Submitted:
03 November 2023
Posted:
06 November 2023
You are already at the latest version
Abstract
The decline in assisted reproductive technology (ART) success among older women, attributed to decreased oocyte quantity and quality, poses a significant challenge. Currently, no consensus ex-ists on the optimal ovarian stimulation protocol for older women undergoing IVF. This retrospec-tive registered cohort study aimed to compare cumulative live birth rates (CLBR), time to live birth (TTLB), and cost-effectiveness in women over 35 years using gonadotropin-releasing hor-mone agonist (GnRHa) or clomiphene-primed ovarian stimulation (CPOS). We performed pro-pensity score matching (PSM) on 2,871 IVF cycles in women over 35 who received either GnRHa or CPOS protocols, resulting in 375 cycles in each group to compare treatment outcomes. Addition-ally, a decision tree model was utilized to assess the cost-effectiveness of the two protocols. Fol-lowing PSM, both groups showed similar baseline characteristics. The CPOS protocol exhibited a higher cycle cancellation rate (13.07% vs 8.00%, p=0.032), yet maintained comparable fertilization and embryo quality. While CLBRs per initial cycle (41.07% vs. 45.33%, p=0.269) and delivery out-comes were similar between the groups after a 24-month follow-up, TTLB was longer in the CPOS group. Notably, the average cost per live birth in the CPOS group was 21.27% less than that in the GnRHa group (¥32,301.42 vs ¥39,174.22). In conclusion, for women over 35 undergoing IVF, the CPOS protocol demonstrated similar CLBR to GnRHa but with lower costs, suggesting its potential as a viable and cost-efficient ovarian stimulation option.
Keywords:
older women
; ovarian stimulation protocol
; in-vitro fertilization and embryo transfer
; cumulative live birth rate
; time to live birth
; cost-effectiveness.
1. Introduction
According to epidemiological data, the incidence of infertility is increasing in many countries and regions around the world [1], including China [2]. Increased chances for education and career advancement, as well as the promotion of effective contraceptive measures, are causing an increasing number of women to choose to have children after the age of 35, which is a major factor contributing to the rise in the incidence of infertility [3]. Age-related fertility decline [4] is an increasing proportion of the causes of assisted reproductive technology. However, the pregnancy rate of IVF treatment in older women over 35 years of age is also significantly reduced due to a decline in oocyte quantity and quality [5,6] and probable endometrial receptivity changes [7]. The current primary strategy to compensate for age-related decline in oocyte quality and quantity is to maximize ovarian response by developing patient-specific protocols [8]. So various ovarian stimulation protocols, such as gonadotrophin releasing hormone agonist (GnRHa) protocol, GnRH antagonist (GnRHA) protocol, mild-stimulation protocol, progestin-primed ovaraian stimulation protocol, double stimulation/dual stimulation protocol, and modified natural cycle protocol, have been tried for older women [9], but the advantages and disadvantages of each protocol in terms of efficacy, safety, and cost-effectiveness still need to be further clarified.
Clomiphene citrate (CC) is a selective estrogen receptor modulator with strong anti-estrogen effect and weak estrogen effect. CC is orally administrated, inexpensive and clinically accessible. The pharmacological mechanism of clomiphene is still not very clear. Currently, it is believed that low-dose drugs may act on the hypothalamus, compete with estrogen to bind receptors, block estrogen negative feedback, and promote the release of GnRH and endogenous gonadotropin [10]. CC was first approved by the United States Food and Drug Administration for human ovulation stimulation in 1961; its use is believed to improve ovarian responsiveness and minimize gonadotropin dosage by promoting the release of endogenous gonadotropin. The guidelines of European Society of Human Reproduction and Embryology (ESHRE) in 2020 also recommend the use of clomiphene alone or in combination with gonadotropin for ovarian stimulation in patients with predicted poor responder [11]. Currently, the most commonly discussed ovarian stimulation protocol in combination with clomiphene and gonadotropin is the mild-stimulation protocol. across high responder, normal responder, and poor responder patients, numerous studies have indicated that while the combination of gonadotropin and clomiphene can lower the cost of ovarian stimulation without compromising embryo quality, it also leads to an increase in cycle cancellation rate, a decrease in the number of oocytes retrieved, and a decrease in the cumulative pregnancy rate [12,13,14,15]. As a result, mild-stimulation has a lower application efficiency in individuals with "non-severe decline" in ovarian reserve than conventional GnRH agonist or antagonist protocol [16]. Recent research has also tried to extend the usage of CC until the trigger day. Because CC's anti-estrogenic effect can inhibit endogenous LH peaks, it can reduce the need for GnRH agonists or GnRH antagonists, lowering the cost of ovarian stimulation [17,18]. Based on this consideration, our center has tried a continuous combination of clomiphene and adequate dose of gonadotrophin ovarian stimulation (we named it clomiphene-primed ovarian stimulation, CPOS) in older women, and has achieved good results. In this study, we retrospectively analyzed the cumulative live birth rate (CLBR), time to live birth (TTLB) and cost-effectiveness ratio (C/E) of CPOS and GnRHa in women aged > 35 years in order to evaluate the application value of CPOS in older women.
2. Materials and Methods
Study Design
This is a retrospectively registered study. All patients who received IVF/ICSI treatment at the Reproductive Center of Union Hospital, Tongji Medical College, and Huazhong University of Science and Technology between January 2016 and June 2021 were included. Patients meeting the following criteria were included in the statistical analysis: female patients >35 years old, < 50 years old; Indications for IVF or ICSI treatment; Ovarian stimulation was performed using either the GnRHa protocol or the CPOS protocol. Patients were excluded if they had any of the following criteria: hysterosalpingography or hysteroscopy indicating uterine abnormalities, recurrent miscarriage, rAFS stage III-IV (rAFS stage) endometriosis, donor oocyte/sperm cycles, preimplantation genetic testing cycles, or oocyte freezing cycles. All patients who became pregnant after IVF/ICSI treatment will be followed up on regularly during their pregnancy, and the post-birth follow-up will be done within one week after delivery. The patient's attending physician or the patient himself with full informed consent, decided whether the patient received ovarian stimulation using the CPOS or GnRHa protocol. Our center did not have any mandatory requirements for the ovarian stimulation protocol for women above the age of 35 during the observation period of this study. The two groups were further matched using baseline data for standard propensity score matching (PSM). The current study was approved by the Ethical Committee of Union Hospital (no. 2023-S0455) and has been registered in the Chinese Clinical Trial Registry (ChiCTR2300076537), and individual consent for this retrospective analysis was waived.
Ovarian Stimulation
- GnRHa protocol: Tripreilin acetate was injected 0.05mg/d (Ferring Pharmaceuticals, SaintPrex, Switzerland) at the middle luteal stage of the previous cycle for pituitary down-regulation. When the down-regulation standard was reached (serum luteinizing hormone (LH) < 5IU/L, serum estradiol (E2) < 50pg/ml, endometrial thickness <10mm, no functional ovarian cyst, urine follicle-stimulating hormone (uFSH) (Zhuhai Lizon Pharmaceutical, Zhuhai, China) or recombinant follicle-stimulating hormone (rFSH) (Merck Serono, Buchs, Switzerland) was initiated with 225-300U, and the adjustment was made according to the ovarian response.
- CPOS protocol: From the second or third day of menstruation until the trigger day, 100mg of CC (Fertila, Codal Synto Ltd., Cyprus) was administered orally; 225-300IU of uFSH were also administered daily, with the dosage being adjusted based on ovarian response.When bilateral ovaries had ≥2~3 follicles with diameter >18mm, 10000 IU human chorionic gonadotropin (hCG) (Lizhu Pharmaceutical Trading Co., China) or 250mg Ovidrel (Merck Serono S.p.A., Modugno, Italy) was administered to trigger the final maturation of the oocytes. Oocytes were retrieved 34~36h later. Transvaginal oocyte retrieval was performed 34–36h after hCG administration. Supplementary Figure S1.
Fertilization and Embryo Evaluation
Oocyte fertilization was achieved by IVF or ICSI based on the male partner’s sperm quality. For IVF fertilization, approximately 20,000 motile sperm are added to each oocyte. ICSI was conducted if the total motile sperm concentration was less than 5×106/ml or the proportion of normal sperm was less than 1%. The presentation of two pronuclei (2PN) 16–18 h after insemination was regarded as normal fertilization. The embryos were evaluated after 72 hours of in-vitro culture based on blastomere homogeneity and embryo fragmentation rate [19]. Embryos with 6-8 cells and grades 1 or 2 were regarded as top-quality embryos. Embryos that were not transferred at day (D) 3 were cultured in G2-plus medium (Vitrolife, Gothenburg, Sweden) for further 2-4 days to develop blastocysts. Blastocysts were graded using Gardner's grading scale [20].
