
Submitted:
06 November 2023
Posted:
07 November 2023
You are already at the latest version
Abstract
Background and purpose: Chronic kidney disease (CKD) is a common chronic disease usually associated with cardiovascular disease (CVD), and premature death and millions of people are at increased risk for CKD. As this disease is extremely complex, multidisciplinary care (MDC) is needed to provide complete and continuous care. Usually, the nephrology units need coopera-tion from several other Healthcare Professionals (HCPs) such as cardiologists, nutritionists, ob-stetricians, and so forth. All modalities of treatments, peritoneal dialysis (PD) and Hemodialysis (HD) require HCPs and patients to develop a variety of skills to effectively deliver and manage dialysis tasks in the center or at home. Information and Communication Technology (ICT) in-terventions can offer tools that provide HCPs and patients with tools that facilitate the manage-ment of kidney patients in centers or at home. ICT interventions can allow to automate registra-tions, videoconferencing, minimize the geographic burden and resource cost savings. ICT can be the best way to promote cost saving on health spending and ensure the sustainability of the health system and, the environment as well. In the Iberian Peninsula, kidney patients consume about 3% of the total cost of healthcare. The cost of kidney transplants and dialysis is around 1.8 billion euros annually, and 75 % of this amount goes to dialysis treatment. Objective: This study aimed to evaluate and analyze the opinion of Healthcare Professionals (HCP) in Nephrology units about the Intervention of ICT in nephrology care and the Clinical benefits results from the use of ICT in Nephrology Services and dialysis Units in Portugal and Spain. Thus we collected the opinion of Health care professionals concerning the role of ICT intervention in nephrology. Understanding HCPs' feelings and attitudes is essential to understand if such technologies are correctly adjusted to the workflow and really bring huge benefits for the clinical practice of nephrology and also what features need improvement and what should be implemented in the future. ICT intervention has been implemented to promote better healthcare in nephrology units and improve patient outcomes. In the Survey, we intended to evaluate nephrology HCPs' opinions concerning the ICT interventions, in nephrology, represented by several tools that al-low the HCPs to implement solutions such as Remote Patient Monitoring(RPM); Remote Moni-toring of Treatment (RMT); Tele homecare; Telehealth (Tele-nephrology); Home Dialysis; mHealth; mobile App; Web Portal, Telemedicine, and so forth. Key Points: In many countries particularly in the Iberian Peninsula (Portugal and Spain) the incidence of CKD is substantially high. The “treatments” for kidney disease have not improved substantially over the past 50 years, leaving too many kidney patients with a poor quality of life and reduced life expectancy. This situation is associated with staggering aggregate annual costs amounting to €140 billion per year in Europe, more than the annual healthcare costs of cancer or diabetes [1]. The increased daily use of information and communication technologies may lead to the need for healthcare professionals to incorporate technology use competencies into practice.
Keywords:
Information and Communication Technology (ICT)
; Nephrology in Iberian Peninsula
; Chronic Kidney Disease (CKD)
; Renal Replacement Therapy (RRT)
; Healthcare Professional (HCP)
Introduction
CKD is defined as persistent “abnormalities of kidney structure or function, present for 3 months, with health implications”, and classified based on cause, glomerular filtration rate (GFR<60mL/min/1.72m2 [G1-G5]) category, albuminuria category (CGA>= 30mg per 24 hours [A1-A3]), age and in some cases the ethnicity. This results in the inability of the kidneys to filter the blood, resulting in an excessive build-up of fluid and waste products (e.g. drugs or their metabolites). CKD affects 8% to 26% of the population worldwide [2,13].
Nowadays improvements in assisting chronic disease patients, there is a wide possibility of using ICT in nephrology for training, assisting, or monitoring CKD patients. Due to those features, nephrology practice is experiencing improvements in safety quality of care, and quality of life for patients and HCPs as well.
This disease behaves like a multi-organ disease with complications that affect different organ systems and ICT can work as an excellent support in the activities of healthcare professionals of nephrology interchanging information with other healthcare professionals.
Information and communication technologies have the potential to improve health care for patients with chronic diseases [3].
More than 55 million people in the European Union (EU) are affected by CKD. In 2016, 64 387 people died from kidney diseases and this caused almost 130,000 deaths in 2019. A vast majority of deaths from kidney disease concern people 65 years old or above. In the EU the death rate from kidney diseases is highest in Croatia (23 deaths per 100 000 inhabitants) and lowest in Finland (4 deaths per 100 000 inhabitants). The average standardized rate for the EU as a whole is approximately 14 deaths from kidney disease per 10,000 inhabitants. In 2016 Spain recorded about 14 deaths from Kidney diseases per 100 000inhabitants and Portugal registered about 16 deaths per 100 000 inhabitants [4].
In Portugal and Spain, the prevalence and incidence of patients under Renal Replacement Therapy (RRT) are high due to the high prevalence of patients with Diabetes, High Blood Pressure (HBP), and Obesity.
The use of information and communication technology in nephrology will be efficient only when the tools are correctly adjusted and integrated into the workflow processes and the users are trained.
CKD affects 9.1% of the global population and is spread heterogeneously throughout the world (10-13% in Europe). All indications are that the incidence is higher in the elderly population and considering the aging trend of the European population, it is easy to understand that the number of patients will tend to grow, boosted by the increase in survival/longevity. The prevalence in stages 1 and 2 are about 50% and over time there have been no variations in age-adjusted prevalence this means that the increase is due to the aging of the world population and everything indicates that the numbers will continue to increase with the aging of the population.
According to the available data, in 2019, in Portugal 2673 patients started Renal Replacement Therapy. Portugal registered 378 kidney transplant transplants in 2020 and more than 1950 were on the waiting list [5]. According to the Spanish Society of Nephrology, the number of patients in Renal Replacement Therapy is 3363, corresponding to 1922 patients on hemodialysis in health centers, 1334 to renal transplant recipients, 91 to peritoneal dialysis, and 16 to home hemodialysis [6].
The April 2021 publication shows that the survival trend is lower than in many cancer cases [7,8].
Overall in Europe, we are 10% of the population with CKD, amounting to >800 million individuals [8]. In Portugal, the adult population is about 9 million, and 10% of this population (90 thousand) have DRC [9].
In Spain, there are also 10% of the population with CKD, representing about 1300 Nephrologists for 3,7 million patients with CKD [10].
The incidence of CKD in Europe is 128 cases per million inhabitants, in Spain it is a lithe higher, 170 cases per million inhabitants, and in Portugal is higher than in Spain, 229 cases per million inhabitants [11].
Thus CKD places a considerable burden on healthcare systems and government budgets. Indeed, annually there were millions of deaths in the EU resulting from CKD disease that used to be related to high blood pressure.
The persistent effect of high blood pressure in arteries may lead to the chronic failure of vital organs such as the heart, kidneys, or brain. In 2019, 22% of people in the EU aged 15 years and over reported having high blood pressure. Concerning the Iberian Peninsula, high blood pressure in Portugal affects around 27.5%, and in Spain 20% of inhabitants with 15 years old or above.
DIGITAL HEALTH that is the Information and Communication Technology intervention in medicine is spreading new tools to manage and support the clinical practice in distinct areas of medicine including nephrology, enhancing the possibility of including Tele-nephrology, Home Dialysis, RPM, RTM, and commercially available medical devices or technologies, such as mobile phone-enabled self-monitoring of biometrics data. Many of these new digital or ICT tools impact positively the patient-physician relationship. To ensure and speed up the widespread of ICT intervention in nephrology, it's crucial to know the feelings and perceptions of healthcare professionals about these technologies, and that is why we consider this study to be very useful for nephrology in the Iberian Peninsula.
Accordingly, we surveyed the nephrology HCPs, through the Portuguese and Spanish nephrology associations, societies, and units of nephrology to better know their needs and the professional perceptions of patients and their comfort level towards ICT interventions.
Materials and Methods
Research Design and Data Collection Procedures
The questionnaire was pre-tested, in Azores Island Hospital where the RRT Platform was put in place recently, to verify the appropriateness of the questionnaire content. Content validity was ensured through an extensive literature review of academic and practical journals, as well as discussions with experts in this domain. Since ICT intervention is in its initial stage in several Units of Nephrology, numerous Societies and Units of Nephrology and Units of Dialysis were contacted to try to reach as many nephrology HCPs as possible, which could enhance the effectiveness and scope of the Survey.
We have contacted the Information and communication departments of the Hospitals of the main islands of the Azores (Ponta Delgada, Faial, and Ilha Terceira) and asked them to spread the questionnaire by the HCPs. The feedback was enough to guide the second and definitive survey.
We created a definitive survey focusing on the 15 main subfields highlighted by the respondents of the pre-tested questionnaire. The definitive survey was distributed to the Spanish Society of Nephrology (SEN), Portuguese Society of Nephrology (SPN), Renal nurses associations, nephrologists associations, and nephrology and Dialysis Centers located in the Iberian Peninsula (Portugal and Spain). We ask those institutions to distribute the Survey to their nephrology HCPs.
To avoid the need for informed consent for ethical approval and accomplishment with personal data protection, we insert informed consent as the first, mandatory, and required answer to proceed with the other questions of the survey. In addition, the only personal data that were requested are the genre, the range of age, and profession.
A web-based (Google Forms) survey was completed by nephrologists and renal nurses working in the Spanish and Portuguese institutions of Nephrology.
A detailed description of the survey objective was provided in the survey introduction. A total of 20 valid samples were retrieved, with females accounting for 55% of the respondents. Most of the respondents are in the 40–49 age group (60%), followed by the 26–39 age group (30%); 75% of the respondents have more than 3 years using computer to manage renal patients; the time working in Nephrology Units is 16-20 years group (30%), followed by 10-15 years group (25%) (see Table 1).
The Questionnaire
At the beginning, we explained the objective of the questionnaire and asked for consent. Only the user that answers “Yes” forms for the first question can proceed with other questions of the survey. The first sentence was: “Please complete this ANONYMOUS survey, as your opinion is very important to us. Thank you, in advance, for taking the time to complete our survey”.
This study accomplishes all principles of good ethical research and does not use participants/respondents' data. Therefore this study does not require official approval from the ethics committee. Furthermore, the study is completely anonymous.
Firstly, respondents were asked for the genre, range of age, and profession, how long he/she has been working in nephrology, and how long she or he been using ICT tools in nephrology.
Secondly, respondents were asked about the RRT modality that he/he use to manage, the geographic area where he/she works, rural or Urban, whether they use daily any kind of ICT tools to manage renal patients and some details and a deep opinion about the strengths and weakness that he found in ICT tools that he knows or uses daily. The respondents were asked about the advantages and disadvantages that they found in ICT intervention.
The ten topics of the questionnaire used in this study are shown in Table 2.
