
Submitted:
02 November 2023
Posted:
09 November 2023
You are already at the latest version
Abstract
Trend patterns of melanoma skin in Serbia from 1999 to 2020
*Rancic K. Natasa 1,2, Tiodorovic B. Danica 1,4, Ilic V. Mirko 2, Biljana N. Kocic 1,2, Maksimovic S. Natasa 3, Ilija D. Kocic 4, Dusan P. Miljkovic 4, Otasevic A. Suzana 1,2
Introduction. Melanoma of the skin represents about 1% of all skin cancers and it causes nearly 80% of skin cancer deaths. Due to its increasing incidence, particularly in the most developed countries it represents a great challenge for primary prevention.
Objective. To explore patterns and analyze incidence trends of melanoma in Central Serbia from 1999 to 2020.
Materials and Methods. Descriptive study was done and data were obtained from the Population-based Cancer Registry of Serbia. The joinpoint regression analysis was done to assess the incidence trend of the melanoma skin: the annual percent change (APC) along with its 95% confidence interval (95% CI) was calculated.
Results. A total number of 9952 new melanoma cases were registered melanoma (5204 in males and 4748 in females) during the observed period. Males represented 52.3% of all patients, with male to female ratio of incidence 2.09:1. A non significant increasing trend of incidence in males from 1999 to 2013 with APC of 2.53% (95%CI: from -18.2 to 21.9, p=1) and significantly increasing trend from 2013 to 2020 with the APC of 11.29 % (95%CI: from 1.4 to 5.8, p<0.001) was established. An incidence trend in females has stabilized in the whole studied period, with APC of 0.42% (95%CI: from -3.3 to 6.8, p=0.1). Melanoma of the skin was not common before the age of 30. Out of all cases and about of 76% new cases were diagnosed in persons ≥ 50 years of age.
Conclusion. The incidence trend of new melanoma cases significantly increase in the whole population from 1999 to 2020. The significant increasing of incidence trend in males and stabilization of incidence trend in females was established. Males had significantlly higher incidence rates than femalesand over of 76% new melanoma cases were diagnosed in persons above 50 years of age.
Keywords:
incidence
; trend
; melanoma of the skin
1. Introduction
Melanoma, whose incidence has been significantly increased in the previous period of time, represents about 1% of all skin cancers [1]. Moreover, it was determined that melanoma causes about 80% of all skin cancer deaths [2]. This malignant neoplasm could develop from the existing nevus in about 30% of cases, however, more than 60% of melanomas arise de novo, from the isolated melanocytes [3,4].
According to the GLOBOCAN data there were 324,635 of new cases of melanoma and 57,043 deaths in 2020 from this tumor worldwide [1]. The age-standardized incidence rate is 3.8/100,000 for males and 3.0/100,000 for females, with cumulative lifetime risks of 0.42% and 0.33%, respectively in 2020. 150 672 new cases in 2020, close to half the global melanoma cases occurred in Europe (46.4%), followed by North America (32.4%), Asia (7.3%), Oceania (5.8%) and Latin America and the Caribbean (LAC), (5.9%), [1,2].
A male predominance in incidence was consistently observed across world regions, apart from Eastern and Western Africa as well as Northern Europe and Melanesia, where rates of melanoma in females exceeded those observed in males [5]. The highest incidence rates among males (42 per 100, 000 person-years) and females (31 per 100, 000 person-years) observed in Australia/New Zealand [7], followed by Western Europe (19 per 100, 000 person-years for males and females), North America (18 per 100, 000 person-years for males, 14 per 100 000 person-years for females), and Northern Europe (17 per 100, 000 person-years for males, 18 per 100, 000 person-years for females) with highest incidence rates in Denmark, the Netherlands, Sweden, Finland and Germany [8,9]. The European Union (EU) countries with the lowest incidence rates are Romania, Bulgaria, Cyprus, Portugal and Poland [10]. In the United States of America (USA), melanoma represents the fifth most common cancer among males and the sixth most common cancer among females [11].
It is known that the risk and the incidence of this malignant neoplasm is still low in the population of African or Asian origin and in the population with darker pigmentation [12] with the lowest incidence and mortality rates in South and Central Asia and Africa (except in the white population in the South African Republic), in Southern and in Eastern European countries [13].
The most important environmental risk factor for the appearance of melanoma is solar ultra violet radiation (UVR), [14,15] especially UVA radiation, which can influence a direct DNA damage, the production of oxidative stress, free-radical generation, and the degradation of vitamin D on the skin cells. Additionally, other risk factors for melanoma are: the number of common and atypical nevi, skin phenotype, a family history of melanoma (in 8-12% patients), actinic damage, ≥65 years of age, history of sunburns and intermittent sun exposure (especially in childhood) [16,17], additional exposure to indoor UVA and UVB and use of tanning beds [18,19]. Data from the literature indicate that infection/colonization due to Malassezia yeasts could have a possible impact on skin carcinogenesis and can be a risk factor for the melanoma occurrence on non-sun exposed body localizations (uveal melanomas, in the vulva and in the perianal/anorecatal regions) [20]. These yeasts could be responsible for alterations of melanocyte function and development of melanoma, particularly through the production of Aryl hydrocarbon receptor (AhR) agonists [21,22].
