X.; writing—BC, SY, KF, SC.; visualization, BC, SY, KF, SC. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding
Institutional Review Board Statement
As this was a scoping review, no ethical approval was required.
Conflicts of Interest
The authors declare no conflict of interest, beyond the fact that some of them are authors of papers which appear in the review.
References
- Ford, K.; Dickinson, A.; Water, T.; Campbell, S.; Bray, L.; Carter, B. Child Centred Care: Challenging Assumptions and Repositioning Children and Young People. Journal of Pediatric Nursing 2018, 43, e39–e43. [Google Scholar] [CrossRef]
- Carter, B.; Bray, L.; Dickinson, A.; Edwards, M.; Ford, K. Child-centred nursing: promoting critical thinking.; Sage Publications: London, 2014. [Google Scholar]
- Coyne, I.; Hallström, I.; Söderbäck, M. Reframing the focus from a family-centred to a child-centred care approach for children's healthcare. Journal of child health care: for professionals working with children in the hospital and community 2016, 20, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Coyne, I.; Holmström, I.; Söderbäck, M. Centeredness in Healthcare: A Concept Synthesis of Family-centered Care, Person-centered Care and Child-centered Care. Journal of pediatric nursing 2018, 42, 45–56. [Google Scholar] [CrossRef]
- Nolte, E.; Merkur, S.; Anell, A. Person-centredness: exploring its evolution and meaning in the health system context. In Achieving Person-Centred Health Systems., Nolte, E., Merkur, S., Anell, A., Eds. Cambridge University Press: Cambridge, 2020; pp. 19-40.
- Ahmann, E. Family-centered care: shifting orientation. Pediatric nursing 1994, 20, 113–117. [Google Scholar] [PubMed]
- 7. Ministry of Health. The Welfare of Children in Hospital. Report of the Committee (The Platt Report).
- Shields, L. What is ‘family-centred care’? European Journal for Person Centered Healthcare 2015, 3, 139. [Google Scholar] [CrossRef]
- Carter, B.; Ford, K. Researching children's health experiences: The place for participatory, child-centered, arts-based approaches. Research in Nursing & Health 2013, 36, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Bray, L.; Snodin, J.; Carter, B. Holding and restraining children for clinical procedures within an acute care setting: an ethical consideration of the evidence. Nursing Inquiry 2015, 22, 157–167. [Google Scholar] [CrossRef]
- 11. United Nations. UN Convention on the Rights of the Child. 1989.
- James, A.; Jenks, C.; Prout, A. Theorizing childhood; Polity Press in association with Blackwell Publishers Ltd.: Cambridge, UK, 1998. [Google Scholar]
- Franck, L.S.; Callery, P. Re-thinking family-centred care across the continuum of childrens healthcare. Child: Care, Health and Development 2004, 30, 265–277. [Google Scholar] [CrossRef]
- Foster, M.; Blamires, J.; Moir, C.; Jones, V.; Shrestha-Ranjit, J.; Fenton, B.; Dickinson, A. Children and young people's participation in decision-making within healthcare organisations in New Zealand: An integrative review. J Child Health Care, 1177. [Google Scholar] [CrossRef]
- Shields, L. All is not well with family-centred care. Nursing Children and Young People 2017, 29, 14–15. [Google Scholar] [CrossRef]
- Söderbäck, M.; Coyne, I.; Harder, M. The importance of including both a child perspective and the child’s perspective within health care settings to provide truly child-centred care. Journal of Child Health Care 2011, 15, 99–106. [Google Scholar] [CrossRef]
- Ford, K.; Campbell, S.; Carter, B.; Earwaker, L. The concept of child-centered care in healthcare: a scoping review protocol. JBI Database of Systematic Reviews and Implementation Reports 2018, 16, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P.; The, P.G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. 2015.
