
Submitted:
02 November 2023
Posted:
03 November 2023
You are already at the latest version
Abstract
The relationship between arterial stiffness and oxygen uptake (VO2) in patients with acute myocardial infarction (AMI) remains unclear. We aimed to investigate this relationship and factors contributing to VO2 in patients with AMI. The role of arterial stiffness in cardiac-skeletal muscle coupling during exercise was then elucidated. The exercise capacity via cardiopulmonary exercise testing (CPX), cardio-ankle vascular index (CAVI), and body composition of 101 patients with AMI were measured at discharge. Patients were categorized based on their CAVI into three groups: (i) normal (CAVI: ≤7.9), (ii) borderline (CAVI: 8.0–8.9), and (iii) abnormal (CAVI: ≥9.0). Subsequently, VO2 was compared among these groups. The relationship between the CAVI and peak VO2 (VO2 Peak) during CPX and factors contributing to VO2 Peak were investigated. The abnormal CAVI group had a significantly lower VO2 Peak than the normal and borderline groups. The CAVI was associated with VO2 Peak in patients with AMI. Furthermore, the CAVI was found to be a factor contributing to VO2 Peak. These findings suggest that arterial stiffness in tissue blood distribution and blood supply defines systemic exercise limits in patients with AMI. This suggested that arterial stiffness plays a significant role in cardio-vascular-skeletal muscle coupling.
Keywords:
cardio-ankle vascular index
; acute myocardial infarction
; VO2 Peak
; cardio-vascular-skeletal muscle coupling
1. Introduction
Aging is a primary factor contributing to the increasing incidence of heart failure (HF) [1]. Several other factors contribute to the increasing prevalence of HF in the older population, including increased life expectancy, accumulated risk factors, and comorbidities. Therefore, addressing the increasing number of older patients with HF is necessary. Additionally, research and development are necessary to elucidate the pathophysiology, prevention, diagnosis, treatment, and rehabilitation of patients with prevalent cardiovascular diseases in Japan [2]. Ischemic heart diseases, such as acute myocardial infarction (AMI), account for approximately 50% of the major etiologies of HF in Japan [3]. The American College of Cardiology Foundation and American Heart Association stages provide useful and complementary information regarding the stages of HF [4]. AMI corresponds to stage B HF, i.e., structural heart disease without signs or symptoms of HF. However, without adequate secondary prevention, HF progresses, leading to physical dysfunction and terminal disease. The decline in physical function, including exercise tolerance, is one of the most important factors associated with the rate of HF exacerbation and mortality in patients with cardiovascular disease [5,6,7].
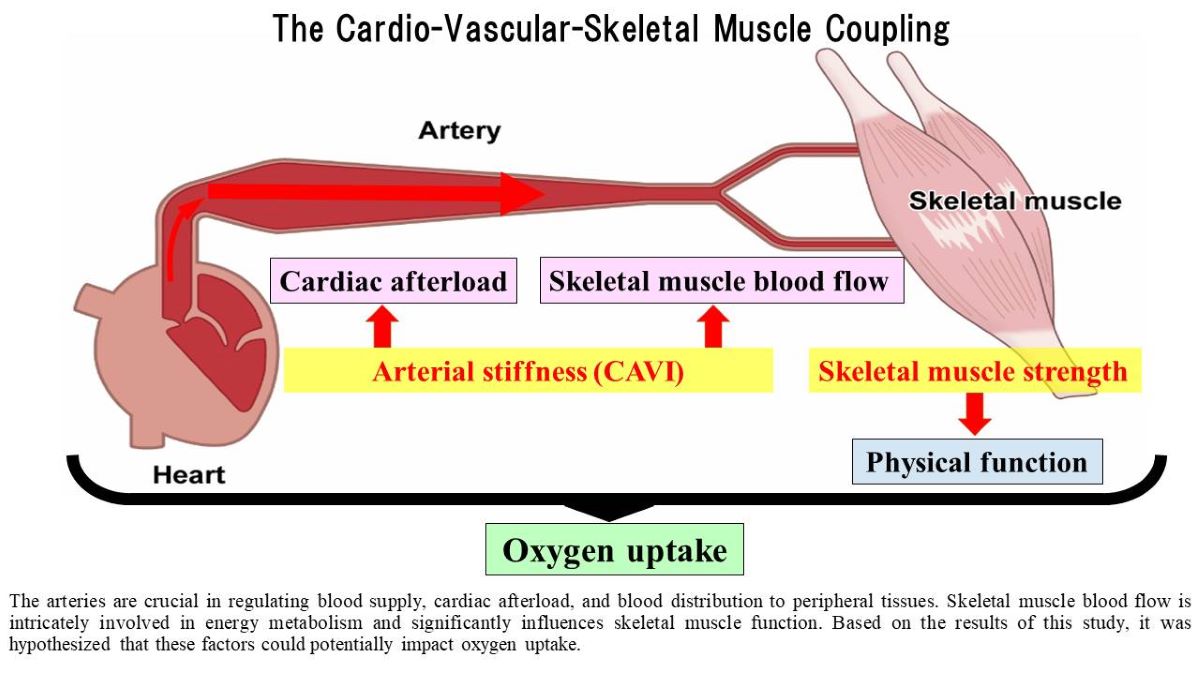
Oxygen uptake (VO2) is determined by cardiac and skeletal muscle function and is a common physiological parameter used as an indicator of exercise tolerance and aerobic capacity. Moreover, blood vessels connect the cardiac and skeletal muscles and supply oxygen and nutrients throughout the body. Blood vessels also regulate circulatory dynamics, among which arterial stiffness regulates cardiac afterload and blood flow to peripheral tissues [8,9]. The cardio-ankle vascular index (CAVI) is recognized as an indicator of arterial stiffness throughout the arterial tree, extending from the aortic origin to the ankle [10]. Previous studies have reported that an abnormal CAVI value (>9.0) is associated with a significant incidence of cardiovascular events, including cardiovascular death, myocardial infarction, stroke, hospitalization for HF, and coronary revascularization [11]. Therefore, arterial stiffness and VO2 are prognostic factors for cardiovascular disease, although the relationship between arterial stiffness and VO2 in patients with AMI remains unclear. We defined the response to exercise and physical activity as "the Cardio-vascular-skeletal muscle coupling" and hypothesized that arterial stiffness serves as a determinant of oxygen uptake. This study aimed to investigate the (i) relationship between arterial stiffness and VO2, and (ii) factors contributing to VO2 in patients with AMI. This study contributes to the understanding of the role of arterial stiffness in the cardio-vascular-skeletal muscle coupling.