The incidence of melanoma continues to increase in Southern and Eastern Europe [23]. The incidence of melanoma is law to intermediate in the countries of the Balkan Peninsula [12,23,24] which we also proved for Central Serbia where the annual average age-standardized rate (ASR) of melanoma was 8.2 in 100,000 males and 6.8 in 100,000 females in 2020 [25]. In the Southern Europe age-standardized rate of melanoma was 9.2 in 100,000 males and 8.9 in 100,000 females in 2020 [1]. This ranks Central Serbia in the group of countries with low melanoma incidence.
Concerning the fact that the incidence of melanoma has been increasing during the recent period of time in the population of Central Serbia [26], the objective of the paper was to explore patterns and analyze incidence trend of melanoma in Central Serbia from 1999 to 2020.
2. Material and Method
2.1. Study Design
A descriptive study was conducted by analyzing data on all new melanoma cases for the population of Central Serbia, excluding the territory of Autonomous Province Vojvodina and Autonomous Province of Kosovo and Metohija, because cancer registry of Vojvodina is autonomous and data about cancer incidence and mortality for Kosovo and Metohija has been missing since 1998. The analysis was carried out based on the data extracted from the Population Cancer Registry of Central Serbia, from 1999 to 2020. Skin melanoma was coded according to the Tenth Revision of International Classification of Diseases-ICD-(codes-C43) [27]. As we have used already published data from available Yearbooks of the Institute of Public Health of Serbia the approval of Ethical Committee was not necessary.
Malignant Tumors: http://www.batut.org.rs/index.php?content=2096
Incidence and Mortality from cancer in Central Serbia:
2.2. Statistical Analysis
Crude rates, age-specific and age-standardized rates (ASRs) of incidence were calculated per 100,000 inhabitants. Rates were standardized by the Sagy [28] direct method, and the world population was used as the standard. The data about the population of Central Serbia were obtained from Censuses 1991, 2002, 2011.
Age-standardized rates (ASRs) per 100,000 persons during the period 1999-2020 were calculated using the direct method according to the World Standard Population. Data regarding population of Central Serbia were obtained from 1991, 2002, 2011 Censuses. To estimate incidence trend of melanoma with the corresponding 95% confidence interval (95%CI) joinpoint regression analysis was used: the average annual percent change (AAPC) was calculated. The optimal number of Joinpoints was identified using the Monte Carlo permutation method. For regression analyses, the Joinpoint Regression Program version 4.4.0.0. was used (available at http: //surveillance.cancer.gov/joinpoint). The trend was considered to be significantly increasing (positive change) or decreasing (negative change) when the p-value was below 0.05 (p< 0.05). Additionally, analysis was performed by sex and age. In this paper, the trend analysis included only countries with high and medium data quality.
3. Results
In observed 22-years period in Serbia a total number of 9952 new cases of melanoma (5204 in males and 4748 in females) with the annual average number of 452 new cases. Males represented 52.3% of all patients, with male- to- female ratio of incidence 2.09:1.
The significant increase of incidence trend of new melanom cases was established, y=16,77x + 259,4, R² = 0,747 in the whole population of Central Serbia, in the studied period. The incidence was the highest in 2018, 2016 and 2019 and the lowest recorded in 2006 (Figure 1).
Number of new cases and age-standardized incidence rates (per 100,000 inhabitants) of melanoma of the skin in population of Central Serbia in the observed period are in the Table 1.
The annual ASRs of incidence ranged from 3.4 (in 2006) up to 11.4 (in 2018) in males and in females ranged from 3.0 (in 2006) to 9.2 (in 2016), (Table 1).
Figure 2 presents melanoma incidence trends in men and women in Central Serbia.
A non significant increasing trend of incidence in males from 1999 to 2013 with APC of 2.53% (95%CI: from -18.2 to 21.9, p=1) and significantly increasing trend from 2013 to 2020 with the APC of 11.29% (95%CI: from 1.4 to 5.8, p<0.001) was established. An incidence trend in females has stabilized in the whole studied period, with APC of 0.42% (95%CI: from -3.3 to 6.8, p=0.1).
Based on the obtained and analyzed data, it can be pointed out that melanoma of the skin was registered in all age groups but it was not common before the age of 30. Out of all cases, 7387(76.0%) new cases of melanoma were diagnosed in persons ≥ 50 years of age with the statistical significance: (p<0.001), (Figure 3).
New cases of melanoma were registered in individuals under the age of 20 (Figure 3).
The incidence of melanoma increased by age both in men and in women. The sudden jump in incidence in men was recorded after 39 years of age and in women over 49 years of age. The highest incidence in men was at the age group 60-69 and in women above 70 years of age (Figure 3).
4. Discussion
Melanoma is the most deadly skin cancer and due to its increasing incidence, particularly in the most developed countries, it represents a great challenge for primary prevention. Despite its being less common than non-melanoma skin cancer, it is one of the most invasive and treatment-resistant skin cancer [29]. The existing therapy of melanoma is very expensive and it could be used in some patients with predisposition for the good outcome. According to the recent analyses, the burden of melanoma will continue to increase until 2030 and it is expected to determine more than double of new melanoma cases [7].