The measurement was clearly defined in each question. The entire questionnaire can be accessed through the links:
English Version:
Portuguese Version:
Spanish Version:
Results
Between July 2021 and July 2023, the questionnaire was available online, and 20 answers were obtained (10 from Portugal and 10 from Spain). Of those replying to the survey, 80% were from public Hospital centers and 20% were from private centers.
In Portugal, 100% of respondents had HD patients, 60% had PD patients, 30% had patients in conservative integral treatment, 0% had patients in HHD and 10% had kidney transplanted patients.
100% of respondents from Spain had HD patients, 40% had PD patients, 20% had patients in conservative integral treatment, 10% had patients in HHD and 10% had kidney transplanted patients.
A high percentage of the respondents had HD patients in both countries. From Portugal, we had a higher percentage of respondents with PD patients (60% vs 40%). Any respondent from Portugal had patients in HHD but for kidney transplant we got the same number of respondents as Spain (10%).
Concerning using some ICT tools to manage Kidney patients, 80 % of Portuguese respondents said yes, and we got 90% yes from Spanish respondents. 77.8% of respondents from Spain have been using ICT to manage Kidney patients for more than 3 years, while in Portugal we found only 37.5% of respondents in this situation.
When questioned about the reasons for not using ICT tools to manage kidney patients, the answers were: from Portuguese respondents, lack of awareness of decision-makers (10%), lack of resources (10%), and tools unavailable (10%). Spanish respondents point to unawareness of the benefits (10%) and lack of resources (10%).
Referring to ICT available in the market, 40% of respondents from Spain declared that they were using Versia from Baxter, 10% were using Therapy Monitor from Fresenius, 10% were using Nexadia®, and the remaining 40% were using other solutions, instance: Nefrosoft and Irinis/Tgs (Diaverum). In Portugal 60% were using Therapy Monitor from Fresenius, 20% were using Versia from Baxter, and the remaining 20% declared that they were any ICT tool available.
Asking about RRT available in the workplace, 100% of the Portuguese respondents declared that HD (in the center) was available, 80% were PD available, 20% were self-care available, and 40% were comprehensive conservative management. 100% of Spanish respondents were HD available, 10% were HHD available, 40% were PD available, 30% were self-care available and 30% were comprehensive conservative management.
When asked about benefits received from ICT intervention, Spanish respondents refer to the Great efficiency of practices, taking into account the scarcity of human resources ( 20%), Facilitating the creation, management, updating, and use of clinical information (10%); allow RPM (10%); allow to create reports and data analysis (10%); enhancing the patient autonomy and self-care (10%); Improve workflow and time-saving. The Portuguese respondents highlighted the ability to create and manage clinical information (100%); Allow automatic registration and reduce human error (90%); Enhance data access ( 80%); Show information about the patient status (70%); time-saving, paper-free, effective integrated care (60%).
When asked to summarize the role that ICT intervention can play in RRT, 70% of Spanish respondents mentioned patient safety; 60 % mentioned personalized treatment; 50 % mentioned productivity, paper-free, information-integrated, and reduced human error. The Portuguese respondents highlighted Patient safety (30%); Total focus on the patient (20%); and 10% refer tTo, Information integration, treatment adherence observation, improvement of quality of care, agility and practicality for procedures, flexibility, and easy access to patient history.
From Portugal 40% of respondents were more than 5 years working without ICT intervention, 30% were more than a year, 20% were more than 20 years and 10% were between 1 and 5 years. 50% of Spanish respondents were between 1 and 5 years working without ICT interventions, 30% spent more than 5 years working without ICT intervention,10 & spent more than 20 years working without ICT intervention and 10 % spent less than 1 year working without ICT interventions the remains 10 % were more than 20 years working without ICT intervention.
The respondents were using ICT intervention daily (80%) in Portugal and (70%) in Spain.
80% of Spanish respondents considered the ICT intervention as an excellent tool for BLERRT and the remaining 20% classified it as a good tool. 40% of Portuguese respondents considered it excellent, 40 % considered it good, 10% considered it neutral and 10% did not know.
Table 3 shows the comparative results by profession and country.
Figure 1, below, shows the results on the barriers that impede the use of ICT in Renal Replacement Therapy (RRT) in % (provided by the Portuguese nephrology HCP).
In Figure 2, below, we have the results (in %) given by the Spanish nephrologist HCPs on the barriers that impede the Use of ICT in Renal Replacement Therapy (RRT).
In Figure 3, below, we have the results in % of the answers given by the Portuguese HCPs on the barriers that prevent Nephrology units from providing Home Dialysis.
In Figure 4, below,we have the results regarding the barriers that prevent Nephrology units from providing Home Dialysis in % (answers given by the Spanish nephrology HCP).
In Figure 5, below, we have the results regarding the barriers that would prevent Nephrology units from expanding Home Dialysis in % (answers given by Portuguese HCP).
Figure 6, below, shows the results regarding the barriers that would prevent Nephrology units from expanding Home Dialysis - HD and PD in % (answers given by Spanish HCPs).
In Figure 7, below, we have the results regarding the Nephrology HCP's opinion on the potential value of the Platform or Software to manage Renal Replacement Therapy (RRT) (answers given by Portuguese HCP).
Figure 8, below, represents the results in % of the answers given by the Spanish HCPs on the opinion of the Nephrology HCPs on the potential value of the Platform or Software to manage Renal Replacement Therapy (RRT).
Figure 9, below, corresponds to the results on the attitude of the Nephrology HCP towards the Platform or Software for the management of Renal Replacement Therapy (RRT).
The results of the answers given by the Spanish HCP (in %) regarding the attitude of the Nephrology HCP towards the Platform or Software for the management of Renal Replacement Therapy are represented in Figure 10.
Relevant Comments from the Respondents
Bellow, (Table 4) we transcript questions and respective additional comments from survey respondents when we gave them space for comments about the previous question.
When compared the traditional process with the ICT intervention in RRT, the opinion of Iberian Peninsula nephology HCPs (Portuguese and Spanish) is consensual: Almost the total respondents agree that ICT intervention brings the following benefits to nephrology care:
- ▪
- Improves the quality of RRT service
- ▪
- Improves the quality of care
- ▪
- HCPs feel comfortable using ICT tools for RRT
- ▪
- Have positive effects on the patients
- ▪
- Financial barriers and practical and logistic aspect is the main burden for the spread of ICT in RRT
- ▪
- Financial barriers, Knowledge, or attitude of nephrology HCPs is another burden for the spread of ICT in nephrology
- ▪
- Knowledge or attitude of nephrology HCP is the main burden for the impulse of Dialysis at home
- ▪
- HCP's attitude towards ICT in RRT is very positive
- ▪
- Promote Better patient management
- ▪
- Reducing the risk of complications
- ▪
- Optimize the use of resources
- ▪
- It is excellent for RRT
Therefore the above list of benefits, a high percentage of Portuguese nephrology HCPs also mentions the following benefits:
- ▪
- Improve patient safety
- ▪
- Personalize treatment
- ▪
- Put total focus on the patient
- ▪
- Promote integration and mobility of information
- ▪
- Promote cost saving
- ▪
- Reduce Human error
Discussion
This study was performed to collect the opinion of Health care professionals concerning the role of ICT intervention in nephrology. Understanding HCPs' feelings and attitudes is essential to understand if such technologies are correctly adjusted to the workflow and really bring huge benefits for the clinical practice of nephrology and also what features need improvement and what should be implemented in the future.
Both surveys implemented collected the feeling of HCP professional about the roles of ICT intervention in Nephrology care. The first one found the HCPs jumping form the traditional procedures to the lead with the ICT interventions. The first survey gave good references to conduct the second and definitive that was made available for al dialysis units and societies of nephrology of Portugal and Spain.
Meanwhile, the survey model showed a good fit with our proposal and looks very good to guide future research to the primary care HCPs that lead to patients at risk of CKD. The results showed that ICT could also address the burdens of kidney disease spending, facilitating the implementation of multidisciplinary work, as demanded by multifactorial diseases such as CKD. The very demanded establishment of active cooperation between distinct departments of medical care can be enhanced by ICT interventions, and address the major problem caused. The survey results were analyzed using the core outcomes recommended by the Standardized Outcomes in Nephrology. There were no answers reported adverse effects of ICT interventions, only positive or null effects. Despite the high interest in ICT interventions in Nephrology, good quality evidence over a wider amount of HCPs and patients is needed to explore their real effectiveness and search for a better focus for exploring the Potentialities of ICT intervention for CKD prevention through improving kidney disease screening.
The results indicated that the nephrology HCPs have a very good attitude towards the ICT interventions, they agree that the ICT tools bring better management of kidney patients and improve several aspects that impact the quality of service in nephrology.
CKD is extremely common and has emerged as one of the leading causes of death worldwide. CKD affects populations in different regions of the world unequally, likely as a result of differences in population demographic characteristics, comorbidities, and access to healthcare resources. The common nature and devastating effects of CKD should prompt major efforts to develop and implement effective preventative and therapeutic efforts aimed at lowering the development of CKD and slowing its progression.
The ICT can bring a better integrated approach to improve CKD patient management. A good integrated approach in dialysis will impact enormously inpatient life, healthcare services, and global climate change considering the environmental cost resulting from dialysis treatment.
According to the results, the nurses look to be more interested in ICT intervention in Nephrology, which can explain why globally nurse corresponds to 80% of respondents. In our point of view this is very important because, in nephrology care, the nurse is who spends more time with the patient. They treat and care for patients throughout their lifespan from infancy or, in this case, from the beginning of renal problems to the end of life. The role of nephrologists, in addition to consultations, is to prescribe treatments. The execution, which is the phase where there is usually the greatest intervention of the ICTs, is in charge of the nurses.
Conclusions Including Relevant Outcomes and Findings
From the results of the survey, we can conclude that the ICT intervention is a good tool for managing kidney patients through clinical management systems since it allows the continuity of care of the entire disease process in a single integrative platform, which entails a global vision of the patient.
However, we also conclude that the best way to manage kidney disease is by acting on early detection and prevention. The bioengineer and researcher in this field must focus on the development of ICT tools that act at the level of primary care to reduce the incidence of CKD.
We believe that future research should consist of a survey of primary care to better understand how ICT tools can support them in improving the screening of patients at risk of kidney disease and enhance and
Improve communication between primary care and nephrology services. The main goal should be to detect patients in the early stages of kidney disease and delay or even prevent CKD.