Fresh and Frozen Embryo Transfer
Patients in the CPOS group underwent frozen embryo transfers using the "Freeze-all" strategy. patients in the GnRHa group who were eligible for fresh embryo transfer underwent the fresh embryo transfer at D3, D5, or D6. A maximum of two cleavage-stage embryos or blastocysts were transferred each time under the guidance of abdominal ultrasound. Those blastocysts that did not undergo fresh embryo transfer were frozen by vitrification. For frozen embryo transfer (FET), most cycles underwent hormone replacement cycles. The specifics of the vitrification, warming technique and endometrial preparation were previously detailed [21]. 10 mg twice-daily oral dydrogesterone (Duphaston, Abbott, USA) and 90 mg vaginal progesterone gel (Crinone; Merck Serono) were used for luteal support. In fresh embryo transfer cycle, luteal support was initiated on the second day after oocyte retrieval; while in frozen embryo transfer, it begins on the day of endometrial transformation. For pregnant patients, luteal support continues until 12 weeks of gestation.
Luteal Support
Luteal support was initiated from the embryo transfer, with the application of 10 mg twice-daily oral dydrogesterone (Duphaston, Abbott, USA) and 90 mg vaginal progesterone gel (Crinone; Merck Serono). 12-14 days following embryo transfer, pregnancy tests were conducted. Luteal support will be continued for pregnant patients until about 12 weeks of gestation.
Outcome Measures
The primary outcome measures of this study were the CLBR within 24 months after the patient initiated ovarian stimulation and TTLB. Secondary outcome measures included the incidence of premature LH surge, fertilization rate, blastocyst formation rate, clinical pregnancy rate and abortion rate. Furthermore, the number of retrieved oocytes, the rate of mature oocytes, the number of available embryos, the incidence of ovarian hyperstimulation syndrome (OHSS), the rate of multiple pregnancy, birth weight, and gestational age were compared between the two groups.
A live birth is defined as the birth of a live baby at 28 weeks of gestation or with a birth weight of more than 1000g. The CLBR defined as the number of cycles with at least one live birth in all fresh embryo or frozen embryo transfer cycles divided by the total number of initiated cycles over a two-year period. A clinical pregnancy was defined as the identification of a gestational sac 4 weeks after embryo transfer. The miscarriage rate was defined as the number of miscarriages before 28 weeks of gestation divided by the total number of clinical pregnancies. Cycle cancellation rate is the number of patients with no available embryos divided by the total number of patients initiating ovarian stimulation. The time to live birth is the interval between the initiation of ovarian stimulation and live birth. Only the first live birth was included when multiple live births occurred within a single ovarian stimulation cycle.
Cost-Effectiveness Analysis
The decision tree model of TreeAge Pro 2019 (TreeAge software, Inc., Williamstown, MA, USA) was used for cost-effectiveness analysis of the two ovarian stimulation protocol (Figure 1). A decision tree is a decision-making method that simulates a group of patients making decisions according to a pre-defined method, with associated probabilities, costs, and outcomes. Cost-effectiveness analysis based on decision tree model is a useful method to help assess the costs and outcomes of adopting new interventions [22].
The decision tree model constructed in this study incorporates key and costly major clinical events including pre-IVF examination, ovarian stimulation, oocyte retrieval, in-vitro embryo culture, embryo freezing and warming, embryo transfer, luteal support, miscarriage and childbirth fee. For both groups of patients, each embryo transfer will have three possible outcomes: no pregnancy, miscarriage and live birth. The decision tree model analysis provided us with an opportunity of no pregnancy, miscarriage, and live birth in each scenario. The CLBR is the major outcome/validity of this model.
In the cost-effectiveness analysis, the probability of live birth rate was calculated as the average live birth over all embryo transfer cycles. We generated estimates of probabilities of live birth or miscarriage per clinical pregnancy and estimates of probabilities of clinical pregnancy per embryo transfer. All probabilities used in our current study are shown in Supplementary Table S1.
This study's research perspective is the health-care system. As a result, non-medical costs, lost productivity, and time costs have been excluded from the cost analysis. The prices are based on approved IVF rates in Hubei Province, China in 2022. Discounts were not considered because the cost of each IVF procedure remained stable during the study period. Direct medical expenses mainly include the cost of the pre-IVF examination as well as costs incurred throughout the IVF cycle. We divided the direct medical costs of IVF into three categories in this study: examination costs (including laboratory and ultrasound fees), drug costs, and IVF-related procedure costs. The drug's cost covers ovarian stimulation, endometrial preparation, and luteal support. The costs of IVF procedures include oocytes retrieval, IVF laboratory procedures, cryopreservation and warming, and embryo transfer. The cost of patient abortion is assumed to include dilation and curettage under anesthesia. Only direct medical costs were included in the cost- effectiveness analysis of this study, as indirect costs are highly variable and difficult to calculate. All consolidated costs in RMB are shown in Table 1.
Sensitivity Analysis
One-way sensitivity analysis is performed to ensure the robustness of the cost-effectiveness analysis results by adjusting one parameter to the highest or lowest value at a time. Assume that each input parameter varies independently. The cost expenditure is set to fluctuate within a range of -20% to +20%. The live birth rate of fresh embryo transfer for GnRHa group was estimated to achieve comparable cost-effectiveness between two protocols. Use the tornado chart to show the results of the influence variables and one-way sensitivity. All parameters are based on real-world data from this study. The parameters used and their distribution are shown in Table 1.
Statistics Analyses
The Shapiro test was used to determine the normality of all continuous variables. Variables having a normal distribution were denoted by . The Student's t-test was used for statistical comparison. Variables that did not have a normal distribution were presented as median + interquartile range (IQR), and the Mann-Whitney U test was used to analyze differences between groups. The categorical variables were described in terms of n (%), the difference test was the Chi-square test, and the Fisher exact probability test was employed when the predicted number was small.
Because of the large difference in sample sizes between the two groups, subjects with similar features were selected through propensity score matching (PSM) with nearest neighbor matching and a caliper of 0.02. Female age (year), infertility duration (year), body mass index (BMI, kg/m2), basal follicle stimulation hormone (bFSH, IU/L), and infertility cause were the factors utilized for matching. Subclassfaction and Nearest Neighbor Matching are the methods for selecting a Matching object. Comparisons of important baseline characteristics between groups were not statistically significant. The logistic regression model was used to analyze the influencing factors that affect the live birth rate, the Kaplan-Meier curve was used for the cumulative live birth curve of the two protocols, and the log-rank test was utilized for the difference test. The influencing factors of cumulative live birth rate were analyzed by Cox proportional risk model.
Statistical analyses were performed using the Statistical Program for Social Sciences (SPSS Inc., Version 24.0, Chicago) and R version 4.1.0 (R Core Team, Vienna, Austria). The 2-tailed value of P<.05 was considered statistically significant.
3. Results
Between January 2016 and June 2021, 11 809 IVF/ICSI cycles were done in our center. There were 2871 cycles that matched the inclusion criteria but did not meet the exclusion criteria, with 1074 cycles using the GnRHa protocol and 1797 cycles using the CPOS protocol. Supplementary Figure S2.
3.1. Comparisons of Baseline Characteristics between the Two Groups
Before matching, there were significant differences in female age, infertility length, infertility types, basal AMH, basal serum FSH, infertility causes, and insemination methods between the CPOS and GnRHa groups. To reduce bias caused by differences in baseline characteristics between the two groups, PSM was performed at a 1:1 ratio using the 9 aforementioned variables. After matching, 375 cycles were assigned to the GnRHa and CPOS groups respectively, with no significant difference in baseline characteristics between the matched groups. The comparison of baseline characteristics between the two groups before and after matching is shown in Table 1.
3.2. Comparisons of Ovarian Stimulation and Embryonic Laboratory Outcomes
The rate of cycle cancellation in CPOS group was significantly higher than that in GnRHa group (13.07% vs 8.00%, p=0.032). However, this was mainly due to the implementation of blastocyst embryo culture and freeze-all strategy in the CPOS group, which resulted in more patients in this group having no available embryos after in vitro blastocyst culture (6.13% vs 2.4%, p=0.018). Meanwhile, the number of cycles of ovarian stimulation failure, premature ovulation, oocyte retrieval failure and no normal fertilized oocytes exhibited no significant difference (all p>0.05). There was no significant difference in the duration of ovarian stimulation and the total of gonadotropin dosage between the two groups. Premature LH surge was more common in the CPOS group than in the GnRHa group (6.13% vs 0.53%, p< 0.001), although there was no difference in premature ovulation rate between the two groups. Table 2.
In the outcomes of the embryonic laboratory, the CPOS group had significantly fewer retrieved oocytes and a significantly higher rate of oocyte maturation than the GnRHa group [6(4, 10) vs. 11(7, 11), p<0.001; 88.89% (75%, 100%) vs. 85.71% (72.73%, 100%), p = 0.001, respectively]. However, there were no significant differences in normal fertilization rate, cleavage rate, top-quality embryo rate and blastocyst formation rate between the two groups. Table 2.