Based on our results, there is significant increasing trend of new melanoma cases in the population of Central Serbia and the incidence trend significantly increased in males since 2013 up to 2020. The incidence trend stagnats in females. Additionally, melanoma was not common before the age of 30 but it was more diagnostic in females in the aged group 20 to 39 years of age than in males. Out of all cases, more than 75.0% of new cases of melanoma were diagnosed in persons≥ 50 years of age with the statistical significance. Males had higher ASRs of incidence compared with females from 1999 up to 2020.
So far, in Europe, melanoma was the sixth most commonly diagnosed cancer in 2020 [9], and the incidence has been increasing in the Norway more than 3% annually [2], Sweden and United Kingdom [6,9,30]. The recent studies have shown that the trend of the melanoma incidience in Australia has been declining since 2005, with an annual percentage incidence change of -0.68 between the years 2005-2011 [7].
Most countries in South-Eastern Europe have lower melanoma incidence, but higher melanoma mortality rates compared to North-Western Europe [6,9,11,23,24,30]. Contrary, the South parts of the United States of America (USA) are regions with the higher rates of melanoma mortality and incidence [11].
Comparing the epidemiological data with the data from the neighboring countries, we can point out that Central Serbia has the higher average ASRs of incidence of melanoma than the ones that were reported in Montenegro (2.6 per 100,000), Greece (2 per 100,000) and Albania (1.7 per 100,000), Bulgaria, and Romania (incidence rates are under 2 per 100,000). However, the average ASR of melanoma incidence in Serbia was lower than in Croatia (8.7 per 100,000 males and 7.0 per 100,000 females) and in Slovenia (rates are up to 6 per 100, 000) [3,31].
Regarding the gender, in the studies conducted in the European countries the highest average incidence of melanoma was reported both for men and women in Denmark, the Netherlands, Sweden, Finland and Germany [2,6,9,10]. In many countries, including most European countries with low melanoma incidence rate, where Serbia belongs, the incidence of melanoma in females is higher than in males [5,8,11]. The estimates of the melanoma incidence ASRs in females vary from under 2 to over 16 per 100, 000 inhabitants [5,8,11].
The incidence of melanoma among young people in England has stabilized in recent decades, whereas it continues to increase substantially in older population [30]. Melanoma incidence has begun to decline in adolescents and adults ages 30 and younger in the USA [32]. The risk of melanoma generally increases with age and incidence is greater among older populations, with more pronounced increases in people ages 80 and older [33,34].
Younger women are more exposed to indoor UVA and UVB because they more frequently use tanning beds compared with men [14,15,16,17,18,19]. In Duch population about 25% of population use tanning beds [35] and they in the group of EU countries with highest melanoma incidence.
Higher melanoma incidence rates were our findings in men and can be explained owing to the fact that we analyzed the data from the post-war period, after bombing, which is characterized by better monitoring and reporting of this disease, followed by the preventive measures, such as the examinations of nevi, earlier detection of melanoma, enhanced public awareness through continuous education and campaigns. It is known that males are more exposed to UVR due to their job or during their free time. Furthermore, both younger and older males do not use, or if they do, they use less protective creams on the regular bases, sun protection as sunsreens or they do not use them so often as females [11,21]. The lack of concern and lack of self-detection of nevi are contributing factors.
Aging is a natural process, which is influenced by genetically determined processes, but can also be modified by the environmental factors such as UVR, air pollution, which all could be connected with the higher risk of cancer. Aging influences the weakness of specific immune defense [36]. Concerning the age of the patients, our results showed that both the incidence in middle-aged males and females continuously increased in the observed period. There were 2.9 more new melanoma cases in persons older than the age of 50, which is in agreement with the other studies [37]. Midlife is a period of life when the prevalence of multiple cancer risk factors is high and incidence rates begin to increase for many types of cancer [37,38].
Very important findings in our study were 34 (0.6%) new cases of melanoma in individuals under the age of 20. Kandolf-Sekulovic, L et al. (2012) showed that low melanoma incidence rates in central Serbia and probably other countries of South-East Europe are accompanied by a large percentage of thick tumors and a significant proportion of younger patients with thick tumors [31].
There was insufficient evidence in 2016 for clinical skin cancer screening for asymptomatic adults without a history of malignancy or skin lesions in the USA. However, adults with a family history, genetic predisposition, pertinent past medical history, or history of sun exposure and fair skin are recommended to be regularly screened [39]. A meta-analysis of 15 studies from 2017 found a clinical benefit to skin cancer screening programs [40].
A Belgian study found that lesion-directed skin exams had similar rates of detection to whole-body skin exams, which take six times longer [41]. The evidence for skin self-exam was highly variable, and performance was highly associated with spouse involvement and the availability of a wall mirror [42].
5. Conclusions
However, based on the obtained results, we can point out that Central Serbia has low incidence rates of melanoma, but the increasing trend of melanoma incidence in males and in females trend is stagnant in the last 22 years. Males had significantly higer melanoma incidence than women especially above the 50 years of age are on greater risk for melanoma.The screening for the skin melanoma does not exist in Serbia and there is need for more preventive organized check ups of population for the early discovering of melanoma. The continuous education of population about self-examination of skin and nevi regularly, the usage of sun protective products and screening of the melanoma of the skin could be successful measures in the prevention and reducing of melanoma.
