
Submitted:
09 November 2023
Posted:
09 November 2023
You are already at the latest version
Abstract
Background: Infective endocarditis(IE) is a serious disease and in many cases surgery is necessary. Whether the type of prosthesis implanted for aortic valve replacement(AVR) for IE impacts patient survival is a matter of debate. The aim of the present study is to quantify differences in long-term survival, recurrence of endocarditis AVR for IE according to prosthesis type among patients aged 40 to 65 years. Methods: This was an analysis of the INFECT-REGISTRY. Overall, 4365 patients were diagnosed and operated on for IE from 2000 to 2021. Of these, 549 aged between 40 and 65 years underwent AVR. 268(48.8%) received mechanical prostheses, and 281(51.2%) biological ones. Confounders were adjusted using optimal full matching propensity score. Results: A significant trend in reduction of implantation of mechanical vs biological prostheses was observed during the study period(p<0.0001). Long-term survival was significantly higher among patients receiving a mechanical prosthesis than those receiving a biological prosthesis (hazard ratio [HR] 0.546,95%CI: 0.322-0.926, p=0.025). Mechanical prostheses were significantly associated with less recurrent endocarditis after AVR (HR 0.268,95%CI:0.077-0.933,p=0.039).Conclusions: The present analysis of the INFECT-REGISTRY shows increased survival and reduced recurrence of endocarditis after mechanical aortic valve prosthesis implant for IE in middle-aged patients.
Keywords:
endocarditis
; aortic valve replacement
; prosthetic heart valve.
1. Introduction
Infective endocarditis (IE) is a serious disease and in many cases surgery is necessary [1]. From a theoretical point of view, the use of foreign material should be minimized: however, when the native valve is severely compromised, a prosthetic replacement is needed [2]. For the general population with aortic valve disease, the European Society of Cardiology (ESC) suggested surgical implantation of mechanical valves in patients younger than 60 years and of bioprostheses in patients over 65 years [3]. However, there is no consensus recommendation on the type of prosthetic valve to use in case of IE, [2] and few studies compared mechanical and biological prostheses in IE patients so far, leading to contradictory results [4,5,6,7]. Furthermore, in recent years, middle-aged patients have tended to prefer biological valves to mechanical ones due to concerns related to the use of anticoagulants and the rise in valve-in-valve procedures [8]. The aim of the present study is to quantify differences in long-term survival, recurrence of endocarditis and early postoperative complications after aortic valve replacement (AVR) for IE according to prosthesis type among patients aged 40 to 65 years.
2. Materials and Methods
The ItaliaN Registry For surgical trEatment of valve and prosthesis infeCtive endocardiTis (INFECT-REGISTRY) includes surgically treated patients with IE since February 1979. The Registry is endorsed by the Italian Society for Cardiac Surgery (SICCH) with the Italian Group of Research for Outcome in Cardiac Surgery (GIROC). The ethical committee approved the study with protocol number 0009040 on 29/1/2015. Included patients met criteria for possible or definite IE diagnosis based on modified Duke criteria [9]. Only the first episode of IE recorded for an individual patient was used in the analysis. Patients with definite IE who underwent aortic valve surgery consisting of isolated biological valve replacement with stentless/stented porcine and bovine pericardial valves or of isolated mechanical valve replacement with monoleaflet or bileaflet prostheses were included. Exclusion criteria were: age < 40 years old and > 65 years old; patients undergoing valve repair rather than replacement or receiving a homograft/autograft; patients undergoing aortic root or ascending aortic replacement; patients receiving AVR combined with another valve procedure; and patients whose survival data were missing. A standard case report form was used at all sites to collect data of the index hospitalization. Clinical features including demographics, comorbidities, pre-existing valvular conditions, and details regarding the current IE episode - including source of acquisition, microbiology, echocardiographyc findings, complications, management, and outcome - were collected. All the clinical variables collected in the dataset were defined according to Euroscore [10].
From 2000 to 2021, 4365 patients with native valve endocarditis (NVE) or prosthetic valve endocarditis (PVE) were operated on in Italian Cardiac Surgery Centers (Appendix A). Of these, 549 met the inclusion and exclusion criteria mentioned above and represent the study population. The primary end-points were long-term mortality, defined as any-cause death at follow-up, and recurrence of endocarditis, defined as a diagnosis of IE in a re-admission following discharge after completion of antibiotic therapy recommended for endocarditis [2]. Secondary end-points were: duration of mechanical ventilation (MV), intensive care unit (ICU) stay, hospital stay, permanent pacemaker implantation, atrial fibrillation onset, intra-aortic balloon pump (IABP) use, perioperative stroke, acute kidney injury, reoperation for bleeding, sepsis, multiorgan failure (MOF), and early mortality (in-hospital or 30 days after surgery) due to any cause.
Statistical Analysis
Categorical data were presented as frequencies and percentages and compared using the Chi-square test or Fisher’s exact test where appropriate. Continuous variables were expressed as means with SD and compared with t test for normal distributions, and expressed as median and interquartile range [IQR] and compared using two-tailed Mann–Whitney test for non-parametric distributions. Trends in proportion of the use of mechanical prostheses versus biological ones over time were tested by applying the sieve bootstrapped t-test. Confounding due to differences in baseline characteristics was addressed using propensity score matching [11]. To calculate the propensity score, a hierarchical logistic regression model was fitted with mechanical implantation as the outcome. Covariates entered into the model include all measured baseline characteristics listed in Supplementary Table S1 in the Appendix. The area under the receiver operating characteristic curve for this model was 0.704 (Appendix, Supplementary Figure S3). Optimal full matching method, a subclassification approach that optimally forms subclasses where 1 subject is matched to 1 or more counterparts, has been used [11]. Full matching involves the formation of strata consisting of treated and control subjects and incorporates weights that are derived from the stratification. The baseline characteristics of the patient pairs matched by propensity score were compared using the Kolmogorov–Smirnov test. Standardized difference that was less than 0.1 was deemed indicative of acceptable balance. For the primary end point, survival curves estimates were derived from Kaplan-Meier method. For the other primary endpoint recurrence of endocarditis, a competing risk analysis was performed to construct cumulative incidence function curves and to calculate estimates. For all end primary points, marginal Cox proportional hazards regression models with robust sandwich variance estimators were fitted with only prosthesis type entered as a covariate. The difference in overall survival was compared using the Cox model, whereas the differences in recurrence of endocarditis were evaluated using the Gray test. Secondary endpoints were analyzed regressing the binary outcome on a treatment status indicator using a logistic regression model expressed as odds ratio (OR) and 95% confidence interval (CI). The model incorporates the weights induced by full matching. A robust, sandwich-type variance estimator has been used to account for the clustering of subjects within strata [12]. The significance level was set for an alpha value of 0.05. Statistical analyses were performed using R software (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria).