3.3. Comparisons of Clinical Outcomes between the Two Groups
During the two-year study period, 445 FETs were performed in the CPOS group. 562 transfer cycles were conducted in the GnRHa group (214 fresh embryo transfer and 348 FET). Because the blastocyst culture and freeze-all strategy were implemented in the CPOS group, the embryo implantation rate (45.42% vs 39.46%, p=0.028) and the clinical pregnancy rate per transfer (52.36% vs 46.02%, p=0.049) were significantly higher than those in the GnRHa group. However, there were no significant differences in the rate of multiple pregnancy, miscarriage and ectopic pregnancy per transfer between the two groups (all p>0.05). The incidence of moderate or severe OHSS was not significantly different between the two groups. Table 3.
To calculate the cumulative clinical outcomes over 24 months of follow-up, the total of the initial cycle was used as the denominator. The CPOS group had a significantly lower cumulative clinical pregnancy rate than the GnRHa group (51.73% vs 60.27%, P=0.023). The CLBR, however, did not differ significantly between the two groups (41.07% vs 45.33%, p=0.269). (Table 3). Furthermore, no significant difference in the cumulative live birth rate was observed between the two groups in the Kaplan-Meier analysis at the final follow-up point (24 months) (p=0.081, HR (95%CI) =0.82 (0.66-1.02)) (Fig. 2). There were no significant differences in gestational age, birth weight, or preterm birth rate between the two groups. The time to live birth (TTLB) is calculated from the day of oocyte retrieval to the day of live birth. The TTLB in the CPOS group was considerably longer than in the GnRHa group [360(315.8, 445) vs 326.5(257.5, 435.8), p=0.001], and the median time to live birth in the CPOS group was about 33.5 days later. Table 3.
A binary logistics regression analysis was performed, which included female age, infertility type, duration of infertility, number of IVF cycles, BMI, basal FSH, AMH, total gonadotropin dosage, duration of ovarian stimulation, number of oocytes retrieved, number of available embryos, infertility causes, and the ovarian stimulation protocol. After controlling for other confounding factors, female age, AMH, and the number of available embryos were found to be significantly associated with CLBR. However, the ovarian stimulation protocol (CPOS or GnRHa protocol) had no effect on the CLBR (hazard ratio (HR) 95%CI=1.475(0.994-2.187); p=0.084). Table 4.
3.4. Subgroup Analysis
Subgroup analysis was conducted based on age (≥ 40 or < 40 years) and cycle number (1st or 2nd cycle). The Kaplan-Meier subgroup analysis results also demonstrated that, at the last follow-up time point (24 months), there was no statistically significant difference in CLBR between the CPOS treatment and the GnRHa protocol, regardless of age or cycle number stratification (all p-values > 0.05). (Figure 2A–E). Particularly in the 2nd cycle subgroups, the differences in CLBR between CPOS and GnRHa were even more marginal. Figure 2E.
3.5. Cost-Effectiveness Analysis
The average cost per patient in the CPOS group was 21.27% less than that in the GnRHa group (¥32301.42 vs ¥39174.22). The cost per live birth in the CPOS group was ¥79,367.07, while the cost per live birth in the GnRHa group was ¥84,996.05. Compared with the CPOS group, the cumulative live birth rate in the GnRHa group was higher, but the incremental cost-effectiveness ratio (ICER) for each additional live birth was ¥127493.9.
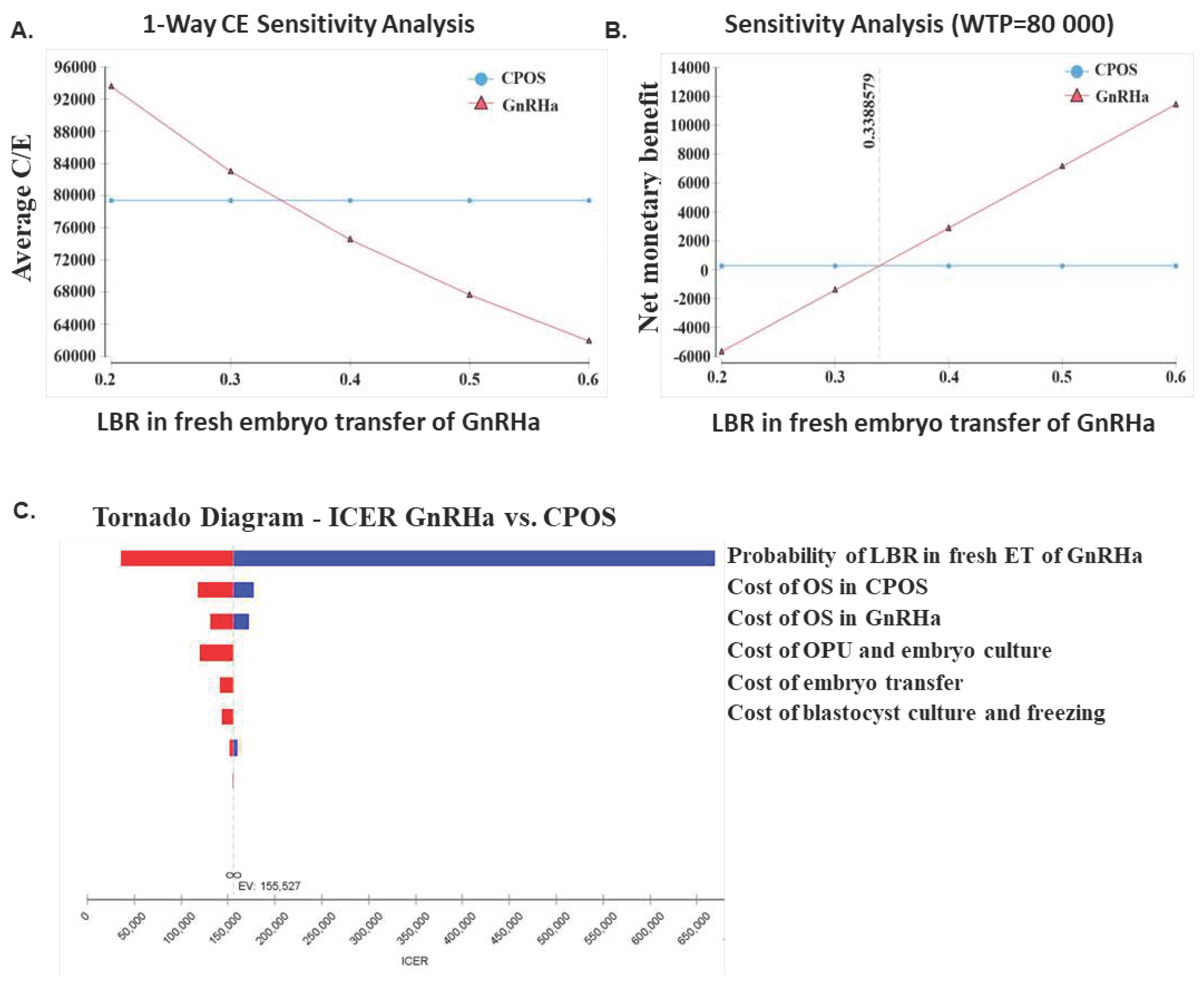
When the live birth rate of fresh embryo transfer in the GnRHa group increased to 33.89%, the cost per live birth in the GnRHa group was comparable to that in the CPOS group, according to one-way sensitivity analysis. The tornado chart of one-way sensitivity analysis revealed that the live birth rate of fresh embryo transfer and the cost of ovarian stimulation were the most important factors influencing ICERs. All of these data indicate that our model is very robust.
Figure 3.
One-way sensitivity analysis of cost-effectiveness ratio between CPOS and GnRHa. (A) one-way C/E sensitivity analysis. (2) one-way NMB sensitivity analysis. (3) Tornado diagram. The parameters affecting the ICER are shown. CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonists; LBR, live birth rate; OS, ovarian stimulation; OPU, oocyte pick-up; ICER, incremental cost-effectiveness ratio; NMB, Net monetary benefit.
Figure 3.
One-way sensitivity analysis of cost-effectiveness ratio between CPOS and GnRHa. (A) one-way C/E sensitivity analysis. (2) one-way NMB sensitivity analysis. (3) Tornado diagram. The parameters affecting the ICER are shown. CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonists; LBR, live birth rate; OS, ovarian stimulation; OPU, oocyte pick-up; ICER, incremental cost-effectiveness ratio; NMB, Net monetary benefit.