2. Materials and Methods
2.1. Participants
This retrospective observational study used the cardiac rehabilitation database of Toho University Sakura Medical Center. In total, 366 consecutive patients with AMI who underwent cardiac rehabilitation between January 2017 and March 2023 were studied.
The inclusion criteria were patients who underwent (i) CAVI measurement of arterial stiffness and (ii) cardiopulmonary exercise testing (CPX). The exclusion criteria were: (i) lack of CAVI and CPX measurements and (ii) an ankle brachial index value of ≤0.9. This study included 101 patients (Figure 1). All parameters were evaluated immediately before discharge.
Abbreviations: CAVI, cardio-ankle vascular index; ABI, ankle brachial index
2.2. Ethics
This study was approved by the Ethics Committee of Toho University Sakura Medical Center (ethics number: S22019) and followed the Declaration of Helsinki and the ethical standards of the responsible committee on human experimentation. Patients were given the opportunity to opt-out when enrolling in this study.
2.3. Measured Parameters
2.3.1. CAVI
Arterial stiffness was assessed using the VaSera1500 vascular screening system (Fukuda Denshi Co., Ltd., Tokyo, Japan) as an indicator, following established protocols [9,10]. The patient was placed in a supine position with the head in a neutral position, and cuffs were applied to both the upper arms and ankles. After a 10-min resting period, measurements were taken to ensure a low cuff pressure of 30–50 mmHg to minimize its impact on hemodynamics. During the examination, blood pressure was recorded, and the CAVI value was calculated using the following equation:
CAVI = a {(2p/ΔP) × ln (Ps/Pd) PWV2} + b
where Ps and Pd represent systolic and diastolic blood pressure, respectively, PWV indicates the pulse wave velocity from the origin of the aorta to the junction of the tibial and femoral arteries, ΔP is the difference between Ps and Pd, p denotes the blood density, and a and b are constants.
This equation was derived from Bramwell-Hill's equation and adjusted for blood pressure based on the stiffness parameter (β). Three skilled examiners carefully observed the pulse waveforms to ensure accurate CAVI assessment in cases of atrial fibrillation.
A CAVI value of ≥8.0 potentially correlates with the presence of asymptomatic or potential atherosclerosis, whereas a CAVI value of ≥9.0 indicates the presence of advanced atherosclerosis and an elevated risk of cardiovascular complications [12]. Consequently, patients in this study were categorized into three groups utilizing their CAVI outcomes as follows: (i) normal (≤7.9), (ii) borderline (8.0–8.9), and (iii) abnormal (≥9.0) [13].
2.3.2. CPX
CPX and expiratory gas analysis were performed to evaluate VO2 quantitatively. CPX measures VO2, ventilatory carbon dioxide output, and respiratory and ventilation rates. CPX also calculates the minute ventilation rate from these measurements [14]. In the CPX test, the Strength Ergo 240 (Mitsubishi Electric Engineering Co., Ltd., Tokyo, Japan) was used for exercise load, the AE-310s Aeromonitor (Minato Medical Science Co., Ltd., Osaka, Japan) was used for breath gas analysis, and an STS-2100 (Nihon Kohden Co., Ltd., Tokyo, Japan) was used for exercise load electrocardiogram. In the study protocol, the patients began with a 3-min warm-up on a bicycle ergometer, followed by a 10-watt/min or 20-watt/min ramp incremental protocol. Continuous 12-lead electrocardiography was performed during the assessment, and blood pressure was recorded every minute during the exercise and recovery periods. After reaching the peak load, all patients pedaled at 0 watts, with a cool-down period of ≥2 min to prevent excessive venous pooling. The testing procedure adhered to published guidelines [15].
2.3.3. Skeletal muscle mass and handgrip strength
Skeletal muscle mass was measured using a body composition analyzer (MC-980A; Tanita Corp., Tokyo, Japan) based on direct segmented multifrequency bioelectrical impedance analysis [16]. By inputting the patient’s age, sex, and height, the bioimpedance analysis device yielded segmental muscle mass (arms, legs, and trunk), absolute fat mass, and body fat percentage. The sum of arm and leg skeletal muscle mass represents the appendicular skeletal muscle mass (ASM). The skeletal muscle mass index (SMI) value was defined as the ASM divided by the body height (in meters) squared as follows:
SMI = ASM (kg)/Height (m)2
Muscle strength was determined by measuring handgrip strength. An electronic hand dynamometer (Takei Scientific Instruments Co., Ltd., Tokyo, Japan) was used to measure handgrip strength. Two consecutive measurements of handgrip strength were made for both hands and recorded to the nearest kilogram, with the patient standing and the arm of the hand measured parallel to the body.