3. Results
Among the 549 patients aged between 40 and 65 years and operated on for AVR for IE, 268 (48.8%) received mechanical prostheses, and 281 (51.2%) biological ones. The baseline and operative characteristics of the overall unadjusted cohort are shown in Table 1. Patients who underwent AVR with a mechanical prosthesis were younger (median 52.00, interquartile range (IQR): 45.37- 57.56, vs median 57.00, IQR: 48.74-62.00, p <0.001), and more likely to be female (23.9% vs 14.2%, p=0.006). Patients who received biological prosthetic valves more likely had heart failure symptoms (21.0% vs 10.4%, p= 0.001), cardiogenic shock (9.6% vs 4.9%, p=0.048), and had significantly higher orotracheal intubation rates before surgery (10.0% vs 3.0%, p=0.002). Leaflet perforation (17.8% vs 10.8%, p=0.043) and large vegetation (36.3% vs 45.1%, p=0.043) were more frequent in the bioprosthesis group. Logistic Euroscore was higher (median 6.45 vs 4.68, p= 0.005), and both cardiopulmonary bypass time (90.94 min vs 79.26 min, p=0.004) and aortic cross-clamp time (73.39 min vs 65.53 min, p=0.001) were longer in patients receiving replacement with biological prostheses. Culture negative endocarditis accounted for 30.4% of cases, and the most frequently isolated germs were Streptococci (21.1%) and Staphylococcus aureus (12.9%). No significant differences were found in pathogens responsible for IE in patients undergoing AVR with mechanical vs biological prostheses (Table 2).
Mean follow-up was 65 ± 53 months.An optimal full matching propensity-score matching produced an adjusted cohort of 268 vs 281 patients. Age and all baseline comorbidities resulted in balance between groups (Appendix, Supplementary Table S1 and Figures S1–2).
3.1. Trends in AVR with Mechanical vs. Biological Valves in Middle-Aged Patients
For AVR, mechanical prostheses were less implanted than bioprostheses (268 [48.8%] vs 281 [51.2%]) among 40-to-65 years-old patients operated on for IE from January 2000 to December 2021. The mechanical versus biological prosthesis ratio (MBPR) during the entire period was 0.95. We observed a shift towards less mechanical AVR (p < 0.0001, Figure 1), to reach a MBPR of 0.73 during the last 5 years of the series. A significant trend in reduction of mechanical vs. biological prostheses implantation across time was consistent in age subclasses 40-49 years (p=0.03) and 50-65 years (p=0.02, Figure 1).
3.2. Long Term Survival
A total of 42 (15.7%) deaths occurred in the mechanical prostheses group and 66 (23.5%) deaths occurred in the bioprostheses group at follow-up; the actuarial survival at 1, 5, 10, and 15 years were 93.9%, 89.7%, 80.3%, and 70.1% in the mechanical prostheses group, and 87.5%, 78.2%, 63.9%, and 57.5% in the bioprostheses group, respectively. 2 (0.7%) deaths during follow-up occurred after major bleeding in patients who received mechanical prostheses versus 1 (0.4%) death in bioprostheses group. Only 1 patient treated with bioprothesis died after re-operation for structural valve degeneration (SVD)-related bioprosthetic valve failure, 42 months after the index operation. Among patients matched by propensity score, mid- to long-term survival was significantly higher among patients treated with a mechanical prosthesis than those treated with a biological prosthesis (hazard ratio [HR], 0.546, 95% CI: 0.322-0.926, p= 0.025; Figure 2).
3.3. Recurrence of Endocarditis
During 15-years of follow-up, the cumulative IE recurrence after AVR in our cohort was 3.8% (N=21/549), of which 2.6% (N = 7/268) and 5.0% (N = 14/281) for mechanical and biological protheses group, respectively (Figure 3). Cumulative incidence of recurrence at 1, 5, 10, and 15 years were 2.6%, 3.4%, 7.1%, and 9.5% in the mechanical prostheses group, and 1.9%, 8.6%, 14.6%, and 30.8% in the bioprostheses group, respectively. In adjusted analysis, prosthesis type was associated with recurrent endocarditis after AVR (HR 0.268, 95% CI: 0.077-0.933, p= 0.039, reference mechanical prothesis group, Figure 3). 2 out of 7 patients (28.6%) with recurrence of IE on mechanical prosthesis and 4 out of 14 patients (28.6%) with recurrence of IE on bioprosthesis underwent redo operation. 6 out of 21 (28.6%) patients with recurrence of IE died during hospitalization.
3.4. Early Postoperative Complications
Early outcomes after AVR in patients aged 40-65 years are shown in Table 3. In brief, early mortality after surgery was 6.2%. Patients with mechanical valves and bioprostheses had comparable early mortality rates (4.1% vs 8.2%, p=0.07; adjusted OR in matched cohort 0.480, 95% CI:0.229-1.005, p=0.052). Postoperative acute kidney injury (2.6% vs 7.1%, p=0.02, adjusted OR in matched cohort 0.349, 95% CI: 0.145-0.839, p=0.019) and atrial fibrillation (6.3% vs 15.6%, p=0.001, adjusted OR in matched cohort 0.362, 95%CI: 0.198-0.662, p<0.0001) onset were likely less frequent in case of mechanical valve implantation vs bioprosthesis. Other perioperative complications including need for intra-aortic balloon pump (IABP), stroke, dialysis, reoperation for bleeding, sepsis, multiorgan failure (MOF), pacemaker implantation, mechanical ventilation (MV), intensive care unit (ICU) stay, and hospital stay did not show significant differences between groups (Table 3).
4. Discussion
The main results stemming from the present analysis of the INFECT-REGISTRY data in middle-aged patients undergoing AVR for IE are the following: (1) patients tended to prefer a biological valve over a mechanical one; (2) patients treated with mechanical prostheses had greater survival and lower recurrence of endocarditis compared to those treated with biological prostheses at 15 years.
Preference of Prosthetic Valve Types in Middle-Aged Patients
IE is a serious disease associated with high mortality and morbidity [1,13]. Surgical debridement and valve repair or replacement is often required [1,13]. The cornerstone of the surgical treatment of aortic valve IE is represented by AVR with the implantation of a mechanical or biological prosthesis. The homograft implant is less used and with inconsistent results [14,15].
According to the recent ESC guidelines for the management of IE, prosthetic valve selection in IE is influenced by the presence of the following features: recent ischemic stroke, evidence of intracranial bleeding, woman of childbearing age, high likelihood of prolonged mechanical circulatory support, advanced age or frailty, poor or unknown medical compliance, expected complicated and prolonged postoperative course [2].