4. Discussion
After ovarian stimulation, retrieving a specific number and quality of oocytes is critical for IVF success. The largest barrier to achieving an optimal IVF live birth rate in women over the age of 35 is the aging-related reduction in oocyte development potential and/or oocyte number. Over the last two decades, older patients have been subjected to various ovarian stimulation protocols such as GnRHa [23], GnRH antagonist, mild-stimulation [24], double ovarian stimulation, natural/modified natural cycle [25], etc., as well as complementary drugs [26,27] such as growth hormone, recombinant luteinizing hormone, dehydroepiandrosterone, coenzyme Q10, etc. However, the efficacy, safety, and cost-effectiveness of each treatment have yet to be determined. In this PSM retrospective cohort study of infertile women over the age of 35, we found no significant difference in CLBR between CPOS group and conventional GnRHa group (41.07% vs 45.33%). The TTLB for those using the CPOS protocol was increased, but the cost per live birth was significantly lower than for those using the conventional GnRHa protocol.
In our current study, we first compared the oocyte and embryo quality between the CPOS and GnRHa protocols after PSM, and discovered that while the number of oocytes retrieved was lower in the CPOS group, the oocyte maturity rate was significantly higher. It is worth noting that there were no significant differences between the two groups in terms of normal fertilized oocyte rate, high-quality embryo rate and blastocyst formation rate, suggesting that there was no difference in oocyte competence and embryonic development potential. This is consistent with the findings of Bhor SA et al., who discovered that ovarian stimulation with CC and gonadotropin had no effect on blastocyst formation rate when compared to a GnRH antagonist strategy [17]. Furthermore, Utilizing CC to induce ovulation has been reported in PCOS animal models to reverse insulin-like growth factor family gene and transforming growth factor family gene expression disorders in the ovum, increase oocyte maturation, and improve IVM-IVF treatment outcome [28].
In our current study, due to the continuous usage of CC in the CPOS protocol until the trigger day, and considering the influence of CC on endometrial receptivity, the CPOS group underwent blastocyst culture and a “freeze-all” strategy. This also explains why the TTLB time in the CPOS group is much longer than in the GnRHa group. Meanwhile, it is not possible to directly compare the pregnancy outcomes of single embryo transfer under the two protocols, hence the CLBR of one IVF cycle was chosen as one of the key outcome measures in this study. Our results showed that the CPOS group had higher rates of embryo implantation and clinical pregnancy per transfer, therefore even though this group had a higher rate of cycle cancellation, there was no significant difference in the CLBR per initiating cycle between the two groups. In addition, there were no significant differences in gestational age, average weight, preterm birth rate and incidence of congenital malformations between the two groups. The results showed that CPOS protocol did not have adverse effects on embryonic development potential and progeny health. A recent retrospective study also showed that recent (<90 days) CC exposure did not affect the implantation potential of mono-euploid embryo transfer [29]. Furthermore, a small sample size retrospective cohort analysis found that, when compared to an antagonist protocol, using their CC and gonadotropin protocol had no influence on live birth rate of frozen embryo transfer [17]. In terms of cumulative live birth rate and progeny safety, the CPOS protocol is equivalent to the GnRHa protocol in infertile women over the age of 35.
The rate of ART utilization is largely related to the technology's affordability and accessibility [30]. The expensive expense of IVF is a major reason why many couples discontinue treatment [31,32,33]. Multiple cycles of ovarian stimulation and oocyte retrieval may be required in older women due to a decrease in the quantity of oocytes retrieved or oocyte competence, which raises the cost. As a result, selecting the right ovarian stimulation protocol for these patients should take into account not only the success rate, but also the cost-effectiveness [33]. The cost of various ovarian stimulation protocols might vary greatly depending on the drug dosage and the number of embryo transfer cycles. For example, mild-stimulation protocols, which have been studied more frequently in IVF of older patients in recent years, may have a higher average cost per live birth than conventional protocols, due to their low oocyte retrieval per cycle and high cycle cancellation rate, which often necessitate multiple cycles of ovarian stimulation and embryo transfer [34]. As a result, some physicians believe that retrieving a sufficient number of mature oocytes in a single ovarian stimulation cycle is necessary. Blastocyst culture, single blastocyst transfer and vitrification of excess embryos after oocyte retrieval are less expensive and more efficient than "unconventional" protocols such as natural cycle, modified natural cycle, aromatase inhibitor/low-dose FSH protocol, and CC/low-dose FSH protocol [35]. In our current study, we found that the cost per live birth in the CPOS group was significantly lower than that in the GnRHa group. The observed outcome can be attributed to two significant factors: First, the CPOS group uses CC in combination with gonadotropin for ovarian stimulation, which reduces pharmaceutical expenditures significantly. Second, CPOS patients underwent blastocyst culture and freeze-all strategy, resulting in fewer embryo transfer cycles per live birth. CPOS is less expensive than GnRHa for women over the age of 35, which justifies its use in this age group.
In this study, we further carried out subgroup analysis based on the female age and number of cycles, and the results showed that no significant difference was observed in CLBR between subgroups regardless of whether CPOS or GnRHa was used. Especially in the 2nd cycle subgroup comparison, the CLBR curves of the two protocols almost overlap. Since many patients in repeat IVF cycles are unexpected poor ovarian response or poor embryo quality, several studies have reported that the addition of CC therapy in repeat IVF cycles can improve ovarian response and minimize cycle cancellation rate [36,37]. Based on these results, we believed that the application of CPOS protocol in older patients with repeated IVF cycles deserves further investigation in future prospective studies.
To our knowledge, this is the first study to compare a CC-based ovarian stimulation protocol with the GnRHa protocol to investigate its CLBR, TTLB, and cost-effectiveness. Doctors should consider cost-effectiveness while recommending ovarian stimulation to patients. Secondly, we included non-selective infertile couples older than 35 years, and calculated the CLBR of one IVF cycle in the 24 months after oocytes retrieval, and none of the patients were lost to follow-up. Our cohort's results are therefore applicable to general population above the age of 35. The other advantage of the current study was the use of PSM to balance the baseline characteristic differences between the CPOS and GnRHa groups. This is because selective bias and imbalance of baseline characteristics between groups are very common problems in observational studies [38]. The main advantage of propensity score matching (PSM) is its capacity to eliminate potential bias between treatment and control groups in observational studies, improving internal validity and enabling more reliable outcome comparisons [39].
There are some limitations to our current study. First, this was a single-center retrospective study, and a variety of potential confounding factors could have affected the results. Although the PSM method was adopted in this study to match 9 baseline characteristics at a 1:1 ratio and eliminate the influence of confounding factors as much as possible, some known or unknown confounding factors may still affect the statistical results. Secondly, during the study period, the main ovarian stimulation protocols for older patients in our center were CPOS and GnRHa, and a few patients underwent GnRH antagonists and mild-stimulation protocol. Hence, in this current study, we were unable to directly compare CPOS with other ovarian stimulation protocols.
5. Conclusions
This study found that cumulative live birth rates among CPOS in older women were similar to GnRHa. Despite CPOS having a longer TTLB than GnRHa, the economic cost per live birth was significantly lower with CPOS. This suggests that CPOS is a viable choice for ovarian stimulation protocol in older women undergoing IVF.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Schematic diagram of the two ovarian stimulation protocols; Figure S2: The study flow chart; Table S1: Decision tree model input parameters.
Author Contributions
Conceptualization, Y.L. (Yanhui Li) and Y.L. (Yi Liu); Data curation, Y.L. (Yanhui Li), D.L. and T.L.; Formal analysis, Y.L. (Yanhui Li) and T.L.; Investigation, Y.L. (Yanhui Li), D.L., T.L. and H.D.; Methodology, H.D.; Supervision, Y.L. (Yi Liu); Writing—original draft, Y.L. (Yanhui Li) and T.L.; Writing—review & editing, Y.L., D.L., H.D. and Y.L. (Yi Liu). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The study has been approved by the Medical Ethical Committee of Union Hospital (no. 2023-S0455) and registered in the Chinese Clinical Trial Registry (ChiCTR2300076537).
