Submitted:
07 November 2023
Posted:
08 November 2023
You are already at the latest version
Abstract
Benign prostatic obstruction (BPH) is a common disease with male and surgical treatment is the gold standard for symptomatic disease. Prostate Artery Embolization (PAE) is one of emerging therapies which aims to minimize the lower urinary tract symptoms (LUTS) of BPH and volume of enlarged prostate. We reported here a case of 100-year-old man with 90 cm3 prostate and severe symptoms secondary to BPH, who underwent a successful PAE through distal transradial access without any complication. The patient satisfied with this treatment and no symptoms recurrence after PAE. It demonstrated that PAE was a safe and effective treatment for BPH and was indicated in elderly/ non-surgical candidate.
Keywords:
distal TransRadial (dTRA)
; PAE
; BPH
1. Introduction
Benign prostatic obstruction (BPH) is a common disease with male and surgical treatment is the gold standard for symptomatic disease. Prostate Artery Embolization (PAE) is one of emerging therapies which aims to minimize the lower urinary tract symptoms (LUTS) of BPH and volume of enlarged prostate. Recently, there was a 100-year-old man with good past health admitted for BPH treatment presenting refractory urinary tract infections (UTI), recurrent gross haematuria and nocturia 3 times every night. He was diagnosed with BPH since 2013 and prior medical treatments including Tamsulosin, Dutasteride, and Bethanechol etc. failed to control the BPH-related symptoms. His prostate volume was found to be 89.39 cm3. Surgical treatments were not considered, and he was referred to our department for PAE in September 2020 as he was committed to treat BPH for better quality of life and lower frequent hospitalization for UTI and haematuria.
2. Methods
Pre-PAE MRI showed an enlarged prostate with central gland 89.39 cm3 (5.90cm x 4.41 cm x 3.84cm) (Figure 1a- b). After discussion with urologist, this patient was identified as a PAE candidate.
The PAE procedure was done via left distal transradial access (dTRA). After local anaesthesia (LA), 3000IU Heparin was injected via sheath. A 125cm catheter (Ultimate, Merit Medical Inc.) was introduced via distal radial artery straight-down to the common iliac artery and navigated to right internal iliac artery. The procedure was complicated by severe stenosis in right internal iliac artery and microcatheter advancement toward right prostate artery was not feasible. Right femoral access was attempted but again failed due to stenosis. (Figure 2a) Left prostate artery showed both sides prostate perfusion and was accessible uneventfully by a 2.4F microcatheter (150cm Maestro, Merit Medical Inc.) through intraprostatic anastomosis (Figure 2 b-c). A pre-filled syringe of 300-500um Tri-acryl gelatin microspheres (Embosphere, Merit Medical Inc.) was mixed with 10ml iodinated contrast agent, and 1ml of the microsphere was injected slowly until the antegrade flow stopped. Unilateral PAE was performed due to severe stenosis at the right side. Procedural time was 220 min. Haemostasis by compression was 2 hours and bedrest was 4 hours. Patient was discharge on the next day without complication.
3. Results
Patient was followed up at 1 week in the Department of Urology, significant improvement in symptom score was noted. Further improvement was found along the follow-ups with 78.3% at month 12 and a total of IPSS 18 points improvement. Quality of life (QoL) was improved significantly from 5 to 1 at week 1 and good through the last follow-up. 6-month MRI showed a significant prostate volume reduction of 20.3% and 12- & 24-month MRI with 28.6% and 35% reductions, respectively. (Figure 1 c-d) PSA dropped 47.3% from baseline to month 12. The post-void residual volume improved by 43.5% at 1-year follow-up from 155ml at baseline to 87.6ml. Patient stopped medical treatment at month 12 and no longer continue thereafter. No further hospitalization regarding BPH after PAE nor symptom recurrence for more than 3 years. Patient lived a normal life with minimal LUTS. Table 1 describes the clinical outcomes of this patient.