Limitations of the study. In Serbia, there is still the insufficient and delayed reporting of melanoma to population-based and hospital-based cancer registries. There are no thematic registers, the complete reporting of certain cancer registry data items, including histological subtypes and primary cancer site.
Author Contributions
Conceptualization, Natasa Rancic, Danica Tiodorovic, Natasa Maksimovic and Suzana Otasevic; Data curation, Mirko Ilic, Biljana Kocic and Ilija Kocic; Formal analysis, Mirko Ilic and Biljana Kocic; Methodology, Danica Tiodorovic; Resources, Natasa Rancic and Dusan Miljkovic; Software, Ilija Kocic and Dusan Miljkovic; Supervision, Suzana Otasevic; Writing—original draft, Natasa Rancic; Writing—review & editing, Natasa Maksimovic.
Funding
No funding.
References
- Centers for Disease Control and Prevention, Skin Cancer Statistics, U.S. Cancer StatisticsWorking Group. https://www.cdc.gov/ cancer/skin/statistics/.
- Sung, H, Ferlay, J, Siegel, RL, Laversanne M, Soerjomataram, I, Jemal, A, Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71: 209-249. [CrossRef]
- Ferlay, J, Colombet, M, Soerjomataram, I, Parkin, D.M.; Piñeros, M, Znaor, A. et al. Cancer statistics for the year 2020: An overview. Int J Cancer 2021; Epub ahead of print.
- Bandarchi, B.; Ma, L.; Navab, R.; Seth, A Rasty, G. From Melanocyte to Metastatic Malignant Melanoma. Dermatology Research and Practice Volume 2010, Article ID 583748, 8 pages. [CrossRef]
- Stanga, A.; Hauschildc, A. Descriptive epidemiology of cutaneous melanoma. A treasure for generating hypotheses The Lancet Regional Health - Europe 2 (2021) 100040. [CrossRef]
- Forsea, A.M. Melanoma Epidemiology and Early Detection in Europe: Diversity and Disparities. Dermatol Pract Concept. 2020 Jun 29;10(3):e2020033. [CrossRef]
- Arnold, M.; Singh, D.; Laversanne, M.; Vignat,J.; Vaccarella, S; Meheus, F.; et al. Global Burden of Cutaneous Melanoma in 2020 and Projections to 2040. JAMA Dermatol. 2022 May; 158(5): 495–503. Published online 2022 Mar 30. [CrossRef]
- Australian Institute of Health and Welfare 2017. Cancer in Australia 2017. Cancer series no. 101. Cat. no. CAN 100. Canberra: AIHW.
- Lyth, J. Clinical-epidemiological studies on cutaneous malignant melanoma-A register approach. 2015. Linköping University Medical Dissertations No. 1428, Linköping 2015, Sweden.
- Leeneman, B.; Schreuder, K.; Carin, A. Uyl - de Groot , Alexander, C.J;. van Akkooi, D.; John, B.A.G.; Haanen, et al. Stage-specific trends in incidence and survival of cutaneous melanoma in the Netherlands (2003e2018): A nationwide population-based study. European Journal of Cancer 154 (2021) 111e119. [CrossRef]
- Howlader, N, Noone, A.M, Krapcho, M, Mille,r D, Brest, A, Yu, M et al. SEER Cancer Statistics Review, 1975-2018, National Cancer Institute. 2021 Apr 15 [cited 22 June 2021]. Bethesda, MD, based on November 2020 SEER data submission, posted to the SEER web sit. Available from: https://seer.cancer.gov/csr/1975_2018/.
- Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept 2017;7(2):1-6. [CrossRef]
- Grupta, K.A.; Bharadwaj, M.; Mehrotr R. Skin Cancer Concerns in People of Color: Risk Factors and Prevention. Asian Pac J Cancer Prev. 2016; 17(12): 5257–5264. [CrossRef]
- Leslie, K.D. Cumulative Sun Exposure and Melanoma in a Population-Based Case–Control Study: Does Sun Sensitivity Matter? Cancers 2022, 14, 1008. [CrossRef]
- Raimondi, S.; Suppa, M.; Gandini, S.. Melanoma Epidemiology and Sun Exposure. Epub ahead of print Apr 28, 2020. Acta Derm Venereol 2020; 100: adv00136.
- D’Orazio, J.; Jarret ,S.; Amaro-Ortiz, A.; Timothy, Scott. UV Radiation and the Skin. Int. J. Mol. Sci. 2013, 14, 12222-12248; [CrossRef]
- Vogel, I.R.; Strayer, G.L.; Engelman, L.; Nelson, H.H.; Blaes, HA, Anderson, E.K. et al. Sun Exposure and Protection Behaviors among Long-term Melanoma Survivors and Population Controls. Cancer Epidemiol Biomarkers Prev. 2017 Apr; 26(4):. [CrossRef]
- Geller, L.M Pan. Update on indoor tanning legislation in the United States. ClinDermatol. 2015; 33(3):387-392. [CrossRef]
- Bowmanm, D.M.; Lewis, R.C.; Lee, M.S.; Yao, C.J. The Growing Public Health Challenges of Exposure to Ultraviolet Radiation From Use of Indoor Tanning Devices in the United States. New Solut. 2015 Aug; 25(2):164-71. [CrossRef]
- Thibault, C.; Sagar, P.; Nivatvongs, S.; Ilstrup, D.M.; Wolff, B.G. Anorectal melanoma-an incurable disease? Dis Colon Rectum. 1997; 40:661–668.