Informed Consent Statement
Patient consent was waived because this study was a retrospective study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We would like to express our gratitude to Pro. Yajia Lan for his statistical advice. We also would like to thank our colleagues at the Reproductive Medicine Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vollset SE, Goren E, Yuan CW, Cao J, Smith AE, Hsiao T, Bisignano C, Azhar GS, Castro E, Chalek J et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020;396:1285-1306. [CrossRef]
- Zhou Z, Zheng D, Wu H, Li R, Xu S, Kang Y, Cao Y, Chen X, Zhu Y, Xu S et al. Epidemiology of infertility in China: a population-based study. Bjog. 2018;125:432-441. [CrossRef]
- Kushnir VA, Smith GD, Adashi EY. The Future of IVF: The New Normal in Human Reproduction. Reprod Sci. 2022;29:849-856. [CrossRef]
- Chua SJ, Danhof NA, Mochtar MH, van Wely M, McLernon DJ, Custers I, Lee E, Dreyer K, Cahill DJ, Gillett WR et al. Age-related natural fertility outcomes in women over 35 years: a systematic review and individual participant data meta-analysis. Hum Reprod. 2020;35:1808-1820. [CrossRef]
- Kouvidi E, Zachaki S, Tsarouha H, Pantou A, Manola KN, Kanavakis E, Mavrou A. Female Reproductive Ageing and Chromosomal Abnormalities in a Large Series of Women Undergoing IVF. Cytogenet Genome Res. 2021;161:551-555. [CrossRef]
- Cimadomo D, Fabozzi G, Vaiarelli A, Ubaldi N, Ubaldi FM, Rienzi L. Impact of Maternal Age on Oocyte and Embryo Competence. Front Endocrinol (Lausanne). 2018;9:327. [CrossRef]
- Pathare ADS, Loid M, Saare M, Gidlöf SB, Zamani Esteki M, Acharya G, Peters M, Salumets A. Endometrial receptivity in women of advanced age: an underrated factor in infertility. Human Reproduction Update. 2023. Online ahead of print. [CrossRef]
- Ubaldi FM, Cimadomo D, Vaiarelli A, Fabozzi G, Venturella R, Maggiulli R, Mazzilli R, Ferrero S, Palagiano A, Rienzi L. Advanced Maternal Age in IVF: Still a Challenge? The Present and the Future of Its Treatment. Front Endocrinol (Lausanne). 2019;10:94. [CrossRef]
- Pai AH, Sung YJ, Li CJ, Lin CY, Chang CL. Progestin Primed Ovarian Stimulation (PPOS) protocol yields lower euploidy rate in older patients undergoing IVF. Reprod Biol Endocrinol. 2023;21:72. [CrossRef]
- Sovino H, Sir-Petermann T, Devoto L. Clomiphene citrate and ovulation induction. Reproductive biomedicine online. 2002;4:303-310.
- Ovarian Stimulation TEGGO, Bosch E, Broer S, Griesinger G, Grynberg M, Humaidan P, Kolibianakis E, Kunicki M, La Marca A, Lainas G et al. ESHRE guideline: ovarian stimulation for IVF/ICSI(†). Hum Reprod Open. 2020;2020:hoaa009. [CrossRef]
- Bechtejew TN, Nadai MN, Nastri CO, Martins WP. Clomiphene citrate and letrozole to reduce follicle-stimulating hormone consumption during ovarian stimulation: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2017;50:315-323. [CrossRef]
- Lin HT, Wu MH, Tsai LC, Chen TS, Ou HT. Co-Administration of Clomiphene Citrate and Letrozole in Mild Ovarian Stimulation Versus Conventional Controlled Ovarian Stimulation Among POSEIDON Group 4 Patients. Front Endocrinol (Lausanne). 2021;12:780392. [CrossRef]
- Revelli A, Chiadò A, Dalmasso P, Stabile V, Evangelista F, Basso G, Benedetto C. "Mild" vs. "long" protocol for controlled ovarian hyperstimulation in patients with expected poor ovarian responsiveness undergoing in vitro fertilization (IVF): a large prospective randomized trial. J Assist Reprod Genet. 2014;31:809-815. [CrossRef]
- Gleicher N, Weghofer A, Barad DH. A case-control pilot study of low-intensity IVF in good-prognosis patients. Reprod Biomed Online. 2012;24:396-402. [CrossRef]
- Le H, Nguyen DD, Cao AT, Nguyen HTL, Tham DC, Le TD, Hugues JN. Comparative Effectiveness of Mild or Conventional GnRH-Antagonist Protocols for Ovarian Stimulation in Poor Responders (Poseidon Group 4). Front Reprod Health. 2020;2:606036. [CrossRef]
- Bhor SA, Nakayama K, Ono H, Iwashita T, Kinoshita K. Effects of controlled ovarian stimulation regimens on top-quality blastocyst development and perinatal outcomes with the freeze-all strategy: A retrospective comparative study. Clin Exp Reprod Med. 2023;50:132-140. [CrossRef]
- Singh A, Bhandari S, Agrawal P, Gupta N, Munaganuru N. Use of clomiphene-based stimulation protocol in oocyte donors: A comparative study. J Hum Reprod Sci. 2016;9:159-163. [CrossRef]
- Veeck LL. Oocyte assessment and biological performance. Ann N Y Acad Sci. 1988;541:259-274. [CrossRef]
- Gardner DK, Lane M, Stevens J, Schlenker T, Schoolcraft WB. Blastocyst score affects implantation and pregnancy outcome: towards a single blastocyst transfer. Fertil Steril. 2000;73:1155-1158. [CrossRef]
- Liu L, Li YH, Ding XF, Geng YH, Chen CY, Gao Y. Influence of blastocysts morphological score on pregnancy outcomes in frozen-thawed blastocyst transfers: a retrospective study of 741 cycles. J Huazhong Univ Sci Technolog Med Sci. 2014;34:750-754. [CrossRef]
- Payne K, Gavan SP, Wright SJ, Thompson AJ. Cost-effectiveness analyses of genetic and genomic diagnostic tests. Nat Rev Genet. 2018;19:235-246. [CrossRef]
- Liu M, Zhao X, Peng Y, Zheng J, Guo K, Fan Y, Jiang L, Yang A, Cui N, Hao G. Outcomes After a Single Ovarian Stimulation Cycle in Women of Advanced Reproductive Age: A Retrospective Analysis. Frontiers in Endocrinology. 2022;13:792159.
- Cozzolino M, Cecchino GN, Bosch E, Garcia-Velasco JA, Garrido N. Minimal ovarian stimulation is an alternative to conventional protocols for older women according to Poseidon’s stratification: a retrospective multicenter cohort study. Journal of Assisted Reproduction and Genetics. 2021;38:1799-1807.
- Drakopoulos P, Romito A, Errázuriz J, Santos-Ribeiro S, Popovic-Todorovic B, Racca A, Tournaye H, De Vos M, Blockeel C. Modified natural cycle IVF versus conventional stimulation in advanced-age Bologna poor responders. Reproductive biomedicine online. 2019;39:698-703.
- Haahr T, Dosouto C, Alviggi C, Esteves SC, Humaidan P. Management Strategies for POSEIDON Groups 3 and 4. Front Endocrinol (Lausanne). 2019;10:614. [CrossRef]
- Zhu F, Yin S, Yang B, Li S, Feng X, Wang T, Che D. TEAS, DHEA, CoQ10, and GH for poor ovarian response undergoing IVF-ET: a systematic review and network meta-analysis. Reprod Biol Endocrinol. 2023;21:64. [CrossRef]
- Ghasemian F, Esmaeilnezhad S. Metformin, clomiphene citrate and flutamide effects on oocyte ultrastructure status and quality in PCOS mouse model. Reprod Biomed Online. 2022;45:191-201. [CrossRef]
- Hernandez-Nieto C, Lee J, Alkon-Meadows T, Soto-Cossio L, Sandler B, Mukherjee T, Copperman A. Recent clomiphene citrate exposure does not impact subsequent clinical outcomes in single euploid frozen embryo transfer cycles. Hum Reprod. 2023. [CrossRef]
- Chambers GM, Adamson GD, Eijkemans MJ. Acceptable cost for the patient and society. Fertility and sterility. 2013;100:319-327.
- Chambers GM, Sullivan EA, Ishihara O, Chapman MG, Adamson GD. The economic impact of assisted reproductive technology: a review of selected developed countries. Fertility and sterility. 2009;91:2281-2294.
- Verberg M, Eijkemans M, Heijnen E, Broekmans F, de Klerk C, Fauser B, Macklon N. Why do couples drop-out from IVF treatment? A prospective cohort study. Human reproduction. 2008;23:2050-2055.
- Dewi AK, Wicaksana AL, Lutfi M, Dewanto A. The barriers of joining in vitro fertilization programs among infertile couples in developing countries: A scoping review. Asian Pacific Journal of Reproduction. 2023;12:147-154.
- Liu Y, Su R, Wu Y. Cumulative live birth rate and cost-effectiveness analysis of gonadotropin releasing hormone-antagonist protocol and multiple minimal ovarian stimulation in poor responders. Frontiers in Endocrinology. 2021;11:605939.
- Zech NH, Zech M, Baldauf S, Comploj G, Murtinger M, Spitzer D, Hradecký L, Ajayi R, Schuff M, Zech H. Ovarian stimulation in ART - Unwinding pressing issues. Minerva Ginecol. 2015;67:127-147.