4. Discussion
Benign prostatic obstruction (BPH) is a common disease with male. 50 percent of male who aged 51 to 60 will have BPH, and the percentage will increase by age and 75% by 70 years.1 Although treatments of BPH have been emerged in recent decades, surgical treatments are the gold standard for symptomatic BPH refractory to medical therapy.2 However, for patients older than 80 years of age is usually not suitable for surgeries and minimal invasive options must be explored. PAE has been proposed for many years as an alternative to surgery and been recognised in many countries.3-4 The indications of PAE in our institute includes BPH-related LUTS management, and the advantages of PAE are minimal invasive under LA while maintaining the sexual function.
To our knowledge, this is the first case presents the PAE treatment for a 100-year-old man via dTRA demonstrating the feasibility, safety and clinical efficacy with 2 years follow up. This patient had severe LUTS secondary to BPH since 2013 with IPSS score of 23 and refractory to medical treatment and a non-surgical candidate. PAE brought a new insight into symptomatic BPH management and together with dTRA, patient does not require to stop antiplatelet drugs with the ease of haemostasis, a shorter post-procedural bedrest, and an ambulatory procedure, which is demonstrated to safe for elderly and non-surgical candidates.5-6 This patient reminded us of the needs of bothersome LUTS management and a better quality of life.
Aligned with previous investigations, our report also showed significant LUTS improvement from Severe at baseline to Moderate at 1-month and further down to Mild at 6-month. 78.3% improvement relevant to 18 IPSS points at 1 year and good through 2-year. PAE was demonstrated to be effective to reduce prostate volume of 35% without any complications.7 Although only unilateral prostate artery was selection by microcatheter, both sides PAE was done for this case by cone beam CT(CBCT) image confirm. This is the first reporting image show both sides prostate perfusion by unilateral prostate artery due to severe stenosis on the other side. Although unilateral PAE was done for this case, which was shown to be one of the negative factors for clinical success, the clinical outcomes were found to be comparable to the existing reports.8 In Bilhim et al 2013, bilateral PAE lead to better clinical results but 50% of patients received unilateral PAE also showed a good clinical outcome like this case.8 From our experience, unilateral PAE is considered a technical success and improvement of IPSS 25% or more from baseline is determined as a clinical success. In this case, both technical and clinical successes were achieved, and PAE was shown to be safe and effective for elderly who is eager to treat the bothersome LUTS secondary to BPH. No symptoms recurrence after PAE was identified.
The learning of this PAE case is procedural time management. A prior Pelvic CTA must be performed to identify the vessels and stenosis for better PAE planning and a potential saving in procedural time. Technical aspect is still the main hurdles due to the anatomical variants of prostate artery and arterial stenosis. CTA is suggested to map all vessels for PAE. To promote PAE as a treatment option for BPH in Taiwan, standardised measurements of clinical outcomes from PAE have to be implemented in our institute including IIEF, QoL and Urodynamics. A technical guide for PAE via dTRA must be established. dTRA could be the first choice of access if the patient radial artery is larger than 2.6mm with radial sheath use or larger than 1.6mm with thin-walled sheath use. It is now spreading in many institutes for outpatient/ day procedure.9 However, due to the limitation of catheter availability in Taiwan, BPH patients, who are fit for PAE and taller than 175cm, dTRA is not feasible and Transfemoral Access will be chosen.
5. Conclusions
Herein this case report, a 100-year-old patient showed that PAE was a safe and efficient treatment for BPH, even though unilateral PAE was achieved. For elderly/ non-surgical candidates, PAE is preferable to surgery especially via TRA/ dTRA approach.
Declarations
The authors declared that they have no conflict of interest financially and non- financially. This study was not supported by any funding.
Acknowledgments
Pansy TSE supported the editing of this report.