2.3.4. Echocardiography
Cardiac function was assessed using echocardiography. Left ventricular ejection fraction and diastolic function were assessed according to the American Society of Echocardiography guidelines [17,18]. Tissue Doppler imaging was used to estimate the left ventricular systolic function and early diastolic relaxation by averaging the peak systolic velocity and e' at the mitral annulus in both the medial and lateral walls. The ratio of early transmitral flow filling velocity (E) to tissue Doppler-derived early diastolic velocity (e') (E/e') was employed to estimate left ventricular filling. Trained laboratory technicians conducted all measurements, and a cardiologist verified the results. Echocardiography was performed on admission and before discharge.
2.3.5. Hematology and biochemistry data
Data on the peak creatine phosphokinase, albumin (Alb), creatinine, brain natriuretic peptide (BNP), and hemoglobin (Hb) levels were extracted from the clinical records of patients.
2.4. Statistical Analyses
Normally distributed data were assessed using the Shapiro–Wilk test. The CAVI values were categorized into three groups (≤7.9, 8.0–8.9, and ≤9.0). Subsequently, VO2 Peak was compared among these groups using the Kruskal–Wallis test with Bonferroni adjustment. The statistical significance level was set at p<0.016 (0.05/3≈0.016).
The relationship between the CAVI value and other clinical parameters was also analyzed using Spearman's rank correlation coefficient. Finally, the variance inflation factor was examined to assess multicollinearity among the indicators significantly correlated with VO2 Peak. Forced-entry multiple regression analysis was used to investigate the VO2 Peak determinants. Results are expressed as the median (interquartile range (IQR)). The statistical significance level was set at 5%, and the analysis was conducted using SPSS Ver29.0 (IBM, Chicago, IL, USA).
3. Results
3.1. Patient Characteristics
A total of 101 (86 male and 15 female) patients with AMI underwent CPX. The median age was 67.0 (IQR: 54.5, 73.0) and 72.0 (IQR: 68.0, 76.0) years for male and female patients, respectively. The CAVI values were 9.1 (IQR: 8.1, 9.9) and 9.5 (IQR: 8.8, 10.5) for male and female patients, respectively. The patient characteristics are shown in Table 1.
Data are presented as medians (interquartile ranges), unless otherwise indicated.
3.2. Physical Function and CPX
Peak VO2 (VO2 Peak) measured by CPX was 17.9 (IQR: 15.7, 20.9) and 15.4 (IQR: 12.8, 16.3) mL/kg/min for male and female patients, respectively. The physical function and results obtained using CPX are listed in Table 2.
Data are presented as medians (interquartile ranges).
3.3. Comparison of O2 Peak According to CAVI Classification
VO2 Peak in groups classified according to the CAVI values was (i) 20.1 (IQR: 16.5, 25.2) mL/kg/min in 16 patients with a normal CAVI value (≤7.9), (ii) 18.5 (IQR: 15.9, 22.6) mL/kg/min in 31 with a borderline CAVI value (8.0–8.9), and (iii) 16.2 (IQR: 12.8, 18.2) mL/kg/min in 54 with an abnormal CAVI value (≥9.0). As shown in Figure 2, patients with an abnormal CAVI value had a significantly lower VO2 Peak than those with normal and borderline CAVI values.
Abbreviation: VO2, oxygen uptake.
3.4. Association Between VO2 Peak and Clinical Parameters
Age, the Alb, Hb, and BNP levels, E/e', the CAVI value, the SMI value, and handgrip strength were significantly correlated with VO2 Peak in patients with AMI. Table 3 shows the relationship between VO2 Peak and clinical indices, and Figure 3 shows a scatter plot of the CAVI value and VO2 Peak in patients with AMI.
3.5. Factors Contributing to VO2 Peak
Multiple regression analysis was performed using the forced-entry method to determine the factors contributing to VO2 Peak in patients with AMI. The parameters correlated with VO2 Peak and sex as independent variables. The results revealed that handgrip strength and the CAVI value significantly contributed to the VO2 Peak in patients with AMI. In comparison, age, sex, Alb, Hb, and BNP levels, E/e', and SMI value were found to have no significant impact. Table 4 shows the factors identified to contribute to VO2 Peak in patients with AMI.
4. Discussion
This study examined the relationship between the CAVI value and VO2 Peak and factors contributing to VO2 Peak to establish a basis for determining the role of arterial stiffness in the cardio-vascular-skeletal muscle coupling during exercise in patients with AMI.
The study results showed that the CAVI value and VO2 Peak were related (Table 3). Patients with an abnormal CAVI value were found to have significantly lower VO2 Peak than those with normal and borderline CAVI values (Figure 2). Part of the stroke volume during left ventricular contraction is delivered directly to peripheral tissues, while the other part is stored instantaneously in the aorta and central arteries [19]. Inhibition of arterial dilation during left ventricular ejection due to atherosclerosis limits arterial blood storage and blood supply to peripheral tissues [20]. Shiba et al. [21] reported that with an increase in the CAVI value, the peripheral retinal vascular blood flow changes from steady to pulsatile, and the blood supply decreases. This study hypothesized that a similar reduction in blood flow and supply occurs in the skeletal muscles of patients with AMI. Furthermore, it has been reported that increased cardiac afterload due to atherosclerosis increases myocardial oxygen demand, decreases cardiac output during peak exercise, and decreases cardiorespiratory function [22]. Therefore, the association between the CAVI value and VO2 Peak in this study suggests that arterial stiffness affects the blood supply to skeletal muscles and other organs, resulting in changes in skeletal muscle metabolism during exercise.