- Solaz Moreno, E.; Morales, V.; Silla Búrdalo, G.; Cervera Migue, J.I; Beveridge, D.; Rayón, J.M.; Primary melanoma of the rectum: an infrequent neoplasia with an atypical presentation. Clin Transl Oncol. 2005; 7:171–173.
- Morlino, A.; La Torre, G.; Vitagliano, G.; Cammarota, A. Malignant rectal melanoma. Case report. Ann Ital Chir. 2015; 86.
- Barbaric J, Sekerija M, Agius D, Coza D, Dimitrova N, Demetriou A, et al. Disparities in melanoma incidence and mortality in South-Eastern Europe: Increasing incidence and divergent mortality patterns. Is progress around the corner? Eur J Cancer. 2016 Mar;55:47-55. [CrossRef]
- Znaor, A.; van den Hurk, C.; Primic-Zakelj, M.; Agius, D.; Coz,a D.; Demetriou, A.; et al. Cancer incidence and mortality patterns in South Eastern Europe in the last decade: Gaps persist compared with the rest of Europe. European Journal of Cancer. 2013 May:49 (7):1683-169. [CrossRef]
- Institute for Public Health of Serbia Dr. Milan Jovanovic “Batut”: Malignant tumors in Republic of Serbia 2020; Belgrade, Serbia, 2022.
- Novaković, M.; Džodić, R.; Babović, N.; Kandolf Sekulović, L.; Brašanac, D.; Ferenc, V. National Guide: Melanoma-prevention, diagnostics and treatment. Belgrade, Serbia: Grafolik d.o.o., 2019.
- World Health Organization. International Classification of Diseases and Related Health Problems, 10th Revision. Available online: www.who.int/classifications/icd/en/.
- Segi, M. Cancer Mortality for Selected Sites in 24 Countries (1950–1957); Tohoku University School of Public Health: Sendai, Japan, 1960.
- Antonijevic, A.; Rancic, N.; Ilic, M.; Kocic, K.; Stevanovic, J.; Milic, M. Trends in incidence of non-melanoma and melanoma skin cancers in central Serbia. Srp Arh Celok Lek. 2018 Jul-Aug;146(7-8):391-395. [CrossRef]
- Memona, A.; Bannistera, P.; Rogersa, I.; Sundina, J.; Al-Ayadhyb, B.; Peter W. Jamesc,W.P. et al. Changing epidemiology and age-specific incidence of cutaneous malignant melanoma in England: An analysis of the national cancer registration data by age, gender and anatomical site, 1981-2018. The Lancet Regional Health - Europe 2 (2021) 100024. [CrossRef]
- Kandolf-Sekulovic, L.; Zivkovic-Perisic, S.; Radevic, T.; Rajović, M.;D inić, M.; Zolotarevski, L. et al. Melanoma in South-East Europe: epidemiological data from the central cancer registry and clinico pathological characteristics from the hospital-based registry in Serbia. Int J Dermatol. 2012;51(10):1186–1194. [CrossRef]
- Thrift, A.P.; Gudenkauf, F.J. Melanoma incidence among non-Hispanic whites in all 50 US states from 2001 through 2015. J Natl Cancer Inst 2019. [CrossRef]
- Paulson, K.G.; Gupta, D.; Kim, T.S. Age-Specific Incidence of Melanoma in the United States. JAMA Dermatol 2020;156(1):57-64. [CrossRef]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Barsouk, A. Epidemiology of Melanoma. Med. Sci. 2021, 9, 63. [CrossRef]
- de Winter, S.; Pavel, S. Zonnebanken: onduidelijk effect op huidkankerrisico [Tanning beds: effect on skin cancer risk unclear]. Ned Tijdschr Geneeskd. 2000 Mar 4;144(10):467-470.
- Bucchi, L.; Mancini, S.; Crocetti, E.; Dal Maso, L.; Baldacchini, F.; Vattiato, R.; et al. Mid-term trends and recent birth-cohort-dependent changes in incidence rates of cutaneous malignant melanoma in Italy. Int. J. Cancer. 2021;148:835–844. [CrossRef]
- Incidence of melanoma as defined by ICD-10 codes C43, D03, in the population aged under 55 years. FACT SHEET 4.2 z December 2009 z CODE: RPG4_UVrd_E1 www.euro.who.int/ENHIS.