References
- Berry, S.J.; Coffey, D.S.; Walsh, P.C.; Ewing, L.L. The development of human benign prostatic hyperplasia with age. J Urol. 1984, 132, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Shvero, A.; Calio, B.; Humphreys, M.R.; Das, A.K. HoLEP: the new gold standard for surgical treatment of benign prostatic hyperplasia. Can J Urol. 2021, 28, 6–10. [Google Scholar] [PubMed]
- Bhatia, S.; Harward, S. H.; Sinha, V. K.; Narayanan, G. Prostate Artery Embolization via Transradial or Transulnar versus Transfemoral Arterial Access: Technical Results. J Vasc Interv Radiol. 2017, 28, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Ontario Health (Quality). Prostatic Artery Embolization for Benign Prostatic Hyperplasia: A Health Technology Assessment. Ont Health Technol Assess Ser. 2021, 21, 1–139. [Google Scholar]
- Thakor, A.S.; Alshammari, M.T.; Liu, D.M.; Chung, J.; Ho, S.G.; Legiehn, G.M.; Machan, L.; Fischman, A.M.; Patel, R.S.; Klass, D. Transradial Access for Interventional Radiology: Single-Centre Procedural and Clinical Outcome Analysis. Can Assoc Radiol J. 2017, 68, 318–327. [Google Scholar] [CrossRef] [PubMed]
- 6. Xu, C.; Zhang, G.; Wang, J.J.; Zhou, C.X.; Jiang, M.J. Safety and efficacy of prostatic artery embolization for large benign prostatic hyperplasia in elderly patients. Int Med Res. 2021, 49, 1–11. [Google Scholar]
- Carnevale, F.C.; Moreira, A.M.; de Assis, A.M.; Antunes, A.A.; de Paula Rodrigues, A.C.; Srougi, M., et al.; et al. Prostatic Artery Embolization for the Treatment of Lower Urinary Tract Symptoms Due to Benign Prostatic Hyperplasia: 10 Years' Experience. Radiology 2020, 2, 191249. [Google Scholar] [CrossRef] [PubMed]
- Tiago Bilhim, Joa˜o Pisco, Hugo Rio Tinto, Lu´cia Fernandes, Luı´s Campos Pinheiro, Marisa Duarte, Jose´ A. Pereira, Anto´nio G. Oliveira, Joa˜o O’Neil. Unilateral Versus Bilateral Prostatic Arterial Embolization for Lower Urinary Tract Symptoms in Patients with Prostate Enlargement. Cardiovasc Intervent Radiol 2013, 36, 403–411.