Outcome and Findings
The survey confirms that HCP is satisfied with ICT intervention in nephrology because it brings several benefits listed below:
Improves patients' quality of life, allows real-time data visualization or online communication, alleviates the geographic burden and associated cost for travel, Improves outcomes, permits the adjustment of prescription more easily and frequently, enhances patient self-management of the disease at home, diagnosis of infections by pictures or video consultation, improving Adherence, improve outcomes and treatment satisfaction, can improve the management of supplies, improve patient education, improve patient and disease management, bring time-saving benefits, permit transmission of patients data from several sources on-time, check patients data, from everywhere, in a glance, more proactive nurse care, optimize resources, very good acceptance of the nephology staff. Can also, increase the coverage area of nephrologists, and increase patient safety.
This study survey also ratified benefits that were already found by other researchers, for instance:
- ➢
- Ability to rapidly change prescription and diagnosis problems in response to data that is monitored previously.
- ➢
- Demonstrates the utility of telemedicine platforms to exchange data between patients and providers and that this data exchange can improve outcomes such as blood pressure control.
- ➢
- A more long-term goal of this system would be to allow patients to remain at home without the need for routine face-to-face visits.
- ➢
- Patients find the system useful and obtain an increased sense of security and connectivity through the use of the application.
- ➢
- Researchers such as Nayak et al. developed and tested a phone-based system and demonstrated that it was useful in caring for PD patients with excellent results in patients in very remote locations.
- ➢
- Investigators have also applied remote monitoring to PD with encouraging but limited results.
- ➢
- The researchers were able to demonstrate that the study group had fewer hospitalizations, hospital days, emergency room visits, and associated healthcare expenditures.
Future research should be focused on developing ICT tools to act in the prevention of Kidney disease. This is under-exploited because this idea is not interesting for the few big companies that develop and provide devices, monitors, and fungibles for dialysis. Some company also provides ICT tools to manage For instance, Versia and Sharesource from Baxter, Therapy Monitor from Fresenius, and so forth.
A study survey of primary care HCPs about Kidney disease should be done as soon as possible.
Author Contributions
Conceptualization, A.M.L. and A.R.P.; methodology, A.M.L.; software, A.M.L.; validation, J.J.S.O., A.M.L. and A.R.P.; formal analysis, A.R.P.; investigation, A.M.L.; resources, X.X.; data curation, A.M.L.; writing—original draft preparation, A.M.L.; writing—review and editing, A.R.P.; visualization, A.M.L.; supervision, J.J.S.O.; project administration, A.M.L.; funding acquisition, J.J.S.O.. All authors have read and agreed to the published version of the manuscript.
Funding
The authors did not receive financial support for the research, authorship, and /or publication of this article.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Consent was asked of all participants before starting to answer the questionnaire.
Acknowledgments
The authors thank especially the Portuguese and Spanish societies and associations of nephrology, Nephrology Nurse Associations, Nephrologist associations, and public and private Units of Nephrology that kindly offer to distribute the survey through Nephrology Healthcare professionals. We warmly thank those HCPs who kindly the time to answer the Questionnaires, Margarida Nieves from the information and technology communication department of the Hospital of Horta who supported motivating the HCP, and Nieves Linares for assisting in searching the Nephrology Units in Portugal and Spain and with language review.
Conflicts of Interest
The authors declare no conflict of interest.
Conflicts of Interest Statement/Disclosure Statement
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
ICT: Information and Communication Technology; CKD: Chronic kidney disease; DKD: Diabetic kidney disease; GFR: Glomerular Filtration Rate; ESRD: End-Stage Renal Disease; KDIGO: Kidney Disease: Improving Global Outcomes; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT: Randomized Controlled Trial; RRT: Renal replacement therapy; RPM: Remote Patient Monitoring; PD: Peritoneal Dialysis; HD: Hemodialysis or Hemodialysis; APD: Automatic Peritoneal Dialysis; CAPD: Continuous Ambulatory Peritoneal Dialysis; HHD: Home Hemodialysis; RRT: Renal Replacement Therapy; TX: Transplantation; RMT:Renal Management Therapy; RTS: Renal Therapy Services; EKHA: European Kidney Health Alliance; ICHD: In-Center Hemodialysis; HCP: Healthcare Professional, EU: European Union; ICHD: In-Center Hemodialysis; THC: Tele homecare; PGHD: Patient-Generated Health Data; AAKP: American Association of Kidney Patients (AAKP); PAHO: Pan American Health Organization; WHO: World Health Organization.
Appendix
The Questionnaires are available online at the links below:
Links to access the Surveys
English Version:
For HCP from Spain:
For HCP from Portugal: https://docs.google.com/forms/d/1LM2gkC6N0o0Hzmi4bVdO76MEKobUWR6WDQTgrFVQkpo/edit
References
- Cao H. Medication in Chronic Kidney Disease. In: Yang J, He W (eds). Chronic Kidney Disease: Diagnosis and Treatment. Singapore: Springer Singapore; 2020. p. 187–198.
- Chen, T. K., Knicely, D. H., & Grams, M. E. (2019). Chronic Kidney Disease Diagnosis and Management. JAMA, 322(13), 1294. [CrossRef]
- Hamine, S, Gerth-Guyette, E, Faulx, D, et al. Impact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic review. J Med Internet Res 2015; 17(2): e52.
- Eurostat- An official website of the European Union https://ec.europa.eu/eurostat/web/products-eurostat-news/ [accessed on September 15, 2023].
- sociedade portuguesa de nefrología. www.spnefro.pt: [ accessed in August 10, 2023].
- Sánchez-Álvarez E, et al. Posicionamiento de la Sociedad Espanola ˜ de Nefrología ante la vacunación frente al SARSCoV-2. Nefrologia. 2021. [CrossRef]
- Raymond Vanholder;Lieven Annemans;Aminu K Bello;Boris Bikbov;Daniel Gallego;Ron T Gansevoort;Norbert Lameire;Valerie A Luyckx;Edita Noruisiene;Tom Oostrom;Christoph Wanner;Fokko Wieringa; (2021). Fighting the unbearable lightness of neglecting kidney health: the decade of the kidney. Clinical Kidney Journal, (), –. [CrossRef]
- Kovesdy, 2022Csaba P Kovesdy, Epidemiology of chronic kidney disease: an update 2022, Kidney Int Suppl (2011). 2022 Apr;12(1):7-11. [CrossRef]
- Santos-Araújo C. Twenty years of real-world data to estimate chronic kidney disease prevalence and staying in an unselected population. Clin Kidney J. 2022 Sep12; 16 (1): 111-124].
- Patricia Barber Pérez, Beatriz González López-Valcárcel, Informe Oferta-Necesidad de Especialistas Médicos 2021-2035: EcoSalud. Universidad de Las Palmas de Gran Canaria. [https://www.sanidad.gob.es/areas/profesionesSanitarias/profesiones/necesidadEspecialistas/docs/20182030]. [CrossRef]
- (Megan E Astley et al., The ERA Registry Annual Report 2020: a summary, Clinical Kidney Journal, 2023).
- KDIGO 2023 CLINICAL PRACTICE GUIDELINE FOR THE EVALUATION AND MANAGEMENT OF CHRONIC KIDNEY DISEASE https://kdigo.org/wp-content/uploads/2017/02/KIDIGO-2023 [accessed on September 15, 2023].
- Masood Ahmad, Eric L. Wallace, Gaurav Jain: Setting Up and Expanding a Home Dialysis Program: Is There a Recipe for Success?, Kidney360. 2020 Jun 25; 1(6): 569–579. Published online 2020 May 1. [CrossRef]
- Duvuru Geetha, Andreas Kronbichler, Megan Rutter, Divya Bajpai, Steven Menez, Annemarie Weissenbacher, et al.: Impact of the COVID-19 pandemic on the kidney community: lessons learned and future directions, Nat Rev Nephrol. 2022; 18(11): 724–737. Published online 2022 Aug 24. [CrossRef]
- Mario Cozzolino, Ferruccio Conte, Fulvia Zappulo, Paola Ciceri, Andrea Galassi, Irene Capelli, et al.: COVID-19 pandemic era: is it time to promote home dialysis and peritoneal dialysis?, Clin Kidney J. 2021 Mar; 14(Suppl 1): i6–i13. Published online 2021 Feb 2. [CrossRef]
- Arora P, Vasa P, Brenner D, Iglar K, McFarlane P, Morrison H, et al. Prevalence estimates of chronic kidney disease in Canada: results of a nationally representative survey. Can Med Assoc J. 2013;185:E417–23.
- Berns J. Patient education: Chronic kidney disease (Beyond the Basics). In: UpToDate, Curhan GC and Motwani S (Ed), UpToDate, Waltham, MA. Accessed 4 May 2021.
- Philip Kam-Tao Li, Wanhong Lu, Siu-Ka Mak, Neil Boudville, Xueqing Yu, Ming Ju Wu, et al.: Peritoneal dialysis first policy in Hong Kong for 35 years: Global impact, Nephrology (Carlton) 2022 Oct; 27(10): 787–794. Published online 2022 Apr 13. [CrossRef]
- Susie Q. Lew, Eric L. Wallace, Vesh Srivatana, Bradley A. Warady, Suzanne Watnick, Jayson Hood, et al.: Telehealth for Home Dialysis in COVID-19 and Beyond: A Perspective From the American Society of Nephrology COVID-19 Home Dialysis Subcommittee, Am J Kidney Dis. 2021 Jan; 77(1): 142–148. Published online 2020 Sep 28. [CrossRef]
- Na Liu, Jinman Kim, Younhyun Jung, Adani Arisy, Mary Ann Nicdao, Mary Mikaheal, Tanya Baldacchino, et al.: Remote Monitoring Systems for Chronic Patients on Home Hemodialysis: Field Test of a Copresence-Enhanced Design, JMIR Hum Factors. 2017 Jul-Sep; 4(3): e21. Published online 2017 Aug 29. [CrossRef]
- Benjamin Talbot, Sara Farnbach, Allison Tong, Steve Chadban, Shaundeep Sen, Vincent Garvey, et al.: Patient and Clinician Perspectives on the use of Remote Patient Monitoring in Peritoneal Dialysis, Can J Kidney Health Dis. 2022; 9: 20543581221084499. Published online 2022 Mar. [CrossRef]
- Nayak, K. S.; Ronco, C.; Karopadi, A. N.; Rosner, M. H. (2016). Telemedicine and Remote Monitoring: Supporting the Patient on Peritoneal Dialysis. Peritoneal Dialysis International, 36(4), 362–366. [CrossRef]
- National Kidney Foundation: kidney.org; 2023. [accessed on September 22, 2023].
- Ekha-European Kidney Health Alliance: htts://ekha.eu; 2023. [accessed on May 22, 2023].
- European Parliament: https://www.europarl.europa.eu/: 2023. [accessed on September 12, 2023].
- Rachael C Walker, Kirsten Howard, Rachael L Morton: Home hemodialysis: a comprehensive review of patient-centered and economic considerations, Clinicoecon Outcomes Res. 2017; 9: 149–161. Published online 2017 Feb 16. [CrossRef]
- Pilotto A, D’Onofrio G, Benelli E, et al. Information and communication technology systems to improve quality of life and safety of Alzheimer’s disease patients: a multicenter international survey. J Alzheimers Dis. 2011;23(1):131–141.