- Ochin H, Ma X, Wang L, Li X, Song J, Meng Y, Shen J, Cui YG, Liu J. Low dose clomiphene citrate as a mild stimulation protocol in women with unsuspected poor in vitro fertilization result can generate more oocytes with optimal cumulative pregnancy rate. J Ovarian Res. 2018;11:37. [CrossRef]
- Triantafyllidou O, Sigalos G, Gkoles L, Kastora S, Vakas P, Batsiou E, Vlahos N. The addition of clomiphene citrate to ovarian stimulation protocols for poor responders. Eur J Obstet Gynecol Reprod Biol. 2020;251:136-140. [CrossRef]
- Schuster NA, Rijnhart JJM, Bosman LC, Twisk JWR, Klausch T, Heymans MW. Misspecification of confounder-exposure and confounder-outcome associations leads to bias in effect estimates. BMC Med Res Methodol. 2023;23:11. [CrossRef]
- Austin PC. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivariate Behav Res. 2011;46:399-424. [CrossRef]
Figure 1.
Decision tree model based on the real-world data of this study. Note: CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonist; Nodes within the model are marked by circles, triangles define endpoints.
Figure 1.
Decision tree model based on the real-world data of this study. Note: CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonist; Nodes within the model are marked by circles, triangles define endpoints.
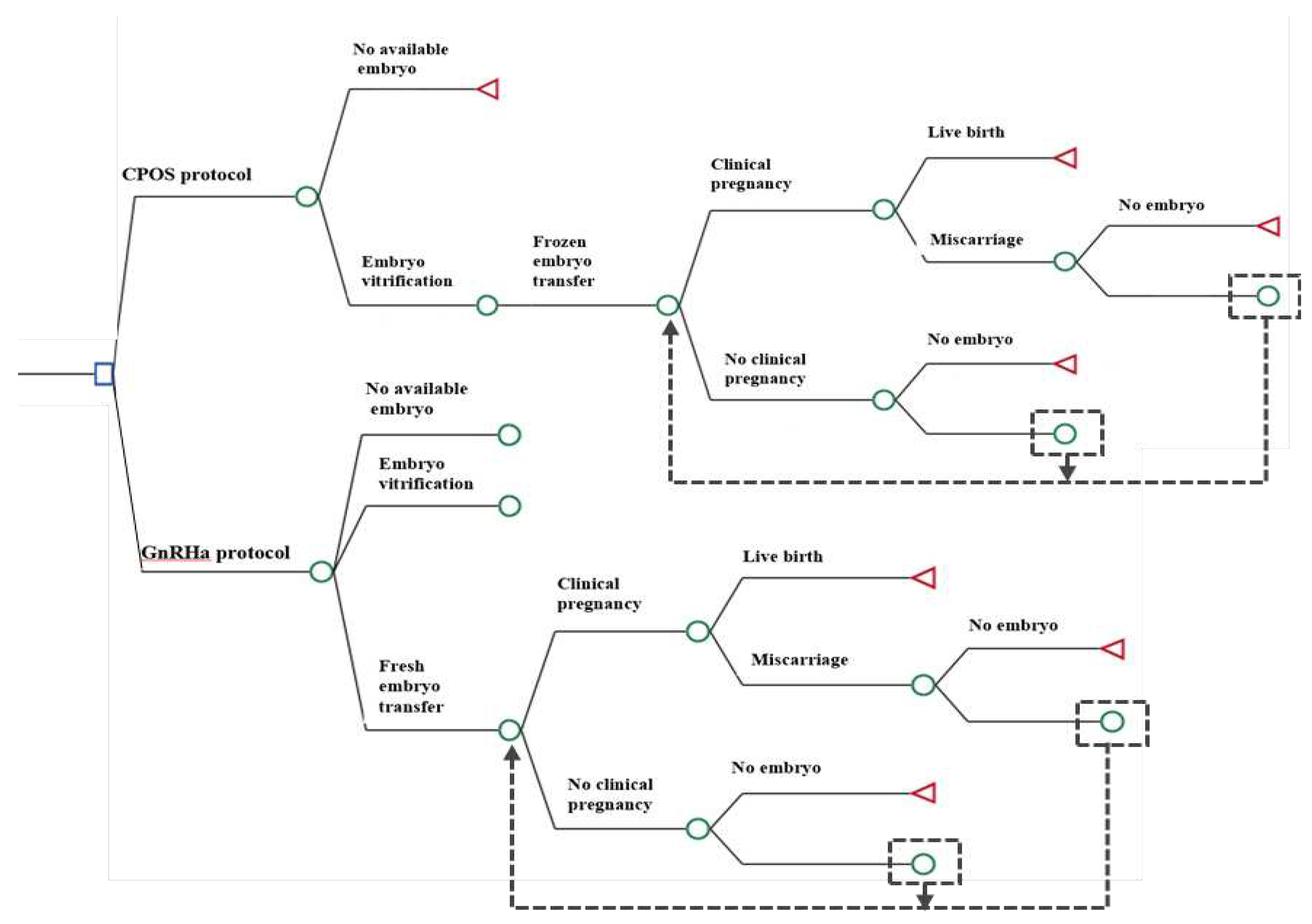
Figure 2.
Kaplan-Meier curves of the cumulative live birth rate (CLBR) in patients using CPOS and GnRHa protocol. (A) CLBRs of all the patients; (B) CLBRs in women aged >35 and <40 years; (C) CLBRs in women aged≥40 years; (D) CLBRs in women with first IVF cycle; (E)CLBRs in women with second IVF cycles. CI=confidence interval; CPOS= clomiphene-primed ovarian stimulation; GnRHa=gonadotropin-releasing hormone agonist; HR=Hazard ratio.
Figure 2.
Kaplan-Meier curves of the cumulative live birth rate (CLBR) in patients using CPOS and GnRHa protocol. (A) CLBRs of all the patients; (B) CLBRs in women aged >35 and <40 years; (C) CLBRs in women aged≥40 years; (D) CLBRs in women with first IVF cycle; (E)CLBRs in women with second IVF cycles. CI=confidence interval; CPOS= clomiphene-primed ovarian stimulation; GnRHa=gonadotropin-releasing hormone agonist; HR=Hazard ratio.
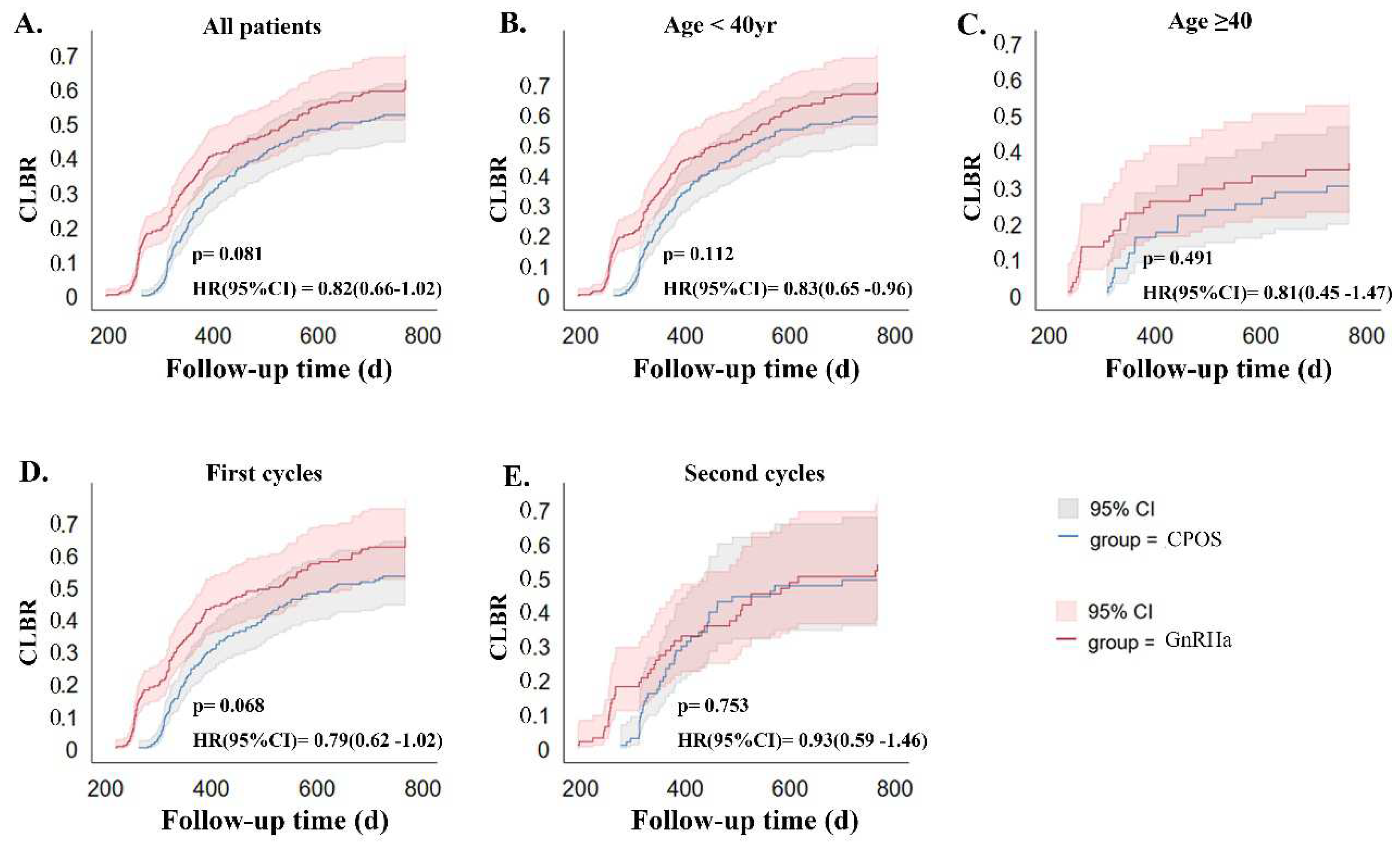

Table 1.