The CAVI value and handgrip strength contributed to VO2 Peak in patients with AMI. The limiting factors for VO2 involve the following factors: i) reduction in oxygen delivery, ii) decrease in cardiac output, and iii) overperfusion of a small muscle mass during exercise [23]. Therefore, an optimal blood flow distribution to peripheral tissues such as skeletal muscles is important during exercise. During exercise and physical activity, the increased demand for oxygen requires a coordinated response from both the cardiac and skeletal muscles. The cardiovascular system responds by increasing the heart rate, cardiac output, and blood flow to meet the increased metabolic demands of skeletal muscles. Vasodilation of the arteries and redistribution of the blood flow accomplish this response. Thus, the results of this study suggest that impaired arterial stiffness results in decreased blood supply to peripheral tissues and increased cardiac load, making it difficult to continue exercising and decreasing VO2. A lower VO2 during exercise was associated with a worse long-term prognosis in patients with AMI [24]. Thus, this novel finding in this study suggests that an increased CAVI value also affects the prognosis of patients with AMI.
Although skeletal muscle mass is a determinant of VO2 [25], the SMI, an index of skeletal muscle mass calculated from body composition, did not contribute to VO2 Peak in this study. However, handgrip strength was identified as a contributing factor. The Health, Aging, and Body Composition Study [26] reported that the mortality risk was strongly associated with quadriceps power and handgrip strength but not muscle mass. The study also reported that measures of muscle quality were more important in estimating mortality risk. The results of this study also support the importance of skeletal muscle quality, such as muscle performance. Concurrently, the influence of qualitative changes in skeletal muscle was considered in patients with AMI. Skeletal muscle dysfunction accompanying HF is not limited to skeletal muscle atrophy but also involves muscle fiber type transformation, leading to decreased exercise tolerance [27]. This indicates that the metabolic function of skeletal muscle, rather than cardiac function, is an important determinant of oxygen consumption [28]. Patients with AMI in this study were likely to have skeletal muscle dysfunction similar to that in those with HF. Therefore, skeletal muscle mass measurements alone do not adequately capture skeletal muscle dysfunction in patients with cardiac disease.
In summary, this study obtained a novel insight regarding the role of the CAVI in relation to VO2 Peak. It has been suggested that arterial stiffness determines blood supply from the arteries and its distribution to peripheral tissues through cardiac afterload. Furthermore, blood flow distribution to skeletal muscles contributes to energy metabolism, and it has been speculated that skeletal muscle function plays an important role in VO2.
This study had some limitations. First, the number of patients with AMI who underwent CPX was low (27.6%). This was because some could not undergo CPX due to their decline in physical function and old age. Therefore, this study may have been limited to patients with AMI and relatively preserved motor function who could undergo CPX. On the other hand, the authors have previously reported an association between the 6-min walking distance and CAVI value in older patients with HF aged ≥65 years [29]. Together with the present results, this suggests an association between exercise tolerance and arterial stiffness in patients with heart disease. Second, cautious clinical assessment was considered necessary to determine skeletal muscle mass using bioelectrical impedance analysis. Skeletal muscle tissue generally contains much more water than fat tissue. Although bioelectrical impedance analysis uses this property to measure the body composition, edema may overestimate skeletal muscle tissue in some patients with AMI. However, the patients with AMI in this study received cardiac rehabilitation during their hospitalization, and their body composition was measured at discharge when their condition was stable. Therefore, edema was considered to have little effect on body composition.
5. Conclusions
This study showed that VO2 Peak and the CAVI value were associated at discharge in patients with AMI and that handgrip strength and the CAVI value contributed to VO2 Peak. The study suggests a role for arterial stiffness during whole-body endurance exercise in the cardio-vascular-skeletal muscle coupling. This indicates the importance of measuring arterial stiffness as an index of cardiac rehabilitation in patients with AMI.
Author Contributions
Conceptualization, A.O. and K.S.; methodology, A.O., S.K., Y.I., M.I., T.N., S.S., H.M and K.S.; software, A.O, S.K. and K.S.; validation, A.O., S.K. and K.S.; formal analysis, A.O., S.S., H.M and K.S.; investigation, A.O and K.S.; resources, A.O.; data curation, A.O.,S.K., Y.I., M.I., T.N., S.S., H.M., A.N. and K.S; writing—original draft preparation, A.O.; writing—review and editing, S.K. and K.S.; visualization, A.O. S.K. and S.S; supervision, S.K., A.N. and K.S.; project administration, A.O. and K.S.; funding acquisition, A.O. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by JSPS KAKENHI (grant number: JP 22K17575).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Toho University Sakura Medical Center (ethics number: S22019).
Informed Consent Statement
Informed consent was obtained in the form of opt-out on the website.
Data Availability Statement
The original contributions presented in the study are included in the article, and further inquiries can be directed to the corresponding author.