- Lowe, C.G.; Saavedra, A.; Reed, B.K.; Velazquez, I.A.; Dronca, S.R. et al. Increasing Incidence of Melanoma among Middle-Aged Adults: An Epidemiologic Study in Olmsted County, Minnesota, Mayo Clin Proc. Author manuscript; available in PMC 2015 April 08. [CrossRef]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Ebell, M.; Epling, J.W. et al. Screening for skin cancer US preventive services task force recommendation statement. JAMA-J. Am. Med. Assoc. 2016, 22, 652–665. [CrossRef]
- Brunssen, A.; Waldmann, A.; Eisemann, N.; Katalinic, A. Impact of skin cancer screening and secondary prevention campaigns on skin cancer incidence and mortality: A systematic review. J. Am. Acad. Dermatol. 2017, 76, 129–139. [CrossRef]
- Hoorens, I.; Vossaert, K.; Pil, L.; Boone, B.; De Schepper, S.; Ongenae, K. et al. Total-body examination vs lesion-directed skin cancer screening. JAMA Dermatol. 2016, 152, 27–34. [CrossRef]
- Weinstock, M.A.; Risica, P.M.; Martin, R.A.; Rakowski, W.; Smith, K.J.; Berwick, M. et al. Reliability of assessment and circumstances of performance of thorough skin self-examination for the early detection of melanoma in the Check-It-Out Project. Prev. Med. (Baltim) 2004, 38, 761–765. [CrossRef]
Figure 1.
Incidence trend of skin melanoma in the population of Central Serbia in the study period 1999-2020.
Figure 1.
Incidence trend of skin melanoma in the population of Central Serbia in the study period 1999-2020.
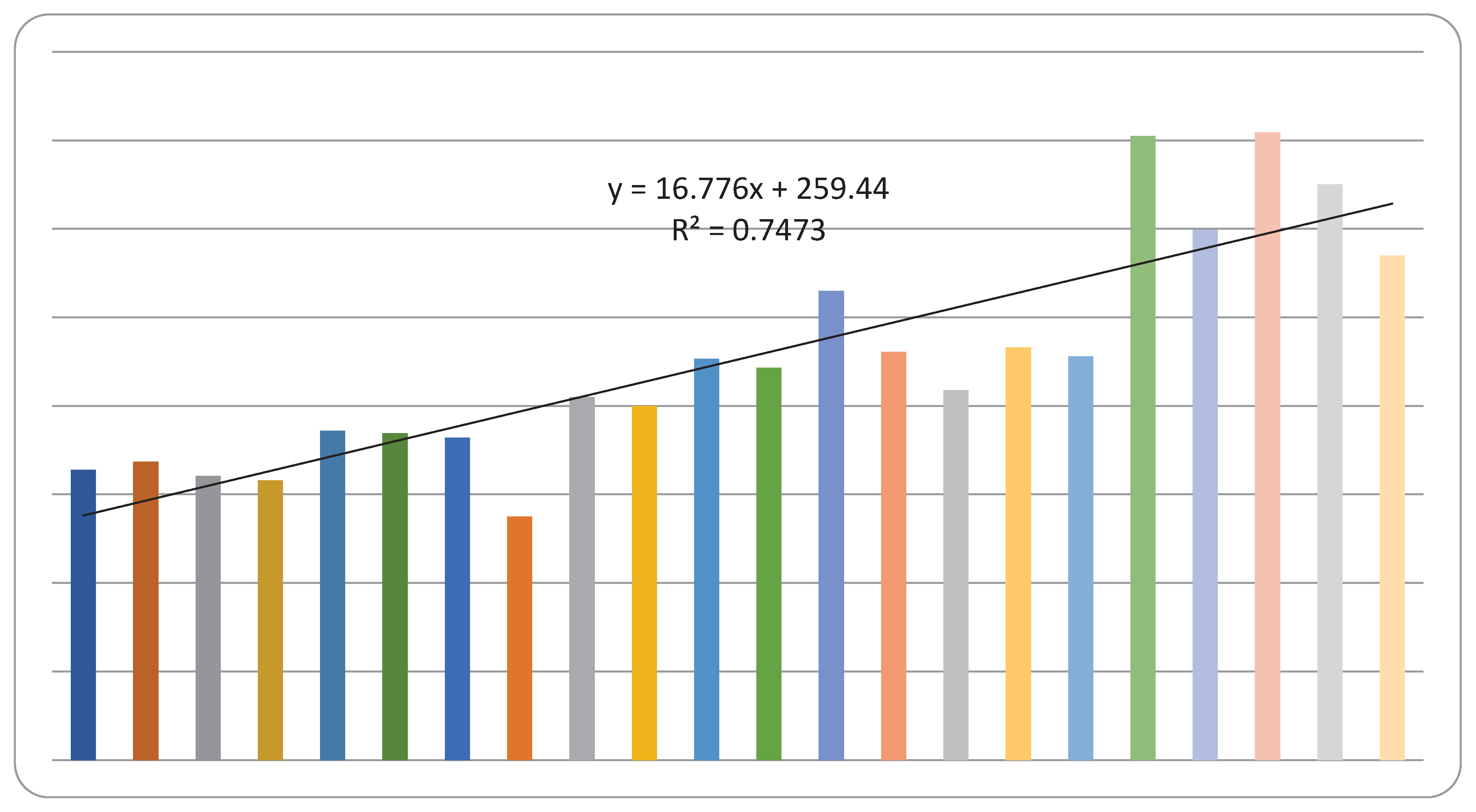
Figure 2.
The incidence trend of skin melanoma in males and in females based on the age-standardized incidence rates in Central Serbia, with the annual percentage change (APC) from to 1999-2020.
Figure 2.