Baseline characteristics of women in the CPOS and GnRHa groups before and after matching.
| Before Propensity Score Matching | Before Propensity Score Matching | |||||
|---|---|---|---|---|---|---|
| Characteristic | GnRHa group (n=1,074) |
CPOS group (n=1,797) |
P value | GnRHa group (n=375) |
CPOS group (n=375) |
P Value |
| Age of women (y) | 36(35, 38) | 39(37,42) | <0.001 | 37(36, 39) | 37(36, 39) | 0.410 |
| Infertility duration (y) | 3(2, 7) | 4(2, 8) | 0.023 | 4(2, 8) | 3(2, 7) | 0.268 |
| Primary infertility, n (%) | 349(32,50) | 381(21.20) | <0.001 | 110(29.33) | 99(26.40) | 0.415 |
| Cycle number, n (%) | <0.001 | 1 | ||||
| First cycle | 909(84.64) | 1116(62.10) | 278(74.10) | 279(74.40) | ||
| Repeated cycles | 165(15.36) | 681(37.90) | 97(25.90) | 96(25.60) | ||
| Basal FSH level (IU/L) | 6.70(5.68, 7.96) | 8.36(6.77, 10.92) | <0.001 | 7.24(6.13, 8.21) | 7.12(6.01, 9.07) | 0.376 |
| Basal LH level (IU/L) | 4.75(3.50, 6.56) | 4.51(3.36, 6.15) | 0.001 | 5.15(3.65, 6.45) | 5.09(3.47, 6.42) | 0.340 |
| AMH (ng/ml) | 3.43(2.22, 5.23) | 1.09(0.63, 1.74) | <0.001 | 1.35(1.01,2.55) | 1.45(0.94, 2.13) | 0.270 |
| Body mass index (kg/m2) | 22.71(20.80, 25.03) | 22.60(20.80, 24.70) | 0.189 | 22.88(21.01, 24.93) | 22.91(21.13, 25.12) | 0.237 |
| Casue of infertility, n(%) | <0.001 | 0.956 | ||||
| Tubal | 376(35.01) | 810(45.08) | 133(35.47) | 145(38.67) | ||
| Male factor | 106(9.87) | 251(13.97) | 35(9.33) | 29(7.73) |
0.230 |
|
| Anovulatory | 39(3.63) | 57(3.17) | 42(11.20) | 35(9.33) | ||
| Unexplained | 327(30.45) | 294(16.36) | 104(27.73) | 98(26.13) | ||
| Diminished ovarian reserve | 181(16.85) | 304(16.92) | 39(10.40) | 40(10.67) | ||
| Endometriosis | 40(3.72) | 66(3.67) | 16(4.27 | 22(5.87) | ||
| Mixed factors | 5(0.47) | 15(0.83) | 6(1.60) | 6(1.60) | ||
| Insemination method, n(%) | <0.001 | |||||
| IVF | 714(66.48) | 916(50.97) | 250(66.66) | 229(61.07) | ||
| ICSI | 320(29.80) | 818(45.52) | 111(29.60) | 133(35.47) | ||
| IVF+RICSI | 40(3.72) | 63(3.51) | 14(3.73) | 13(3.47) | ||
Note: Data are presented as the median (25th and 75th percentile) or number (%). Mann–Whitney U statistics were used for continuous variables and chi-square tests were used for categorical variables. There were no significant differences after propensity score matching. CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonists; FSH, follicle-stimulating hormone; LH, luteinizing Hormone; AMH, anti-Müllerian hormone; IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; RICSI, early rescue intracytoplasmic sperm injection.
Table 2.
Ovarian stimulation and embryonic laboratory outcomes between two groups after propensity score matching.
Table 2.
Ovarian stimulation and embryonic laboratory outcomes between two groups after propensity score matching.
| Characteristic | CPOS Group | GnRHa Group | p Value | Subgroup Analysis | |||||
|---|---|---|---|---|---|---|---|---|---|
| CPOS <40yr | GnRHa <40yr | P Value | CPOS ≥40yr | GnRHa ≥40yr | P Value | ||||
| Patients, n | 375 | 375 | - | 296 | 298 | - | 79 | 77 | - |
| Failure of Ovarian stimulation | 4(1.07) | 3(0.80) | 1.000 | 3(1.01) | 1(0.34) | 0.372 | 1(1.27) | 2(2.60) | 0.618 |
| Premature LH surge, n (%) | 23(6.13) | 2(0.53) | <0.001 | 17(5.74) | 0(0) | <0.001 | 7(8.86) | 2(2.60) | 0.167 |
| Premature ovulation | 9(2.40) | 3(0.80) | 0.143 | 5(1.69) | 2(0.67) | 0.285 | 4(5.06) | 1(1.30) | 0.367 |
| No oocyte retrieved cycles during OPU, n (%) | 9(2.40) | 4(1.06) | 0.263 | 5(1.69) | 2(0.67) | 0.285 | 4(5.06) | 3(3.90) | 1.000 |
| No. of cycles without available embryo after culture, n (%) | 23(6.13) | 9(2.4) | 0.018 | 15(5.07) | 5(1.68) | 0.024 | 8(10.13) | 4(5.19) | 0.369 |
| Total no. of cycle cancellations, n (%) | 49(13.07) | 30(8.00) | 0.032 | 32(10.81) | 19(6.38) | 0.06 | 17(21.52) | 11(14.29) | 0.298 |
| Not undergo embryo transfer, n (%) | 5(1.33) | 9(2.40) | 0.420 | 4(1.35) | 8(2.68) | 0.383 | 1(1.27) | 1(1.30) | 1.000 |
| LH on trigger day (mIU/mL) | 7.83(4.92, 10.49) | 2.81(2.29, 3.48) | <0.001 | 2.81(2.36, 3.53) | 7.62(4.65, 10.41) | <0.001 | 5.36(2.03, 11.37) | 2.42(1.90, 3.44) | <0.001 |
| E2 on trigger day (pg/ml) | 1447(884.2, 2268) | 1609(936, 2516) | 0.18 | 1665(883.4, 2351) | 1884(1014, 2809) | 0.09 | 1193(881.4, 1986) | 1248(824, 1989) | 0.453 |
| Progesterone on trigger day (ng/ml) | 0.97(0.64, 1.38) | 0.95(0.70, 1.24) | 0.728 | 1.10(0.68, 1.45) | 0.92(0.69, 1.22) | 0.170 | 0.83(0.56, 1.15) | 0.92(0.71, 1.24) | 0.581 |
| Gn dosage (IU) | 2495(2025, 3075) | 2400(2000, 3088) | 0.356 | 2362(2025, 3000) | 2400(2000, 2925) | 0.545 | 3000(2700, 3675) | 3000(2700, 3450) | 0.773 |
| Gn duration, d | 10(9, 12) | 10(9, 12) | 0.071 | 10(9, 12) | 10(9, 12) | 0.108 | 10(9, 12) | 11(10, 12) | 0.301 |
| Moderate or severe OHSS n (%) | 7(1.86) | 9(2.40) | 0.801 | 7(2.36) | 8(2.68) | 1.000 | 0 | 1(1.30) | 0.494 |
| Average no. of oocytes retrieved | 6(4, 10) | 11(7, 11) | <0.001 | 7(5, 13) | 11(8, 14) | 0.006 | 5(3, 9) | 7(4, 10) | 0.007 |
| Mature oocyte rate, % | 88.9(75.0, 100) | 85.7(72.7, 100) | 0.001 | 87.5(75.0, 100) | 85.7(72.8, 96.4) | 0.008 | 97.1(78.1, 100) | 87.5(71.4, 100) | 0.058 |
| Normal fertilization rate, % | 75.0(60.0, 100) | 75.0(57.3, 87.4) | 0.255 | 75.0(59.6, 100) | 75.0(60.0, 87.5) | 0.575 | 75.0(60, 100) | 71.43(50.0, 83.3) | 0.190 |
| Cleavage rate, % | 100(100, 100) | 100(100, 100) | 0.147 | 100(100, 100) | 100(100, 100) | 0.069 | 100(100,100) | 100(100,100) | 0.665 |
| High quality embryo rate, % | 37.5(0, 60.0) | 33.33(1.11, 50.0) | 0.092 | 37.50(0, 60.0) | 33.33(10.4, 50.0) | 0.084 | 38.10(0, 66.7) | 33.33(11.1, 60.0) | 0.811 |
| Blastocyst formation rate, % | 70.1(50.0, 91.9) | 71.3(50.0, 92.3) | 0.156 | 71.0(50.0, 92.2) | 71.8(50.0, 93.0) | 0.124 | 70.0(50.0, 90.9) | 70.2(50.0, 91.7) | 0.255 |
Note: Data are presented as the median (25th and 75th percentile) or number (%). Mann–Whitney U statistics were used for continuous variables and chi-square tests were used for categorical variables. CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonists; OPU, oocyte pick-up; LH, luteinizing Hormone; E2, Estradiol; P, progesterone; Gn, gonadotropin; OHSS, ovarian hyperstimulation syndrome.