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O'Malley, L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Al-Motlaq, M.; Neill, S.; Foster, M.J.; Coyne, I.; Houghton, D.; Angelhoff, C.; Rising-Holmström, M.; Majamanda, M. Position Statement of the International Network for Child and Family Centered Care: Child and Family Centred Care during the COVID19 Pandemic. Journal of pediatric nursing 2021, 61, 140–143. [Google Scholar] [CrossRef]
- Foster, M. A new model: the family and child centered care model. Nursing praxis in New Zealand 2015, 31, 4–6. [Google Scholar]
- Foster, M.; Shields, L. Bridging the Child and Family Centered Care Gap: Therapeutic Conversations with Children and Families. Comprehensive child and adolescent nursing 2020, 43, 151–158. [Google Scholar] [CrossRef]
- Gerlach, A.; Varcoe, C. Orienting child- and family-centered care toward equity. Journal of child health care: for professionals working with children in the hospital and community 2021, 25, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Lake, L. Children's rights education: An imperative for health professionals. Curationis 2014, 37, 1–7. [Google Scholar] [CrossRef]
- Carlsson, I.-M.; Arvidsson, S.; Svedberg, P.; Nygren, J.M.; Viklund, Å.; Birkeland, A.-L.; Larsson, I. Creating a communication space in the healthcare context: Children’s perspective of using the eHealth service, Sisom. Journal of Child Health Care 2021, 25, 31–43. [Google Scholar] [CrossRef]
- Carnevale, F.A.P.; Teachman, G.; Bogossian, A. A Relational Ethics Framework for Advancing Practice with Children with Complex Health Care Needs and Their Parents. Comprehensive child and adolescent nursing 2017, 40, 268–284. [Google Scholar] [CrossRef]
- Carter, B. “They’ve got to be as good as mum and dad”: Children with complex health care needs and their siblings’ perceptions of a Diana community nursing service. Clinical Effectiveness in Nursing 2005, 9, 49–61. [Google Scholar] [CrossRef]
- Castor, C.; Derwig, M.; Borg, S.J.; Ollhage, M.E.; Tiberg, I. A challenging balancing act to engage children and their families in a healthy lifestyle - Nurses' experiences of child-centred health dialogue in child health services in Sweden. Journal of clinical nursing 2021, 30, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Coombes, L.; Braybrook, D.; Roach, A.; Scott, H.; Harðardóttir, D.; Bristowe, K.; Ellis-Smith, C.; Bluebond-Langner, M.; Fraser, L.K.; Downing, J.; et al. Achieving child-centred care for children and young people with life-limiting and life-threatening conditions—a qualitative interview study. European Journal of Pediatrics 2022, 181, 3739–3752. [Google Scholar] [CrossRef] [PubMed]
- Derwig, M.; Tiberg, I.; Björk, J.; Hallström, I. Child-Centred Health Dialogue for primary prevention of obesity in Child Health Services – a feasibility study. Scandinavian Journal of Public Health 2021, 49, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Derwig, M.; Tiberg, I.; Hallström, I. Elucidating the child's perspective in health promotion: children's experiences of child-centred health dialogue in Sweden. Health promotion international 2021, 36, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.; Whitehead, L. Using drawings to understand the child's experience of child-centred care on admission to a paediatric high dependency unit. Journal of child health care: for professionals working with children in the hospital and community 2019, 23, 102–117. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, K.A.; Dickinson, A.; Rasmussen, S. Caring for Children with Non-Accidental Head Injuries: A Case for a Child-Centered Approach. Comprehensive Child and Adolescent Nursing 2020, 43, 274–285. [Google Scholar] [CrossRef]
- Gondek, D.; Edbrooke-Childs, J.; Velikonja, T.; Chapman, L.; Saunders, F.; Hayes, D.; Wolpert, M. Facilitators and Barriers to Person-centred Care in Child and Young People Mental Health Services: A Systematic Review. Clinical Psychology & Psychotherapy 2017, 24, 870–886. [Google Scholar] [CrossRef] [PubMed]
- Lipman, T.H.; Murphy, K.M.; Kumanyika, S.K.; Ratcliffe, S.J.; Jawad, A.F.; Ginsburg, K.R. Racial differences in parents' perceptions of factors important for children to live well with diabetes. The Diabetes educator 2012, 38, 58–66. [Google Scholar] [CrossRef]
- Bodén, L. On, to, with, for, by: ethics and children in research. Children's Geographies, 1080; -16. [Google Scholar] [CrossRef]
- Abebe, T. Reconceptualising Children’s Agency as Continuum and Interdependence. Social Sciences 2019, 8, 81. [Google Scholar] [CrossRef]
- Larkins, C.; Satchwell, C. Learning How to Know Together: Using Barthes and Aristotle to Turn From ‘Training’ to ‘Collaborative Learning’ in Participatory Research with Children and Young People. International Journal of Qualitative Methods 2023, 22, 16094069231164607. [Google Scholar] [CrossRef]
- Larkins, C. Deeping the roots of children’s participation. Sociedad e Infancias 2023, 7, 147–163. [Google Scholar] [CrossRef]
- Montreuil, M.; Carnevale, F.A. A concept analysis of children's agency within the health literature. J Child Health Care 2016, 20, 503–511. [Google Scholar] [CrossRef]