- World Health Organization. eHealth, https://www.who.int/ehealth/en/ (accessed 1 February 2019).
- Agar J, Hawley C, Kerr G. Home hemodialysis in Australia and New Zealand: how and why it has been successful. Semin Dial 2011;24:658-63.
- Matteson, M. L. & Russel, C. (2010). Interventions to improve hemodialysis adherence: A systematic review of randomized controlled trials. Hemodialysis International, 14, 370–382.
- Skiadas M, Agroyiannis B, Carson E, et al. Design, implementation, and preliminary evaluation of a telemedicine system for home hemodialysis. J Telemed Telecare. 2002; 8: 157– 64.
- Urbina O, Ferrández O, Grau S, Luque S, Mojal S, Marin-Casino M, et al. Design of a score to identify hospitalized patients at.
- Chen, J. H., Chiu, Y. W., Hwang, S. J., Tsai, J. C., Shi, H. Y., & Lin, M. Y. (2019). Effect of nephrology referrals and multidisciplinary care programs on renal replacement and medical costs on patients with advanced chronic kidney disease: A retrospective cohort study. Medicine (Baltimore), 98(33), e16808. [CrossRef]
- Chen, P. M., Lai, T. S., Chen, P. Y., Lai, C. F., Yang, S. Y., Wu, V. C., … Tsai, T. J. (2015). Multidisciplinary care program for advanced chronic kidney disease: Reduces renal replacement and medical costs. The American Journal of Medicine, 128(1), 68–76. [CrossRef]
- Chen, Y. R., Yang, Y., Wang, S. C., Chou, W. Y., Chiu, P. F., Lin, C. Y., … Lin, C. L. (2014). Multidisciplinary care improves clinical outcomes and reduces medical costs for pre-end-stage renal disease in Taiwan. Nephrology (Carlton), 19(11), 699–707. [CrossRef]
- Chiou, C. P., Lu, Y. C., & Hung, S. Y. (2016). Self-management in patients with chronic kidney disease. The Journal of Nursing, 63(2), 5–11. [CrossRef]
- Collister, D., Rigatto, C., Hildebrand, A., Mulchey, K., Plamondon, J., Sood, M. M., … Komenda, P. (2010). Creating a model for improved chronic kidney disease care: Designing parameters in quality, efficiency, and accountability. Nephrology Dialysis Transplantation, 25(11), 3623– 3630. [CrossRef]
- Fishbane, S., Agoritsas, S., Bellucci, A., Halinski, C., Shah, H. H., Sakhiya, V., & Balsam, L. (2017). Augmented nurse care management in CKD stages 4 to 5: A randomized trial. American Journal of Kidney Disease, 70(4), 498–505. [CrossRef]
- Fluck, R. J., & Taal, M. W. (2018). What is the value of multidisciplinary care for chronic kidney disease? PLoS Med, 15(3), e1002533. [CrossRef]
- Helou, N., Talhouedec, D., Shaha, M., & Zanchi, A. (2016). The impact of a multidisciplinary self-care management program on quality of life, self-care, adherence to anti-hypertensive therapy, glycemic control, and renal function in diabetic kidney disease: A cross-over study protocol. BMC Nephrology, 17(1), 88. [CrossRef]
- Johns, T. S., Yee, J., Smith-Jules, T., Campbell, R. C., & Bauer, C. (2015). Interdisciplinary care clinics in chronic kidney disease. BMC Nephrology, 16, 161. [CrossRef]
- McCrory, G., Patton, D., Moore, Z., O’Connor, T., & Nugent, L. (2018). The impact of advanced nurse practitioners on patient outcomes in chronic kidney disease: A systematic review. Journal of Renal Care, 44(4), 197–209. https://doi. org/10.1111/jorc.12245.
- Wouters, O. J., O’Donoghue, D. J., Ritchie, J., Kanavos, P. G., & Narva, A. S. (2015). Early chronic kidney disease: Diagnosis, management and models of care. Nature Reviews Nephrology 11(8), 491–502. [CrossRef]
- Arora P, Vasa P, Brenner D, Iglar K, McFarlane P, Morrison H, et al. Prevalence estimates of chronic kidney disease in Canada: results of a nationally representative survey. Can Med Assoc J. 2013;185:E417–23.
- Michel Rosner et al.: Health Economic Implications of Remote Patient Management in Peritoneal Dialysis. Contrib Nephrol. Basel, Karger, 2019, vol 197, pp 133–142. [CrossRef]
- ReLongkai Li; Jeffrey Perl (2019). [Contributions to Nephrology] Remote Patient Management in Peritoneal Dialysis Volume 197 || Can Remote Patient Management Improve Outcomes in Peritoneal Dialysis?.10.1159/isbn.978-3-318-06477-3(), 113–123. [CrossRef]
- Mitchell Rosner et al.: Health Economic Implications of Remote Patient Management in Peritoneal Dialysis. Contrib Nephrol. Basel, Karger, 2019, vol 197, pp 133–142 (DOI: 10.1159/000496999).
- Michael Whitlow; Eric Wallace: Remote Patient Management in Home Dialysis: Planning Considerations for the Future.2019;197:154-162. [CrossRef]
- Michelle Blaauw: Use of Sharesource in Remote Patient Management in Peritoneal Dialysis: A UK Nurse´s Perspective. Contrib Nephrol. Basel, Karger, 2019, vol 197, pp 73–83. [CrossRef]
- Sobrinho A. et al.: Design and evaluation of a mobile application to assist the self-monitoring of the chronic kidney disease in developing countries (Brasil - 2018), BMC Medical Informatics and Decision Making (2018) 18:7. [CrossRef]
- Martínez García MA, Fernández Rosales MS, López Domínguez E, Hernández Velázquez Y, Domıínguez Isidro S (2018) Telemonitoring system for patients with chronic kidney disease undergoing peritoneal dialysis: Usability assessment based on a case study. PLoS ONE 13 (11): e0206600. [CrossRef]
- Hailey, David M., "Telehealth in nephrology care - promises and challenges" (2016). Faculty of Engineering and Information Sciences - Papers: Part A. 5971. https://ro.uow.edu.au/eispapers/5971. [CrossRef]
- Natália Maria da Silva Fernandes, Marcus Gomes Bastos, Nivalda A. C. de Oliveira, Alex do Vale Costa, Heder Soares Bernardino: Development of a distance care system for pre-dialysis chronic kidney disease patients (Brasil 2014). [CrossRef]
- Scofano, R., Monteiro, A. & Motta, L. Evaluation of the experience with the use of telemedicine in a home dialysis program—a qualitative and quantitative study. BMC Nephrol 23, 190 (Brazil 2022). [CrossRef]
- Lianne Jeffs,Arsh Kumar Jain,Rachel HiuTung Man,Nike Onabajo… (2017). Exploring the utility and scalability of a telehomecare intervention for patients with chronic kidney disease undergoing peritoneal dialysis—a study protocol. BMC Nephrology, 18(1), –. [CrossRef]
- Morosetti M, Michelina Peccerillo,Fama MI. MO029 CLINICAL AND SOCIAL ADVANTAGES OF REMOTE PATIENT MONITORING IN HOME DIALYSIS | Nephrology Dialysis Transplantation | Oxford Academic. Nephrol Dial Transplant 2020 Jun;35(Supplement 3). G Ital Nefrol. 2020 Apr 9;37(2):2020-vol2. [CrossRef]
- El Shamy, Osama; Tran, Ha; Sharma, Shuchita; Ronco, Claudio; Narayanan, Mohanram; Uribarri, Jaime (2020). Telenephrology with Remote Peritoneal Dialysis Monitoring during Coronavirus Disease 19. American Journal of Nephrology, (), 1–3. [CrossRef]
- Milan Manani, Sabrina; Michele Beretta, Giuliani, Anna; Virzì, Grazia Maria; Garzotto, Francesca Martino; Carlo Crepaldi & Ronco, Claudio (2020). Remote Monitoring of in Peritoneal Dialysis: Benefits on Clinical Outcomes and on Quality of Life. Journal pf Nephrology 33(), 1301–1308. [CrossRef]
- Nygård HT, Nguyen L, Berg RC. Effect of remote patient monitoring for patients with chronic kidney disease who perform dialysis at home: a systematic review. BMJ Open 2022;12:e061772. [CrossRef]
- Rachael C Walker, Kirsten Howard, Rachael L Morton: Home hemodialysis: a comprehensive review of patient-centered and economic considerations,Clinicoecon Outcomes Res. 2017; 9: 149–161. Published online 2017 Feb 16. [CrossRef]
- Yang Y, Chen H, Qazi H, Morita PP. Intervention and evaluation of mobile health technologies in management of patients undergoing chronic dialysis: A scoping review. Vol. 8, JMIR mHealth and uHealth. JMIR Publications; 2020.
- Donald, M, Kahlon, BK, Beanlands, H, et al. Self-management interventions for adults with chronic kidney disease: a scoping review. BMJ Open 2018; 8(3): e019814.
- Wang, Su-Ming; Hsiao, Lien-Cheng; Ting, I-Wen; Yu, Tung-Min; Liang, Chih-Chia; Kuo, Huey-Liang; et al. (2015). Multidisciplinary care in patients with chronic kidney disease: A systematic review and meta-analysis. European Journal of Internal Medicine, (), S0953620515002289–. [CrossRef]
- Nesrallah GE, Mustafa RA, MacRae J, Pauly RP, Perkins DN, Gangji A, et al. Canadian Society of Nephrology guidelines for the management of patients with ESRD treated with intensive hemodialysis. Am J Kidney Dis 2013;62(1):187-98.
- Osterlund K, Mendelssohn D, Clase C, Guyatt G, Nesrallah G. Identification of facilitators and barriers to home dialysis selection by Canadian adults with ESRD. Semin Dial 2014;27(2):160-72.
- Abdel-Kader et al.: Primary care physicians’ familiarity, beliefs, and perceived barriers to practice guidelines in non-diabetic CKD: a survey study. BMC Nephrology 2014 15:64.
Figure 1.
Results about barriers that prevent from Use of ICT in Renal Replacement Therapy (RRT) in % (given by Portuguese nephrology HCP).
Figure 1.
Results about barriers that prevent from Use of ICT in Renal Replacement Therapy (RRT) in % (given by Portuguese nephrology HCP).