Beyond the aforementioned patient-specific characteristics, heart valve diseases guidelines recommend a mechanical valve replacement in patients under 60 year and a biological valve implant in patients over 65 year, claiming that also patient preference should be taken into account [2,3]. These general considerations may be even more crucial in patients under 65 years of age, since each type of prosthetic valve carries risks and benefits. Mechanical prostheses require long-lasting anticoagulant treatment, with risk of hemorrhage and thromboembolism, whereas biological valves are associated with a higher risk of failure due to structural valve degeneration (SVD) [16].
In the present study, biological substitutes were predominantly implanted in patients aged between 40 and 65 years. This complies with the study by Caus et al., according to which biological prostheses recently tended to be preferred over mechanical ones in patients between 50 and 60 years-old [17]. In this regard, our study shows a decreasing trend in the preference for mechanical prostheses both for the 40-49 years and for the 50-65 years age groups. This phenomenon seems not to be related to patient comorbidities, and is even more marked in the last 5 years. It seems that the concerns about the lifelong anticoagulation required for mechanical valve implantation outweigh the risk of failure of the bioprosthesis due to SVD. The transcatheter-based approach of valve-in-valve (ViV) to treat the failed surgical aortic valve is the primary determinant [7,18]. However, surgeons should be aware that ViV procedures should be planned during the first operation, thus implanting at least a 23 mm diameter valve. For smaller prosthetic sizes, aortic valve regurgitation and severe patient-prosthesis mismatch occur more frequently in ViV than in surgical aortic valve re-replacement [18].
Perioperative Outcomes, Long-Term Survival and Recurrence of IE after AVR for IE in Middle-Aged Patients
Studies comparing outcomes of different prosthetic valves types in AVR for EI are scarce and mostly not focused on middle-aged patients [4,5,6,7,19].
Our study showed no significant difference in early mortality among the two groups. Overall mortality was 6.2% after AVR for EI, consistent with mortality rates reported in the literature [1,19,20]. In our series, patients receiving a mechanical prosthesis had significantly lower occurrence of atrial fibrillation and acute kidney injury. It was confirmed after adjustment for propensity score. Since these results after AVR for IE have not been reported in the literature, they need further studies to be confirmed.
Contradictory results have been reported for long-term survival in patients undergoing AVR with mechanical prostheses versus bioprostheses for IE [4,5,6,20,21,22]. A propensity weighted observational study on 395 patients with left sided endocarditis in patients over 18 years of age showed lower mortality at 10 years, 51.4 ± 6.3% versus 73.7 ± 12.0%, for the mechanical valve group vs biological valve group. This study missed to analyze subgroups for aortic valve disease or age stratification [22]. Said et al. and Musci et al. in their retrospective not adjusted studies showed no difference in late survival after the implantation of biological or mechanical prostheses [23,24]. Nguyen et al. found that patients <65 years of age receiving a bioprosthetic aortic valve for IE had a significantly increased risk of 5-year mortality compared with those receiving a mechanical valve [21]. Toyoda et al. found no difference in 12-year survival among patients undergoing AVR for IE with either a mechanical or a biological prosthesis, without interaction between the age group and the prosthetic type for survival [6]. In a large retrospective observational study, Delahaye et al. found a 1-year mortality of 28.4% in the bioprostheses group and 19.7% in the mechanical prostheses group. Use of bioprostheses was independently associated with 1-year mortality, and the hazard ratio was significantly higher in patients under 65 years of age [5]. Kytö et al. selected 213 patients aged 16–70 years who underwent first-time AVR for IE with a mechanical or biological prosthetic valve in Finland, between 2004 and 2014. A significantly lower 5-year mortality with mechanical prosthesis (19% vs 35%), with HR of 0.47, 95% CI: 0.23–0.92, was reported. The association was not modified by age <60 years versus 60–70 years [4]. Our results are consistent with previous findings. In patients aged 40 to 65 years of age survival rates at 1, 5, 10, and 15 years were 93.9%, 89.7%, 80.3%, and 70.1% in the mechanical prostheses group, and 87.5%, 78.2%, 63.9%, and 57.5% in the bioprostheses group.
Mid- to long-term survival was significantly higher even in propensity matched patients treated with a mechanical prosthesis than in those treated with a biological prosthesis. In the absence of randomized controlled trials in middle-aged IE patients undergoing AVR, it is uncertain which the real cause is for this difference in long-term survival. It may be at least in part due to the need for reoperation of patients with bioprostheses. According to Chiang et al. 12.1% of patients who received biological prostheses subsequently underwent aortic valve reoperation for SVD-related bioprosthetic valve failure, compared with 6.9% of mechanical prostheses group. 30-day mortality after reoperation was 9.0%; however, efforts can be made to reduce mortality [16]. High-volume valve centers report early mortality rates of 3% to 5% for redo AVR: notably, it may be note different from mortality for primary AVR [25]. Furthermore, transcatheter valve-in-valve implantation has emerged as an alternative to redo valve surgery in high-risk patient group [26]. SVD includes a wide range of valve abnormalities such as calcification, leaflet tear, stent creep, and suture line disruption of components of the bioprosthesis, resulting in valve stenosis or incompetence, and finally to biological valve failure [27]. It is likely that the smaller effective valve area of prosthetic valves compared with normally functioning native valves produces a certain degree of left ventricular overload that could affect ventricular function over time, causing symptoms and ultimately reducing survival. A correlation between SVD and IE has also been hypothesized [28]. Conversely, SVD could mutually accelerate SVD. The assumption, which requires confirmation, is that platelet–fibrin complex formation on damaged endothelium and subsequent establishment of non-bacterial thrombotic endocarditis is an essential component of bacterial adherence and eventual infiltration [28]. There is no demonstration of the above, however, our study has shown that patients aged between 40 and 65 years undergoing AVR for IE have less recurrence of endocarditis at follow-up after the implantation of a mechanical prosthesis. Similar results are reported by the few studies published in the literature on the recurrence of infective endocarditis in biological vs mechanical prostheses. According to Rubino et al. the need for valve reoperation due to recurrent PVE occurred in 7.3% of patients after mechanical valve replacement and in 17.3% after bioprosthetic valve replacement [22]. Havers-Borgersen et al. showed that the risk of IE recurrence was significantly higher among patients with biological prostheses than among the ones receiving mechanical prostheses (6.3% vs 4.6%). On the contrary, Toyoda et al. failed to show a difference between the prosthesis types after 12 years of follow-up in IE patients [6]. Again, randomized studies on the topic are needed to confirm or refute these findings.