The incidence trend of skin melanoma in males and in females based on the age-standardized incidence rates in Central Serbia, with the annual percentage change (APC) from to 1999-2020.
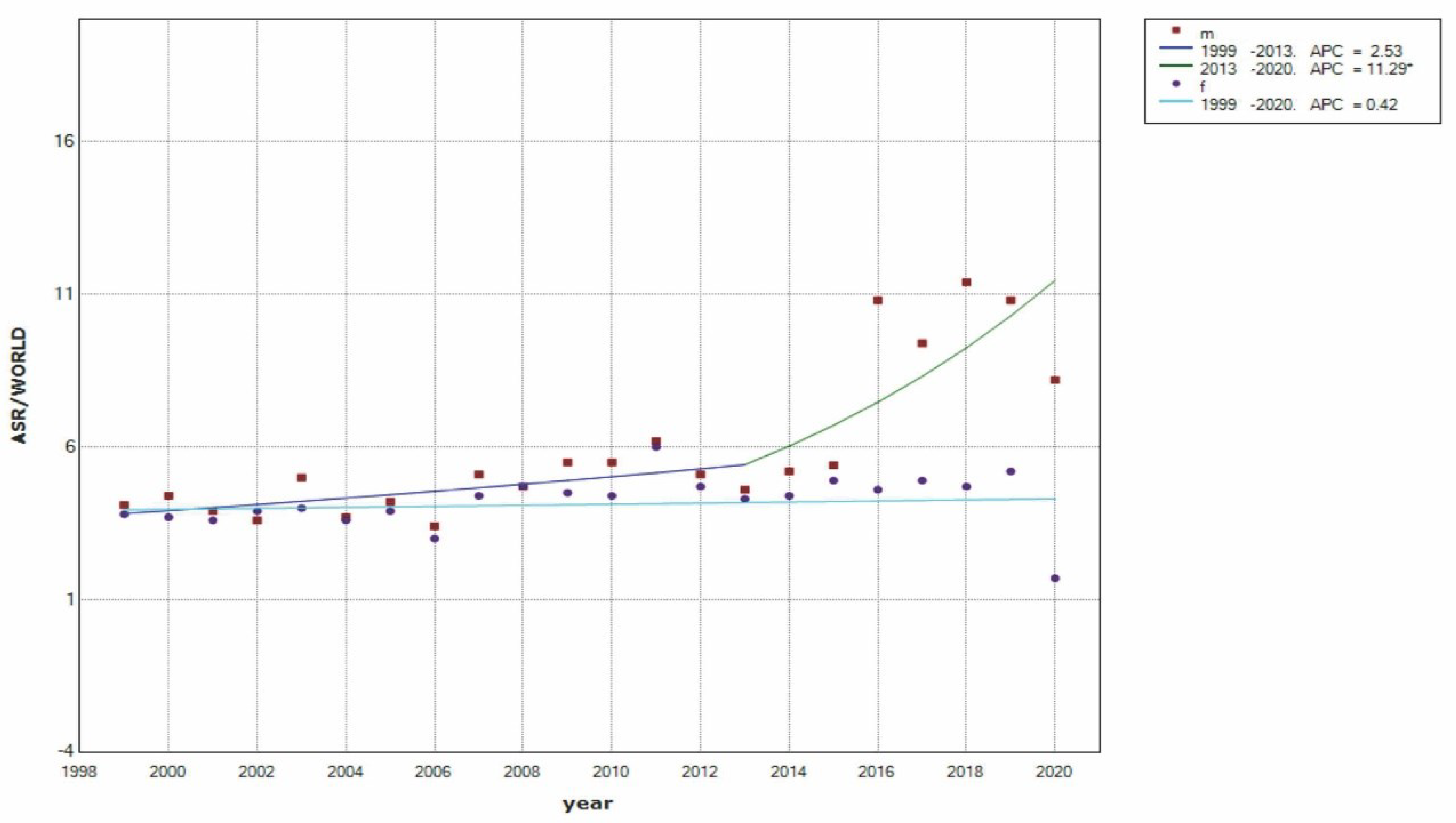
Figure 3.
Incidence trend of new melanoma cases by sex and by age in the population of Central Serbia, during the 1999-2020 period.
Figure 3.
Incidence trend of new melanoma cases by sex and by age in the population of Central Serbia, during the 1999-2020 period.