Acknowledgments
We sincerely thank Prof. Koji Shirai and Prof. Hiroshi Maruoka for his invaluable guidance and encouragement. We also appreciate the dedicated staff of the Cardiovascular Unit and Department of Rehabilitation at Toho University Sakura Medical Center.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Shimokawa, H.; Miura, M.; Nochioka, K.; Sakata, Y. Heart failure as a general pandemic in Asia. Eur. J. Heart Fail. 2015, 17, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Mori, M.; Komoto, S. Japanese national plan for promotion of measures against cerebrovascular and cardiovascular disease. Circulation 2021, 143, 1929–1931. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Sakata, Y.; Sato, K.; Nochioka, K.; Miura, M.; Abe, R.; Oikawa, T.; Kasahara, S.; Aoyanagi, H.; Yamanaka, S.; et al. Clinical characteristics and prognostic factors in elderly patients with chronic heart failure-a report from the CHART-2 study. Int. J. Cardiol. Heart Vasc. 2020, 27, 100497. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013, 128, e240–327. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef] [PubMed]
- McNallan, S.M.; Singh, M.; Chamberlain, A.M.; Kane, R.L.; Dunlay, S.M.; Redfield, M.M.; Weston, S.A.; Roger, V.L. Frailty and healthcare utilization among patients with heart failure in the community. JACC Heart. Fail. 2013, 1, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Fülster, S.; Tacke, M.; Sandek, A.; Ebner, N.; Tschöpe, C.; Doehner, W.; Anker, S.D.; von Haehling, S. Muscle wasting in patients with chronic heart failure: results from the studies investigating co-morbidities aggravating heart failure (SICA-HF). Eur. Heart J. 2013, 34, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Ohira, M.; Iizuka, T.; Mikamo, H.; Nakagami, T.; Suzuki, M.; Hirano, K.; Takahashi, M.; Shimizu, K.; Sugiyama, Y.; et al. Cardio-ankle vascular index relates to left ventricular ejection fraction in patients with heart failure. A retrospective study. Int. Heart J. 2013, 54, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Yamamoto, T.; Takahara, A.; Shirai, K. Clinical assessment of arterial stiffness with cardio-ankle vascular index: theory and applications. J. Hypertens. 2015, 33, 1742–1757. [Google Scholar] [CrossRef] [PubMed]
- Shirai, K.; Utino, J.; Otsuka, K.; Takata, M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J. Atheroscler. Thromb. 2006, 13, 101–107. [Google Scholar] [CrossRef]
- Okamoto, Y.; Miyoshi, T.; Ichikawa, K.; Takaya, Y.; Nakamura, K.; Ito, H. Cardio-ankle vascular index as an arterial stiffness marker improves the prediction of cardiovascular events in patients without cardiovascular diseases. J. Cardiovasc. Dev. Dis. 2022, 9, 368. [Google Scholar] [CrossRef]
- Tanaka, A.; Tomiyama, H.; Maruhashi, T.; Matsuzawa, Y.; Miyoshi, T.; Kabutoya, T.; Kario, K.; Sugiyama, S.; Munakata, M.; Ito, H.; et al. Physiological diagnostic criteria for vascular failure. Hypertension 2018, 72, 1060–1071. [Google Scholar] [CrossRef]
- Saiki, A.; Ohira, M.; Yamaguchi, T.; Nagayama, D.; Shimizu, N.; Shirai, K.; Tatsuno, I. New horizons of arterial stiffness developed using cardio-ankle vascular index (CAVI). J. Atheroscler. Thromb. 2020, 27, 732–748. [Google Scholar] [CrossRef]
- Adachi, H. Cardiopulmonary exercise test. Int. Heart J. 2017, 58, 654–665. [Google Scholar] [CrossRef] [PubMed]
- ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [CrossRef]
- Pietrobelli, A.; Morini, P.; Battistini, N.; Chiumello, G.; Nuñez, C.; Heymsfield, S.B. Appendicular skeletal muscle mass: prediction from multiple frequency segmental bioimpedance analysis. Eur. J. Clin. Nutr. 1998, 52, 507–511. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- London, G.M.; Pannier, B. Arterial functions: how to interpret the complex physiology. Nephrol. Dial. Transplant. 2010, 25, 3815–3823. [Google Scholar] [CrossRef] [PubMed]
- Briet, M.; Boutouyrie, P.; Laurent, S.; London, G.M. Arterial stiffness and pulse pressure in CKD and ESRD. Kidney Int. 2012, 82, 388–400. [Google Scholar] [CrossRef]
- Shiba, T.; Takahashi, M.; Matsumoto, T.; Shirai, K.; Hori, Y. Arterial stiffness shown by the cardio-ankle vascular index is an important contributor to optic nerve head microcirculation. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Palombo, C.; Kozakova, M. Arterial stiffness, atherosclerosis and cardiovascular risk: Pathophysiologic mechanisms and emerging clinical indications. Vascul. Pharmacol. 2016, 77, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bassett, D.R.; Howley, E.T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med. Sci. Sports. Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, RF.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J. 2020 Jan 14;41(3):407-477. [CrossRef]
- Karpman, V.L.; Fick, A. [The theoretical analysis of Fick's equation. On the centennial of the use of Fick's principle in physiology]. Z. Kardiol. 1975, 64, 801–808. [Google Scholar] [PubMed]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. A. Biol. Sci. Med. Sci. 2006, 61, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Kinugawa, S.; Takada, S.; Matsushima, S.; Okita, K.; Tsutsui, H. Skeletal muscle abnormalities in heart failure. Int. Heart J. 2015, 56, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Okita, K.; Kinugawa, S.; Tsutsui, H. Exercise intolerance in chronic heart failure--skeletal muscle dysfunction and potential therapies. Circ. J. 2013, 77, 293–300. [Google Scholar] [CrossRef]
- Ogawa, A.; Shimizu, K.; Nakagami, T.; Maruoka, H.; Shirai, K. Physical function and cardio-ankle vascular index in elderly heart failure patients. Int. Heart J. 2020, 61, 769–775. [Google Scholar] [CrossRef]
Figure 1.
Study enrollment procedure.