Study Limitations
Our study has some limitations. The first is the retrospective observational nature of the analysis, which may imply differences in surgical and medical treatment over a 21-year period. In order to minimize the differences between the analyzed groups, full propensity score matching was applied. Second, this is an analysis of a registry not primarily dedicated to the assessment of the objectives of the present study. For instance, we do not have a complete follow-up on reoperations for biological valves for SVD. Similarly, we are not aware of all major bleeding events related to mechanical valves. However, information on reoperations due to SVD-related bioprosthetic valve failure or recurrent IE, and on deaths after reoperation or major bleeding is included in the registry. Third, standards of treatment could be different in certain centers. Finally, several guidelines were published during the study period, so we decided to cite just the current one.
5. Conclusions
Among propensity-matched patients aged 40 to 65 years who underwent AVR for IE, mechanical prosthesis implantation was associated with significant survival benefit and reduction in IE recurrence. These findings suggest that mechanical valves are a reasonable choice for patients aged 40 to 65 years in this setting. Nonetheless, real-world data show that the majority of patients nowadays prefer a biological prosthesis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, A.S. and F.S.; methodology, A.S.; software, A.S.; validation, A.S., M.D.M. and F.S.; formal analysis, A.S.; investigation, A.S, M.D.M., L.L., A.D.C., F.L.P., M.D.B., C.T., M.R. E.C.S., G.A.D., G.P., F.N., D.C., C.D.V., A.G., G.C., A.M., D.C., M.M., D.P., G.F., S.S., I.V., A.P.C., F.R., E.M., C.S., F.O., G.B.L., R.S., F.E., F.M., A.L., A.C., G.F., N.S., Z.S., E.V., A.P., G.M., E.V. and M.D.T.; resources, A.S., S.F., M.D.M., F.P., F.B., A.P. and R.L.; data curation, A.S., M.D.M. and F.S.; formal analysis, A.S.; investigation, A.S., M.D.M., L.L., A.D.C., F.L.P., M.D.B., C.T., M.R., E.C.S., G.A.D., G.P., F.N., D.C., C.D.V., A.G., G.C., A.M., D.C., M.M., D.P., G.F., S.S., I.V., A.P.C., F.R., E.M., C.S., F.O., G.B.L., R.S., F.E., F.M., A.L., A.C., G.F., N.S., Z.S., E.V., A.P., G.M., E.V., M.D.T. and F.S.; writing—original draft preparation, A.S.; writing—review and editing, A.S., M.D.M. and F.S.; formal analysis, A.S.; investigation, A.S., M.D.M., L.L., A.D.C., F.L.P., M.D.B., C.T., M.R., E.C.S., G.A.D., G.P., F.N., D.C., C.D.V., A.G., G.C., A.M., D.C., M.M., D.P., G.F., S.S., I.V., A.P.C., F.R., E.M., C.S., F.O., G.B.L., R.S., F.E., F.M., A.L., A.C., G.F., N.S., Z.S., E.V., A.P., G.M., E.V. and M.D.T.; visualization, A.S., M.D.M., and F.S.; formal analysis, A.S.; investigation, A.S., M.D.M., L.L., A.D.C., F.L.P., M.D.B., C.T., M.R., E.C.S., G.A.D., G.P., F.N., D.C., C.D.V., A.G., G.C., A.M., D.C., M.M., D.P., G.F., S.S., I.V., A.P.C., F.R., E.M., C.S., F.O., G.B.L., R.S., F.E., F.M., A.L., A.C., G.F., N.S., Z.S., E.V., A.P., G.M., E.V., M.D.T., F.P., F.B., A.P., R.L. and F.S.; supervision, M.D.M. and F.S.; project administration, A.S., M.D.M., F.S., F.P., F.B., A.P. and R.L. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The ItaliaN Registry For surgical trEatment of valve and prosthesis infeCtive endocardiTis (INFECT-REGISTRY endorsed by the Italian Society for Cardiac Surgery (SICCH) with the Italian Group of Research for Outcome in Cardiac Surgery (GIROC). The ethics committee of the Istituto Europeo di Oncologia and Centro Cardiologico Monzino approved the study with protocol number 0009040 on 29/1/2015.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The Italian Group of Research for Outcome in Cardiac Surgery (GIROC) for Italian Society for Cardiac Surgery (SICCH) had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgments
The authors thank Italian Society for Cardiac Surgery (SICCH) for support to research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Citro R, Chan KL, Miglioranza MH, Laroche C, Benvenga RM, Furnaz S, Magne J, Olmos C, Paelinck BP, Pasquet A, Piper C, Salsano A, Savouré A, Park SW, Szymański P, Tattevin P, Vallejo Camazon N, Lancellotti P, Habib G; EURO ENDO Investigators group. Clinical profile and outcome of recurrent infective endocarditis. Heart 2022, 108:1729-1736. [CrossRef]
- Delgado V, Ajmone Marsan N, de Waha S, Bonaros N, Brida M, Burri H, Caselli S, Doenst T, Ederhy S, Erba PA, Foldager D, Fosbøl EL, Kovac J, Mestres CA, Miller OI, Miro JM, Pazdernik M, Pizzi MN, Quintana E, Rasmussen TB, Ristić AD, Rodés-Cabau J, Sionis A, Zühlke LJ, Borger MA; ESC Scientific Document Group. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J 2023, 25:ehad193. [CrossRef]
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2022, 43:561-632. [CrossRef]
- Kytö V, Ahtela E, Sipilä J, Rautava P, Gunn J. Mechanical versus biological valve prosthesis for surgical aortic valve replacement in patients with infective endocarditis. Interact Cardiovasc Thorac Surg 2019, 29:386-392. [CrossRef]
- Delahaye F, Chu VH, Altclas J, Barsic B, Delahaye A, Freiberger T, Gordon DL, Hannan MM, Hoen B, Kanj SS, Lejko-Zupanc T, Mestres CA, Pachirat O, Pappas P, Lamas C, Selton-Suty C, Tan R, Tattevin P, Wang A; International Collaboration on Endocarditis Prospective Cohort Study (ICE-PCS) Investigators. One-year outcome following biological or mechanical valve replacement for infective endocarditis. Int J Cardiol 2015, 78:117-23. [CrossRef]
- Toyoda N, Itagaki S, Tannous H, Egorova NN, Chikwe J. Bioprosthetic Versus Mechanical Valve Replacement for Infective Endocarditis: Focus on Recurrence Rates. Ann Thorac Surg 2018, 106:99-106. [CrossRef]