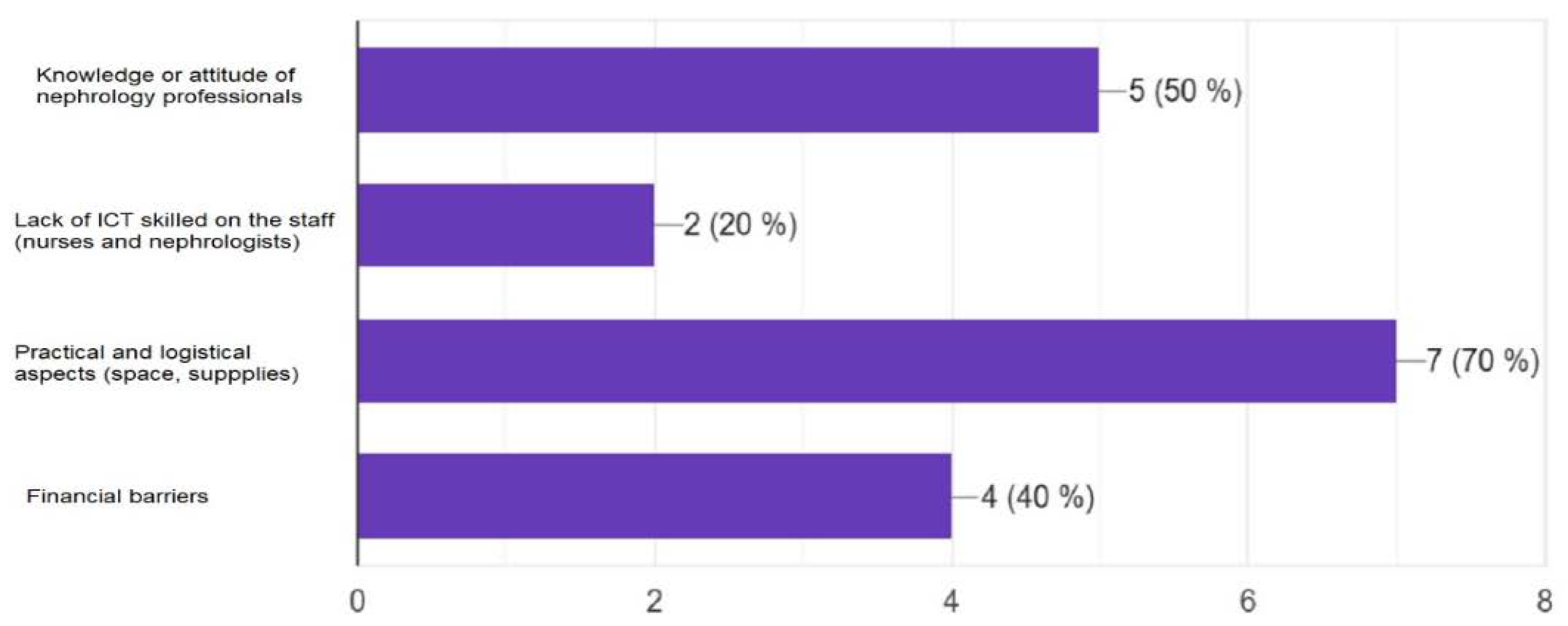
Figure 2.
Results about barriers that prevent from Use of ICT in Renal Replacement Therapy (RRT) in % (given by Spanish nephrology HCP).
Figure 2.
Results about barriers that prevent from Use of ICT in Renal Replacement Therapy (RRT) in % (given by Spanish nephrology HCP).
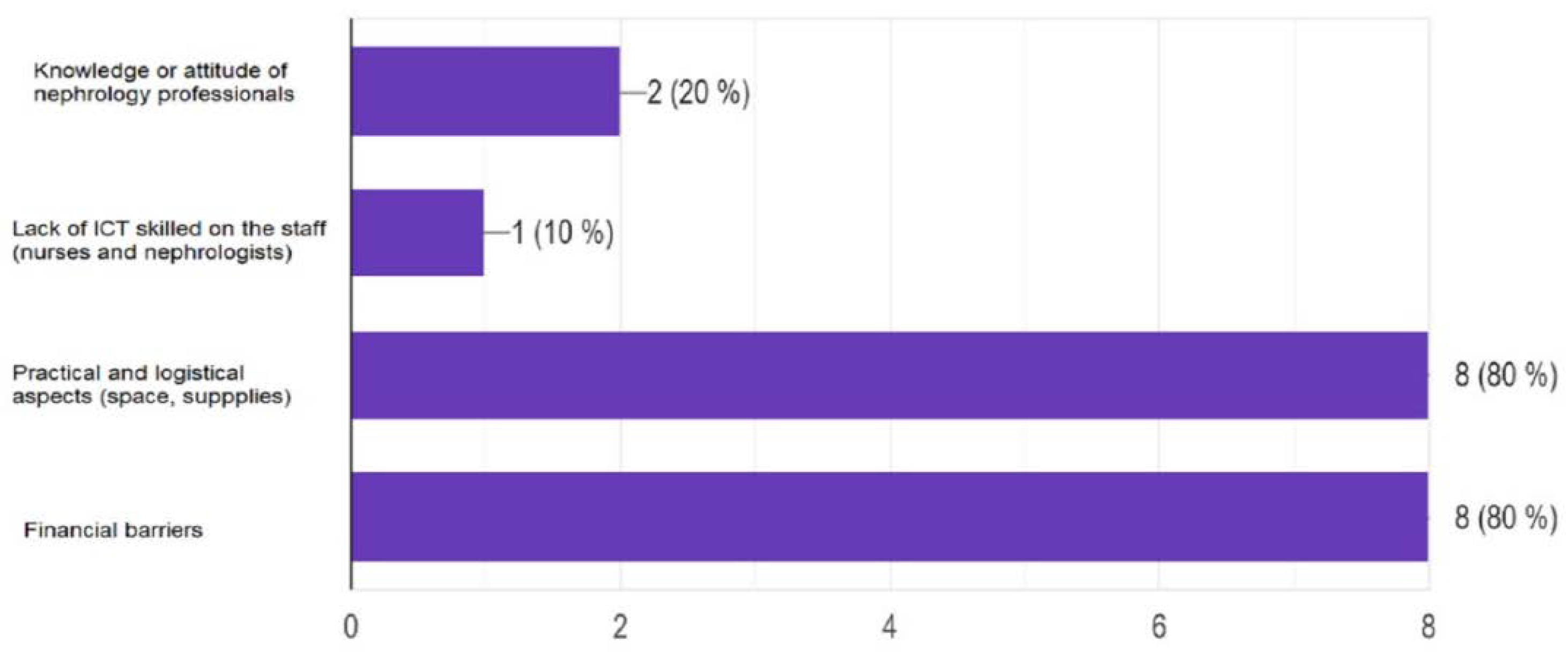
Figure 3.
Results concerning the barriers that prevent Nephrology units from providing Home Dialysis in % (answers given by Portuguese HCP).
Figure 3.
Results concerning the barriers that prevent Nephrology units from providing Home Dialysis in % (answers given by Portuguese HCP).
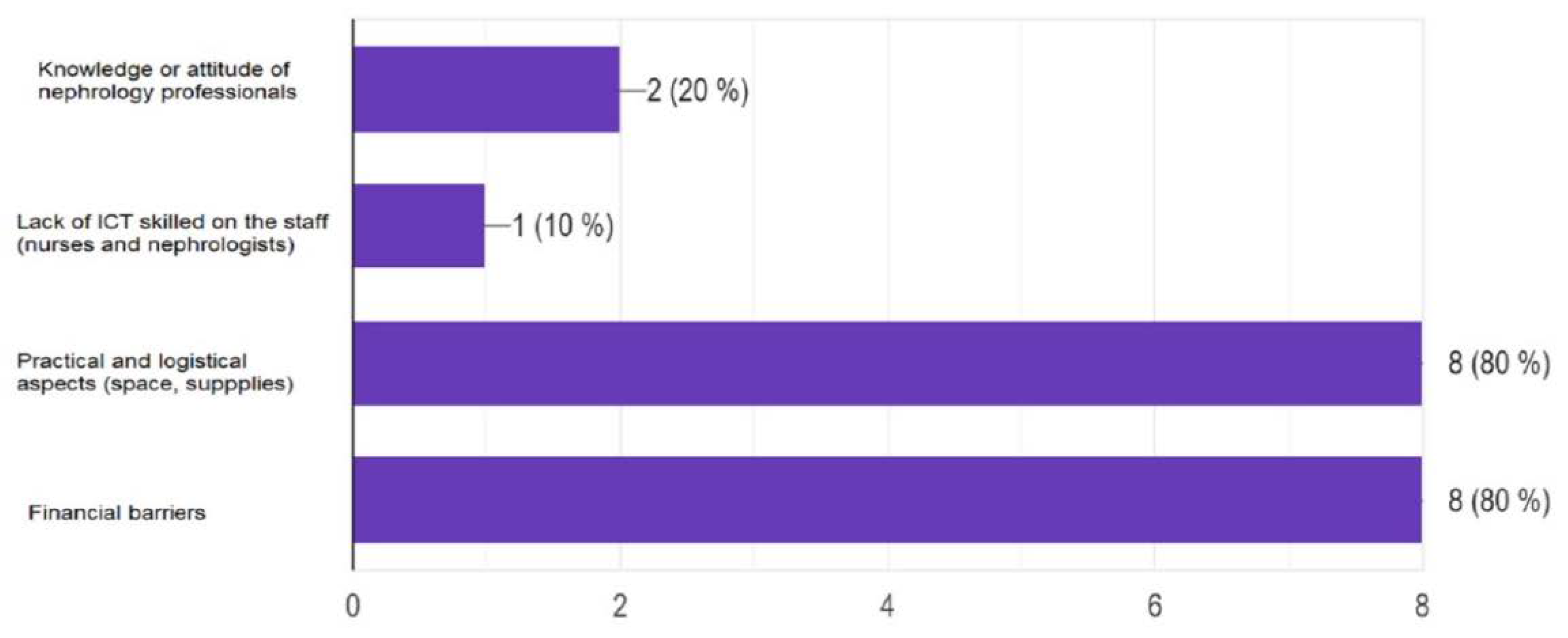
Figure 4.
Results concerning the barriers that prevent Nephrology units from providing Home Dialysis in % (answers given by Spanish nephrology HCP).
Figure 4.
Results concerning the barriers that prevent Nephrology units from providing Home Dialysis in % (answers given by Spanish nephrology HCP).