Table 3.
Pregnancy and cumulative outcome between CPOS group and GnRHa group after propensity score matching.
Table 3.
Pregnancy and cumulative outcome between CPOS group and GnRHa group after propensity score matching.
| Characteristic | CPOS Group | Gnrha Group | p Value | Subgroup Analysis | |||||
|---|---|---|---|---|---|---|---|---|---|
| CPOS <40yr | GnRHa <40yr | P Value | CPOS ≥40yr | GnRHa ≥40yr | P Value | ||||
| Patients, n | 375 | 375 | - | 296 | 298 | - | 79 | 77 | - |
| Cycle type of embryo transfer, n (%) | |||||||||
| Fresh embryo transfer | / | 217 | - | / | 174 | - | / | 43 | - |
| Frozen embryo transfer | 445 | 348 | - | 346 | 269 | - | 99 | 79 | - |
| Implantation rate in fresh embryo transfer, %(n) | / | 27.39(103/376) | - | / | 27.96(85/304) | - | / | 25.00(18/72) | - |
| Clinical pregnancy rate in fresh embryo transfer n (%) | / | 87(40.09) | - | / | 75(43.10) | - | / | 12(27.90) | - |
| Live birth rate in Fresh embryo transfer n (%) | 60(28.04) | - | / | 51(29.31) | - | / | 10(23.26) | - | |
| No. of patients underwent embryo transfer | 321 | 336 | - | 260 | 271 | - | 61 | 65 | - |
| Implantation rate per transfer, %(n) | 45.42(263/579) | 39.46(324/821) | 0.028 | 48.25(221/458) | 41.71(269/645) | 0.032 | 34.71(42/121) | 30.68(54/176) | 0.528 |
| Clinical pregnancy rate per transfer cycle, n (%) | 233/445(52.36) | 260/565(46.02) | 0.049 | 198/346(57.23) | 223/443(50.34) | 0.062 | 35/99(35.35) | 37/122(30.33) | 0.472 |
| Multiple birth rate per transfer cycle, n (%) | 40/233(17.17) | 44/260(16.92) | 1.000 | 38/198(19.19) | 38/223(17.04) | 0.612 | 2/35(5.71) | 6/37(16.22) | 0.262 |
| Miscarriage rate per transfer cycle, n (%) | 69/233(29.61) | 88/260(33.85) | 0.334 | 58/198(29.29) | 74/223(33.18) | 0.402 | 11/35(31.42) | 14/37(37.84) | 0.626 |
| Ectopic pregnancy rate per transfer cycle, n (%) | 1/233(0.43) | 2/260(0.77) | 1.000 | 1/198(0.51) | 2/223(0.90) | 1.000 | 0 | 0 | 1.000 |
| Cumulative biochemical pregnancy rate per initial cycle | 225(60.00) | 258(68.80) | 0.015 | 191(64.53) | 214(71.81) | 0.06 | 34(43.04) | 44(57.14) | 0.109 |
| Cumulative clinical pregnancy rate per initial cycle, n (%) | 194(51.73) | 226(60.27) | 0.023 | 167(56.42) | 194(65.10) | 0.036 | 27(34.18) | 32(41.56) | 0.41 |
| Miscarriage rates per initial cycle, n (%) | 39(20.10) | 54(23.89) | 0.409 | 33(19.76) | 45(23.20) | 0.445 | 6(22.22) | 9(28.13) | 0.766 |
| CLBR per initial cycle | 154(41.07) | 170(45.33) | 0.269 | 133(44.93) | 147(49.33) | 0.287 | 21(26.58) | 23(29.87) | 0.723 |
| Preterm birth rate, n(%) | 13(8.44) | 25(14.71) | 0.086 | 12(9.02) | 23(15.65) | 0.106 | 1(4.76) | 2(8.70) | 1.00 |
| Average birth weight | 3300(2973, 3550) | 3280(2650, 3600) | 0.143 | 3300(2950, 3550) | 3250(2750, 3600) | 0.427 | 3200(3000, 3500) | 3265(2563, 3550) | 0.448 |
| Average gestational age at birth | 38(38, 39) | 38(37, 39) | 0.005 | 38(38, 39) | 38(37, 39) | 0.052 | 38(38, 39) | 37.5(36, 39) | 0.351 |
| Congenital malformation rates | 0 | 0 | 1.000 | 0 | 0 | 1.000 | 0 | 0 | 1.000 |
| TTLB | 360(315.8, 445) | 326.5(257.5, 436) | <0.001 | 357(313, 445) | 325(257, 418) | 0.0002 | 361(322.5, 468) | 313(255, 389) | 0.012 |
Note: Data are presented as the median (25th and 75th percentile) or number (%). Mann–Whitney U statistics were used for continuous variables and chi-square tests were used for categorical variables. CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonists; CLBR, cumulative live birth rate; TTLB, time to first live birth.
Table 4.
Regression analysis of factors for prediction of a cumulative live birth from the fresh plus all frozen embryo transfer cycles.
Table 4.
Regression analysis of factors for prediction of a cumulative live birth from the fresh plus all frozen embryo transfer cycles.
| Factors to Predict a Cumulative Live Birth |
Coefficient(B) | S.E. | Wald(χ2) | P Value | Hazard Ratio (95% CI) |
|---|---|---|---|---|---|
| Age of women | -0.135 | 0.039 | 11.877 | 0.001 | 0.874(0.809-0.943) |
| Type of infertility | |||||
| primary infertility | 1 | ||||
| secondary infertility | -0.052 | 0.198 | 0.069 | 0.794 | 0.949(0.644-1.400) |
| Infertility duration | 0.000 | 0.022 | 0.000 | 0.988 | 1.000(0.958-1.043) |
| Cycle number | |||||
| The first cycle | 1 | ||||
| The second cycle | 0.084 | 0.200 | 0.175 | 0.676 | 1.087(0.734-1.610) |
| Treatment protocol | |||||
| GnRHa | 1 | ||||
| CPOS | 0.388 | 0.201 | 3.725 | 0.084 | 1.475(0.994-2.187) |
| Body mass index | 0.000 | 0.000 | 0.160 | 0.689 | 1.000(1.00-1.00) |
| Basal FSH | 0.026 | 0.035 | 0.545 | 0.461 | 1.026(0.958-1.098) |
| AMH | 0.116 | 0.041 | 18.77 | <0.001 | 1.112(1.017-1.431) |
| Total Gn dosage | 0.000 | 0.000 | 0.570 | 0.450 | 1.000(1.00-1.00) |
| Days of stimulation | -0.106 | 0.073 | 2.102 | 0.147 | .900(0.780-1.038 |
| No. of oocytes retrieved | 0.023 | 0.020 | 1.378 | 0.240 | 1.023(0.985-1.063) |
| No. of available embryos | 0.352 | 0.050 | 50.517 | <0.001 | 1.422(1.290-1.567) |
| Cause of infertility | |||||
| Tubal | 1 | ||||
| Male factor | 0.439 | 0.307 | 2.043 | 0.153 | 1.551(0.850-2.830) |
| Anovulatory | -0.460 | 0.456 | 1.017 | 0.313 | 0.631(0.258-1.543) |
| Unexplained | 0.087 | 0.210 | 0.173 | 0.678 | 1.091(0.723-1.657) |
| Diminished ovarian reserve | 0.055 | 0.308 | 0.032 | 0.857 | 1.057(0.578-1.933) |
| Endometriosis | 0.371 | 0.420 | 0.782 | 0.376 | 1.449(0.637-3.298) |
| Mixed | 0.689 | 0.741 | 0.865 | 0.352 | 1.991(0.466-8.506) |
Note: CPOS, clomiphene-primed ovarian stimulation; GnRHa, Gonadotropin-releasing hormone agonists; FSH, follicle-stimulating hormone; AMH, anti-Müllerian hormone; Gn, gonadotropin; CI, confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