- Havers-Borgersen E, Butt JH, Østergaard L, Bundgaard H, Smerup M, Bruun NE, Gislason GH, Torp-Pedersen C, Køber L, Fosbøl EL. Recurrent infective endocarditis versus first-time infective endocarditis after heart valve surgery. Clin Res Cardiol 2020, 109:1342-1351. [CrossRef]
- Caus T, Chabry Y, Nader J, Fusellier JF, De Brux JL; EpiCard investigators. Trends in SAVR with biological vs. mechanical valves in middle-aged patients: results from a French large multi-centric survey. Front Cardiovasc Med 2023, 10:1205770. [CrossRef]
- J.S. Li, D.J. Sexton, N. Mick, et al., Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000, 30:633–638. [CrossRef]
- Nashef SA, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg 1999, 16:9-13. [CrossRef]
- Zhao QY, Luo JC, Su Y, Zhang YJ, Tu GW, Luo Z. Propensity score matching with R: conventional methods and new features. Ann Transl Med 2021, 9:812. [CrossRef]
- Austin PC, Stuart EA. Estimating the effect of treatment on binary outcomes using full matching on the propensity score. Stat Methods Med Res 2017, 26:2505-2525. [CrossRef]
- Kong WKF, Salsano A, Giacobbe DR, Popescu BA, Laroche C, Duval X, Schueler R, Moreo A, Colonna P, Piper C, Calvo-Iglesias F, Badano LP, Srdanovic I, Boutoille D, Huttin O, Stöhr E, Timóteo AT, Vaskelyte JJ, Sadeghpour A, Tornos P, Abid L, Poh KK, Habib G, Lancellotti P. Outcomes of culture-negative vs. culture-positive infective endocarditis: the ESC-EORP EURO-ENDO registry. Eur Heart J 2022, 43:2770-2780. [CrossRef]
- Salsano A, Giacobbe DR, Sportelli E, Olivieri GM, Natali R, Prevosto M, Del Bono V, Viscoli C, Santini F. Aortic cross-clamp time and cardiopulmonary bypass time: prognostic implications in patients operated on for infective endocarditis. Interact Cardiovasc Thorac Surg 2018, 27:328-335. [CrossRef]
- Nappi F, Nenna A, Spadaccio C, Avtaar Singh SS, Almazil A, Acar C. The Use of the Cryopreserved Aortic Homograft for Aortic Valve Replacement: Is It Still an Option? J Cardiovasc Dev Dis. 2023,6:248. [CrossRef]
- Chiang YP, Chikwe J, Moskowitz AJ, Itagaki S, Adams DH, Egorova NN. Survival and long-term outcomes following bioprosthetic vs mechanical aortic valve replacement in patients aged 50 to 69 years. JAMA 2014, 312:1323-9. [CrossRef]
- Caus T, Chabry Y, Nader J, Fusellier JF, De Brux JL; EpiCard investigators. Trends in SAVR with biological vs. mechanical valves in middle-aged patients: results from a French large multi-centric survey. Front Cardiovasc Med 2023,10:1205770. [CrossRef]
- Raschpichler M, de Waha S, Holzhey D, Schwarzer G, Flint N, Kaewkes D, Bräuchle PT, Dvir D, Makkar R, Ailawadi G, Abdel-Wahab M, Thiele H, Borger MA. Valve-in-Valve Transcatheter Aortic Valve Replacement Versus Redo Surgical Aortic Valve Replacement for Failed Surgical Aortic Bioprostheses: A Systematic Review and Meta-Analysis. J Am Heart Assoc 2022, 11:e7965. [CrossRef]
- Savage EB, Saha-Chaudhuri P, Asher CR, Brennan JM, Gammie JS. Outcomes and prosthesis choice for active aortic valve infective endocarditis: analysis of the Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann Thorac Surg 2014, 98:806-14. [CrossRef]
- Formica, F.; Maestri, F.; Gripshi, F.; Gallingani, A.; Grossi, S.; Nicolini, F. Long-Term Outcome of Mechanical and Biological Prostheses in Patients with Left-Side Infective Endocarditis: A Systematic Review and Meta-Analysis. J. Clin. Med 2021, 10:4356. [CrossRef]
- Nguyen, D.T.; Delahaye, F.; Obadia, J.-F.; Duval, X.; Selton-Suty, C.; Carteaux, J.-P.; Hoen, B.; Alla, F. for the AEPEI Study Group. Aortic valve replacement for active infective endocarditis: 5-year survival comparison of bioprostheses, homografts and mechanical prostheses. Eur. J. Cardio-Thorac. Surg 2010, 37:1025–1032. [CrossRef]
- Rubino AS, Della Ratta EE, Galbiati D, Ashurov R, Galgano VL, Montella AP et al. Can prosthesis type influence the recurrence of infective endocar- ditis after surgery for native valve endocarditis? A propensity weighted comparison. Eur J Cardiothorac Surg 2021,60:1388–94. [CrossRef]
- Said SM, Abdelsattar ZM, Schaff HV, Greason KL, Daly RC, Pochettino A, Joyce LD, Dearani JA. Outcomes of surgery for infective endocarditis: a single-centre experience of 801 patients. Eur J Cardiothorac Surg 2018,53:435-439. [CrossRef]
- Moon MR, Miller DC, Moore KA, Oyer PE, Mitchell RS, Robbins RC, Stinson EB, Shumway NE, Reitz BA. Treatment of endocarditis with valve replacement: the question of tissue versus mechanical prosthesis. Ann Thorac Surg 2001,71:1164-71. [CrossRef]
- Potter DD, Sundt TM 3rd, Zehr KJ, Dearani JA, Daly RC, Mullany CJ, McGregor CG, Puga FJ, Schaff HV, Orszulak TA. Operative risk of reoperative aortic valve replacement. J Thorac Cardiovasc Surg 2005,129:94-103. [CrossRef]
- Attias D, Nejjari M, Nappi F, Dreyfus J, Eleid MF, Rihal CS. How to treat severe symptomatic structural valve deterioration of aortic surgical bioprosthesis: transcatheter valve-in-valve implantation or redo valve surgery? Eur J Cardiothorac Surg 2018, 54:977-985. [CrossRef]
- Flameng W, Herregods MC, Vercalsteren M, Herijgers P, Bogaerts K, Meuris B. Prosthesis-patient mismatch predicts structural valve degeneration in bioprosthetic heart valves. Circulation 2010,121:2123-9. [CrossRef]
- Kossar AP, George I, Gordon R, Ferrari G. Bacterial infiltration and bioprosthetic valve failure: Emerging diagnostics for emerging therapies. J Thorac Cardiovasc Surg 2020,159:1279-1282. [CrossRef]
Figure 1.
Trend in proportion of the implanted mechanical versus biological prostheses in the overall cohort (A), in age class 40-49 years (B), and in age class 50-65 years (C).
Figure 1.
Trend in proportion of the implanted mechanical versus biological prostheses in the overall cohort (A), in age class 40-49 years (B), and in age class 50-65 years (C).