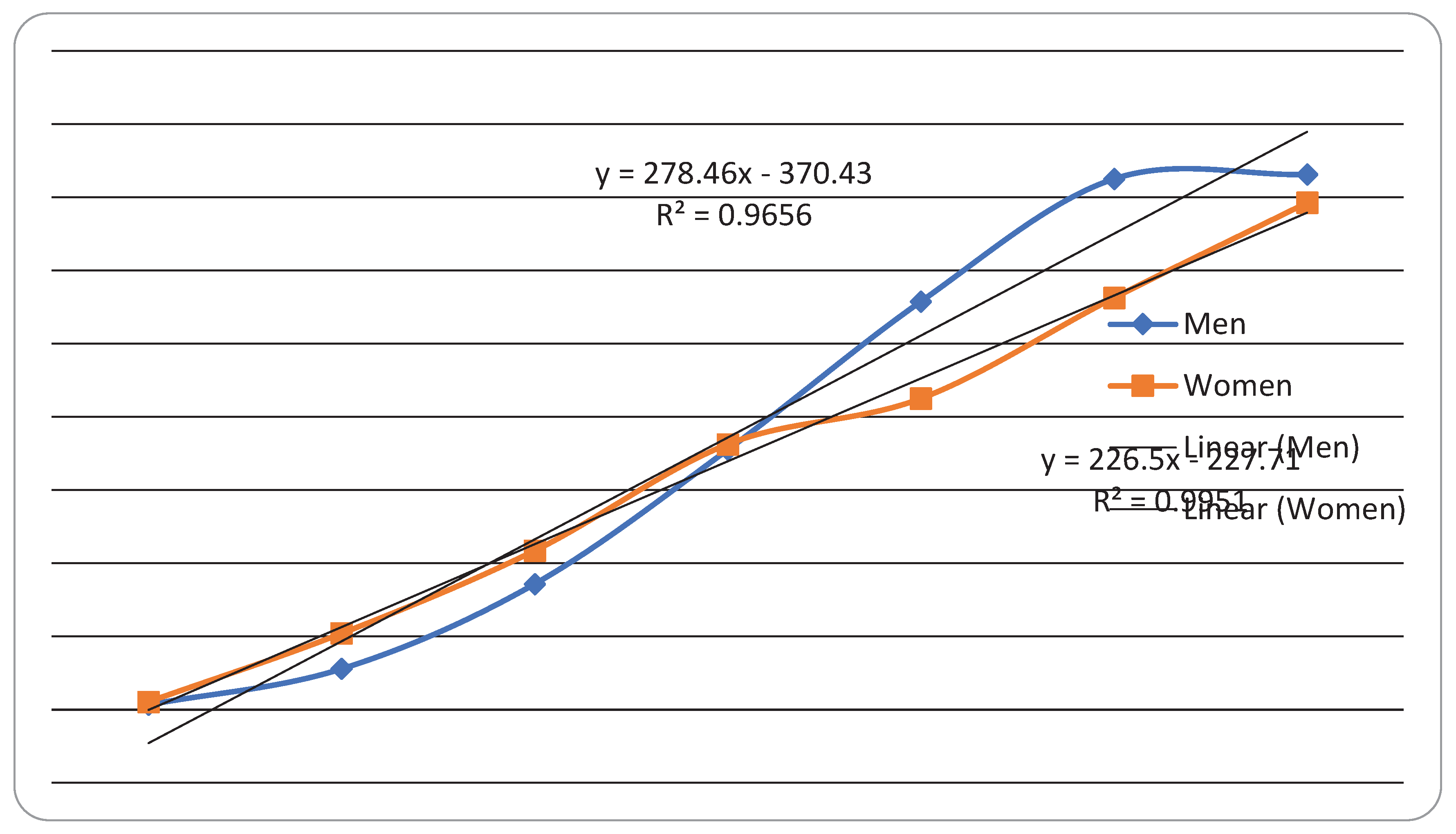

Table 1.
Number of new melanoma cases and age-standardized Incidence Rates (per 100,000 population) of skin melanoma in population of Central Serbia, 1999-2020.
Table 1.
Number of new melanoma cases and age-standardized Incidence Rates (per 100,000 population) of skin melanoma in population of Central Serbia, 1999-2020.
| Year | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| * No. of cases | Age-standardized incidence rate | No. of cases | Age-standardized incidence rate | No. of cases | ||
| 1999 | 154 | 4.1 | 174 | 3.8 | 328 | |
| 2000 | 175 | 4.4 | 162 | 3.7 | 337 | |
| 2001 | 161 | 3.9 | 160 | 3.6 | 321 | |
| 2002 | 152 | 3.6 | 164 | 3.9 | 316 | |
| 2003 | 197 | 5.0 | 175 | 4.0 | 372 | |
| 2004 | 215 | 3.7 | 154 | 3.6 | 369 | |
| 2005 | 185 | 4.2 | 179 | 3.9 | 364 | |
| 2006 | 145 | 3.4 | 130 | 3.0 | 275 | |
| 2007 | 214 | 5.1 | 196 | 4.4 | 410 | |
| 2008 | 197 | 4.7 | 203 | 4.7 | 400 | |
| 2009 | 241 | 5.5 | 212 | 4.5 | 453 | |
| 2010 | 233 | 5.5 | 210 | 4.4 | 443 | |
| 2011 | 266 | 6.2 | 264 | 6.0 | 530 | |
| 2012 | 241 | 5.1 | 220 | 4.7 | 461 | |
| 2013 | 206 | 4.6 | 212 | 4.3 | 418 | |
| 2014 | 239 | 5.2 | 227 | 4.4 | 466 | |
| 2015 | 231 | 5.4 | 225 | 4.9 | 456 | |
| 2016 | 372 | 10.8 | 333 | 9.2 | 705 | |
| 2017 | 322 | 9.4 | 277 | 7.7 | 599 | |
| 2018 | 389 | 11.4 | 320 | 8.9 | 709 | |
| 2019 | 364 | 10.8 | 286 | 8.0 | 650 | |
| 2020 | 305 | 8.2 | 265 | 6.8 | 570 | |
* No-number of cases.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