- Wijngaarde, R.O.; Hein, I.; Daams, J.; Van Goudoever, J.B.; Ubbink, D.T. Chronically ill children's participation and health outcomes in shared decision-making: a scoping review. Eur J Pediatr 2021, 180, 2345–2357. [Google Scholar] [CrossRef] [PubMed]
- Dedding, C.; Reis, R.; Wolf, B.; Hardon, A. Revealing the hidden agency of children in a clinical setting. Health Expectations 2015, 18, 2121–2128. [Google Scholar] [CrossRef] [PubMed]
- Quaye, A.A.; Coyne, I.; Söderbäck, M.; Hallström, I.K. Children's active participation in decision-making processes during hospitalisation: An observational study. J Clin Nurs 2019, 28, 4525–4537. [Google Scholar] [CrossRef] [PubMed]
- Larsson, I.; Staland-Nyman, C.; Svedberg, P.; Nygren, J.M.; Carlsson, I.-M. Children and young people’s participation in developing interventions in health and well-being: a scoping review. BMC Health Services Research 2018, 18, 507. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.Q.; Mendoza, M.M.; Saini, S.K.; Sweeny, K. Let the Kid Speak: Dynamics of Triadic Medical Interactions Involving Pediatric Patients. Health Commun 2023, 38, 1762–1769. [Google Scholar] [CrossRef]
- van Woerden, C.S.; Vroman, H.; Brand, P.L.P. Child participation in triadic medical consultations: A scoping review and summary of promotive interventions. Patient Educ Couns 2023, 113, 107749. [Google Scholar] [CrossRef]
- Stoecklin, D. Theories of action in the field of child participation: In search of explicit frameworks. Childhood 2013, 20, 443–457. [Google Scholar] [CrossRef]
- Davison, G.; Conn, R.; Kelly, M.A.; Thompson, A.; Dornan, T. Fifteen-minute consultation: Guide to communicating with children and young people. Archives of disease in childhood - Education & Practice Edition 2023, 108, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Navein, A.; McTaggart, J.; Hodgson, X.; Shaw, J.; Hargreaves, D.; Gonzalez-Viana, E.; Mehmeti, A. Effective healthcare communication with children and young people: a systematic review of barriers and facilitators. Archives of Disease in Childhood 2022, 107, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Thunberg, G.; Johnson, E.; Bornman, J.; Öhlén, J.; Nilsson, S. Being heard – Supporting person-centred communication in paediatric care using augmentative and alternative communication as universal design: A position paper. Nursing Inquiry 2022, 29, e12426. [Google Scholar] [CrossRef] [PubMed]
- Gutman, T.; Hanson, C.S.; Bernays, S.; Craig, J.C.; Sinha, A.; Dart, A.; Eddy, A.A.; Gipson, D.S.; Bockenhauer, D.; Yap, H.K.; et al. Child and Parental Perspectives on Communication and Decision Making in Pediatric CKD: A Focus Group Study. Am J Kidney Dis 2018, 72, 547–559. [Google Scholar] [CrossRef]
- Bell, J.; Condren, M. Communication Strategies for Empowering and Protecting Children. J Pediatr Pharmacol Ther 2016, 21, 176–184. [Google Scholar] [CrossRef]
- RCPCH. Engaging children and young people - improving communication. Availabe online: https://www.rcpch.ac.uk/resources/engaging-children-young-people/communication (accessed on 25th August).
- Boland, L.; Graham, I.D.; Légaré, F.; Lewis, K.; Jull, J.; Shephard, A.; Lawson, M.L.; Davis, A.; Yameogo, A.; Stacey, D. Barriers and facilitators of pediatric shared decision-making: a systematic review. Implement Sci 2019, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- Shields, L.; Munns, A.; Taylor, M.; Priddis, L.; Park, J.; Douglas, T. Scoping review of the literature about family-centred care with caregivers of children with cystic fibrosis. Neonatal, Paediatric & Child Health Nursing 2013, 16, 21–25. [Google Scholar]
- Shields, L.; Pratt, J.; Hunter, J. Family centred care: a review of qualitative studies. Journal of Clinical Nursing 2006, 15, 1317–1323. [Google Scholar] [CrossRef]
- Janerka, C.; Leslie, G.D.; Gill, F.J. Development of patient-centred care in acute hospital settings: A meta-narrative review. Int J Nurs Stud 2023, 140, 104465. [Google Scholar] [CrossRef]
- Scott, H.M.; Braybrook, D.; Harðardóttir, D.; Ellis-Smith, C.; Harding, R. Implementation of child-centred outcome measures in routine paediatric healthcare practice: a systematic review. Health Qual Life Outcomes 2023, 21, 63. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, K.S.; Kirkorian, H.; Choi, K.; Jiang, M.J.; Raimer, C.; Tolkin, E.; Sartin-Tarm, A. Attempting to break the fourth wall: Young children's action errors with screen media. Human Behavior and Emerging Technologies 2021, 3, 468–483. [Google Scholar] [CrossRef]
- Håkansson Eklund, J.; Holmström, I.K.; Kumlin, T.; Kaminsky, E.; Skoglund, K.; Höglander, J.; Sundler, A.J.; Condén, E.; Summer Meranius, M. “Same same or different?” A review of reviews of person-centered and patient-centered care. Patient Education and Counseling 2019, 102, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Rossiter, C.; Levett-Jones, T.; Pich, J. The impact of person-centred care on patient safety: An umbrella review of systematic reviews. International Journal of Nursing Studies 2020, 109, 103658. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram for the scoping review process.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