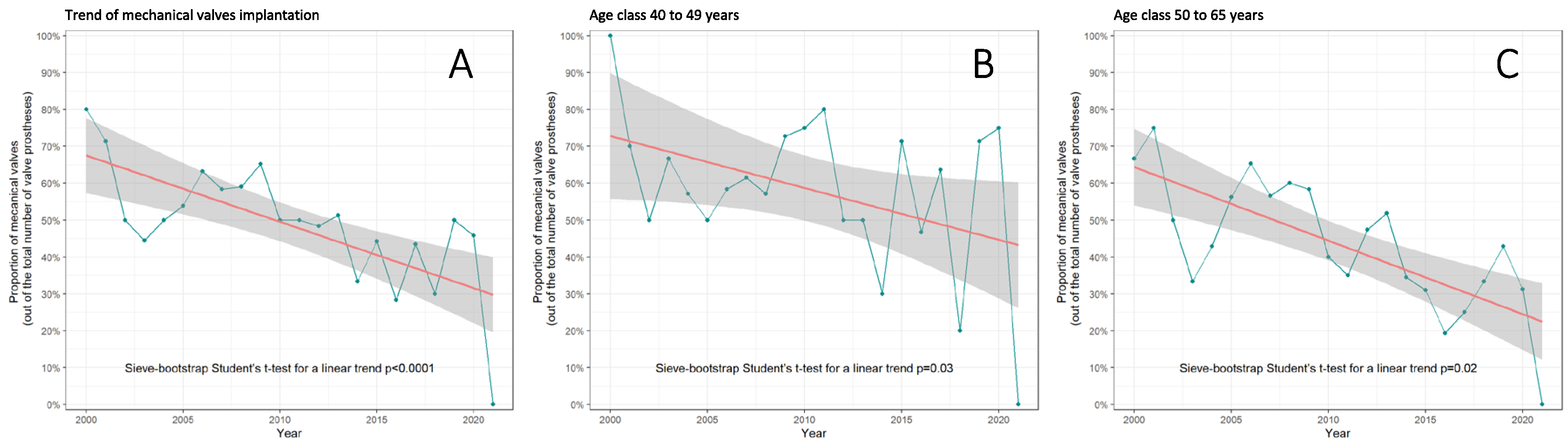
Figure 2.
Fifteen-year survival after AVR for IE patients aged 40 to 65 years according to prosthetic type: mechanical prostheses (green line) or bioprostheses (red line). Adjusted survival in patients matched by propensity score has been reported as hazard ratio (HR) and 95% confidence interval (CI).
Figure 2.
Fifteen-year survival after AVR for IE patients aged 40 to 65 years according to prosthetic type: mechanical prostheses (green line) or bioprostheses (red line). Adjusted survival in patients matched by propensity score has been reported as hazard ratio (HR) and 95% confidence interval (CI).
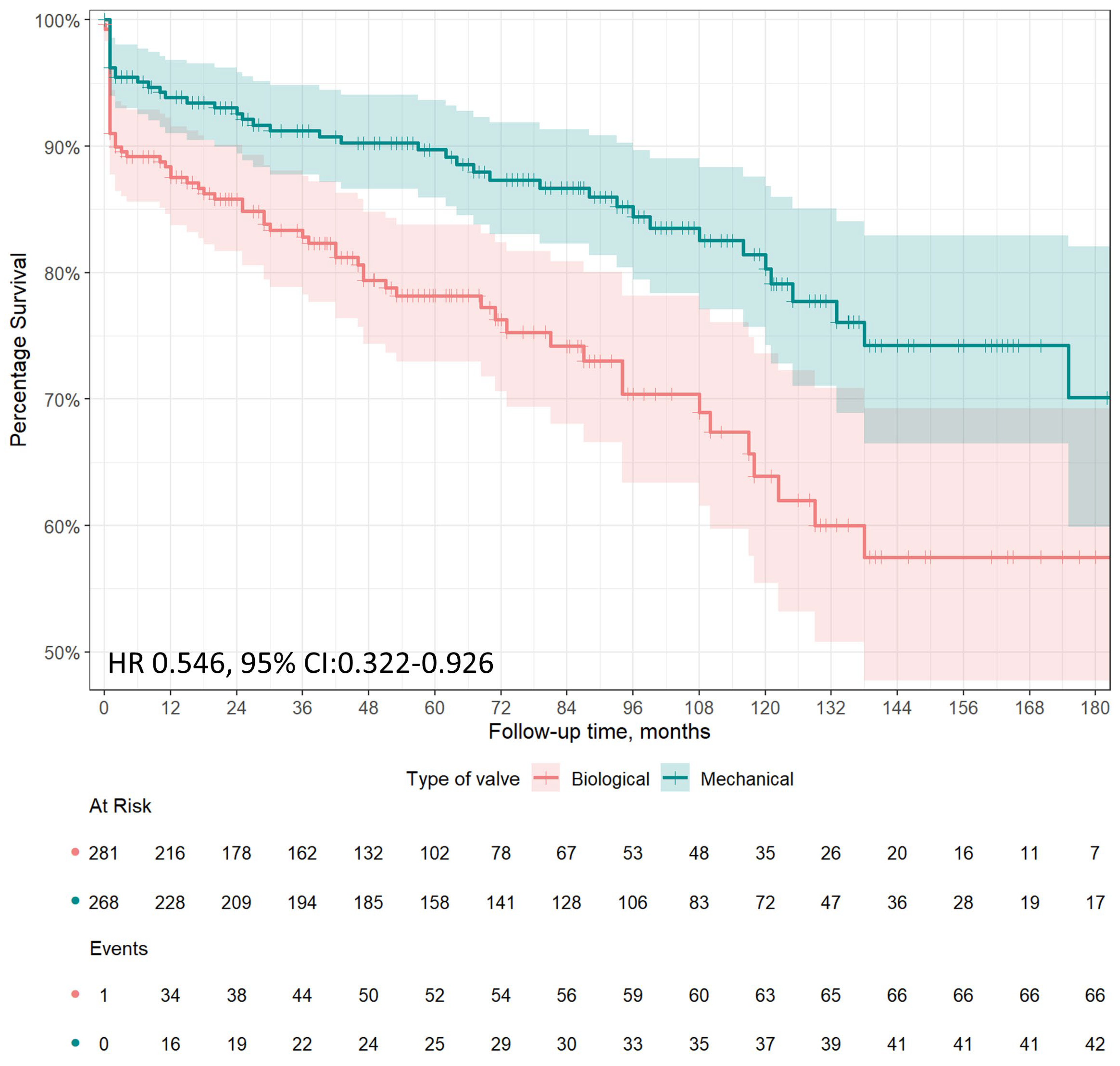
Figure 3.
Cumulative incidence of recurrent endocarditis after aortic replacement in IE patients aged 40 to 65 years according to prosthetic type: mechanical prostheses (green line) or bioprostheses (red line). Adjusted estimates in patients matched by propensity score has been reported as hazard ratio (HR) and 95% confidence interval (CI).