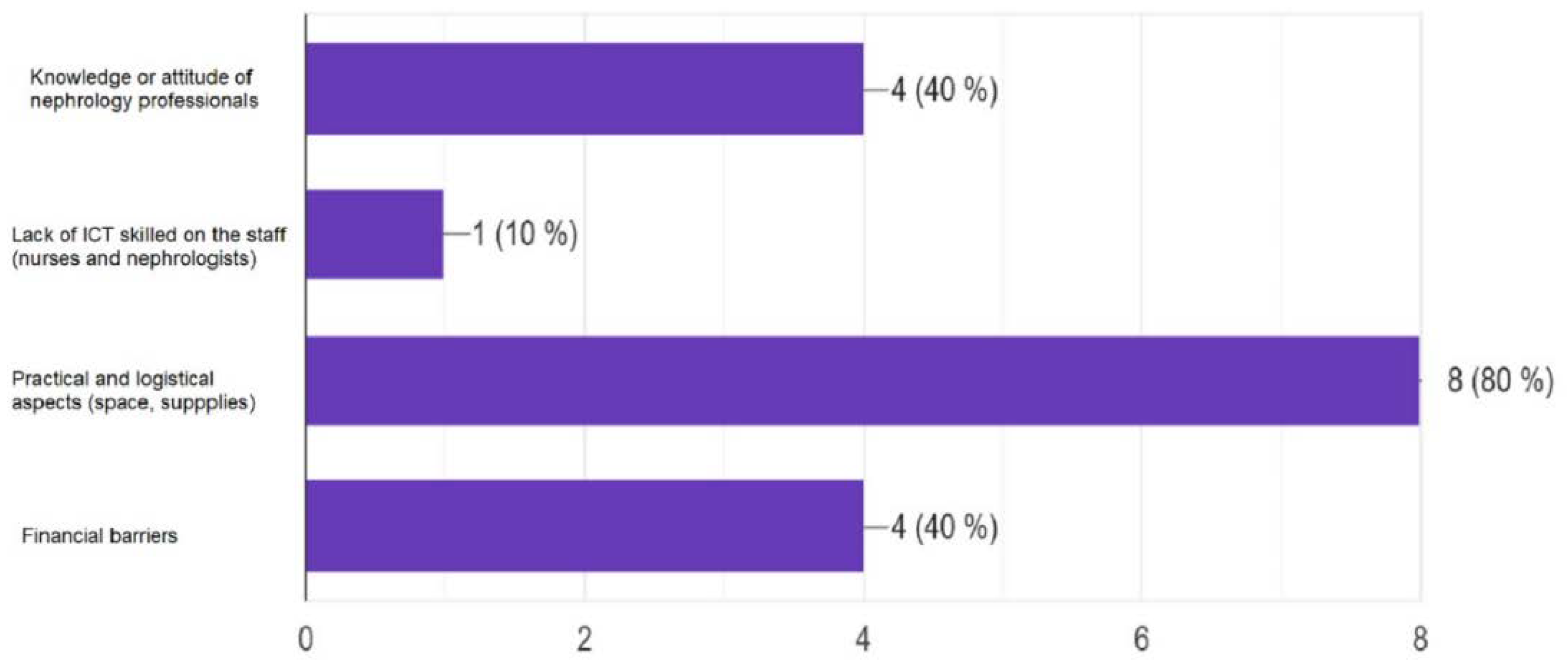
Figure 5.
Results concerning the barriers that would prevent Nephrology units from expanding Home Dialysis in % (answers given by Portuguese HCP).
Figure 5.
Results concerning the barriers that would prevent Nephrology units from expanding Home Dialysis in % (answers given by Portuguese HCP).
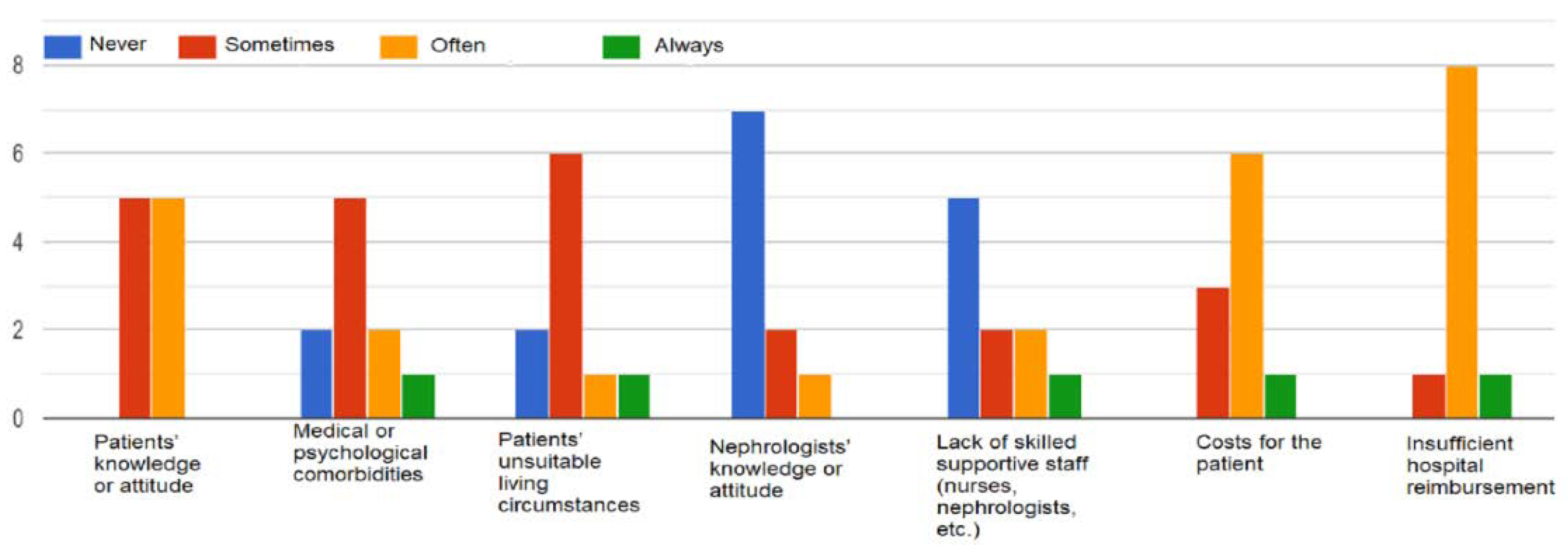
Figure 6.
Results concerning the barriers that would prevent Nephrology units from expanding Home Dialysis - HD and PD in %. (Answers given by Spanish HCP).
Figure 6.
Results concerning the barriers that would prevent Nephrology units from expanding Home Dialysis - HD and PD in %. (Answers given by Spanish HCP).
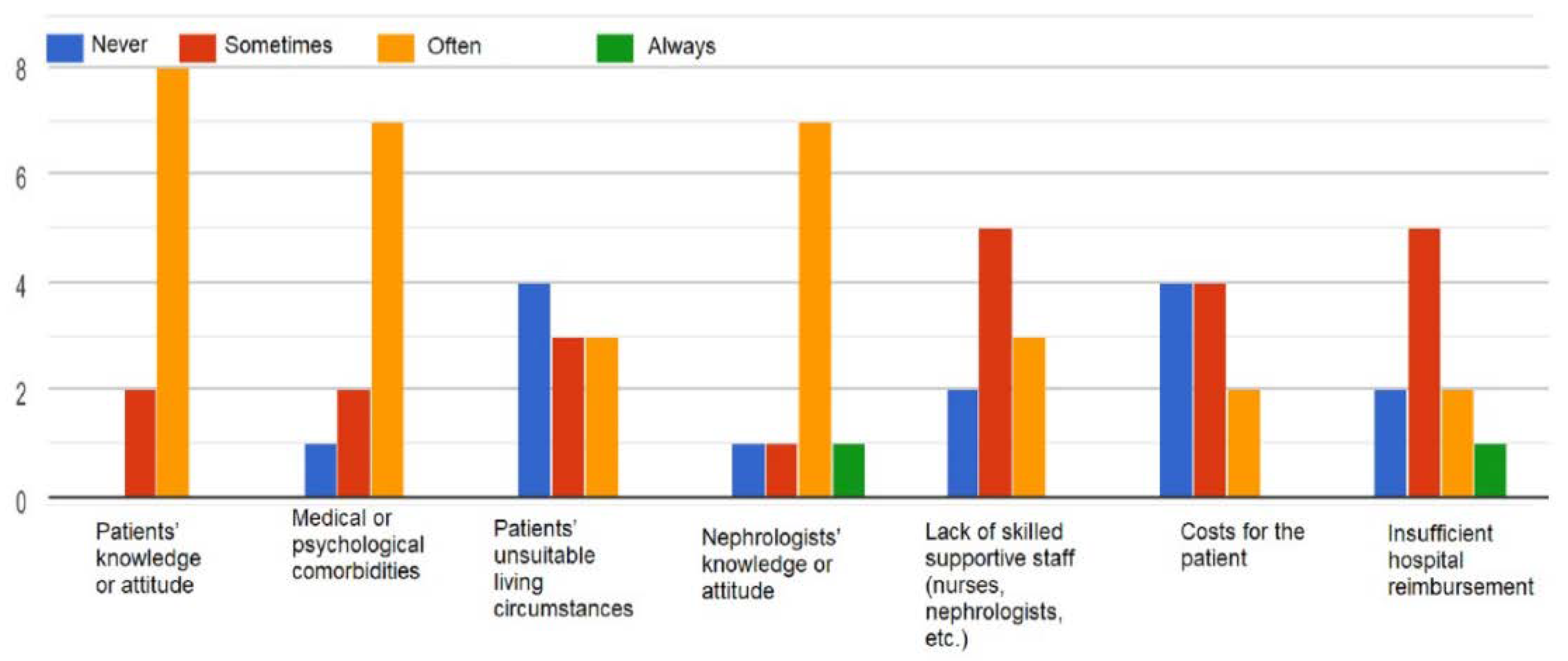
Figure 7.
Results concerning Nephrology HCP opinion about the potential value of Platform or Software to manage Renal Replacement Therapy (RRT) (answers given by Portuguese HCP).
Figure 7.
Results concerning Nephrology HCP opinion about the potential value of Platform or Software to manage Renal Replacement Therapy (RRT) (answers given by Portuguese HCP).