- 9. Amouyal, G.; Tournier, L.; de Margerie-Mellon, C.; Bouda, D.; Pachev, A.; Assouline, J.; et al. Feasibility of Outpatient Transradial Prostatic Artery Embolization and Safety of a Shortened Deflation Protocol for Hemostasis. J. Pers. Med. 2022, 12, 12. [Google Scholar] [CrossRef]
Figure 1.
MRI images of patient’s BPH. (a-b) Pre-Procedural MRI showed enlarged prostate of 89.39 cm3 (5.90cm x 4.41 cm x 3.84cm). (c-d) Post-procedural MRI at 24-months showed 66.05 cm3 (4.92cm x 3.58 cm x 3.75cm).
Figure 1.
MRI images of patient’s BPH. (a-b) Pre-Procedural MRI showed enlarged prostate of 89.39 cm3 (5.90cm x 4.41 cm x 3.84cm). (c-d) Post-procedural MRI at 24-months showed 66.05 cm3 (4.92cm x 3.58 cm x 3.75cm).
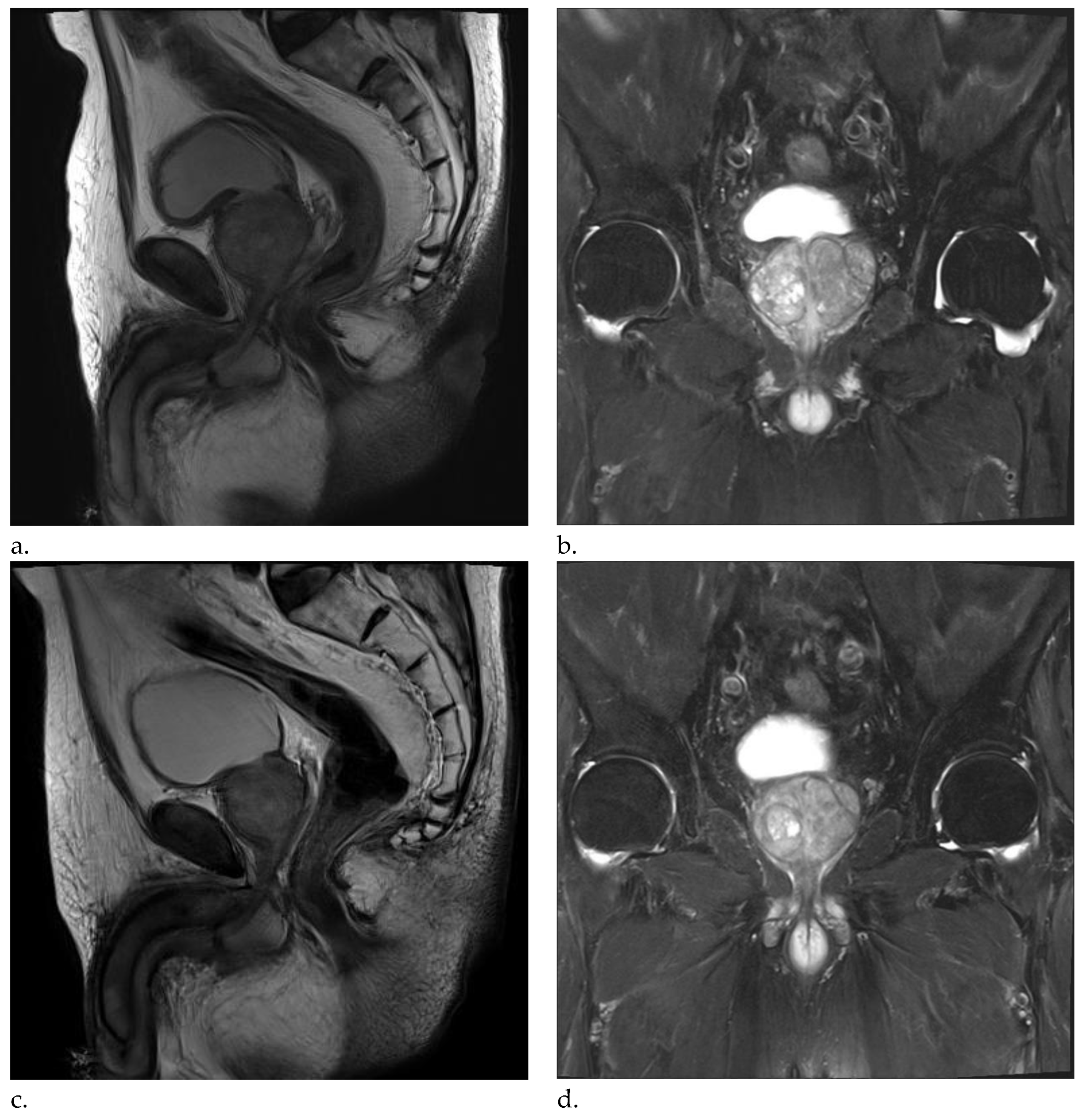
Figure 2.
(a) Right internal iliac angiography (oblique view RAO 30 degrees) show high grade stenosis (circle) at branch to the right prostate artery (green arrow) (b) Left internal iliac angiography (oblique view LAO 30 degrees) show the left prostate artery (red arrow) with contrast opacified at right side prostate artery (green arrow) (c) Left prostate angiography (AP view) show both side prostate perfusion via intraprostatic anastomosis (arrowhead). (d) CBCT images showed prostate perfusion at both sides on left prostate angiography.
Figure 2.
(a) Right internal iliac angiography (oblique view RAO 30 degrees) show high grade stenosis (circle) at branch to the right prostate artery (green arrow) (b) Left internal iliac angiography (oblique view LAO 30 degrees) show the left prostate artery (red arrow) with contrast opacified at right side prostate artery (green arrow) (c) Left prostate angiography (AP view) show both side prostate perfusion via intraprostatic anastomosis (arrowhead). (d) CBCT images showed prostate perfusion at both sides on left prostate angiography.