Figure 3.
Cumulative incidence of recurrent endocarditis after aortic replacement in IE patients aged 40 to 65 years according to prosthetic type: mechanical prostheses (green line) or bioprostheses (red line). Adjusted estimates in patients matched by propensity score has been reported as hazard ratio (HR) and 95% confidence interval (CI).
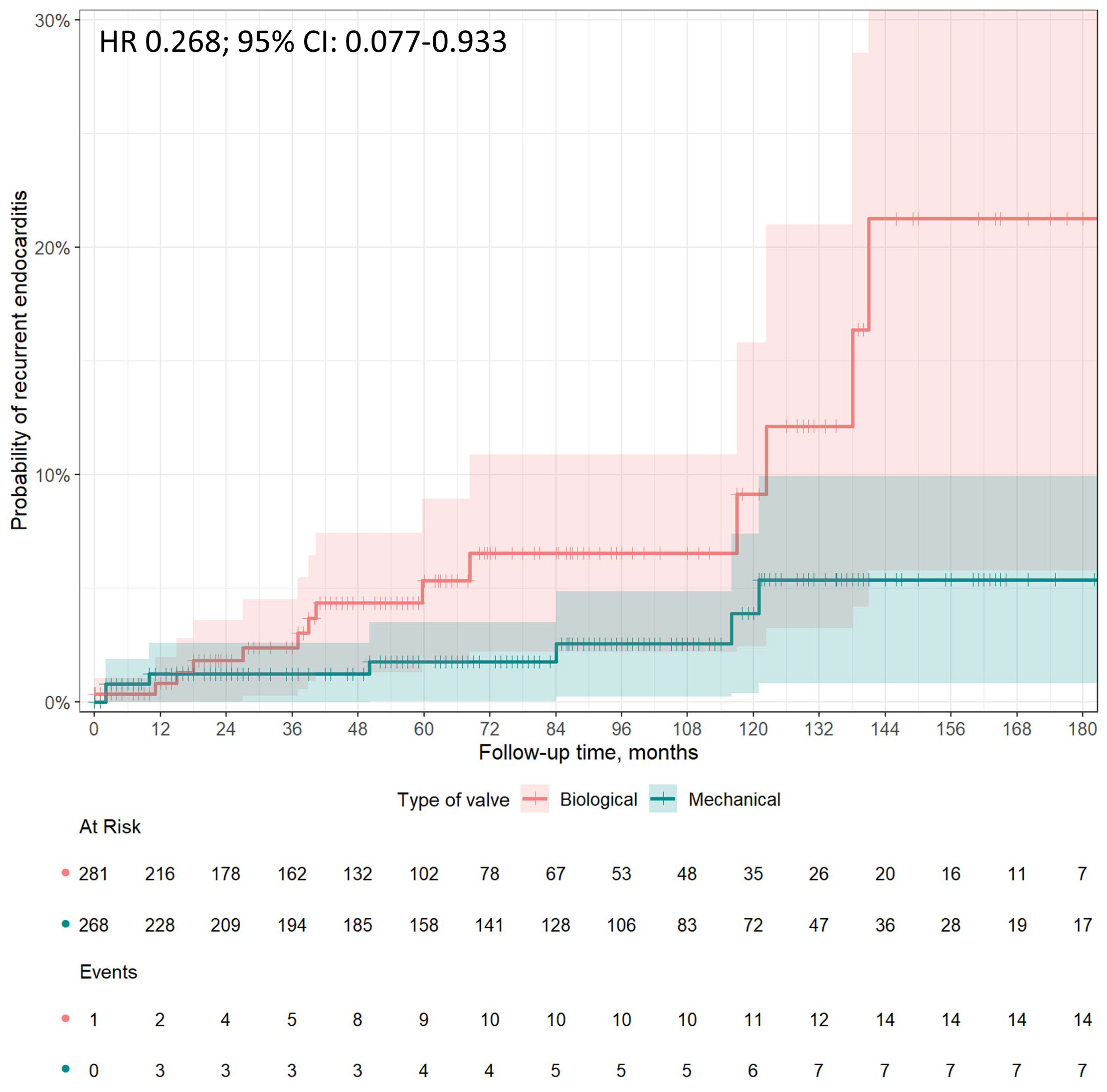

Table 1.
Baseline and operative characteristics of patients, aged between 40 and 65 years, with IE treated with mechanical versus biological aortic valve prosthesis.
Table 1.
Baseline and operative characteristics of patients, aged between 40 and 65 years, with IE treated with mechanical versus biological aortic valve prosthesis.
| Variables | Mechanical Valve (N=268) |
Biological Valve (N=281) |
p Value |
|---|---|---|---|
| Age (years, median [IQR]) | 52.00 [45.37, 57.56] | 57.00 [48.74, 62.00] | <0.001 |
| Female gender, n (%) | 64 (23.9) | 40 (14.2) | 0.006 |
| Hypertension, n (%) | 64 (23.9) | 75 (26.7) | 0.510 |
| Diabetes, n (%) | 23 (8.6) | 32 (11.4) | 0.341 |
| Obesity, n (%) | 18 (6.7) | 22 (7.8) | 0.736 |
| COPD, n (%) | 13 (4.9) | 16 (5.7) | 0.802 |
| Drug abuse, n (%) | 14 (5.2) | 13 (4.6) | 0.900 |
| Previous cardiac surgery, n (%) | 8 (3.0) | 14 (5.0) | 0.330 |
| LVEF (%, mean (SD)) | 54.94 (8.45) | 54.22 (9.47) | 0.346 |
| Peripheral arteriopathy, n (%) | 8 (3.0) | 13 (4.6) | 0.436 |
| Preoperative stroke, n (%) | 30 (11.2) | 34 (12.1) | 0.843 |
| Heart failure, n (%) | 28 (10.4) | 59 (21.0) | 0.001 |
| Cardiogenic shock, n (%) | 13 (4.9) | 27 (9.6) | 0.048 |
| Acute myocardial infarction (within 90 days), n (%) | 3 (1.1) | 4 (1.4) | 1.000 |
| Active endocarditis, n (%) | 205 (76.5) | 226 (80.4) | 0.309 |
| Preoperative MV, n (%) | 8 (3.0) | 28 (10.0) | 0.002 |
| Pulmonary hypertension (<50mmHg), n (%) | 15 (5.6) | 19 (6.8) | 0.697 |
| CKD, n (%) | 26 (9.7) | 28 (10.0) | 1.000 |
| Dialysis, n (%) | 11 (4.1) | 11 (3.9) | 1.000 |
| IABP, n (%) | 1 (0.4) | 5 (1.8) | 0.241 |
| Preoperative pacemaker implantation, n (%) | 2 (0.7) | 6 (2.1) | 0.317 |
| NVE, n (%) | 267 (99.6) | 281 (100) | 1.000 |
| PVE, n (%) | 1 (0.4) | 0 (0.0) | 1.000 |
| Abscess, n (%) | 27 (10.1) | 43 (15.3) | 0.088 |
| Large vegetation (>1 cm), n (%) | 121 (45.1) | 102 (36.3) | 0.043 |
| Leaflet perforation, n (%) | 29 (10.8) | 50 (17.8) | 0.027 |
| Paravalvular leak, n (%) | 1 (0.4) | 1 (0.4) | 1.000 |
| CABG, n (%) | 0.367 | ||
| 0 | 257 (95.9) | 265 (94.3) | |
| 1 | 9 (3.3) | 12 (4.3) | |
| 2 | 1 (0.4) | 4 (1.4) | |
| ≥3 | 1 (0.4) | 0 (0.0) | |
| Logistic Euroscore (median [IQR]) | 4.68 [2.78, 8.90] | 6.45 [3.62, 13.61] | 0.005 |
| Cardiopulmonary bypass time (min, mean (SD)) | 79.26 (33.47) | 90.94 (49.47) | 0.004 |
| Aortic cross-clamp time (min, mean (SD)) | 63.53 (23.62) | 73.39 (34.97) | 0.001 |
CABG, coronary artery bypass grafting; CKD, chronic kidney disease, COPD, chronic obstructive pulmonary disease; IABP, intra-aortic balloon pump; LVEF, left ventricular ejection fraction; MV, mechanical ventilation; NVE, native valve endocarditis; PVE, prosthetic valve endocarditis.