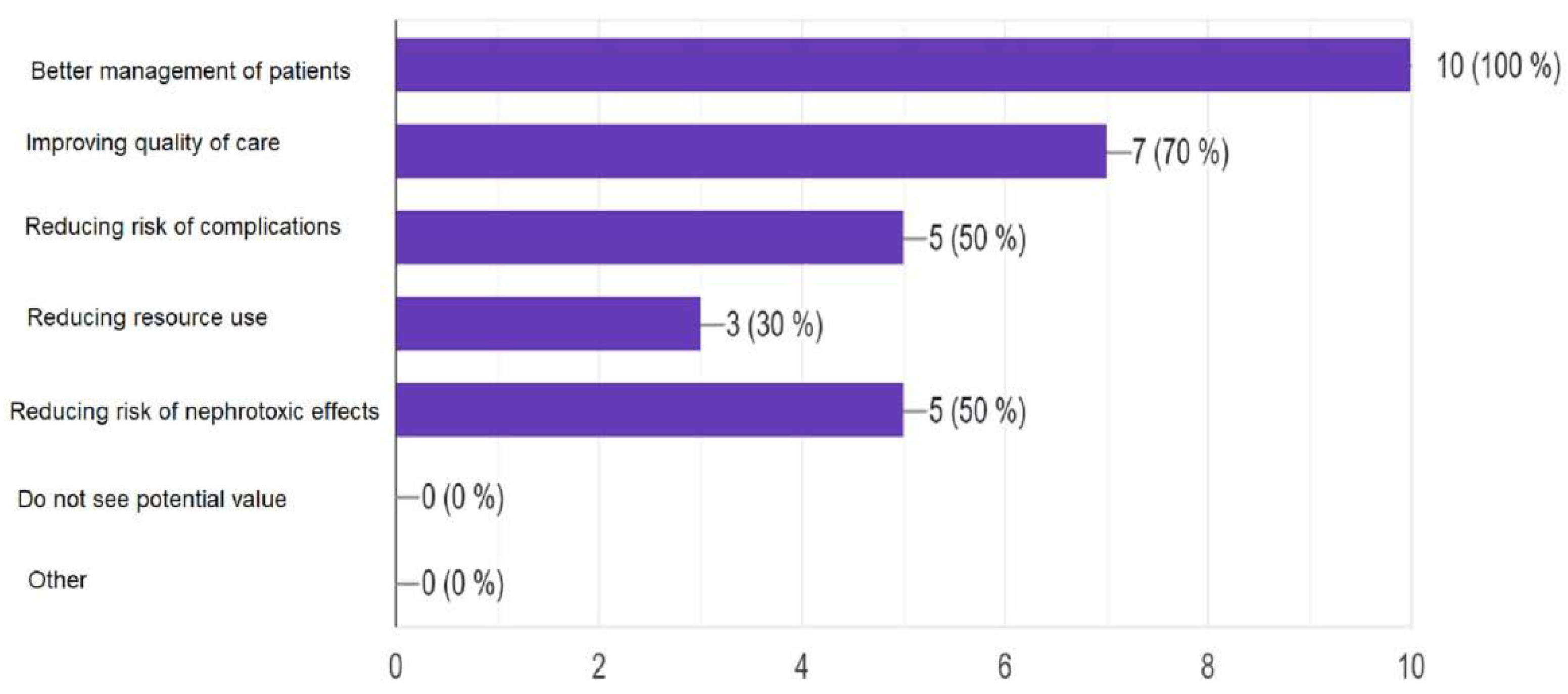
Figure 8.
Results concerning Nephrology HCP opinion about the potential value of Platform or Software to manage Renal Replacement Therapy (RRT) in % (answers given by Spanish HCP).
Figure 8.
Results concerning Nephrology HCP opinion about the potential value of Platform or Software to manage Renal Replacement Therapy (RRT) in % (answers given by Spanish HCP).
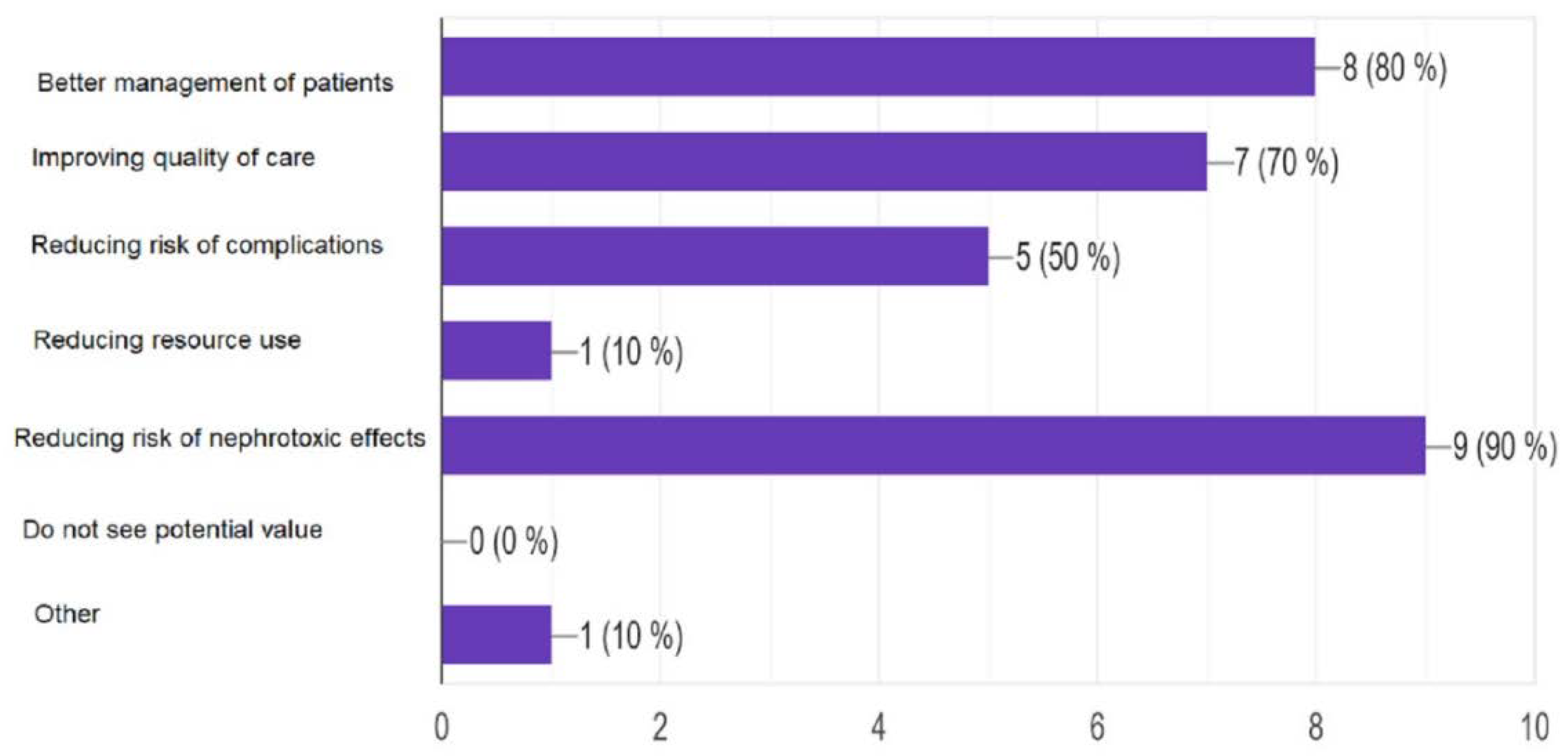
Figure 9.
Results concerning Nephrology HCP attitude towards Platform or Software to manage the Renal Replacement Therapy (RRT) in % (answers given by Portuguese HCP).
Figure 9.
Results concerning Nephrology HCP attitude towards Platform or Software to manage the Renal Replacement Therapy (RRT) in % (answers given by Portuguese HCP).
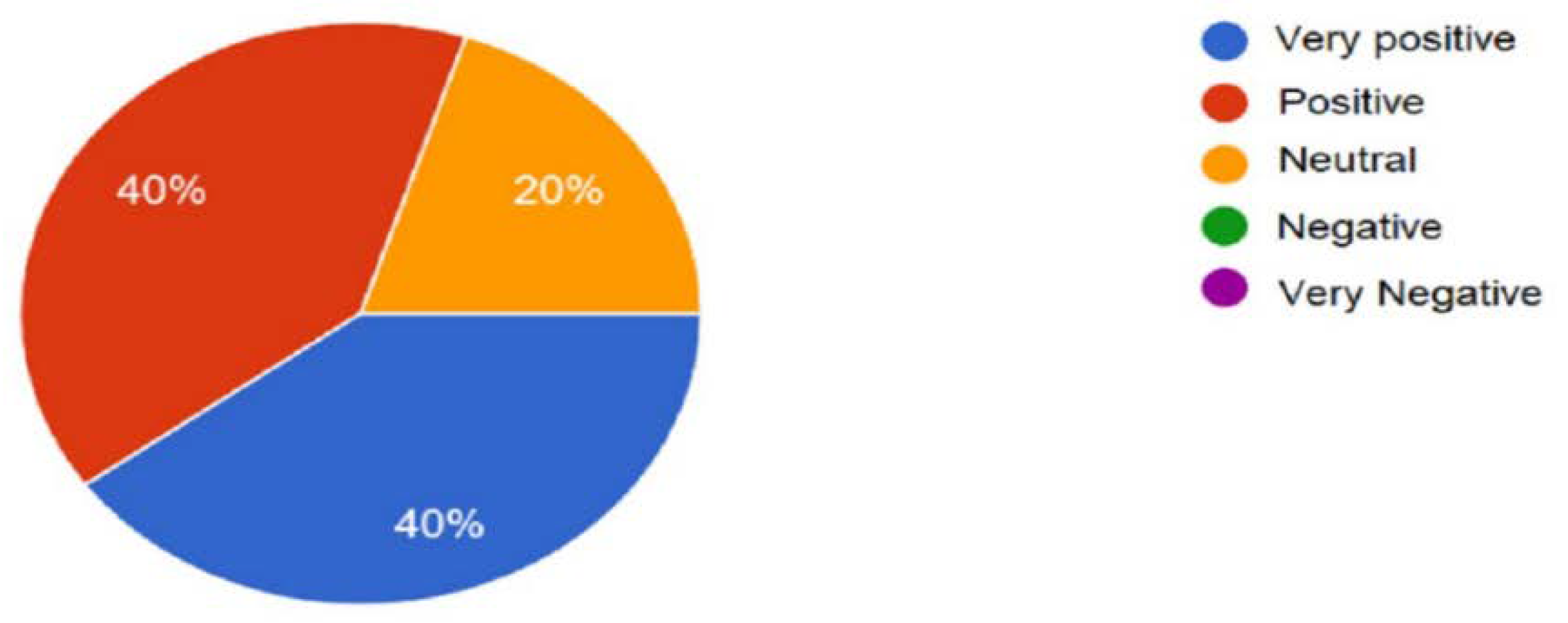
Figure 10.
Results concerning Nephrology HCP attitude towards Platform or Software to manage the Renal Replacement Therapy (RRT) in % (answers given by Spanish HCP) in %.
Figure 10.
Results concerning Nephrology HCP attitude towards Platform or Software to manage the Renal Replacement Therapy (RRT) in % (answers given by Spanish HCP) in %.