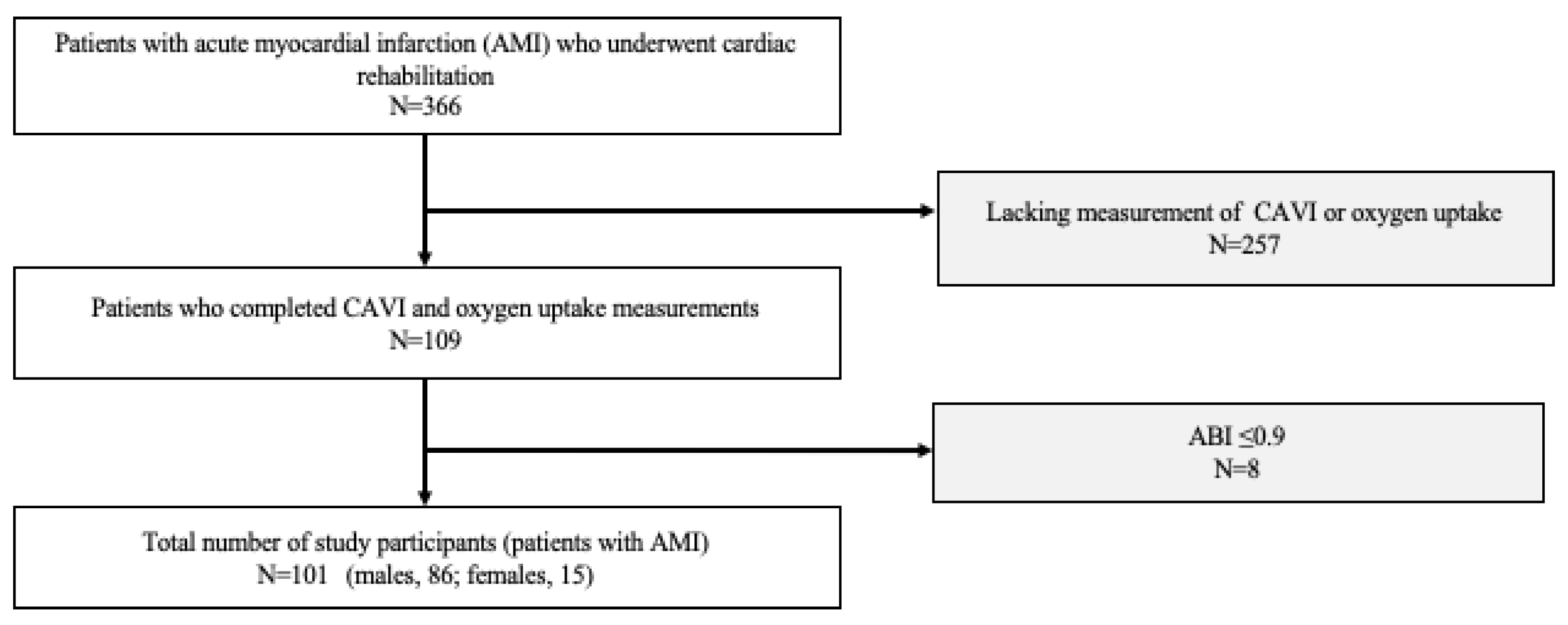
Figure 2.
Comparison of peak oxygen uptake according to cardio-ankle vascular index classification.
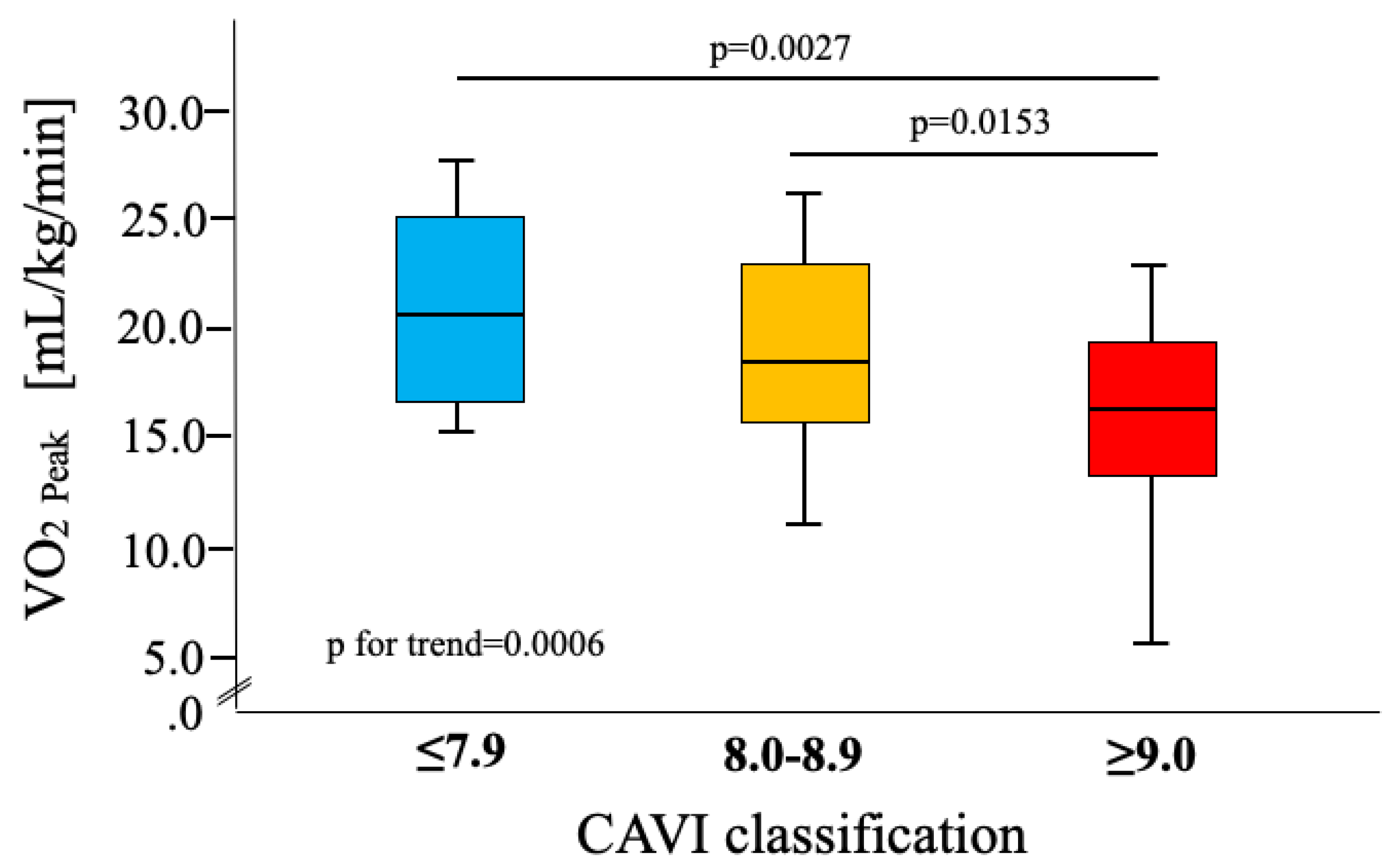
Figure 3.