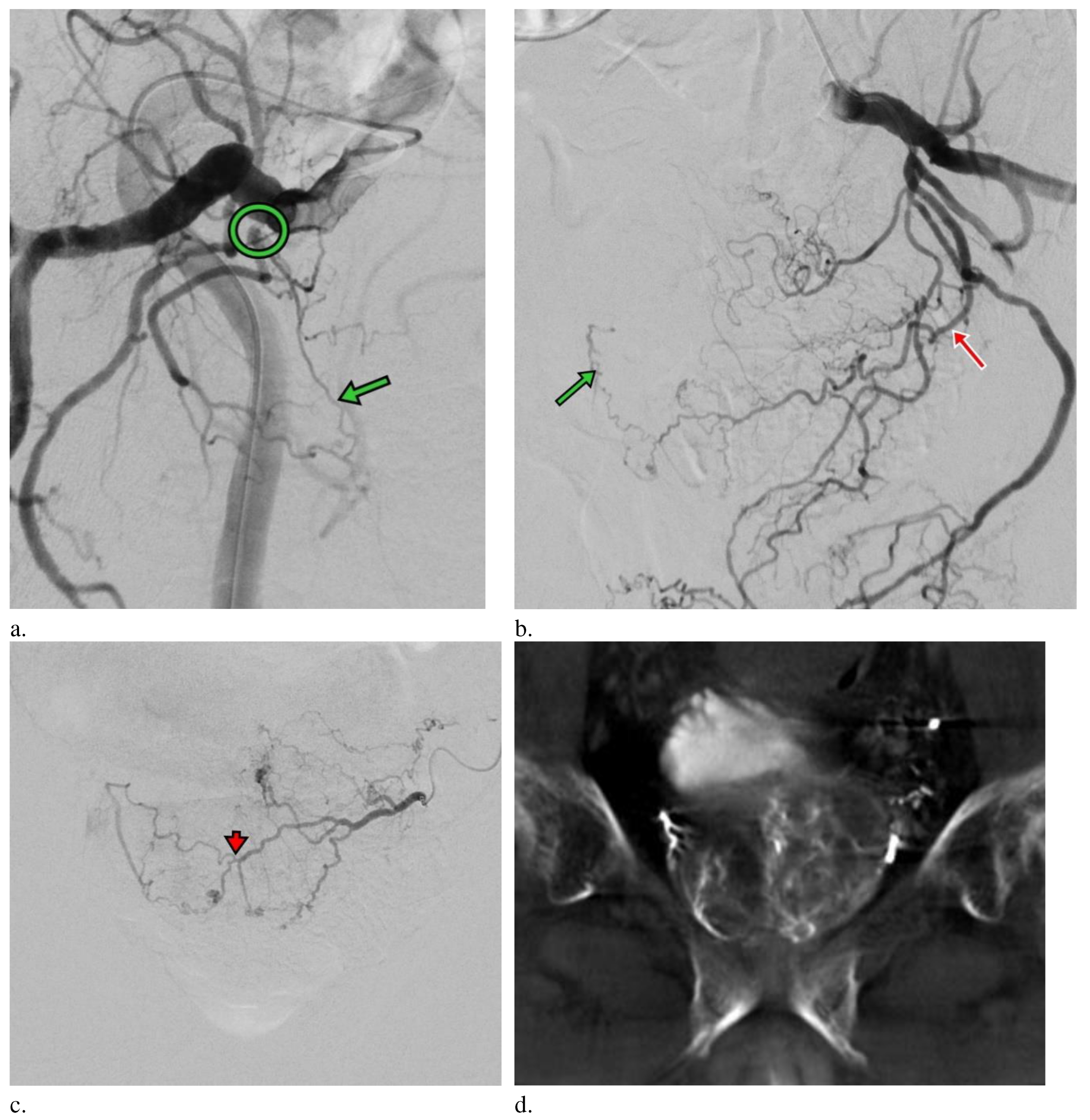

Table 1.
Baseline Characteristics of patient and clinical outcomes after PAE.
| Baseline | 1-week | 1-month | 6-months | 12-months | 24-months | |
|---|---|---|---|---|---|---|
| IPSS | 23 | 15 | 8 | 7 | 5 | 5 |
| Prostate Volume | 89.39 cm3 | NA | NA | NA | 63.78 cm3 | 66.05 cm3 |
| Post-void residual volume | 155 ml | NA | NA | NA | 87. 6ml | NA |
| Quality of Life | 5 | 1 | 1 | 1 | 1 | 1 |
| Complication | NA | 0 | 0 | 0 | 0 | 0 |
| Severe Complication | NA | 0 | 0 | 0 | 0 | 0 |
| Clinical Success | NA | Yes | Yes | Yes | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