Table 2.
Causative agents of IE in patients treated with mechanical versus biological aortic valve prosthesis.
Table 2.
Causative agents of IE in patients treated with mechanical versus biological aortic valve prosthesis.
| Causative Agent | Mechanical Valve (N=268) |
Biological Valve (N=281) |
p Value |
|---|---|---|---|
| Culture negative endocarditis, n (%) | 84 (31.3) | 83 (29.5) | 0.714 |
| Streptococci, n (%) | 55 (20.5) | 61 (21.7) | 0.814 |
| Staphylococcus aureus, n (%) | 34 (12.7) | 37 (13.5) | 0.600 |
| Viridans group streptococci*, n (%) | 30 (11.2) | 28 (10.0) | 0.742 |
| Coagulase-negative staphylococci*, n (%) | 23 (8.6) | 20 (7.1) | 0.632 |
| Gram-negative bacteria (non HACEK), n (%) | 5 (1.9) | 9 (3.2) | 0.470 |
| Nutritionally variant streptococci*, n (%) | 2 (0.7) | 3 (1.1) | 1.000 |
| Candida spp, n (%) | 2 (0.7) | 1 (0.4) | 0.967 |
| HACEK group*, n (%) | 1 (0.4) | 0 (0.0) | 0.981 |
| Enterococcus faecalis, n (%) | 1 (0.004) | 1 (0.004) | 1.000 |
| Other organisms, n (%) | 32 (11.9) | 37 (13.2) | 0.591 |
All etiological diagnoses of surgically treated IE were made through cultures. No diagnosis was made through molecular through cultures. No diagnosis was made through molecular methods, and there were no serological diagnoses of Coxiella burnetii endocarditis in operated patients. * Viridans group streptococci included Streptococcus bovis group, Streptococcus pyogenes, Streptococcus penumoniae; Coagulase-negative staphylococci included Staphylococcus epidermidis, Staphylococcus hominis, Staphylococcus capitis, Staphylococcus haemolyticus; Nutritionally variant streptococci included Abiotrophia defectiva, Granulicatella adiacens; HACEK group included Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae.
Table 3.
Early outcomes in overall series and matched cohort of patients, aged between 40 and 65 years, with IE treated with mechanical versus biological aortic valve prostheses.
Table 3.
Early outcomes in overall series and matched cohort of patients, aged between 40 and 65 years, with IE treated with mechanical versus biological aortic valve prostheses.
| Variables | Overall Series | Estimation in Matched Cohort§ | ||||
|---|---|---|---|---|---|---|
| Mechanical Valve (N=268) |
Biological Valve (N=281) |
p Value | Odds Ratio | 95% CI | P value | |
| Early mortality, n (%) | 11 (4.1) | 23 (8.2) | 0.071 | 0.480 | 0.229-1.005 | 0.052 |
| Sepsis, n (%) | 9 (3.4) | 11 (3.9) | 0.898 | 0.849 | 0.346-2.084 | 0.722 |
| MOF, n (%) | 1 (0.4) | 7 (2.6) | 0.088 | 0.147 | 0.018-1.207 | 0.074 |
| Reoperation for bleeding, n (%) | 7 (2.6) | 11 (3.9) | 0.537 | 0.658 | 0.251-1.724 | 0.395 |
| Pacemaker implantation, n (%) | 4 (1.5) | 7 (2.5) | 0.592 | 0.591 | 0.171-2.042 | 0.406 |
| Atrial fibrillation, n (%) | 16 (6.3) | 42 (15.6) | 0.001 | 0.362 | 0.198-0.662 | <0.0001 |
| IABP, n (%) | 3 (1.1) | 6 (2.1) | 0.544 | 0.517 | 0.128-2.088 | 0.354 |
| Stroke, n (%) | 6 (2.2) | 3 (1.1) | 0.460 | 0.712 | 0.523-8.541 | 0.293 |
| Acute kidney injury, n (%) | 7 (2.6) | 20 (7.1) | 0.024 | 0.349 | 0.145-0.839 | 0.019 |
| Dialysis, n (%) | 1 (0.4) | 4 (1.5) | 0.401 | 0.261 | 0.029-2.350 | 0.231 |
| MV (hours, mean (SD)) | 23.74 (76.34) | 33.56 (82.75) | 0.315 | -9.819§ | 9.763§ | 0.315§ |
| ICU stay (days, median [IQR]) | 2.00 [1.00, 3.00] | 4.00 [2.00, 9.00] | <0.001 | -17.700§ | 13.599§ | 0.194§ |
| Hospital stay (median [IQR]) | 12.00 [8.50, 17.00] | 12.50 [8.00, 19.00] | 0.356 | -2.041§ | 1.367§ | 0.136§ |
CI, confidence interval; IABP, intra-aortic balloon pump; ICU, intensive care unit; MOF, multiorgan failure; MV, mechanical ventilation; Reference for the events: Mechanical valve cohort. § Least squares regression for continuous dependent variables has been expressed as standard regression coefficient, standard error and P value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