Scatter plot of the cardio-ankle vascular index and peak oxygen uptake in patients with acute myocardial infarction.
Figure 3.
Scatter plot of the cardio-ankle vascular index and peak oxygen uptake in patients with acute myocardial infarction.
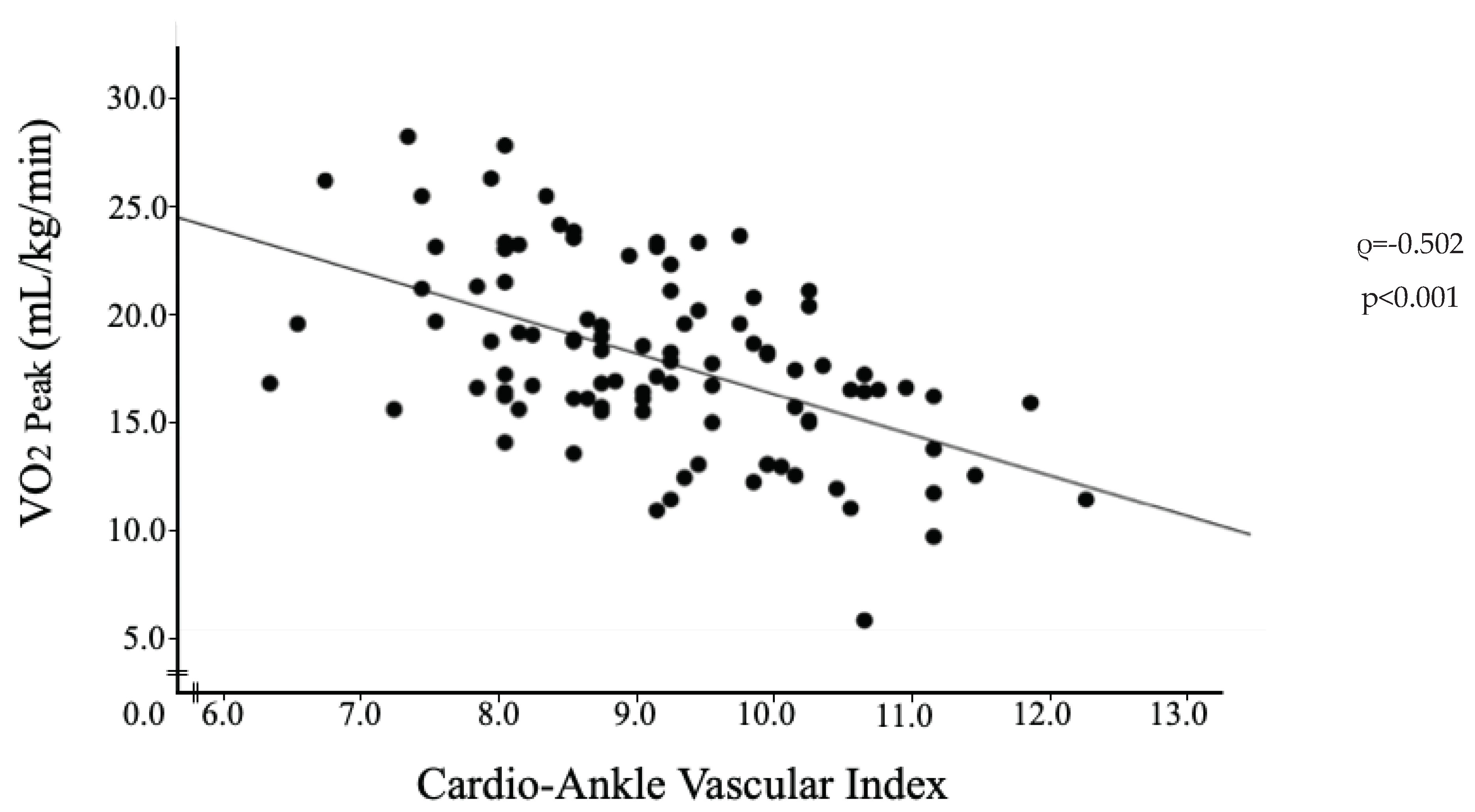

Table 1.