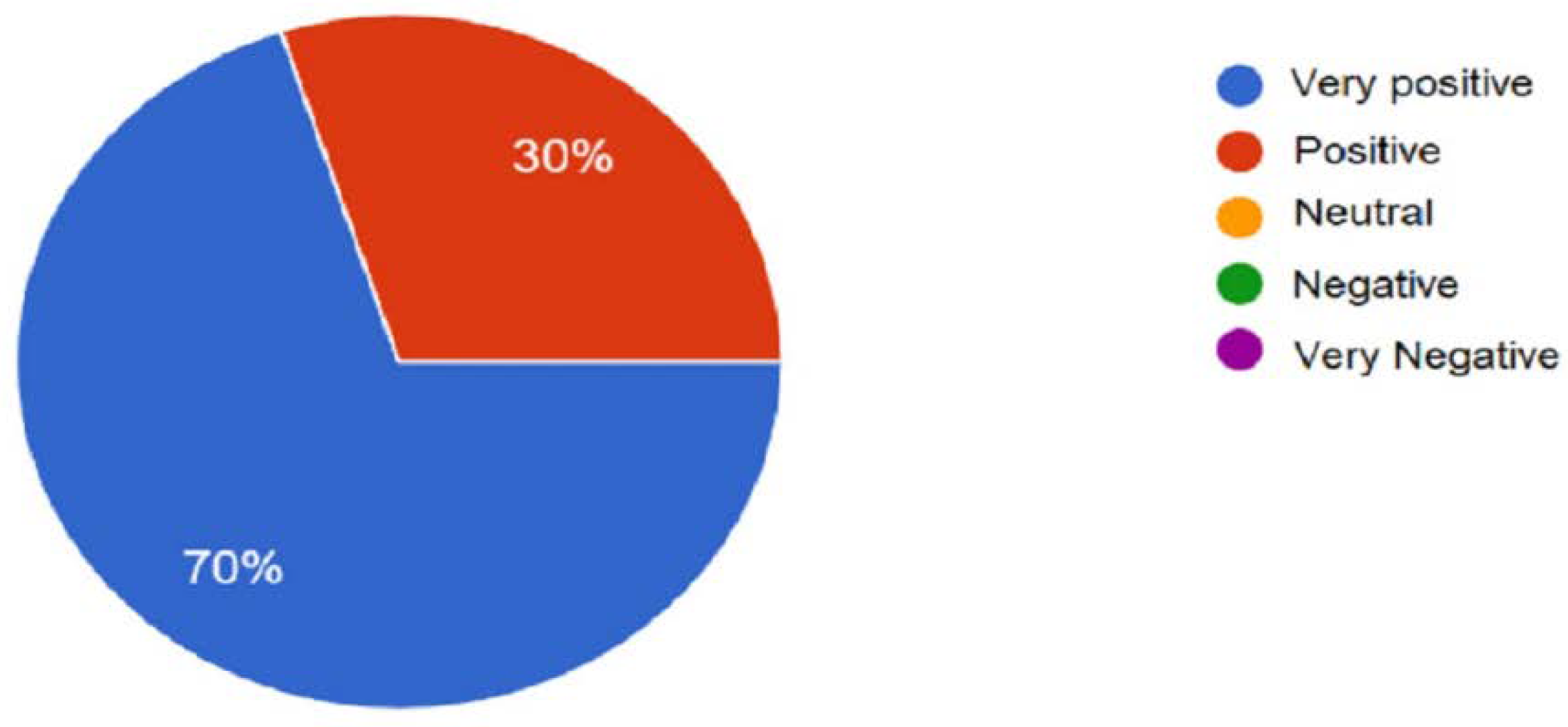

Table 1.
Demographic characteristics of respondents.
| Characteristic | n= 20 | |||
|---|---|---|---|---|
| Portugal | Spain | Global | ||
| Age group | 26-39 => 1 | 26-39 =>5 | 26-39 => 6 | |
| 40-49 => 7 | 40-49 =>5 | 40-49 => 12 | ||
| 50-59 => 1 | 50-59 =>0 | 50-59 => 1 | ||
| 60-69 => 1 | 60-69 =>0 | 60-69 => 1 | ||
| woman | 4 (40%) | 7 (60%) | 11(55%) | |
| profession | ||||
| nephrologist | 3 (30%) | 1 (10%) | 4 (20%) | |
| nephrology/renal nurse | 7 (70%) | 9 (90%) | 16 (80%) | |
| geographic area | rural | 1 (10%) | 0 | 1 (5%) |
| urban | 9 (90%) | 10 (100%) | 19 (95%) | |
Table 2.
Comparative summary of results with relevant (the highest) percentage.
| Questionnaire Topic | Portugal (%) | Spain (%) | ||||
|---|---|---|---|---|---|---|
| ICT intervention in RRT … | Affirmative | NULL | Negative | Affirmative | NULL | Negative |
| Improve patient safety | 70 | - | 30 | - | - | |
| Personalized treatment | 60 | - | - | - | - | |
| Total focus on the patient | - | - | 20 | - | - | |
| More than 5 years working without ICT intervention | 40 | - | 30 | - | - | |
| 1-5 years working without ICT intervention | 10 | - | - | 50 | - | - |
| Use ICT tools for RRT daily | 80 | 10 | 70 | |||
| The ICT tools is Excellent for RRT | 40 | - | - | 80 | - | - |
| ICT tools are Good for RRT | 40 | - | - | 20 | - | - |
| ICT improves the quality of RRT service | 50 | - | - | 60 | - | - |
| HCP feels comfortable using ICT for RRT | 80 | - | - | 80 | - | - |
| ICT for RRT has a positive effect on the patients | 50 | - | 10* | 80 | - | 20* |
| Not sure if ICT for RRT has a positive effect on the patients | - | 40 | - | - | - | - |
| The technical issue occurs sometimes | 70 | - | - | 70 | - | |
| Sometimes organizational issue occurs | 50 | - | - | 70 | - | |
| Would you recommend the ICT for RRT? | 80 | - | - | 90 | - | - |
| Using ICT for RRT is a very good solution. | 50 | - | - | 70 | - | - |
| Total of CKD patients in your center is =or > 100? | 50 | - | - | 30 | - | - |
| Total of CKD patients in your center is =or > 200? | - | - | - | 30 | - | - |
| Practical and logistic aspect is the main burden for the spread of ICT in RRT | 80 | - | - | 80 | - | - |
| Financial barriers are the main burden for the spread of ICT in nephrology | 40 | - | - | 80 | - | - |
| Knowledge or attitude of nephrology HCP is the main burden for the spread of ICT in nephrology | 50 | - | - | 40 | - | - |
| Practical and logistic aspect is the main burden for the impulse of HHD | 80 | -- | - | 80 | - | - |
| Financial barriers are the main burden for the impulse of HHD | 80 | - | - | 40 | - | - |
| Knowledge or attitude of nephrology HCP is the main burden for the impulse of ICT in HHD | 20 | - | - | 40 | - | - |
| Your attitude towards ICT in RRT is very positive | 40 | 20 | - | 70 | - | - |
| Your attitude towards ICT in RRT is positive | 40 | - | - | 30 | - | - |
| Your attitude towards ICT in RRT is negative | 0 | - | - | 0 | - | - |
| Better patients management | 100 | - | - | 80 | - | - |
| Improving the quality of care | 70 | - | - | 70 | - | |
| Reducing the risk of complications | 50 | - | - | 50 | - | - |
| Optimize the use of resources | 50 | - | - | 90 | - | |
*respondents that said “Nothing changed, it is still the same”.
Table 3.
Comparative results by profession and country.
| Questionnaire Topics | Portugal | Spain | ||
|---|---|---|---|---|
| Implications of ICT intervention in RRT | Nephrologist | Nurse | Nephrologist | Nurse |
| Improve patient safety | 66,7% | 71,4% | 0% | 33,3% |
| Personalized treatment | 100% | 71,4% | 0% | 0% |
| Total focus on the patient | 66,7% | 42,9% | 0% | 22,2% |
| ICT tools promote the integration and mobility of information | 100% | 57,1% | 0% | 11,1% |
| ICT tools promote cost-saving | 66,7% | 0% | 0% | 0% |
| ICT tools are Excellent for RRT | 66,7% | 28,6% | 100% | 77,8% |
| ICT tools are Good for RRT | 33,3% | 57,1% | 0% | 22,2% |
| ICT improves the quality of RRT service | 66,7% | 57,1% | 100% | 77,8% |
| ICT reducing Human error | 66,7% | 42,9% | 0% | 0% |
| HCP feels comfortable using ICT for RRT | 66,7% | 100% | 100% | 88,9% |
| ICT for RRT has a positive effect on the patients | 66,7% | 42,9% | 100% | 77,8% |
| Not sure if ICT for RRT has a positive effect on the patients | 33,3% | 42,9% | 0% | 22,2% |
| Practical and logistic aspect is the main burden for the spread of ICT in RRT | 66,7% | 57,1% | 100% | 6/9% |
| Financial barriers are the main burden for the spread of ICT in nephrology | 66,7% | 28,6% | 100% | 77,8% |
| Knowledge or attitude of nephrology HCP is the main burden for the spread of ICT in nephrology | 66,7% | 42,9% | 100% | 33,3% |
| Practical and logistic aspect is the main burden for the impulse of Dialysis at home | 100% | 6/7% | 100% | 77,8% |
| Financial barriers are the main burden for the impulse of Dialysis at home | 66,7% | 6/7% | 100% | 33,3% |
| Knowledge or attitude of nephrology HCP is the main burden for the impulse of Dialysis at home | 66,7% | 0% | 100% | 33,3% |
| Your attitude towards ICT in RRT is very positive | 66,7 | 28,6% | 100% | 66,7% |
| Your attitude towards ICT in RRT is positive | 0% | 57,1% | 0% | 33,3% |
| Your attitude towards ICT in RRT is negative | 0% | 0% | 0% | 0% |
| Better patients management | 100% | 100% | 100% | 88,9% |
| Improving the quality of care | 100% | 57,1% | 100% | 55,6% |
| Reducing the risk of complications | 66,7% | 42,9% | 100% | 44,4% |
| Optimize the use of resources | 66,7% | 57,1% | 100% | 88,9% |
| ICT promotes paper-free | 100% | 57,1% | 0% | 0% |
Table 4.
Set of additional comments given by the respondents.
| Open Questions | Portuguese HCPs comments | Spanish HCPs comments |
|---|---|---|
| How do you rate the quality of care delivered using the Platform for Renal Replacement Therapy when compared to the quality of traditional care? Please justify your answer. |
|
|
| Would you recommend the Software or Platform for Management of Renal Replacement Therapy? Please justify your answer. |
|
|
| Tell us what you most LIKE about using this Platform for Renal Replacement Therapy management. Please justify your answer. |
|
|
| Where do you see the potential value of Platform or Software to manage the Renal Replacement Therapy (RRT)? Please justify your answer. |
|
|
| If you have any additional comments, we would be very pleased to hear/read them. |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