Patient characteristics.
| Variable | Patients with AMI n=101 |
|---|---|
| Male, n (%) | 86 (85.1) |
| Age, years | 67.5 (56.0, 74.0) |
| BMI, kg/m2 | 22.3 (20.9, 25.2) |
| sBP, mmHg | 115.0 (106.5, 126.5) |
| dBP, mmHg | 71.0 (63.5, 80.5) |
| HR, bpm | 68.0 (59.3, 77.8) |
| Alb, g/dL | 3.8 (3.6, 4.2) |
| Cre, mg/dL | 0.92 (0.82, 1.06) |
| Hb, mg/dL | 13.4 (11.9, 14.2) |
| CPK Peak | 1162.0 (374.5, 2240.0) |
| BNP, pg/mL | 86.9 (52.0, 163.2) |
| EF, % | 61.0 (53.5, 67.0) |
| E/e’ | 11.2 (9.0, 15.5) |
| CAVI | 9.1 (8.2, 9.9) |
| Smoking, n (%) | 34 (33.7) |
| Complications, n (%) | |
| AF | 5 (4.9) |
| HT | 42 (41.6) |
| DM | 31 (31.7) |
| DL | 63 (62.4) |
| Use of medications, n (%) | |
| Ca-antagonists | 9 (8.9) |
| RAS-inhibitors | 53 (52.5) |
| β-blockers | 72 (71.3) |
| Diuretics | 28 (27.7) |
| Statins | 76 (75.2) |
| Nitrate drug | 42 (41.6) |
Abbreviations: AMI, acute myocardial infarction; BMI, body mass index; sBP, systolic blood pressure; dBP, diastolic blood pressure; HR, heart rate; Alb, albumin; Cre, creatinine; CPK, creatine phosphokinase; BNP, brain natriuretic peptide; EF, ejection fraction, E/e’, ratio of early transmitral filling velocity to early diastolic velocity; CAVI, cardio-ankle vascular index; AF, atrial fibrillation; HT, hypertension; DM, diabetes mellitus; DL, dyslipidemia; Ca-antagonists, calcium antagonists; RAS-inhibitors, renin-angiotensin aldosterone inhibitors.
Table 2.
Assessment of physical parameters and cardiopulmonary exercise testing.
| Variable | Patients with AMI n=101 |
|---|---|
| SMI, kg/m2 | 6.37 (5.68, 7.38) |
| Handgrip strength, kg | 21.7 (16.2, 28.2) |
| VO2 AT, mL/kg/min | 13.7 (11.4, 15.7) |
| VO2 Peak, mL/kg/min | 17.7 (15.6, 20.7) |
| HR AT, beat/min | 104.5 (94.8, 111.0) |
| HR Peak, beat/min | 124.5 (110.3, 134.0) |
| VO2/HR Peak, mL/beat | 9.5 (7.9, 10.9) |
| VE vs VCO2 slope | 32.0 (29.1, 37.0) |
| ΔVO2/ΔWR, mL/min/watt | 8.1 (7.0, 9.5) |
Abbreviations: SMI, skeletal muscle mass index; VO2, oxygen uptake; AT, anaerobic threshold; VE, ventilation rate; VCO2, ventilatory carbon dioxide output; WR, work rate.
Table 3.
Correlation between peak oxygen uptake and clinical parameters.
| Variable | Correlation coefficient (ρ) | 95% CI | p-value |
|---|---|---|---|
| Age | -0.487 | -0.628–-0.315 | <0.001 |
| BMI | 0.136 | -0.075–0.335 | 0.191 |
| sBP | -0.026 | -0.230–0.180 | 0.798 |
| dBP | 0.024 | -0.182–0.228 | 0.812 |
| CPK Peak | -0.09 | -0.410–0.251 | 0.598 |
| Alb | 0.297 | 0.094–0.476 | 0.004 |
| Cre | -0.121 | -0.319–0.087 | 0.240 |
| Hb | 0.454 | 0.270–0.603 | <0.001 |
| BNP | -0.326 | -0.509–-0.115 | 0.002 |
| EF | 0.049 | -0.204–0.296 | 0.698 |
| E/e’ | -0.212 | -0.403–-0.004 | 0.04 |
| CAVI | -0.502 | -0.640–-0.333 | <0.001 |
| SMI | 0.479 | 0.302–0.624 | <0.001 |
| Handgrip strength | 0.501 | 0.325–0.643 | <0.001 |
Abbreviations: Hb, hemoglobin. Spearman's rank correlation coefficient was analyzed. The significance level was set at p<0.05.
Table 4.
Factors to the peak oxygen uptake in patients with acute myocardial infarction.
| Variable | r | r2 | β | 95% CI | p-value |
|---|---|---|---|---|---|
| Age | 0.657 | 0.432 | 0.098 | -4.494-35.936 | 0.125 |
| Sex | -0.103 | -4.132-1.917 | 0.467 | ||
| Alb | -0.011 | -2.243-2.042 | 0.926 | ||
| Hb | 0.106 | -0.296-0.789 | 0.368 | ||
| BNP | -0.046 | -0.008-0.005 | 0.678 | ||
| E/e’ | -0.043 | -0.225-0.149 | 0.684 | ||
| CAVI | -0.258 | -1.856--0.070 | 0.035 | ||
| SMI | -0.014 | -1.170-1.075 | 0.933 | ||
| Handgrip strength | 0.541 | 0.074-0.402 | 0.005 |
A forced-entry multiple regression analysis was used to investigate VO2 peak determinants. Adjustment factors: age, sex, Alb, Hb, BNP, E/e’, CAVI, SMI, and handgrip strength. Abbreviations: R, multiple correlation coefficient; R2, coefficient of determination; β, standardized partial regression coefficient; CI, confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



